new ajcc/uicc staging system...new ajcc/uicc staging system jean-pascal machiels cliniques...
TRANSCRIPT

NEW AJCC/UICC STAGING SYSTEM
Jean-Pascal Machiels
Cliniques universitaires Saint-Luc, Brussels
With the help of Brian O’Sullivan
The Princess Margaret Hospital / University of Toronto, Canada
UICC TNM Committee, and Liaison to the AJCC

DISCLOSURE SLIDE
Advisory board member or speaker with honoraria (managed by my Institution): Pfizer,
Roche, Astra/Zeneca, Bayer, Innate, Merck Serono, Boerhinger, BMS, Novartis, Janssen,
Incyte, …
Travel expenses: Amgen, BMS, Pfizer, MSD, …
Data safety monitoring board with honoraria: Debio, Nanobiotix
Institutional conflict of interest (Funding to institution for research support): all companies
Uncompensated advisory role: MSD
EORTC: investigator and study coordinator

Learning Objectives
▪ To understand background and purpose of TNM
▪ To appreciate the process of updating the TNM
▪ To discuss major changes, rationale, and caveats
concerning the 8th edition TNM

Clinical Applications of New TNM
ResearchRegistry
▪ Cancer control activities, e.g. • Time trends• Surveillance
Research
▪ Predict prognosis▪ Communication
▪ Framework for future guidelines
Clinical Care
▪ Clinical trial design▪ Comparing outcomes
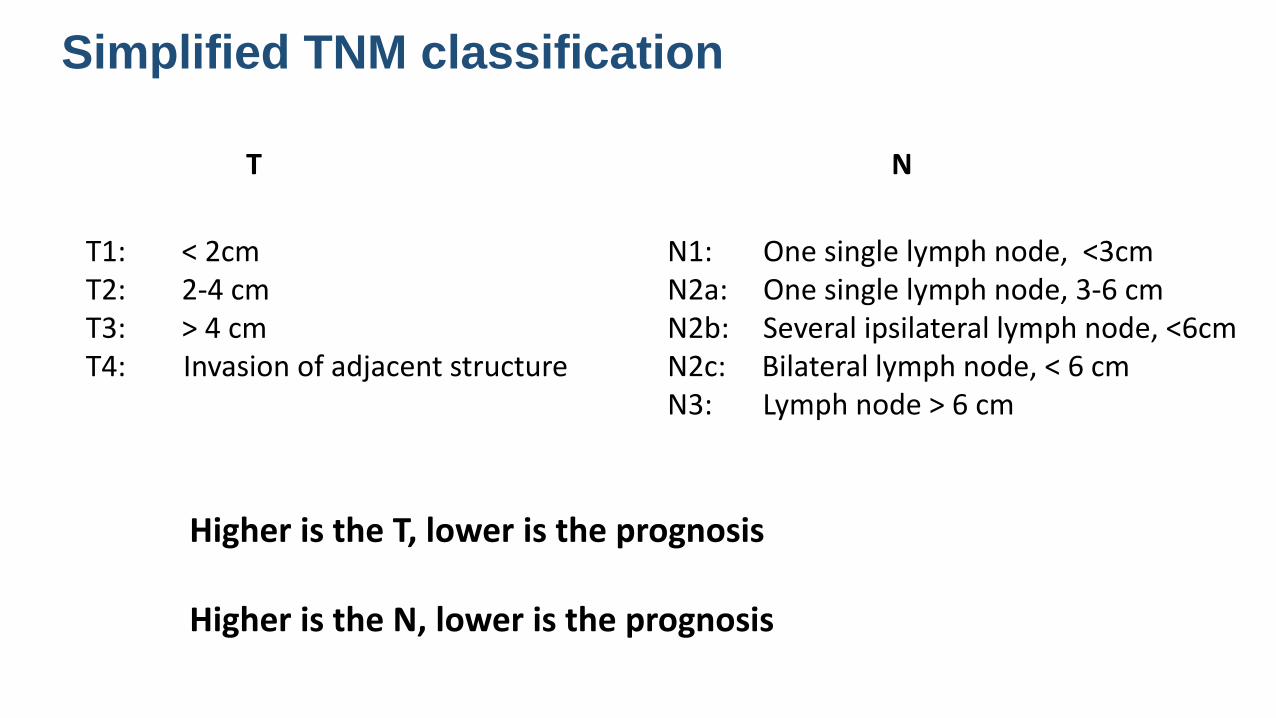
T1: < 2cmT2: 2-4 cmT3: > 4 cmT4: Invasion of adjacent structure
Simplified TNM classification
N1: One single lymph node, <3cmN2a: One single lymph node, 3-6 cmN2b: Several ipsilateral lymph node, <6cmN2c: Bilateral lymph node, < 6 cmN3: Lymph node > 6 cm
Higher is the T, lower is the prognosis
Higher is the N, lower is the prognosis
T N

