newborn bloodspot screening training presentation bloodspot screening training presentation ......
TRANSCRIPT

www.newbornbloodspotscreening.wales.nhs.uk
Version 6 April 2016
Newborn Bloodspot Screening Training Presentation
• Introduction to Newborn Bloodspot Screening
• Gaining informed consent for newborn bloodspot screening • How to take a good quality bloodspot sample • Laboratory requests for further newborn bloodspot screening samples • Scenarios

Aims
To enable you to gain a clear understanding of the following:
• Newborn bloodspot screening (NBS) in Wales
• Process for gaining informed consent for NBS
• Knowledge and skills required to consistently take good quality NBS samples
• Reasons why requests for further NBS samples are made by the laboratory, and action required following these requests

Introduction to Newborn Bloodspot Screening

Introduction to Newborn Bloodspot Screening
Objectives
At the end of this session you should be able to:
• Explain the aim and the rationale for newborn bloodspot screening
• Assess eligibility for newborn bloodspot screening
• Give an overview of the conditions screened for in Wales

What is Screening?
‘Screening is a process of identifying apparently healthy people who may be at increased risk of a disease or condition. They can then be offered information, further tests and appropriate treatment to reduce their risk and/or any complications arising from the disease or condition.’
Wilson Junger WHO 1968

What is newborn bloodspot screening?
• Newborn bloodspot screening is when a small sample of blood is taken from the baby’s heel on day 5 of life, (counting day of birth as day 0)
• This blood sample is screened for rare but serious diseases that respond to early intervention to reduce mortality and/or morbidity
• The screening test is part of routine postnatal care
• In exceptional circumstances, if it is not possible to take the sample on day 5 then the sample must be taken between day 5 and day 8
What is the aim of newborn bloodspot screening?
To offer all eligible babies, at day 5 of life, quality assured screening for rare but serious diseases that would benefit from early intervention, and reduce mortality and morbidity from the disease.

Principles of newborn bloodspot screening
The purpose of screening is to identify babies more likely to have the conditions • Screening is strongly recommended
• Parents have a right to decline screening for all or specific tests
• Screening relies on a sample being taken at the right time and reaching the laboratory without delay
• Benefits depend on timely treatment
• Further tests are needed for diagnosis
• All results need to be communicated clearly to parents

Limitations of screening
• Screening is not 100% accurate
• Sometimes a baby with an abnormal screening result may, after having further tests, be found not to be affected by the condition (false positive)
• In other cases, a baby with a normal screening result may later be found to have the condition (false negative). This happens rarely.

Who is eligible for newborn bloodspot screening?
• All newborn babies
• Babies up to one year of age who are resident in Wales, or who move into Wales from elsewhere in the UK, if there is no evidence that:
– they have an appropriate UK newborn bloodspot screening result, or
– that it has been declined in the UK
• Any baby who is resident outside Wales but is receiving routine postnatal care in Wales

Who is eligible for newborn bloodspot screening?
• All babies up to the age of one year who move into Wales from outside the UK
• Screening for cystic fibrosis is only offered for babies up to 8 weeks of age because the test is unreliable after this time

Newborn Bloodspot Screening Wales System (NBSWS) Failsafe
• Information based failsafe system to ensure every baby is screened (or has had screening declined)
• Identifies eligible babies in Wales who do not have a newborn bloodspot screening sample in the laboratory by day 14 of life
• Every baby identified by the failsafe will be followed up
• The Newborn Screening Administration Failsafe teams contact the relevant health professionals in the health boards to follow up these babies

What conditions are screened for in Wales?
Babies are offered screening for:
• Congenital hypothyroidism (CHT)
• Cystic fibrosis (CF)
• Inherited metabolic disorders:
– Medium-chain acyl-CoA dehydrogenase deficiency (MCADD)
– Phenylketonuria (PKU)
– Maple syrup urine disease (MSUD)
– Isovaleric acidaemia (IVA)
– Glutaric aciduria type 1 (GA1)
– Homocystinuria (pyridoxine unresponsive) (HCU)
• Sickle cell disorders (SCD)

