nhs west lancashire clinical … 4 of 7 west lancashire clinical commissioning group governing body...
TRANSCRIPT

NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING
24 SEPTEMBER 2013, 9:30 - 11:30 Boardroom, Hilldale Building, Wigan Road, Ormskirk
15 minutes to be allocated for questions from members of the public based on agenda items.
I – Information D – Discussion DR – Decision Required Members of the governing body will be available after the close of the meeting for informal discussion,
time permitting
Item WLCCGB
Time Agenda item Action Presenter
9/13/01 09:30 Welcome Greg Mitten
9/13/02 09.35 Declaration of Interests All
9/13/03 09.40 Minutes of previous meeting held on 23 July 2013 DR Greg Mitten
9/13/04 09.45 Matters arising - Action sheet DR Greg Mitten
Communication
9/13/05 09.50 Chair’s update I Greg Mitten
9/13/06 10.00 Chief Officer’s Update I Mike Maguire
Governance 9/13/07 10.10 BAF and risk register I Paul Kingan
Operational Management Section 9/13/08 10.20 Integrated business report D Paul Kingan
9/13/09 10.40 Medicines management bi-yearly report D Nicola Baxter
9/13/10 10.50 Armed forces covenant DR Dr Frampton
9/13/11 11.00 Local safeguarding children board – annual report 2013-14
I Helen Clarke
Consent items
9/13/12 11.10 Minutes of sub-committees: - Quality Improvement Committee – 20
August 2013 - Executive Committee – 25 June, 16, 30
July, 6, 13, 20 August and 3 September 2013
- Remuneration Committee – 20 August 2013
Other minutes: - Lancashire CCG network – June and July
2013
I Greg Mitten
Other Business 9/13/13 11.20 Any other business
Greg Mitten
Date and Time of Next Meeting – 26 November 2013, 9:30 am Boardroom, Hilldale, Ormskirk

Page 1 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
Minutes D R A F T
Meeting Title: NHS West Lancashire Clinical Commissioning Group Governing Body Meeting
Date: 23 July 2013
Time: 9.30 – 11.30 am Venue: Tanhouse Community Centre, Ennerdale, Skelmersdale, WN8 6AN
Present: Dr John Caine, Chair Dr Anand Bisarya, GP Executive Lead Dr Bapi Biswas, GP Executive Lead Dr John (Jack) Kinsey, GP Executive Lead Dr Simon Frampton, GP Executive Lead Greg Mitten, Lay Member Douglas Soper, Lay Member Paul Kingan, Chief Financial Officer In attendance Jo Worswick, Deputy Chief Officer Lucinda Cawley, Senior Operating Officer Planning and Service Redesign Jackie Moran, Head of Contracting, Performance & Quality Dr Rosalind Bonsor, Interim GP Executive Lead Nicola Baxter, Head of Medicines Optimisation. Lancashire CSU Joanna Rimmer, Administrative Officer
Apologies: Mike Maguire, Chief Officer Katie Wightman, Head of Corporate Affairs Karen Thompson, Public Health Specialist Dr Adam Robinson, Secondary Care Doctor Helen Clarke, Chief Nurse Steve Gross, Lancashire County Council
Agenda
Item WLCCGB/
Summary of Discussion Action
7/13/01 Welcome and apologies for absence John Caine opened the meeting of the West Lancashire Clinical Commissioning Governing Body meeting. Introductions were made by the governing body to the members of the public. No questions had been received from the public in respect of the agenda. Five members of the public were in attendance for the meeting. Apologies for absence were received from the above noted.
7/13/02 Declarations of interests There were no declarations of interests pertinent to agenda items.
7/13/03 Minutes of previous meeting held on 23 May 2013 The minutes of the meeting held on 23 May 2013 were agreed as an accurate record. The governing body:
- approved the previous minutes

Page 2 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
7/13/04 Matters arising The action sheet was updated.
COMMUNICATION
7/13/05 Chair’s update The report provided members with an update on both strategic and operational issues since the last meeting. John Caine highlighted key areas of interest:
Quality premium update – the aim of the quality premium is to reward CCGs for improvements in quality of services and deliver the patient rights and pledges on waiting times with the NHS Constitution. NHS England have confirmed that the CCG’s proposed local measures for improving services have been accepted and will be assessed at the end of 12 months.
Urgent and emergency care review – NHS England is seeking views on a review of urgent and emergency care, led by Professor Sir Bruce Keogh, NHS England Medical Director. Comments received will be used to develop a national framework to assist commissioners ensure high quality, consistent standards of care across the country. The engagement period for comments closes on 11 August 2013.
Update 111 – the chair attended a meeting of North West CCGs to discuss the way forward for the 111 service, where the proposed model was discussed. Further information is expected from NHS England in the summer. It was noted that approximately 70% of out of hours providers in the North West are still using previous systems.
Commissioning conference – the Commissioning Show in London on 12 June consisted of speakers and workshops to work through real life scenarios. It was a useful day with challenges and solutions shared. The main theme for this year is integrated care.
Governing Body development day – the development day on 9 July was arranged to reflect the CCG performance at 101 days of existence. The results were very positive and recognised the work completed to date and the work still to be achieved.
Following concerns raised at the previous Governing Body meeting in regards to ambulance waiting times at Southport and Ormskirk Hospital NHS Trust, West Lancashire CCG has been working with Southport and Formby CCG looking at key issues and it was noted that improvements have been made. The governing body:
- noted the content of the report
5/13/06 Chief Officer’s update The report provided members with an update on both strategic and operational issues since the last meeting. On behalf of Mike Maguire, Jo Worswick highlighted key areas of interest:
Quality improvement event – Following on the success of the Care Closer to home event that took place on 6 June 2013, work is currently in the process of assessing all the outputs and actions from the day to determine the most appropriate way to take this forward
West Lancashire CCG and West Lancashire Community Safety

Page 3 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
Partnership – On 1 April 2013, the CCG became ‘responsible authorities’ on community safety partnership. The CCG is now working in partnership with other responsible authorities to tackle crime and disorder. The CCG has been actively involved with the community safety partnership since 1 April 2013.
CCG Constitution – Amendments that were agreed during the last Governing Body meeting have been made. The amended constitution has been submitted to NHS England for final approval. Once feedback from NHS England is received, it will be reported back to both the Governing Body and Membership Council.
Primary Care Trust and Strategic Health Authority Transfer Schemes – Both the staff transfer scheme and the property transfer scheme were formally received by the CCG on 6 June 2013. The CCG is working with internal audit to ensure that all property transfers are appropriate.
The governing body: - noted the content of the report
GOVERNANCE
7/13/07 Register of Interests As part of governance the CCG informs the governing body of any alterations to the register of interests. The report recorded one additional declaration of interest which had been added to the comprehensive list of declarations of interest for all West Lancashire CCG governing body members. The governing body:
- noted the updated declared interests of its members
7/13/08 Medicines Optimisation Committee – draft terms of reference The report reviews the responsibilities of the CCG Medicines Management Committee (MMC) in the light of nationally defined organisational competencies and suggests actions for the CCG to consider in terms of taking early responsibility for medicine management functions. The CCG became responsible for medicine management on 1 April 2013. Key area that were highlighted included:
The role of the CCG medicine management committee is based on the National Prescribing Centre competencies
The main objects of the committee is to develop strategies and an operations plan to improve the management of medicines, manage the financial risk associated with prescribing and ensure that medicines use issues are given due weight in wider healthcare planning and service delivery agreements
It was agreed that only one GP is required for the quorum of the meeting. Agreement was also made that there will be public health involvement in this meeting and that a member of the Local Pharmacy Network and Lancashire Care Foundation Trust would be a co-opted member if appropriate.
- The governing body approved the draft terms of reference and the Medicines Management Committee will make recommendations to the clinical executive of which it is a sub-committee.

Page 4 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
OPERATIONAL MANAGEMENT SECTION
7/13/09 Integrated Business Report The report provided summary information on the financial position and activity performance of the CCG for May 2013. It also included quality and performance analysis for community based targets for Southport and Ormskirk Hospital NHS Trust. The CCG is currently working with the Lancashire Commissioning Support Unit (CSU) to develop the format of the report to ensure that all information is relevant. Paul Kingan highlighted key information from the report:
- At month 2 the CCG remains on course to deliver its financial plan for the year
- The CCG is currently forecasting a surplus of £1.4 million including 1% surplus required by NHS England.
- There has been a 4% decrease in GP referrals compared to May 2012.
- It was noted that the activity analysis results that have been provided are very early results and more detailed information will be available within the next few month. The information will be reported back to the governing body.
Doug Soper expressed that there is a need for activity plan profiling information to be provided. Paul Kingan confirmed this would be ready for the next report.
Jackie Moran reported on quality and performance and highlighted the key
information from the report. It was noted that this report focuses on
Southport and Ormskirk Hospital NHS Trust, as this is West Lancashire
CCG’s largest provider. We are aware that patients also attend other
hospitals around the area. The performance of these other hospitals
continue to be monitored and issues will be brought to the governing body
should they arise.
The key performance areas identified at Southport & Ormskirk Hospital NHS
Trust:-
- Planned care – praise was given to Southport and Ormskirk Hospital NHS Trust for the work that has been done to improve 18 week appointment time. This will continue to be monitored by the CCG.
- Unplanned care – again Southport and Ormskirk Hospital NHS Trust are performing well with 97% of patients seen in A & E, the walk in centre and the health centre being treated within four hours. Concern was however raised regarding eight minute ambulance response time. Dr Jack Kinsey noted that there are two categories for ambulance response times, it was stated that the data that has been provided is only for eight minutes. It was also suggested that delays may be due to ambulance turnaround times at A & E. Jackie Moran to write a letter to North West Ambulance Service to raise the concerns and request further information.
- Sickness rates at Southport and Ormskirk Hospital NHS Trust – staff sickness levels at Southport and Ormskirk Hospital NHS Trust are indicated as red against a stretching target that has been set internally, however the CCG has been informed that the trust is tackling this issue this year. The CCG has also compared the data to other acute trusts in the area and findings have shown that
Paul Kingan Jackie Moran

Page 5 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
Southport and Ormskirk Hospital NHS Trust are not performing too badly in comparison.
- Mortality rates for stroke patients at Southport and Ormskirk Hospital NHS Trust – This issue has also been raised by the Merseyside Quality Surveillance group. The mortality figure for diabetes has also seen an increase. The CCG’s Quality Improvement Committee agreed to raise this with the trust, discussion are also taking place with Rob Gillies, Medical Director.
- Complaints – Serious untoward incidents data from Lancashire Care Foundation NHS Trust regarding unexpected deaths, a report will be received in autumn and benchmarking work is to be completed with other mental health trusts. Jo Worswick informed the governing body that the CCG is informed of all unexpected deaths of West Lancashire patients. Serious untoward incidents are only closed once the lead CCG and the Quality Improvement Committee are satisfied.
The governing body:
- noted the performance to date and the actions in place to improve performance.
Greg Mitten
7/13/10 Funding Allocation Risk Paul Kingan presented the paper, which outlined the current position in terms of the financial risk associated with CCG funding allocations. The funding allocation issues are preventing contracts from being signed and the Local Area Team from agreeing the CCG’s non-recurrent spending plans. The key areas of risk were identified: Specialist commissioning funding – the scope for specialist commissioning has expanded. A further adjustment was made to the CCG allocation by the Department of Health to transfer more resources to the specialist commissioning teams. The CCG is expecting resources to come back to it based on further work carried out by the specialist commissioning team. Paul Kingan will keep the CCG executive and governing body aware of this on a regular basis. Central Lancashire PCT budget – an exercise was carried out by the central Lancashire finance team to split the Central Lancashire PCT budget in to three CCGs, however it is apparent from retrospective review that some budgets were split on a ‘fair share’ basis even though the activity predominantly relates to a particular CCG. The CCG has brought this to the attention of the relevant CCGs as well as the Lancashire Area Team, and is working collaboratively to resolve this. Prop Co – The CCG is currently working with Prop Co assessing the proposed recharges to understand any funding anomalies associated with recharges from former PCT leased buildings. Prop Co has also made a charge across all CCGs for unoccupied building space which it cannot recharge to tenants. Paul Kingan will update the governing body on any emerging financial risks. Doug Soper acknowledged the positive progress that has been made by the CCG finance team with regard to understanding the funding allocation risk.
The governing body:

Page 6 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
- noted the report and were satisfied that this matter is being addressed appropriately.
7/13/11 Dementia appraisal
The report provided an update on the progress of the work by Lancashire CCGs to undertake an option appraisal for the single specialist dementia facility. Key areas of the report discussed:
- A public consultation took place early 2013 regarding the reconfiguration of specialist dementia beds in Lancashire. The outcome of this consultation was an agreement that there should be a single facility of 30 beds in Lancashire, with additional local community services. However there was not overwhelming support for the site to be in Blackpool and the Lancashire CCGs were asked to undertake a site option appraisal.
- A joint CCG Specialist Dementia Committee has been established for CCGs and other local authorities to work in collaboration to move this forward. Dr Simon Frampton attends on behalf of West Lancashire CCG.
- An appraisal methodology has been developed with various criteria. - A report is due September 2013 for agreement by CCGs. - Dr Simon Frampton noted that there is not a perfect site for all
patients in Lancashire. - Dr John Caine noted that the number of patients admitted to
specialist dementia beds from west Lancashire is relatively small and that most patients will receive services that will be locally provided in the community.
The governing body:
- noted the report and were satisfied that this matter is being addressed.
CONSENT ITEMS
7/13/12 Minutes of sub-committees: Quality Improvement Committee The draft minutes of the Quality Improvement Committee (QIC) meeting held on 25 June were noted. Executive Committee The minutes of the Executive Committee meetings held on 18 June 2013 were noted. Other minutes: Lancashire CCG network The minutes of the Lancashire Clinical Commissioning Network meeting held on 25 April and 30 May 2013 were noted.
Other business
7/13/13 Any other business One West Lancashire is holding an event on 12 September 2013, it was agreed it would be beneficial for members of the CCG to be involved in this event, where a number of issues could be raised.

Page 7 of 7 West Lancashire Clinical Commissioning Group Governing Body meeting 23 July 2013
Meeting closed at 11am
Date and time to next meeting: Tuesday 24 September 2013, 9:30 am Boardroom, Hilldale, Ormskirk

Page 1 of 2
Agenda item no: WLCCGB
West Lancashire CCG Governing Body meeting 23 July
Action Lead Date required by Action completed
7/13/09 – Integrated Business Report – it was agreed that activity profiling information is to be provided
Paul Kingan 24 September 2013
7/13/09 – Integrated Business Report – Write a letter to North West Ambulance Service to raise concerns and request further information
Jackie Moran 24 September 2013
7/13/09 – Integrated Business Report – Issues regarding mortality rates to be raised with Southport and Ormskirk Hospital NHS trust.
Greg Mitten 24 September 2013
28 May
Action Lead Date required by Action completed
5/13/06 - Chief Officer’s update – Whistleblowing – it was agreed to amend the constitution and seek Membership Council approval.
Katie Wightman 19 June 2013
Complete
5/13/09 – Integrated Business Report – enquire if advanced nurse practitioners are used in the A&E department as an alternative for junior doctors – confirmation received clarifying that nurse practitioners are not used.
Mike Maguire 23 July 2013
Complete

Page 2 of 2
5/13/11 – Minutes – Lancashire CCG Network – Further information regarding domestic violence will be provided at the Executive Committee.
Lucinda Cawley June 2013
Complete
23 April
Action Lead Date required by Action completed
4/13/07 Integrated business report – Complaints reporting – A record of GP’s concerns is fedback to the GP Operational Forum, which report to the Strategic Partnership Group. Jo Worswick will look to see what benchmarking information is available and include in future reports.
Jo Worswick Sept 2013
26 March 2013
Action Lead Date required by Action completed
3/13/14 Frances report - A formal letter to the provider was sent on 5 March suggesting collaborative work take place, as yet no reply had been received and it was recommended that this was escalated
to the chair or chief officer to follow-up. A
follow up letter was sent, with some of the outstanding information received. The quality issues will be raised at the executive committee and return to the next governing body meeting.- The Quality Committee will continue to push this forward
Dr John Caine and Mike Maguire 23 July
Complete

Chair’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
1
Agenda item no: WLCCGB 9/13/05
WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT
DATE OF BOARD MEETING: DRAFT 24 September 2013 TITLE OF REPORT: Chair’s Update BRIEFING POINTS:
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact No
2. Commissioning of hospital and community services – please outline
impact Winter funding and preparedness
Yes
3. Commissioning and performance management of GP Prescribing –
please outline impact No
4. Delivering Financial Balance – please outline impact No 5. Development of the commissioning group as a commissioning
organisation – please outline impact
Yes
B. Governance – Yes 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice
No
2. Additional resource implications
(either financial or staffing resources) No
3. Health Inequalities No
4. Human Rights, Equality and Diversity Requirements No
5. Clinical Engagement
No
6. Patient and Public Engagement Yes
REPORT PREPARED BY: Katie Wightman, Head of Corporate Affairs
REPORT PRESENTED BY: Greg Mitten, CCG Vice Chair

Chair’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
2
WEST LANCASHIRE CLINICAL COMMISSIONING GOVERNING BODY CHAIR’S UPDATE
PURPOSE 1. This report provides an update on both strategic and operational issues of interest to Governing
Body members in the months since the last meeting.
Dementia Update
2. As members are aware a Joint CCG Specialist Dementia Committee (JCCGSDC) was established to respond to the recommendations from the outgoing NHS Lancashire Board in March 2013. The membership of the JCCGSDC included representatives from all 8 CCGs in Lancashire, together with representatives from Lancashire County Council and Blackpool and Blackburn with Darwen Borough Councils. The Committee invited representatives from Healthwatch, Age UK and the Alzheimer’s Society to assist them in their deliberations.
3. It was charged with the responsibility of undertaking an appraisal of the options for the specialist dementia unit location. The group was also asked to consider, and where appropriate, develop solutions to the access and travel issues raised in the consultation and to ensure a range of support is available for people and families living with dementia.
4. The preferred option arising from the 12-week consultation on specialist inpatient dementia services, conducted by former PCTs across Lancashire, was for one specialist dementia inpatient unit for the County and for this to be located at the Harbour site close to Blackpool.
5. The JCCGSDC has reviewed the options for site location and set out their recommendations to the Lancashire CCG Network. The CCG Network, as a non-decision making body, is recommending CCG Governing Bodies consider the recommendations and approve the Harbour as the site for the 30 bed inpatient specialist dementia unit for Lancashire. It was recognised that some residents of West Lancashire may prefer to be treated in facilities closer to home and therefore the CCG is looking to commission alternatives from other providers.
6. Investigations into services which may offer a more local service commenced in August and it being proposed that these investigations should be allowed to be completed prior to the Governing Body taking the decision on whether to approve the Harbour site for the inpatient dementia unit.
7. It is proposed that the local options will be investigated and reported back to the Clinical Executive Committee and a recommendation from that Committee will be made to the Governing Body at the meeting in November 2013.
CCG Development Framework 2013/14 - Working together to achieve excellence in clinically led commissioning
8. On 6 September NHS England published the CCG Development Framework. Co-produced with
CCGs and open to continuous improvement as the organisations learn more together, the CCG Development Framework supports CCGs in developing and is a key part of NHS England’s commitment to support CCG development nationally.
9. The framework, developed and overseen by the NHS Commissioning Assembly CCG development working group, sets out how further insight into what constitutes a great CCG will be gained and how every CCG will be supported to access development support that recognises its local circumstances and differing stages of maturity.
10. The CCG development framework identifies the most important areas for future development if CCGs are to succeed in securing great outcomes and leading transformation. It is intended to support CCGs and area teams of NHS England in identifying where to prioritise development

Chair’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
3
efforts; it will guide NHS England in its leverage of development resources with national partners; and it will signal to suppliers of development where they can most effectively add value. CCGs and NHS England will work in partnership to take forward the CCG development agenda.
11. The CCG development framework will be refreshed annually in partnership with CCGs, improving and adapting as CCGs progress along their development journey to become great local commissioners. From this framework an annual CCG development programme will be developed with CCGs identifying who will do what by when
12. The framework can be downloaded at http://www.england.nhs.uk/wp-content/uploads/2013/08/20130829-CCG-Development-Framework-final-v5.0.pdf
Integrated Care Fund
13. In June the Local Government Association and NHS England published their planning vision for how the pooling of £3.8 billion of national funding, announced by the Government in the June spending round, will ensure a transformation in integrated health and social care.
14. The ‘Integration Transformation Fund’ is a single pooled budget for health and social care services to work more closely together in local areas. The current plans are for the budget to be held by local health and well-being boards.
15. As the money to be invested in the integration transformation fund will have to be found by CCGs largely from existing budgets we are, like other CCGs, currently considering the implications of this. The fund equates to approximately 3% of current CCG allocations and plans will need to be developed during 2013/14 and 2014/15 in advance of funding transferring to a pooled budget from 2015/16.
16. We are clear however that the fund must be used for local initiatives that are multi-agency, support integration and improve outcomes for people in both health and social care. The CCG is currently working with partners across Lancashire and the local health economy to prepare for further integration of health and social care.
One West Lancashire
17. The CCG had representation at the inaugural meeting of One West Lancashire. This is a “strategic forum with representation from all sectors harnessing and directing the combined local assets across health, education, environment and the economy to improve the opportunities for and wellbeing of West Lancashire”.
18. The CCG is pleased to be a partner in this forum as it compliments the focus and direction of the Strategic Partnership Board and Care Closer to Home that it is an active member of across the health economy. One West Lancashire will afford the CCG the opportunity to participate in areas more focussed on the wider determinants of health, helping to ensure and enhance long term health and wellbeing improvements for the West Lancashire population.
19. The West Lancashire Health and Wellbeing Group and the Community Safety Partnership that the CCG participates in sit under the One West Lancashire arrangements. These forums continue to be important for the CCG’s contribution to delivery of the Lancashire Joint Health and Wellbeing strategy.
North West Ambulance Service – Foundation Trust Application
20. North West Ambulance Service has recently been informed by Monitor that they have not been successful in their FT license at this time.

Chair’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
4
21. They have been deferred for a period of 6 to 12 months on the basis of requiring better processes for quality governance, I understand there have been no issues raised with the fundamental running or delivery of the organisation.
22. North West Ambulance Service have accepted Monitors feedback and will now work to quickly rectify the areas of weakness.
Public Engagement
23. As governing body members are aware we have established a new group called My View, which anyone living or working in West Lancashire can join.
24. My View enables public/patients who join to keep updated with healthcare news and be able to share their views on areas of interest.
25. I am please to report that 500 people have joined My View to date. We have issued a small introductory e-bulletin to the group and we plan to produce a quarterly bulletin.
26. We are keen to encourage more people to join My View as the views of patient and the public are essential to what we do and vital to the future of healthcare in West Lancashire.
27. More information about My View can be found on our website at
http://www.westlancashireccg.nhs.uk/have-your-say/get-involved/
Recommendation 28. Members are asked to note the content of the report and support the proposed process for
completing the investigations in relation to the dementia service in time for a decision to be made at the November meeting of the Governing Body.
Greg Mitten
Vice Chair September 2013
Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
1
Agenda item no: WLCCGB 9/13/06
WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT
DATE OF MEETING: DRAFT 24 September 2013 TITLE OF REPORT: Chief Officer’s Update BRIEFING POINTS:
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact No
2. Commissioning of hospital and community services – please outline
impact
No
3. Commissioning and performance management of GP Prescribing –
please outline impact No
4. Delivering financial balance – please outline impact No 5. Development of the commissioning group as a commissioning
organisation – please outline impact CCG Assurance process
Yes
B. Governance – information governance Yes 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice
2. Additional resource implications
(either financial or staffing resources) No
3. Health Inequalities No
4. Human Rights, Equality and Diversity Requirements Yes
5. Clinical Engagement
No
6. Patient and Public Engagement Yes
REPORT PREPARED BY: Katie Wightman, Head of Corporate Affairs REPORT PRESENTED BY: Mike Maguire, Chief Officer

Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
2
WEST LANCASHIRE CLINICAL COMMISSIONING GOVERNING BODY CHIEF OFFICER’S UPDATE
Purpose 1. This report provides an update on both strategic and operational issues of interest to
Governing Body members in the months since the last meeting.
CCG Constitution 2. I am pleased to report that following the CCG’s submission of its amended
constitution to NHS England confirmation was received on 15 August that all the proposed amendments have been approved by NHS England.
3. The constitution can be found on our website http://www.westlancashireccg.nhs.uk/wp-content/uploads/sites/4/2013/08/WL-constitution-Final-Aug-2013.pdf
CCG Assurance 4. Following the publication by NHS England of the interim arrangements for the CCG
assurance process earlier in the year I can confirm that we have had our first quarterly assurance checkpoint meeting with local area team of NHS England to assess our performance against the framework, our strategic plan and financial position.
5. The framework itself is designed to give assurance that CCGs are delivering quality
and improving outcomes for patients locally, and as part of national standards, and in respect of continuous improvement as developing organisations from authorisation, which was a point in time. The full framework can be found at http://www.england.nhs.uk/wp-content/uploads/2013/05/ccg-af.pdf
6. I am please to inform the governing body that we received positive feedback from
the local area team. In the main we were rated as ‘green’ or ‘amber/green’. We were required however to submit an action plan against two indicators which was 62 days cancer waits and the Friends and Family Test response rate in A&E department at Southport Hospital.
7. We submitted the action plan in line with the deadline of 4 September and are
awaiting feedback. 8. The balanced scorecard detailing the CCG’s performance will be published on the
CCG website by the end of September.
Preparing for Winter 2013 9. The CCG has, via the Care Closer to Home, progressed on key work streams
detailed in the diagram on the following page.

Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
3
10. Phase 1 is approaching completion in terms of understanding the current position and designing future state requirements. Phase 2 is commencing to implement actions.
11. Preparing for winter is a key part of this programme which commenced in June
across the health economy to ensure that all partners are co-ordinated. Progress since June is as follows:
An A&E task and finish group commenced in August to progress actions. The
group will report back to the Care Closer to Home Board. Monthly meeting are taking place between West Lancashire CCG and Southport and Formby CCG and their respective local area teams of NHS England; Lancashire and Mersey discuss winter planning and assurance.
The Emergency Care Intensive Support Team undertook an internal and whole system pathway reviews for urgent care during July and early August. The recommendations have been interpreted and shared with the executive boards of Southport and Ormskirk Hospital Trust, Trust Development Authority, Care Closer to Home, Strategic Partnership Board and the CCG Executive teams.
A whole system action plan has been created to support the ECIST recommendations.
Specific winter assurance plans have been created for key Southport and Ormskirk Hospital Trust and mental health services for escalation and delivery plans.

Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
4
Winter Funding 12. As part of the above planning and review key gaps and costs to support
development during winter were produced in August. The key gaps to address were frail elderly services, discharge, intermediate care and ambulatory emergency care provision. These were costed at £5.9million and a bid was submitted against winter monies from NHS England.
13. On the 10 September a national announcement was made to confirm allocation of monies and our health economy was given £4,041,800.
14. Discussions are now taking place over the arrangements for the on-going monitoring of delivery of these
Care Closer to Home Update 15. In July a Programme Sponsor for Care Closer to Home (Janice Horrocks) was
appointed to work across Southport and Ormskirk Hospitals, West Lancashire CCG and Southport and Formby CCG The post will take lead responsibility for the Care Closer to Home (CCtH) Programme and the delivery of expected benefits.
16. Since starting in the post Janice Horrocks has undertaken a review of the
programme by canvassing views during her induction with over 30 individual stakeholders and a number of groups, which included teams of clinicians and West Lancashire CCG Clinical Executive Committee and CCG staff.
17. Janice presented her findings in a report which highlighted the need to strengthen
partnership working, improve the governance of the CCtH Programme and ensure that there is greater focus on achieving the desired outcomes and benefits for patients. IT infrastructure was identified as a critical barrier to successful service transformation. A number of new roles and functions have been put in place and the review highlighted the need to ensure that these ways of working are fully incorporated and embedded in a consistent and systematic way by undertaking a review of how community services (including primary and social care) work effectively as a seamless system actively working with communities and the third sector.
18. In considering the review, the CCtH Programme Board approved a number of
recommended actions, which are summarised as follows:
The adoption of the new governance and architecture for the CCtH Programme and a review of the membership and terms of reference of programme meetings to support this.
Progress the development of ‘enabling’ work to support change. For example, Communication, a consistent approach to project management and equality impact assessment.

Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
5
Equality Duty 19. As part of the CCG Authorisation process, the CCG declared that at the point of
authorisation it would be compliant with the public sector Equality Duty and will demonstrate the use of the Equality Delivery System to help obtain compliance and ensure good equality performance.
20. The public sector Equality Duty, part of the Equality Act 2010, is made up of a
‘general duty’ which is the overarching requirement and the ‘specific duties’ which are intended to help performance of the general duty. The general duty has three aims and it applies to most public authorities, including NHS England and CCGs (and bodies exercising public functions such as private healthcare providers), who must, in the exercise of their functions, have due regard to the need to:
o Eliminate unlawful discrimination, harassment and victimisation and other
conduct prohibited under the Act. o Advance equality of opportunity between persons who share a relevant
protected characteristic and persons who do not share it. o Foster good relations between persons who share a relevant protected
characteristic and persons who do not share it. 21. Under the specific duties of the public sector Equality Duty, CCGs are required to
publish in a manner that is accessible to the public.
a) Information to demonstrate its compliance with the public sector Equality Duty at least annually, starting by 31 January 2014. This information must include, in particular, information relating to people who share a protected characteristic who are:
Its employee – (as a public authority with fewer than 150 employees the CCG
will be exempt from this requirement) People affected by its policies and practices
b) Equality objectives at least every four years starting by 13 October 2013. All such
objectives must be specific and measurable.
West Lancashire CCG will discharge its duties with the support of the Lancashire and Staffordshire Commissioning Support Unit. Progress to date is outlined below:
The CCG must agree and publish its Equality Objectives by 13 October 13;
the proposed objectives will be presented to the Quality Improvement Committee in the coming weeks for consideration.
The CCG has in place an Equality Diversity Strategy, currently being reviewed to ensure it links with the organisations business objectives following the refresh of the Integrated Plan.
The Equality Delivery System is a tool for assessing the CCGs performance and compliance against the Equality and Human Rights Legislation. The CCG will be undertaking a review (with the involvement of public/stakeholders) of its baseline self assessment against four goals of the Equality Delivery System during October 2013. This will provide the CCG with clear areas for development in 2014/15.

Chief Officer’s Update West Lancashire Clinical Commissioning Group Governing Body Meeting – 24 September 2013
6
Practice managers meeting 22. Along with Donna Roberts, head of primary care commissioning at the local area
team of NHS England, I attended the practice managers meeting. The purpose of the meeting was to give practice managers the opportunity to raise questions directly with us as commissioners. The meeting was productive and provided answers to several areas where clarity was needed. The area team and CCG will both continue to attend the practice managers meeting on a quarterly basis. Practice managers continue to receive a weekly bulletin from the CCG, which goes out to all practice staff.
Recommendation 23. Members are asked to note the content of the report. Mike Maguire
Chief Officer September 2013

Board Assurance Framework - Update 3 – August 2013 West Lancashire Clinical Commissioning Group Governing Body meeting – 24 September 2013 Page 1 of 13
Agenda item no: WLCCGB 9/13/07 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP
GOVERNING BODY REPORT
DATE OF BOARD MEETING: 24 September 2013 TITLE OF REPORT: Board Assurance Framework and Risk Register BRIEFING POINTS: Outlines key risk areas
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience)
– please outline impact No
2. Commissioning of hospital and community services – please outline impact No
3. Commissioning and performance management of GP Prescribing – please
outline impact No
4. Delivering Financial Balance – please outline impact No 5. Development of the commissioning group as a commissioning organisation –
please outline impact Yes
Part of governance arrangements
B. Governance – please outline impact Yes 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice
Provides overview and updates on all strategic and operational risks 2. Additional resource implications
(either financial or staffing resources) No
3. Health Inequalities No
4. Human Rights, Equality and Diversity Requirements No
5. Clinical Engagement No
6. Patient and Public Engagement No
REPORT PREPARED BY: REPORT PRESENT BY:
Katie Wightman, Head of Corporate Affairs Paul Kingan, Chief Finance Officer

Board Assurance Framework - Update 3 – August 2013 West Lancashire Clinical Commissioning Group Governing Body meeting – 24 September 2013 Page 2 of 13
Board Assurance Framework and Risk Register Introduction 1. A Board Assurance Framework (BAF) and risk register are key parts of the CCG’s governance
arrangements. These arrangements include a requirement for the Governing Body to review the documents at least twice per year. There has been significant progress on both the BAF (appendix 1) and the Risk Register (appendix 2) since the last report.
Board Assurance Framework
2. Below is a summary of developments in the key areas.
Engagement There have been a number of positives since the last update. The CCG engagement strategy was approved by the Governing Body in May and implementation is progressing. The ownership programme, ‘My View’ has been launched, information disseminated and the first meeting of the group is expected in the autumn. Governing Body meetings are now scheduled to take place in public venues, except for September where the meeting will be held in the CCG’s new accommodation. The GP newsletter is now published weekly and an improved communications system has been implemented to assist information flows around the patch. Taking into consideration the current status of the BAF and the progress on linked areas from the risk register the overall risk rating for engagement has moved from moderate to low.
Delivery
Internal teams are up to full capacity, CSU input agreed and any initial issues regarding specific roles resolved. Internal reporting systems are in place and further development will include examination of a dashboard approach. A national assurance reporting process has been established, overseen by the local area team, which the CCG will be required to report against. Quarter one assessments are currently being worked through. Taking into consideration the current status of the BAF and the linked areas from the risk register the overall risk rating for delivery remains moderate.
Contracts
There has been progress but no sign-off of main contracts due to a lack of clarity and agreement around the allocation for specialist commissioning with other CCGs. Contracted services are however operating to contract specifications pending sign-off with no major pressures expected. With regard to monitoring, work is ongoing and data flows have been established but some issues remain relating to data access. The CCGs response to a Serious Untoward Incident (SUI) has been tested and the process and outcomes are positive but will be subject to review. Taking into consideration the current status of the BAF and the linked areas from the risk register the overall risk rating for contracts remains moderate.
Operational Systems
The new finance ledger system is live and fully operational with any initial issues satisfactorily resolved. There is still some uncertainty around the budget allocation and assignment but this is the subject of ongoing discussions and a positive outcome is anticipated. The CCG now has a comprehensive financial plan in place based on individual contract values. Internal systems are becoming embedded and the finance team is fully established. The CSU support is also now in

Board Assurance Framework - Update 3 – August 2013 West Lancashire Clinical Commissioning Group Governing Body meeting – 24 September 2013 Page 3 of 13
place. Taking into consideration the current status of the BAF and the linked areas from the risk register the overall risk rating for operational systems remains moderate.
Risk Register
3. The risk register is a management tool designed to enable the CCG to understand its
comprehensive risk profile. Each risk has been considered in terms of the possible consequence in the event that the risk materialises against the likelihood that it will occur. These two elements are assessed using objective descriptors which are translated into numeric values to support the creation of a risk score. Scores of 15 or more are routinely reported to the governing body. There are at this time no risks on the register with a score of above 15 and therefore the CCG is not currently managing any high risks. The register contains 16 risks, 15 in the moderate band (score of 6 to 10) and 1 significant (score of 10 to 15). The significant risk (no. 10b) relates to lack of nursing input into safeguarding and the management of serious untoward incidents (SUI’s). Plans to manage/reduce this risk are progressing but not yet fully implemented.
Updates
4. One risk score (no. 5) has been reduced from significant to moderate because of the improving prospects of a positive outcome in relation to the budget allocation and assignment. Two risk scores (nos. 9 and 10a) have reduced as a result of progress on the action plans but still remain in the moderate bracket. One risk score (no. 3) has increased but still remains in the moderate bracket. The increase is due to the limited progress on agreement of the CCG business intelligence needs with the CSU. Five risk scores (nos. 1, 2, 12, 14, 15) have been downgraded to low (score of 1 to 5) as a result of good progress on action plans and the reduction in likelihood. The position will be monitored until the next review and if the situation remains the same the risks will be removed from the active register.
The risk register will continue to be presented to the clinical executive committee for appropriate action and the CCG’s audit committee for monitoring of that action.
Recommendations
5. Members are asked to receive the board assurance framework and risk register and consider
the arrangements in place for identifying and managing strategic and operational risk. Paul Kingan Chief Finance Officer September 2013

Appendix 1
West Lancashire CCG Board Assurance Framework Update 3 – August 2013
West Lancashire CCG Board Assurance Framework
Aim: To identify and manage potential risk of failure to achieve the objectives of the Integrated Commissioning Plan 2012 - 2017
GB
Lead
Critical Outcome
Key Controls
Assurance on controls
Board Reporting Mitigation
OP
Lead
Principle areas
of risk Gaps in control
Gaps in assurance
Level of
assurance
Link to Risk
Register
Status
Gov. Body Lead
Operational
Lead
The possible
outcome should risks not be controlled
These are the specific
areas where failure will risk a critical
outcome
Processes and plans in place or actions being taken to mitigate risk in
principle areas
Internal or
external reporting arrangements that provide assurance to the Board that
controls are effective
Areas where controls are
not in place or are ineffective
Areas of
insufficient evidence to assure the Board that
controls are being effective
Must state either
None Limited
Significant Full
Colour
indicates current level
of risk (based on risk score)
Colour indicates current
status of principle risk area Red = off Track
Amber = On Track Green = Completed
Dr.SF (Comm) Dr. JK (Clinical)
Katie
Wightman
Failure to engage effectively with stakeholders
Key targets for effective collaboration and shared vision. 1. Membership & practice staff 2. Provider clinicians 3. Patients & public 4. Partners and other groups - including :
Councils Voluntary sector MPs Media
1a) Weekly newsletter 1b) Clinical exec. Feedback to practices 1c) Sharepoint (inter practice info sharing) 1d) Clinical exec. Feedback to practices 2a) Replacement engagement mechanisms being considered by Trust to replace Clinical Senate and operational groups 2b) Direct CO links 3a) Website & Media coverage 3b) Public Board Mtgs 3c) Joint networking 3d) Patient participation groups 3e) Patient focus groups 3d) My View group 4a) Media briefings via CO & Chair 4b) Regular briefings and mtgs with local MPs 4c) Commissioning toolkit has specific engagement element
Membership Council Meetings Peer review meetings Gov Body GP practice visits Service specific clinical meetings Specialist services groups CSU support re comms and statutory requirements i.e Freedom of Info CCG representation on LCC Health & Wellbeing Board Strategic Partnership Board
Feedback arrangements need embedding Limited engagement with secondary providers Systems in place to receive feedback from hard to reach groups need improving
Feedback from practices to be improved Co-ordination of information flow between key stakeholder groups needs improving
Full
Comprehensive communications and engagement strategy in place
Limited Improvements to feedback arrangements for all target groups
Full Dedicated CSU input in place
Overall rating
based on linked risks:
Low
Green
Amber
Green

West Lancashire CCG Board Assurance Framework Update 3 – August 2013 Page 5 of 13
GB
Lead
Critical Outcome
Key Controls
Assurance on controls
Board Reporting Mitigation
OP
Lead
Principle areas
of risk Gaps in control
Gaps in assurance
Level of
assurance
Link to Risk
Register
Status
Gov. Body Lead
Operational
Lead
The possible
outcome should risks not be controlled
These are the specific
areas where failure will risk a critical
outcome
Processes and plans in place or actions being taken to mitigate risk in
principle areas
Internal or
external reporting arrangements that provide assurance to the Board that
controls are effective
Areas where controls are
not in place or are ineffective
Areas of
insufficient evidence to assure the Board that
controls are being effective
Must state either
None Limited
Significant Full
Colour
indicates current level
of risk (based on risk score)
Colour indicates current
status of principle risk area Red = off Track
Amber = On Track Green = Completed
MM
Jo
Worswick
Failure to deliver
1. Actual failure to deliver service priorities to plan including QUIPP targets
1a) Integrated Commissioning Plan 1b) Shared vision and specific targets agreed with strategic partners 1c) Project planning and implementation:
i) Commissioning toolkit designed for large projects ii) Project management system for smaller projects
1d) KPIs, priorities and targets defined for key projects 1e) Monitoring of QUIPP linked into financial reporting system 1f) CSU support for comms, finance and business intelligence
CCG fully authorised with no conditions Strategic Partnership Board (SPB) (5 key priorities agreed) 6 care pathways agreed with SPB and programme of work developed Commissioning toolkit scheduled for adoption by strategic partners Integrated business report to Exec. Group and Gov. Body Quality Committee reporting to Exec. Group and Gov. Body Local Area Team to report to NCB
CCG not lead commissioner
KPIs not yet in place for all areas
Specific monitoring tool for QUIPP not yet in place (being developed)
Lack of clarity around external reporting requirements
Full
i) CCG and partners authorised ii) All projects and teams up to full capacity iii) CSU support established. Issues regarding specific tasks being resolved as they arise
Limited iv) LAT in place. National reporting process established. Currently working through Q1 assessment v) Internal reporting systems in development
Overall rating
based on linked risks:
Moderate
Green
Green
Green
Amber
Amber

West Lancashire CCG Board Assurance Framework Update 3 – August 2013 Page 6 of 13
GB
Lead
Critical Outcome
Key Controls
Assurance on controls
Board Reporting Mitigation
OP
Lead
Principle areas
of risk Gaps in control
Gaps in assurance
Level of
assurance
Link to Risk
Register
Status
Gov. Body Lead
Operational
Lead
The possible
outcome should risks not be controlled
These are the specific
areas where failure will risk a critical
outcome
Processes and plans in place or actions being taken to mitigate risk in
principle areas
Internal or
external reporting arrangements that provide assurance to the Board that
controls are effective
Areas where controls are
not in place or are ineffective
Areas of
insufficient evidence to assure the Board that
controls are being effective
Must state either
None Limited
Significant Full
Colour
indicates current level
of risk (based on risk score)
Colour indicates current
status of principle risk area Red = off Track
Amber = On Track Green = Completed
Dr. BB
Jackie Moran
Failure to effectively manage contracts to ensure high quality services
1. Contract sign-off 2. Monitoring of key performance indicators inc. resilience and recovery planning 3. Lack of suitable providers
1a) Contract process action plan 1b) Internal and external escalation process 1c) Negotiation framework 2a) KPIs agreed and monitored for each contract 2b) Quality improvement committee collecting information from various data streams 2c) Direct feedback reports from secondary providers re trends 2c) Informal GP information sharing (e groups) 3a) Robust health market analysis tool in use 3B) CSU business intelligence support
SHA monitoring (All aspects) External arbitration process Integrated business report to Exec. Group and Gov. Body Quality improvement committee reporting to Exec. Group and Gov. Body SHA monitoring of AQP procurement
Contracts not signed off –heads of terms signed Timeliness of escalation process to embedded Resilience of CCG response to provider failure not tested
Non-specific gaps as follows : i) Lack of clarity around external audit and reporting arrangements for CCGs ii) Lack of clarity of future role of NCB in managing and influencing the system
Limited
Lack of contract
sign-off may impact on CCG ability to control
payment and performance
Significant
Data flows are established but
not yet embedded
No issues expected for
13/14 contracts
Overall rating
based on linked risks:
Sign-off
Moderate
Monitoring: Moderate/
Amber
Amber
Green

West Lancashire CCG Board Assurance Framework Update 3 – August 2013 Page 7 of 13
GB
Lead
Critical Outcome
Key Controls
Assurance on controls
Board Reporting Mitigation
OP
Lead
Principle areas
of risk Gaps in control
Gaps in assurance
Level of
assurance
Link to Risk
Register
Status
Gov. Body Lead
Operational
Lead
The possible
outcome should risks not be controlled
These are the specific
areas where failure will risk a critical
outcome
Processes and plans in place or actions being taken to mitigate risk in
principle areas
Internal or
external reporting arrangements that provide assurance to the Board that
controls are effective
Areas where controls are
not in place or are ineffective
Areas of
insufficient evidence to assure the Board that
controls are being effective
Must state either
None Limited
Significant Full
Colour
indicates current level
of risk (based on risk score)
Colour indicates current
status of principle risk area Red = off Track
Amber = On Track Green = Completed
PK
Paul
Jones
Failure of operational systems
1. Not balancing the books 2. Poor finance information – New IT systems not delivering - new national finance ledger 3. Poor activity and quality info – unknown performance, failing services or poor patient experience 4. Lack of people/capacity in system to provide the robust information
1a) Robust financial controls (ledger) and budget setting 1b) Some budget holders assigned 1c) Mitigation arrangements in place between CCGs 1d) Budget allocation agreed by DoH 2a) National financial ledger system in place (by 31/03/13) 2b) Comprehensive financial plan in place 3a) Established activity & performance monitoring for secondary care contracts 4a) CCG structure in place with CSU support element identified
SHA monitoring of financial performance currently via PCT Area Team monitoring role Dept. of Health NHS shared business services DoH /Private venture Robust internal validation of data
Still uncertainty around budget allocation and assignment but resolution expected following re-examination by GP and C&SR PCTs Detailed analysis of budget allocation across services not yet complete Limited activity info for community block contracts (not a pressure for 13/14)
Future external monitoring of CCGs financial performance is unclear CSU SLA in place but the CSU embedded team is not yet established which my effect CCG capacity
Full
National system established. CCG performance overseen by area team
Limited
Budget allocation and assignment awaiting resolution
Full
New IT system is live Comprehensive financial plan in place
Permanent CSU support now in place for finance team
Overall rating
based on linked risks:
Moderate
Green
Amber
Green
Green
Green

West Lancashire CCG Board Assurance Framework Update 3 – August 2013 Page 8 of 13
GB
Lead
Critical Outcome
Key Controls
Assurance on controls
Board Reporting Mitigation
OP
Lead
Principle areas
of risk Gaps in control
Gaps in assurance
Level of
assurance
Link to Risk
Register
Status
Gov. Body Lead
Operational
Lead
The possible
outcome should risks not be controlled
These are the specific
areas where failure will risk a critical
outcome
Processes and plans in place or actions being taken to mitigate risk in
principle areas
Internal or
external reporting arrangements that provide assurance to the Board that
controls are effective
Areas where controls are
not in place or are ineffective
Areas of
insufficient evidence to assure the Board that
controls are being effective
Must state either
None Limited
Significant Full
Colour
indicates current level
of risk (based on risk score)
Colour indicates current
status of principle risk area Red = off Track
Amber = On Track Green = Completed
Dr. JC
Katie
Wightman
Failure to achieve authorisation
1. Failure to achieve authorisation 2. Authorisation achieved but with restrictive conditions
1a) National authorisation template and process in place 1b) Lead officer appointed 1c) Currently proceeding to plan 2a) Notification of conditions received 2b) Response in draft for discussion with LAT
Regular monitoring by Exec. Group and Gov. body LAT acting on behalf of NCB to oversee process Seeking LAT support for CCG response to conditions
CCG not lead commissioner
(CCG not the accountable body in relation to some aspects of the conditions)
Full
Full
Green
Green
Green

West Lancashire CCG Risk Register Update 4 - August 2013 9
Appendix 2 West Lancashire CCG Risk Register
No. Lead Description Controls Score Risk Action Plan (AP) Updates Status
of AP Residual risk
Link to BAF C L R A G
1 BAF Theme:
Operational
Systems
KW
The Central Support Unit (CSU) do not the have the capacity /capability to ensure the CCG can fulfill statutory duties
i) Regular discussion with CSU regarding the ongoing position ii) CSU seeking specialist advice to address gaps in service offer ii) CCG have contracted specialist support directly in short term
3
1
3
Continue to manage on a week by week basis during transition Maintain contract for specialist cover in the interim Development of suite of policies. Inspections completed and reported to Audit Committee. No significant issues
Regular liaison with CSU maintained. Interim specialist staff recruited by CSU for health and safety, fire and risk management. Robust CSU support now in place Development of suite of policies nearing completion
Low
2
BAF Theme:
Op Systems
JW
Impact of shortfall in recruitment to the CSU in terms of specific support posts
i)Good liaison with CSU regarding gaps in recruitment
3
1
3
Continue to manage on a week by week basis When vacancies arise any short term pressures are covered
Embedded team is now fully established and residual issues regarding hub functions are resolved
Low
3
BAF Theme:
Contracts/ Delivery
JW
The business intelligence information provided by the CSU is insufficient for the CCG to make informed decisions.
i) Working closely with CSU to clarify CCG business intelligence needs ii) Recruitment process is complete
3
3
9
Clarification and agreement of specific information requirements of the CCG remain unresolved Continue ongoing development of data sets
Continuing to press with regard to the business intelligence needs of the CCG
Low/ Moderate
Status Key: Green – Complete Amber – On track Red - Off target

