new regulatory flexibility: how should your compliance
TRANSCRIPT

Copyright © 2021 by SullivanCotter
New Regulatory Flexibility: How Should
Your Compliance Program Change?
Wednesday, October 13, 2021
Copyright © 2021 by SullivanCotter
Presenters
1
Patty Bohney
Principal,
Physician
Compensation
SullivanCotter
pattybohney@
sullivancotter.com
Ron Vance
Managing Principal,
Physician
Compensation
SullivanCotter
ronvance@
sullivancotter.com
Ralph DeJong
Partner
McDermott Will &
Emery LLP
rdejong@
mwe.com
Jennifer Skeels
Attorney
Hall, Render,
Killian, Heath &
Lyman, P.C.
jskeels@
hallrender.com
765.231.6252 470.481.6471 312.984.6918 317.977.1497

Copyright © 2021 by SullivanCotter
Webinar Instructions
2
• Today’s session will include approximately 1 hour and 45
minutes of presentation and additional time for questions
• How to submit questions:
– Use the control panel on the right side of
your screen
– Type your question at any time during the webinar and
click “SEND”
– If you’re on a mobile device, click on the question mark
icon and follow the same steps
– Panelists will answer as many questions as possible
during Q&A time
All attendees can access the slide deck via the Converve platform
Copyright © 2021 by SullivanCotter
Agenda
3
1 Market Update
Stark Law and AKS
Regulatory Update23
New Value-Based
Exceptions / Safe
Harbors & Application45 Compliance Program
Implications
Compensation
Implications 6 Answering Your
Questions

Copyright © 2021 by SullivanCotter
1. Market Update
4
Copyright © 2021 by SullivanCotter
Government’s Role in Changing Health Care Delivery
5
New initiatives represent CMS’ push to change health care delivery with a coordinated approach with the Office of the Inspector General (OIG) and Department of Justice (DOJ)
Stark Law and Anti-
Kickback Statute
• Signaling more flexibility in value-
based arrangements between
health systems and physicians –
including expanded options that
include financial risk.
• Permit expanded use of
“outcomes” performance metrics
to take into account financial savings
and enhanced clinical quality for a
defined population of patients.
• With respect to fair market value
(FMV) and commercial
reasonableness (CR), the new
definitions are less formulaic and
more situation-specific. Value-
based arrangement payments may
not require FMV testing, but
aggregate payments may
require both FMV and CR.
“Patients Over Paperwork”
Burden Reduction
• Reduce unnecessary burden.
• Increase efficiencies.
• Improve the beneficiary experience.
Example:
Physician Fee Schedule Changes
• Impact on physician productivity
(wRVUs) and reimbursement.
• Significant changes to the wRVU
values for broadly utilized
E&M codes.
“Primary Care First”
Program
• Promotes patient access, both
inside and outside the office, and
rewards high quality to reduce
preventable hospitalizations through
population health payments.
• Model options emphasize flexibility
and accountability and drive
primary care compensation
designs that incorporate panel size.
• Models provide greater
compensation for
higher-risk patients.

Copyright © 2021 by SullivanCotter
Impact of COVID-19Long-Term Considerations
The pandemic is driving fundamental change and uncertainty with respect to
health care organization budgets, reimbursement, internal processes and operations
Pandemic-driven change and organizational response may have
long-term impact and requires aligned administrative and physician leadership
Financial Sustainability
• Decreases in
volume/revenue
• Increases in expense
Patient Access
• Constraints on in-person
patient consults due to
COVID-19 protocol
• Requires expanded
in-office hours
Population Health
• Flexibility to adapt to traditional and non-traditional
access to care
• Increased focus on care coordination
Continuing Priorities: Additional Pressures
Virtual Medicine
• Development/expansion of nontraditional
patient access
• Long-term uncertainty in virtual care
reimbursement
Optimizing Clinical Workforce Resources
• Physician/APP redeployment
• Expanding APP scope
Emerging as Top Priorities
6