Stage I: T1 Stage II: T2 Stage III: T3 or N1 Stage IVa: T4a or N2 Stage IVb: T4b or N3Stage IVc: M1
Simplified TNM classification

Reasons for Periodic Staging “Updates”
▪ Emergence of a new disease requiring new classification
• e.g. HPV+ oropharyngeal cancer
▪ Validation of new prognosis markers prompts new parameters in TNM classification
• e.g. importance of extra-nodal extension (ENE) for non-viral HNC, depth of invasion (DOI) for oral cavity SCC
▪ Improvement in tumor assessment and/or treatment triggers T-and N-classification refinement
• e.g. MRI for staging / target delineation in NPC; IMRT/chemo improved NPC outcomes
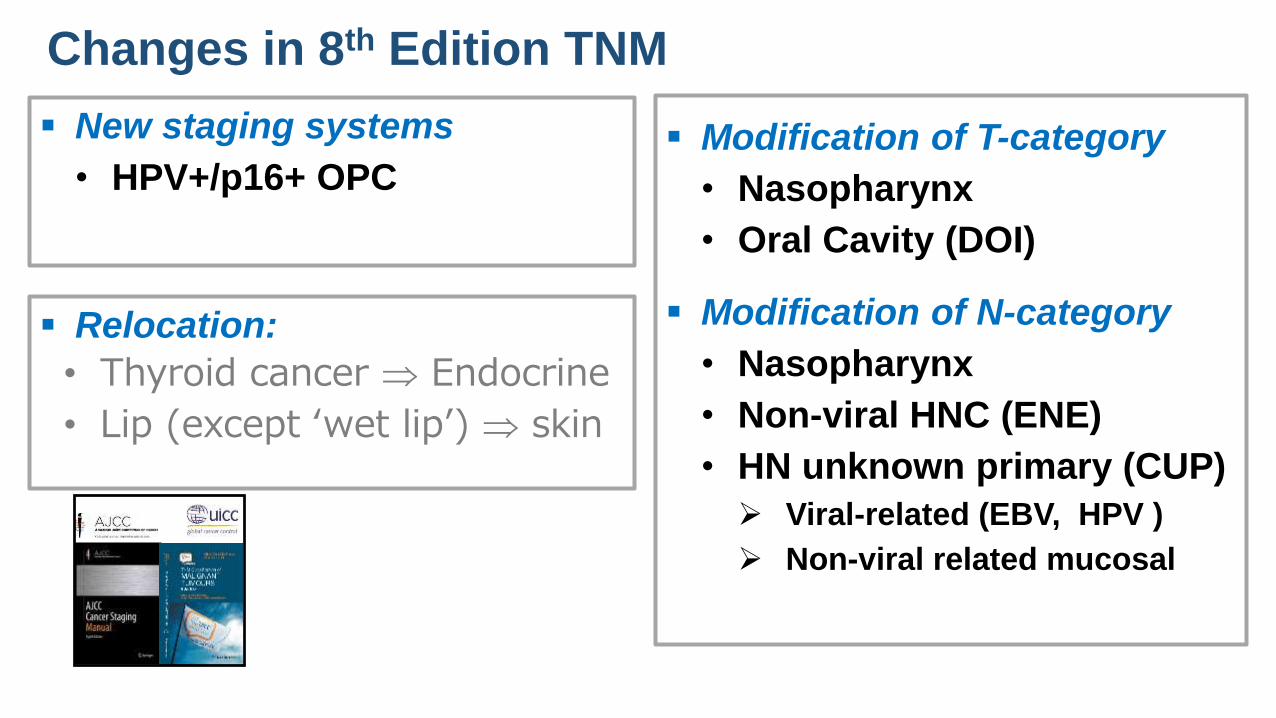
Changes in 8th Edition TNM
▪ New staging systems
• HPV+/p16+ OPC
▪ Relocation:
• Thyroid cancer Endocrine
• Lip (except ‘wet lip’) skin
▪ Modification of T-category
• Nasopharynx
• Oral Cavity (DOI)
▪ Modification of N-category
• Nasopharynx
• Non-viral HNC (ENE)
• HN unknown primary (CUP)
➢ Viral-related (EBV, HPV )
➢ Non-viral related mucosal

