new experimental targets for gastric...
TRANSCRIPT

Newexperimentaltargetsforgastric cancer
AndrésCervantesProfessor ofMedicine
Outline
• Acquired capabilities ofCancer• IGFRpathway• PI3K-AKT-m-TORpathway• METpathway• FGFRpathway• Check point inhibitors

Cancer cells Fibroblasts
Immune cells
Endothelial cells
Acquired Capabilities of Cancer
Hanahan & Weinberg, Cell 100, 2000
1. Self-Sufficiency in Growth Signals
a. Receptors: EGFR-family, IGF1R, MET, FGFR
b. Downstream effectors: PI3K, mTOR, AKT
2. Insensitivity to Antigrowth Signals
3. Evading Apoptosis
4. Limitless Replicative Potential
5. Sustained Angiogenesis
6. Tissue Invasion and Metastasis

ADQUIRED CAPABILITIES OF CANCER: SELF SUFFICIENCY IN GROWTH SIGNALS
• RECEPTORS:– EGFR FAMILY– IGFR1– MET– FGFR
• DOWNSTREAM EFFECTORS:– PI3K– AKT– m-TOR

The IGF-1R signaling pathway THE IGF-1R SIGNALING PATHWAY

The IGF-1R signaling pathway THE IGF-1R SIGNALING PATHWAY IN GASTRO-ESOPHAGEAL CANCER
MatsubaraJetal.ClinCancerRes2008;14:3022
MultivariateCoxregressionanalysesofoverallsurvivalsincethestartoffirst-linechemotherapy:correlationwithproteinexpressionandclinicalcharacteristics
HR (95%CI) pIGF-1Rnegvspositive 2.14 1.20-3.820.01PS0vs1-2 1.83 1.15-2.910.01IntestinalvsDiffusse 1.71 1.08-2.700.02
COEXPRESSIONWITHEGFR+(55%)ANDHER2+++(15%)

Rationale for Targeting Other Receptors & Downstream Signaling Proteins
l Met receptor
– Hepatocyte growth factor (HGF) & c-Met highly expressed in GC specimens: 73% and 77% (Chen, 2007)
– MET gene amplification in 10-15% GC (Bechletner, 2008)
– Estimulation of c-Met with HGF induces signal transduction, that is abrogated with c-Met TKIs (Catenacci, 2008)
– Met inhibitors in the clinic in GC: Foretinib - GSK089 (Jhawer, 2009) and XL880 (Jhawer, 2008)



MolecularHeterogeneity andReceptorCoamplificationDriveResistance to Targeted TherapyinMET-Amplified EsophagogastricCancer
Kwak EL,etal.Cancer discov2015;5:1271–1281

