new zealand influenza pandemic action plan -...
TRANSCRIPT

New Zealand Influenza Pandemic Action Plan
Version 14
National Health Emergency Plan: Infectious Diseases, Appendix III
200
5
DRAFT FOR DISCUSSION

New Zealand Influenza Pandemic Action Plan v14 NHEP:ID, Appendix III
Draft for Discussion 16th November 2005 ISBN 0-478-29902-8 HP 4206 Ministry of Health 133 Molesworth Street PO Box 5013 Wellington http://www.moh.govt.nz/pandemicinfluenza
Table of Contents
NOTES............................................................................................................................................................... 5 ACRONYMS AND ABBREVIATIONS............................................................................................................... 6 PANDEMIC INFLUENZA................................................................................................................................... 7
INTRODUCTION................................................................................................................................................. 7 CHARACTERISTICS ........................................................................................................................................... 7 PANDEMIC INFLUENZA....................................................................................................................................... 7 POTENTIAL SCALE OF A PANDEMIC .................................................................................................................... 7 STAGES OF PANDEMIC INFLUENZA ..................................................................................................................... 8 INTER-PANDEMIC PERIOD.................................................................................................................................. 8
ACCELERATED PANDEMIC PLANNING ........................................................................................................ 9 MINISTRY OF HEALTH PANDEMIC PLANNING ....................................................................................................... 9 WHOLE OF GOVERNMENT PANDEMIC PLANNING ................................................................................................10
STRATEGY OF NEW ZEALAND PANDEMIC PLANNING..............................................................................11 PANDEMIC MANAGEMENT ............................................................................................................................11
MINISTRY OF HEALTH RESPONSE .....................................................................................................................11 COMMUNICATIONS WITH THE PUBLIC AND MEDIA................................................................................................11 VACCINATION..................................................................................................................................................12 DRUG TREATMENT AND ANTI-VIRALS.................................................................................................................12 STEPS TO REDUCE THE RATE OF SPREAD .........................................................................................................12 IMPACT ON SOCIETY ........................................................................................................................................13 CARE IN THE COMMUNITY ................................................................................................................................13 CARE OF DEPENDANTS....................................................................................................................................13 CARE OF THE DECEASED .................................................................................................................................14
NEW ZEALAND INFLUENZA PANDEMIC ACTION PLAN .............................................................................15 INTERPANDEMIC PERIOD .....................................................................................................................16
Interpandemic Period Phase 1 .............................................................................................................16 Interpandemic Period Phase 2 � Scenario 1 ........................................................................................18 Interpandemic Period Phase 2 � Scenario 2 � CODE WHITE .............................................................19
PANDEMIC ALERT PERIOD ...................................................................................................................20 Pandemic Alert Period Phase 3 � Scenario 1 � CODE WHITE............................................................20 Pandemic Alert Period Phase 3 � Scenario 2 � CODE WHITE............................................................22 Pandemic Alert Period Phase 3 � Scenario 3 � CODE YELLOW ........................................................23 Pandemic Alert Period Phase 3 � Scenario 4 � CODE YELLOW ........................................................23 Pandemic Alert Period Phase 4 � Scenario 1 � CODE RED................................................................24 Pandemic Alert Period Phase 4 � Scenario 2 � CODE RED................................................................26 Pandemic Alert Period Phase 5 � Scenario 1 � CODE RED................................................................27 Pandemic Alert Period Phase 5 � Scenario 2 � CODE RED................................................................29
PANDEMIC PERIOD................................................................................................................................30 Pandemic Period Phase 6 � Scenario 1 � CODE RED........................................................................30 Pandemic Period Phase 6 � Scenario 2 � CODE RED........................................................................31
POST PANDEMIC PERIOD .....................................................................................................................32 Post Pandemic Period � CODE GREEN..............................................................................................32
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 3

APPENDIX A: INTERSECTORAL PANDEMIC GROUP (IPG) � SUMMARY OF WORK PROGRAMMES ....33 APPENDIX B: COMPARISON OF PHASES PUBLISHED BY WHO IN 1999 AND 2005................................35 APPENDIX C: ALERT CODE COMMUNICATIONS � MINISTRY OF HEALTH AND DHB ACTIONS............36 APPENDIX D: INTERIM GUIDELINES FOR PERSONAL PROTECTIVE EQUIPMENT .................................37
PURPOSE OF THIS DOCUMENT ..........................................................................................................................37 HOW IS PANDEMIC INFLUENZA TRANSMITTED?....................................................................................................37 HEALTH CARE WORKERS..................................................................................................................................37 FIRST RESPONDERS ........................................................................................................................................37 THE PUBLIC.....................................................................................................................................................37 GENERAL AND SPECIFIC INFECTION PREVENTION AND CONTROL MEASURES..........................................................37 HAND HYGIENE................................................................................................................................................38 RESPIRATORY HYGIENE/COUGH ETIQUETTE .......................................................................................................38 SOCIAL DISTANCING.........................................................................................................................................38 PROTECTIVE BARRIERS....................................................................................................................................39 USING MASKS .................................................................................................................................................39 RECOMMENDATIONS FOR PPE USE ..................................................................................................................39 USING DISPOSABLE SURGICAL MASKS, GLOVES AND GOWNS/APRONS...................................................................39 GLOVES AND GOWNS/APRONS (FULL PPE) ........................................................................................................39 USING THESE MEASURES HELPS COMPLY WITH THE HEALTH AND SAFETY IN EMPLOYMENT ACT 1992 ....................39
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 4

Notes 1. This document, the New Zealand Influenza Pandemic Action Plan, is the proposed update to
Appendix III of the National Health Emergency Plan: Infectious Diseases (NHEP:ID), released June 2004 and available at www.moh.govt.nz/nhep
2. This is a dynamic working document and will be continuously updated over the coming weeks and
months. 3. Please observe version control in the footer to determine last edited time / date. 4. This version should be discarded if subsequent versions are received. 5. Please do not circulate this document outside your organisation without permission from the Ministry
of Health (email [email protected]). 6. Framework (Periods, Phases) is fixed based on the new WHO guidelines (2005). Scenarios are New
Zealand-specific and may differ from other countries. 7. Content is subject to change and serves as a basis for discussion and development. 8. All �Actions� are cumulative with those from the preceding Phase.
9. Critical decision points are noted in the document as !!KKEEYY DDEECCIISSIIOONN"" indicating where a major
decision will need the involvement of DES.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 5

Acronyms and Abbreviations
AMF Additional Mortuary Facilities BNZ Biosecurity New Zealand CAA Civil Aviation Authority CBAC Community-Based Assessment Centre CCS Critical Clinical Supplies CDEM Civil Defence Emergency Management CIMS Coordinated Incident Management System DES Domestic and External Security (Group) DG Director-General (of Health) DHA (Australian) Department of Health & Ageing DHB District Health Board DOL Department of Labour DoPH Director of Public Health DPMC Department of Prime Minister and Cabinet ESR Environmental Science and Research Ltd FAQ Frequently Asked Questions HA Health Act 1956 H2H Human to Human (Transmission) HPAI Highly Pathogenic Avian Influenza ILI Influenza-Like Illness IPG Intersectoral Pandemic Group JTO Journalists Training Organisation MAF Ministry of Agriculture and Forestry MED Ministry of Economic Development MFAT Ministry of Foreign Affairs and Trade MCDEM Ministry of Civil Defence & Emergency Management MoE Ministry of Education MoH Ministry of Health MOoH Medical Officer of Health MSD Ministry of Social Development NHEP National Health Emergency Plan NHEP:ID National Health Emergency Plan: Infectious Diseases NIAVM Neuraminidase Inhibitor Antiviral Medication (Tamiflu) NIR National Immunisation Register NZFSA New Zealand Food Safety Authority ODESC Officials Committee for Domestic and External Security Oped Opinion/Editorial OSH Occupational Safety and Health PEG Pandemic Emergency Group PEP Post-Exposure Prophylaxis PHE Public Health Emergency PHO Primary Health Organisation PHS Public Health Services PHU Public Health Unit PIRC Pandemic Influenza Reference Committee PITAG Pandemic Influenza Technical Advisory Group PPE Personal Protective Equipment RFP Request For Proposal RNZCGP Royal New Zealand College of General Practitioners WHO World Health Organisation
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 6

Pandemic Influenza Introduction An influenza pandemic is the most likely event to cause a large-scale health emergency. Three major influenza pandemics occurred in the 20th century, reaching New Zealand in 1918, 1957 and 1968. Recent estimates put mortality from the 1918 pandemic at between 50 and 100 million worldwide. In this country, the 1918 pandemic is estimated to have infected a third to half of the entire population, causing approximately 8000 deaths. This appendix addresses some of the key considerations specific to a new pandemic influenza threat. Characteristics Influenza is a highly contagious viral disease of the respiratory tract. It continues to be a major threat to public health worldwide because of its ability to spread rapidly through populations and to cause a range of complications. Relatively minor epidemics of influenza typically occur in New Zealand during winter months, often affecting all age groups and causing many complications, including viral or bacterial pneumonia. Influenza is a significant and under-recognised cause of mortality in the New Zealand population. There are approximately 100 deaths per year directly attributable to influenza, but this does not include many cases where influenza contributes to an elderly or chronically ill person�s death. Influenza is characterised by rapid onset of respiratory and generalised signs and symptoms, including fever, chills, sore throat, headache, dry cough, fatigue and aching. Influenza is easily spread through droplets from an infected person (suspended in the air through coughing or sneezing) being inhaled by another person, or through contact with contaminated objects. The incubation period can range from one to seven days, but is commonly one to three days. Adults are contagious for one to two days before most symptoms start until about day five of the illness. Children generally remain infectious for up to seven days. Pandemic Influenza Pandemics are characterised by the global spread of a novel type of influenza virus, and can cause unusually high morbidity and mortality for an extended period. Most people are immunologically naive to the novel virus and therefore susceptible to infection. A pandemic can overwhelm the resources of a society due to the exceptional number of those affected. A pandemic requires not only the emergence of a new viral subtype, but also that the virus has the capacity to spread efficiently from person to person, and to cause significant human illness. Potential Scale of a Pandemic The Ministry of Health (the Ministry) has taken a �maximum credible event� approach to pandemic planning. Using the November 1918 pandemic influenza wave in New Zealand as a basis, the Ministry has developed a standard planning model to provide planners with an indicative pandemic wave scope, scale and duration. The New Zealand standard planning model assumes a pandemic wave in which 40% of the NZ population become ill over an 8-week period. The model indicates that over 1.6M people could become ill over this time. The peak incidence is over weeks 3 � 5, when about 1.3M people, around a third of New Zealand�s population, would be ill, convalescent, or only just recovered.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 7