Copyright © 2021 by SullivanCotter
Changing Care Delivery — Virtual Medicine
7
Source: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-
reality#:~:text=13.,Survey%2C%20April%2027%2C%202020.&text=Beacon's%20claims%20data%20suggest%20that,processed%20at%20a%20later%20date.
Copyright © 2021 by SullivanCotter
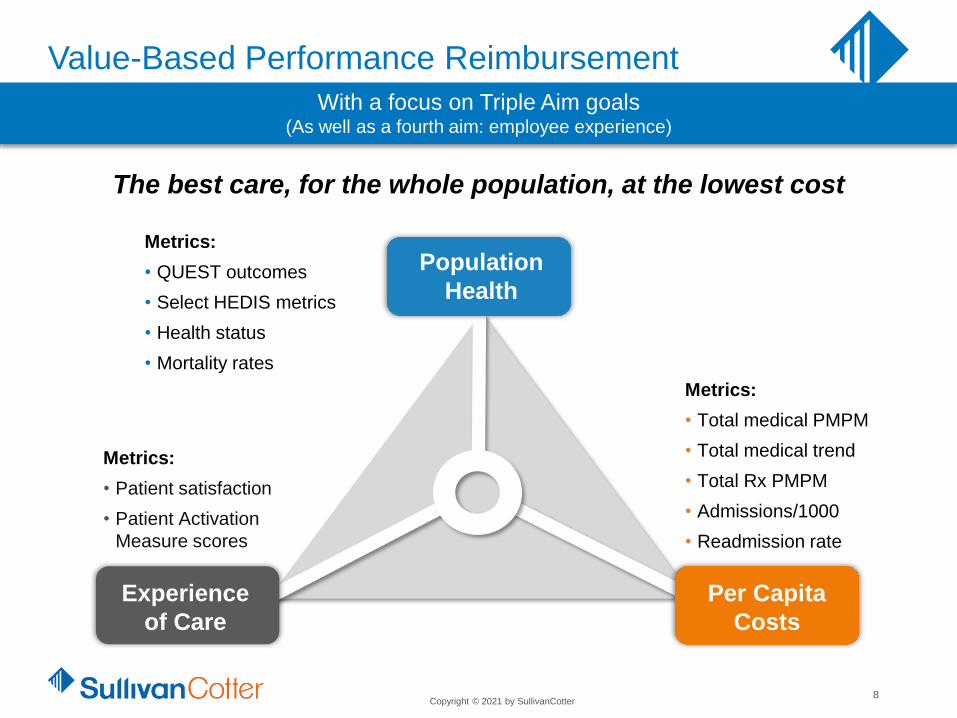
Value-Based Performance Reimbursement
8
Metrics:
• QUEST outcomes
• Select HEDIS metrics
• Health status
• Mortality rates
Metrics:
• Patient satisfaction
• Patient Activation
Measure scores
Metrics:
• Total medical PMPM
• Total medical trend
• Total Rx PMPM
• Admissions/1000
• Readmission rate
Experience
of Care
Per Capita
Costs
The best care, for the whole population, at the lowest cost
Population
Health
With a focus on Triple Aim goals (As well as a fourth aim: employee experience)
Copyright © 2021 by SullivanCotter
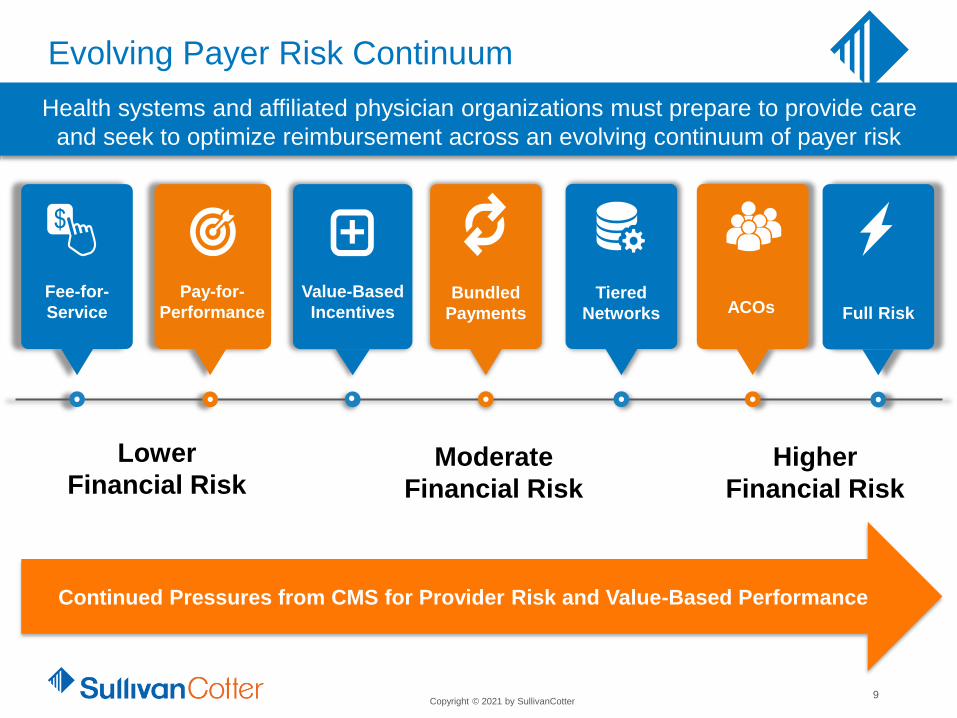
Evolving Payer Risk Continuum
9
Tiered
Networks Full RiskACOsValue-Based
Incentives
+Pay-for-
Performance
Fee-for-
ServiceBundled
Payments
Lower
Financial RiskModerate
Financial Risk
Higher
Financial Risk
Health systems and affiliated physician organizations must prepare to provide care
and seek to optimize reimbursement across an evolving continuum of payer risk
Continued Pressures from CMS for Provider Risk and Value-Based Performance

Copyright © 2021 by SullivanCotter
Prevalence and Growth of Medicare Advantage Plans
10
Source: https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2021-enrollment-update-and-key-trends/

Copyright © 2021 by SullivanCotter
Identifying the right number and mix of physicians and advanced practice
providers (APPs) is critical to advancing an organization’s mission
and supporting strategic priorities
HEALTH SYSTEMInpatient, outpatient and
ancillary services provided
across multiple delivery sites
The Imperative of Physician and APP Alignment
1 2 3 4 5 6 7 8 9 10 11
Telemedicine
and Non-
Medical Staff
Referring
Physicians
Traditional
Hospital
Independent
Medical Staff
Physician
Recruitment
and
Retention
Support
Medical
Directorship
Services
MSO
(Practice
Mgmt)
Joint
Managed
Care (with
limited
risk)
Specialty
Institute/
Service
Line Co-
Mgmt
Joint
Venture and
Shared
Equity
Clinical
Integration
and Payer
Contracting
Exclusive
Foundation
/PSA
Full Practice
Integration/
Employment
Supported by a wide range of system and physician/APP affiliation relationships
Sample continuum
11
Advancing Key Partnership Strategies
Health Care Delivery
Payment Systems
and Structures

