new drug evaluation: lesinurad tablet, oral - orpdl.org€¦ · allopurinol or febuxostat . ......
TRANSCRIPT

© Copyright 2012 Oregon State University. All Rights Reserved
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 | Fax 503-947-1119
Author: Dave Engen, PharmD Date: May 2016
New Drug Evaluation: lesinurad tablet, oral Date of Review: May 2016 End Date of Literature Search: April 2016 Generic Name: lesinurad Brand Name (Manufacturer): Zurampic® (AstraZeneca) PDL Class: Gout AMCP Dossier Received: Yes Research Questions: • What are the differences in efficacy between lesinurad and other antigout agents at reducing acute attacks of gout, either when treated alone or
concomitantly with another anti-gout agent? • What are the differences in harms between lesinurad and other antigout agents when used to prevent acute attacks of gout? • Are there any subpopulations based on demographics (age, race, gender, etc.) or comorbid conditions or concomitant drugs that lesinurad has
demonstrated greater efficacy/effectiveness or less harm than other anti-gout agents? Conclusions: • There is insufficient comparative evidence from 3 unpublished trials that lesinurad is superior to existing antigout agents when used in combination with
allopurinol or febuxostat. • There is low quality evidence that the use of lesinurad 200 mg and 400 mg once daily in combination with at least 300 mg of allopurinol daily demonstrates a
statistically significant higher proportion of patients able to reduce serum uric acid <6mg/dL versus placebo over 6 months [Les200+allo: RR 0.26 (95% CI, 0.17 to 0.36), p=<0.0001 and RR 0.32 (95% CI, 0.23 to 0.41), p=<0.0001; Les400+allo: RR 0.31 (95% CI, 0.22 to 0.41) P=<0.0001 and RR 0.43 (95% CI,0.34 to 0.52), P=<0.001], and is able to achieve statistically significant mean reductions (mg/dL) in serum uric acid levels versus placebo over 6 months [Les200+allo: -1.00; 95% CI -1.35 to -0.66, p <0.001, Les400+allo: -1.23; 95% CI -1.58 to -0.89, p <0.001]; however, the clinical significance of this reduction is unknown.
• There is low quality evidence that the use of lesinurad once daily in combination with febuxostat 80 mg daily demonstrates a statistically significant higher proportion of patients able to reduce serum uric acid <5mg/dL versus placebo over 6 months in lesinurad 400 mg [RR 0.29 (95% CI, 0.17 to 0.42); p<0.0001] but not in lesinurad 200 mg [RR 0.10 (95% CI, -0.03 to 0.23), p=0.1298. Lesinurad did show statistically significant reductions in serum uric acid levels versus placebo over 6 months [Les200+FBX (-0.79 95% CI -1.28 to -0.30, p =0.002) and Les400+FBX (-1.88 95% CI -2.36 to -1.40, p <0.001)]; the clinical significance of this reduction is unknown.
• There is insufficient evidence that lesinurad in combination with a xanthine oxidase inhibitor demonstrates efficacy in reduction of gout flares, provides symptom relief, results in function improvement, or improves health-related quality of life.
• There is moderate quality evidence that lesinurad treatment is associated with an increased risk of renal adverse events, including reversible and non-reversible creatinine elevations and serious renal-related adverse events such as acute renal failure.
• There is insufficient evidence that any subgroups may benefit from lesinurad more than the general population for which it has been studied. All patients studied were adults, mostly white males with an age range 21 to 82.

Author: Dave Engen, PharmD Date: May 2016
Recommendations: • Due to limited evidence of improvement in clinically relevant outcomes and unknown long term safety risks, maintain Zurampic ® as non-preferred on
PMPDP until demonstration of benefit over existing preferred agents in this class is established. Background: Gout is an inflammatory arthritic disease initiated by monosodium urate (MSU) crystal deposition in joints and connective tissue tophi which often lead to significant pain and disability.1,2,3,4 Gout affects 3.9% of the adult US population but is most prevalent in middle-aged men and post-menopausal women.3 Chronic hyperuricemia stems from physiologic disturbances of urate metabolism and clearance which is the most important risk factor for the development of gout.1,2,3 Other risk factors for the development of gout in men include obesity, weight gain, hypertension, use of diuretic agents, and