West Lancashire CCG Risk Register Update 4 - August 2013 10
No. Lead Description Controls Score Risk Action Plan (AP) Updates Status
of AP Residual risk
Link to BAF C L R A G
4 BAF Theme:
OP Systems/ Engagement
KW
Limited GP capacity to the CCG results in increased management costs and/or limited involvement in local meetings and groups
i) Specific GP portfolios supported by CCG managers ii) Planning of GP engagements to ensure maximum benefit for CCG
3
2
6
Planned improvements to communications pathways to improve efficiency, Ongoing development of engagement strategy will target better use of GP capacity Continue watching brief
Refreshed communication and engagement strategy approved at May governing body. Additional clinical input through prescribing committee Status remains satisfactory
Low/ Moderate
5
BAF Theme:
Contracts/ Delivery
PJ
Financial shortfall possible due to: i) Reduction in allocation following redefinition of specialised services may compromise ability to meet contract costs ii) Disaggregation of budgets from CLPCT
i) Ongoing verbal assurances regarding the system wide allocation issues ii) Agreement with Chorley and Gtr. Preston CCGs regarding reallocation of resources
4
2
8
Regular dialogue and updates on a weekly basis Continue to scrutinize allocations to ensure sufficient and equitable allocation of resources
Satisfactory resolution expected following further examination. Status reduced from significant to moderate
Moderate
6
BAF Theme:
OP Systems
PJ
Limit on running costs resulting in lack of flexibility to manage staff shortages
i) Establishment is considered appropriate to meet current needs ii) Staff encouraged to work flexibly to ensure adequate cover
3
2
6
Regular monitoring of staffing levels and capacity Examine development of matrix working to mitigate impact of staff shortages Continue watching brief
Finance team fully established No current pressures status remains satisfactory
Moderate

West Lancashire CCG Risk Register Update 4 - August 2013 11
No. Lead Description Controls Score Risk Action Plan (AP) Updates Status
of AP Residual risk
Link to BAF C L R A G
7 BAF Theme:
Delivery
JM
Unclear process for demonstrating redistribution of resource as a result of redesign/efficiency savings (QIPP)
i) Current QIPP programme regularly monitored and updated ii) Regular review by Exec Committee
3
3
9
Cross reference QIPP programme to redesign programme Continuously refresh assumptions around QIPP programme outcomes
Cross reference process is complete but still looking to influence and improve.
Moderate/ Significant
8
BAF Theme:
Engagement
LC
Lack of understanding and consistency between partners regarding outcomes of specific schemes
i)Strategic Partnership board ii) Regular dialogue with Southport & Formby ii) ‘In attendance’ place for LCC at Governing Board
4
2
8
Joint planning for integrated care pathway group Adoption of a programme management approach to include key partners.
ICPGs have commenced. CCG continues to monitor No change to action plan at this time
Moderate
9
BAF Theme:
Engagement
LC
Ongoing pressure from MPs and interested parties to provide information
i) Regular meetings with local MP ii) Ensuring staff are aware of the importance of briefing MPs and elected members about large scale changes
3
2
6
Improving dialogue and providing training/information for elected members Improving staff awareness of working in a democratic environment
Relationship with local MPs remains positive Continue watching brief
Moderate
West Lancashire CCG Risk Register Update 4 - August 2013 12
No. Lead Description Controls Score Risk Action Plan (AP) Updates Status
of AP Residual risk
Link to BAF C L R A G
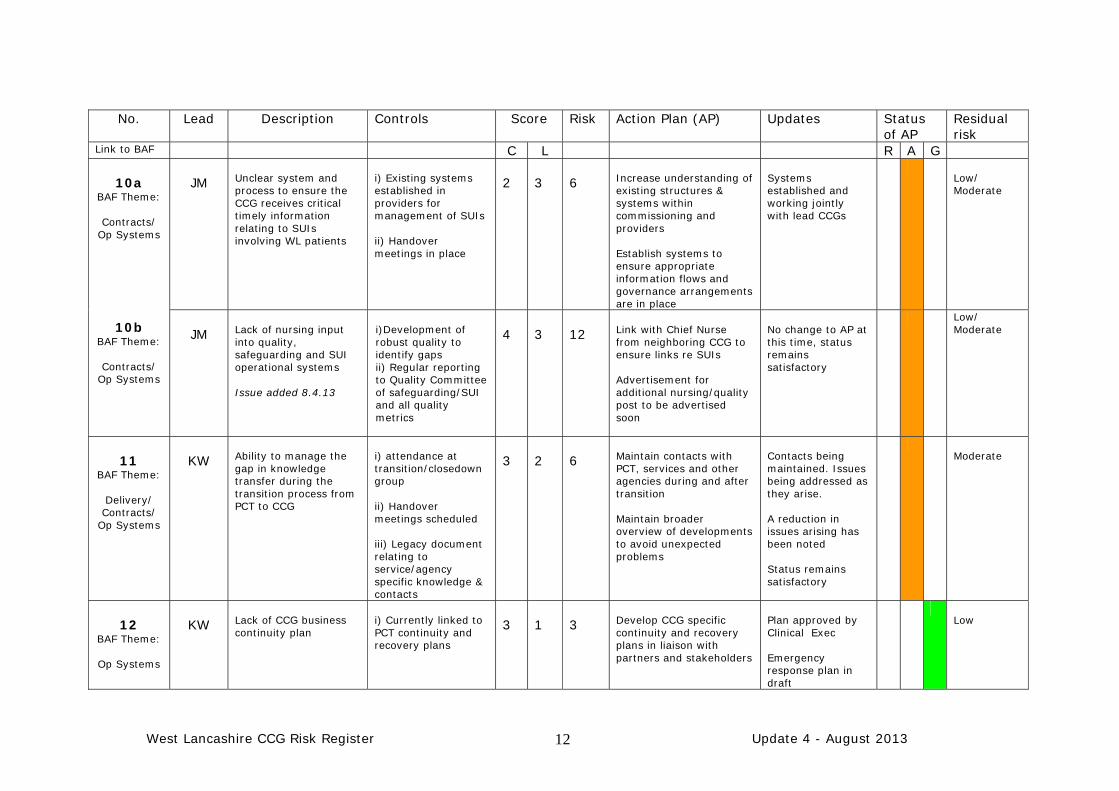
10a BAF Theme:
Contracts/
Op Systems
10b BAF Theme:
Contracts/
Op Systems
JM
Unclear system and process to ensure the CCG receives critical timely information relating to SUIs involving WL patients
i) Existing systems established in providers for management of SUIs ii) Handover meetings in place
2
3
6
Increase understanding of existing structures & systems within commissioning and providers Establish systems to ensure appropriate information flows and governance arrangements are in place
Systems established and working jointly with lead CCGs
Low/ Moderate
JM
Lack of nursing input into quality, safeguarding and SUI operational systems Issue added 8.4.13
i)Development of robust quality to identify gaps ii) Regular reporting to Quality Committee of safeguarding/SUI and all quality metrics
4
3
12
Link with Chief Nurse from neighboring CCG to ensure links re SUIs Advertisement for additional nursing/quality post to be advertised soon
No change to AP at this time, status remains satisfactory
Low/ Moderate
11
BAF Theme:
Delivery/ Contracts/
Op Systems
KW
Ability to manage the gap in knowledge transfer during the transition process from PCT to CCG
i) attendance at transition/closedown group ii) Handover meetings scheduled iii) Legacy document relating to service/agency specific knowledge & contacts
3
2
6
Maintain contacts with PCT, services and other agencies during and after transition Maintain broader overview of developments to avoid unexpected problems
Contacts being maintained. Issues being addressed as they arise. A reduction in issues arising has been noted Status remains satisfactory
Moderate
12
BAF Theme:
Op Systems
KW
Lack of CCG business continuity plan
i) Currently linked to PCT continuity and recovery plans
3
1
3
Develop CCG specific continuity and recovery plans in liaison with partners and stakeholders
Plan approved by Clinical Exec Emergency response plan in draft
Low

West Lancashire CCG Risk Register Update 4 - August 2013 13
No. Lead Description Controls Score Risk Action Plan (AP) Updates Status
of AP Residual risk
Link to BAF C L R A G
13 BAF Theme:
Contracts/ Delivery/
Engagement
JW
Managing the demands of the Local Area Team (LAT) regarding the performance of CCG contracted services
i) Established links with LAT ii) Agreement with LAT regarding CCG Annual Plan
2
4
8
Develop open culture with LAT regarding performance issues Ensure strong links with other CCGs is maintained
Examining specifics around areas such as quality in primary care Status remains satisfactory
Moderate
14
BAF Theme:
Contracts/ Delivery
JW
Possible breaks in continuity of contracted services during and post transition
i) Comprehensive database of contracts in place ii) PCT support to ensure all contracts are handed over to plan
3
1
3
Ongoing verification of data relating to all contracts during transition
All contracts now in place and any transition issues resolved
Low
15
BAF Theme:
Contracts/ Delivery
JW
Inherited risk from PCT- Lack of governance in the Brief Therapy Support Services.
i) Issues being investigated by former CL PCT CCGs
3
1
3
CCG have fully investigated the issues.
Any issues have been resolved and sound governance arrangements are in place
Low

Integrated Business Report – September 2013 West Lancashire Clinical Commissioning Group Governing Body meeting – 24 September 2013
Agenda item no: WLCCGB 9/13/08
WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERING BODY REPORT
DATE OF BOARD MEETING: 24 September 2013 TITLE OF REPORT: Integrated Business Report BRIEFING POINTS: This report provides summary information on the financial
and activity performance of West Lancashire Clinical Commissioning Group for July 2013 and a financial position for August 2013. Quality and performance analysis is also provided for community based targets and for the Southport and Ormskirk Hospitals.
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact Yes
The report outlines quality and performance issues relevant to the CCG and describes key actions to address these.
2. Commissioning of hospital and community services – please outline impact
Yes
The report includes financial and activity information in relation to commissioned services and highlights areas of risk and actions.
3. Commissioning and performance management of GP Prescribing – please outline impact
No
4. Delivering Financial Balance – please outline impact Yes The report summarises the financial position of the CCG and highlights areas of financial risk.
5. Development of the commissioning group as a commissioning organisation – please outline impact
Yes
This report will support the CCG in developing clear and credible plans. B. Governance – please outline impact 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework
have any legal implications promote effective governance practice
Yes
Links to financial risks. 2. Additional resource implications
(either financial or staffing resources) No
3. Health Inequalities Yes Links to health outcomes framework (all five domains) 4. Human Rights, Equality and Diversity Requirements No 5. Clinical Engagement No 6. Patient and Public Engagement No REPORT PREPARED BY: Paul Kingan, Chief Finance Officer

2 | P a g e
West Lancashire Clinical Commissioning Group
Integrated Business Report
September 2013

3 | P a g e
TABLE OF CONTENTS
1 Executive Summary 32 Financial Position 43 Planned Care: Referrals 64 Planned Care: Acute Contract 75 Unplanned Care: Acute Contract 96 Lancashire Care Foundation Trust (LCFT) Activity 107 Quality and Performance
a West Lancashire CCG Performance Dashboard 11
b Southport & Ormskirk hospitals NHS Trust Urgent Care Performance Dashboard 14
c Southport & Ormskirk Hospitals NHS Trust Planned Care Performance Dashboard 15d e f g
Southport & Ormskirk Hospitals NHS Trust Trust Wide Performance Dashboard Areas of Under‐Performance Early Warnings & Future Performance CCG Outcome Indicator Set
16171819
h Alternative Quality Contract metrics 20
i j k l
NHS England summary quality report June 2013 Friends and family inpatients Friends and family A&E Trust level narrative summaries to be completed from next month
21232323
8 Complaints a West Lancashire Complaints 24
b GP Issues with Southport & Ormskirk Hospitals Trust 25
c
Southport and Ormskirk Compliments and Complaints
25
9 Serious and Untoward Incident reporting a New Incidents in August 26
b On‐going investigations 26
NB: CAVEAT TO THIS REPORT
As contracts have not yet been signed for all providers, in some cases actual activity has been used as a proxy for plans in the absence of a supplied plan. Not all quality and performance information is available on a West Lancashire footprint. There are national issues with access to CCG level data by Commissioning Support Units which is delaying reporting to Clinical Commissioning Groups. Data has been provided at this level where available and Southport and Ormskirk Hospital Trust level data is used where not. Given only data to July is available at present, it would not be prudent to forecast year‐end

4 | P a g e
performance from financial and activity trends. Financial figures presented show a small underspend position.
1. Executive Summary
This report provides summary information on the financial and activity performance of West Lancashire Clinical Commissioning Group to July 2013 and a financial position for August 2013. Quality and performance analysis is also provided for community based targets and for the Southport and Ormskirk Hospitals NHS Trust.
OVERALL POSITION Footprint
PCT delivery of financial duties CCG
CCG forecast CCG
DEMAND
GP referrals CCG
Other referrals CCG
PLANNED CARE
Finance
Total planned care PBR CCG
Key performance concerns
Cancer screening 62 day to treatment S&O
Cancer 31 days ‐ surgery S&O
Cancer 14 day – breast cancer S&O
Elective Length of Stay (LoS) S&O
UNPLANNED CARE
Finance
Total unplanned care PBR CCG
Key performance concerns
A&E 4 hour target S&O
30 Day readmissions CCG
Non‐elective Length of Stay (LoS) S&O
S&O Trust Wide
Key performance concerns
Ambulance responses within 8 mins CCG
Sickness Absence S&O
Key information from this report
NHS West Lancashire CCG As at August the CCG is forecasting a surplus of £1.431m, including a 1% surplus (£1.374m) as required by NHS England. There has been a 3.5% decrease in GP referrals compared to July 2012. Indicative performance to the end of July 2013 against the planned care element of the contract is under plan by £142K. The performance over the same period against the planned care element of the Southport and Ormskirk contract is under plan by £92k. Indicative performance for July against the unplanned care element of the contract is under plan by £181K. Unplanned care performance for July against the Southport and Ormskirk Hospital contract is under plan by £149K.
Southport & Ormskirk Hospital Trust 4 hour targets in A&E were achieved by S&O. Provisional August data also suggests that the Trust will remain compliant. LTH is also meeting the target and YTD figures for both Trusts are currently Amber. Cancer 31 day surgery underperformance represents 1 urology breach where a patient wanted to wait until after a holiday, therefore this breach is due to patient choice. Data for 62day cancer treatment data is not available from S&O. Cancer 14 day symptomatic breast referrals are red and S&O report this as due to patient initiated delays. Planned changes include a patient leaflet, changes to booking script and Patient Access Centre (PAC) audit. Sickness Absence at S&O is red however this has improved month on month since April and the implementation of a Staff Health and Wellbeing team. Elective and non‐elective length of stay are higher than target for S&O. All Consultants have been tasked with carrying out ward rounds to ensure patients are reviewed and other staff are fully supported to manage patients. A discharge group meets regularly to review discharge processes.
The CCG footprint is performing poorly against the target to reduce readmissions within 30 days, the metric has consistently been reported as red this year but performance is deteriorating. Further analysis is being undertaken to establish trusts / specialties contributing to this performance and to build patient profiles to ensure targeted solutions.

5 | P a g e
2. Financial Position
The following table summarises the financial position for West Lancashire CCG at Month 5 2013/14.
Table 1
As at Month 5 the CCG has a year to date underspend of £602k, which is forecast to increase to £1.431m
by the end of the financial year. This forecast position includes the delivery of a 1% surplus (£1.374m) as
required by NHS England.
Annual Year to Date Forecast
Budget Variance Variance
£000 £000 £000
Resources
Allocation ‐ Commissioning (134,746) 0 0
Allocation ‐ Running Costs (2,680) 0 0
Return of 2012‐13 Surplus (1,262) 0 0
Total Resources (138,688) 0 0
Expenditure ‐ Commissioned Services
Acute Services 77,137 0 0
Mental Health Services 12,734 0 0
Community Health Services 10,264 (19) (45)
Continuing Care 4,991 0 0
Funded Nursing Care 988 4 9
Local Authority / Joint Services 691 0 0
Prescribing 18,101 0 0
Enhanced Services 746 0 0
Out of Hours 931 0 0
Other Primary Care Services 1,514 0 0
Other Programme Services 520 0 0
Sub Total Commissioned Services 128,617 (15) (36)
Expenditure ‐ Corporate Budgets
Running Costs 2,680 (14) (21)
GP IT 525 0 0
Other Corporate Costs 2,148 0 0
Non Recurrent Headroom 1,350 0 0
Contingency 1,275 0 0
Reserves 719 0 0
Sub Total Corporate Budgets 8,697 (14) (21)
Total Expenditure 137,314 (29) (57)
Planned Surplus (1%) 1,374 (573) (1,374)
Total CCG (Surplus)/Deficit 0 (602) (1,431)
NHS West Lancashire CCG
Financial Position as at Month 5 2013/14

6 | P a g e
Key points to note are:
Acute Services – Month 4 activity monitoring information is showing only minor variations from
Plan. As such a break even position is stated. Risk within the CCG’s largest contract, Southport &
Ormskirk NHS Trust is contained within a cost‐certainty arrangement.
Mental Health Services – The CCG has a block contract with its main provider, Lancashire Care
Foundation Trust to control financial risk.
Funded Nursing Care – Information for the period April to August indicates that these weekly
payments to Nursing Homes are slightly in excess of budgeted levels.
Corporate Services – There were 2 vacant posts (now filled) within the CCG’s structure,
generating a small underspend against budget.
There are significant financial risks to the CCG that are not included in the above position, these are
detailed below:
Table 2
The above table clealy demonstrates that the single biggest risk to the CCG’s financial position is the
failure to satisfactorily resolve ongoing uncertainty on allocations, with regard to both Specialised
Services and the split of resources relating to the former Central Lancashire PCT between the three
successor CCGs.
The CCG could deploy its Contingency and Non‐Recurrent funding to mitigate this potential shortfall but
as a consequence this funding would be unavailable to invest in healthcare services for West Lancashire.
Risk
Full value of
risk
£'000s
Risk
assessment
(%)
Potential
value of
risk
£'000s Commentary
Acute Services 993 25% 248Main acute contract covered by cost certainty arrangement. Risk relates
to 5% overperformance with other providers.
Continuing Care/High Cost Packages 149 50% 75 Risk that activity increases by 12% pa (instead of planned 9.6%)
QIPP Under‐Delivery 632 50% 316 Risk of non‐delivery/delayed delivery of QIPP schemes
Prescribing 890 25% 223 Impact of a 5% variance
Specialised Commissioning ‐ impact of
allocation error remaining uncorrected6,800 20% 1,360
Assumption that there will be a system wide solution to the issue,
including recurrent resolution
Split of former C Lancs PCT ‐ impact of
allocation error remaining uncorrected1,200 50% 600
Discussions ongoing with other CCGs; this issue is not mutually
exclusive from the Specialised Commissioning error.
TOTAL RISKS 10,664 2,822
Potential mitigations
Full value of
mitigating
action
£'000s
Probability
of success
%
Expected
value of
mitigation
£'000s Commentary
Contingency Held 1,275 100% 1,275 1% contingency set aside by the CCG could be deployed to partially
offset the above risks.
Non‐recurrent measures 1,547 100% 1,547
Utilise a proportion of the 2% headroom to balance the position. LAT not
authorising spending plans (including AQC with S&O) until allocations
issues resolved
TOTAL MITIGATION 2,822 2,822
NET RISK / HEADROOM (7,842) ‐

7 | P a g e
3. Planned Care: Referrals
The following section provides an overview of referrals to secondary care to July 2013.
Chart A (below) shows the number of GP and ‘other’ referrals for the CCG across all providers. There has
been a 3.5% decrease in GP referrals compared to July 2012.
Chart A: Referrals May 2013 to March 2014 Compared to 2012/13.
Referrals from ‘other’ sources have increased (by 165) to trauma and orthopaedics, however this is likely to be due to referrals to Southport and Ormskirk being triaged via the Musculoskeletal Clinical Assessment Service (MCAS), as over the same period GP referrals to trauma and orthopaedics have reduced by 19%. There has been a 136% increase (15) in GP referrals to Plastic Surgery to date year on year. Referrals to Plastic Surgery are small and therefore variation month on month would be expected. However referrals year to date have been higher than mean average, and at the upper control limit for the dataset in June 2013 as depicted in chart B. The suggestion is that most of the extra referrals are to Ramsey Healthcare. Chart B: GP Referrals to Plastic Surgery Apr 12 to July 13.
‐10
‐5
0
5
10
15
Apr‐12
May‐12
Jun‐12
Jul‐12
Aug‐12
Sep‐12
Oct‐12
Nov‐12
Dec‐12
Jan‐13
Feb‐13
Mar‐13
Apr‐13
May‐13
Jun‐13
Jul‐13
Number
Plastic Surgery Referrals
GP Referrals mean LCL UCL

8 | P a g e
4. Planned Care: Acute Contract
All providers
Performance to month 04 against the planned care element of the contract is shown below in table 2a.
This shows the planned care element of the contract is under plan by £142k.
It should be noted that for some providers actual activity has been used as a proxy for plans in the
absence of a supplied plan.
Table 2a: Month 04 Planned Care – All Providers
Southport and Ormskirk Hospitals NHS Trust
Performance to month 04 against the planned care element of the contract is shown below in table 2b.
This shows the planned care element of the contract is under plan by £92k. For elective admissions there
are no HRGs with significant performance issues.
Table 2b: Month 04 Planned Care at Southport and Ormskirk Hospitals
Plan Actual Variance Plan Actual VarianceDaycase 4359 4357 -2 £2,827,335 £2,756,953 -£70,382Elective 762 774 12 £2,065,855 £2,121,552 £55,697Elective Excess Beddays 205 267 62 £49,171 £63,594 £14,423LTH Assessment and Treatment Centre 5 4 -1 £1,472 £1,122 -£350Outpatient First Attendance 9483 9701 218 £1,394,887 £1,424,859 £29,972
Outpatient Follow-Up Attendance 22175 21245 -930 £1,915,596 £1,749,726 -£165,870
Outpatient Procedure 5374 5447 73 £906,682 £900,815 -£5,867Outpatient Non Face to Face Consultation 169 396 227 £5,480 £5,565 £85Grand Total 42,531 42,191 -340 £9,166,480 £9,024,186 -£142,293
Point of DeliveryActivity 2013/14 Cost 2013/14
Plan Actual Variance Plan Actual VarianceDaycase 3180 3258 78 £1,835,722 £1,776,546 -£59,176Elective 472 487 15 £1,225,086 £1,286,139 £61,053Elective Excess Beddays 47 109 62 £10,873 £24,973 £14,101Outpatient First Attendance 6686 6995 309 £1,019,982 £1,050,627 £30,645Outpatient Follow-Up Attendance 15045 14579 -466 £1,325,369 £1,200,776 -£124,593Outpatient Procedure 4067 4090 23 £677,215 £662,740 -£14,476Outpatient Non Face to Face Consultation 0 208 208 £0 £0 £0Grand Total 29,498 29,726 228 £6,094,246 £6,001,800 -£92,446
Point of DeliveryActivity 2013/14 Cost 2013/14