9
A New Classification:
HPV+ OPC / CUP
cTNM - ICON-S
pTNM

OS by 7th edition TNM Stage Groups (PMH 2000-2010)
Huang, Xu, Siu, Waldron, O’Sullivan, et al. JCO, March, 2015
HPV(–) OPC (n=237)
HPV(+) OPC (n=573)
HPV(+) Stage IV disease does not have the
same outcome than smoking-related OPC
80.4%

HPV+ OS by 7th T- & N-category (multi-institutional dataset: n=1907)
T Events/Total 5-year OS P value N Events/Total 5-year OS P value
Total 395 / 1907 80% (78-82) Total 395 / 1907 80% (78-82)
T1 60 / 504 89% (87-92) <0.001 N0 32 / 173 80% (73-87) <0.001
T2 116 / 716 83% (80-87) N1-N2a 59 / 416 87% (83-90)
T3 106 / 412 76% (72-81) N2b 136 / 749 83% (80-86)
T4a 93 / 231 58% (51-65) N2c 112 / 436 74% (70-79)
T4b 20 / 44 57% (44-75) N3 56 / 133 59% (51-69)
O’Sullivan, Huang et al 2016
N3
N2c
T4b
T4a
Unilateral Neck LNs, <6 cm
Bilat/contralatNeck LNs, <6 cm
ICON-S Study: Canada, with international collaboration from Europe and USA for validation
T4