alcohol.1,2,4 Accumulation of excessive serum uric acid (SUA) may also result in a range of destructive renal complications such as urolithiasis, chronic urate nephropathy, and acute renal failure.1,2,4 The goals of gout treatment are to alleviate the pain and inflammation of acute gout attacks and to prevent gout flares and uric acid (UA) crystal deposition.1,2 The American College of Rheumatology (ACR) and European League against Rheumatism (EULAR) guidelines recommend SUA levels < 6 mg/dL (or = 6 mg/dL, EULAR) in patients with gout.1,2,5,6 Although most patients with elevations in uric acid will not develop gout, if left untreated, progression towards gout generally follows 4 stages: asymptomatic hyperuricemia, acute gout, interval gout, and chronic tophaceous gout. Pharmacologic therapy for gout is typically initiated for acute attack.7 Non-steroidal anti-inflammatory drugs (NSAIDs), colchicine, or corticosteroids have been used to control the symptoms of acute gout. NSAIDs and colchicine are commonly used to relieve associated inflammation and pain but do not affect urate excretion or metabolism.7,8,9 Corticosteroids such as the oral glucocorticoid prednisone are used as an alternative to NSAIDs or colchicine in patients with renal impairment or risk of hemorrhage. 7,8,9 The management of chronic gout is largely based upon effective control of SUA concentrations.7,8,9 Elevated serum urate levels (>7 mg/dL in men; >6 mg/dL in women) are related to purine metabolism defects, under-excretion of uric acid, amplified nucleic acid turnover, or hyper-synthesis of purine.1,2 Three main pharmacologic mechanisms are targeted for gout treatment: management of hyperuricemia through reduction of uric acid production, increased urate secretion through reabsorption inhibition, or by enhanced enzymatic breakdown of uric acid.7,8,9 Xanthine oxidase inhibitors (XOIs) such as allopurinol and febuxostat represent the mainstay of chronic gout therapy.7,8,9 XOIs are utilized to manage overproduction and/or underexcretion of urate and by the inhibition of xanthine to uric acid conversion. 7,8,9 Probenecid, a second-line uricosuric agent, inhibits uriate transporters (URAT) in the proximal renal tubules to prevent UA reabsorption and accelerate uric acid excretion.9 Other agents such as pegloticase and rasburicase are recombinant enzymatic proteins used to catalyze the oxidation of urate to allantoin.9,10 These enzymes are typically reserved for individuals unresponsive or intolerant to XOIs or uricosuric therapy.9,10 Lesinurad (Zurampic®) is a new agent proposed to increase excretion of UA through inhibition of URAT1 transport proteins in a mechanism similar to probenecid. 9,10
Author: Dave Engen, PharmD Date: May 2016
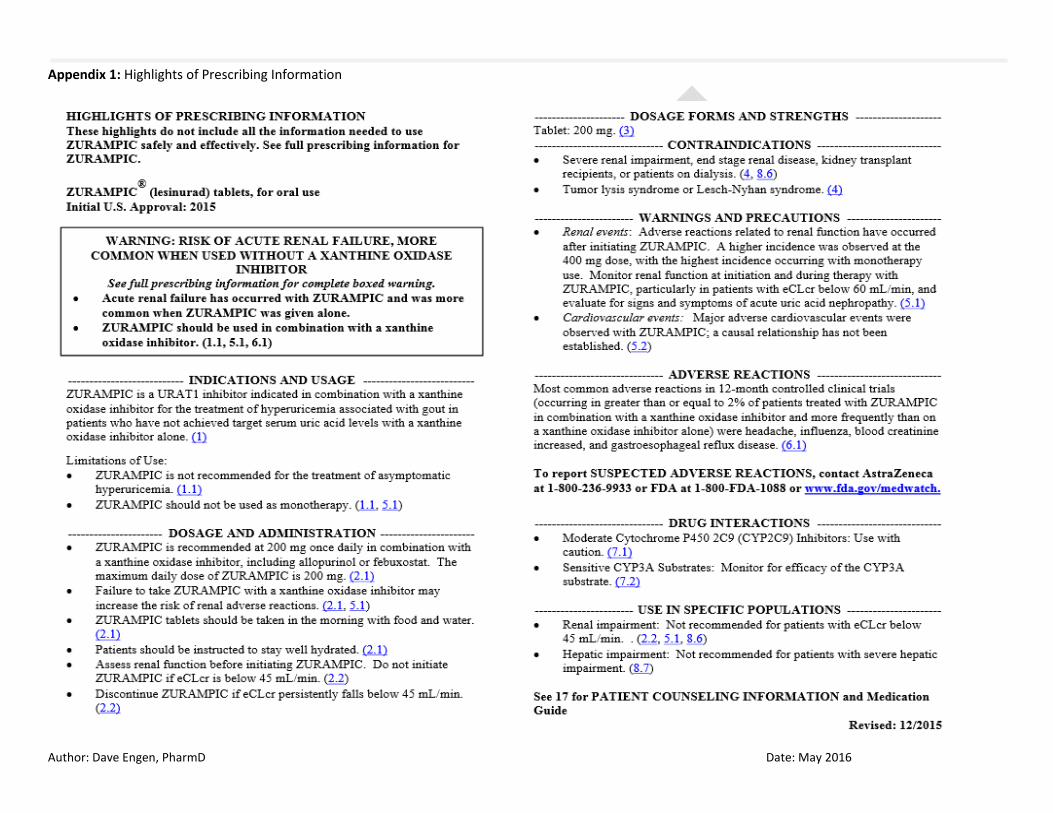
See Appendix 1 for Highlights of Prescribing Information from the manufacturer, including Black Boxed Warning and Risk Evaluation Mitigation Strategies (if applicable), indications, dosage and administration, formulations, contraindications, warnings and precautions, adverse reactions, drug interactions and use in specific populations. Clinical Efficacy: Approval for lesinurad was based on 3 unpublished Phase III, double-blind, randomized, placebo-controlled clinical trials (Studies 301, 302, and 304)11 that compared lesinurad plus a background xanthine oxidase inhibiting (XOI) agent to active placebo plus a XOI over 12 months. Study 303 investigated the efficacy and safety of lesinurad monotherapy but were later dropped by the manufacturer for renal safety concerns. 11 The effectiveness of lesinurad was evaluated based on the proportion of gout patients who achieved goal a pre-defined serum uric acid reduction at month 6.11 All studies were conducted in adults between 22-82 years with inadequate hypouricemic response to a stable dose of a XOI. Patients were instructed to take lesinurad at the same time each day in the morning with their XOI. For gout flare prophylaxis, patients received colchicine or NSAIDs +/- proton pump inhibitor through month 5 in each of the studies. Patients with significant cardiac disease (unstable angina, myocardial infarction, stroke, DVT, uncontrolled hypertension during screening, etc) or hepatic disease were excluded. Concomitant use of urate lowering medications besides allopurinol, immunomodulating agents, salicylates, or