9 | P a g e
All Other Providers
Performance to month 04 against the planned care element of the contract is shown below in table 2c.
This shows the planned care element of the contract is under plan by £50k. It should be noted however
that contract monitoring information had not been received from the majority of Liverpool Trusts, and
that for providers such as Ramsay Healthcare UK where no plan has been supplied the plan has been set
to actuals to avoid a significant over performance.
Table 2c: Month 04 Planned Care at All other Providers.
Key Risks and Actions
Over performance in elective activity is reported at S&O, particularly in trauma and orthopaedics (T&O) with knee and hip replacements making up the largest part of this increase. General Surgery and T&O are also contributing to an increase in excess bed days. The T&O back log has been stabilised due to waiting time initiatives, however there are issues because the Consultants are specialists in different body areas and therefore it is not possible to pool work. There continues to be an issue with existing 18 weeks breaches creating a ‘backlog’ of patients waiting in excess of 18 weeks for treatment, consequently the elective workload will continue to increase until this backlog is cleared. Breast surgery first appointments are pushing outpatient 1st appointments above plan, as increases in breast surgery and ophthalmology are also causing follow‐up outpatient appointments to be above plan at Southport & Ormskirk. Breast surgery increases, result from the need to meet cancer two week wait and 62 days to treatment targets. Ophthalmology follow up appointments continue to present challenges due to the continuing demands of an aging population. A new consultant appointment is planned to create capacity to address this growth. However in the absence of other schemes our contract plan with Southport and Ormskirk may need to increase in 2014/15. The over performance at Lancashire Teaching Hospital and Aintree Hospitals is being investigated and we await further information.
Plan Actual Variance Plan Actual VarianceWrightington Wigan and Leigh 5621 4936 -685 £1,221,503 £1,166,989 -£54,514Ramsay Operations (UK) 2569 2569 0 £762,485 £762,485 £0Aintree University Hospitals 2382 2486 104 £515,350 £532,818 £17,468St Helens and Knowsley Hospitals 1258 1189 -69 £282,032 £253,413 -£28,619Lancashire Teaching Hospitals 843 913 70 £205,127 £221,994 £16,867
Other 359 372 13 £85,736 £84,687 -£1,049Grand Total 13,033 12,465 -568 £3,072,233 £3,022,386 -£49,847
ProviderActivity 2013/14 Cost 2013/14
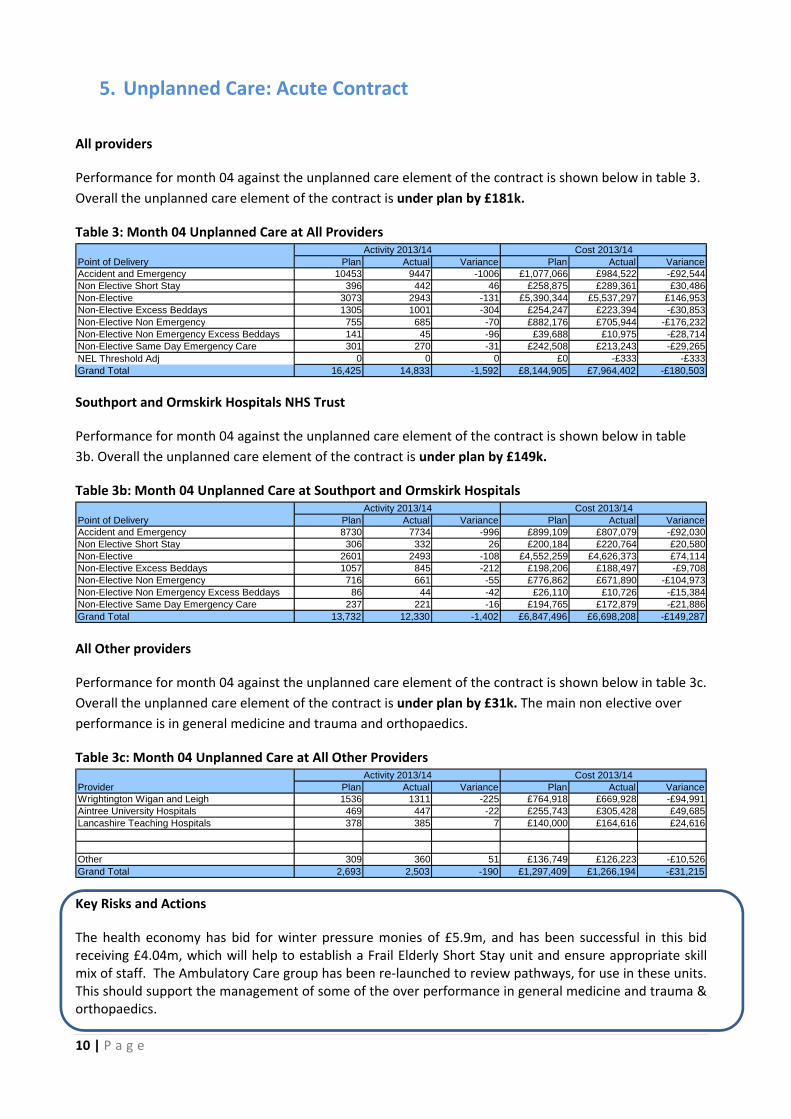
10 | P a g e
5. Unplanned Care: Acute Contract
All providers
Performance for month 04 against the unplanned care element of the contract is shown below in table 3.
Overall the unplanned care element of the contract is under plan by £181k.
Table 3: Month 04 Unplanned Care at All Providers
Southport and Ormskirk Hospitals NHS Trust
Performance for month 04 against the unplanned care element of the contract is shown below in table
3b. Overall the unplanned care element of the contract is under plan by £149k.
Table 3b: Month 04 Unplanned Care at Southport and Ormskirk Hospitals
All Other providers
Performance for month 04 against the unplanned care element of the contract is shown below in table 3c.
Overall the unplanned care element of the contract is under plan by £31k. The main non elective over
performance is in general medicine and trauma and orthopaedics.
Table 3c: Month 04 Unplanned Care at All Other Providers
Key Risks and Actions
The health economy has bid for winter pressure monies of £5.9m, and has been successful in this bid receiving £4.04m, which will help to establish a Frail Elderly Short Stay unit and ensure appropriate skill mix of staff. The Ambulatory Care group has been re‐launched to review pathways, for use in these units. This should support the management of some of the over performance in general medicine and trauma & orthopaedics.
Plan Actual Variance Plan Actual VarianceAccident and Emergency 10453 9447 -1006 £1,077,066 £984,522 -£92,544Non Elective Short Stay 396 442 46 £258,875 £289,361 £30,486Non-Elective 3073 2943 -131 £5,390,344 £5,537,297 £146,953Non-Elective Excess Beddays 1305 1001 -304 £254,247 £223,394 -£30,853Non-Elective Non Emergency 755 685 -70 £882,176 £705,944 -£176,232Non-Elective Non Emergency Excess Beddays 141 45 -96 £39,688 £10,975 -£28,714Non-Elective Same Day Emergency Care 301 270 -31 £242,508 £213,243 -£29,265NEL Threshold Adj 0 0 0 £0 -£333 -£333Grand Total 16,425 14,833 -1,592 £8,144,905 £7,964,402 -£180,503
Activity 2013/14 Cost 2013/14Point of Delivery
Plan Actual Variance Plan Actual VarianceAccident and Emergency 8730 7734 -996 £899,109 £807,079 -£92,030Non Elective Short Stay 306 332 26 £200,184 £220,764 £20,580Non-Elective 2601 2493 -108 £4,552,259 £4,626,373 £74,114Non-Elective Excess Beddays 1057 845 -212 £198,206 £188,497 -£9,708Non-Elective Non Emergency 716 661 -55 £776,862 £671,890 -£104,973Non-Elective Non Emergency Excess Beddays 86 44 -42 £26,110 £10,726 -£15,384Non-Elective Same Day Emergency Care 237 221 -16 £194,765 £172,879 -£21,886Grand Total 13,732 12,330 -1,402 £6,847,496 £6,698,208 -£149,287
Point of DeliveryActivity 2013/14 Cost 2013/14
Plan Actual Variance Plan Actual VarianceWrightington Wigan and Leigh 1536 1311 -225 £764,918 £669,928 -£94,991Aintree University Hospitals 469 447 -22 £255,743 £305,428 £49,685Lancashire Teaching Hospitals 378 385 7 £140,000 £164,616 £24,616
Other 309 360 51 £136,749 £126,223 -£10,526Grand Total 2,693 2,503 -190 £1,297,409 £1,266,194 -£31,215
ProviderActivity 2013/14 Cost 2013/14

11 | P a g e
6. Lancashire Care Foundation Trust Contract Activity
The contract value for Lancashire Care Foundation Trust (LCFT) mental health services is £9.7m. A brief summary of monthly and year‐to‐date activity will be reported through the IBR each month. Quality data will be included as it becomes available. The LCFT contract is for a range of mental health services such as rehabilitation, community mental health teams, hospital liaison, memory assessment, CAMHS and child psychology and prison in‐reach.
Apr‐13 May‐13 Jun‐13
Row Labels Activity Activity Activity Activity YTD
NHS WEST LANCASHIRE CCG 9792 10476 10109 11391 31558
Caseloads
Caseloads: Adult CMHT ‐ Referrals Received (External) 8 5 4 3 20
Caseloads: Adult Community Restart ‐ Referrals Received (Internal\External) 12 24 17 24 77
Caseloads: Criminal Justice Liaison ‐ Referrals Received (Internal\External) 14 14 40 23 91
Caseloads: Older Adults CMHT ‐ Referrals Received (External) 37 44 43 39 163
Caseloads: Older Adults Intermediate Support ‐ Referrals Received (Internal\External) 3 5 10 13 31
Caseloads: Recovery Team ‐ Referrals Received (Internal\External) 6 2 2 2 12
Caseloads: Referrals Received (External) 413 446 358 371 1588
Caseloads: Caseload at Month End 2378 2344 2365 2336 0
Caseloads: Older Adults CMHT – Caseload at Month End 151 155 159 148 0
Community
Community: Actualised Contacts 4972 5482 5289 6518 22261
Contacts
Contacts: Adult A & E Liaison 60 45 10 4 119
Contacts: Enhanced Memory Services (MAS) 437 374 316 376 1503
EIS
EIS: New EIS Patients in Year ‐ VSMR 5378 3 6 6 0
EIS: Unclustered EIS Patients not seen for 8 weeks ‐ VSMR 5379 2 1 1 1 5
EIS: Caseload at Month End ‐ VSMR 5319 37 40 41 41 0
Inpatients
Inpatients: Admissions for Adult,Older Adult and PICU Wards 19 18 19 19 75
Inpatients: Adult IP Wards – Admissions 15 16 15 18 64
Inpatients: Older Adult IP Wards – Admissions 3 1 4 1 9
Inpatients: PICU Wards – Admissions 1 1 2
Inpatients: Occupied Bed Days for Adult,Older Adult and PICU Wards 612 728 705 724 2769
Inpatients: Adult IP Wards – Occupied Bed Days 363 471 420 473 1727
Inpatients: Older Adult Wards – Occupied Bed Days 110 164 189 172 635
Inpatients: PICU Wards – Occupied Bed Days 139 93 96 79 407
Grand Total 9792 10476 10109 11391 31558
Jul‐13

12 | P a g e
7. Quality and Performance
A selection of indicators is set out below. The targets are drawn from both the NHS Operating Framework and local priorities. The first dashboard (table 5a) relates to
West Lancashire CCG data covering the experience of patients resident in the CCG footprint through all providers. Areas of under‐performance are then explored by
provider.
7a West Lancashire CCG Performance Dashboard
Q2
Jun Jul
RAG G A
Act ual 95.42% 91.78%
Target 93.00% 93.00%
RAG R A
Act ual 87.10% 90.91%
Target 93.00% 93.00%
RAG G G
Act ual 97.96% 100%
Target 96.00% 96.00%
RAG G G
Act ual 100% 100%
Target 94.00% 94.00%
G G
Act ual 100% 100%
Target 98.00% 98.00%
RAG G G
Act ual 100% 100%
Target 94.00% 94.00%
RAG G G
Act ual 90.48% 95.00%
Target 85.00% 85.00%
RAG
Act ual N/ A N/ A
Target 90.00% 90.00%
RAG G G
Act ual 100% 100%
Target 86.00% 86.00%
P H Q24: % P atients seen within two weeks fo r an urgent GP referral fo r suspected cancer
P H Q25: % o f pat ients seen within 2 weeks fo r an urgent referral fo r breast sympto ms
P H Q06: % o f pat ients receiving def init ive treatment within 1 mo nth o f a cancer diagno sis
P H Q07: % o f pat ients receiving subsequent treatment fo r cancer within 31 days (Surgery)
P H Q08: % o f pat ients receiving subsequent t reatment fo r cancer within 31 days (D rug T reatment)
P H Q09: % o f pat ients receiving subsequent t reatment fo r cancer within 31 days (R adio therapy)
P H Q03: % o f pat ients receiving 1st def init ive treatment fo r cancer within 2 mo nths (62 days)
P H Q05: % o f pat ients receiving treatment fo r cancer within 62 days upgrade their prio rity
G
G G
100.00% 100.00% 100.00%
86.00% 86.00% 86.00%
W Lancs CCG
G G
82.143% 90.36%
85.00% 85.00% 85.00%
G A G
Gaps in data indicate no pat ients required treatment.
N/ A 100.00% 100.00%
90.00% 90.00% 90.00%
W Lancs CCG
100.00% 100.00% 100.00%
94.00% 94.00% 94.00%
G G G
100.00%
G
98.00%
W Lancs CCG
G95.238% 100.00% 98.039%
98.00% 98.00%
A G
98.413% 98.53%
96.00%
G
100.00% 100.00% 100.00%
94.00% 94.00% 94.00%
G G
87.805% 98.077% 91.57%
93.00%
W Lancs CCG
96.00% 96.00%
R G A
G G
97.619%
95.359% 93.191% 93.82%
93.00% 93.00% 93.00%
G G G
Y T D
A p r M ay
M et r icR ep o rt ing
Level
2 0 13 - 2 0 14
T rend C omment sQ1
W Lancs CCG
W Lancs CCG
P revent ing P eo ple fro m D ying P rematurely
W Lancs CCG
C ancer Wait ing T imes
P H Q04: % o f pat ients receiving treatment fo r cancer within 62 days fro m an N H S C ancer Screening Service
W Lancs CCG
93.00% 93.00%
W Lancs CCG

13 | P a g e
Q2
Jun Jul
RAG G A A
Act ual 95.918% 94.27%
Target 95.00% 95.00%
RAG R R
Act ual 67.742% 44.83%
Target 75.00% 75.00%
RAG G G
Act ual 79.577% 75.45%
Target 75.00% 75.00%
RAG R R
Act ual 61.219% 71.55%
Target 75.00% 75.00%
RAG G G
Act ual 81.071% 77.88%
Target 75.00% 75.00%
RAG R R R
Act ual 10.7%
Target 5.6 5.6
RAG G G
Act ual 93.228% 92.21%
Target 90.00% 90.00%
RAG G G
Act ual 97.385% 97.45%
Target 95.00% 95.00%
Act ual 95.088% 95.53%
Target 92.00% 92.00%
RAG G G
Act ual 0 0
Target 0 0
RAG G G
Act ual 0.085% 0.15%
Target 1.00% 1.00%
61: R eferral to T reatment (A djusted A dmitted)
62: R eferral to T reatment (N o n-A dmitted)
P ercentage o f pat ients wait ing at perio d end (R T T ) fo r inco mplete pathways (C o mmissio ner)
1839: R eferral to T reatment - N o o f Inco mplete P athways Wait ing >52 weeks
P H Q22: % o f patients wait ing 6 weeks o r mo re fo r a diagno sic test
W Lancs CCG
W Lancs CCG
W Lancs CCG
P H Q02: C atego ry A calls respo nded to within 19 minutes
1887: C atego ry A C alls R espo nse T ime (R ed1) Category A (Red 1) calls resulting in an emergency response arriving at the scene of the incident within 8 minutes
1889: C atego ry A (R ed 2) 8 M inute R espo nse T ime Number of Category A (Red 2) calls resulting in an emergency response arriving at the scene of the incident within 8 minutes
M et r icR ep o rt ing
Level
2 0 13 - 2 0 14
T rend C omment sY T D
A p r M ay
75.601% 80.801% 81.071%
W Lancs CCG 0.953% 1.359% 0.15%
1.00% 1.00% 1.00%
G R G
0 0 0
0 0 0
G G G
92.00%
W Lancs CCG
RAG G
94.703% 95.007% 95.08%
92.00% 92.00%
G G G
97.05% 97.845% 97.418%
95.00% 95.00% 95.00%
G G G
92.42%
90.00% 90.00% 90.00%
G G G
G
R eferral to T reatment (R T T )
R
W Lancs CCG 7.72% 8.1 8.84%
5.65.65.6
H QU16: Emergency R e-admissio ns within 30 days o f discharge
Emergency R eadmissio ns
Only Lancashire f leet has electronic device for recording t imes. M ersey f leet uses paper records st ill.
62.791% 70.145% 66.30%
75.00% 75.00% 75.00%
R R R
W Lancs CCG
NWAS
G G
G R
W Lancs CCG
NWAS
75.00% 75.00% 75.00%
G
75.612% 77.729% 77.02%
75.00% 75.00% 75.00%
GG G
Only Lancashire f leet has electronic device for recording t imes. M ersey f leet uses paper records st ill.
61.765% 78.125% 63.49%
75.00% 75.00% 75.00%
R
W Lancs CCG 93.824% 96.021% 94.98%
95.00% 95.00% 95.00%
A G
Q1
A mbulance
91.969% 92.296%
Enhancing Quality o f Life fo r P eo ple with Lo ng T erm C o ndit io ns
Lancs fleet are using electronic data capture
to record response times, Mersey fleet uses
paper records. Paper method can cause
slight delay in time keeping and may be
more prone to inaccuracy.

14 | P a g e
Q2
Jun Jul
RAG G
YTD 0
Target 0.00 0.00
RAG
YTD 2.00
Target
RAG G G
Act ual 97.057% 96.00%
Target 95.00% 95.00%
RAG G G
Act ual 95.91% 97.40%
Target 95.00% 95.00%
RAG G G
YTD 3,216 4,354
Target 3,341 4,390
RAG G G
YTD 677 926
Target 3,962 5,413
T'Hold 3,884
RAG R G G
YTD 8,612 11,573
Target 8,608 11,640
Q1
P H S10_02: A ll f irst o utpatient at tendances (co nsultant- led) in general and acute specialt ies
P H Q27: N umber o f M R SA B acteraemias
P H Q28: N umber o f C .D if f ic ile infect io ns
P H Q23: 4-H o ur A &E Wait ing T ime T arget (M o nthly / P ro vider)
P H S06_02: N umber o f G&A no n-elective F F C Es in the perio d
A ct iv ity
Lancs T Hospitals
W Lancs CCG
W Lancs CCG
G G
2,876 5,870 11,573
2,737 5,883 11,640
R G
W Lancs CCG
244 476 926
1,258 2,709 5,413
G G G
1,107 2,192 4,354
1,109 2,203 4,390
G
1,233 2,656 3,884
W Lancs CCG
89.16% 97.169% 94.63%
95.00% 95.00% 95.00%
R G A
S & O Hospitals
A ctivity
A ccident & Emergency
88.145% 95.212% 94.95%
95.00% 95.00% 95.00%
R G A
A p r M ay
1.00 2.00 2.00
0.00 0.00 0.00
0.00 0.00 0.00
H C A I
G G G
W Lancs CCG
Y T D
P H S11_04: N umber o f G&A elect ive o rdinary admissio n F F C Es in the perio d
T reat ing and C aring fo r P eo ple in a Safe Enviro nment and P ro tect them fro m A vo idable H arm
M et r icR ep o rt ing
Level
2 0 13 - 2 0 14
T rend C omment s

15 | P a g e
7b Southport & Ormskirk Hospitals NHS Trust Urgent Care Performance Dashboard
Subject Q prem Indicator Description Data Jul‐12 Aug‐12 Sep‐12 Oct‐12 Nov‐12 Dec‐12 Jan‐13 Feb‐13 Mar‐13 Apr‐13 May‐13 Jun‐13 Jul‐13Target
2013‐14
Urgent care
Target 15 15 15 15 15 15 15 15 15 15 15 15 15
Month Actual 8 8 9 9 10 9 8 8 7 7 5 6 5
Month RAG G G G G G G G G G G G G G
Target 60 60 60 60 60 60 60 60 60 60 60 60 60
Month Actual 43 43 43 42 40 50 41 47 48 49 41 42 44
Month RAG G G G G G G G G G G G G G
Target 240 240 240 240 240 240 240 240 240 240 240 240 240
Month Actual 238 238 239 240 240 271 337 240 311 390 238 295 239
Month RAG G G G G G R R G R R G R G
Target YTD 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0%
YTD Actual 96.81% 97.18% 95.96% 95.23% 95.54% 94.60% 91.84% 95.06% 93.06% 90.28% 97.26% 93.38% 96.12%
YTD RAG G G G G G G R G R R G R G
Month Actual 2.3% 2.6% 2.8% 2.7% 2.06% 2.8% 2.2% 2.2% 2.6% 2.3% 2.1% 2.1% 2.1%
Target YTD 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 2.6% 2.8%
YTD RAG G G G G G G G G G G G G G
Target 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0% 5.0%
Month Actual 4.11% 3.77% 3.25% 3.85% 3.64% 3.22% 3.5% 3.0% 3.5% 3.0% 3.0% 3.0% 2.8%
Month RAG G G G G G G G G G G G G G
Month Actual 1.20% 0.59% 0.93% 0.46% 0.72% 0.81% 1.17% 0.89% 1.19% 1.58% 0.00%
Target YTD 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.80% 0.80% N/A 0.00% N/A
YTD Actual 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80%
YTD RAG A G A G G R R R R R G
Target 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Month Actual 78.3% 96.4% 92.0% 92.1% 82.9% 78.3% 91.4% 79.3% 79.2% 82.1% 87.5% 82.6% 81.5%
Month RAG A G G G G A G A A G G G G
Target 60% 60% 60% 60% 60% 60% 60% 60% 60% 60% 60% 60% 60%
Month Actual 63.6% 60.0% 70.0% 81.8% 71.4% 75.0% 60.0% 66.7% 60.0% 60.0% 57.1% 44.4% 66.0%
Month RAG G G G G G G G G G G A R G
Target YTD 0 0 0 0 0 0 0 0 0 0 0 0 0
Month Actual 0 0 0 10 0 0 0 0 0 0 0 0 0
YTD Actual 0 0 0 10 10 10 10 10 10 0 0 0 0
YTD RAG G G G R G G G G G G G G G
Month Actual 0 0 0 0 0 0 0 0 0 0 0 0 0
Target YTD 1 2 2 2 2 3 3 3 3 0 0 0 0
YTD Actual 0 0 0 0 0 0 0 0 0 0 0 0 0
YTD RAG G G G G G G G G G G G G G
Month Actual #REF! 0 5 0 1 0 5 2 4 1 1 2 4
Target YTD 10 12 14 17 19 22 25 28 30 1.58 19 19 19
YTD Actual 5 5 10 10 11 11 16 18 22 1 2 2 4
YTD RAG G G G G G G G G G G G G G
HCAI
YesPHQ27: Number of MRSA
Bacteraemias0
YesPHQ28: Number of C. Difficile
infections19
60.0%
EMSA
PHQ26: Mixed Sex
Accommodation ‐ Numbers of
unjustified breaches
Yes 0
Stroke
SQU06: % stroke patients
spending 90%+ time on a
stroke unit
80%
SQU06: % TIA (mini stroke)
patients assessed and treated
<> 24 hrs
5.0%
Cancellations YesCancellations: % for non
clinical reasons 0.80%
HQU11: Patient Impact: Left
department without being
seen rate
5.0%
Yes Timeliness: A&E 4 Hour Target 95.0%
HQU10: Timeliness: total time
spent in A&E department ‐
95th centile –
240
15
HQU13:Timeliness: Time to
treatment in department –
median
60
Accident and
emergency
targets
HQU12: Timeliness: Time to
initial assessment ‐ 95th
centile (arrival by ambulance)
HQU09: Patient Impact:
unplanned re‐attendance at
A&E within 7 days of original

16 | P a g e
7c Southport & Ormskirk Hospitals NHS Trust Planned Care Performance Dashboard
Subject Q prem Indicator Description Data Jul‐12 Aug‐12 Sep‐12 Oct‐12 Nov‐12 Dec‐12 Jan‐13 Feb‐13 Mar‐13 Apr‐13 May‐13 Jun‐13 Jul‐13Target
2013‐14
Planned care
Target 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0%
Month Actual 93.4% 92.4% 91.2% 91.5% 86.5% 85.6% 83.1% 78.4% 90.9% 91.0% 90.9% 90.4% 90.7%
Month RAG G G G G R R R R G G G G G
Target 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0%
Month Actual 97.3% 97.9% 97.6% 97.9% 97.4% 96.6% 95.5% 95.7% 97.1% 96.6% 97.7% 97.5% 96.7%
Month RAG G G G G G G G G G G G G G
Target 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0%
Month Actual 94.1% 92.6% 92.2% 92.7% 94.2% 92.0% 92.9% 93.6% 93.2% 94.1% 94.4% 94.2% 94.5%
Month RAG G G G G G G G G G G G G G
Target 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0%
Month Actual 93.7% 92.0% 91.9% 95.5% 93.7% 94.4% 93.8% 94.3% 95.2% 94.5% 91.7% 94.5% N/A
Month RAG G A A G G G G G G G A G
Target 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0%
Month Actual 97.4% 98.2% 98.4% 95.7% 91.3% 95.2% 95.8% 87.5% 96.0% 86.0% 93.5% 84.1% N/A
Month RAG G G G G A G G R G R G R
Target 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0%
Month Actual 98.8% 98.6% 98.7% 97.6% 100.0% 100.0% 98.6% 100.0% 98.5% 97.1% 98.7% 96.2% N/A
Month RAG G G G G G G G G G G G G
Target 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0%
Month Actual 86.7% 100.0% 88.2% 93.8% 100.0% 100.0% 92.3% 100.0% 90.9% 100.0% 100.0% 87.5% N/A
Month RAG R G R A G G A G A G G R
Target 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0%
Month Actual 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% N/A
Month RAG G G G G G G G G G G G G
Target 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0%
Month Actual 79.4% 88.0% 83.6% 89.2% 83.6% 92.2% 90.4% 83.3% 84.6% 90.5% 79.6% 90.4% N/A
Month RAG R G A G A G G A A G R G
Target 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0%
Month Actual 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 50.0% 100.0% N/A N/A
Month RAG G G G G G G G G G R G
PHQ06: 1 month (subsequent
anti‐cancer drug regime)Yes 98.0%
PHQ03: 62 days (first definitive
treatment from Cancer
Screening Service)
Yes 90.0%
PHQ03: 62 days (first definitive
treatment from urgent GP
referral)
Yes
PHQ24: 2 weeks (urgent
referral breast symptoms) Yes 93.0%
PHQ06: 1 month (subsequent
surgery for cancer)Yes 94.0%
Cancer waiting
times
PHQ24: 2 weeks (urgent GP
referral) Yes 93.0%
PHQ06: 1 month (definitive
treatment of cancer diagnosis)Yes 96.0%
85.0%
92.0%PHQ21: RTT ‐
IncompleteTargetYes
95.0%PHQ20: RTT ‐ Non Admitted
TargetYes
90.0%PHQ19:RTT ‐ Admitted TargetYes
RTT ‐ 18 weeks