The model assumes a total case fatality rate of 2%, which would see about 33,000 deaths over the 8 week period, peaking at about 10,000 in week 4. It is important to note that this is not a prediction or a forecast of what will happen should a pandemic occur � it is not possible to make any such forecast before a pandemic develops. A 21st century pandemic may not reflect the course, incidence, or fatality rates of the 1918 pandemic. The model�s purpose is to provide a structure around which Health, Government and New Zealand as a whole can plan for a very large event with severe impacts on all aspects of society. As the 1918 pandemic in New Zealand is relatively well understood and documented it has been selected to provide the basis for the standard planning model, and clearly it is necessary that plans be based on the extreme circumstances that 1918 may represent. Stages of Pandemic Influenza The World Health Organization (WHO) has a set of definitions that classify the stages of a pandemic. They will announce the onset of Phase 1 and progression to subsequent phases based on evidence collected by the WHO Pandemic Taskforce and international consultation. These definitions are given in the table on p35, along with the macro characteristics that are used to define escalation steps to each stage (or sub-stage). The time periods between confirmation and widespread outbreak are unlikely to be predictable and will quite likely be compressed. If the pandemic has a particularly rapid onset, some of the phases may progress very rapidly or be missed altogether. Again, this points to the need to prepare emergency responses in the inter-pandemic period. Inter-pandemic Period The National Pandemic Planning Committee (NPPC), an advisory committee to the Ministry of Health, provides advice on the appropriate strategies to progress inter-pandemic measures to strengthen New Zealand�s response capacity. The National Influenza Immunisation Strategy Group (NIISG) co-ordinates the promotion of influenza vaccination and awareness, thereby providing the first line of defence against infection in the workforce and general population. While routine influenza vaccination is unlikely to protect against a new pandemic strain, the immunisation programme has the virtue of raising general awareness of influenza. DHB major incident and emergency plans and regional incident co-ordination plans need to provide for situations such as influenza pandemics. Among other things, these plans need to make allowance for the delivery of services and the maintenance of infrastructure in the face of both increasing absenteeism (caused by the pandemic) and demand. In the pandemic situation, it is particularly important to ensure that any emergency plan meets the needs and requirements posed by the primary health care sector, because this is where demand will most likely manifest itself. An effective national surveillance system during the inter-pandemic period is an essential component of preparedness. There are currently two national influenza surveillance systems in New Zealand.
• The general practice (GP) sentinel disease and virological surveillance system, involving more than 90 practices, operates annually during the winter months (May to September), recording the daily number of consultations that fit the case definition of an influenza-like illness. Collated national data is available on the ESR website (www.esr.cri.nz).
• Ongoing virological surveillance is carried out by designated virology diagnostic laboratories, and by the ESR virology laboratory. Specimens are collected from hospitalised patients with an influenza-like
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 8
illness throughout the year for analysis. Data collected from these laboratories is reported nationally in the Virology Weekly Report.
An important inter-pandemic priority is to enhance and improve influenza surveillance. With the assistance of NIISG and the NPPC, the Ministry of Health will collect and analyse data to allow early determination of national trends, using its networks to facilitate prompt public health action. The Ministry of Health will promote influenza immunisation and awareness to the public and health care professionals.
Accelerated Pandemic Planning
Ministry of Health Pandemic Planning Planning for an event of the scale, scope, complexity and potential impact of a pandemic requires expertise from a range of fields. Some aspects of the national response are clearly beyond Health�s scope. Accordingly the Ministry is engaged in a whole of government response with several groups which have defined pandemic planning roles and functions. The Ministry has established an internal Pandemic Emergency Group (PEG) to oversee and coordinate pandemic planning for the Health sector. PEG is partly a subset of, and reports to, the National Health Emergency Plan (NHEP) group. PEG and NHEP report to the Ministry of Health Executive Team and the Minister through normal Ministry channels (see Figure 1). The Pandemic Influenza Technical Advisory Group (PITAG) has been established to provide expert clinical, virological, epidemiological, infection control and ethical advice to inform Ministry pandemic response planning. PITAG will inform Ministry policy on communications, key messages, public health interventions and a range of associated issues. A large number of groups and organisations within the wider health sector will be progressively involved in pandemic planning. Because of the scope, range and complexity of relationships involved a Pandemic Influenza Reference Committee (PIRC) has been established to ensure a coordinated approach without duplication of effort or communication. Work is also being commenced to facilitate an effective flow of information between DHBs and the primary health care sector on the management of a pandemic. Primary care practitioners including General Practitioners, Accident and Medical practitioners, pharmacists and primary care nurses will be placed under great pressure and will need ongoing information, advice and assistance. Other primary health carers, such as those working with the disabled and those in aged care, will need similar help.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 9

Figure 1. NEW ZEALAND PANDEMIC PLANNING PROCESS
P
Em
EmPITAG
Pandemic Influenza Technical Advisory Group
PIRC Pandemic Influenza
Reference Committee
DES Domestic and External
HEA
LTH
SEC
TOR
LTH NT
DHBs / Other District Health Boards and other providers
Whole of Government Pandemic Plan The Ministry has engaged with the wider gThe IPG coordinates thirteen workgroups led by a key agency. Further detail about th
Table 1. LIST OF INTERSE
WORKGROUP Health Border Economy Workplaces Education Community & Logistics Law, Order & Emergency Services External Infrastructure Welfare Coordination Communications Legislation
New Zealand Influenza Pandemic Action Pla
MINISTER
Minister of Health
PEG andemic Emergency
Group
NHEP-AG National Health
ergency Plan Advisory Group
NHEP-SG National Health
ergency Plan Steering Group
IPG Intersectoral Pandemic
Group
ET Ministry of Health Executive Team
DPMC Department of Prime Minister and Cabinet
Security
ODESC Officials Committee for Domestic and External
Security
MIN
ISTR
Y O
F H
EA
WH
OLE
OF
GO
VER
NM
E
ning
overnment sector through the Intersectoral Pandemic Group (IPG). addressing critical areas of the national pandemic response, each ese workgroups can be found in Appendix A (page 33).
CTORAL WORKGROUPS AND LEAD AGENCIES
LEAD AGENCY Ministry of Health (MoH) NZ Customs Service Treasury Department of Labour Ministry of Education Ministry of Civil Defence & Emergency Management NZ Police Ministry of Foreign Affairs and Trade Ministry of Economic Development Ministry of Social Development Department of Prime Minister & Cabinet (DPMC) MoH / DPMC DPMC / Crown Law
n v14: DRAFT FOR DISCUSSION 10

Each lead agency has accepted responsibility for developing workgroup action plans coordinated between all other agencies involved in their particular workgroup area. Customs, for example, leads the border workgroup, which includes Aviation Security, Maritime Safety Authority, ports, airports, Biosecurity and other relevant agencies who have to work together in a coordinated manner to enable border management or closure in the event of a pandemic.
Strategy of New Zealand Pandemic Planning New Zealand pandemic planning is based around a sequential five-stage strategy:
STRATEGY POTENTIAL TRIGGER GOAL Planning �Plan for it�
Interpandemic period To plan to reduce the health, social and economic impact of a pandemic on New Zealand.
Border Management �Keep it out�
Human-to-human transmission overseas, OR very high suspicion of human-to-human transmission overseas, OR Australia and/or Singapore close borders.
To keep pandemic influenza out of New Zealand.
Cluster Control �Stamp it out�
Human pandemic strain case(s) found in New Zealand.
To control and/or eliminate any clusters that may be found in New Zealand.
Pandemic Management �Manage it�
Multiple (>10) clusters at separate locations, or clusters spreading out of control.
To reduce the impact of pandemic influenza on New Zealand�s population.
Recovery �Recover from it�
Population protected by vaccination, or pandemic abated in New Zealand.
To expedite the recovery of population health where impacted by the pandemic, pandemic management measures, or disruption to normal services.
NB: Movement into Border Management, Cluster Control or Pandemic Management is a decision for DES.
Pandemic Management Ministry of Health Response The Ministry of Health strategic response will utilise the framework detailed in the body of this Plan. As an emergency escalates, greater Ministry resources will need to be dedicated to the response. As a result, there should be an understanding and expectation that, as the emergency escalates, Ministry business will be affected. Ministry business is also likely to be affected by high levels of illness among staff. This scenario will be replicated in all government departments, sectors and industry as a whole. Communications with the Public and Media A key role in a pandemic is to provide clear and accurate information to the public. This will facilitate home care and also help to alleviate some of the pressure on health sector services. This material can be prepared in the inter-pandemic period, but it is important that it is either generic or easily modified to reflect specific circumstances.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 11