epoxide hydrolase inhibitors were prohibited. Agents with secondary uricosuric effects were not permitted. At the conclusion of the 12-month study period for each trial, patients had a 14-day follow-up.11 Study 301 was a US-based, multicenter trial (n=603) that assessed the clinical benefits, safety and serum urate-lowering ability of lesinurad plus allopurinol versus placebo plus allopurinol.11 Patients successfully screened during the initial 28-day period were randomized 1:1:1 by renal function (60 ml/min cutoff) and presence of tophi to one of the following treatment groups: Placebo plus allopurinol daily (P+allo), lesinurad 200 mg plus allopurinol daily (Les200+allo), or lesinurad 400 mg plus allopurinol daily (Les400+allo). All subjects had received 300 mg/day of allopurinol unless renal impairment (estCrCl > 45-60 ml/min) necessitated dose reduction to 200 mg/day. The primary endpoint measured was the proportion of patients with a sUA level <6.0 mg/dL at Month 6. A greater proportion of patients treated with Les200+allo and Les400+allo demonstrated a modest statistically significant response to therapy compared to P+allo (RR 0.26 (95% CI, 0.17 to 0.36), p=<0.0001 and RR 0.31 (95% CI, 0.22 to 0.41), P=<0.0001, respectively). There was no clear evidence of a dose response difference between les200+allo and les400+allo. The mean change in serum acid (mg/dL) from baseline to month 6 was statistically significant for Les200+allo (-1.00 95% CI -1.35 to -0.66, p <0.001) and Les400+allo (-1.23 95% CI -1.58 to -0.89, p <0.001). A secondary endpoint which assessed proportion of subjects requiring treatment for a gout flare during the time period from Month 6 to Month 12 was not met for either Les200+allo (P=0.98) or Les400+allo (P=0.61). Another secondary endpoint which was not met for this trial had assessed the proportion of subjects with > 1 target tophus at baseline who experienced complete resolution of at least 1 target tophus by Month 12. The results actually favored placebo for les200+allo [RR: -0.29(95% CI, -0.51 to -0.08) p=0.02] and were not significant for les400+allo (P=0.60). There were multiple secondary efficacy variables for patient reported outcomes regarding disease activity, pain, and functioning (see section on “comparative clinical efficacy” for complete listing), however, these findings were not considered statistically significant due to the hierarchical testing method used for multiple endpoints.11 Study 302 was a 12-month trial (n=610) which had an identical study design to Study 301 but also included US and multinational sites.11 The primary endpoint for this trial was also met as the proportion of patients achieving target sUA level<6.0 mg/dL by month 6 was higher in both Les200+allo and Les400+allo versus P+allo ([RR 0.32 (95% CI, 0.23 to 0.41), p=<0.0001] and [RR 0.43 (95% CI, 0.34 to 0.52), P=<0.001] respectively). Unlike trial 301, a dose-response effect between the two lesinurad groups plus allopurinol was observed. The mean change in serum acid (mg/dL) from baseline to month 6 was statistically significant for Les200+allo (-1.08 95% CI -1.41 to -0.75, p <0.001) and Les400+allo (-1.36 95% CI -1.69 to -1.03, p <0.001). A secondary endpoint which assessed proportion of
Author: Dave Engen, PharmD Date: May 2016
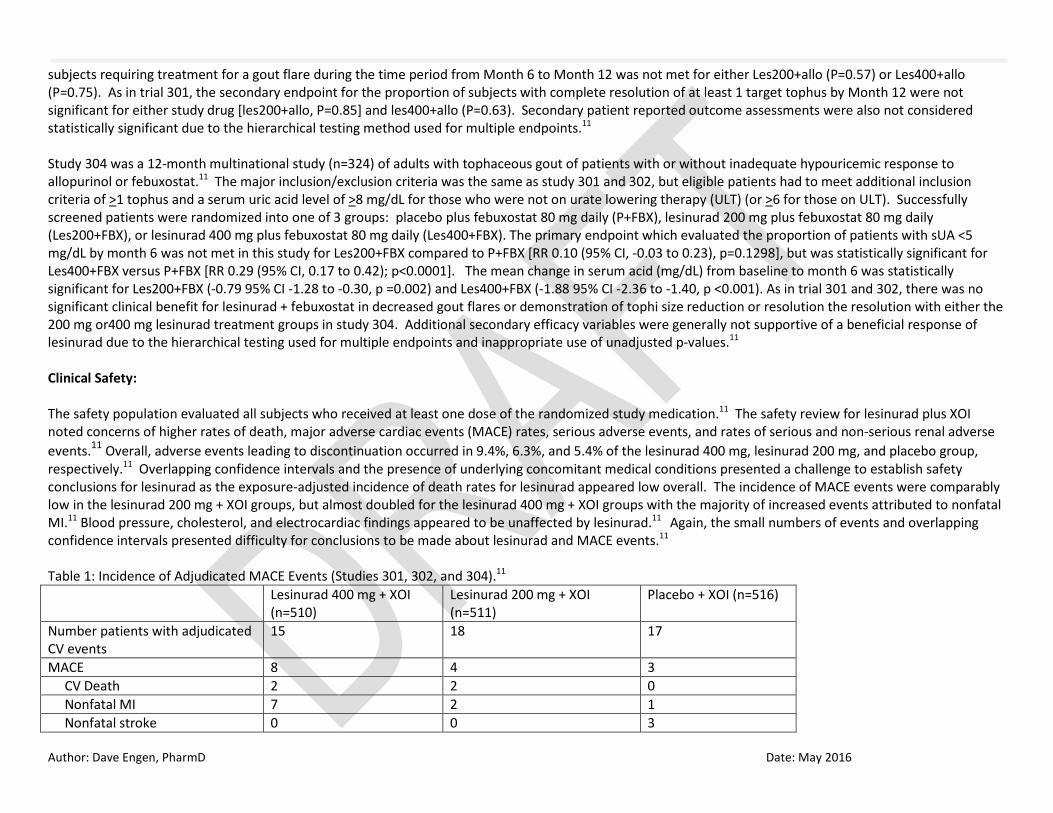
subjects requiring treatment for a gout flare during the time period from Month 6 to Month 12 was not met for either Les200+allo (P=0.57) or Les400+allo (P=0.75). As in trial 301, the secondary endpoint for the proportion of subjects with complete resolution of at least 1 target tophus by Month 12 were not significant for either study drug [les200+allo, P=0.85] and les400+allo (P=0.63). Secondary patient reported outcome assessments were also not considered statistically significant due to the hierarchical testing method used for multiple endpoints.11 Study 304 was a 12-month multinational study (n=324) of adults with tophaceous gout of patients with or without inadequate hypouricemic response to allopurinol or febuxostat.11 The major inclusion/exclusion criteria was the same as study 301 and 302, but eligible patients had to meet additional inclusion criteria of >1 tophus and a serum uric acid level of >8 mg/dL for those who were not on urate lowering therapy (ULT) (or >6 for those on ULT). Successfully screened patients