Copyright © 2021 by SullivanCotter
Physician Fee Schedule Changes
E&M wRVU Value Changes2020 vs. 2021
1 This code is eliminated in 2021. 2 This is an add-on code for every 15 minutes of extended patient office visit time.3 The Consolidated Appropriations Act of 2021 has delayed the implementation of add-on code G2211 until at least
January 1, 2024. This deferral, along with an additional $3 billion investment to the Physician Fee Schedule has
significantly impacted the budget neutrality calculations. 4 2022 Medicare conversion factor as proposed.
HCPCS Code2020
wRVU Value
2021
wRVU Value
Percentage
Change in
wRVU Value
992011 0.48 N/A N/A
99202 0.93 0.93 0%
99203 1.42 1.60 13%
99204 2.43 2.60 7%
99205 3.17 3.50 10%
99211 0.18 0.18 0%
99212 0.48 0.70 46%
99213 0.97 1.30 34%
99214 1.50 1.92 28%
99215 2.11 2.80 33%
G22122 N/A 0.61 N/A
CMS Conversion
Factor Change3
2020
$36.092021
$34.89
(3.3%)
Significant
increases in
OB and ESRD
ambulatory visit
wRVU values are
also included in
2021
CMS Conversion
Factor Change4
2021
$34.89
2022P
$33.58
12

Copyright © 2021 by SullivanCotter
Additional Regulatory Considerations for
Physician Compensation Planning
13
Insurance Laws
Anti-Trust
Laws
Civil
Monetary
Penalties
Stark LawAnti-Kickback
Statute
With the exception of the new value-based framework, the enforcement climate is
increasingly focused on fair market value (FMV) and commercial reasonableness
Stark Law
Anti-Kickback Statute
Civil Monetary Penalties
False Claims Act
Intermediate Sanctions
Office of the
Inspector General
(OIG)
Department of
Justice
(DOJ)
Internal Revenue
Service
(IRS)
Physician Compensation
• Structured to satisfy
exceptions and
safe harbors
• Must be at FMV
• Cannot take into
consideration value or
volume of Medicare
referrals
• Must be commercially
reasonable

Copyright © 2021 by SullivanCotter
2. Stark Law and Anti-Kickback Statute
(AKS) Regulatory Update
14

Copyright © 2021 by SullivanCotter
Summary of Fines and Penalties
15
Anti-Kickback
Civil monetary
penalties up to
$100,000 per
violation
Assessment up to
3x the kickback
Criminal fines
Imprisonment
Stark
Civil monetary
penalties of $15,000
per claim
Treble damages for
prohibited referrals
False Claims Act
3x damages of
overpayment
$11,181 to $22,363
per claim penalty
IRS
Intermediate
sanctions
Excise taxes and
disgorgement
Reputational Risk Burden on Resources High Settlements
Fines and Penalties

Copyright © 2021 by SullivanCotter
Overview of Changes
16
• October 9, 2019 - CMS and the OIG published
proposed changes to Stark Law, Anti-Kickback
and Civil Monetary Penalties
• CMS introduced “Regulatory Sprint to
Coordinated Care” with the goal of reducing
regulatory burden and incentivizing
value-based care
• December 2, 2020 - CMS and the OIG published
Final Rules including historic revisions to the Stark
Law, Anti-Kickback and Civil Monetary Penalties
• Effective January 19, 2021 - New definitions for
FMV/CR and new value-based exceptions
became effective and provide new potential
arrangement opportunities

Copyright © 2021 by SullivanCotter
Overview of Changes
17
• Modifications to existing Stark Law terms and
exception requirements
• Effective January 19, 2021 - Other new
Stark exceptions
• Effective January 1, 2022 - Stark group practice
exception changes to special rules for profit sharing
and bonus payments
• Expanded AKS Safe Harbor for personal service
arrangements and limits to what qualifies under the
safe harbor

Copyright © 2021 by SullivanCotter
Physician Self-Referral Law The Big Three
18
The final rule indicates that each of the “Big Three” continues to remain
relevant in assessing physician compensation arrangements
Fair Market
Value
Commercial
Reasonableness
Volume/Value
Standard

Copyright © 2021 by SullivanCotter
New rule attempts to clarify the definition of FMV:
• FMV is defined as: The value in an arm's-length transaction, consistent with the
general market value of the subject transaction.
• General market value is defined as: The compensation that would be paid at
the time the parties enter into the service arrangement as the result of bona fide
bargaining between well-informed parties that are not otherwise in a position to
generate business for each other.
Physician Self-Referral Law Fair Market Value
New Definition of Fair Market Value (FMV)
19