Channels of communication that will be considered for use during a pandemic include:
• fact sheets and FAQs that include general information on influenza vaccines, home nursing, medication and treatment guidelines � these can be produced physically or displayed electronically on the Ministry of Health website (www.moh.govt.nz)
• video presentations for broadcast via electronic media • establishment of a pandemic national free phone line to provide information to the public � the Ministry
of Health has a phone line available for emergencies that can be put into action within a few hours • national advertisements to increase awareness of the national response to the pandemic • regular media briefings to ensure accurate and up-to-date reports on the status of the pandemic.
Vaccination New Zealand does not have the capacity to manufacture human vaccines, but has an agreement in place with an Australia-based manufacturer to get priority access to vaccines in the event of a future influenza pandemic. However, because a vaccine that will protect against the pandemic strain won�t be able to be produced until that strain is actually identified, there will be a delay between declaration of the pandemic and the arrival of the vaccine supplies in New Zealand. The vaccine strategy is to immunise all New Zealanders once supplies are available. Drug Treatment and Anti-virals Many complications from influenza are due to secondary infection with bacterial pathogens. Antibiotics are required for secondary infections, although ineffective in the treatment of uncomplicated influenza. The anti-viral drugs amantadine, zanamavir and oseltamivir (all currently licensed in New Zealand) can shorten the course of infection if given early in the disease, and can provide short-term protection against influenza. Only oseltamivir (�Tamiflu�) is licensed for both treatment and prophylaxis. The Ministry has followed WHO advice and secured a Tamiflu stockpile sufficient to treat 21% of the population. During a pandemic, ongoing flexible recommendations for anti-viral treatment and prophylaxis will be made by the PITAG, with expert advice from relevant agencies and committees (e.g., the NIISG, Pharmac and Medsafe). WHO is developing guidelines for the use of anti-viral agents during pandemics, and these will also assist in future contingency planning. DHBs need to consider the need to build their own supplies of anti-viral drugs in such an emergency, over and above the supplies held in the national stockpile. It is possible that the effective use of any or all of these medicines may be limited in a pandemic because of the development of anti-viral resistance in the pandemic strain. Steps to Reduce the Rate of Spread While it would be very difficult to halt the spread of a future influenza pandemic once the virus has entered New Zealand, there are options to slow transmission that should be considered to slow its advance. These will help reduce pressure on health services over a longer time period and increase the opportunity to protect people, when a vaccine becomes available. Such measures include:
• recommending that sick people stay at home • advising the public against unnecessary travel • utilising the powers of medical officers of health to cancel public events • closing childcare facilities, schools and tertiary education institutions.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 12

Impact on Society A pandemic will likely be characterised by a high level of absenteeism in the workforce as people fall ill or stay at home to care for sick relatives. Essential services such as police, fire, transportation, communications and emergency management services need to be maintained during a pandemic. Other services and supplies � including food, water, gas, electricity supplies, educational facilities, postal services and sanitation � are also likely to be affected. It is right to assume that normal business activities, regardless of their nature, will suffer during a pandemic. The Officials� Committee for Domestic and External Security Co-ordination (ODESC) is chaired by the chief executive officer of the DPMC and is likely to be given the task of providing the necessary whole-of-government co-ordination. The key objective of ODESC is to minimise social disruption and the economic impact of a pandemic. Services need to be assessed regularly and support measures implemented promptly in response to most urgent need. The Ministry of Health will work with ODESC and the DPMC to minimise social and economic disruption to the greatest extent possible, but all government agencies should factor an incident such as a pandemic into their emergency planning. Care in the Community Due to the high rates of infection possible during pandemic influenza, all except the seriously ill may need to be cared for at home. Public and private hospitals will need to prioritise admissions, rationalise services and review staff rosters. DHBs will need to consider additional supplies of medication and equipment (e.g., ventilators, oxygen supplies and syringes). It may be necessary to utilise other facilities (e.g., community centres or hotels) if extra space is required, particularly for outpatients or patients post discharge. In general, emphasis should be given to out-of-hospital care and saving hospital beds for only the most severe cases. DHBs will need to liaise with local councils, their civil defence emergency management groups and voluntary groups so that they can assist in providing community care. Health professionals, such as nurses, general practitioners, paramedics, locums, health clinic staff and social service personnel, will require DHB support and co-ordination. Pharmacists will experience a rise in workload, with increased demand for medication, dispensing prescriptions and over-the-counter products. They will be closely involved in the provision of frontline advice to members of the community and in the management of adverse reactions to the usual prescribed medications. Care of Dependants During a pandemic, there are likely to be substantial numbers of people whose normal care givers are unable to provide assistance. This could include children when parents are sick, elderly , people with chronic illness or disability, and people living on their own. Modelling work undertaken by the Ministry and overlaid with population data provides scenario analysis for a pandemic event. Two situations were considered:
• children orphaned due to the death of their caregiver(s) • children left without their prime caregiver(s) due to that person or persons being hospitalised.
Both cases will result in children requiring care being present at a hospital or primary health centre. It would not require very many of these children to reduce the capacity of the institution to function to its full capacity. In the first instance, modelling (using the 35 percent infection rate) indicates that approximately 200 children nationwide would be left without their caregiver(s), or with temporary care from an alternative relative. These numbers are unlikely to stretch the capacity of the local social services, particularly when regional distribution is taken into account. Of greater short-term concern during a pandemic is the second instance, which may
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 13

involve over 800 children in 400+ family groupings. In the Auckland region alone this could mean up to 400 dependants located at hospitals after caregivers were hospitalised. To prepare for this, the social sector is an integral part of whole of government planning. However, all government departments need to be aware of the need for their intervention in such circumstances. It is equally important that DHBs consider their individual circumstances in such an eventuality and determine how they will address the problem. As part of their preparedness, it is recommended that they set up protocols with the regional offices of the relevant government agencies to ensure that arrangements to deal with such a problem can be implemented quickly. At the community level, neighbourhoods will need to prepare for the possibility that they may need to assist each other and their families when care givers become ill. Local social networks of support will be particularly important for people living on their own. Care of the Deceased The standard planning model assumes about 33,000 deaths over an 8-week pandemic wave, with a peak of around 10,000 in the peak week. For context, New Zealand averages about 550 deaths per week in normal times. Clearly normal services will be unable to manage the numbers involved, and special arrangements will be necessary for the storage, management and eventual disposal of the deceased. Normal DHB emergency planning processes include provision for managing larger than normal numbers of the deceased. Some DHB plans may need to be resized or extended to manage the planning model numbers. Processes around certification of the dead, and other issues that may need to be expedited, are being examined by an intersectoral working party.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 14
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
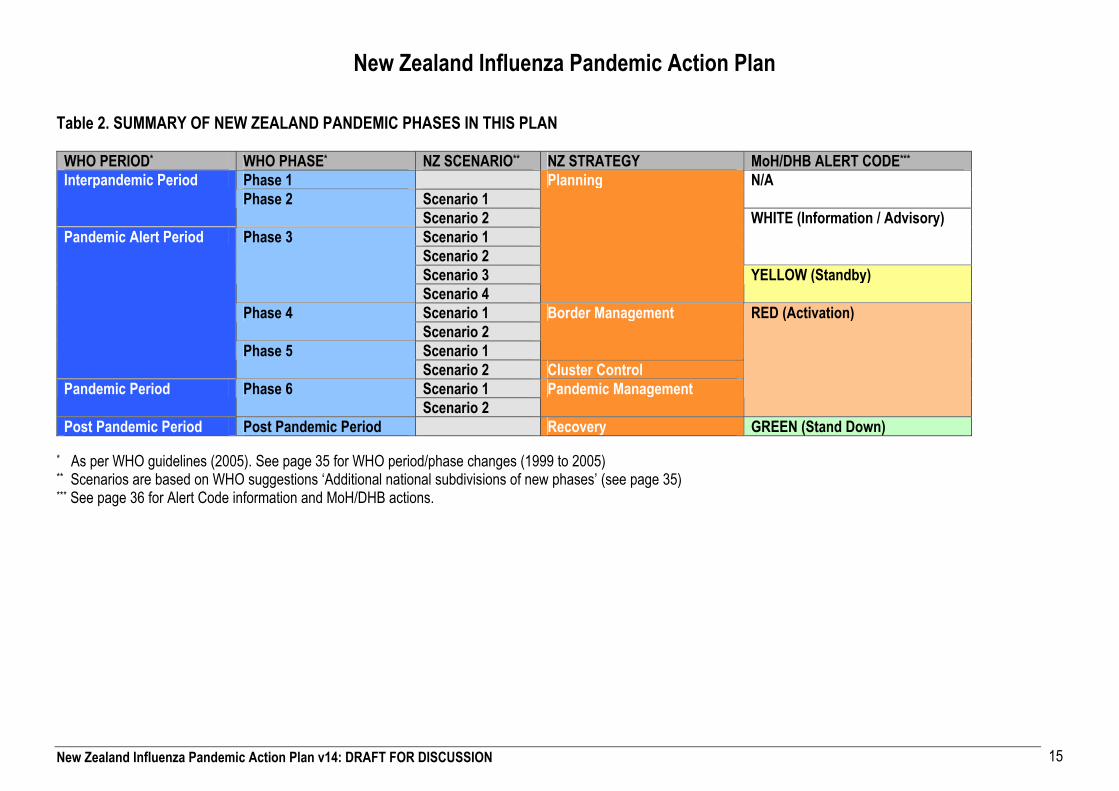
New Zealand Influenza Pandemic Action Plan Table 2. SUMMARY OF NEW ZEALAND PANDEMIC PHASES IN THIS PLAN
WHO PERIOD* WHO PHASE* NZ SCENARIO** NZ STRATEGY MoH/DHB ALERT CODE***
Phase 1 Scenario 1
N/A Interpandemic Period Phase 2
Scenario 2 Scenario 1 Scenario 2
WHITE (Information / Advisory)
Scenario 3
Phase 3
Scenario 4
Planning
YELLOW (Standby)
Scenario 1 Phase 4 Scenario 2 Scenario 1
Border Management
Pandemic Alert Period
Phase 5 Scenario 2 Cluster Control Scenario 1 Pandemic Period Phase 6 Scenario 2
Pandemic Management
RED (Activation)
Post Pandemic Period Post Pandemic Period Recovery GREEN (Stand Down)
* As per WHO guidelines (2005). See page 35 for WHO period/phase changes (1999 to 2005) ** Scenarios are based on WHO suggestions �Additional national subdivisions of new phases� (see page 35) *** See page 36 for Alert Code information and MoH/DHB actions.
15