were randomized into one of 3 groups: placebo plus febuxostat 80 mg daily (P+FBX), lesinurad 200 mg plus febuxostat 80 mg daily (Les200+FBX), or lesinurad 400 mg plus febuxostat 80 mg daily (Les400+FBX). The primary endpoint which evaluated the proportion of patients with sUA <5 mg/dL by month 6 was not met in this study for Les200+FBX compared to P+FBX [RR 0.10 (95% CI, -0.03 to 0.23), p=0.1298], but was statistically significant for Les400+FBX versus P+FBX [RR 0.29 (95% CI, 0.17 to 0.42); p<0.0001]. The mean change in serum acid (mg/dL) from baseline to month 6 was statistically significant for Les200+FBX (-0.79 95% CI -1.28 to -0.30, p =0.002) and Les400+FBX (-1.88 95% CI -2.36 to -1.40, p <0.001). As in trial 301 and 302, there was no significant clinical benefit for lesinurad + febuxostat in decreased gout flares or demonstration of tophi size reduction or resolution the resolution with either the 200 mg or400 mg lesinurad treatment groups in study 304. Additional secondary efficacy variables were generally not supportive of a beneficial response of lesinurad due to the hierarchical testing used for multiple endpoints and inappropriate use of unadjusted p-values.11 Clinical Safety: The safety population evaluated all subjects who received at least one dose of the randomized study medication.11 The safety review for lesinurad plus XOI noted concerns of higher rates of death, major adverse cardiac events (MACE) rates, serious adverse events, and rates of serious and non-serious renal adverse events.11 Overall, adverse events leading to discontinuation occurred in 9.4%, 6.3%, and 5.4% of the lesinurad 400 mg, lesinurad 200 mg, and placebo group, respectively.11 Overlapping confidence intervals and the presence of underlying concomitant medical conditions presented a challenge to establish safety conclusions for lesinurad as the exposure-adjusted incidence of death rates for lesinurad appeared low overall. The incidence of MACE events were comparably low in the lesinurad 200 mg + XOI groups, but almost doubled for the lesinurad 400 mg + XOI groups with the majority of increased events attributed to nonfatal MI.11 Blood pressure, cholesterol, and electrocardiac findings appeared to be unaffected by lesinurad.11 Again, the small numbers of events and overlapping confidence intervals presented difficulty for conclusions to be made about lesinurad and MACE events.11 Table 1: Incidence of Adjudicated MACE Events (Studies 301, 302, and 304).11 Lesinurad 400 mg + XOI
(n=510) Lesinurad 200 mg + XOI (n=511)
Placebo + XOI (n=516)
Number patients with adjudicated CV events
15 18 17
MACE 8 4 3 CV Death 2 2 0 Nonfatal MI 7 2 1 Nonfatal stroke 0 0 3

Author: Dave Engen, PharmD Date: May 2016
The number of serious adverse events were reported to be highest under the Metabolism and Nutritional Disorder System Organ Class but with pooled data the incidence was still 1% for both doses of lesinurad + XOI. 11 The increased risk of adverse renal events was highest with lesinurad 400 mg while lesinurad 200 mg + XOI appeared to be more similar to placebo + XOI.11 Increased blood creatinine was the most common adverse event leading to discontinuation in 1.8%, 0.8%, and 0.8% of the lesinurad 400 mg, lesinurad 200 mg, and placebo groups, respectively.11 A black box warning identifies risk of acute renal failure when lesinurad is given without concomitant XOI therapy.12 The overall summary of renal events are listed in the table below. Table 2: Incidence of Renal-related Adverse Events in Studies 301, 302, and 30411 Lesinurad 400 mg + XOI
(n=510) Lesinurad 200 mg + XOI (n=511)
Placebo + XOI (n=516)
Blood creatinine increased 11.8% 5.7% 4.5% Blood urea increased 7.8% 4.3% 2.3% Renal failure 1.2% 0.8% 1.2% Renal failure, acute 0.8% 0.0% 0.4% Nephrolithiasis 2.2% 0.6% 1.7% Other common adverse events were upper respiratory tract infection, hypertension, headache, and influenza.11 Table 3 Common Adverse Events in Studies 301, 302, and 30412 Preferred Term Placebo + XOI (n=516) Lesinurad 400 mg + XOI
(n=510) Lesinurad 200 mg + XOI (n=511)
Total Lesinurad + XOI (n=1021)
Upper respiratory tract infection
44 (8.5%) 57 (11.2%) 46 (9.0%) 103 (10.1%)
Hypertension 25 (4.8%) 35 (6.9%) 31 (6.1%) 66 (6.5%) Headache 21 (4.1%) 30 (5.9%) 27 (5.3%) 57 (5.6%) Influenza 14 (2.7%) 16 (3.1%) 26 (5.1%) 42 (4.1%) Look-alike / Sound-alike Error Risk Potential: FDA deemed Zurampic® acceptable from both a promotional and safety perspective.11