Congenital hypothyroidism (CHT)
• Affects approximately 18 babies per year in Wales
• Congenital condition - it is very rarely inherited
• Affected babies do not have enough thyroxine
• Untreated babies develop serious, permanent, physical and mental disability
• Early treatment with thyroxine tablets prevents disability
• Treatment should start by day 17 of life

Cystic fibrosis (CF)
• Affects approximately 12-14 babies per year in Wales
• 1 in 25 of population are carriers
• Autosomal recessive inherited condition – some carriers identified
• Affects the digestive system, the lungs or both
• Some babies fail to thrive
• Screening avoids delays in diagnosis
• Early treatment may improve health
• Treatment is with nutrition, medication and physiotherapy

Inherited Metabolic Disorders (IMDs)
• Expanded screening from mid-January 2015 means that four additional IMDs are now included in the newborn bloodspot screening programme in Wales:
– Glutaric aciduria type 1 (GA1)
– Homocystinuria (pyridoxine unresponsive) (HCU)
– Isovaleric acidaemia (IVA)
– Maple syrup urine disease (MSUD)
• Screening is now for six IMDs including MCADD and PKU

Screening for the IMDs
• Screening for the IMDs is offered as one test, in addition to the tests for CHT, CF and SCD
• Parents can only consent to screening for all six IMDs - not possible to test for only some of them
• The four bloodspots on the screening card must be of good quality or a repeat will be requested

Medium-chain acyl-CoA dehydrogenase deficiency (MCADD)
• Affects approximately 4 babies per year in Wales
• Autosomal recessive inherited condition
• Babies with MCADD cannot easily break down fat to make energy for the body
• Affected babies or children are usually well until potentially life-threatening symptoms occur due to metabolic crisis
• Metabolic crises can be caused by illness, fasting or vomiting

MCADD
• Screening means that babies who have MCADD can be identified early so that they can receive care to prevent potentially life threatening metabolic crises
• Treatment is by ensuring a regular ‘safe’ feeding schedule and the active management of illness or vomiting
• Emergency regimen for affected individuals who are unwell and/or not feeding well – glucose polymer

Phenylketonuria (PKU)
• Affects approximately 4 babies per year in Wales
• Autosomal recessive inherited metabolic condition
• Affected babies are unable to break down phenylalanine (an amino acid in protein) to tyrosine
• Tyrosine is required for normal brain development
• High levels of phenylalanine are neurotoxic
• Untreated babies develop serious, irreversible, mental disability
• Early treatment with a strictly controlled diet prevents disability
• Treatment should start by day 17 of life

GA1, HCU, IVA and MSUD
• Approximately one or two babies will be born each year in Wales with one of these autosomal recessive inherited disorders
• Affected babies are unable to breakdown certain amino acids contained in the protein eaten, leading to a harmful build up of toxins in the blood
• Untreated babies develop serious problems - may include coma and permanent brain damage
• Treatment is low protein diet with medications and/or supplements – with advice from specialist metabolic team
• Babies with MSUD and IVA are at risk of metabolic crisis in first days or weeks of life
• Emergency regimen during illness to prevent metabolic crisis

Benefits of screening for GA1, HCU, IVA and MSUD
• These conditions are very rare but there are significant benefits of this screening
• Babies can be identified early and given treatment – to improve long term outcome. Treatment before symptoms develop can usually prevent brain damage
• Parents can be made aware of the management of their baby if they become unwell
• If an affected baby is not screened, diagnosis may only be made if they develop symptoms which may include the sudden and severe symptoms of metabolic crisis
IMDs - Implications for other family members
• If parents have a child with one of the IMDs the risk of them having another child with that disorder is 1 in 4 (25%)
• If an affected child has older siblings, the metabolic clinician will offer, if appropriate for the disorder, testing of those children if they have not had newborn screening for that disorder
• Parents can be offered and referred to specialist genetic services for further information and advice
• Other family members can also be referred