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
INTERPANDEMIC PERIOD
Interpandemic Period Phase 1 No new influenza virus subtypes have been detected in humans. An influenza virus subtype that has caused human infection may be present in animals overseas. If present in animals, the risk of human infection or disease is considered to be low. Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Aim 1: Strengthen pandemic preparedness at national and local levels • Maintain/develop public, and other agency support • Establish/revise pandemic plans • Establish legal framework for pandemic interventions • Prepare communication plan and resources (public information, health system�s
disease assessment and management tools, information for other authorities e.g. border control)
• Ensure antiviral stockpile and rapid access to sufficient vaccine, develop plans/policies for their use
• Plan laboratory services, assessment facilities, antiviral and vaccine delivery mechanisms (including registers of individuals who have received each)
• Plan local quarantine facilities and social distancing measures • Promote uptake of interpandemic influenza vaccine
Aim 2: Plan to minimise risk of transmission to humans, rapid detection of transmission • Assess likelihood of animal / bird infection being the vector to NZ • Maintain baseline animal surveillance • Restrict importation of animals / untreated animal products from affected areas
MoH
MAF MAF MAF
No powers needed.
Monitoring and Surveillance
Ensure appropriate surveillance (national sentinel and international threats) Monitor situation offshore
MoH, MAF No powers needed.
Health Care and Emergency Response
Ensure training and preparation of health and essential services, including in particular, DHBs, PHUs, PHOs etc - DHB emergency plan, planning for assessment centres etc.
MoH No powers needed.
Communications and Health Education
Part 1: Interagency communications/consultation Ongoing liaison WHO/Australian Dept of Health and Ageing Building public awareness of influenza and potential for pandemic through routine media Reinforcing health sector awareness / preparedness Promulgating pandemic key messages ie • Be aware • Know that we are preparing for a pandemic at some time Reiterating key public health messages ie • Handwashing • Cough and sneeze etiquette Routine media monitoring
MoH No powers needed.
STRATEGY: PLANNING
16

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Part 2: Inform key stakeholders of emergence of new strain Promulgation key messages as above with added emphasis on:
• Personal protection / preparedness • Where to go for help (0800, websites, etc) • The likely impact of pandemics • What the authorities will do in the event of a pandemic • Travel advice
Review and update key messages/communications channels inc yellow pages, basic user-friendly FAQs Co-produce appropriately-endorsed information for primary care providers re
• vigilance with returning travellers • infection control
(ref Aus posters, leaflet) MoH comms co-ordinates with DHB comms (workshop, draft media / communications protocols) MoH comms co-ordinates with Whole-of-Government comms Creation Pandemic webpage with links Briefing all health journalists at national JTO training day Creation pandemic intranet for health sector use Ensure all key health sector audiences and their information needs identified. NOTE: production of this material requires specialist authorship. Comms role = co-ordination of production and distribution Finalise content for short videos on self care and care of others Initiate background briefings for all health spokespeople Investigate Family Health Diary slot for ensuing phase(s) Part 3: Preparation and production of foundation document for tailoring for/by other sectors esp.
• Agriculture • Education • Border control (incoming travellers) • MFAT (for posts, travellers) • Police, Fire, Ambulance • MCDEM • Welfare • Travel and tourism • Business/unions • Whole-of-Government • Local government
Develop media plan for ensuing phases, incl Oped, background briefings, regular updates template, talkback monitoring etc Explore culturally appropriate information/channels for Maori and Pacific audiences
17

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Explore Asian channels for communication Develop format for regular health sector updates. Format should be adaptable to increased frequency in ensuing phases Interagency communications/consultation
Ongoing liaison WHO/Australian Dept of Health and Ageing
Interpandemic Period Phase 2 � Scenario 1 International: No new influenza virus subtypes have been detected in humans. However, a circulating animal influenza virus subtype poses a substantial risk of human disease New Zealand Scenario 1: no animal or human cases in New Zealand Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Aim 1 (as above) Aim 2 (as above) plus: • Increase surveillance, in both humans and animals • Provide public advice on limiting risk of transmission from animals • Assess animal response options and finalise response policies and plans • Ensure appropriate protection and training for animal workers & exposed humans
(poultry& pigs most likely) to reflect WHO guidelines and NZ guidelines and legislation • Provide OSH guidelines
MoH / MAF MoH MAF MAF, DOL Dept Labour
No powers needed.
Communications and Health Education
Inform key stakeholders of increased risk Communications as for level 1 but intensified Extension of key messages to cement public expectation of significant changes in the event of a pandemic, e.g.
• restrictions on public gatherings • school closures • border management • greater emphasis on self-care • reduced availability of �normal� health services • prioritised use of antivirals
Implement appropriate phase of media plan incl regular media updates, constant promulgation of key messages via all media Provide user-friendly version of FAQs for talkback hosts/general media use/leafletting Initiate regular teleconferences comms managers Review and update Healthline material Develop scripts for dedicated 0800 line. RFP for provider Secure Family Health Diary slot / television awareness Finalise/produce short videos on self care and care of others. Add to web material, finalise bulk distribution/circulation Implement/update culturally appropriate information/channels for Maori and Pacific audiences Implement/update information for Asian communication channels
MoH No powers needed.
18

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Interpandemic Period Phase 2 � Scenario 2 � CODE WHITE New Zealand Scenario 2: No new influenza virus subtypes have been detected in humans. However, infected animals in NZ pose a substantial risk of human disease in NZ (this scenario may not precede human infection in NZ) NOTE* MAF is ODESC lead agency in absence of human disease* Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Aim 1 & 2 (above) plus expanded Aim 2: • Update human detection and clinical care guidelines • Develop surveillance of animal workers • Investigate rapidly any reported possible human cases • Enhance laboratory diagnostic capacity for novel strain • Target surveillance of humans in area(s) where animals affected • Increase surveillance, in both humans and animals • Implement response plans • Ensure appropriate protection and training for animal workers & exposed humans
(poultry& pigs most likely) to reflect WHO guidelines and NZ guidelines and legislation • Restrict movement of animals or any risk goods from affected areas in New Zealand
under Biosecurity Act (1993)
MoH MoH MoH, DHB MAF MAF MAF, DOL MAF
Potential application of ss 77 HA (power of MooH to enter any premises and examine persons)
Communications and Health Education
Note: infection in birds or other animals, e.g. pigs, in NZ is MAF comms response MOH comms as above but intensified. Review and update and increase frequency of communications for all health sector audiences Regular updates Whole-of-Government (led by MAF) comms to ensure appropriate key messages/material for other sectors including
• Agriculture • Education • Border control (incoming travellers) • MFAT (for posts, travellers) • Police, Fire, Ambulance • MCDEM • Welfare • Travel and tourism • Business/unions • Whole-of-Government • Local Government • Non Government Organisations (NGOs)
Introduce dedicated 0800 number with regular monitoring of calls used to refresh scripts Initiate web, talkback and all media monitoring Initiate wide distribution of short videos Secure broadcast of short videos Regular briefing of Government stakeholders for Monday radio i/vs Increase frequency of media updates Review and formalise all media and comms protocols
Initiate production of new materials for paid media advertising in next/ensuing phases. Note: move to �authority figure� presenter recommended here.
No powers required.
19

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Initiate buying plan for national media for next phase Interagency communications/consultation Ongoing liaison WHO/Australian Dept of Health and Ageing
PANDEMIC ALERT PERIOD
Pandemic Alert Period Phase 3 � Scenario 1 � CODE WHITE International: Human infection(s) with a new subtype, but no human-to-human spread, or at most rare instances of spread to a close contact. New Zealand Scenario 1: no human or animal cases in New Zealand. Functional Area Action Responsibility Authority Planning, Coordination and Reporting
As above
Monitoring and Surveillance
Increased vigilance and surveillance • Public health services work with airports of first arrival to ensure all reports of illness
on board incoming aircraft are reported to, and responded to by, public health services. Airlines informed of symptoms of particular concern, and reminded of the statutory requirement for all symptoms suggestive of infectious disease to be reported to the destination airport prior to arrival.
MoH/DHBs Aircraft: If symptoms are reported that give rise to suspicion of a quarantinable disease, plane and passengers/crew can be detained for inspection � r 22 H(Q)R, s 101 HA. MOoH can examine any person suspected of suffering from, or being exposed to in the past 6 days, a quarantinable disease (H(Q)R 24(a) and (b) If quarantinable disease is found, plane can be disinfected (r 24(c) H(Q)R). If it is found that persons on the plane have an infectious disease, or are suspected of having a quarantinable disease, they remain liable to quarantine (s 97 HA). Those with quarantinable diseases can be removed and detained (r 25 (H(Q)R) and their contacts placed under surveillance (rr 24(d), 26(3) H(Q)R). Ships: Masters of ships must seek radio pratique from a MOoH or HPO between 12 and 24 hours before expected arrival (rr 10 and 13 H(Q)R). Where the MOoH or HPO is not satisfied that the state of health is satisfactory, he or she may withhold radio pratique (r 13(3) H(Q)R).
20