MolecularHeterogeneity andReceptorCoamplificationDriveResistance to Targeted TherapyinMET-Amplified EsophagogastricCancer
Kwak EL,etal.CancerDiscov 2015;5:1271–1281
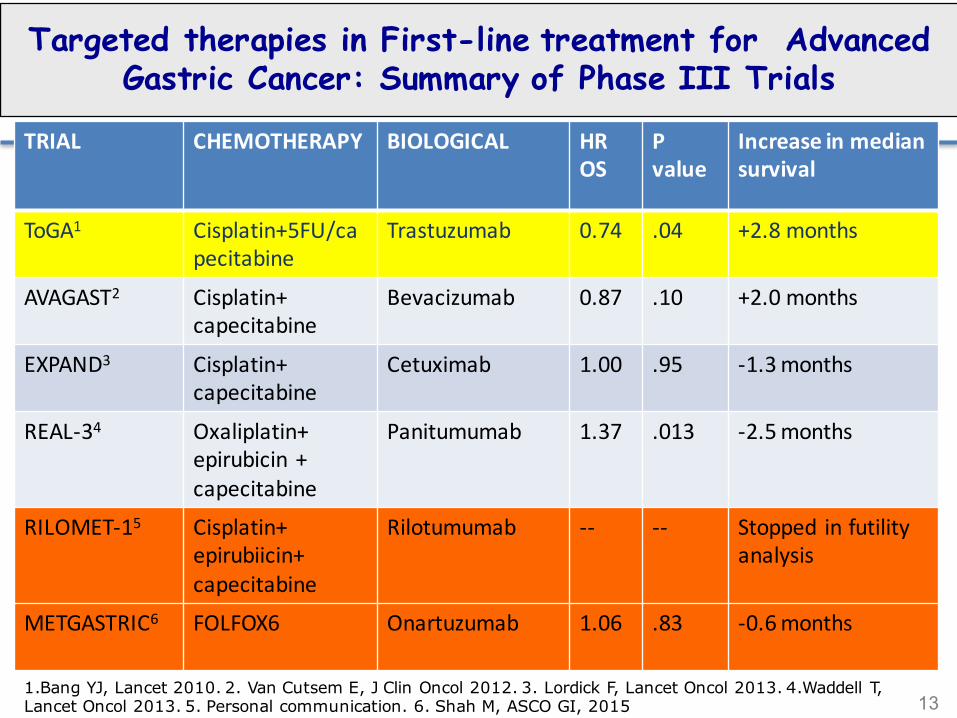
131.Bang YJ, Lancet 2010. 2. Van Cutsem E, J Clin Oncol 2012. 3. Lordick F, Lancet Oncol 2013. 4.Waddell T, Lancet Oncol 2013. 5. Personal communication. 6. Shah M, ASCO GI, 2015
Targeted therapies in First-line treatment for Advanced Gastric Cancer: Summary of Phase III Trials
TRIAL CHEMOTHERAPY BIOLOGICAL HROS
Pvalue
Increaseinmediansurvival
ToGA1 Cisplatin+5FU/capecitabine
Trastuzumab 0.74 .04 +2.8months
AVAGAST2 Cisplatin+capecitabine
Bevacizumab 0.87 .10 +2.0months
EXPAND3 Cisplatin+capecitabine
Cetuximab 1.00 .95 -1.3months
REAL-34 Oxaliplatin+epirubicin+capecitabine
Panitumumab 1.37 .013 -2.5months
RILOMET-15 Cisplatin+epirubiicin+capecitabine
Rilotumumab -- -- Stopped infutilityanalysis
METGASTRIC6 FOLFOX6 Onartuzumab 1.06 .83 -0.6months







PearsonA,etal.Cancer Discovery 2016,
High-level clonal FGFR amplification and response to FGFR Inhibition in a translational clinical trial
ADQUIRED CAPABILITIES OF CANCER: SELF SUFFICIENCY IN GROWTH SIGNALS
• RECEPTORS:– EGFR FAMILY– IGFR1– c-MET
• DOWNSTREAM EFFECTORS:– PI3K– AKT– m-TOR

Rationale for Targeting Other Receptors & Downstream Signaling Proteins
l PI3K-mTOR inhibitors
– RAD001 (everolimus) is a derivative of rapamycin which act as a signal transduction inhibitor of mTOR
– RAD001 attenuates production of HIF-1α and VEGF in GC in vitro and markedly inhibits NCI-N87 GC xenografts growth (Cejka, 2008)
– Preliminary results showed that RAD001 monotherapy is generally well tolerated with promising activity in pts with previously treated advanced GC1
1Muro et al. J Clin Oncol 2008 (ASCO)

THE PHOSPHATIDYLINOSITOL 3 KINASE (PI3K) SIGNALING PATHWAY

GENETIC VARIATIONS IN THE PI3K/PTEN/AKT/ MTOR PATHWAY IN ESOPHAGEAL CANCER
HildebrandtMAT,etal.JClinOncol2009;27:857.

GENETIC VARIATIONS IN THE PI3K/PTEN/AKT/m-TOR PATHWAY IN ESOPHAGEAL CANCER
HildebrandtMAT,etal.JClinOncol2009;27:857.