What should happen if there is a family history of an IMD?
• Pregnant women should be asked if they have any children or other closely related family members who are known to have an IMD
• If so, the midwife should, in the antenatal period:
• Refer to a paediatrician for advice and the development of a plan of care for the baby after birth – to be recorded in the maternity notes
• Notify the Newborn Screening Laboratory by telephone and in writing. Advice will be given regarding any action required
• Appropriate advice should be given to the parents on care of their baby

Contact details for the Wales Newborn
Screening Laboratory
For clinical enquiries and when notifying the laboratory of:
• Family history of an IMD
• Earlier bloodspot sample taken due to family history of IMD:
Roanna George, Principal Clinical Scientist:
Telephone - 029 2074 3561
Email - [email protected], or
Dr Stuart Moat (Consultant Clinical Biochemist), Director of Wales Newborn Screening Laboratory:
Telephone – 029 2074 3562
Email – [email protected]

Family history of an IMD – Action after birth
• The Newborn Screening Laboratory and paediatrician should be contacted to discuss and arrange any early testing that may be needed for the specific IMD
• The laboratory will advise what tests are needed and when they should be carried out
• The tests required depend on the specific IMD and may include early bloodspot samples, urine samples and plasma samples
• In all cases, a bloodspot sample should be taken for routine newborn screening on day 5 to include the other screening tests. The family history should be documented on the card

Sickle cell disorders (SCD)
• In Wales the aim is to identify babies who have a sickle cell disorder and is not to identify babies who are carriers of a sickle cell disorder
• Affects approximately 3 or 4 babies each year in Wales
• Autosomal recessive inherited condition
• Red blood cells become sickle shaped
• Causes pain, tissue damage, infection and even death
• Early treatment including antibiotics, as well as parent education, improves health
• Treatment should be started by 2 months of age

SCD - Newborn bloodspot screening
pathway in neonatal units
• Every baby admitted to a neonatal unit in Wales should
have a single bloodspot sample taken on admission (labelled pre-transfusion sample)
• This is required because transfused blood interferes with the interpretation of SCD screening results
• The pre-transfusion sample will be used to screen for SCD if the baby had a blood transfusion between admission and day 5 of life, when the routine bloodspot sample is taken
• All information fields on the card must be completed fully at the time of the pre-transfusion sample collection
• The pre-transfusion sample should be clearly documented in the baby’s records and transfer or discharge notes

Gaining informed consent for newborn bloodspot screening

Gaining informed consent for NBS
Objectives
At the end of this session you should be able to:
• Understand why informed consent is required
• Explain what is required to gain informed consent
• Explain what should happen if parents consent to the screening
• Explain what should happen if parents decline screening

Why is informed consent required?
Newborn bloodspot screening is an invasive medical procedure and cannot be undertaken on babies without informed consent from a person with parental responsibility.

What is required to gain informed consent?
• A person with parental responsibility must receive sufficient information and have opportunity to ask questions such that they are able to give informed consent for newborn bloodspot screening
• A person with parental responsibility must receive sufficient information and the opportunity to decline consent to be contacted for future research

What information is available for parents?
• Leaflet ‘Newborn Bloodspot Screening – Information for parents’
• Explains the purpose of NBS, the conditions screened for and how the sample is taken
• Leaflet is bilingual (Welsh) and is available in other languages
• Different formats are available including large print and mp3 audio version
• All versions of the leaflet, and further information can be found on the website: www.newbornbloodspotscreening.wales.nhs.uk

When should parents receive information about this screening?
• A person with parental responsibility must receive the information leaflet in the antenatal period and again in the postnatal period as required
• This is so that they are informed as to the nature of the screening and can ask relevant questions
• They should have the opportunity to ask questions and discuss the screening with an appropriate health professional