17 | P a g e
7d Southport & Ormskirk Hospitals NHS Trust Trust Wide Performance Dashboard
Subject Q prem Indicator Description Data Jul‐12 Aug‐12 Sep‐12 Oct‐12 Nov‐12 Dec‐12 Jan‐13 Feb‐13 Mar‐13 Apr‐13 May‐13 Jun‐13Target
2013‐14
Trust wide
Target 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40% 3.40%
Month Actual 4.51% 3.98% 3.79% 3.38% 4.56% 4.36% 4.96% 4.65% 4.49% 4.54% 3.84% 3.99% 3.83%
Month RAG R R R G R R R R R R R R R
Target N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/AMonth Actual 9 5 6 8 3 4 3 10 6 11 13 11 5
Target 2.58 2.58 2.58 2.58 2.58 2.58 2.58 2.58 2.58 2.3 2.3 2.3 2.3
Month Actual 3 0 2 2 3 1 2 1 6 3 3 3 0
Month RAG R G G G R G G G R R R R G
Target 90 90 90 90 90 90 90 90 90 90 90 90
Month Actual 94.7 94.2 91.7 91.6 90.9 91.4 90.6 90.8 91.5 93 93.1 93.7% N/A
Month RAG A A A A A A A A A A A G
Target 100 100 100 100 100 100 100 100 100 100 100 100Month Actual 86.9 96.6 75.5 99.7 85.6 104.1 80.3 92.7 92.5 125.1 81.8% 99.3% N/A
Month RAG G G G G G R G G G R G G
Target 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3
Month Actual 2.45 2.69 2.52 2.49 2.35 2.62 2.55 2.26 2.47 2.68 2.63 2.57 N/A
Month RAG R R R R R R R G R R R R
Target 0.37 0.37 0.37 0.37 0.37 0.37 0.37 0.37 0.37 0.37 0.37 0.37
Month Actual 0.41 0.45 0.38 0.33 0.4 0.41 0.32 0.38 0.47 0.37 0.33 0.43 N/A
Month RAG R R R G R R G R R G G R
Target 4.3 4.3 4.3 4.3 4.3 4.3 4.3 4.3 4.3 4.3 4.3 4.3
Month Actual 4.3 4.59 4.36 4.57 4.17 4.33 4.64 4.1 4.19 4.91 4.8 4.58 N/A
Month RAG G R R R G R R G G R R R
4.3
2.3
ALOS ‐ elective 0.37length of stay
Average length of stay
(ALOS) overall ‐ Trust
ALOS ‐ non‐elective
90
HSMR monthly ‐ Trust 100
Mortality
HSMR YTD ‐ Trust
N/A
hospital acquired pressures
sores grade 2‐42.3
Pressure sores
Community acquired
pressure sores grade 2‐4
Staffing Sickness absence rate ‐ Trust 3.40%

18 | P a g e
7e Areas of under‐ performance
A number of areas of underperformance are reported to end of June 2013; the detail below is presented
by indicator for each of these areas with actions identified as required and on‐going, seeking to improve
performance.
‘Direction of travel’ of performance against indicator from previous reporting period is provided to demonstrate if performance is deteriorating where an indicator has remained at the same performance level and a details improving performance.
Indicator: Emergency readmissions 30 days following DischargeTarget: 5.6% Current Performance 10% Direction of travel Forecast
Current Issues: Figures from April show that Emergency readmissions have been above target and are increasing. National data shows that for S&O emergency readmissions within 30days and within 2 days are below or in line with national averages. However, for emergency readmissions for non‐electives where the patients is readmitted to the same speciality the Trust is an outlier.
Improvement Plans: Further information has been requested to better understand where the re‐admissions are occurring and which specialties.
Indicator: Ambulance category A call outs Target: 75% Current Performance 44.8% Direction of travel Forecast
Current Issues: Category A call outs within 8 minutes are green for NWAS as a whole, but for WL CCG patients the target of 75% achieved within 8 minutes is not being met.
Improvement Plans: A presentation has been received by the executive team from NWAS, week of 9th September, and information on the causes of poor performance and solutions regarding the achievement of this target are being considered.
Indicator: Average length of stay (Unplanned and Planned)Target: Unplanned 4.30 days Planned 0.37 days
Current Performance 4.58 0.43
Direction of travel Forecast
Current Issues: The Trust failed to meet the average length of stay target for each month in 2013/14, however for planned care this is the first month this year that the Trust has not met their target. Unplanned Care showed a small improvement in May and June, however July data has not been received. The trust has reported that LOS are as expected by Dr Foster and are lower than neighbouring Trusts. Dr Foster applies risk adjustment based on demography and would expect overall LOS to be 6.6 bed days. The regional mean at March 13 for LOS was 4.45 days.
Improvement Plans: All Consultant physicians have been asked to undertake ward rounds to ensure patients are reviewed and Juniors and nursing staff are supported in their management of patients. The Ambulatory Care group has been re‐instated to review patient pathways and recommendations for admission avoidance. Subject to Winter monies, there is a proposal for a Frail Elderly Short Stay unit with appropriate staff skill mix to meet demand of this patient group.
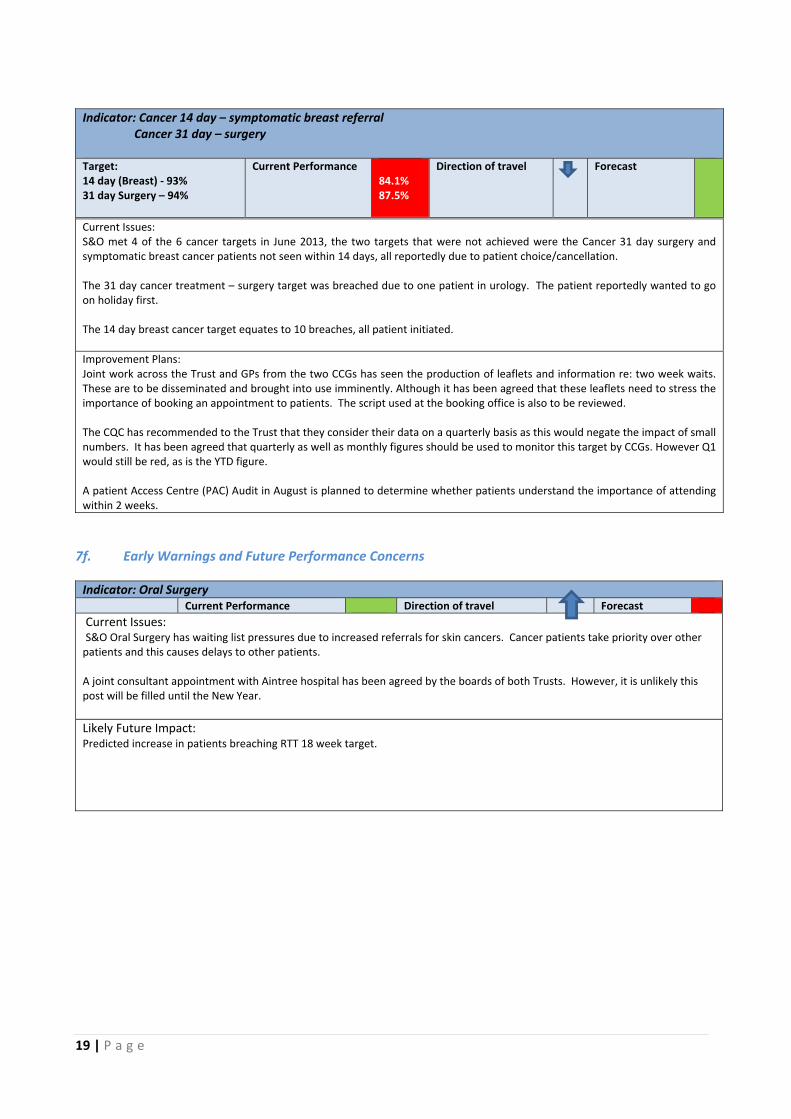
19 | P a g e
Indicator: Cancer 14 day – symptomatic breast referral Cancer 31 day – surgery Target: 14 day (Breast) ‐ 93% 31 day Surgery – 94%
Current Performance 84.1% 87.5%
Direction of travel Forecast
7f. Early Warnings and Future Performance Concerns
Indicator: Oral Surgery Current Performance Direction of travel Forecast
Current Issues: S&O Oral Surgery has waiting list pressures due to increased referrals for skin cancers. Cancer patients take priority over other patients and this causes delays to other patients. A joint consultant appointment with Aintree hospital has been agreed by the boards of both Trusts. However, it is unlikely this post will be filled until the New Year.
Likely Future Impact: Predicted increase in patients breaching RTT 18 week target.
Current Issues: S&O met 4 of the 6 cancer targets in June 2013, the two targets that were not achieved were the Cancer 31 day surgery and symptomatic breast cancer patients not seen within 14 days, all reportedly due to patient choice/cancellation. The 31 day cancer treatment – surgery target was breached due to one patient in urology. The patient reportedly wanted to go on holiday first. The 14 day breast cancer target equates to 10 breaches, all patient initiated.
Improvement Plans: Joint work across the Trust and GPs from the two CCGs has seen the production of leaflets and information re: two week waits. These are to be disseminated and brought into use imminently. Although it has been agreed that these leaflets need to stress the importance of booking an appointment to patients. The script used at the booking office is also to be reviewed. The CQC has recommended to the Trust that they consider their data on a quarterly basis as this would negate the impact of small numbers. It has been agreed that quarterly as well as monthly figures should be used to monitor this target by CCGs. However Q1 would still be red, as is the YTD figure. A patient Access Centre (PAC) Audit in August is planned to determine whether patients understand the importance of attending within 2 weeks.

20 | P a g e
7g CCG Outcome Indicator Set (OIS)
The CCG Outcomes Indicator Set (OIS) is still in development but is designed to provide clear, comparative
information for CCGs about the quality of health services and the associated health outcomes. The
indicators measure outcomes at CCG level to help inform priority setting and drive local improvement.
The areas covered by the indicators contribute to the five domains of the NHS Outcomes Framework. The
CCG OIS does not set thresholds or levels of ambition. It is accepted that the CCG OIS currently provides
limited insight into quality of service provision across CCG footprint due to the ‘historical’ nature of much
of the data presented and the timescales for data refreshes, however as the HSCIC (Health and Social Care
Information Centre), operationalize publication plans, these indicators will become nationally published
measures of CCG quality, hence the inclusion of them in the IBR. A further release is expected in late
September 2013, as data is published more indicators from the framework will be presented.
The table below provides the published West Lancashire CCG position and rank; projects from the Care
Closer to Home initiative should address some of the areas of poor performance reported.
Ref. Indicator Description Reporting Period
Last reported data
CCG Ranking Trend Next update
Data
Preventing people from dying prematurely
1.1 i Potential years of life lost considered amendable to healthcare (MALES)
2011 2736.3 161 out of
211 ↓
Jun ’14 (Annual)
DSR (per 100,000)
1.1 ii
Potential years of life lost considered amendable to healthcare (FEMALES)
2011 2628.2 203 out of
211 ↑
Jun ’14 (Annual)
DSR (per 100,000)
1.2 Under 75 mortality rate from CVD 2011 76.6 155 out of
211 Not
Available Jun ’14 (Annual)
DSR (per 100,000)
1.6 Under 75 mortality rate from Respiratory Disease 2011 28.0 114 out of
211 Not
Available Jun ’14 (Annual)
DSR (per 100,000)
1.7 Under 75 mortality rate from Liver Disease 2011 14.6 91 out of 211 Not
Available Jun ’14 (Annual)
DSR (per 100,000)
1.8 Emergency admissions for alcohol related liver disease 2011/12 25.3 127 out of
211 ↓
Dec 2013 (Quarterly)
DSR (per 100,000)
1.9 under 75 mortality rate from Cancer 2011 126.4 131 out of
211 Not
Available Jun ’14 (Annual)
DSR (per 100,000)
Enhancing quality of life for people with long term conditions
2.6 Unplanned hospitalisation for chronic ambulatory care sensitive conditions
2011/12 963.0 167 out of
211 ↓
Dec 2013 (Quarterly)
DSR (per 100,000)
2.7 Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s
2011/12 533.3 203 out of
211 ↓
Dec 2013 (Quarterly)
DSR (per 100,000)
Helping people to recover from episodes of ill health or following injury
3.1 Emergency admissions for acute conditions that should not usually need hospital admission
2011/12 1370.25 188 out of
211 ↓
Dec 2013 (Quarterly)
DSR (per 100,000)
3.2 Emergency re‐admissions within 30 days of discharge from hospital
2010/11 12.5 157 out of
211 Not
Available Dec 2013 (Quarterly)
ISR (per 100,00)
3.3a Patient reported outcome measures for elective procedures: hip replacement
2011/12 0.416 Not Available ↑ Sept ’14 (Annual)
case mix adjusted health gain
3.3b Patient reported outcome measures for elective procedures: knee replacement
2011/12 0.355 Not Available ← Sept ’14 (Annual)
case mix adjusted health gain
3.3c Patient reported outcome measures for elective procedures: groin hernia
2011/12 0.085 Not Available ↓ Sept ’14 (Annual)
case mix adjusted health gain
3.3d Patient reported outcome measures for elective procedures: varicose veins
2011/12 Numbers are too small
Sept ’14 (Annual)
case mix adjusted health gain
Ensuring that people have a positive experience of care
4.1 Patient experience of GP out‐of‐hours services July 2011 to March 2012
73.99 151 out of
211 Not
Available Sept ’14 (Annual)
Percentage (adjusted)

21 | P a g e
7h Alternative Quality Contract (AQC) metrics
The Schedule below presents the additional quality performance metrics, required to be reported against
as part of the Alternative Quality Contract (AQC) with Southport & Ormskirk Hospitals NHS Trust. Data is
in the process of being baselined with the aim of presenting performance against these metrics from
quarter three 2013/14.
No. AQC Priority Indicators Description
1
All Non Elective admitted patients with fractured NOF (suitable for surgery) to be operated on within 36 hours of admission
For exclusions see 'Better Care Better Value' guidance. Data to be gathered showing monthly achievement, 90% to be achieved by year end.
2 Increase percentage of patients that are discharged with a LACE score
Patients >18yrs on the General medical wards and Short Stay Unit (11b,11a,14b,7a,9a,9b,eau,h,obs,ssu) that are discharged with a LACE score ‐ Target to be agreed after baseline data pulled
2.1
Increase proportion of identified patients with a LACE score of 10‐12 to be contacted by ICO staff by telephone within 1 working day of discharge.
Criteria as above, data to be split by CCG as different community provision across each patch
2.2
Increase proportion of identified patients with a LACE score >12 that get a visit by ICO staff <24hrs (exclude GP visits)
Criteria as above, data to be split by CCG as different community provision across each patch
2.3 Re‐admission rates for patients with a LACE score >12 within 30 days of discharge (track only)
Criteria as above, data to be split by CCG as different community provision across each patch, monitor only ‐ link to CC2H project
3 Communicate with CCGs ‐ Staffing Levels
Share with CCGs report and recommendations for Keith Hurst work
3.1 Communicate with CCGs ‐ Staffing Levels
Provide quarterly report ‐ containing spend on bank and agency staff and any incident reporting relating to staffing levels. Both split by ward and reported by month. To have previous 2 quarters also included in first report (ICO to share draft report first).
4 Electronic discharges/outpatients/x‐rays ‐ To be agreed
97% of electronic communication to be sent to patients GP practice within 24hrs of discharge/appointment ‐ no agreement as yet
4.1 Electronic discharges/outpatients/x‐rays ‐ To be agreed
Data quality audit on electronic communication ‐ On agreement of indicator 4
5 Specialist stroke team and rehab Increase number of patients assessed by specialist stroke nursing staff within 24 hours of admission to hospital
5.1 Specialist stroke team and rehab Increase number of patients assessed by specialist stroke rehab staff within 24 hours of admission to hospital (WORKING WEEK ONLY ‐ track admissions on mon‐thur only ‐ Rehab team not working 7 days a week yet)

22 | P a g e
7i West Lancashire CCG summary of NHS England – North Region, quality report June 2013
Tables one to three on the following page present a summary of the NHS England ‐ North Region, Quality Report of June 2013 and covers performance of the key acute trusts from which West Lancashire CCG commissions services, it does not comment on the impact of the quality / performance of trusts on West Lancashire patients or provide rationale for trust performance. Please exercise caution in taking decisions based on this data as some data is not timely and represents 'historic' performance. Common themes emerging from this report for the five trusts summarised include less then optimal performance against;
A&E Friends and Family return rates
Patients waiting over 4 hours in A&E
Incidences of MRSA and C Diff
Mean ‘Lengths of Stay’ above regional average
Table one represents how well each trust is performing across the quality metrics, (pages 4 and 5 of full report and summarised in table 2 below). Table one presents in month performance for June 2013, with trends from the previous month in table two ‐ all trusts in the West Lancashire footprint reported deterioration in performance from May to June 2013, with three of the five trusts ranking in the bottom 20% in the region in June 2013. Key areas of concern are commented on in table two against each trust. Table three, presents in a simplified form the performance against key quality measures for trusts in West Lancashire footprint to end of June 2013. Please refer to page six of full report for guidance notes including data source and RAG tolerances / targets.
5.2 Specialist stroke team and rehab Increase number of patients offered 6 week post discharge satisfaction survey ‐ documenting reasons for decline ‐ split by CCG
6
Reduction in the number of hospital cancelled outpatient appointments ‐ all specialties, report split by specialty (threshold to be agreed)
Report to show number of hospital cancelled outpatient appointments by month by specialty ‐ reduction to be agreed after baseline
7 Reduce delayed discharges Monitor the delayed discharges (when patients are "medically optimised" to "discharge" Gen med patients only)
8 Reduce total NEL heart failure bed days
9 Increase the number of patients discharged with a rescue pack
NEL admissions with a primary/secondary diagnosis of COPD (denominator) discharged with a rescue pack (numerator)
10 Increase number of patients with stable hba1c after six months
Increase the number of patients of the specialist diabetes service that have an acceptable hba1c six months after initial appointment (measure to be defined ‐ currently reduce by 1%, ‐ currency changed so need clarification)

23 | P a g e
Performance far worse than expected
Table 1 – High level quality overview of trust performance against quality targets
Table 2 – Ranking of trusts for quality targets and areas of poor performance
Table 3 – Detailed poor performance

24 | P a g e
7j Friends and Family Inpatients
A summary of performance against the inpatient ‘Friends and Family’ test covering the key acute trusts
commissioned by West Lancashire CCG for the month of July 2013 will be shared with the CCG Quality
Committee. Key points to note are;
1. All trusts achieved the response rate target of 15%
2. One trusts (RLBUH) scored below national average
3. Two trusts (S&O, RLBUH) ranked in the bottom third nationally based on score.
7k Friends and Family A&E
A summary of performance against the A&E ‘Friends and Family’ test covering the key acute trusts
commissioned by West Lancashire CCG for the month of July 2013 will be shared with the CCG Quality
Committee. Key points to note are;
1. Only one trust (Aintree) achieved the response rate target of 15%, however three trusts achieved
batter than national average response rates (S&O, Aintree, WWL). Consequently comment can
only be made on the score of Aintree.
2. Aintree reported a score below national average and in the bottom 10 nationally.
7l Trust level narrative summaries of quality
It is acknowledged that sections 7g ‐7k provide basic data with limited context and explanation of actions
to be taken to address reported underperformance in relation to quality.
Plans have now been established within the CCG Business Analysis function to enable the development of
trust level intelligence, consequently in future reports areas of underperformance and /or early warning
triggers in relation to quality will reported by trust for the key contracts commissioned by West
Lancashire CCG. Detailed action plans will be requested and reported to seek improvement in quality.
Performance will be reported for the following trusts;
1. Southport and Ormskirk Hospitals NHS Trust
2. Wrightington, Wigan and Leigh NHS Foundation Trust
3. Aintree University Hospital NHS Trust
4. Royal Liverpool and Broadgreen Hospitals NHS Trust
5. Lancashire Teaching Hospitals NHS Foundation Trust
6. St Helens and Knowsley Hospitals NHS Trust
In future months data presented in this section will be expanded to track trends in performance month on
month, with the purpose of increasing the usefulness of this information.
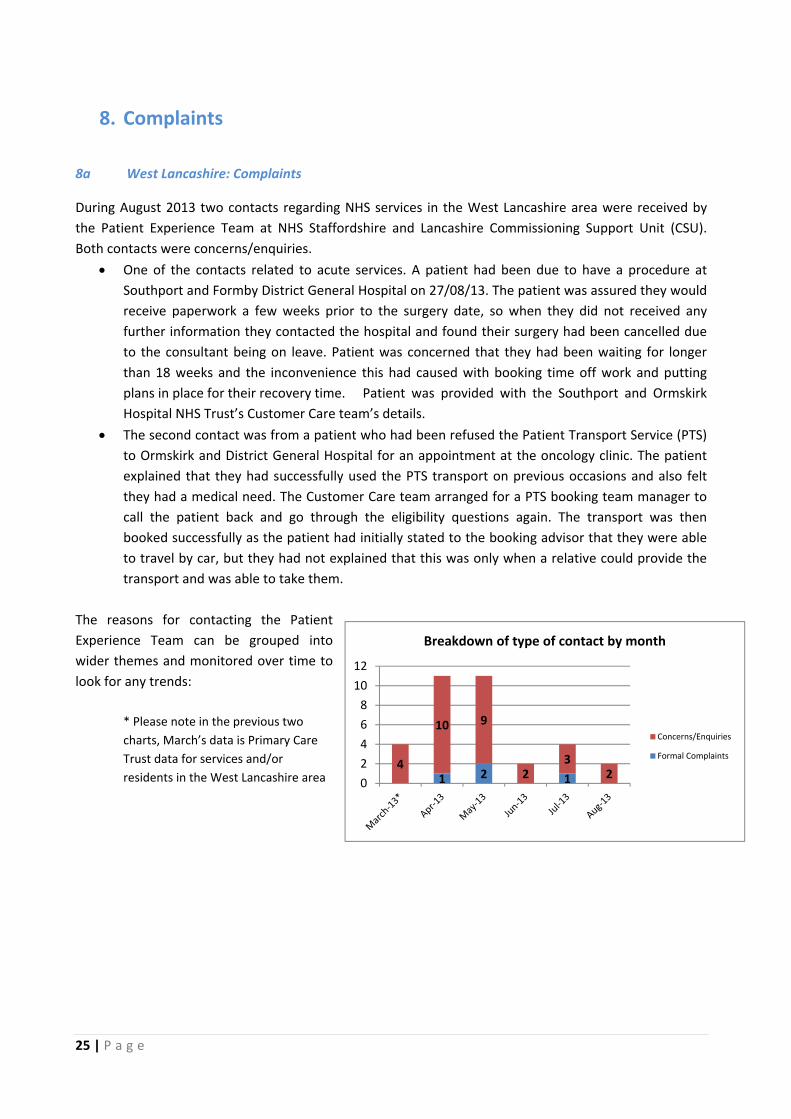
25 | P a g e
8. Complaints
8a West Lancashire: Complaints
During August 2013 two contacts regarding NHS services in the West Lancashire area were received by
the Patient Experience Team at NHS Staffordshire and Lancashire Commissioning Support Unit (CSU).
Both contacts were concerns/enquiries.
One of the contacts related to acute services. A patient had been due to have a procedure at
Southport and Formby District General Hospital on 27/08/13. The patient was assured they would
receive paperwork a few weeks prior to the surgery date, so when they did not received any
further information they contacted the hospital and found their surgery had been cancelled due
to the consultant being on leave. Patient was concerned that they had been waiting for longer
than 18 weeks and the inconvenience this had caused with booking time off work and putting
plans in place for their recovery time. Patient was provided with the Southport and Ormskirk
Hospital NHS Trust’s Customer Care team’s details.
The second contact was from a patient who had been refused the Patient Transport Service (PTS)
to Ormskirk and District General Hospital for an appointment at the oncology clinic. The patient
explained that they had successfully used the PTS transport on previous occasions and also felt
they had a medical need. The Customer Care team arranged for a PTS booking team manager to
call the patient back and go through the eligibility questions again. The transport was then
booked successfully as the patient had initially stated to the booking advisor that they were able
to travel by car, but they had not explained that this was only when a relative could provide the
transport and was able to take them.
The reasons for contacting the Patient
Experience Team can be grouped into
wider themes and monitored over time to
look for any trends:
* Please note in the previous two
charts, March’s data is Primary Care
Trust data for services and/or
residents in the West Lancashire area
1 2 14
10 9
23
20
2
4
6
8
10
12
Breakdown of type of contact by month
Concerns/Enquiries
Formal Complaints