Training Cohort (n=661)5-year OS: 85%5-year OS: 78%5-year OS: 53%
Validation Cohort (n=1246)
5-year OS: 88%5-year OS: 81%5-year OS: 65%
ICON-S StudyO’Sullivan, Huang
et al 2016
ICON-S Study: Canada, with international collaboration from Europe and USA for validation
N1 = unilateral lymph node; N2 = Bilateral lymph node; N3: > 6 cm
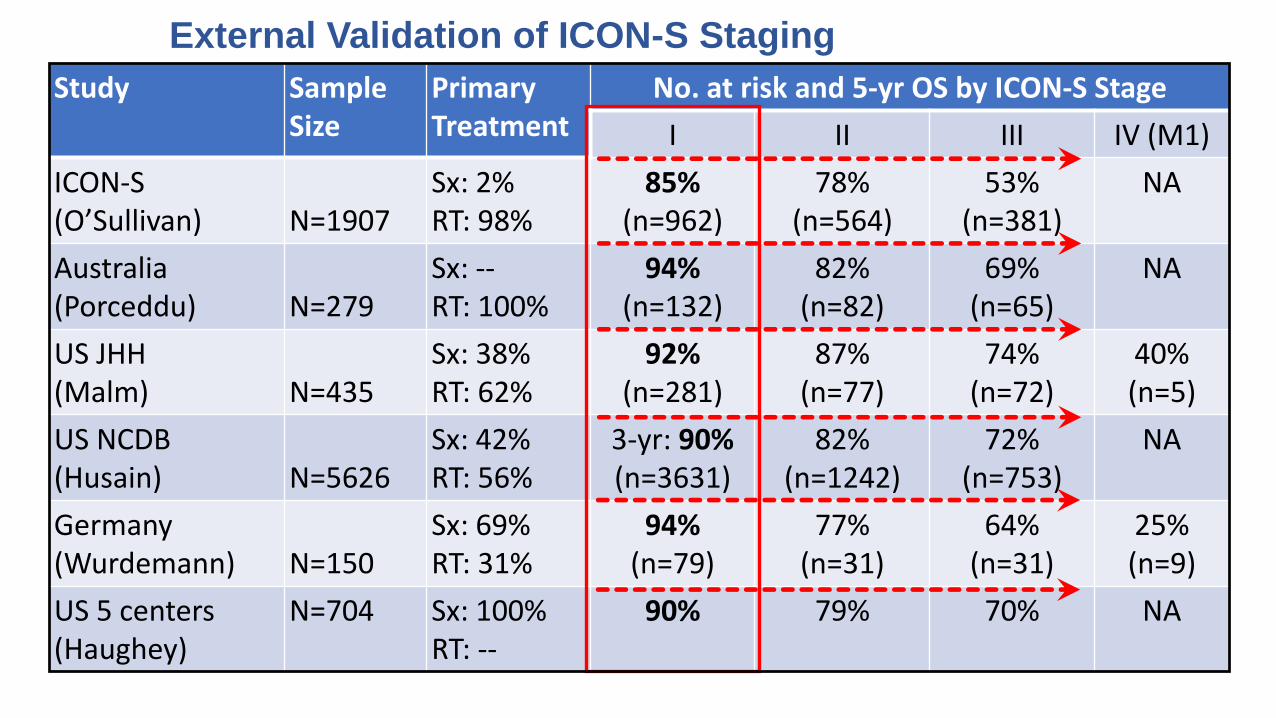
External Validation of ICON-S Staging
Study Sample Size
Primary Treatment
No. at risk and 5-yr OS by ICON-S Stage
I II III IV (M1)
ICON-S(O’Sullivan) N=1907
Sx: 2%RT: 98%
85%(n=962)
78% (n=564)
53% (n=381)
NA
Australia(Porceddu) N=279
Sx: --RT: 100%
94%(n=132)
82%(n=82)
69%(n=65)
NA
US JHH(Malm) N=435
Sx: 38%RT: 62%
92%(n=281)
87%(n=77)
74%(n=72)
40%(n=5)
US NCDB(Husain) N=5626
Sx: 42%RT: 56%
3-yr: 90%(n=3631)
82%(n=1242)
72%(n=753)
NA
Germany (Wurdemann) N=150
Sx: 69%RT: 31%
94%(n=79)
77%(n=31)
64%(n=31)
25%(n=9)
US 5 centers(Haughey)
N=704 Sx: 100%RT: --
90% 79% 70% NA

Comments About HPV+ cTNM (clinical)
▪ The 8th ed HPV+ cTNM reflects prognosis with current treatment
• Many received intensified treatment (even stage 1)
• Treatment modification may influence
▪ Stage I disease does very well
• Stage I could be considered de-intensification trial candidates

Derivation of HPV+ pTNM
OS (UVA) N (%) HR p
pT1 (7th)
pT2
pT3
pT4
279 (40)
290 (41)
92 (13)
43 (6)
1.00
1.77 (1.08-3.05)
2.67 (1.38-5.16)
5.69 (2.67-11.31)
0.039
0.004
<0.001
pN0 (7th)
pN1
pN2a
pN2b
pN2c
pN3
44 (6)
91 (13)
141 (20)
337 (48)
52 (7)
39 (6)
1.00
0.89 (0.23-3.47)
1.24 (0.35-4.40) 1.89 (0.59-6.08)
3.56 (1.01-12.65)
2.70 (0.64-11.31)
0.870
0.737
0.285
0.049
0.174
pENE(-)
pENE(+)
233 (35)
427 (65)
1.00
1.61(0.98-2.63) 0.060
≤4 pN+
≥5 pN+
589 (84)
115 (16)
1.00
2.93 (0.21-0.53) <0.001
Definition of pN
pN0 No regional LNs
pN1 ≤4 pN+ LNs
pN2 ≥5 pN+ LNs
Haughey el al Oral Oncology 2016
MVA: adjusting for age, treating centers, and treatment