Copyright © 2021 by SullivanCotter
CMS summarized and responded to comment submissions:
• Published survey data continue to be relevant in assessing FMV
“Consulting salary schedules or other hypothetical data is an appropriate starting point in
the determination of fair market value, and in many cases, it may be all that is required.”
“Nothing in our commentary was intended to imply that an independent valuation is
required for all compensation arrangements.”
• CMS commentary appears to support SullivanCotter’s current approach of
assessing compensation using market survey data as well as an assessment of
relevant facts and circumstances.
“A hospital may find it necessary to pay a physician above what is in the salary schedule,
especially where there is a compelling need for the physician’s services.”
Physician Self-Referral Law Fair Market Value
Relevant FMV Discussion Commentary
20

Copyright © 2021 by SullivanCotter
CMS summarized and responded to comment submissions:
• Circumstances (e.g., declining reimbursement and poor payer mix) may impact
what well-informed parties agree is FMV
“Salary schedules should not be used by a physician to demand compensation that is
above what well-informed parties…would agree is FMV.”
• P75 is not a bright-line in determining FMV
“We are uncertain why the commenters believe that it is CMS policy that compensation
set at or below the 75th percentile in a salary schedule is always appropriate, and that
compensation set above the 75th percentile is suspect, if not presumed inappropriate.
The commenters are incorrect that this is CMS policy.”
Physician Self-Referral Law Fair Market Value
Relevant FMV Discussion Commentary
21
Copyright © 2021 by SullivanCotter
Final Rule FMV Impacts
Physician Self-Referral Law Fair Market Value
• Market survey data continues to be relevant and “in many cases may be all that
is required”
• CMS does not consider P75 to be a bright line test in determining FMV
‒ Parties do not necessarily fail to satisfy FMV simply because compensation
exceeds a particular percentile
‒ Employers should not be held hostage by physician compensation demands
based solely on survey data
• Clients should be cautious about making FMV determinations on survey
data alone
‒ Online tools can provide benchmarking assessments but should not serve as
evidence of FMV
22

Copyright © 2021 by SullivanCotter
Physician Self-Referral LawCommercial Reasonableness
New Definition of Commercial Reasonableness (CR)
Commercially reasonable means that the particular arrangement furthers a legitimate
business purpose of the parties to the arrangement and is sensible, considering the
characteristics of the parties, including their size, type, scope and specialty. An
arrangement may be commercially reasonable even if it does not result in profit for one or
more of the parties.
• CR and FMV are not the same thing
• When assessing CR, one must put themselves in the shoes of the parties
directly involved
• Profitability is not a condition precedent to CR
The new rule includes a definition of CR :
Key considerations on the revised definition:
23

Copyright © 2021 by SullivanCotter
Physician Self-Referral Law Volume/Value Standard
No longer included in FMV definition, but still required:
• Requires that compensation is not determined in any manner that takes into
account the volume or value of a physician’s referrals
• No effective change from the previous prohibition
• Removed from the definition of FMV but still required to be met as a
separate standard
• Final rule examples make it clear that productivity plans do not constitute
compensation based on the volume/value of physician referrals
The new rule includes clarification of the volume/value standard:
Key considerations on the clarification:
24

Copyright © 2021 by SullivanCotter
Physician Self-Referral LawGroup Practice Exception
Special Rules for Profit Shares and Productivity Bonuses
25
• §411.352 - New requirements for distribution of Group Practice Profit
Shares and Productivity Bonuses
• Effective January 1, 2022 – Allowing groups time to revise compensation
plans and achieve compliance with Final Rules
Designated Health Services (DHS) Profit Sharing
• A physician in the group may be paid a share of overall profits that is not directly related to the volume or
value of the physician’s referrals
• Overall profits are defined as: Profits derived from all the designated health services of any component of
the group that consists of at least five physicians - overall profits must be divided in a reasonable and
verifiable manner
• Profits from all DHS for all physicians participating in the component of the group must be aggregated
prior to distribution
• Split-pooling of ancillary services revenue is now prohibited which may impact historical group
practice internal distribution plans and result in a need for compensation planning assistance
• A group practice physician can therefore not participate in more than one DHS distribution
methodology

Copyright © 2021 by SullivanCotter
Physician Self-Referral LawGroup Practice Exception
Special Rules for Profit Shares and Productivity Bonuses
26
• Contemplates and addresses the intersection of value-based activities
and compensation with group practice special rules
• Effective January 1, 2022 - Allowing groups time to revise
compensation plans and achieve compliance with Final Rules
Value-Based Enterprise Participation by Group Practice Physicians
• Profits from designated health services that are directly attributable to a group
practice physician’s participation in a value-based enterprise may be
distributed to the participating physician
• The value-based enterprise distribution is not subject to FMV

Copyright © 2021 by SullivanCotter
Modification to Safe Harbor
Anti-Kickback StatuteSafe Harbor PSA/Management Contract
27
Protects outcomes-based payments when certain requirements are met including:
• Collaboration between parties to:
‒ Measurably improve or maintain improvement in the quality of patient care, or
appropriately and materially reduce costs to, or growth in expenditures of, payors while
improving or maintaining quality of care for patients
• Payments are for outcomes measurement achievement or recoupment or reduced
payment for failure to achieve an outcome measure
• Outcomes-based payments must be conditioned on achieving one or more
legitimate outcome measures that are selected based on clinical evidence or
credible medical support measurably improving (or maintaining improvement in) the
quality of patient care and have benchmarks that are used to quantify:
‒ Improvements, or the maintenance of improvements in the quality of patient care
‒ A material reduction in costs to, or growth in, expenditures of payors while maintaining or
improving quality of care for patients or both