When should this screening be discussed?
• In the antenatal period
• After birth, at least 24 hours before taking the sample
• Provide further opportunity for discussion at time of sample collection

Do parents have a choice?
• Newborn bloodspot screening is strongly recommended but parents have the right to choose
• The benefits of screening should be clearly explained
• Parents can decline screening for all or any of the conditions
• All discussions and decisions should be recorded in the maternity notes or other appropriate record, and in the baby’s Personal Child Health Record

What should happen when parents consent to the screening?
• Record the decision
• Explain the procedure
• Explain what happens to the baby’s completed bloodspot card after the sample is tested
• Explain the possibility of future invitations to take part in research. If parents decline this, tick the ‘no further research contact’ box on the screening card at the time of sample collection
• Take the bloodspot sample in line with NBSW guidance

What happens to the baby’s bloodspot screening card after screening?
• The section of the card that has the written details of the baby is separated and destroyed
• The bloodspots section is identified by a barcode number unique to both the card and the baby
• This section will be stored securely for at least five years and may be used:
- To check the result
- To carry out other tests recommended by the baby’s doctor
- To improve the screening programme
- For research to help improve the health of babies and their families in the UK

What should happen if parents decline screening?

What should happen if parents decline screening?
• Explore the reasons for their decision
• Confirm and record their decision
• Complete all information fields on the bloodspot screening card and record in the comments box ‘Decline’ for ‘All’ or specific test(s)
• Ask parents to sign the screening card confirming their decision to decline
• Send screening card to the Newborn Screening Laboratory
• Provide parents with contact details in case they change their mind
• Inform GP and Health Visitor of the screening test(s) declined

Record in the comments box
‘Decline’ for ‘All’ or specific tests 2
1
Completing the bloodspot card if parents decline screening
2
Ask parents to sign the screening card confirming their
decision to decline 3
Complete all information fields on screening card
1
3

What information should be given to parents if they decline screening?
Inform parents that:
• NBS can be offered up to one year of age
• Cystic fibrosis is only offered up to eight weeks of age because the test becomes unreliable after this time

How to take a good quality bloodspot sample
Circlefilled and evenly saturated

How to take a good quality bloodspot sample
Objectives
At the end of the session you should be able to:
• Understand the importance of taking a good quality bloodspot sample
• Know the characteristics of a good quality sample
• Know how to take a good quality sample
• Know what to do after taking the sample

The importance of taking a good quality bloodspot sample
• The aim is to enable early referral of babies for diagnostic tests and treatment by:
- Taking samples at the right time
- Taking good quality samples that do not need to be repeated
• A good quality sample is important to:
- Obtain accurate results
- Avoid false positives and false negatives
- Prevent delay in referral if repeat samples are required
- Avoid anxiety/distress associated with repeat samples
- Prevent wasting healthcare resources

What is a good quality sample?
A good quality sample has the following characteristics:
• Each of the four circles are filled by one drop of blood
• The blood has soaked through to the back of the card
• Blood has been applied to the front of the card only
• Pressure has not been applied to the bloodspots

The importance of complete and accurate information on the bloodspot card
• All information fields on the bloodspot screening card must be completed accurately so that:
– Babies can be correctly identified
– The sample can be processed by the laboratory
– Babies suspected of having one of the conditions can be followed up promptly
• The information fields should be completed at the time of the sample collection, by the health professional who has responsibility for ensuring the parents have given informed consent