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
If radio pratique is withheld, the ship may not berth and people cannot leave or board the ship without the MOoH or HPO�s authority (s 99 HA). The ship can then be inspected (s 101 HA). MOoH can examine any person suspected of suffering from, or being exposed to in the past 6 days, a quarantinable disease (H(Q)R 24(a) and (b). If quarantinable disease is found, ship can be disinfected (r 24(c) H(Q)R). If it is found that persons on the ship have an infectious disease, or are suspected of having a quarantinable disease, they remain liable to quarantine (s 97 HA) Those with quarantinable diseases can be removed and detained (r 25 (H(Q)R) and their contacts placed under surveillance (rr 24(d), 26(3) H(Q)R). Post-border: General power of MOoH to detain and isolate any person who he or she believes is likely to cause the spread of an infectious disease (s 79 HA). If authorised by the Minister or if an emergency has been declared under the CDEM Act, a MOoH can require people to submit to medical examinations (s 70(1)(e) HA) and isolate or quarantine them as he or she sees fit (s 70(1)(f) HA)
DHBs review plans for managing a pandemic DHBs No power needed. DHBs review plans for rapid immunisation campaign (once vaccine available) DHBs No power needed.
Health Care and Emergency Response
Quarantine planned for � travellers, plane crews, shipping crews etc See above under Monitoring and Surveillance.
21

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
As above but intensified Secure media buy/finalise production for high-frequency, radio-loaded campaign Ongoing review/extension of key messages to reflect changes Accelerate production of media materials Intensified media monitoring Set up 0800 no for health professionals Ongoing review of materials for health sector � e.g. infection control in primary care setting, assessment protocols, contact tracing and isolation, case definitions etc Ongoing review of materials for Maori/Pacific/Asian audiences
MoH No power needed.
Ongoing review of materials for specialist sector audiences: • Agriculture • Education • Border control (incoming travellers) • MFAT (for posts, travellers) • Police, Fire, Ambulance • MCDEM • Welfare • Travel and tourism • Business/unions • Primary healthcare • Older people • Disabled people
Communications and Health Education
Introduce new materials for people facing public • Transport operators • Retail industry • Hospitality industry
Increase frequency of media updates. Move from formatted bulletin to regular media conference
Pandemic Alert Period Phase 3 � Scenario 2 � CODE WHITE International: Human infection(s) with a new subtype, but no human-to-human spread, or at most rare instances of spread to a close contact. New Zealand Scenario 2: First case identified in NZ animal; No evidence of consistent human to human transmission (as above) Functional Area Action Responsibility Authority Planning, Coordination and Reporting
• Increase surveillance in animals within & outside affected areas • Implement response • Ensure appropriate protection and training for animal workers & exposed humans
(poultry& pigs most likely) to reflect WHO guidelines and NZ guidelines and legislation • Restrict movement transport of animals or any risk goods from affected areas in New
Zealand under Biosecurity Act (1993)
MAF MAF, DOL
Monitoring and Surveillance
• Target surveillance of humans in area(s) where animals affected • Monitor situation off shore
MoH MoH
22

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Pandemic Alert Period Phase 3 � Scenario 3 � CODE YELLOW International: Human infection(s) with a new subtype, but no human-to-human spread, or at most rare instances of spread to a close contact. New Zealand Scenario 3: First human case in NZ (confirmed by lab test) from identification at border (within 12-48hrs swab taken). No evidence of consistent human to human transmission (as above) No animal cases in NZ. Functional Area Action Responsibility Authority Planning, Coordination and Reporting
CIMS structure activated Code Yellow nationally, possible Code Red regionally
MoH
Increased vigilance in surveillance National and international reporting
Notification requirements (to MOoH): ss 74 (doctors), 75 (occupiers of premises), 76 (masters of ships), 85 (funeral directors) HA. Pilots � r 3 of the H(Q)R
Ensure labs have sufficient viral test primer (and clarify supply constraints) No powers required. Advise WHO of first case identified in New Zealand MoH
Monitoring and Surveillance
Target surveillance of animals in area(s) where humans affected MAF Health Care and Emergency Response
Isolate case(s) for 48 hrs and treat (Tamiflu). Contact tracing to provide advice.
All aircraft reporting a person sick on board, passengers assessed, advised and released (in absence of H2H transmission)
See above in Phase 3, Scenario 1, Monitoring and Surveillance.
National and international agencies notified. MoH Communications and Health Education
Implement multi-media campaign fronted by trusted authority figure covering self care/caring for others/staying safe/limiting spread/possible closures mass gathering centres/where to go for help/community resources such as home-help, shopping help etc for a wide range of audiences. NOTE possible introduction of video-streaming here media conferences/hand hygiene demos etc Regular media conferences (daily) to support regular media updates Review and update foundation documents with special reference to border control/tourism and travel sectors Produce health leaflet for incoming travellers
MoH
Pandemic Alert Period Phase 3 � Scenario 4 � CODE YELLOW International: Human infection(s) with a new subtype, but no human-to-human spread, or at most rare instances of spread to a close contact. New Zealand Scenario 4: First human case in NZ; (confirmed by lab test) from community surveillance (within 1-2 weeks of swab taken) No evidence of consistent human to human transmission (as above) No animal cases in NZ. Functional Area Action Responsibility Authority Planning, Coordination and Reporting
CIMS structure activated Code Yellow nationally, possible Code Red regionally
MoH
Advise WHO of first case identified in New Zealand MoH No power required. Monitoring and Surveillance Target surveillance of animals in area(s) where humans affected MAF Public Health Interventions
Dependent upon Case history • If travelled o/s recently (within 8 days) increase monitoring and surveillance at the
border
Prescribed form under s 132 Immigration Act.
23

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
• Identify exposure to birds/wildlife sources of infection • If not travelled within 8 days AND no animal/bird exposure assume human to human
transmission. Contact tracing to provide advice As above.
Pandemic Alert Period Phase 4 � Scenario 1 � CODE RED International: Human to human transmission; Small cluster(s) with limited human-to-human transmission but spread is highly localised, suggested that the virus is not well adapted to humans. No animal cases in NZ. New Zealand Scenario 1: Cluster(s) occurring offshore Functional Area Action Responsibility
Code Red; MoH CIMS; Full activation of National Health Coordination Centre MoH - DoPH Order pandemic vaccine following pandemic declaration by WHO MoH Release ready use antivirals to local MOoH for PEP or other use as appropriate MoH
Planning, Coordination and Reporting
Prepare for release of national reserve volumes � pre-position supplies in affected area MoH Introduce enhanced staff surveillance and sickness reporting � follow up any ILI Review recent surveillance of ILI
DHB hospital, ambulance services, GP practices, border group organisations
Monitoring and Surveillance
Monitor offshore situation MoH, MAF Border management !!KKEEYY DDEECCIISSIIOONN"" Border groupHold all pax and aircrew incoming by air from affected regions until full scan for match with case definition completed !!KKEEYY DDEECCIISSIIOONN""
Border group s 70-73 HA In addition: Aircraft from outside NZ or affected area inside NZ liable to quarantine (s 96 HA No power to detain aircraft after inspection unless quarantinable disease is suspected (ie refuse pratique). If special powers activated, can hold persons (but probably not aircraft) under HA s 70(1)(f), prevent their access under s 70(1)(g) HA, or prevent their leaving under s 70(1)(h) HA. Police can enforce quarantine under s 112 HA.
Issue travel advisories for affected areas MoH
Public Health Interventions
Scan incoming pax and aircrew for match with case definition PHU s 79 HA � general power of detention. If authorised by the Minister or if an emergency has been declared under the CDEM Act, s 70(1)(e) HA � power to require medical examinations.
STRATEGY: BORDER MANAGEMENT
24

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Match found � swab for PCR PHU s 79 HA � general power of detention. If authorised by the Minister or if an emergency has been declared under the CDEM Act, s 70(1)(e) HA � power to require medical examinations.
Match found � hold all pax and aircrew until PCR result (at least 12 hours) !!KKEEYY DDEECCIISSIIOONN""
Border group s 79 HA � general power of detention. If authorised by the Minister or if an emergency has been declared under the CDEM Act, s 70(1)(e) HA � power to require medical examinations.
No match found � release passengers and aircrew PHU PCR positive � provide PEP for close contacts, release asymptomatic people with health advice
PHU
PCR positive � transport case/s to local hospital Ambulance service If authorised by the Minister or if an emergency has been declared under the CDEM Act, MOoH can order people isolated under s 70(f) HA
Health Care and Emergency Response
PCR negative � isolate person/s, treat as appropriate Local DHB hospital If authorised by the Minister or if an emergency has been declared under the CDEM Act, s 70(1)(f) HA. NZBORA issues with enforcing compulsory treatment.
Communications and Health Education
Reiteration of all above (Phase 3) plus • Introduce or intensify text messaging campaign • Review and promulgation new key messages reflecting health action e.g. on vaccines,
community assessment centres/isolation centres etc • Review and increase frequency of media conference updates (1 or 2x daily) Ongoing review/updating of all comms in conjunction with all key agencies Review and update foundation documents with special reference to border control/tourism and travel sectors
Interagency communications/consultation Ongoing liaison WHO/Australian Dept of Health and Ageing Ongoing review communications strategy, incorporating material all feedback loops incl.
• Talkback monitoring • All media monitoring • Call centre reports • Web monitoring • Sector intelligence • Other agency intelligence
Ongoing evaluation/freshening paid media campaign(s)
MoH No powers required.
25