Copyright © 2021 by SullivanCotter
Anti-Kickback StatuteSafe Harbor PSA/Management Contract
Modification to Safe Harbor
28
Other requirements in addition to those under PSA Exception of Stark Law
• Must include the outcome measures that the agent must satisfy to receive payment
• Must include clinical evidence or credible medical support relied on to select each
outcome measure and must include the schedule for monitoring and assessing the
outcome measures
• The parties must do the following for each outcome measure under the agreement:
‒ Regular monitoring and assessment of the agent’s performance, including the impact of
the outcomes-based payment arrangement on patient quality of care and periodic
assessment and revision of benchmarks and remuneration to ensure remuneration is
FMV in an arm’s length transaction.
• The principal must have policies and procedures to promptly address and correct identified material performance failures or material deficiencies in the quality of care resulting from the arrangement
• The methodology for determining the aggregate compensation must be FMV and CR and
not consider volume or value of referrals

Copyright © 2021 by SullivanCotter
Modification to Safe Harbor
Anti-Kickback StatuteSafe Harbor PSA/Management Contract
29
The safe harbor does not protect payments:
• Related solely to internal cost savings for a principal
• Based solely on patient satisfaction convenience measures
• Made directly or indirectly by: a pharmaceutical manufacturer, distributor or wholesaler;
pharmacy benefit manager; laboratory company; compounding pharmacy; manufacturer of a
device or medical supply; other medical device distributor or wholesalers; an entity or
individual that sells or rents DMEPOS covered by federal health care programs
Copyright © 2021 by SullivanCotter
Scenarios, Case Study and Refinements to FMV Testing
3. Compensation Implications
30

Copyright © 2021 by SullivanCotter
FMV Testing Methods and Emerging Implications
31
Level 1
Level 2
Level 3
• Percentile ranking
• Compensation-per-production ratio
• Compensation-per-FTE considerations
Testing Description
• Additional analysis on any physicians falling
outside initial testing parameters
• Review individual components of compensation
• Identify remaining outlier physicians
• Expanded assessment of quantitative and
qualitative performance and circumstances
• Documentation of business judgment factors to
support upper-end compensation
The new Stark regulations support continued facts and circumstances considerations

Copyright © 2021 by SullivanCotter
Evidence of achievement of stretch goals for quality, service and efficiency may reduce
the reliance upon personal productivity, but the market and data is still in transition
FMV Compensation and Testing Considerations
32
The scrutiny on the market reasonableness of compensation, including aggregate compensation,
rates and correlation of work and performance to pay increases as compensation increases
Quantitative
Considerations
Qualitative
Considerations
Compensation Level
P75
P50
P90+
Wider
levels of
acceptable
correlation
Narrower
levels of
required
correlation
Highest
levels of
required
correlation
Attorney Client Privileged / Subject to Common Interest Agreement

Copyright © 2021 by SullivanCotter33
Key Takeaways
Compensation should/must
be structured to satisfy
various exceptions and
safe harbors
Compensation must not
exceed FMV
Compensation cannot take
into consideration volume or
value of Medicare referrals
Compensation above FMV
may be recharacterized
by outside entities as
payment for referrals
In addition to FMV,
compensation
arrangement(s) must be
commercially reasonable
Active enforcement
environment today
1
2
3
4
5
6

Copyright © 2021 by SullivanCotter
4. New Value-Based Exceptions / Safe
Harbors and Application

Copyright © 2021 by SullivanCotter
New Value-Based Framework Exceptions
Value-Based Arrangements
• Proposed rules intend to remove complexities that have inhibited movement to value-
based compensation arrangements
• Three similar but distinguished value-based categories were finalized:
Three Confirmed New Categories for Value-Based Exceptions
35
Stark Exceptions AKS Safe Harbors
1 Full Financial Risk Full Financial Risk
2Meaningful Downside
Financial Risk
Substantial Downside
Financial Risk
3 Value-Based Arrangement Care Coordination

Copyright © 2021 by SullivanCotter
Proposed New Value-Based Exceptions
36
Value-Based Arrangements
Newly-Defined Key Terms
Proposed rules provide fairly similar definitions for
numerous terms related to the value-based
exceptions/safe harbors:
• Value-Based Activity
• Value-Based Arrangement
• Value-Based Enterprise
• Value-Based Purpose
• VBE Participant
(w/ more limitations under the AKS rules)
• Target Patient Population

Copyright © 2021 by SullivanCotter
Option 1
Value-Based ExceptionsOption 1
Stark Exceptions AKS Safe Harbors
Full Financial Risk Full Financial Risk
• Requires full financial risk for all patient
care for at least 12 months
• Remuneration for achieving
value-based purposes
• Tied to health improvement of a defined
patient population
• May not reduce/limit medically
necessary services or be conditioned on
referrals of patient or business not
covered under the agreement
• Allows industry participants
(e.g., Pharma, DME, etc.)
• Other standard requirements
• Confirmed no separate
FMV requirement
• Similar requirements as Stark
• Under the value-based framework,
neither the Stark nor AKS regulations
require that remuneration be FMV, nor
do they prohibit taking into account the
volume or value of referrals of patients
within the target patient population or
business covered by the value-based
arrangement (traditional Stark and AKS
exceptions require that compensation
represent FMV and prohibit taking into
account volume or value of referrals)
37