The Cancer Genome AtlasResearchNetwork.Nature 2014;513:202-209
Comprehensive Molecular Characterization of Gastric Adenocarcinoma: Molecular platforms

Comprehensive Molecular Characterization of Gastric Adenocarcinoma: Molecular platforms
• Array-based somatic copy number analysis• Whole exome sequencing• Array-based DNA methylation profiling• Messenger RNA sequencing• microRNA sequencing• Reverse Phase Protein Array (RPPA)
The Cancer Genome AtlasResearchNetwork.Nature 2014;513:202-209
Comprehensive Molecular Characterization of Gastric Adenocarcinoma: Molecular platforms

The Cancer Genome AtlasResearchNetwork.Nature 2014;513:202-209
9%
22%20%
50%

The Cancer Genome AtlasResearchNetwork.Nature 2014;513:202-209
Comprehensive Molecular Characterization of Gastric Adenocarcinoma: PI3KCA mutations by subtype

MTOR AND PHOSPORILATED MTOR IN GASTRIC CANCER
YuG,etal.ClinCancerRes2009;15:1821
NEGATIVENEGATIVE
POSITIVEPOSITIVE
1072samplesfromgastriccancerpatientsaftersurgeryImmunohystochemicalassessmentofmTORandpmTOR

Yamada,etal.ProcASCOGI2009
• PhaseI:2PRsoutof4patientswithmetastatic,heavilypretreatedcancerofthestomachorgastroesophagealjunction• PhaseII:NoOR,DCRwas55%(29/53pts),mPFSwas83days(95%CI:50-91days)
Everolimusingastriccancer
Baseline 2monthsafterRAD00110mg
EVEROLIMUS IN GASTRIC CANCER

Gastric Cancer: Second Line ChemotherapyTrials Comparing BSC versus Active Treatment
1. Eur J Cancer 2011; 47:2306-2314. 2. J Clin Oncol 2012; 30:1513-1518. 3. Lancet Oncol 2014; 15:78-86. 4.JClin Oncol 2013;31:3935-3943. 5.Lancet2014;383:31-39.
TrialAuthor
Year PatientsRandom(n)
Treatment HROS
Pvalue
Gain inMedianSurvival
Thuss-Patienceetal.1
2011 401:1
Irinotecan 0.48 .0023 2,4months
Park etal. 2 2012 1932:1
IrinotecanDocetaxel
0.65 .004 1,3months
Fordet al. 3 2014 1681:1
Docetaxel 0.67 .01 1,6months
Otshu etal4 2013 6562:1
Everolimus 0.90 .124 0.9months
Fuchs etal5 2014 3552:1
Ramucirumab 0.77 .047 1.4months

Phase II Study of weekly Paclitaxel +/-Olaparib for second line in advanced gastric cancer
Stratification:n ATM Low A: weekly Paclitaxel
B: weekly Paclitaxel plus Olaparib 100 mg bid
n Primary end point: PFSn Co-Primary end point: PFS in ATM Lown Secondary end points: OS, OS in ATM Low, Toxicity
Bang JY, et al. J Clin Oncol 2015;33:3858–3865
R

Phase II Study of weekly Paclitaxel +/-Olaparib for second line in advanced gastric cancer
Bang JY, et al. J Clin Oncol 2015;33:3858–3865

Phase II Study of weekly Paclitaxel +/-Olaparib for second line in advanced gastric cancer
Bang JY, et al. J Clin Oncol 2015;33:3858–3865

Challenges• Target discovery has resulted in numerous novel drugs in
clinical development
• Signal transduction inhibition does not guarantee tumor response:
– Target presence and dependence– Redundancy– Cross-talk
• Molecular-based population enrichment needed
• Combinations: mechanistic interactions
• Phase III trials are warranted

• PD-1isanegativeco-stimulatoryreceptorexpressedprimarilyonactivatedTcells1
• BindingofPD-1toitsligandsPD-L1andPD-L2inhibitseffectorT-cellfunction1
• ExpressionofPD-L1ontumorcellsandmacrophagescansuppressimmunesurveillanceandpermitneoplasticgrowth2
1.Keir ME et al. Annu Rev Immunol. 2008;26:677-704. 2.Pardoll DM. Nat Rev Cancer. 2012;12:252-64.
PD-1 Pathway and Immune Surveillance