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Pandemic Alert Period Phase 4 � Scenario 2 � CODE RED International: Human to human transmission; Small cluster(s) with limited human-to-human transmission but spread is highly localised, suggested that the virus is not well adapted to humans. New Zealand Scenario 2: Single case or small cluster in NZ not related to birds or travel (will probably be picked up by routine surveillance by GP or virology of hospitalised patients). No animal cases in NZ. Functional Area Action Responsibility Authority
Code Red; MoH CIMS; Full activation of National Health Coordination Centre MoH � DoPH Release ready use antivirals to local MOoH for post-exposure prophylaxis (PEP) or other use as appropriate
MoH
Prepare for release of national reserve volumes � pre-position supplies in affected area MoH Inform WHO MoH No powers required.
Planning, Coordination and Reporting
Order pandemic vaccine MoH No powers required. Review recent surveillance of ILI ESR No powers required. Monitoring and
Surveillance Target surveillance of animals in area(s) where human affected MAF Border management !!KKEEYY DDEECCIISSIIOONN"" Border group As above, Phase 4, scenario 2, Public
Health Interventions Contact tracing and review, with antivirals for those exposed PHU As above, Phase 4, scenario 2, Public
Health Interventions Closure of educational facilities !!KKEEYY DDEECCIISSIIOONN"" Education If authorised by the Minister or if an
emergency has been declared under the CDEM Act, publish a notice in the newspaper preventing children under 16 from attending schools (s 70(1)(o) HA). No specific power to stop 16+ pupils from attending.
Public Health Interventions
Restriction of regional public gatherings !!KKEEYY DDEECCIISSIIOONN"" Local MOoH If authorised by the Minister or if an emergency has been declared under the CDEM Act, ss 70(1)(m) and (n) HA.
Isolate patient (if not already isolated) DHB hospital s 79, and, If authorised by the Minister or if an emergency has been declared under the CDEM Act, s (70(1)(f) HA.
Track all staff contacts and review health status GP practices, hospitals Examination under s 79 and, if regs amended rr 10 and 11 of the H(IND)Rs.
Activate community assessment centres for active case finding DHB If authorised by the Minister or if an emergency has been declared under the CDEM Act, MOoH can use or authorise a local authority to use any reserve or endowment as a hospital or place of isolation (s 70(1)(l) HA).
Health Care and Emergency Response
Activate workforce contingency plans if impacted by school closures or other issues DHB hospitals, GP practices
26

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Consider possible pre-school, school, tertiary education closures, also cinemas, sporting and cultural events, restaurants, churches. !!KKEEYY DDEECCIISSIIOONN""
MoH, MoE If authorised by the Minister or if an emergency has been declared under the CDEM Act, ss 70(1)(m)-(o) HA.
Communications and Health Education
Reiterate media protocols with DHB comms, ensuring clear understanding of comms re local cases.
Pandemic Alert Period Phase 5 � Scenario 1 � CODE RED International: Human to human transmission; Larger cluster(s) but human-to-human spread is still localised, suggested that the virus is becoming increasingly better adapted to humans, but may not yet be fully transmissible (substantial pandemic risk). New Zealand Scenario 1: Clusters of cases offshore Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Code Red; MoH CIMS Full activation of National Health Coordination Centre
MoH � DoPH
Monitoring and Surveillance
Monitor offshore situation MoH, MAF
Public Health Interventions
Intensified border management and control areas !!KKEEYY DDEECCIISSIIOONN"" • Quarantine incoming passengers from aircraft on the way to New Zealand when
the border is closed
Customs All overseas aircraft liable to quarantine (s 96 HA), but no power to refuse pratique in this blanket manner (s 107 HA). However, a craft coming from a known infected area could give rise to a reasonable suspicion of illness, which would trigger many of the quarantine powers discussed below: Aircraft: Standing requirement under H(Q)R, r 3. Aircraft captains must report symptoms to airline, and airline must report such symptoms to MOoH or HPO. If symptoms are reported that give rise to suspicion of a quarantinable disease, plane and passengers/crew can be detained for inspection � r 22 H(Q)R, s 101 HA. MOoH can examine any person suspected of suffering from, or being exposed to in the past 6 days, a quarantinable disease (H(Q)R 24(a) and (b). If quarantinable disease is found, plane can be disinfected (r 24(c) H(Q)R). If it is found that persons on the plane have an infectious disease, or are suspected of
27

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
having a quarantinable disease, they remain liable to quarantine (s 97 HA) . Those with quarantinable diseases can be removed and detained (r 25 (H(Q)R) and their contacts placed under surveillance (rr 24(d), 26(3) H(Q)R). Ships: Masters of ships must seek radio pratique from a MOoH or HPO between 12 and 24 hours before expected arrival (rr 10 and 13 H(Q)R). Where the MOoH or HPO is not satisfied that the state of health is satisfactory, he or she may withhold radio pratique (r 13(3) H(Q)R). If radio pratique is withheld, the ship may not berth and people cannot leave or board the ship without the MOoH or HPO�s authority (s 99 HA). The ship can then be inspected (s 101 HA). MOoH can examine any person suspected of suffering from, or being exposed to in the past 6 days, a quarantinable disease (H(Q)R 24(a) and (b). If quarantinable disease is found, ship can be disinfected (r 24(c) H(Q)R). If it is found that persons on the ship have an infectious disease, or are suspected of having a quarantinable disease, they remain liable to quarantine (s 97 HA). Those with quarantinable diseases can be removed and detained (r 25 (H(Q)R) and their contacts placed under surveillance (rr 24(d), 26(3) H(Q)R).
Communications and Health Education
As per Phase 4. Ongoing review communications strategy, incorporating material all feedback loops incl
• Talkback monitoring • All media monitoring • Call centre reports • Web monitoring • Sector intelligence
MoH
28

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
• Other agency intelligence Ongoing evaluation/freshening paid media campaign(s) Interagency communications/consultation Ongoing liaison WHO/Australian Dept of Health and Ageing (especially regarding border management)
Pandemic Alert Period Phase 5 � Scenario 2 � CODE RED International: Human to human transmission; Larger cluster(s) but human-to-human spread is still localised, suggested that the virus is becoming increasingly better adapted to humans, but may not yet be fully transmissible (substantial pandemic risk). No animal cases in NZ. New Zealand Scenario 2: Clusters of cases onshore Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Code Red; MoH CIMS Full activation of National Health Coordination Centre
MoH � DoPH
Monitoring and Surveillance
Monitor situation offshore Target surveillance of animals in area(s) where human affected
MoH, MAF MAF
Declare public health emergency (authorise use of special powers, 70-73, Health Act); possible declaration of local or national emergency under the CDEM Act 2002 !!KKEEYY DDEECCIISSIIOONN""
MoH, MCDEM ss 70-73 HA, ss 66-69 CDEM Act
Border management and control measures • Quarantine incoming passengers from aircraft on the way to New Zealand when
the border is closed !!KKEEYY DDEECCIISSIIOONN""
Customs
Isolate NZ area affected if possible !!KKEEYY DDEECCIISSIIOONN"" Police/DefenceIssue ``Don�t Travel�� warnings MoH Closure of educational facilities !!KKEEYY DDEECCIISSIIOONN"" MoH/Education As above, Phase 4, scenario 2, Public
Health Interventions Restriction of public gatherings !!KKEEYY DDEECCIISSIIOONN"" MoH As above, Phase 4, scenario 2, Public
Health Interventions Encourage tele-work practices DOL? Prioritise work activities ALL Protect unaffected island(s) MoH/Police/Defence If authorised by the Minister or if an
emergency has been declared under the CDEM Act, s 70(1)(g) HA � forbid people or things from an infected place coming to the health district; If authorised by the Minister or if an emergency has been declared under the CDEM Act, s 70(1)(h) HA � forbid people from leaving a health district or a place within it. Consider detaining people attempting to leave/enter under s 79 HA.
Public Health Interventions
Immunise priority populations first DHBs Health Care and Role shifts (triggered ≥ 15 percent attack rate or doubling of death rate)
STRATEGY: CLUSTER CONTROL
29

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Activate additional mortuary facilities (AMFs) ss 84 and 86 HA Surveillance of unaffected areas Inspectors under the H(IND)R, r 7. Monitor prevalence of ILI � CATI (computer assisted telephone interviews) Increase treatment focus of Community Based Assessment Centres DHBs By agreement, or, if authorised by the
Minister or if an emergency has been declared under the CDEM Act, using MOoH powers under s 71HA.
Emergency Response
Activate security measures for treatment centres Police/Defence Communications and Health Education
As per Phase 5 MoH/Whole-of-Government
PANDEMIC PERIOD
STRATEGY: PANDEMIC MANAGEMENT
Pandemic Period Phase 6 � Scenario 1 � CODE RED International and New Zealand: Increased and substantial transmission in the general population. No animal cases in NZ. Functional Area Action Responsibility Authority Planning, coordination and Reporting
Code Red, MoH CIMS Full activation of National Health Coordination Centre
MoH � DoPH
Monitoring and Surveillance
Monitor mortality data Computer Assisted Telephone Interviews Target surveillance of animals in area(s) where humans affected
MoH MAF
Public Health Interventions
Public Heath Emergency (as above) Community support intensified
MoH
Health Care and Emergency Response
Community based treatment centres for priority groups for antiviral treatment • computer based adverse event monitoring
Commence vaccination programme if vaccine available (most people will want vaccination)
• computer based adverse event monitoring DHB activate mass casualty plans
DHBs / MoH
Communications and Health Education
Ongoing review communications strategy, with special reference to audiences and key messages, incorporating material all feedback loops including:
• Talkback monitoring • All media monitoring • Call centre reports • Web monitoring • Sector intelligence • Other agency intelligence
Ongoing evaluation/freshening paid media campaign(s) Interagency communications/consultation Ongoing liaison WHO/Australian Dept of Health and Ageing on all issues
Whole-of-Government Comms
No powers required.
30