Copyright © 2021 by SullivanCotter
Option 2
Value-Based ExceptionsOption 2
Stark Exceptions AKS Safe Harbors
Meaningful Downside Financial RiskSubstantial Downside
Financial Risk
• Physicians must accept meaningful downside
financial risk for failure to achieve the VB
purpose during the entire term of the
agreement
• May not reduce/limit medically necessary
services or be conditioned on referrals of
patient or business not covered
• “Meaningful” risk is defined as the potential to
repay or forgo 10% or more of the total value
of the remuneration the physician would be
eligible to earn under this exception
• Same standard requirements
• Confirmed no separate FMV requirement
• Similar requirements as Stark
• However, the value-based enterprise
must also share in the substantial
downside risk
• Methodologies to meet risk
requirements include: (1) Shared
Savings and Losses [30%
threshold]; (2) Episodic Payment
[20% threshold]; (3) VBE Partial
Capitation
38

Copyright © 2021 by SullivanCotter
Option 3
Value-Based ExceptionsOption 3
Stark Exceptions AKS Safe Harbors
Value-Based Arrangement Care Coordination
• Potential default option for initial entry
into VBE participation
• Does not require financial risk
• Requires higher documentation of
performance results based upon clinical
evidence or outcomes results
• May not reduce/limit medically
necessary services or be conditioned on
referrals of patient or business not
covered
• Quarterly monitoring requirements
• Same standard requirements
• Permits only in-kind remuneration
between a value-based enterprise and
other VB participants to encourage care
coordination
• The VBE participant receiving the in-
kind remuneration must contribute at
least 15 percent of either the cost or the
fair market value of the
in-kind remuneration
• Unlike Stark exception, AKS safe harbor
requires documentation that the
arrangement is CR
39

Copyright © 2021 by SullivanCotter
Proposed New Value-Based Exceptions
For Options 1-3:
• Value-based arrangement set forth in writing
• Signed by the parties
• Include key descriptions of:
‒ Value-based activities to be undertaken
‒ Links to value-based purposes
‒ Links to target population
‒ Nature or type of remuneration
‒ Methodology to determine earned remuneration
‒ Performance or quality standards
‒ Performance metrics that are objective and measurable
Shared Standard Requirements
40
Value-Based Exceptions

Copyright © 2021 by SullivanCotter
Potential Key Implications
• New opportunities to enhance alignment with physicians/groups participating in qualifying
value-based arrangements
• Potential substantial revision (and reduction) of prior FMV testing for qualifying exceptions
• However, likely enhanced focus upon newly clarified CR requirements
• Anticipated further physician/group pressures to expand participation in value-based
arrangements – particularly among employed physicians that have been capped or have
received relatively low value-based performance (VBP) compensation
• Increasing need for access to expertise to design, implement, monitor and report sustained
achievement of value-based purposes for new qualifying value-based arrangements
41
New Stark & AKS Regulations
– Value-Based Exceptions
Copyright © 2021 by SullivanCotter
Outstanding Questions
• What type of value-based purposes meet the proposed value-based
arrangements requirements?
• What types of documentation are requirement to support CR for
value-based arrangements?
• What levels of “outcomes” measurement results will meet the new risk
options requirements?
• For the full risk option, what types and levels of expense risk (e.g., medical costs,
overhead costs and/or other shared infrastructure/support costs) must be assumed?
• Are there implied caps on the level of value-based arrangements payments to physicians
under considerations of their role/participation to achieve value-based purposes or other
CR considerations?
42
New Stark & AKS Regulations
– Value-Based Exceptions

Copyright © 2021 by SullivanCotter
Scenarios/Case Study
Value-Based Arrangements
43

Copyright © 2021 by SullivanCotter
Potential Application of Value-Based Arrangements
Across Affiliation Continuum
44
Likely Value-Based
Arrangement Compensation
Design Inclusion
1 Telemedicine and Non-Medical Staff Referring Physicians
2 Traditional Hospital Independent Medical Staff ✓
3 Physician Recruitment and Retention Support
4 Medical Directorship Services
5 MSO (Practice Mgmt)
6 Joint Managed Care (with limited risk) ✓
7 Specialty Institute / Service Line Co-Management ✓
8 Joint Venture and Shared Equity ✓
9 Clinical Integration and Payer Contracting ✓
10 Exclusive Foundation / PSA ✓
11 Full Practice Integration / Employment ✓

Copyright © 2021 by SullivanCotter
Discussion of Sample Compensation Scenarios
45
• Hospital pays employed physician $600,000 for all clinical services and physician is a
full-time provider of clinical services only
• Physician’s duties include general duties around quality, access, service, outcomes
and cost reduction, but there is no value-based arrangement in place and there are
no separate payments for these quality/value duties and responsibilities
• Hospital participates in shared savings programs and physician works to help
hospital achieve a shared savings payment from the relevant payor
• Hospital is willing to share its payment with physician in light of physician’s
participation in the shared savings program
‒ How formal does this have to be to qualify for a value-based exception?
‒ If physician gets a $60,000 payment, does hospital’s compensation consultant
review the FMV of the $600,000 without the shared savings payment, or the
aggregate $660,000?
‒ If the FMV review is of the $600,000 only, is the physician a 1.0 full-time
equivalent for purposes of that review?
‒ If this has to be a formal arrangement, has the allocation (to the VBA) of the
physician’s contributions in the areas of quality, access, service, outcomes, and
cost reduction actually made it more difficult to support the $600,000 as FMV
(assuming some level of facts and circumstances support was needed)?
Example: Shared Savings Payment