Author: Dave Engen, PharmD Date: May 2016
Pharmacology and Pharmacokinetic Properties:12 Parameter
Mechanism of Action Selective uric acid reabsorption inhibitor (SURI) that reduces the function of the URAT1 and OAT4 transporter proteins involved in renal urate reabsorption
Absorption Rapid, almost 100 % bioavailability; maximum plasma concentrations (Cmax) attained within 1 to 4 hours. Distribution and Protein Binding Vd is 20 L; >98% is bound to albumin Metabolism Oxidative metabolism mainly via CYP2C9 Half-Life Approximately 5 hours Elimination Total clearance is approximately 6 L/hr. Urine (63%; roughly 30% as unchanged drug); feces (32%).
Abbreviations: URAT = urate transporter 1; OAT = organic anion transporter; Comparative Clinical Efficacy: Clinically Relevant Endpoints: 1) Incidence of gout flares 2) Symptom relief 3) Function improvement 4) Health-related quality of life
Primary Study Endpoint: 1. Proportion of patients achieving a target serum Uric Acid level <6.0
mg/dL at Month 6 (Studies 301 & 302) or < 5 mg/dL by month 6 (Study 304)
2. Mean change in serum acid (mg/dL) from baseline to month 6 Secondary Study Endpoints: 1. Mean rate of gout flares requiring treatment between Months 6
and 12; 2. Proportion of patients with ≥1 target tophus at baseline who
experienced complete resolution of at least 1 target tophus by Month 12
3. Mean percent change from baseline in the sum of the areas for all target tophi at each visit
4. Proportion of subjects with improvement from baseline in disease-related disability as measured by self-reported questionnaires: (HAQ-DI, SF-36, TSQM, SDS, PGA)
5. Proportion of subjects whose sUA level is <6.0 mg/dL, <5.0 mg/dL and <4.0 mg/dL at each visit
6. Absolute and percent change from baseline in sUA levels at each visit
7. Proportion of subjects requiring treatment for a gout flare at monthly intervals between Month 6 and Month 12
Author: Dave Engen, PharmD Date: May 2016
Comparative Evidence Table Ref./ Study Design
Drug Regimens/ Duration
Patient Population N Efficacy Endpoints ARR/NNT
Safety Outcomes ARR/NNH Risk of Bias/ Applicability
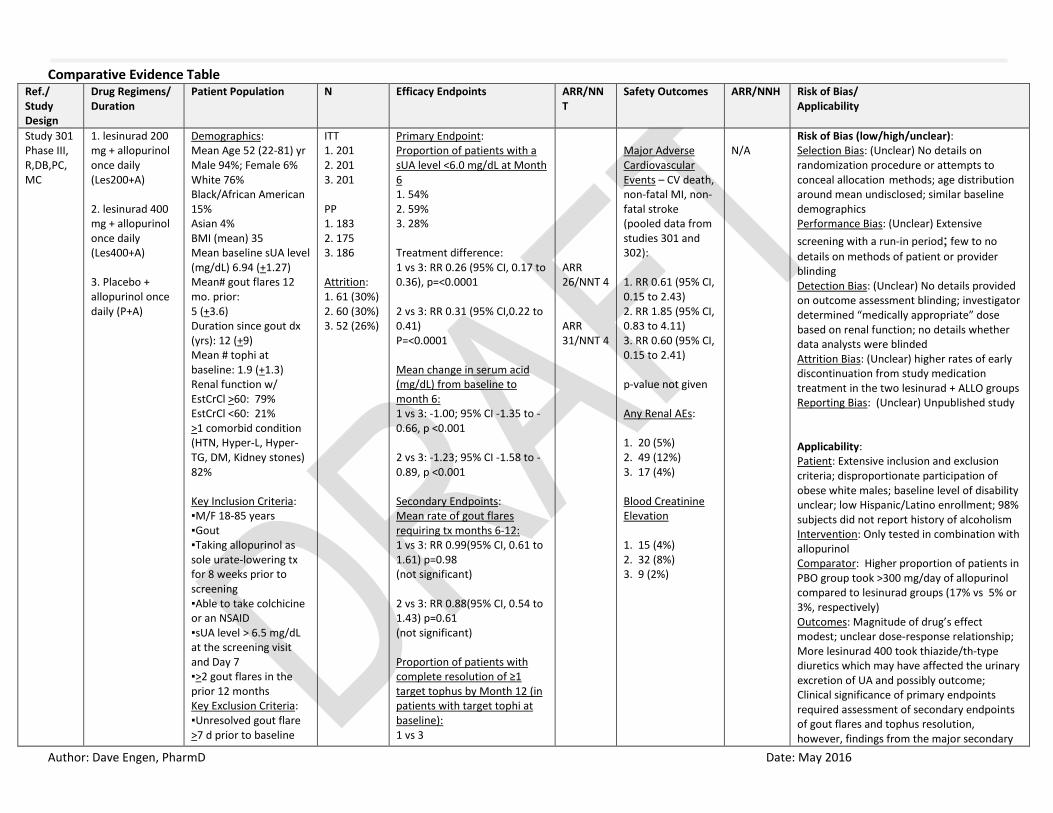
Study 301 Phase III, R,DB,PC,MC
1. lesinurad 200 mg + allopurinol once daily (Les200+A) 2. lesinurad 400 mg + allopurinol once daily (Les400+A) 3. Placebo + allopurinol once daily (P+A)
Demographics: Mean Age 52 (22-81) yr Male 94%; Female 6% White 76% Black/African American 15% Asian 4% BMI (mean) 35 Mean baseline sUA level (mg/dL) 6.94 (+1.27) Mean# gout flares 12 mo. prior: 5 (+3.6) Duration since gout dx (yrs): 12 (+9) Mean # tophi at baseline: 1.9 (+1.3) Renal function w/ EstCrCl >60: 79% EstCrCl <60: 21% >1 comorbid condition (HTN, Hyper-L, Hyper-TG, DM, Kidney stones) 82% Key Inclusion Criteria: ▪M/F 18-85 years ▪Gout ▪Taking allopurinol as sole urate-lowering tx for 8 weeks prior to screening ▪Able to take colchicine or an NSAID ▪sUA level > 6.5 mg/dL at the screening visit and Day 7 ▪>2 gout flares in the prior 12 months Key Exclusion Criteria: ▪Unresolved gout flare >7 d prior to baseline
ITT 1. 201 2. 201 3. 201 PP 1. 183 2. 175 3. 186 Attrition: 1. 61 (30%) 2. 60 (30%) 3. 52 (26%)
Primary Endpoint: Proportion of patients with a sUA level <6.0 mg/dL at Month 6 1. 54% 2. 59% 3. 28% Treatment difference: 1 vs 3: RR 0.26 (95% CI, 0.17 to 0.36), p=<0.0001 2 vs 3: RR 0.31 (95% CI,0.22 to 0.41) P=<0.0001 Mean change in serum acid (mg/dL) from baseline to month 6: 1 vs 3: -1.00; 95% CI -1.35 to -0.66, p <0.001 2 vs 3: -1.23; 95% CI -1.58 to -0.89, p <0.001 Secondary Endpoints: Mean rate of gout flares requiring tx months 6-12: 1 vs 3: RR 0.99(95% CI, 0.61 to 1.61) p=0.98 (not significant) 2 vs 3: RR 0.88(95% CI, 0.54 to 1.43) p=0.61 (not significant) Proportion of patients with complete resolution of ≥1 target tophus by Month 12 (in patients with target tophi at baseline): 1 vs 3
ARR 26/NNT 4 ARR 31/NNT 4
Major Adverse Cardiovascular Events – CV death, non-fatal MI, non-fatal stroke (pooled data from studies 301 and 302): 1. RR 0.61 (95% CI, 0.15 to 2.43) 2. RR 1.85 (95% CI, 0.83 to 4.11) 3. RR 0.60 (95% CI, 0.15 to 2.41) p-value not given Any Renal AEs: 1. 20 (5%) 2. 49 (12%) 3. 17 (4%) Blood Creatinine Elevation 1. 15 (4%) 2. 32 (8%) 3. 9 (2%)
N/A