• Copy of ‘Newborn Bloodspot Screening– Information for parents’ leaflet
• Newborn bloodspot screening card and glassine envelope
• NBSW prepaid envelope/stamped addressed envelope (first class)
• Baby’s NHS number
• Maternity record and personal child health record
Items required for the test
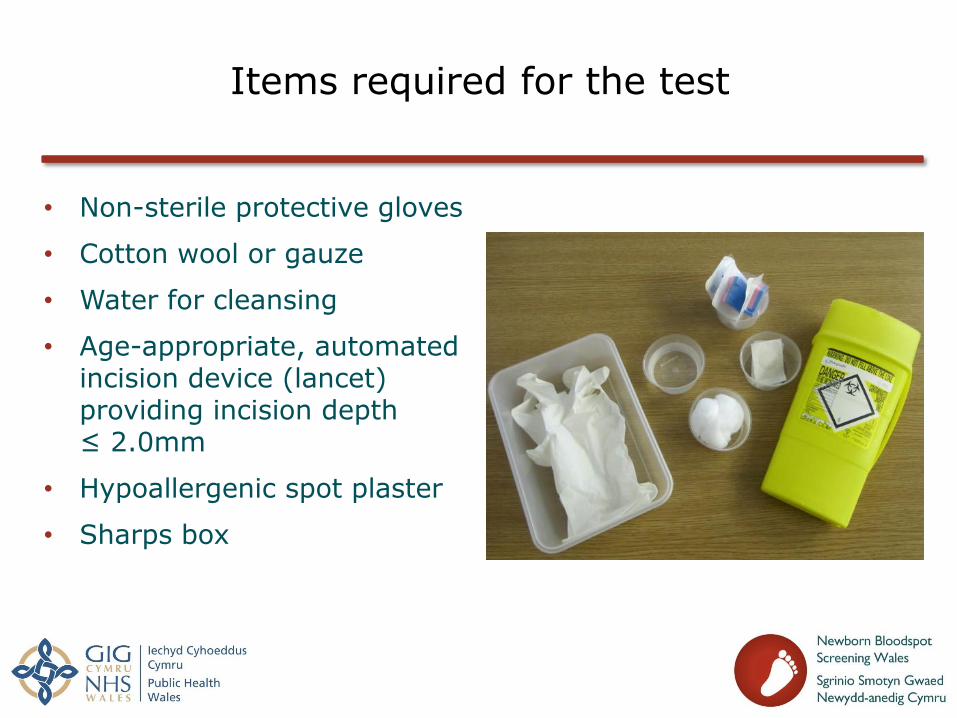
Items required for the test
• Non-sterile protective gloves
• Cotton wool or gauze
• Water for cleansing
• Age-appropriate, automated incision device (lancet) providing incision depth ≤ 2.0mm
• Hypoallergenic spot plaster
• Sharps box

On day of test:
• Ensure parents have information leaflet and opportunity to ask questions
• Explain procedure to parents and confirm their decision to accept screening
• Complete newborn bloodspot screening card contemporaneously
Preparation for taking the bloodspot sample

Preparation for taking the bloodspot sample
• Recording the baby’s NHS number on the bloodspot card is mandatory
• If the NHS number is not available – contact regional Newborn Screening Administration Failsafe team
• Check all information fields are complete and accurate, confirm with parent and make any changes
• The screening card must not be used beyond the expiry date printed on the back of the card

Baby’s NHS Number is essential – it is the only unique identifier for the
baby 1
1
Baby’s Surname This is the surname by which
the baby will be known
Baby’s Date of Birth is essential for the card to be
processed
Date of Sample is essential for the card to
be processed
Baby’s Forenames should be recorded if
known 3
5
2
4
1
2
3
4
5

Gestational age of baby at birth is essential for a
valid CHT result
Rank identifies birth order. Refer to back
of card
GP name, address, telephone number and postcode are essential to enable follow up of baby
Current parent telephone number is
essential to enable follow up of baby
6
6
7
7
8
8
9
10
Birth weight is important - can aid interpretation of
results 8
9 10

Record if a blood transfusion has been given either intrauterine or after birth.
Record date of last transfusion (most recent). If intrauterine, count day of birth as date of last transfusion
Record type of transfusion in comments box.
If baby is in hospital at time of sample, record which
hospital and ward
14
13
12
12
13
11
Is this a repeat? Record reason in the
comments box 11
Parents should be asked if they consent to future contact about research. Tick box if they do not
wish to be contacted. 14