Copyright © 2021 by SullivanCotter
Discussion of Sample Compensation Scenarios
46
• Assume hospital pays employed physician $600,000 for all clinical
services and physician is a full-time provider of clinical services only
• Hospital wishes to formalize some of physician’s clinical duties
and goals (around quality, access, service, outcomes and cost reduction)
and convert them to a value-based arrangement
• Hospital will take $150,000 of the current compensation and use
that as the basis for the value-based arrangements payment and
will add 10% to that amount if the physician meets certain goals
‒ When the compensation consultant assesses the FMV of the
$450,000 in other clinical compensation, does the consultant still
treat the physician as a 1.0 full-time equivalent clinician or as
something less than a 1.0 FTE due to the VBA carve-out?
Example: Compensation Carve-Out for Partial Payment Risk

Copyright © 2021 by SullivanCotter
Discussion of Sample Compensation Scenarios
47
• Independent physician group practice (PGP) whose members make referrals to hospital
• PGP approaches hospital to discuss collaboration opportunities and requests that hospital
furnish a staff member (e.g., advanced practice registered nurse, nurse navigator, care
coordinator) to support the collaboration between the hospital and the PGP
• PGP and hospital agree to create a value-based enterprise whose activities will
be supported by the hospital-furnished staff member
• Neither the value-based enterprise, the hospital, nor the PGP will assume
any risk under the value-based arrangement
‒ Does furnishing a staff member constitute in-kind remuneration under the
Care Coordination Safe Harbor?
‒ May the hospital provide financial reimbursement to the PGP if the PGP
employs the staff member?
‒ Can the PGP’s provision of space, equipment, etc. used by the staff member be included in
the PGP’s 15% minimum contribution?
‒ Can the staff member provide services to patients not included within the value-based
enterprise’s target patient population?
‒ What functions may the staff member fulfill?
‒ What are the parties’ oversight obligations with respect to the staff member?
Example: Provision of Staff to Independent Physician Group Practice

Copyright © 2021 by SullivanCotter
Potential Key Implications
The new rules are signaling more flexibility in value-based
arrangements between health systems and physicians,
including expanded options that include financial risk. 1
2The new rules also permit expanded use of “outcomes”
performance metrics to take into account financial savings and
enhanced clinical quality for a defined population of patients.
3With respect to FMV and CR, the new definitions are less
formulaic and more situation-specific. Value-based
arrangements payments may not require FMV testing, but
aggregate payments may require both FMV and CR.
48

Copyright © 2021 by SullivanCotter
5. Compliance Program Implications
49

Copyright © 2021 by SullivanCotter
Compliance Program Implications
50
Compensation
Governance
PoliciesRequirements
for Exceptions
and Safe
Harbors
Facts and
Circumstances
Capture
Contract
Lifecycle
ManagementAnnual
Performance
Monitoring
Requirements for
Metric Selection
Education and
Training
Risk
Management
Tools and
Thresholds
Compliance
Program
Refresh

Copyright © 2021 by SullivanCotter
Compliance Program Implications
51
Expanded Stark Exceptions and related AKS Safe Harbors
offer new opportunities for achieving regulatory compliance
Requirements for Exceptions and Safe Harbors
Review and refine existing compensation governance
policies to provide a framework for achieving compliance
Evaluate existing processes to improve capture and
documentation of relevant facts and circumstances
including business purpose for the arrangement
Compensation Governance Policies
Risk Management Tools and Thresholds
Contract Request Process
Review and refine existing risk management FMV
guidelines used by your organization and
incorporate CR elements

Copyright © 2021 by SullivanCotter
Compliance Program Implications
52
No longer just good practice, annual performance
monitoring is requirement for meeting some exceptions
Education and Training
Annual Performance Monitoring
Contract Lifecycle Management
Additional requirements for contract management
A broader organizational understanding will help to
support the organization’s compliance program
Requirements for Metric Selection
Internal cost savings and metrics may not be sufficient for meeting
regulatory requirements for exceptions and safe harbors

Copyright © 2021 by SullivanCotter
Review and Approval GuidelinesExample
53
Examples of arrangements that must be approved by Board Level Committee are
typically documented in the Management Committee Charter
ActivityManagement
Committee
Board
Committee
Physician Compensation Philosophy and Design
Physician compensation philosophy, guidelines, timeline and approval process Recommend Approve
Significant changes to physician compensation plans/strategy/benefits plan* Recommend Approve
Physician Compensation Review
Physician clinical cash compensation offers or changes:
Below the 75th percentile Approve None
Between the 75th and 90th percentiles and supported by productivity Approve None
Between the 75th and 90th percentiles and not supported by productivity Recommend Approve
Exceeding the 90th percentile* Recommend Approve
Where total cash compensation exceeds $750,000 Recommend Approve
Highly compensated physicians (exceeding organization-defined threshold)* Recommend Approve
Independent contract arrangements exceeding 75th percentile of the market* Recommend Approve
Disqualified persons under Intermediate Sanctions and physician leadership roles Recommend Approve
Biennial FMV and commercial reasonableness review of all physicians Prepare/oversee report Approve
Physicians Compensated on an Approved Compensation Plan
To Be Developed
*A FMV opinion letter, completed by an independent third party, is recommended in these instances