26 | P a g e
The type of contacts received i.e. formal complaint or concern/enquiry can be recorded over time to
look for any trends:
Items in the “Other” theme relate to issues
with a dental surgery, GP practice, Out of
Hours service and Acute Trusts.
The majority of contacts relate to patient
transport
8b GP Issues with Southport & Ormskirk Hospitals Trust
GPs are able to register their concerns with services provided by Southport & Ormskirk Hospitals NHS Trust by using the GP Response telephone line. The Trust has set a timescale for response of 10 days to acknowledge and set out details of the plan to ameliorate the GPs concern. Feedback for these issues is presented to the GP operational forum. Reports are prepared on the themes of these concerns and these have been requested so that they can be incorporated into this paper. 8c Southport & Ormskirk Hospitals Trust Compliments and Complaints
The Trust received 575 compliments in July.
Based on data for July 2013 the trust received 35 complaints. Those complaints related: 11 to urgent care
16 to planned care 3 to community and long‐term care and 4 related to Women’s and children’s Services.
There were 107 PALS contacts received. Of these:
14 referred to communications issues
5 regarding treatments and care received
10 relate to car parking
4 relate to staff attitude
11 requesting information or advice
2 access and booking
6 medical care
1 end of life
1 discharge arrangements
3 cancellations
1 waiting times
1 medication
The trust has undertaken a number of actions in order to address complaints received including, face to
face discussions with patients/relatives and apologies.
8
2
314
6
Reason for contact by theme
Advice and Information
Communication
Contracting/Commissioning
Funding
Transport
Other
Data shown is for March ‐ August

27 | P a g e
9. Serious Untoward Incidents
This section provides details of the new and on‐going STEIS reportable Serious Untoward Incidents (SUIs)
involving West Lancashire CCG patients for the period up to end August 2013. A Serious Untoward
Incident (requiring investigation) has a nationally set definition but fundamentally is defined as an
incident that occurred in relation to NHS‐funded services and care resulting in ‘avoidable harm or
unexpected death’ or ‘adverse media coverage, severe impact on service provision or loss of person
identifiable data’.
9a. New Incidents in August There have been no new SUIs reported to Lancashire CSU during August involving West Lancashire residents 9b. On‐going investigations
As at 31 August 2013, the, Lancashire Commissioning Support Unit has 7 open SUIs being investigated and performance managed and NHS England is also performance managing a further 1 SUI in relation to the E05 scheme. Lancashire CSU has also received information from Cheshire and Merseyside CSU providing a summary of the open SUIs as at 31 August involving West Lancashire residents. Currently C&M CSU has 7 open SUIs therefor there are a total 15 SUIs on‐going for the CCG. The table overleaf shows the numbers of these open SUIs for West Lancashire residents broken down by the reporting organisations.
Provider Organisation Incident Type Date
reported Total
Lancashire Care NHS Foundation Trust
(Performance managed by Blackburn with
Darwen CCG)
Attempted suicide by inpatient (in receipt) 29/07/13 1
Slip/Trip/Fall 25/10/13 1
Unexpected death Nov 2012 –
April 2013 5
TOTAL 7
Ramsay Healthcare E05 Scheme (Performance
managed by NHS England) Other 14/11/2012 1
TOTAL 1
Southport & Ormskirk Hospitals Trust
(Performance managed by ourselves via
Southport and Formby CCG)
Wrong site surgery – Never Event 07/02/2012 1
Delayed diagnosis Neuroblastoma stage
4 27/02/13 1
Unexpected Maternal death following
discharge 28/02/13 1
Intrauterine death 15/03/2012 1
Medicines (dispensing) 28/06/2012 1
Retained swab – Never Event 30/07/2013 1
Retained swab – data release 30/07/2013 1
Total 7
No. of open SUIs for West Lancashire residents by reporting organisation

28 | P a g e
No SUIs have been closed by the CSU involving West Lancashire CCG patients during July. The root cause analysis reports and action plans will be considered by the lead commissioner in conjunction with West Lancashire CCG and will be agreed as acceptable or if not additional information will be requested. An update on progress with these cases will be presented each month as part of this report. A meeting took place on Friday 13th September to consider the outcome of the root cause analysis of the two retained swab SUI’s. A final report is expected imminently.

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
1
WLCCGB 9/13/09
WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT
DATE OF BOARD MEETING: 24 September 2013 TITLE OF REPORT: West Lancashire Clinical Commissioning Group
Medicines Optimisation Report BRIEFING POINTS:
April – August 2013
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact
2. Commissioning of hospital and community services – please outline impact
3. Commissioning and performance management of GP Prescribing – please outline impact
√
4. Delivering Financial Balance – please outline impact √ 5. Development of the commissioning group as a commissioning
organisation – please outline impact
B. Governance – please outline impact 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice
2. Additional resource implications
(either financial or staffing resources)
3. Health Inequalities 4. Human Rights, Equality and Diversity Requirements 5. Clinical Engagement √ 6. Patient and Public Engagement REPORT PREPARED BY: Nicola Baxter Head of Medicines Optimisation

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
2
West Lancashire Clinical Commissioning Group Medicines Optimisation report April- August 2013-14
Introduction
NHS West Lancashire Clinical Commissioning Group’s strategic vision is: To make effective use of resources by working with local people and our partners in West Lancashire. The CCG strive for the best possible care for the local population and to empower people to be in control of their own health and health care services.
The Clinical Commissioning Group (CCG) recognises that patient centred, good quality, cost effective prescribing and medicines optimisation will contribute to this vision. Medicines optimisation is defined as improving quality, outcomes and value for patients from their use of medicines. It is also about a higher level of engagement with patients and the public as well as breaking down the barriers between professions and for this reason is more sophisticated than medicines management. The CCG medicines optimisation priorities are grouped into three types of activity, namely; those activities focused at individual patient level; those focused at supporting healthcare professionals; and those that focus on services across the CCG population.
Background: The National Context during 2013-14
The financial year 2013-14 still sees the Department of Health’s Quality, Innovation, Prevention and Productivity, or QIPP agenda as centre stage within the NHS as the means to address increasing demand for services against a static funding picture. In addition to this, CCGs are now set up and are taking responsibility for the medicines optimisation agenda. This paper will demonstrate how the medicines optimisation team, working with prescribers and other staff across primary and secondary care, addresses the aspects of the QIPP agenda the CCG is responsible for and also supports the CCG priorities.
Delivering Medicines Optimisation QIPP for patients
Activities supporting this aspect of medicines optimisation focuses on two main areas, as follows: ensuring that patients receive the right medicines for their conditions, and suitable information about medicines; and supporting people to use medicines appropriately for self-care.
The first aim is addressed by focusing the activities of the medicines Optimisation team, so that every GP practice is offered regular support from a pharmacist or technician dependent on their requirements; the frequency of support depends on the area of work and degree of need within each practice. Pharmacist time is spent on undertaking medication reviews, focusing on patients who have long term conditions. The technicians complete a clinical review following a protocol; this may involve preliminary data gathering for review by the pharmacist, or may make recommendations to the patient’s GP, depending on the area being reviewed. This skill mix ensures that the practices gain maximum benefit from the pharmacist’s clinical expertise.
West Lancashire CCG has been taking responsibility since 2011-12, for managing their prescribing budgets. As a result, West Lancashire CCG decided to review how the medicine Optimisation team’s capacity was distributed amongst their practices. This involved focusing capacity intensively within those practices with most potential for improvement, while other practices received less frequent visits. This change has been proven to be very successful, as demonstrated by an increased pace of improvement in intensively supported practices. This approach to supporting practices has continued year on year.

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
3
Delivering Medicines Management QIPP for healthcare professionals
CCG Medicines management duties In order to address the CCG medicines Management duties as defined by the National Prescribing Centres medicines management competency Framework, West Lancashire CCG has set up a Medicines Management Committee (MMC) which makes recommendations to the clinical executive. Medicines management encompasses all systems, policies and procedures designed to ensure the safe, secure and cost-effective use of medicines. This includes:
Evidence-based and cost-effective prescribing practice at an individual and population level
safe and secure supply, storage and administration of medicines efficient purchase and distribution systems for medicines development of pharmaceutical and other services to improve the clinical use of
medicines development of and compliance with contractual requirements relating to medicines
management MMC addresses interface issues around prescribing and medicines use. The committee acts as a focus for developing and agreeing local professional opinion on drugs, therapeutics and associated medicines and pharmaceutical issues conveys such opinion to all relevant organisations and bodies, including the Lancashire Medicines Management Group, Pan Mersey Area Prescribing Committee, the Trust Drugs and Therapeutics Committee and those not directly represented on the committee. The committee makes recommendations on the managed entry of new drugs on to the joint West Lancashire CCG and Southport and Ormskirk hospital trust formulary and guidelines based on the recommendations of the Lancashire medicines Management Group and Pan Mersey Area Prescribing Committee.
Budget setting process At the beginning of financial year 2013-14 the medicines Optimisation team with the support of the Commissioning Support Units (CSU) medicines management core team undertook horizon scanning work, to identify forthcoming cost pressures in the prescribing budget as well as opportunities for improving cost-effectiveness. This work was used in budget setting discussions within the CCG, which resulted in an overall prescribing budget allocation of £16.9million. Work was then done with the CCGs clinical executive committee and MMC to allow the CCG to develop its own method for allocating the budget to individual practices, in a way that is fair to all practices and ensures that they have sensible budget that allows them to implement cost effective prescribing. Monthly monitoring reports at practise and CCG level are provided to the CCG throughout the year so as to enable the CCG to manage the prescribing budgets. These reports are provided by the medicines management core CSU team.
Areas with potential to improve the cost-effectiveness of prescribing have been developed into the CCG medicines Optimisation QIPP savings plans for 2013-14, which resulted in an overall savings target of £500,000 comprised of practice work and liquid specials. Prescribing support pharmacists and technicians are working directly with practices to review prescribing and change to the most cost-effective, evidence based products.

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
4
Medicine Optimisation Team Medicines optimisation is the responsibility of all healthcare staff who have contact with patients, and so they must be supported to ensure the safe and effective use of medicines. The aim of this aspect of the strategy is therefore:
to develop the skills and resources of all health care professionals, and the necessary and appropriate service capacity, to ensure medicines are used effectively to improve health, while minimising risks from treatment.
This work began with the development and agreement with practices of a range of prescribing areas to be worked on. In the past this came under the auspices of the Quality and Outcomes (QOF) Framework aspect of the GMS contract. Medicines management is no longer part of QOF. However, the medicines optimisation team continue to work as part of the practice team to deliver quality and cost-effective prescribing. The areas of work recommended by the Medicines Management Committee were aimed at improving the quality and cost-effectiveness of prescribing.
The following summarises the work conducted by the West Lancashire CCG medicines optimisation team (MOT) from April 2013 to the end of August 2013.
Number of patients reviewed by the MOT is 2206 Number of recommendations made by the MOT is 806 Full year net savings £54,000 out of a maximum potential of £100,000
The full year net savings reflects the work that has been completed and has resulted in the change of medication for a patient. It should be noted that at this point in time approximately half of the potential savings presented to practices have been realised and that this work is on-going. West Lancashire CCG MMC will monitor this progress on a monthly basis alongside the prescribing monitoring report and adapt the work plan if necessary. A significant proportion of the medicines optimisation teams work is based on safety 840 of the patients reviewed so far, had the primary aim of ensuring the implementation of safe prescribing, such reviews include antidepressants, benzodiazepines, diclofenac, metoclopramide, strontium and triptans over use. The team continues to play a part in improving skills around prescribing by offering information and advice on current topics by way of the weekly prescribing tip email; this continues to be well received by prescribers. The team are currently piloting working with nursing homes as part of the practices medicine optimisation work plan. Scriptswitch Ensuring patients receive the right medication has also been addressed utilising Scriptswitch software. Scriptswitch is a computer program that operates at the point of prescribing to promote cost-effective drug switching and rational prescribing. The system is managed by the medicines optimisation team, and messages tailored to fit in with work being done in practices and the cost-effectiveness work programme, as well as local formulary, national guidelines, and NPSA or MHRA drug safety alerts. The system is currently utilised by 19 practices across West Lancashire CCG. The Scriptswitch system sends prescribers over 44,000 quality and safety information messages per month as well as delivering savings of over £61,000 by the end of August 2013. There

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
5
was a potential of saving over £623,000. The cost of the system is £34,877 per year so over £26,000 net profit. This represents a significant improvement compared to the final year net savings of £18,000 for 2012-13. This is a result of a dedicated resource by the medicines optimisation team during 2013-14 to ensure that Scriptswitch messages are comprehensively reviewed and targeted to maximise the impact of the system. The progress of scriptswitch will be monitored on a quarterly basis a decision to continue with scriptswitch should be made at the beginning of the next financial year. There are many quality and safety messages alongside the cost effective messages, which cannot be costed but prompt a review of the medication and instigate behavioural change. Delivering Medicines Management QIPP for the whole population Embedding the principles of safe, effective and cost-effective use of medicines in the CCGs commissioning activities. Safe use of medicines The first element of this work was to continue to address the use of “specials” products across the CCG. Special order products, or “specials”, are unlicensed products which are manufactured to address a particular patient’s needs; for example, a liquid product may be required for a patient with swallowing difficulties. The use and costs of these products has been steadily increasing over recent years and they now represent a significant cost pressure in primary care prescribing. There is also significant variation in the costs to obtain the same product from different manufacturers or wholesalers. Specials products are not subject to the same stringent quality controls as licensed medicines, so there may be issues in relation to the quality of these preparations. For these reasons, it is appropriate to try to minimise the use of such products unless no suitable licensed alternative exists. The team continued to work with practice medicines co-ordinators to identify the use of specials.
Medicines Co-ordinators The second aspect of this work was to address medicines waste. The team takes a multidisciplinary approach to tackle wastage of medicines, working with Medicines Co-ordinators and GP practices to align quantities, review repeat ordering processes and increase the uptake of Repeat Dispensing, which collectively should improve patient adherence and therefore reduce waste medicines.
The scheme is in its 5th year and continues to demonstrate its effectiveness as a means of improving the safety of medicines use, as well as improving cost-effectiveness. There are currently 21 medicines co-ordinators working in 20 practices across West Lancashire. Three practices have employed new medicines co-ordinators within the last 12 months. Training Sessions The medicines optimisation team has developed and delivered monthly training sessions, on the following:-
Drug and Alcohol abuse Pain control Nutrition and coeliac disease Skin and wound Chronic Kidney Disease Asthma

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
6
Areas of work undertaken Implementation of prescribing tips Repeat dispensing sign up Brand to generic switches Ensuring monitoring of high risk medication such as DMARDs and Warfarin Responding to interface issues between the practice, secondary care, community
pharmacy and nursing homes 7 day prescriptions
In summary the medicines co-ordinators have generated savings through their work of £84,600 until the end of July 2013.
The total April 2013 to August 2013 savings delivered within 2013-14 are summarised in the table below:
Cost Effectiveness Area Planned Savings
In Financial Year Savings Delivered
Medicines Management Team work plan
£100,000 £54,000
Medicines Co-ordinators £84,000 Scriptswitch £623,000 £61,000 Category M Price Decreases
£0
TOTAL £723,000 £209,000
Medicines Management in the commissioning process
The medicines Optimisation team provide professional pharmaceutical advice into the CCG commissioning agenda, to assure that the appropriate use of medicines is considered during the service design phase of the commissioning cycle. Team members are actively involved in the integrated care pathway groups.
Robust processes for the managed introduction of new drugs across the health economy have also been further developed, via the MMC and area medicines management committee. A very detailed piece of horizon-scanning work was done together with finance colleagues, to inform the budget setting processes for 2013-14 and beyond.
CCGs from 2013-14 will be responsible for two of the current pharmacy enhanced services including the minor ailments scheme and access to end of life drugs scheme.
The minor ailment scheme allows patients to access the community pharmacy for advice and supply of specific treatment within a SOP this reduces unnecessary consultations for the GP.
Access to end of life drugs is a scheme were community pharmacies stock specific drugs for end of life. The aim is to ensure that patients can access these medicines from a specified number of pharmacies within West Lancashire.
The Minor ailments scheme and End of life drugs scheme will be reviewed and updated if necessary through the MMC with recommendations going to the clinical executive committee.

West Lancashire Clinical Commissioning Group Medicines Optimisation Report West Lancashire Clinical Commissioning Group Board Meeting - 23.09.2013
7
Conclusions This report describes the progress attained against the CCGs medicines Optimisation priorities during the first 5 months of 2013-14. The report demonstrates a high degree of achievement of the CCG Medicines Optimisation priorities to deliver Quality, Innovation, Productivity and Prevention relating to the use of medicines. As a result, prescribing volume and costs in West Lancashire are both significantly below the northwest regional averages. These achievements reflect the results of the sustained efforts of all the pharmacists, pharmacy technicians and administrative staff in the medicines management team, working in collaboration with prescribers in primary and secondary care, to help the people of West Lancashire live for longer and with improved outcomes, by optimising the use of medicines. Nicola Baxter Head of Medicines Optimisation West Lancashire Clinical Commissioning Group September 2013

Armed Forces Community Covenant West Lancashire Clinical Commissioning Group Board Meeting – 24.9.13
1
WLCCGB 9/13/10
WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT
DATE OF BOARD MEETING: 24 September 2013 TITLE OF REPORT: Armed Forces Community Covenant BRIEFING POINTS:
The armed forces covenant sets out the relationship between the nation, the state and the armed forces.
It recognises that the nation has a moral obligation to members of the armed forces and their families and it establishes how they should expect to be treated. It exists to redress the disadvantages and inequalities that the armed forces community faces in comparison to other citizens and to recognise the sacrifices that they have made. Since 2011, at the local level, ‘community covenants’ have been signed bringing military and civilian communities together. The CCG Executive has endorsed proposals to sign up to the Community Covenant which now seeks Governing Body approval.
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact X
Improving the health and wellbeing of armed forces and veterans is part of the annual planning guidance. Whilst many of the commissioning responsibilities for this area of work do not rest with Clinical Commissioning Group’s, committing to the armed forces covenant demonstrates the CCG’s commitment to supporting improvements in health and wellbeing for armed forces and veterans and improving the quality of their experience of health and wellbeing services. 2. Commissioning of hospital and community services – please outline
impact
3. Commissioning and performance management of GP Prescribing – please outline impact
4. Delivering Financial Balance – please outline impact 5. Development of the commissioning group as a commissioning
organisation – please outline impact
B. Governance – please outline impact 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice

Armed Forces Community Covenant West Lancashire Clinical Commissioning Group Board Meeting – 24.9.13
2
2. Additional resource implications (either financial or staffing resources)
3. Health Inequalities Research by the British Legion (Treating Illness and Injury arising on Military Operations, National Audit Office Report, February 2010) showed that just over half (52%) of the adult ex-Service community had a long term illness, disability or infirmity (in comparison to the UK adult population at 35%), and a fifth (20%) had multiple conditions. Expectedly, the proportion reporting any long-term health problems increased with age. However, significantly numbers of younger members of the ex-Service community, ages 16-44 and 45-64 were 8% and 10% respectively more likely to suffer from a long-term disability, illness or infirmity when compared nationally to the same age categories. In addition to this 20% of the ex-Service community say they are not in very good health and 5% say their health is not at all good. 4. Human Rights, Equality and Diversity Requirements 5. Clinical Engagement 6. Patient and Public Engagement REPORT PREPARED BY: Lucinda Cawley
Senior Operating Officer (Planning & Service Redesign)

1 | P a g e
NHS West Lancashire Clinical Commissioning Group Executive
Title: Armed Forces Community Covenant
Paper presented by: Dr Simon Frampton
Paper prepared by: Lucinda Cawley (Senior Operating Officer)
Date: 6th August 2013
Summary The armed forces covenant sets out the relationship between the nation, the state and the armed forces. It recognises that the nation has a moral obligation to members of the armed forces and their families and it establishes how they should expect to be treated. It exists to redress the disadvantages and inequalities that the armed forces community faces in comparison to other citizens and to recognise the sacrifices that they have made. Since 2011, at the local level, ‘community covenants’ have been signed bringing military and civilian communities together. CCGs have responsibility for all veterans health care needs and all health care needs of families and dependants of serving personnel. NHS England holds responsibility for commissioning healthcare for serving military personnel.
Background In 2011 the Government published a tri-Service ‘Armed Forces Covenant’. It set the tone for Government policy aimed at improving the support available for the Armed Forces Community. The notion of a mutual obligation between the nation and the armed forces dates to 1593, enhanced in 2000 to a “military covenant”. In 2011 the tri-forces covenant was published and the principles of the armed forces became enshrined in law with the Secretary of State for Defence having an obligation to report annually to parliament on delivery against the covenant The Government also published ‘The Armed Forces Covenant: Today and Tomorrow’. This document outlines the role of community covenants which it states will “encourage public service providers at Local and Unitary Authority level, the private sector and the voluntary and community sectors to volunteer targeted support for their local Armed Forces community”. It states that “The Community Covenant is intended to be a two way arrangement to actively encourage the local Service population to provide support to their local community”. ‘The Armed Forces Covenant: Today and Tomorrow’ also introduced the MoD led community covenant grant scheme allocating up to £30m over four years. The next submission date for the grant scheme is September 2013 with a further 4 panels meeting through 2014 to early 2015. What is the size of the Armed Forces and veteran population in West Lancashire? Estimating the armed forces and veteran population in West Lancashire is difficult. A JSNA is currently ongoing at the regional level (host commissioner is Bury CCG) which will inform this and is due to report in September. West Lancashire falls within 42 (North West) Brigade which is the regional Army brigade which looks after the Army's interests in North West and the Isle of Man. More than 2,000 regular soldiers are based within the North West, at barracks in Preston, Weeton and Chester. There are 3,600 territorial soldiers and more than 7,000 cadets, and 4 military training areas (Warcop, Halton, Holcombe Moor and Altcar). Every year, about one-fifth of all the Army's new recruits are recruited from the 42 (North West) Brigade region.