Refers to Health Board providing care at the time of
the test
Sample taker ID is their NMC number, or a number
issued by NBSW 15
15 16
16
17
Record in Comments box: • Any screening tests declined, plus a parent’s signature and date of decline. • Any known medical condition in baby, or relevant family history • Reason for any repeat or second samples • Reason for sample being taken at a different time from routine day 5 (5-8) test • Name of person applying blood to card if not recorded as sample taker
17

• Assist parents in providing comfort measures for baby
• Ensure baby is warm and comfortable
• Additional warming of the foot should be avoided
• Position baby to maximise blood flow to heel – allow foot to hang down
• Wash hands and put on gloves (use universal precautions)
• Clean baby’s heel to avoid sample contamination:
– By washing thoroughly with plain water using cotton wool or gauze and ensure skin is dried
– The water should not be heated and the foot should not be immersed
– Do not use alcohol or alcohol wipes
How to take a good quality sample

Skin Puncture Sites for full-term and preterm infants
External and internal limits of the calcaneous (shaded areas indicate puncture sites)
• Before activation place incision device against the heel – avoiding central area and posterior curvature of the heel • Use device according to manufacturer’s instructions

• Wait for flow of blood - and formation of a hanging drop of blood
• Apply single large hanging drop of blood to centre of one circle on the screening card (apply to front of card only)
• Allow blood to fill circle by natural flow from one point in the centre
• Ensure blood seeps through to back of card
• Repeat for remaining circles
• Wipe off excess blood from heel and apply pressure until bleeding stops – apply a spot plaster if required
• Discard all sharps correctly
How to take a good quality sample

Good quality bloodspot sample
• All four circles on the card are filled and evenly saturated with blood
Front of card Back of card

• Wipe away congealed blood firmly with cotton wool or gauze
• Gently massage the foot (avoid rubbing or squeezing)
• Apply large hanging drop of blood to centre of a new circle on the card
• If blood flow does not restart, a second heel prick is necessary
- use a new incision device
- Take sample from a different part of the foot, or from the other foot
What should be done if the flow of blood stops?

• Allow bloodspots to air-dry away from direct sunlight or heat before inserting card into glassine envelope and NBSW prepaid envelope
• Glassine envelopes must be used to provide additional protection from external damage
Once bloodspots have dried

After taking the bloodspot sample
• Record taking sample in mother’s maternity record and baby’s Personal Child Health Record (red book)
• Inform parents how and when they will receive the results – normal results available within 6-8 weeks of sample being taken
• Send screening card to Newborn Screening Laboratory within 24 hours of taking sample, in the NBSW prepaid envelope or by first class post
• Record despatch details
• Record and notify screening status on discharge home or transfer to another unit

Laboratory requests for further newborn bloodspot screening samples

Laboratory requests for further newborn bloodspot screening samples
Objectives
At the end of this session you should be able to:
• Understand why the Newborn Screening Laboratory requests further samples
• Know what should happen when a repeat or additional sample is requested

Why are further samples requested?
Requests can be made for a variety of reasons - requested samples are either:
• Avoidable repeat samples or
• Additional samples for clinical reasons

Avoidable repeat samples
Avoidable repeat samples are requested when the initial bloodspot sample is unacceptable for testing because it is:
• Insufficient:
- Bloodspots made up of small volume of blood, or
- Blood not soaked through to back of card
- Small volume bloodspots give results with up to 25% negative bias
- This means there is a significant risk of a baby with a condition being missed

Avoidable repeat samples
• Poor quality due to:
- Multiple applications (multi-spotted)
- Layering of blood
- Application of blood to both sides of card
- Contamination
• Poor quality samples can cause incorrect results
• Risk of false positive results with over-spotted samples

Avoidable repeat samples
• Compressed bloodspots
- Compressed spots can give up to a 45% negative bias
- This means there is a significant risk of a baby with a condition being missed
• Valid NHS number for baby not recorded on card
• Taken before day 5 (counting day of birth as day 0)