Presentedby:KeiMuro
Antibody
• DualblockadeofPD-L1andPD-L2• Nocytotoxic(ADCC/CDC)activity• Pharmacokineticssupportdosingevery2weeks(Q2W)orevery3weeks(Q3W)• Lowoccurrenceofanti-drugantibodies,whichhavenoimpactonpharmacokinetics• Demonstratedclinicalactivityinmultipletumortypes1-7
• RecentlyapprovedintheUnitedStatesforthetreatmentofpatientswithunresectableormetastaticmelanomaanddiseaseprogressionfollowingipilimumaband,ifBRAFV600mutationpositive,aBRAFinhibitor
1.RibasAetal.JClinOncol.2014;32(suppl5):abstrLBA9000;2.RizviNetal.JClinOncol.2014;32(suppl5):abstr8007;3.GaronEBetal.JClinOncol.2014;32(suppl5):abstr8020;4.SeiwertTYetal.JClinOncol.2014;32(suppl5):abstr6011.5.PlimackEetal.Abstr.LBA23.Presentedat2014ESMOCongress,September26-30,Madrid,Spain.6.MoskowitzCHetal.Bood.2014;124(21):abstr290;7.NandaRetal.Abstract1349(S1-09)presentedatSABCS2014,Dec9-13,SanAntonio,TX.
Pembrolizumab (MK-3475) Is a Humanized IgG4, High-Affinity, Anti-PD-1

:
Screening: 65of162(40%)patientsassessedforPD-L1expressionhadPD-L1-positivetumorsPatients:19patientsfromAsiaand20patientsfromtherestoftheworldTreatment: 10mg/kgIVQ2WResponseassessment:Performedevery8weeks perRECISTv1.1
• Recurrentormetastaticadenocarcinoma ofthestomachorGEJ
• ECOGPS0-1• PD-L1-positivetumora• Nosystemicsteroidtherapy• Noautoimmunedisease
(activeorhistoryof)• Noactivebrainmetastases
Pembrolizumab10mg/kgQ2W
CompleteResponse
PartialResponseorStableDisease
ConfirmedProgressiveDiseaseb
DiscontinuationPermittedc
Treatfor24monthsoruntilprogressionorintolerable toxicity
Discontinue
Muro K, et al. ASCO GI 2015; Abstract nr.03
KEYNOTE-012: Gastric Cancer Cohort

Muro K, et al. ASCO GI 2015; Abstract nr.03
• PD-L1expressionwasassessed inarchivaltumorsamples usingaprototypeIHCassayandthe22C3antibody
• Positivitywasdefined asstaininginthestromaorin≥1%oftumorcells
PD-L1Positive:TumorStaining
PD-L1Positive:StromalandTumorStaining
PD-L1Negative PD-L1Positive:TumorStaining
PD-L1 Expression in Gastric Cancer Samples

PD-L1 Expression in Gastric Cancer Samples
Topalian S,etal.Nature Rev Cancer 2016;16:275-287.

Muro K, et al. Lancet Oncol 2016; 17:717-726.
.
Pembrolizumab induces Responses in Chemorefractory Gastric Cancer

Muro K, et al. Lancet Oncol 2016; 17:717-726.
Maximum Percentage Change From Baseline in Tumor Sizea Keynote-012 (RECIST v1.1, Central Review)

March 22, 2014 July 3, 2014
November 6, 2014September 26, 2014August 28, 2014
May 8, 2014
64-Year-Old Male With Recurrent Gastric Cancer Treated with Pembrolizumab

Topalian S,etal.Nature Rev Cancer 2016;16:275-287.
Multifactorial Biomarkers of Clinical Response to PDL-1 Blockade

The Cancer Genome AtlasResearchNetwork.Nature 2014;513:202-209
9%
22%20%
50%