Risk of Bias (low/high/unclear): Selection Bias: (Unclear) No details on randomization procedure or attempts to conceal allocation methods; age distribution around mean undisclosed; similar baseline demographics Performance Bias: (Unclear) Extensive screening with a run-in period; few to no details on methods of patient or provider blinding Detection Bias: (Unclear) No details provided on outcome assessment blinding; investigator determined “medically appropriate” dose based on renal function; no details whether data analysts were blinded Attrition Bias: (Unclear) higher rates of early discontinuation from study medication treatment in the two lesinurad + ALLO groups Reporting Bias: (Unclear) Unpublished study Applicability: Patient: Extensive inclusion and exclusion criteria; disproportionate participation of obese white males; baseline level of disability unclear; low Hispanic/Latino enrollment; 98% subjects did not report history of alcoholism Intervention: Only tested in combination with allopurinol Comparator: Higher proportion of patients in PBO group took >300 mg/day of allopurinol compared to lesinurad groups (17% vs 5% or 3%, respectively) Outcomes: Magnitude of drug’s effect modest; unclear dose-response relationship; More lesinurad 400 took thiazide/th-type diuretics which may have affected the urinary excretion of UA and possibly outcome; Clinical significance of primary endpoints required assessment of secondary endpoints of gout flares and tophus resolution, however, findings from the major secondary
Author: Dave Engen, PharmD Date: May 2016
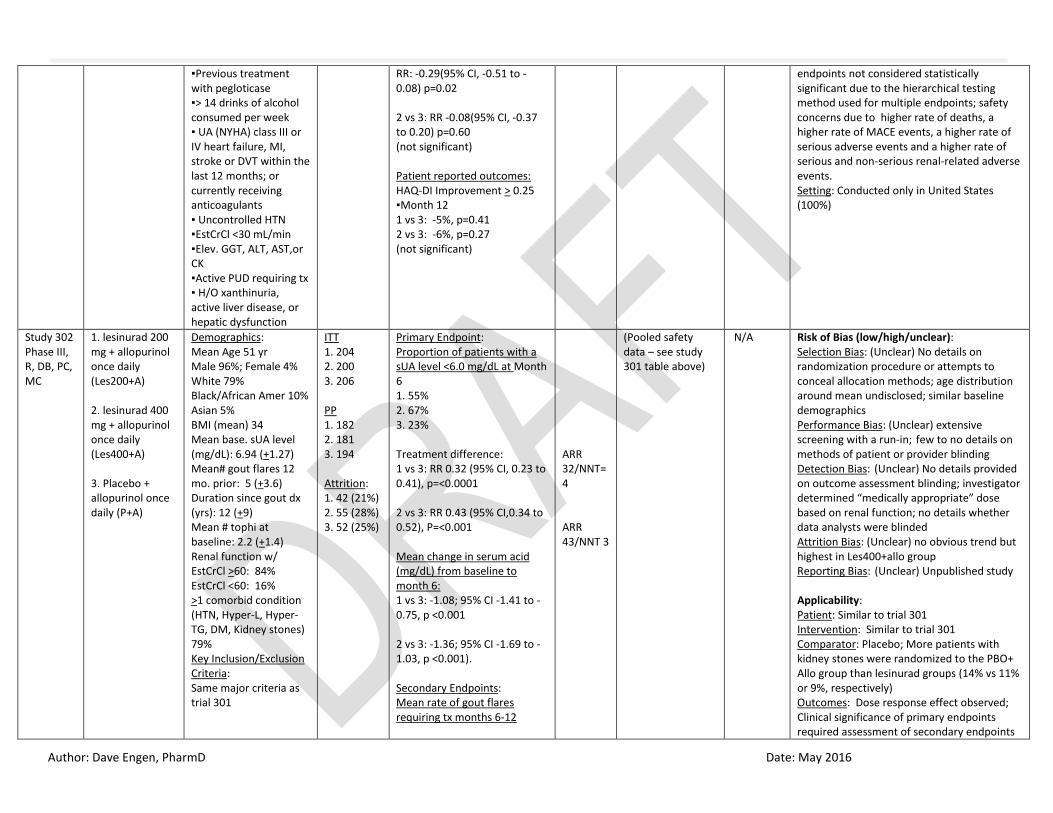
▪Previous treatment with pegloticase ▪> 14 drinks of alcohol consumed per week ▪ UA (NYHA) class III or IV heart failure, MI, stroke or DVT within the last 12 months; or currently receiving anticoagulants ▪ Uncontrolled HTN ▪EstCrCl <30 mL/min ▪Elev. GGT, ALT, AST,or CK ▪Active PUD requiring tx ▪ H/O xanthinuria, active liver disease, or hepatic dysfunction
RR: -0.29(95% CI, -0.51 to -0.08) p=0.02 2 vs 3: RR -0.08(95% CI, -0.37 to 0.20) p=0.60 (not significant) Patient reported outcomes: HAQ-DI Improvement > 0.25 ▪Month 12 1 vs 3: -5%, p=0.41 2 vs 3: -6%, p=0.27 (not significant)
endpoints not considered statistically significant due to the hierarchical testing method used for multiple endpoints; safety concerns due to higher rate of deaths, a higher rate of MACE events, a higher rate of serious adverse events and a higher rate of serious and non-serious renal-related adverse events. Setting: Conducted only in United States (100%)
Study 302 Phase III, R, DB, PC, MC
1. lesinurad 200 mg + allopurinol once daily (Les200+A) 2. lesinurad 400 mg + allopurinol once daily (Les400+A) 3. Placebo + allopurinol once daily (P+A)
Demographics: Mean Age 51 yr Male 96%; Female 4% White 79% Black/African Amer 10% Asian 5% BMI (mean) 34 Mean base. sUA level (mg/dL): 6.94 (+1.27) Mean# gout flares 12 mo. prior: 5 (+3.6) Duration since gout dx (yrs): 12 (+9) Mean # tophi at baseline: 2.2 (+1.4) Renal function w/ EstCrCl >60: 84% EstCrCl <60: 16% >1 comorbid condition (HTN, Hyper-L, Hyper-TG, DM, Kidney stones) 79% Key Inclusion/Exclusion Criteria: Same major criteria as trial 301
ITT 1. 204 2. 200 3. 206 PP 1. 182 2. 181 3. 194 Attrition: 1. 42 (21%) 2. 55 (28%) 3. 52 (25%)
Primary Endpoint: Proportion of patients with a sUA level <6.0 mg/dL at Month 6 1. 55% 2. 67% 3. 23% Treatment difference: 1 vs 3: RR 0.32 (95% CI, 0.23 to 0.41), p=<0.0001 2 vs 3: RR 0.43 (95% CI,0.34 to 0.52), P=<0.001 Mean change in serum acid (mg/dL) from baseline to month 6: 1 vs 3: -1.08; 95% CI -1.41 to -0.75, p <0.001 2 vs 3: -1.36; 95% CI -1.69 to -1.03, p <0.001). Secondary Endpoints: Mean rate of gout flares requiring tx months 6-12
ARR 32/NNT=4 ARR 43/NNT 3
(Pooled safety data – see study 301 table above)
N/A Risk of Bias (low/high/unclear): Selection Bias: (Unclear) No details on randomization procedure or attempts to conceal allocation methods; age distribution around mean undisclosed; similar baseline demographics Performance Bias: (Unclear) extensive screening with a run-in; few to no details on methods of patient or provider blinding Detection Bias: (Unclear) No details provided on outcome assessment blinding; investigator determined “medically appropriate” dose based on renal function; no details whether data analysts were blinded Attrition Bias: (Unclear) no obvious trend but highest in Les400+allo group Reporting Bias: (Unclear) Unpublished study Applicability: Patient: Similar to trial 301 Intervention: Similar to trial 301 Comparator: Placebo; More patients with kidney stones were randomized to the PBO+ Allo group than lesinurad groups (14% vs 11% or 9%, respectively) Outcomes: Dose response effect observed; Clinical significance of primary endpoints required assessment of secondary endpoints