Avoidable repeat samples
• Unacceptably delayed in reaching the laboratory (delayed between sample taking and arrival in laboratory) – sample degradation can cause incorrect results
• Essential information on card not completed or is recorded inaccurately

Poor quality bloodspot samples
Take insufficient samples
This is not acceptable for testing – a repeat will
be required.
Layer the blood
This can cause an incorrect result.
Contaminate the sample
(eg faeces, adult blood or touching the circles)
Contamination may affect the results.
Compress the bloodspot
Never compress the bloodspot because applying
pressure reduces the density of blood. This can
result in babies with a condition being missed.
Insufficient
Layering
Contaminated
Compressed
Incorrect Do Not

Avoidable repeat samples
The majority of samples that require repeating are:
• Insufficient and/or
• Do not have valid NHS number for the baby recorded
To obtain accurate results the blood must:
• Completely fill the circles
• Soak through to the back of the card
• Be evenly saturated using one drop of blood for each circle

Example 1 - Insufficient sample

Example 2 – Insufficient sample

Example 3 – Insufficient sample

Example 4 – Insufficient sample

Example 5 – Insufficient sample

Example 6 – Poor quality/Insufficient

Example 7 – Insufficient sample

Example 8 – Insufficient sample
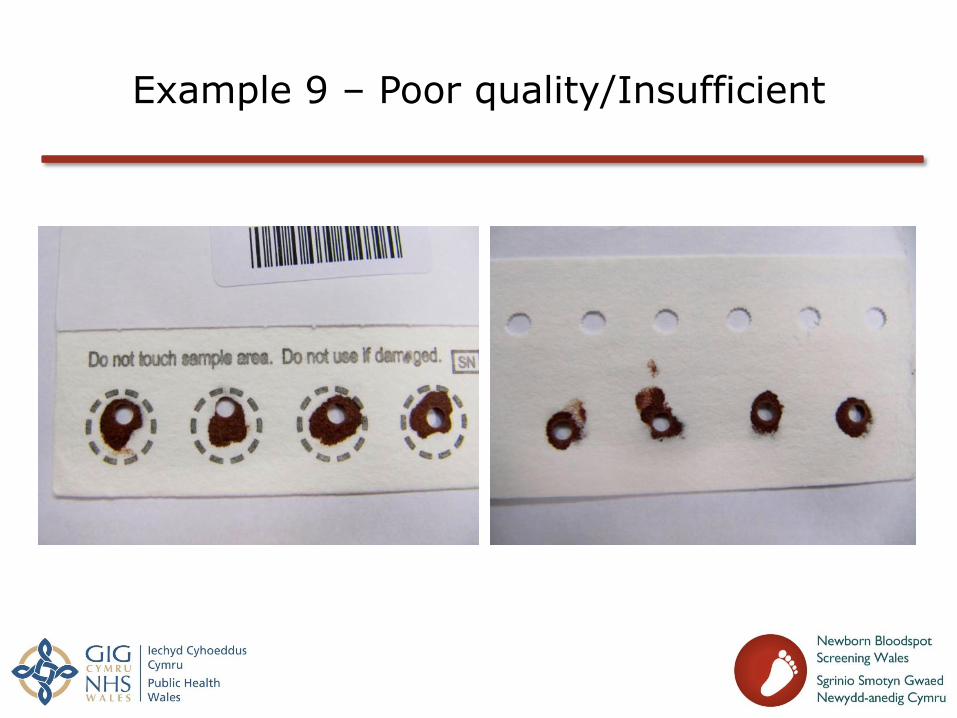
Example 9 – Poor quality/Insufficient