2 | P a g e
For the Royal Air Force, 611 (West Lancashire) Squadron is reforming at RAF Woodvale near Formby and is the only RAF station in North-West of England. As well as its role to provide reserve personnel to support current and future RAF operations, the Squadron will be active in connecting the RAF to local communities in the region. The North West hosts dozens of Royal Navy ship visits every year. The Royal Naval Headquarters for Northern England and Isle of Man are based in Liverpool. Brunswick Dock, Toxteth hosts a number of units, including HMS Eaglet (Liverpool), the region’s Royal Naval Reserve unit. Eaglet is one of the largest such units in the country with around 200 members and regularly sends personnel to support operations in Iraq and Afghanistan. Offshore patrol ship HMS Mersey is affiliated to the borough of Sefton. Royal Marines Reserve Merseyside has around 200 members, most of who have served in Iraq or Afghanistan in the last five years. Progress to Date and Next Steps A draft community covenant is attached at appendix one. The development of this has been led by West Lancashire Borough Council whom the CCG has been liaising with on participating in the Covenant. The Covenant states an expectation of establishing agreed priorities and action against three themed areas;
Education, Skills and Employment
Health and Wellbeing
Families and Housing The expectation is likely to be that the CCG will lead the development of establishing priorities and actions for the health and wellbeing theme. Participating in the Covenant would serve as a mechanism for the CCG to progress work against the national expectation and priority of armed forces and veteran health, a priority which features in the annual NHS planning guidance. Action The Executive is asked to take discussion on the paper and agree;
To participate in the community covenant
To report to the Governing Body annually on its progress

3 | P a g e
Appendix One
West Lancashire Community Covenant
AN ARMED FORCES COMMUNITY COVENANT
BETWEEN
WEST LANCASHIRE BOROUGH COUNCIL, REPRESENTATIVES OF THE PUBLIC, PRIVATE, COMMUNITY AND VOLUNTARY SECTORS, THE CIVILIAN
COMMUNITY OF WEST LANCASHIRE
AND
THE ARMED FORCES COMMUNITY IN WEST LANCASHIRE

4 | P a g e
1 PARTICIPANTS 1.1 This Armed Forces Community Covenant is made between:
The serving and former members of the Armed Forces, whether regular or reserve, and their families, working and residing in West Lancashire And West Lancashire Borough Council And The Public, Private, Community and Voluntary Sectors in West Lancashire And Other members of the civilian community.
2 PRINCIPLES OF THE ARMED FORCES COMMUNITY COVENANT
2.1 The Armed Forces and Community Covenant is a voluntary statement of mutual support between a civilian
community and its local Armed Forces Community. It is intended to complement the Armed Forces Covenant, which outlines the moral obligation between the Nation, the Government and the Armed Forces, at the local level.
2.2 The purpose of this Community Covenant is to encourage support for the Armed Forces Community working and
residing in West Lancashire and to recognise and remember the sacrifices made by members of this Armed Forces Community, particularly those who have given the most. This includes in-Service and ex-Service personnel, their families and widow(er)s in West Lancashire.
2.3 For West Lancashire Borough Council and partner organisations, the Community Covenant presents an opportunity to
bring their knowledge, experience and expertise to bear on the provision of support to members of the Armed Forces Community.
2.4 For the Armed Forces Community, the Community Covenant encourages the integration of service life into civilian life
and encourages members of the Armed Forces Community to help their local community. 3 OBJECTIVES AND GENERAL INTENTIONS
Aims of the Community Covenant 3.1 It aims to encourage all parties within a community to offer support to the local Armed Forces Community and make
it easier for service personnel, families and veterans to access the help and support available from statutory providers and from the Private, Community and Voluntary Sectors.
3.2 This local Armed Forces Community Covenant complements the principles of the national Armed Forces Covenant
which defines the enduring, general principles that should govern the relationship between the Nation, the Government and the Armed Forces Community.
3.3 The scheme is intended to be a two-way arrangement and the Armed Forces Community are encouraged to do as
much as they can to support the civilian community and promote activity which integrates the service community into civilian life.

5 | P a g e
3.4 Recognise the status of serving soldiers and veterans through public events and other public support. 4 MEASURES 4.1 Work in partnership to co-ordinate and direct implementation of mutual support between the Armed Forces and the
community within West Lancashire. 4.2 Develop specific actions to support the delivery of agreed priorities for in service, ex service personnel and their
families where appropriate structured around the following themes:
Education, Skills and Employment
Health and Wellbeing
Families and Housing 4.3 Encourage the recognition of the Armed Forces through such activities as Freedom of the Borough, Remembrance
Parades and support to the annual Armed Forces Day. 4.4 Work with the West Lancashire community to access funding to deliver projects at the local level which support the
objectives and general intentions of the West Lancashire Community Covenant.
4.5 Report annually to West Lancashire Borough Council and Commander 42 (North West) Brigade on progress.

6 | P a g e
THE ARMED FORCES COVENANT An Enduring Covenant Between
The People of the United Kingdom Her Majesty's Government
-and
All those who serve or have served in the Armed Forces of the Crown And their Families
The first duty of Government is the defence of the realm. Our Armed Forces fulfil that responsibility on behalf of the Government, sacrificing some civilian freedoms, facing danger and, sometimes, suffering serious injury or death as a result of their duty. Families also play a vital role in supporting the operational effectiveness of our Armed Forces. In return, the whole nation has a moral obligation to the members of the Naval Service, the Army and the Royal Air Force, together with their families. They deserve our respect and support, and fair treatment. Those who serve in the Armed Forces, whether Regular or Reserve, those who have served in the past, and their families, should face no disadvantage compared to other citizens in the provision of public and commercial services. Special consideration is appropriate in some cases, especially for those who have given most such as the injured and the bereaved. This obligation involves the whole of society: it includes voluntary and charitable bodies, private organisations, and the actions of individuals in supporting the Armed Forces. Recognising those who have performed -military duty unites the country and demonstrates the value of their contribution. This has no greater expression than in upholding this Covenant.

Lancashire Safeguarding Children Board 2012 – 2013 Annual Report West Lancashire Clinical Commissioning Group Board Meeting – 24.9.13
1
WLCCGB 9/13/11 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP
GOVERNING BODY REPORT DATE OF BOARD MEETING: 24 September 2013 TITLE OF REPORT: Lancashire Safeguarding Children Board 2012 –
2013 Annual Report BRIEFING POINTS:
Does this report / its recommendations have implications and impact with regard to the following:
A. Commissioning Board’s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient
experience) – please outline impact x
To inform the Governing Body of the publication of Lancashire’s Safeguarding Children Board Annual Report for 2012/13 2. Commissioning of hospital and community services – please outline
impact
3. Commissioning and performance management of GP Prescribing – please outline impact
4. Delivering Financial Balance – please outline impact 5. Development of the commissioning group as a commissioning
organisation – please outline impact
B. Governance – please outline impact 1. Does this report:
provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number)
have any legal implications promote effective governance practice
x
Provides assurance to the Commissioning Board as to how Lancashire Safeguarding Children Board has fulfilled its statutory functions in respect of safeguarding. 2. Additional resource implications
(either financial or staffing resources)
3. Health Inequalities 4. Human Rights, Equality and Diversity Requirements 5. Clinical Engagement 6. Patient and Public Engagement REPORT PREPARED BY:
Jean Rollinson, Head of Safeguarding
REPORT PRESENTED BY: Helen Clarke, Chief Nurse

Lancashire Safeguarding Children Board 2012 – 2013 Annual Report West Lancashire Clinical Commissioning Group Board Meeting – 24.9.13
2
Lancashire Safeguarding Children Board 2012 – 2013 Annual Report
Purpose of the paper
1. To inform the Governing Body of the publication of Lancashire’s Safeguarding Children Board Annual Report for 2012/13. A copy of the report is attached for reference.
Introduction
2. Lancashire Safeguarding Children Board (LSCB) has recently published its 2012/13 annual report. The annual report aims to demonstrate the extent to which the functions of the Board, as set out in statutory guidance, have been effectively discharged and in so doing provides a rigorous and transparent assessment of the performance and effectiveness of local services.
3. The report outlines how the LSCB is structured, provides a summary of the LSCB business planning processes and details the work undertaken by the various sub groups of the board in order to fulfil its statutory functions. This includes an assessment of single and interagency training on safeguarding to meet local needs; the quality and effectiveness of arrangements and practice to safeguard children; and lessons from serious case reviews and child death overview processes during the reporting period. The report also provides information on the LSCB budget including what has been spent on child death reviews, serious case reviews and other specific expenditure such as learning events or training.
4. The report concludes with an overview of the issues and challenges for the LSCB in ensuring the effectiveness of safeguarding arrangements identifying key areas for development during 2013/14.
Key issues
5. Although there have been notable successes within safeguarding practice across Lancashire, for example, the development of the multi-agency safeguarding hub, and the LSCB child exploitation strategy having a national prominence, the LSCB has faced a number of challenges in 2012/13.
6. These challenges included a national review of child protection which culminated in the revision of statutory guidance for safeguarding children; high profile media interest in child sexual exploitation cases; the reconfiguration of the health economy; organisational restructuring of many partner agencies in response to austerity measure and the Ofsted inspection of safeguarding and children looked after services.
7. By regularly reviewing the LSCB business plan and priority areas for action the LSCB has been able to respond to these emerging issues and developments all of which are detailed in the report.

Lancashire Safeguarding Children Board 2012 – 2013 Annual Report West Lancashire Clinical Commissioning Group Board Meeting – 24.9.13
3
Actions required by Governing Body Members
8. The Governing Body is asked to:
note the content of Lancashire’s Safeguarding Children 2012/13 Annual Report.
Jean Rollinson Head of Safeguarding August 2013

LANCASHIRE SAFEGUARDING CHILDREN BOARD
ANNUAL REPORT 2012/13
Published: August 2013

2

Contents
Foreword Page 4
LSCB members Page 5
LSCB Structure Page 7
Provision of Policies and Procedures Page 7
LSCB Business Planning Cycle Page 8
Single and Multi Agency training provision Page 9
Quality and Effectiveness of Arrangements and Practice Page 11
LSCB Case Reviews Page 14
Update from the eSafety Sub-group Page 18
Update from Child Sexual Exploitation Sub-group Page 19
Update from Safe from Harm Sub-group Page 21
Update from Local Safeguarding Children Sub-Groups (LSCGs)
Page 22
Engagement with and participation of children and young people
Page 24
Equality and diversity Page 25
Priority groups of children Page 25
LSCB effectiveness, contribution and challenge Page 26
Issues and challenges facing safeguarding – statement of effectiveness of safeguarding arrangements in local area
Page 29
Conclusion and recommendations for future priorities and Business Plan
Page 30
Appendices Page 31
3

Foreword
From Nigel Burke, Independent Chair of Lancashire LSCB I am pleased to present the Annual Report from Lancashire Safeguarding Children Board.
This report is different from its predecessors as the Government has published its statutory guidance 'Working Together 2013' which came into effect on the 15th of April 2013; and amongst other things this sets out the requirement for Local Safeguarding Children Boards (LSCBs) to publish an annual report. The guidelines explain that the report should cover the effectiveness of child safeguarding and promoting the welfare of children in our area. It should provide a rigorous and transparent assessment of the performance and effectiveness of local services. The safeguarding of children and young people is challenging. It remains the responsibility of everyone in the community but it is a particular responsibility for all those organisations and individuals who work with children and young people. The challenge has been to maintain that relentless focus on safeguarding in times of financial stringency. Success is entirely dependent on motivated, well trained and highly skilled staff. Wherever I go in Lancashire I find such people. This has not lead to complacency, key decision makers come together in the LSCB to identify how we can all work better together, to identify any weaknesses and put in place improvements. I believe that partnership working in the LSCB has been exemplary and despite significant challenges for all our partners there has, if anything been a greater willingness to work actively together to find efficiencies whilst maintaining the high standards we set ourselves. There have been notable successes, the consolidation of the Multi Agency Safeguarding Hub has seen staff coming together in one place to support the safeguarding effort, our Child Sexual Exploitation strategy has national prominence and Health representation has remained strong despite the major reorganisation in the sector. Voluntary, community and faith organisations continue to play a vital role, as do the other organisations represented on the Board, and our lay member led the production of a report on a key area of interest. Safeguarding is challenging and no more so when dealing with child deaths, now undertaken by the Child Death Overview Panel that spans the local authority areas (Blackpool and Blackburn with Darwen as well as Lancashire), and serious case reviews where a child has died or been seriously harmed through abuse or neglect. The impact on all the professionals involved cannot be underestimated. We do have to learn from where there have been failings in systems or procedures but at the same time staff working with these most challenging cases need our support. The LSCB has in place robust systems for setting strategy, planning and quality assuring both its work and that of its partners. The work of the Board is well supported by a very able business management team and the Board sub-groups. I am optimistic that we can continue to improve the safeguarding of children and their welfare and hope that you will find in this report the evidence to help you share that optimism. Once again my wholehearted thanks to all those who work with our children for their effort and commitment.
4

LSCB Members
AGENCY REPRESENTATIVE
Independent Chair Nigel Burke
NHS Central Lancashire Jean Rollinson (Vice Chair) Associate Director Safeguarding (also Locality Group Chair – South & Central)
NHS North Lancashire Barbara Campbell Head of Standards, Health and Effectiveness
NHS Central Lancashire
NHS East Lancashire
Dr Ruth O'Connor (up to October 2012) Dr Diah Mahmood (October 2012 onwards) Consultant Paediatrician / Designated Doctor for Child Protection Jane Carwardine Lead/Designated Nurse for Safeguarding Vulnerable Adults & Children
Lancashire Constabulary Ian Critchley Detective Superintendant
Lancashire County Council County Councillor Susie Charles Cabinet Member for Children and Schools Helen Denton Executive Director for Children and Young People Louise Taylor Director of Specialist Services Ann Pennell Director of Targeted and Assessment Services Paul Armitage Head of Children's Social Care (Locality Group Chair - East) Paul Hegarty Children's Social Care, District Manager (Locality Group Chair - North) Mike Banks County Head of Active Intervention and Safeguarding (Adult Safeguarding Board Representative)
Lancashire Probation Trust Linda Lock Assistant Chief Executive
Children and Family Court Advisory and Support Service (CAFCASS)
Collette Dutton Head of Service, Cheshire, Merseyside & Lancashire
Lancashire Care NHS Foundation Trust
Gill Frame
5

Network Director, Children and Families Network
Lancashire Teaching Hospitals NHS Foundation Trust
Sue Reed Nursing Director
Secondary Schools Roddy McCowan Head Teacher, Baines School
Voluntary, Community & Faith Sector Debbie Fawcett HARV Outreach, Project Manager
Voluntary, Community & Faith Sector Amanda Forshaw Caritas Care, Director of Services - Children’s Services
Lay Member Abdul Haleem
District Councils Burnley Borough Council Chorley Borough Council Fylde Borough Council Hyndburn Borough Council Lancaster City Council Pendle Borough Council Preston City Council Ribble Valley Borough Council Rossendale District Council South Ribble Borough Council West Lancashire District Council Wyre Borough Council
Lorraine Norris Chief Executive Preston District Council
6

LSCB Structure The LSCB is structured as illustrated in the diagram below. The Executive group is now well established and continues to take forward the day to day business of the Board.
Provision of policies, procedures and guidance for multi-agency arrangements, to protect children and promote their welfare
Lancashire LSCB is now working in collaboration with Blackpool and Blackburn with Darwen LSCBs to provide Pan-Lancashire multi-agency safeguarding policies and procedures. These are available in an interactive e-manual (produced and administered by an external service – Tri-x) which is reviewed and updated three times per annum to account for:
• Changes in national guidance
• Themes emerging from local and national research
• Recommendations from case reviews
7

• Recommendations from quality assurance
• Learning from best practice The procedures are accessible for free, via the LSCB website at the following link: http://www.lancashire.gov.uk/corporate/web/?siteid=3829&pageid=20741&e=e
Where possible all procedures are discussed across the 3 LSCBs and agreed on a pan-Lancashire basis to assist partner agencies who work on footprints which are not co-terminus with the 3 local authority areas. However it is recognised that there will inevitably be some LSCB specific variation and this is recognised within the procedures manual.
During 2012/13 the following additional procedures/guidance have been developed or updated and agreed for inclusion within the manual:
• Multi-agency Supervision Standards
• Guidance for supporting staff following the death of a child
• Multi-agency Pre-birth Protocol
• Sexually Active Under 13s
• Procedure for the assessment of young people who exhibit sexually harmful behaviour
The LSCB Business Planning Cycle The LSCB has developed a robust business planning cycle to ensure strategic priorities and their subsequent delivery plans are effectively monitored, managed and reviewed. This is illustrated in the diagram below.
It is important to note that each sub-group of the LSCB has its own work programme based on the LSCB business plan, but also including specific priorities within the group, which is monitored on a regular basis via formal bi-monthly reports to the LSCB. These reports are discussed in detail and any subsequent corrective action agreed. At
8

the end of the year the LSCB reviews its strategy and objectives based on feedback from the sub-groups and other areas of activity as detailed above.
Single and Multi Agency training provision Update from Learning & Development Sub-group Chair: Jane Carwardine
Summary of Key Functions The principal purpose of LSCB learning & development sub-group is to promote learning and development which leads to:
• Improved practice in safeguarding Children in their context • Reduced incidence of harm to children • Better outcomes for children
The Learning & development sub Group is accountable to the LSCB and contributes to the aims of the LSCB and supports its business plan through the development of staff and organisations on a multi-agency basis. The strategic aims of the group are:
1. Identifying training and development needs for Inter-agency learning 2. Commissioning, quality assuring and evaluating Inter-agency learning opportunities, to enable staff and agencies to access appropriate learning in line with current National guidance:
a. That promotes a shared understanding of the tasks, processes, principles, roles and responsibilities and local arrangements for safeguarding children and young people and promoting their welfare
b. Improves communications between professionals, including developing a common understanding of key terms, definitions and thresholds for action
c. Promotes effective working relationships, based on respect and an understanding of the role and contribution of different disciplines, including an ability to work in multi-disciplinary groups or teams
d. Promotes sound child focussed assessments and decision making e. Promotes learning from Serious Case Reviews, Critical Incident Reviews and Reviews of Child Deaths f. Uses the available resources in the most effective way
Key actions to deliver these aims are as follows: • Develop a workforce Training Needs Analysis in line with 'Working Together 2010' guidance • Develop and review a learning and development programme that is established within the context of local
and national policies, research and practice developments • To commission the design, planning, organisation and implementation of the training/learning programme
via the LSCB strategic training co-ordinator, based on inter-agency priorities and learning from SCRs and reviews of child deaths
• To maintain links with all other LSCB sub groups in order to ascertain learning needs • Ensure that the LSCB learning programme is monitored and evaluated for quality and impact on practice • To recruit, support, develop and monitor the training pool • To ensure membership attendance of learning & development sub group is in accordance with LSCB
guidance Key priorities for 2012/13
• Develop a pan Lancashire approach to Child Sexual Exploitation training • Implement and embed revised e-learning programme • Develop a reporting process with all partners to assure LSCB that all partners comply to national guidance
regarding group 1 & 2 safeguarding training • Implement and embed on line access to LSCB training
9

• Review membership to the LSCB training sub considering organisational transition • Review the training needs of all agencies, including the voluntary and independent sector in respect of
safeguarding training • Run a core training programme of approximately 75 events covering at least 20 topics, potentially adding
further events required by the LSCB Were the priorities achieved effectively? The review of the plan is attached (see appendix 1). As can be seen, most objectives were achieved. The one objective which was not, was part of a large review and the system has been changed. How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 L& D Sub-group contributes to the work of the LSCB by developing the workforce and informing key members of the workforce about the latest developments. Through the business planning cycle above the work of the sub-group informs future LSCB priorities and development. Key Successes and Achievements for 2012/13
• 1378 professionals attended LSCB training events, and 2097 completed e-learning, making a total of 3475 professionals who came through the LSCB learning programme
• In 2012-13, L&D sub planned 80 training events. Of those, 59 ran, and 21 were cancelled. In addition, three Critical Incident Reviews, each lasting two days were facilitated.
• Held SCR briefings, jointly with Blackburn with Darwen and Blackpool LSCBs, which were evaluated and found to provide excellent learning
• Provided advice to 58 organisations which approached the LSCB Training Unit • Recruited new members to the training pool to replace the members who left • Successfully engaged the 12 District Councils in the safeguarding agenda, with the result that all now have a
safeguarding policy and most have training for their staff • Planned on-line sign up for training events, which will happen in 2013-14 • Pilot tested an electronic feedback system, initially for three months to ascertain viability and response rates • Revised e-learning course and separated it into Group 1 and group 2 • Ensured AIM training delivered was in line with the new AIM policy and procedures • Involved Children and Young people as well as parents in the delivery of the Neglect Conference in October
2012. • Successfully delivered a group 8 course in June 2012 • Developed a new Quality Assurance programme to receive feedback from the workforce on how learning
has been used following attendance at courses to influence positive outcomes on children and families. • Expanded the programme to include more ways of learning to ensure we offer a diversity of learning
opportunities which make learning and development accessible for the workforce across agencies in Lancashire. Shorter workshops have proved to be in demand.
• Developed a proposal for inter-agency, case based reflection for front line practitioners. Contributed to the Learning and Improvement Plan, which was approved by LSCB
• Wrote a Child Sexual Exploitation e-learning course, which was agreed across the three LSCBs • Wrote two new e-learning courses which are now on line • Delivered a Neglect conference • Brought new learning and research into SCR learning seminars • Provided three System-based Critical Incident Reviews (now renamed), this has included training up three
facilitators • Met six times in the year, L & D sub membership healthy and the sub works well • Contributed to the regional learning by membership and contributions to the North West Interagency
Trainers (NWIAT)group • Wrote seven new courses • Developed new ways of getting messages over, for example by bookmarks and 'best advice' cards • Proposals for practitioner forums and group supervision written
10

Quality and Effectiveness of Arrangements and Practice Update from the Quality Assurance and Performance Management Sub-group Chair: Barbara Campbell (up to December 2012), Tony Morrissey (December onwards) Summary of Key Functions
• To provide the LSCB with a qualitative and quantitative evidence base to demonstrate how effective multi-agency safeguarding practices and arrangements are
• To coordinate completion and quality assurance of the LSCB Section 11 audit across all partner agencies • To develop and deliver a quality assurance work programme based on priorities and methods specified in
the LSCB Quality Assurance Framework – namely Neglect and Child Sexual Exploitation • To oversee any improvements arising from multi-agency inspections, peer reviews or mock inspections and
inform the LSCB of any significant risks or issues Key Priorities for 2012/13
• Co-ordination and quality assurance of section 11 audits for all member agencies • Development of a strategic quality assurance framework (QAF) • Delivery of the Neglect quality assurance work programme (as specified in the QAF) • Delivery of the Child Sexual Exploitation quality assurance work programme (as specified in the QAF) • Development of a framework to assess the effectiveness of Early Intervention and the Common Assessment
Framework (CAF) • Oversight of the action plan following the safeguarding and looked after children inspection • Review of health performance data to ensure consistency and quality
Were the priorities achieved effectively? All priorities were commenced and progressed effectively during 2012/13. A new QAF was developed based on recognised best practice guidance from the pan-London model. This was ratified by the LSCB and implementation led to the agreement of priorities and work programmes with regard to Child Sexual Exploitation and Neglect as detailed below. There was some slippage on delivery of the Neglect work programme and the final activity, a multi-agency case file audit, has just been completed at the time of writing (June 2013). The development of effective QA pathways with regard to Early Support and the use of the Common Assessment Framework is still ongoing due to the current wholesale review of the Common Assessment Framework and development of the Early Support core offer. This activity will continue into 2013/14 and its conclusion reported in next year's annual report. Neglect work programme: A summary of conclusions from the neglect work programme is as follows:
• The Local Authority has comprehensive monitoring and recording processes in place around Child Protection Plans, referrals, children missing education and some very informative auditing has taken place engaging with families subject to statutory intervention
• It is a concern that there are no systems in place across agencies to capture, collate and analyse information
about neglect lower down the continuum of need
• Health indicators around immunisations, missed appointments and GP registration have proved difficult and problematic to evidence
• The Lancashire housing economy is complex and diverse and seeking assurance from housing providers is a
significant challenge. Work is ongoing to engage with housing providers and develop effective quality assurance pathways
• Planned multi-agency auditing over the coming months will provide further evidence of how effectively
agencies are intervening with families and children
11

• Findings shared with the training sub-group to inform the training priorities for next year
The LSCB will be considering how to address these issues following finalisation of the current audit, and will be reported in full next year's annual report. It is also worth noting that the LSCB has developed a Neglect Strategy which has been informed by the findings of this work – delivery of the strategy will be overseen by the Safe From Harm sub-group and reported fully in next year's annual report Child Sexual Exploitation work programme A summary of conclusions from the Child Sexual Exploitation work programme is as follows:
• Child Sexual Exploitation practices and procedures are very well developed in Lancashire and all aspects of the frame work have been evidenced to a good standard with any areas for future development identified. A number of local and national action plans have been delivered and the strategy and operating protocol effectively embedded
• Child Sexual Exploitation is a high priority locally and nationally and Lancashire Police are leading the way in
partnership with other agencies. The children's commissioner on a recent visit commended the work in Lancashire as a 'beacon of excellent practice'
• There are no identified areas of weakness or gaps to note from this analysis. The areas for development are
recognised and planned for implementation in due course The LSCB has been assured that this area of practice is being effectively addressed by partner agencies in Lancashire. Following this quality assurance activity and implementation of the Child Sexual Exploitation strategy a programme of E-learning has been developed through the Learning and Development Sub-group. Practitioner Survey A survey of over 700 practitioners across all LSCB agencies was completed to ascertain how effective they felt their agencies were in dealing with safeguarding issues and how confident they personally felt at dealing with a range of specified safeguarding issues. The results have been shared with all LSCB agencies who have been asked to consider how they will respond to issues raised. A copy of the report can be accessed at the following link: http://www.lancashire.gov.uk/corporate/web/view.asp?siteid=3829&pageid=31195&e=e How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 As detailed above the work of the sub-group informs the LSCBs priorities through the robust business planning cycle and regular progress updates to the LSCB on priorities specified in the work programme. The 'Toxic Trio', which refers to the combination of parental drug misuse, domestic abuse and parental mental ill health, has been identified through the QAF as a priority for 2013/14 which follows on from issues raised through the work on Neglect and shared learning from the Case Review Sub-group. Key Successes and Achievements for 2012/13
• Development and implementation of a new quality assurance framework • Development of a new section 11 audit tool • Completion of all section 11 audits by partner agencies • Completion of the neglect audit work programme • Completion of the Child Sexual Exploitation work programme • Development of a health performance dataset • Completion of a multi-agency practitioner survey of over 700 practitioners • Development of LSCB multi-agency safeguarding practice inspections
LSCB Section 11 Audit The Section 11 Audit is a self assessment tool which the LSCB requires all statutory agencies to complete to evidence compliance with section 11 of the Children's Act 2004 – the duty to safeguard. (See appendix 2)
12