Author: Dave Engen, PharmD Date: May 2016
1 vs 3: RR 0.88 (95% CI, 0.57 to 1.37) p=0.57 (not significant) 2 vs 3: RR 0.93(95% CI, 0.60 to 1.45) p=0.75 (not significant) Proportion of patients with complete resolution of ≥1 target tophus by Month 12 (in patients with target tophi at baseline) 1 vs 3: RR: -0.02 (95% CI, -0.24 to 0.20) p=0.85 (not significant) 2 vs 3: RR -0.06(95% CI, -0.29 to 0.17) p=0.63 (not significant) HAQ-DI improvement of ≥0.25, month 12 and difference in proportions HAQ-DI Improvement > 0.25 ▪Month 12 1 vs 3: -10%, p=0.10 2 vs 3: -1%, p=0.82 (not significant)
that of gout flares and tophus resolution, however, findings from major secondary endpoints not considered statistically significant due to the hierarchical testing method used for multiple endpoints; safety concerns raised included higher rate of deaths, a higher rate of MACE events, a higher rate of serious adverse events and a higher rate of serious and non-serious renal-related adverse events. Setting: US (51%), Canada, Europe, Australia, New Zealand, South Africa
Study 304 Phase III, R, DB, PC, MC
1. lesinurad 200 mg + febuxostat 80 mg once daily (Les200+F) 2. lesinurad 400 mg + febuxostat 80 mg once daily (Les400+F) 3. Placebo + febuxostat once daily (P+F)
Demographics: Mean Age 54 yr Male 95%; Female 5% White 80% Black/African Amer 11% Asian 6% BMI (mean) 32 Mean base. sUA level (mg/dL): 5.27 (+1.63) Mean# gout flares 12 mo. prior: 7 (+8) Duration since gout dx (yrs): 15 (+11) Mean # tophi at baseline: 1.8 (+1.2) Renal function w/
ITT 1. 106 2. 109 3. 109 PP 1. 102 2. 99 3. 106 Attrition: 1. 30 (28%) 2. 33 (30%) 3. 26 (24%)
Primary Endpoint: Proportion of patients with a sUA level <5 mg/dL at Month 6 1. 57% 2. 76% 3. 47% Treatment difference: 1 vs 3: RR 0.10 (95% CI, -0.03 to 0.23), p=0.1298 2 vs 3: RR 0.29 (95% CI, 0.17 to 0.42); p<0.0001 Mean change in serum acid (mg/dL) from baseline to
NA ARR 29/NNT 4
MACE events – CV death, non-fatal MI, non-fatal stroke: 1. RR 2.35 (95% CI, 0.59 to 9.41) 2. RR 2.28 (95% CI, 0.57 to 9.11) 3. RR 1.13 (95% CI, 0.16 to 7.99) p-value not given Any Renal AEs: 1. 9 (9%) 2. 11 (10%)
N/A Risk of Bias (low/high/unclear): Selection Bias: (Unclear) No details on randomization procedure or attempts to conceal allocation methods; age distribution around mean undisclosed; similar baseline demographics Performance Bias: (Unclear) blinding process not adequately described Detection Bias: (Unclear) insufficient description for blinding of outcome assessors Attrition Bias: (High) Significant withdrawal rate versus PBO and possible incomplete data Reporting Bias: (Moderate) Most primary and secondary outcomes were not statistically significant
Author: Dave Engen, PharmD Date: May 2016
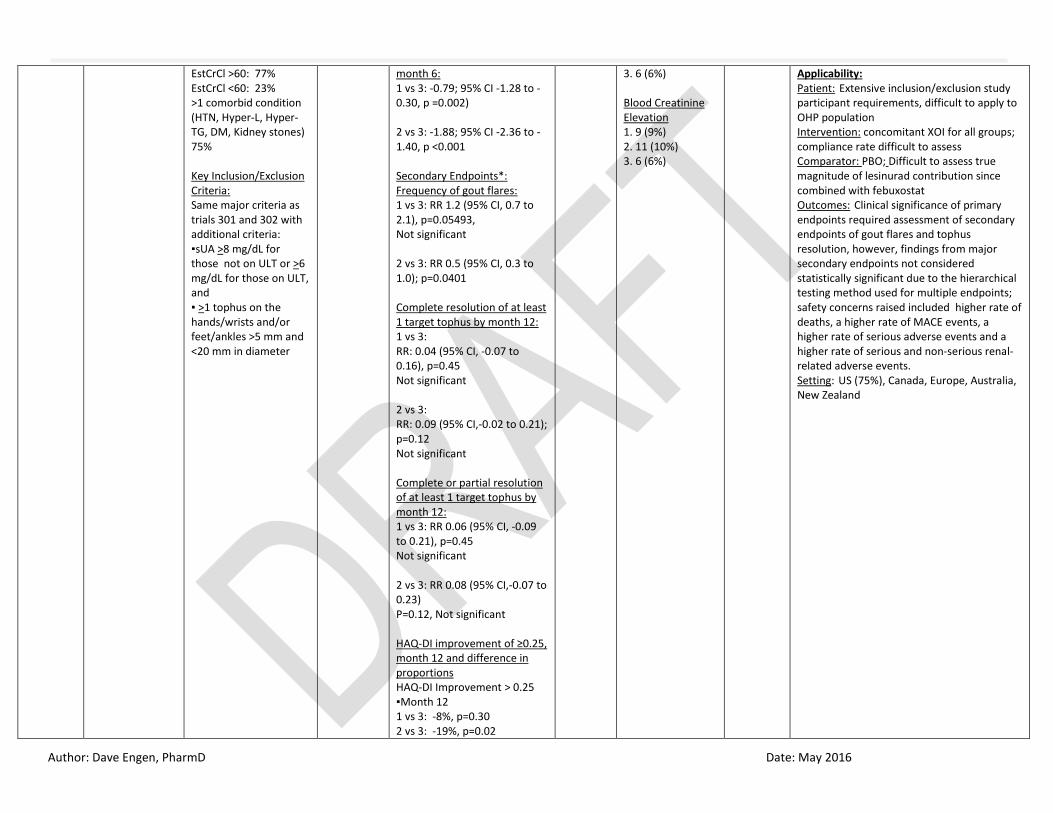
EstCrCl >60: 77% EstCrCl <60: 23% >1 comorbid condition (HTN, Hyper-L, Hyper-TG, DM, Kidney stones) 75% Key Inclusion/Exclusion Criteria: Same major criteria as trials 301 and 302 with additional criteria: ▪sUA >8 mg/dL for those not on ULT or >6 mg/dL for those on ULT, and ▪ >1 tophus on the hands/wrists and/or feet/ankles >5 mm and <20 mm in diameter
month 6: 1 vs 3: -0.79; 95% CI -1.28 to -0.30, p =0.002) 2 vs 3: -1.88; 95% CI -2.36 to -1.40, p <0.001 Secondary Endpoints*: Frequency of gout flares: 1 vs 3: RR 1.2 (95% CI, 0.7 to 2.1), p=0.05493, Not significant 2 vs 3: RR 0.5 (95% CI, 0.3 to 1.0); p=0.0401 Complete resolution of at least 1 target tophus by month 12: 1 vs 3: RR: 0.04 (95% CI, -0.07 to 0.16), p=0.45 Not significant 2 vs 3: RR: 0.09 (95% CI,-0.02 to 0.21); p=0.12 Not significant Complete or partial resolution of at least 1 target tophus by month 12: 1 vs 3: RR 0.06 (95% CI, -0.09 to 0.21), p=0.45 Not significant 2 vs 3: RR 0.08 (95% CI,-0.07 to 0.23) P=0.12, Not significant HAQ-DI improvement of ≥0.25, month 12 and difference in proportions HAQ-DI Improvement > 0.25 ▪Month 12 1 vs 3: -8%, p=0.30 2 vs 3: -19%, p=0.02