Copyright © 2021 by SullivanCotter
Additional Value-Based Enterprise Considerations
54
Value-based enterprise (VBE) governance and monitoring considerations include:
• Regardless of whether VBE is a separate legal entity, it must be
organized pursuant to a written governing document that describes:
‒ The VBE’s value-based purposes
‒ How the VBE participants intend to achieve the VBE’s
value-based purposes
• The VBE must have identified accountable body or
accountable person
• The VBE’s monitoring activities must be tailored to
the level of risk assumed by the VBE

Copyright © 2021 by SullivanCotter
CR Assessment Considerations and DocumentationExample of Certain (but not exhaustive) Factors Typically Examined
55
What is the Business Purpose for this Arrangement?
1Community Need: Briefly summarize the community need met by this physician’s compensation
arrangement (physician workforce plan, other clinical need within provider’s community, number of
patients cared for by physician, demand for clinical specialty, etc.).
2Recruitment/Staffing Plans and Business Purpose: Briefly describe the recruitment/staffing
plans and/or documents describing the business purpose of this on-call proposed arrangement.
3 Licensure/Regulatory/Accreditation Obligation: Briefly describe the regulatory or licensure
obligation met by this arrangement (e.g., to maintain a certain trauma level designation).
4Call Panel: How many physicians and/or APPs will be on this call panel? Do all qualified physicians
within the specialty have an equal opportunity to participate in the panel? Confirmation call panel
physicians meet medical staff qualification criteria required to provide call services including but not
limited to privileges, credentialing etc.
5 Other Legitimate Business Purpose: Briefly describe any other legitimate business
purpose(s) this physician’s employment satisfies.

Copyright © 2021 by SullivanCotter
Contract Management and Documentation
56
• Additional focus on commercial reasonableness implies need to
capture facts and circumstances and to revisit at
contract renewal
• New metric selection criteria and requirements for
monitoring performance
• Requirement to maintain documentation of value-based
purpose and how the arrangement is meeting the
value-based purpose
• Requirement to maintain documentation of distribution
methodologies for value-based arrangements
Expanded Documentation and Storage Requirements

Copyright © 2021 by SullivanCotter
Top 10 Implications of Final Stark/AKS Rules
57
What does the final rule change?
Market surveys are still relevant for FMV assessments. here. 1
Full or “meaningful risk” value-based arrangements can be carved out for FMV purposes if they meet all requirements for Stark Exception and AKS Safe Harbors. For the third option, compensation must still be CR.
6There is no bright line rule for P75 compensation; facts and circumstances matter. 2
“Meaningful risk” definition has been softened to 10% downside risk or forgoing compensation to encourage participation.7
Benchmarking tools should not be used alone to determine FMV.3
The final rule puts more pressure on value-based arrangements to monitor performance and produce results in a short timeframe.8
CR is arguably just as important as FMV; assessment and documentation of CR.4
The final rule tightens the ability within group practices to distribute DHS profits within subgroups of physicians.9
Pay practices information and typical practices may add additional support for evaluation of compensation design CR.5
Restrictions on investments in infrastructure to enhance value-based collaboration are relaxed (cyber-security).10

Copyright © 2021 by SullivanCotter
6. Answering Your Questions
58
All participants have
access to a copy of the
slides via Converve.

Copyright © 2021 by SullivanCotter
Appendix
59

Copyright © 2021 by SullivanCotter
Overview of SullivanCotter Advisory Services
60

Copyright © 2021 by SullivanCotter
SullivanCotter Physician and APP Enterprise CapabilitiesLeading Change in Health Care
Innovative Technology,
Products and Solutions
Unparalleled Survey Data
and Resources Comprehensive
Advisory Services
• Dedicated practice of 60+ consultants
• Deep expertise and knowledge of
physician services and models of care
• Tailored physician and APP
compensation and benefits reward
program strategies that align with
systems goals
• Implementation guidance
• Data analytics with national intelligence:
– Benchmarks360™
– PPMT™
– Physician Needs Assessment
• National trends and benchmarking:
– Single source of truth
– Real-time insights
– Administration and contract
management
• Large Clinic® Group
• National APP Advisory Council
• Largest compensation and productivity
surveys with custom data analytics
• Broad research within the largest
integrated health care systems
Workforce and
Care Model
Optimization
Client
Networks
and Firm
Affiliations
Business
Valuation
and Due
Diligence
Governance
and
Regulatory
Expertise
Compensation
Strategy and
Design
Center for
Information,
Analytics and Insight
Technology
and Solutions
Center for
Information,
Analytics and
Insight
61

Copyright © 2021 by SullivanCotter62
Health systems are evolving based on their unique strategies,
which are influenced by the dynamic market environment
Physician WorkforceComprehensive Advisory Services and Technology Solutions
Physician Workforce
Advisory Services
Physician
Needs
Assessment
Business/
Practice
Valuations and
Transaction
Assistance
Physician/
Hospital
Model
Development
Professional
Services (incl.
FMV/CR)
Valuations
Value-Based
Care and
Population
Health
Readiness
Physician
Compensation
Strategy, Design
and
Implementation
Physician/
Hospital
Affiliation
Assessment
Clinical
Workforce
Optimization
Leadership
Structures and
Performance
Management