• 3745 HPV+ OPC in NCDB
• All had ND in 2010-2014• pT0 4%; pT1: 47%; pT2: 39%; pT3: 7%, pT4: 3%
• pN0 4%, pN1: 76%; pN2: 13%
• 4-yr OS: I: 92%; II: 81%; III: 62%
2017
OS by 7th Edition Stage OS by 8th Edition Stage
Zhan et al Oral Oncol2017

• Presence of pENEappeared to be prognostic within HPV+ pN1 and pN2
NDCB Data - Influence of ENE within pN1, pN2
OS: pN1(by pENE)
OS: pN2(by pENE)

8th Edition cTNM and pTNM for HPV+ OPC / CUP
cTNM 1-4 LNs ≥5 LNsUnilat Bilat
Huang, O’Sullivan Curr Treat Options in Oncol. 2017
Lydiatt, Patel, O’Sullivan et al, CA Cancer J Clin. 2017
pTNM

Rationale for Revising a Stage Classification
Better understanding of disease behavior
Introducing new parameters in TNM classification
19
Extranodal Extension (ENE) in the N Classification for All Non-
viral HNC (United States, Canada)
Depth of Invasion (DOI) in Oral Cavity
(Australia, Asia, Europe, America)

Extranodal extension (ENE)
Pathological ENE
Low power High powercENE/rENE
▪ pENE is prognostically important for regional failure and distant metastasis
▪ pENE is an important indicator for adjuvant concurrent chemotherapy with radiotherapy (Level 1 evidence: pooled analysis of EORTC 22931 and RTOG 9501)
Major pENE (pENE (ma)(> 2 mm from the nodal capsule)
>2 mm
AJCC TNM 8th Edition

Extranodal extension (ENE) (for non-viral HNC)
▪ OS in surgically treated HNSCC based on N classification that incorporate pENE as a
prognostic factor. (NCDB Data 2010-2011 excluding NPC and HPV+ OPC).
OS by pN status(NCDB Data: All sites)
N0
N1
N3A
N2a, N2b, N2c
N3B
Return to the 4th edition
Formerly N1
Formerly N2a, N2c
CLINICAL N-categories (cN)
PATHOLOGICAL
cENE: invasion of skin, infiltration of musculature, fixation to adjacent structures on clinical examination, cranial nerve or brachial plexus invasion with dysfunction
Formerly N1
PATHOLOGICAL N-categories (pN)
Formerly N2a, N2b, N2c

Measuring DOI
A “plumb line” from the basement membrane of the closest intact squamous mucosa to the greatest invasion
DOI on a Exophytic Tumor DOI on an Ulcerated Tumor
Lydiatt, Patel, O’Sullivan et al, CA Cancer J Clin. 2017
Horizon
Plumb Line for DOI
HorizonTT
Plumb Line for DOI
Plumb Line for DOI
Horizon

Oral Cavity –DOI Ebrahimi et al JAMA OtolaryngolHead Neck Surg. 2014)
DFS for pT1 by DOI (<5 mm vs ≥ 5 mm)P=0.01
DFS for pT2 by DOI (<10 mm vs ≥ 10 mm)p<0.001
DFS for pT3 by DOI (<10 mm vs ≥ 10 mm)P=0.004
DFS for pT4 by DOI (<10 mm vs ≥ 10 mm)P=0.11
• Retrospective analysis of 3149 OSCC from 11 cancer centers
• 1990 to 2011
• Surgery adjuvant
• Median follow-up: 40 mos
• Different models explored

Depth of invasion
TNM oral cancer, 8th edition

Rationale for Revising a Stage Classification
Better management
(treatment / assessments)
25
Revised clinical staging (T and N) for NPC
(Hong Kong, Mainland China and Canada)

NPC Stage Classification
▪ NPC management has evolved substantially
• More accurate imaging allows better delineation of tumor extent
and early detection of occult metastases
• Advances in radiotherapy with increasing conformity of tumor
coverage and sparing of non-involved structures
• Combination chemotherapy has improved tumor control and
cure rates especially for advanced locoregional disease