3. 6 (6%) Blood Creatinine Elevation 1. 9 (9%) 2. 11 (10%) 3. 6 (6%)
Applicability: Patient: Extensive inclusion/exclusion study participant requirements, difficult to apply to OHP population Intervention: concomitant XOI for all groups; compliance rate difficult to assess Comparator: PBO; Difficult to assess true magnitude of lesinurad contribution since combined with febuxostat Outcomes: Clinical significance of primary endpoints required assessment of secondary endpoints of gout flares and tophus resolution, however, findings from major secondary endpoints not considered statistically significant due to the hierarchical testing method used for multiple endpoints; safety concerns raised included higher rate of deaths, a higher rate of MACE events, a higher rate of serious adverse events and a higher rate of serious and non-serious renal-related adverse events. Setting: US (75%), Canada, Europe, Australia, New Zealand

Author: Dave Engen, PharmD Date: May 2016
Abbreviations: AE=adverse event; ALT=alanine aminotransferase, ARR = absolute risk reduction; AST=aspartate aminotransferaseorCI = confidence interval;CK=creatinine kinase; DB=double blind; EstCrCl = estimated Creatinine Clearance; GGT=gamma-glutamyltransferase; HAQ-DI=Health Assessment Questionnaire – Disability Index; ITT = intention to treat; MC=multicenter; mITT = modified intention to treat; N = number of subjects; NA = not applicable; NNH = number needed to harm; NNT = number needed to treat; NSAID=non-steroidal anti inflammatory drug; NYHA=New York Heart Association;PBO=placebo; PC=placebo controlled; PP = per protocol. PUD=peptic ulcer disease;R=randomized; SUA = serum uric acid; XOI=xanthine oxidase inhibitor;

Author: Dave Engen, PharmD Date: May 2016
References:
1. Khanna D, Fitzgerald JD, Khanna PP, et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: Systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care & Research. 2012;64(10):1431-1446. doi:10.1002/acr.21772.
2. Khanna D, Khanna PP, Fitzgerald JD, et al. 2012 American College of Rheumatology guidelines for management of gout. Part 2: Therapy and antiinflammatory prophylaxis of acute gouty arthritis. Arthritis Care & Research. 2012;64(10):1447-1461. doi:10.1002/acr.21773.
3. Diagnosis of Gout - Research Review - Final | AHRQ Effective Health Care Program. https://effectivehealthcare.ahrq.gov/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productID=2188. Accessed April 7, 2016.
4. Diagnosis, Treatment, and Prevention of Gout - American Family Physician. http://www.aafp.org.liboff.ohsu.edu/afp/2014/1215/p831.html. Accessed April 7, 2016.
5. Zhang W. EULAR evidence based recommendations for gout. Part I: Diagnosis. Report of a task force of the standing committee for international clinical studies including therapeutics (ESCISIT). Annals of the Rheumatic Diseases. 2006;65(10):1301-1311. doi:10.1136/ard.2006.055251.
6. Zhang W. EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics (ESCISIT). Annals of the Rheumatic Diseases. 2006;65(10):1312-1324. doi:10.1136/ard.2006.055269.
7. Management of Gout - Research Review - Final | AHRQ Effective Health Care Program. https://effectivehealthcare.ahrq.gov/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productID=2195. Accessed April 7, 2016.
8. Sivera F, Andrés M, Carmona L, et al. Multinational evidence-based recommendations for the diagnosis and management of gout: integrating systematic literature review and expert opinion of a broad panel of rheumatologists in the 3e initiative. Ann Rheum Dis. 2014;73(2):328-335. doi:10.1136/annrheumdis-2013-203325.
9. Diaz-Torne C, Perez-Herrero N, Perez-Ruiz F. New medications in development for the treatment of hyperuricemia of gout. [Review]. Current Opinion in Rheumatology. 2015;27(2):164-169. doi:10.1097/BOR.0000000000000146.
10. Crittenden DB, Pillinger MH. New Therapies for Gout. Annual Review of Medicine. 2013;64(1):325-337. doi:10.1146/annurev-med-080911-105830. 11. Lesinurad Summary Review. US Food and Drug Administration Center for Drug Evaluation and Research.
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/207988Orig1s000SumR.pdf. Accessed April 7, 2016. 12. Zurampic (lesinurad) [prescribing information] Wilmington, DE: AstraZeneca Pharmaceuticals LP, 2015.
Author: Dave Engen, PharmD Date: May 2016
Appendix 1: Highlights of Prescribing Information