New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
Pandemic Period Phase 6 � Scenario 2 � CODE RED International and New Zealand: Wave decreasing; Detection of next wave. No animal cases in NZ. Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Code Red, MoH CIMS Full activation of National Health Coordination Centre
MoH � DoPH
Monitoring and Surveillance
Computer Assisted Telephone Interviews indicate decrease in infection rate Increase laboratory surveillance Continue resistance monitoring Activate ILI syndromic surveillance Epidemiological data analysed
• mortality rate • infection rate • adverse events from
# antiviral medication # vaccination
Target surveillance of animals in area(s) where humans affected
MoH MAF
Public Health Emergency continues !!KKEEYY DDEECCIISSIIOONN"" Educational institutions and childcare reopen !!KKEEYY DDEECCIISSIIOONN"" Travel restriction lifted !!KKEEYY DDEECCIISSIIOONN""
Public Health Interventions
Restriction on public gatherings lifted !!KKEEYY DDEECCIISSIIOONN"" Communications and Health Education
As above. Ongoing review communications strategy, with special reference to audiences and key messages, incorporating material all feedback loops incl.
• Talkback monitoring • All media monitoring • Call centre reports • Web monitoring • Sector intelligence • Other agency intelligence
Ongoing evaluation/freshening paid media campaign(s) Initiate production new �back-to-normal� campaign with ref to post-trauma knowledge/best practice
Ongoing consultation all key agencies Ongoing liaison WHO/Australian Dept of Health and Ageing
31
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION
POST PANDEMIC PERIOD
Post Pandemic Period � CODE GREEN Pandemic Over Functional Area Action Responsibility Authority Planning, Coordination and Reporting
Recovery Debriefing Lessons learned
ALL
Health Care and Emergency Response
Recovery Debriefing Lessons learned
ALL
Communications and Health Education
As above. Ongoing review communications strategy, with special reference to audiences and key messages, incorporating material all feedback loops incl
• Talkback monitoring • All media monitoring • Call centre reports • Web monitoring • Sector intelligence • Other agency intelligence
Terminate pandemic media campaign(s) Initiate �back to normal� campaign Ongoing consultation all key agencies
STRATEGY: RECOVERY
32

Appendix A: Intersectoral Pandemic Group (IPG) � Summary of Work Programmes
Workgroup Lead Agency Work Programme Key Linkages Border NZ Customs Preparing border management responses to a range of pandemic
scenarios, including: • impact of border management � trade and travel implications • changes to existing legislation to allow for necessary level of
border management • when, how and level of border management (air and sea
borders) • screening of incoming passengers and vessels • quarantine of arriving passengers (quarantine period, who is
quarantined, where quarantine takes place)
Health Law & Order & ES Workplaces Economy Communication
Education MoE • Drafting plans for schools, early childhood education services, tertiary education organisations, MoE
• communications plan being developed • MoE working with the Education Review Office, NZQA, the
Tertiary Education Commission, the NZ Teachers� Council, Career Services
Health Workplaces Communication
External MFAT • MFAT is developing a specific pandemic plan template for overseas posts
• A plan is being developed for the Wellington-based activities of any consular response related to a pandemic.
• MFAT is developing an internal communications strategy • Planning for appropriate support and response to Pacific Island
countries, including preparing a Response Action Plan for the Pacific
Health Border Welfare
Law & Order & Emergency Services
NZ Police • Determining national and regional law and order response • Identifying where Health and Police will require support • Police national and district emergency plans being updated • NZ Fire Service developing internal and external contingency
plans • Department of Corrections� internal and external planning
continuing • NZDF working with other agencies to clarify its roles in
interpandemic and pandemic phases • Ministry of Justice continuing its continuity planning
Health Workplaces Community & Logistics Border Communication
Welfare MSD • MSD working to strengthen pandemic preparedness within o MSD o Children Young Persons and their Families o Ministry of Agriculture o Inland Revenue Department o Housing New Zealand o Te Puni Kokiri o Ministry of Foreign Affairs and Trade
• MSD working to strengthen pandemic preparedness within the welfare sector (engaging with Welfare Agency Groups)
• MSD strengthening preparedness at the local and regional level (identifying issues, working with regional groups to advise them of national decisions and expectations etc.)
• Welfare planning at the national level • MSD business continuity planning and internal capability
Health Community & Logistics Workplaces Border
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 33

Workgroup Lead Agency Work Programme Key Linkages Community & Logistics
MCDEM • Strengthening CDEM Group planning � identification of key issues and planning requirements
• Determining the role of CDEM Groups in a Health-led emergency
• Securing and maintaining the food supply • Liaison with the Fast Moving Consumer Goods (FMCG) sector • Ministry of Civil Defence & Emergency Management
contingency planning and internal capability • Liaison and joint communications with Health, Infrastructure,
Welfare and Law & Order & ES workgroups.
Health Infrastructure Welfare Law & Order & ES
Economy Treasury • Contingency planning to keep the Government financial system running
• Ensuring financial stability (Reserve Bank and MED) • The Treasury and the Reserve Bank working on ensuring the
robustness of monetary and fiscal policy frameworks • Ongoing work to assist firms to prepare for a pandemic
(disruptions to supply, staffing issues, IRD matters, etc.)
Health Infrastructure Law & Order & ES Workplaces Border Community & Logistics
Infrastructure MED • MED has published a Business Continuity Planning Guide and a Pandemic Planning Information Kit for businesses (14 October 2005; approved by MoH)
• MED working with infrastructure sector � energy, communications, transport, and water and waste, on communications and business continuity planning
• Liaison with regional Lifelines Groups
Health Community & Logistics Workplaces Welfare
Workplaces DoL • DoL�s planning work has close linkages to public health, businesses, communities, welfare provision
• Vast majority of firms employ less than 20 staff and are outside health sector and / or infrastructure planning
• DoL�s role to provide o general information to workplaces about a pandemic o industry specific guidance o employment relations guidance o operating polices for health and safety inspectorate.
• Liaison with key stakeholders o professional groups o unions o representative groups
• DoL developing a Business Continuity Plan for the Workforce workstream
Health Communication Economy Infrastructure
Coordination DPMC Whole of government issues, e.g.: • Strategy • Communications • Public service continuity issues � SSC • PPE
ALL
Communication MoH / DPMC Whole of government communications strategy and planning ALL
Legislation DPMC / CLO / MoH
• Gaps analysis of powers to act • Proposing legislative and regulatory amendments to ensure
that the Crown has powers available to it in the event of a pandemic, and that a proper response can be made.
ALL
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 34

Appendix B: Comparison of Phases published by WHO in 1999 and 2005
PHASES AS PUBLISHED BY WHO IN 1999
NEW WHO PANDEMIC PHASES (2005) ADDITIONAL NATIONAL SUBDIVISIONS OF NEW PHASES (NZ SCENARIOS)
Interpandemic Period Phase 1. No new influenza virus subtypes have been detected in humans. An influenza virus subtype that has caused human infection may be present in animals. If present in animals, the risk a of human infection or disease is considered to be low
Not affected � NZ Scenario 1
Interpandemic Period Phase 0
Phase 2. No new influenza virus subtypes have been detected in humans. However, a circulating animal influenza virus subtype poses a substantial risk a of human disease
Affected or extensive travel/trade links with affected country � NZ Scenario 2 Not affected � NZ Scenario 1 � NZ Scenario 2 � NZ Scenario 3
Pandemic Alert Period Phase 0. Preparedness level 1: human case.
Pandemic Alert Period Phase 3. Human infection(s) with a new sybtype, but no human-to-human spread, or at most rare instances of spread to a close contact.
Affected or extensive travel/trade links with affected country � NZ Scenario 4 Not affected � NZ Scenario 1
Phase 0. Preparedness level 2: limited human transmission.
Phase 4. Small cluster(s) with limited human-to-human transmission but spread is highly localised, suggesting that the virus is not well adapted to humans.
Affected or extensive travel/trade links with affected country � NZ Scenario 2 Not affected � NZ Scenario 1
Phase 0. Preparedness level 3: spread in general population.
Phase 5. Larger cluster(s) but human-to-human spread is still localised, suggesting that the virus is becoming increasingly better adapted to humans, but may not yet be fully transmissible (substantial pandemic risk). b
Affected or extensive travel/trade links with affected country � NZ Scenario 2
Pandemic Period Phase 1. Multiple countries.
Not yet affected
Phase 2. Multiple regions. Affected or extensive travel/trade links with affected country � NZ Scenario 1
Phase 3. Subsiding in initially affected countries but not in other countries.
Subsided � NZ Scenario 2
Phase 4. Next wave.
Pandemic Period Phase 6. Pandemic phase: increased and sustained transmission in general population b.
Next wave Postpandemic Period Phase 5. Return to Phase 0.
Postpandemic Period Return to Interpandemic Period
Return to Interpandemic Period
a The distinction between phase 1 and phase 2 is based on the risk of human infection or disease resulting from circulating strains in animals. The distinction would be based on various factors and their relative importance according to current scientific knowledge. Factors may include: pathogenicity in animals and humans; occurrence in domesticated animals and livestock or only in wildlife; whether the virus is enzootic or epizootic, geographically localized or widespread; other information from the viral genome; and/or other scientific information. b The distinction between phase 3, phase 4 and phase 5 is based on an assessment of the risk of a pandemic. Various factors and their relative importance according to current scientific knowledge may be considered. Factors may include: rate of transmission; geographical location and spread; severity of illness; presence of genes from human strains (if derived from an animal strain); other information from the viral genome; and/or other scientific information.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 35