Contribution of imaging to
NPC Management
• Intracranial disease within
cavernous sinus (dashed
arrow)
➢ Perineural tumor through
foramen ovale (curved arrow)
➢ The solid arrow shows the
normal cavernous sinus
CORONAL
From O’Sullivan and Yu, 2010, Springer Verlag,Berlin
Heidelberg (Editors Lu, Cooper and Lee)
MRI of Skull Base


Adjacent soft tissue involvement → T2

OS for Adjacent vs Extensive Soft tissue Involvement
Extensive soft tissue involvement → T4

Change of NPC TNM from 7th to 8th Edition
2017
√
√
• The definition of lower neck lymph nodes
➢ Lymph node below “caudal border of cricoid cartilage” (replaces “below supraclavicular fossa”)
• No subdivision of N3a and N3b:
➢ T4 and N3 M0 merged as stage IVA while M1 disease is IVB
Take Home Messages Regarding HNC TNM▪ TNM is important for many elements of research, management, and surveillance
• Counselling, prognostic estimation, surveillance, research and clinical trials
• But TNM classification is NOT a treatment guideline:
➢ Treatments should not be altered based on TNM
− Numerous other factors are operational and change requires “best evidence”
▪ Important changes in TNM 8th edition:
• New disease recognised with a new clinical and pTNM (HPV+ OPC)
• Revision due to the successes in management (NPC)
• Modifications for factors used clinically (ENE and DOI)

AJCC Head and Neck Expert Panel
Robert Baatenburg deJongMargaret Brandwein-GenslerDavid BrizelJoseph CalifanoAmy ChenDimitrios ColevasStephen Edge (Editorial Representative)Matthew FuryRonald GhosseinChristine GlastonburyRobert HaddadBruce HaugheyDennis KrausQuynh LeAnne LeeWilliam Lydiatt (Vice Chair)Suresh MukherjiKishwer NehalBrian O’Sullivan (UICC)Snehal PatelJohn RidgeSimon RogersChrysaline SchmultzRaja Seethala (CAP representative)Jatin Shah (Chair)Erich SturgisRandal WeberBruce Wenig
Acknowledgement: UICC and AJCC HN Expert Panel

Erratum in one of the Manuals
or any single contralateral node with ENE+
Erratum needed

Derivation cTNM for HPV+ OPC/CUP
PMH 2000-2010• HPV+ OPC: 573• HPV(-) OPC: 237
All definitive RT
Huang, Xu, O’Sullivan, et al. JCO. 2015
DiscoveryPMH Study
- Feasibility- Statistical models - Evaluation criteria
DerivationICON-S Study
- Training-validation- Derivation of a cTNM
7 Centers 1907 HPV+ Patients• Training (PMH): n=661• Validation: n=1246
RT: 98%; Surgery: 2%
O’Sullivan, Huang, Xuet al. Lancet Oncol 2016
External Validation
Various Datasets
1.Porceddu Oral Oncol 20172.Husain Cancer 20173.Malm, Fakhry Cancer 20174.Wurdemann Front Oncol 2017
1.Brisbane: n=2792.NCDB Data: n=56263.Johns Hopkins: n=4354.Giessen (Germany): n=150

Discovery
- LN No. (≤4 vs ≥5) was prognostic
Derivation
A multicenter study (incorporating LN # pragmatically)
External Validation
Pathologic (post-surgical) pTNM for HPV+ OPC
Washington University• HPV+ OPC: n=220• TLM +/- adjuvant RT
Sinha et al Oral Oncol 51: 154-520, 2015
5 Centers (USA & UK) 704 Patients• TORS/TLM: 100%• pT1-2: 81%; pN0-2b: 87%
Haughey et al Oral Oncol 62:11-19, 2016
Zhan, et al, Oral Oncol73:152-159, 2017
Zhan: NCDB Database• N=3745• Surgery 2010-2014
• For refinement of post-surgical reporting and framework to facilitate post-surgical management • Cases first need to be classified by cTNM