Good quality bloodspot sample

Additional samples requested for
clinical reasons
• Prematurity – all babies born before 32 weeks gestation
- A second CHT test is required at 28 days of age (day of birth = day 0) or on day of discharge, whichever is the sooner
- Required because routine bloodspot screening sample on day 5 could give a false negative result for CHT because of prematurity
- If baby is discharged before day 28 this must be recorded on the bloodspot card. If not, a repeat sample will be requested
• Borderline congenital hypothyroid screening results
- A second bloodspot sample is required 7-10 days after initial sample
- This request is made by letter faxed from the laboratory to the relevant staff
Additional samples requested for
clinical reasons
• If a blood transfusion had been given in the 72 hours before the initial routine bloodspot sample was taken
- Take repeat sample for CHT, CF and IMDs once 72 hours have passed without a blood transfusion
- Awaiting 72 hours enables metabolite concentrations to return to pre-transfusion levels
- Pre-transfusion sample taken on admission to neonatal unit will be used to screen for SCD

What should happen when a repeat or additional sample is requested?
• All samples requested by the laboratory should be taken within 3 calendar days (72 hours) of the request
• The ‘repeat sample’ box on the screening card should be ticked and the reason for the repeat/additional sample should be recorded in the comments box.
• Samples should be sent to the Newborn Screening Laboratory in Cardiff within 24 hours of collection, using the prepaid envelope or first class post
• The parents should be informed of the reason for the repeat or additional sample, and of when they can expect to receive the results

Laboratory requests for further information
• The laboratory sometimes needs to request further information if the documentation on the bloodspot card is incomplete or inaccurate
• These omissions or inaccuracies result in delays in the:
– Processing of the sample
– Issuing of results
– Referral of babies who are suspected of having any of the conditions
• The requested information should be sent promptly to the laboratory in writing, by a health professional who has responsibility for ensuring the information is correct

Further Information
• Website: www.newbornbloodspotscreening.wales.nhs.uk
• Email address: [email protected]
• CLIMB – Children living with Inherited Metabolic Diseases. Support and information from other patients, parents and carers is available
Website: www.climb.org.uk
Telephone: 0800 652 3181

www.newbornbloodspotscreening.wales.nhs.uk
Newborn Bloodspot Screening Scenarios
Newborn bloodspot screening scenarios
Scenario 1
A baby has moved into the area from Birmingham at 4 months of age.
What action would you take?

Newborn bloodspot screening scenarios
Scenario 2
A baby has moved into the area from Japan at 10 months of age.
What action would you take?

Newborn bloodspot screening scenarios
Scenario 3
Parents of a five day old baby have declined newborn bloodspot screening for this baby
What do you do?

Newborn bloodspot screening scenarios
Scenario 4
Parents who had declined newborn bloodspot screening have now decided that they would like their baby to have this screening. Their baby is six months old.
What do you do?
Newborn bloodspot screening scenarios
Scenario 5
A newborn baby who is being cared for by foster parents is due to be offered newborn bloodspot screening.
What issues should you consider when offering the screening?

Newborn bloodspot screening scenarios
Scenario 6
The parents wish their baby to be known by the father’s surname. This is different from the mother’s surname.
What surname should be recorded on the bloodspot card and why?

Newborn bloodspot screening scenarios
Scenario 7
A student midwife who is working with her midwifery mentor takes a bloodspot sample after gaining consent from the mother.
Where should the names of the midwife and her student be recorded on the screening card, and why?

Newborn bloodspot screening scenarios
Scenario 8
You are just about to take a bloodspot sample for newborn screening and you find that the baby’s feet are cool to the touch.
What action do you take?

Newborn bloodspot screening scenarios
Scenario 9
A sample taker obtained adequate drops of blood following skin puncture, but the blood did not seep through to the back of the screening card.
What are the possible reasons for this?
How would you ensure that the blood seeps through to the back of the card?

Newborn bloodspot screening scenarios
Scenario 10
You are just about to take a bloodspot sample for newborn screening and you are unable to find the baby’s NHS number in the records.
The baby is day 5 (counting day of birth as day 0)
What action do you take?