Appendix C: Alert Code Communications � Ministry of Health and DHB Actions
Alert Code Ministry Actions DHB Actions
White Information / Advisory Only
• Advise CEOs of all 21 DHBs; 21 DHB �single
points of contact�; and Public Health Managers of emerging situation and potential developments
• Provide media and public information and advice
• Provide case definitions and other clinical and public health advice on control, where possible
• Advise all relevant staff, services and
service providers • Notify clinical and public health staff of case
definitions, clinical advice, and control measures
• Review clinical emergency plans
Yellow Standby
• Activate Ministry CIMS structure • Identify National Co-ordinator and National
Co-ordination Team members • Identify and activate national Technical
Advisory Group • Contact all 21 DHBs, via DHB single points
of contact and advise of situation and national emergency control contact number(s)
• Manage liaison and communications with other government agencies
• Prepare to activate DHB CIMS structure • Prepare to activate Regional Co-ordination
Teams • Advise and prepare all staff, services and
service providers • Manage own DHB clinical response and
public health response if impacted by emergency
Red Activation
• Inform all DHBs, via single points of contact • Direct activation of the four Regional Co-
ordination Teams • Coordinate response at national level
through the four Regional Co-ordination Teams
• Activate DHB CIMS structure • Activate Regional Co-ordination Teams • Advise of regional emergency control
contact number(s) • Manage own DHB response, as required
under regional co-ordination arrangements.
Green Stand down
• Moving from red to green � inform all
Regional Co-ordinators • Moving from yellow to green � inform all
DHB single points of contact • Advise media and public • Deactivate Ministry CIMS structure • Resume normal functions Post stand down: Design and implement evaluation and review of emergency response.
• Deactivate Regional Co-ordination Teams
(where activated) • Deactivate DHB CIMS structure • Resume normal functions Post stand down: Participate in the Ministry-led review of emergency response.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 36

Appendix D: Interim Guidelines for Personal Protective Equipment
Purpose of this document These interim guidelines for personal protection have been developed as part of the national health emergency planning for a potential influenza pandemic. The recommended personal protective equipment (PPE) and general infection prevention and control measures apply to health care workers and first responders such as ambulance, police, fire and other frontline services. The general infection prevention and control measures also apply to the general public. Concern for personal protection is greater during a pandemic influenza as it is caused by a virus that is markedly different from recently circulating strains such as found in a seasonal influenza, which is a familiar infection, especially during winter. A pandemic influenza causes illness in a large number of the people infected; it spreads widely and quickly because the population will have no immunity. How is pandemic influenza transmitted? Primarily, human influenza is transmitted from person to person via virus-laden large droplets (particles >5 µm in diameter), which are generated when an infected person coughs or sneezes. These large droplets can then be directly deposited onto the mucosal surfaces of the upper respiratory tract of susceptible people who are near the infected person (i.e., within 1 metre). Transmission may also occur through direct contact with infectious (wet) respiratory secretions, such as by touching door handles, taps, lift buttons, stairwell railings, keyboards, etc that have deposits of the infected secretions on their surfaces, and then hand-to-face contact. Health care workers Health care workers are at a greater risk of pandemic influenza than the general public because they will often be caring for infected people who might be hospitalized or seeking primary health care services. To support the protection of health care workers in their workplace in the event of a pandemic influenza, and to ensure that there is a supply of PPE in DHBs beyond that required for everyday use, Cabinet approved funding in February 2005 for DHBs to buy PPE for health care workers and support staff in the secondary/tertiary and primary health care sector. First responders It is important to provide PPE to �first responders�, and to educate and train them in appropriate PPE use, as well as ensuring they know how to use general infection prevention and control strategies. First responders include ambulance, police and fire staff, as well as other workers responding to emergencies as part of their work and coming into close contact with cases of pandemic influenza. The public The Ministry of Health recommends the general public follow the appropriate general infection prevention and control measures described below to decrease influenza transmission. General and specific infection prevention and control measures Organisations of all kinds should have effective policies and processes in place to ensure people with
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 37

symptoms of respiratory disease do not place others at risk of infection. For workplaces, such policies can include sending ill people home and enabling staff to work in more isolated settings, such as from home, during times of influenza outbreak. There is scientific and medical evidence that influenza can spread in inadequately ventilated internal spaces. All internal spaces should be well ventilated, preferably with fresh air, by opening windows, or with properly designed and maintained air-conditioning systems. See www.moh.govt.nz/pandemicinfluenza for specific Ministry of Health advice on air conditioning and influenza. Hand hygiene Hand washing is still the single most important measure to reduce the risks of transmitting infectious organisms from one person to another. Hands should be washed regularly with soap and water, an alcohol-based hand rub or an antiseptic hand wash and then thoroughly dried, preferably using disposable tissues or towels. Hands should always be washed and dried after contact with respiratory secretions or after touching surfaces that have been contaminated with respiratory secretions. Health care workers dealing with respiratory secretions should be wearing gloves as per the Standard Precautions. See Standard Precautions: www.cdc.gov/ncidod/hip/ISOLAT/std_prec_excerpt.htm Hand-to-face contact, which occurs during such activities as eating, normal grooming or smoking, presents significant risks because of the potential for transmitting influenza from surfaces contaminated with respiratory secretions, and for this reason, hands should always be washed and dried before any activity that involves hand-to-face contact. Respiratory hygiene/cough etiquette People with respiratory infection symptoms should practise the following cough/sneeze etiquette whenever they are in the presence of another person. All symptomatic people should: • avoid close contact (less than 1 metre) with other people • cover their nose and mouth when coughing or sneezing • use disposable tissues to contain respiratory secretions • immediately dispose of used tissues in the nearest waste receptacle • immediately wash and dry their hands. Social distancing Crowded places and large gatherings of people should be avoided at times of an influenza pandemic, whether such gatherings are in internal or external spaces. A distance of at least 1 metre should be maintained between persons wherever possible. Greater distances are more effective. Any form of contact with people who are unwell with pandemic influenza, including visiting, should be avoided wherever practicable.
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 38

Protective barriers Protective barriers in the form of perspex or glass may provide useful protection for people such as front-counter staff, supermarket operators or public transport drivers, whose duties require them to have frequent face-to-face contact with members of the public where social distancing is either not possible or not practical. Using masks People with respiratory infection symptoms should consider using a disposable surgical mask to help prevent exposing others to their respiratory secretions. Any mask must be disposed of as soon as it becomes moist or after any cough or sneeze, in an appropriate waste receptacle, and hands must be thoroughly washed and dried after the used mask has been discarded. Patients with respiratory infection symptoms in health care institutions should be masked to contain respiratory secretions at any time they present a potential risk to unprotected people. Recommendations for PPE use Personal protection equipment (PPE) includes masks, goggles, eye/face shields, gloves, gowns and aprons. Varying levels and types of PPE are required, depending on the level of exposure and the risk of transmission. Whatever the level of PPE to be used, education and training is necessary to ensure the equipment is used and disposed of correctly, to maintain the equipment�s effectiveness. Using disposable surgical masks, gloves and gowns/aprons Disposable surgical masks are recommended for first responders and health care/support workers in a health care setting who are at risk from droplet transmission. Disposable gloves are recommended as a means of reducing the likelihood of influenza transmission when handling objects contaminated with respiratory secretions. Apart from health care settings, the use of gloves is less important than careful hand washing. The use of gloves does not replace the need for hand washing. Disposable gowns or splash resistant aprons may also reduce opportunities for transmitting influenza. However, it may not always be practical to use gowns/aprons outside the health care setting. Gloves and gowns/aprons (full PPE) Health care workers should wear particulate respirator masks, eye protection, gloves and gowns/aprons (i.e. full PPE) when there is a high risk of direct contact with respiratory secretions, particularly via aerosols. This will apply mostly in inpatient settings during some invasive procedures. In most other settings a disposable surgical mask (with or without eye protection and disposable gloves) will provide sufficient protection from droplet transmission for health care workers in close contact and/or providing direct personal care to patients with pandemic influenza. Using these measures helps comply with the Health and Safety in Employment Act 1992 The Health and Safety in Employment Act 1992 requires the following measures to be taken.
�Section 6: All practicable steps
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 39

Every employer shall take all practicable steps to ensure the safety of employees while at work; and in particular shall take all practicable steps to: • provide and maintain for employees a safe working environment • provide and maintain for employees while they are at work facilities for their safety and health ... Section 28: Employees may refuse to perform work likely to cause serious harm • An employee may refuse to do work if the employee believes that the work that the employee is
required to perform is likely to cause serious harm to him or her ....� Employers must take all practicable steps to mitigate the risk and protect employees, especially those at high risk, such as health care personnel, support staff and first responders (fire/police/ambulance/other emergency workers) from pandemic influenza. These workers should be educated in hand hygiene, cough etiquette, social distancing and the use of appropriate PPE and should be provided with the supplies required to carry out these techniques. Employers need to actively plan to cover their risks and the risks to their workers and the public. The above measures should assist employers with compliance. TABLE 1: SUMMARY OF PROTECTION MEASURES Protection measure Where applicable
Hand hygiene, cough etiquette, ventilation Everyone, all the time
Organisational policies Every organisation, all the time
Social distancing Everyone, whenever practical
Protective barriers In situations where regular work practice requires unavoidable, relatively close contact with the public
Disposable surgical mask Workers in any community or health care setting who are caring for the sick (this includes first responders) Also as a possible adjunct to protective barriers
Disposable particulate respirator mask, eye protection, gloves, gown/apron
Health care workers participating directly in close contact patient care when there is a high risk of contact with respiratory secretions, particularly via aerosols (mostly inpatient settings).
For more information, visit www.cdc.gov/flu See also: Standard Precautions: www.cdc.gov/ncidod/hip/ISOLAT/std_prec_excerpt.htm Droplet Precautions: www.cdc.gov/ncidod/hip/ISOLAT/droplet_prec_excerpt.htm
New Zealand Influenza Pandemic Action Plan v14: DRAFT FOR DISCUSSION 40