The LSCB section 11 audit follows a triennial business cycle as follows: Year 1 – All agencies complete section 11 audit and receive feedback following quality assurance
with any improvements required clearly specified using a 'RAG' rating (Green=compliant, Amber=partially compliant, Red=non-compliant)
Year 2 – Update on areas for improvement Year 3 – Update on areas for improvement
September 2012/13 marked the start of year 1. At this point the LSCB had been assured that any areas for development / improvement for all applicable agencies from the previous audit had been effectively addressed or were progressing. A new audit tool was developed to ensure information captured was more concise and relevant with regard to the requirements for organisations specified in the guidance. The previous tool was felt by agencies to be rather unwieldy and overly prescriptive. The audit tool can be viewed at appendix 2. All statutory agencies completed the audit tool. This includes the following agencies:
• Central Lancashire PCT (provider & commissioner) • North Lancashire PCT (provider & commissioner) • East Lancashire PCT (provider & commissioner) • Lancashire Care NHS Foundation Trust • East Lancashire Hospital NHS Foundation Trust • Lancashire Teaching Hospitals NHS Foundation Trust • Calderstones NHS Foundation Trust • Blackpool Victoria Hospital NHS Foundation Trust • University Hospitals of Morecambe Bay NHS Foundation Trust • Southport & Ormskirk Hospital NHS Foundation Trust • NHS East Lancashire Community Health Services • Lancashire Constabulary • Probation • Cafcass • Lancashire County Council • Chorley BC • West Lancs BC • Wyre BC • Fylde DC • Lancaster CC • Preston CC • Rossendale DC • Burnley DC • Pendle DC • Hyndburn DC • Ribble Valley DC • South Ribble BC
The LSCB Quality Assurance sub-group maintained oversight of the submission of returns and a process of quality assurance was agreed as follows:
• LSCB Business Coordinator to make an initial screening of returns to identify any obvious issues or omissions • 3 key statutory agencies to be randomly selected to receive a site visit from a small multi-agency team of
peers to look at supporting documentation and speak to key members of staff about the audit • LSCB Business Coordinator to visit 3 randomly selected District Councils for a site visit to check supporting
documentation and speak to key staff about the audit These site visits are planned for completion in 2013/14 and results from these will be reported in the next annual report. Themes from the returns
13

Within the S11 audit returns agencies identify a number of issues to address, progress in resolving these will be tested through annual updates to the QA Sub-group as well as the QA site visits referred to above. Key themes from the screening exercise have revealed the following:
• All organisations have a designated senior officer • All organisations can demonstrate policies and procedures are in place • Safeguarding Supervision arrangements are often not in place – statutory agencies (especially health
agencies) recognise this is an area for development • Evidence of staff training to the required 'levels' is variable – few organisations can demonstrate all staff
have received the appropriate training • Use of the Common Assessment Framework (where referred to) appears inconsistent and patchy • All organisations appear to have at least the essential safe recruitment practices in place, links to the
Local Authority Designated Officer for Allegations (LADO) not always robust • All agencies understand the need to share information and all appear to have appropriate arrangements
with key partners, though this varies depending on the nature of the organisation
LSCB Case Reviews Update from the Review Group Chair: Louise Taylor Summary of Key Functions:
• To consider, at the request of the Chair of Lancashire LSCB, whether a Serious Case Review should take place, and make recommendations to the LSCB Chair who has ultimate responsibility for deciding whether or not such a Case Review should be conducted
• To consider, in the light of each case, the scope of the review process and draw up clear terms of reference and identify any specific expertise needed for the Overview Panel including nomination for independent Chair and Author
• To monitor the SCR process and to oversee changes to this process • The review group will be required to have over sight of all multi-agency action plans and will need to have a
scrutiny role in relation to all single agency action plans. Recommending to LSCB when a SCR can be signed off as being completed
• Advising and facilitating the QA Sub group's role in distilling key learning and audit Key priorities for 2012/13
• To undertake serious case reviews and multi agency learning reviews when appropriate • To ensure that there is an effective system is in place for the monitoring of action plans and dissemination of
learning from case reviews • To adopt any new methods and processes for completing SCRs and CIRs that may come from revised
statutory guidance • To enable and support practitioner development in light of SCR and CIR findings • To develop process of completing good practice reviews and link into best practice panels
Were the priorities achieved effectively? All cases that potentially met the criteria for a serious case review or multi agency learning review were referred into the SCR group in a timely manner. All those cases were considered by the group and a decision reached by the chair of the LSCB within one month of referral. The group considers the progress of all single and multi agency action plans on a bi-monthly basis and takes necessary action when there are felt to be unacceptable delays in implementing learning. The findings from all reviews are also shared with the Learning and Development sub group and Quality Assurance sub groups in order that they reflect them in their work programmes.
14

The SCR group has developed more effective and inclusive models of learning from reviews and has been involved in developing these on a regional basis. The feedback from practitioners about these models has been overwhelmingly positive; they all believe their future practice has changed for the better. The dissemination of lessons from reviews has continued throughout the year. There are regular newsletters that are widely shared throughout Board agencies and the Children and Young People's Trust. The large scale multi-agency SCR briefings continue to be updated and delivered and the actions practitioners take as a result of their attendance at these events continues to be monitored. How do these reflect learning and developments from the previous year? The review group felt that the process for completing reviews was not as effective as it could be and welcomed the findings in the Munro report that suggested a different approach to learning from cases. The group was keen to ensure that practitioners were much more involved with the process of reviewing cases and therefore volunteered to be part of a pilot of a systems methodology being undertaken by the Social Care Institute for Excellence (SCIE). As a result of learning that came from this pilot, the SCR group developed a new model of reviewing cases that didn't meet the criteria for an SCR. This involved practitioners coming together to discuss a case and reflecting on what worked well and what could be improved. They then help to develop that learning to share more widely with other practitioners. The SCR group has completed a number of multi agency learning reviews over the last twelve months and used the findings to develop training and learning events for all staff. The new Working Together guidance will now allow us to develop this successful model of learning to serious case reviews too, and we have been working with neighbouring authorities to develop a consistent framework for this. The monitoring of actions emerging from SCRs and other learning reviews has ensured that the messages and learning are being shared widely across partner agencies. How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 Building on the success of these new models of reviewing cases, the LSCB has developed a proposal for group reflection which is now being piloted. The issue of the 'toxic trio' (combined effect of parental substance misuse, domestic violence and mental health issues) has been present in a number of reviews locally and nationally and has been adopted by the QA sub group as their topic for QA activity for the coming year. The findings from case reviews have assisted in the development of the training programme for the coming year, in that all the lessons are built into existing training courses and new ones are developed where necessary. In addition, a programme of 'bite-sized' briefings around topics that emerge from case reviews will be delivered, and larger conferences around specific topics, such as neglect are also planned. The issue of assessment quality has been incorporated into the LSCB Business Plan for the coming year as a result of potential inconsistencies revealed through case reviews. Key Successes and Achievements for 2012/13 The SCR group continued to hold agencies to account to demonstrate that they learn from cases when appropriate, meaning that there is a continual process of improvement in working with children and young people across agencies. For example, new supervision guidance has been developed as a result of a serious case review, and the LSCB tests the implementation of this through the s11 audit process. The new method of reviewing cases has been a huge success for practitioners and they believe their practice with children and young people has changed for the better. Their engagement in the process has made the learning far more effective which in turn will benefit all children and young people that come into contact with professionals across all partner agencies. This in turn has led to the development of other new ways of engaging with practitioners to ensure the best learning outcomes for them, such as reflective practice sessions and bite-size briefings. The ongoing briefings of staff, on a single and multi-agency basis, has led to a wider understanding of the themes from case reviews, and has given staff tools to use in their practice.
15

Themes from Case Reviews concluded during 2012/13 Lancashire Safeguarding Children Board concluded two serious case reviews (SCRs) during this year and four multi agency learning reviews (for cases that didn't meet the criteria for an SCR but offered a learning opportunity). The LSCB has also undertaken a number of best practice reviews, and the learning from all these processes has been brought together to inform the training programme for the current year, implement improvements in processes and procedures and drive improvements to practice across the County. The findings from all of these review processes can be grouped into broad themes; the first of which is around human behaviour. All the reviews found that practitioners were hard working, committed and really cared about outcomes for the children and young people they worked with. The time and energy that people put into their work is commendable. The LSCB wants to build on this passion and help practitioners to develop their practice even further. Some of the' human themes' that have emerged are natural human behaviour; such as wanting parents to do their best for their children, and believing people when they state their commitment to parenting their children properly. The LSCB has done a great deal of work with practitioners about sceptical curiosity and hypothesising (a tool for practitioners to use to challenge their assumptions about what they see). In addition, the LSCB has worked hard to provide an environment in which practitioners are comfortable in being challenged by others, and comfortable to challenge other practitioners when they don't believe a decision is right for a child. Supervision standards have been developed, and reflective practice is encouraged through the use of multi agency learning reviews, best practice panels and the soon to be operational practitioner forums. There have also been areas for development identified in the tools that practitioners have available to them in their work. The LSCB has become involved in the Graded Care Profile pilot, in the hope that this will deliver an effective way of assessing neglect and its impact on children. The Common Assessment Framework and Continuum of Need are being refreshed, alongside new Thresholds Guidance for practitioners and the LSCB will monitor the roll-out and use of these refreshed processes. The single assessment framework is being developed and will take account of the findings from reviews around the quality of assessments and the use of historical information to judge risk to children. Update from the Child Death Overview Panel (CDOP) Chair: Dr Shelagh Garnett Summary of Key Functions
• To review all child deaths pan-Lancashire • To identify themes and trends and make recommendations to try and prevent future child deaths • Monitor the Sudden Unexpected Death in Infancy (SUDI) Prevention Group and the Safer Sleep Campaign • Ensure there is a coordinated response to each unexpected child death
Key priorities for 2012/13
1. The Panel will review cases and make recommendations regarding themes to the Board 2. CDOP will develop links with other Local Safeguarding Children Board Sub-Groups particularly the Safe from
Harm Group 3. With Public Health department investigate apparent disparity in numbers of deaths between CDOP and ONS
data 4. Further detailed review work to identify themes / trends in deaths categorised as caused by perinatal
/neonatal events 5. The Panel will monitor the re-launch of the Give Me room to Breathe (GMRTB) Campaign 6. CDOP will ensure the Safer Sleeping Guidance is reviewed 7. Ensure and monitor the review of the SUDC Protocol 8. Finalise the multi-agency e-learning and make available to professionals front line multi-agency professionals 9. Develop a Pan-Lancashire communications strategy for disseminating messages and information on a multi-
agency basis 10. Monitor Multi-Board CDOP Budget and develop action plan for utilising the under spend
16
11. Update the data recording/analysis systems to improve reporting on specific modifiable factors identified by the Panel
How do these reflect learning and developments from the previous year? In the 2011/12 annual report it was identified a significant proportion of children died as a result of a perinatal/ neonatal event; consequently further research into this cohort of child deaths was identified as needing an in depth review. When Public Health started this review it was identified they would be best placed to investigate the disparity in data between CDOP and ONS. The data from the previous year identified that for children under one year of age who died unexpectedly, one of the largest categories was sudden unexpected, unexplained death; the risk factors identified within this group were related to safer sleep – which features as a key priority for 2012/13 as above. The SUDC Protocol was approved by the three Boards in 2011, it was suggested it should be for review after 1 year this has been delayed pending the release of the new guidance. In this time, the SUDC Service has had a number of staff changes, system and service developments and consequently the SUDC Protocol review still remains a priority for the Panel going into 2013/14. It was identified that e-learning would be the best method for reaching the multi-agency workforce. The e-learning will inform professionals of CDOPs systems and processes but more importantly, raise awareness to the themes and trends emerging and provide additional contacts and resources for further information. One of the Panel's main functions is to identify themes and trends; the Panel were aware that they collate a large amount of detailed data without the ability to efficiently extract the information and report on it. As a consequence, it was identified a database (rather than excel spreadsheets) would significantly improve the reporting mechanisms of the CDOP particularly in relation to modifiable factors. Were the priorities achieved effectively? (See Appendix 3) Most priorities were achieved effectively. The review of the SUDC Protocol was delayed pending the release of Working Together 2013 and is now a priority for 2013/14. How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 The Panel has regular reporting to the Boards which informs future planning, gaps in service or areas for update/ improvement. The reporting is bimonthly (includes themes and trends from case discussions and issues, recommendations from the business meeting), quarterly statistics are provided and an annual report identifies themes and trends from aggregated data. The CDOP Chair attends and contributes to the annual Board development day. Key Successes and Achievements for 2012/13 The SUDI Prevention Group, a sub group of CDOP, updated and re-launched the Safer Sleep Campaign (previously Give Me Room To Breathe). The Campaign will provide professionals with a consistent message and materials to give parents/ carers for discussing safer sleep. The Campaign aims to inform parents/ cares of the risks associated with safer sleep for babies to help them make an informed decision in relation to bed sharing and consequently make children within pan-Lancashire safer. The CDOP monitored the update and review of the Safer Sleeping Guidance which has been ratified by the three LSCBs and has informed the development of the Safer Sleep Campaign. This was a challenging piece of work which provides frontline staff across pan-Lancashire with clear and consistent evidence based information to support them in having open and honest discussions with parents/ carers about safer sleeping choices. The Panel set up and monitored the Suicide Thematic Task and Finish Group which completed an in depth review of the child deaths which were deemed to be as a consequence of the child/ young person's own actions. The group identified recommendations to be considered by the LSCBs and the report has been shared widely on a multi-agency basis.
17

The CDOP developed posters for professionals and GPs to advise them who to contact to initiate the rapid response and who to notify should a child die in a manner that was expected. This will improve the notification process, ensure relevant systems are initiated and parents/ carers/ families are supported in a timely manner. The Panel has completed a survey of available bereavement services within the pan-Lancashire area; this information is being distributed to GPs and will be included in the updated SUDC Protocol. The CDOP have successfully completed their first year as a tri-partite Panel utilising a rota system for Acute Trusts professionals, Community Health colleagues, Public Health, Children's Social Care and Education representatives.
Update from the eSafety Sub-group
Chair: Graham Lowe (Schools ICT Manager) Summary of Key Functions:
• To develop and oversee delivery of the LSCB eSafety Strategy and Action Plan (including review and monitoring)
• To provide specialist advice to the LSCB on eSafety issues • To provide a forum for sharing single agency practice and developments and provide mutual support • To act as a central point of contact and advice for strategic eSafety issues • To share resources and take forward actions as agreed by the group • To provide regular reports to the LSCB on progress with the Action Plan and contribute to the LSCB Annual
Report • To take forward initiatives and projects as directed by the LSCB
Key priorities for 2012/13 • Continue eSafety Group as a forum for sharing good practice and developing eSafety provision across
member agencies • Enhance awareness of Online Safety issues across stakeholder groups • Maintain and develop the eSafety Group and network of colleagues • Establish a conference activity to engage stakeholders across the region and raise awareness of Online
Safety • Facilitate activities to engage with C&YP on Online Safety activities • Establish and develop links with related agencies and groups (local, regional and national) • Support stakeholder groups in developing Online Safety practices and procedures • Review the existing 2009-2013 eSafety Strategy • Establish definitive local evidence re: Online Safety issues and areas where stakeholders require support • Engage with C&YP to establish concerns and areas requiring further development • Establish overview of current activity across region • Investigate potential for Pan-Lancashire approach to Online Safety with Blackpool, Cumbria and BwD
colleagues • Develop links into national representative forums to promote Lancashire issues • Improve safe access for C&YP in non-school environments
How do these reflect learning and developments from the previous year? • Additional support pathways from national developments • Awareness raising continues to be a priority for all key agencies • Key agencies and individuals continue to provide the most effective support and expertise. More strategic
leadership needs to be developed going forward Were the priorities achieved effectively? 2012/13 has been the most challenging year to-date for the group, particularly as a result of organisational change (majority of eSafety-related activity historically achieved through Schools’ ICT Centre which was ceased and disaggregated in 2012) – current and future position of the various functions is still awaiting clarification though much of the existing provision (e.g. LGfL eSafety) currently remains available as a legacy of the previous service.
18

The majority of the priorities identified above have been achieved to varying extents. Particular successes identified under Key Successes and Achievements below. How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 Whilst much will be dependent on the results of organisational changes, there is significant potential to effectively progress Online Safety on a much greater and more effective scale, particularly if a co-ordinated approach with associated multi-agency partners and wider regional colleagues can be established. However, since its inception, the LSCB eSafety Group has achieved its successes predominantly as a result of committed individuals and local priorities. In order to maintain and build upon these successes, there is a need to formalise the position of Online Safety as a priority area for partners which will require strategic leadership. Subject to approval of the revised Strategy and Action Plan, forthcoming priorities for the Group for 13/14 and beyond will include:
• Commitment from partner agencies and senior members to progress Online Safety as a defined priority area • Development of the Pan Lancashire & Cumbria eSafeguarding Strategy • Establish the Pan-Lancashire eSafeguarding Group (existing eSafety Group will continue during interim) with
agreed ToR/Key Functions • Review of Lancashire membership to ensure appropriate representation • Development of respective Action Plans to address local priorities (e.g. reflect ESL event findings) • Identify appropriate support and resourcing to implement Action Plan priorities • Increased co-ordination of activities across the region • Increase engagement with related internal partners and external agencies to enhance and support the
progression of Online Safety for C&YP across the region
Key Successes and Achievements for 2012/13 • Continuation of LSCB eSafety Group in challenging organisational circumstances • Support and participation in Cover-IT-Live sessions • Support for Safer Internet Day 2013 through themed advice and guidance • Links established with Pan-Lancashire partners • Maintain Lancashire presence on National eSafeguarding Group • Progression towards cohesive Pan-Lancashire & Cumbria approach to Online Safety • Raising Lancashire issues at National level (e.g. AskFM Tip sheet) • Progression and raising awareness of eSafety agenda into related areas and stakeholder groups • Provision of expertise and experience to colleagues looking to address eSafety in respective organisations • Increased networking with recognised expertise to support the successful progression of specific Lancashire
issues • Continuation of eSafety presence at locality events (e.g. Chorley Clockwise) • Increasing number of eSafety ‘marketplace’ at related events and conferences • Continuation of Y6 transition activities re: Information Privacy • Raising awareness of eSafeguarding issues with senior figures in related agencies • Involvement in supporting the updating/development of Online Safety resources for related partners • Planning and preparation for eSafety Live (ESL) in Lancashire 2013 sessions to take place on 25th April 2013
Update from Child Sexual Exploitation Sub-group Chair: Ian Critchley Summary of Key Functions: To set a strategic approach to CSE across the County, to quality assure and monitor agencies compliance of CSE policies and procedures. To respond to emerging threats and reduce the risk of exploitation and abuse of our children and young people
19

Key priorities for 2012/13
• Quality Assurance framework around CSE • Increased work with all diverse communities regarding awareness of CSE and confidence in • the service provided • Develop approach to targeted organised criminal groups committing CSE • Develop public safety awareness campaigns re CSE • Undertake activity to obtain feedback from young people who have been exploited regarding • the service they received in order to continually seek to develop service improvement • Review and Develop training for all frontline professionals re awareness of CSE
How do these reflect learning and developments from the previous year? Child Sexual Exploitation remains a significant issue in Lancashire for the Safeguarding Board. There has been national media focus on this area of our protecting people strategy. In Lancashire across our 6 policing divisions we have led the way in terms of the approach we have taken to tackling the issues with our partners. We must continue to review our approach to safeguarding and preventing children from abuse and exploitation and ensure we bring all perpetrators to justice. Were the priorities achieved effectively? Increased work with all diverse communities regarding awareness of CSE and confidence in the service provided The Deter team - Preston, has benefitted by identifying and establishing community contacts through the local Police and Communities Together (PACT) meetings and the City Council’s Community Engagement Team. These community contacts work with the team to prepare and present briefings to promote awareness of CSE within their own communities. The next step in this initiative to increase the knowledge and skills of ‘Community Champions’ to inform the way in which vulnerable young people are identified and supported within the community. There are a number of projects across the county which have identified concern about the tolerance to exploitive behaviour amongst individuals, groups and communities. The following are just some examples of the awareness raising work being undertaken in our communities to tackle these issues. The Children’s Society - provide a service known as ‘Respect U & Me’ in a Lancashire school where two groups of young men of Asian heritage were identified as displaying demeaning behaviour towards females (both their peers and women in general) and there was evidence of some elements of exploitative behaviour in their personal relationships. The Children’s Society worked with the groups on ‘respect and healthy relationships’ which culminated in the group producing a leaflet on key messages about respecting others this leaflet will be shared with other young men.
Streetlink - an established, voluntary organisation in Preston, provides street based services for sex workers and young people at risk of being involved in prostitution. Their local knowledge and ability to communicate on the street enable their workers to identify and provide targeted intervention to children at risk of CSE being drawn into street sex work. Develop approach to targeted organised criminal groups committing CSE The Constabulary continue to target all those suspected of sexually exploiting children and young people. An investigation into individuals associating in an organised criminal group has been successfully prosecuted at Crown Court. The lessons learned from this case will enable police and their partners to refine the targeting, investigation and prosecution of organised groups. Develop public safety awareness campaigns re CSE September 2012 - The sub group co-ordinated a week long CSE awareness campaign between the 17th September and the 21st September 2012. This campaign was designed to raise awareness and inform and empower the public, especially young people about Child Sexual Exploitation. Events arranged during the week including the use of the media and social media highlighted how successful collaborative working of agencies addresses and tackles the issue of CSE within Lancashire.
20

Undertake activity to obtain feedback from young people who have been exploited regarding the service they received in order to continually seek to develop service improvement The Lancashire co-located teams include statutory and third sector providers. The co-located model provides an essential hub, in which the partners identify the needs of the victim and their family and work together to safeguard, support, investigate and bring offenders to justice. Our VCFS partners are crucial members of the teams and include Brook, The Children’s Society, PACE, and Barnardos. Intensive outreach workers, in the Children’s Society’s Street Safe Lancashire (SSL), provide valuable support to children and young people, at risk of or involved in sexual exploitation, from report through to the court process. They are co-located in 5 of our divisional teams, where they provide support to victims as part of an integrated package of multi-agency intervention. Between October 2012 and March 2013, SSL supported 172 children and young people with interventions which raised awareness of grooming, CSE, healthy relationships and protective behaviours. These continued whilst they were needed by the victim and for varying periods from between 2-3 months and a few years, where young people struggled to cope and build resilience. They have also delivered 151 group sessions in children’s homes, schools, colleges and youth groups. Parents Against Child Sexual Exploitation (PACE) parent support workers provide independent, non-judgmental and confidential support to parents, they understand the rights of parents and carers. They listen to concerns, give information on statutory agencies, court procedures and pass on advice from other affected parents. PACE workers help find the best solution for each family. They are co-located in 3 of our teams and have supported 25 families during October 2012 – March 2013. Both The Children’s Society and PACE are positioned to feedback to the teams the views and opinions of young people and their families of the service they were given and how we, as professionals could improve this experience. Review and Develop training for all frontline professionals re awareness of CSE The members of the LSCB have developed a CSE training package for practitioners; the one day training is delivered by experienced staff who work in the CSE Arena on a daily basis. The feedback from participants of the course has been excellent. A course for Managers is now being written and will be rolled out in autumn 2013. The LSCB CSE E-Learning package received agreement in February and is now ‘live’ this resource is available for all agencies and is aimed at staff who come in to contact with children during their daily work not necessarily as their primary role.
Update from Safe from Harm Sub-group Chair: Louise Taylor Summary of Key Functions:
• Overseeing partner agencies contribution to the CYPP regarding Safe From Harm outcomes • Support development of policies, procedures and strategies in relation the Safe From harm outcomes • Identify cross cutting countywide procedures and developments and work towards a more integrated
approach and work with other groups and partners to ensure integration. • Ensure policies and procedures are developed and revised to enable delivery of priorities in the CYPP • Link with the three other priority groups to identify safeguarding concerns and evidence of good practice. • Identify opportunities for preventative work and early intervention
Key priorities for 2012/13 • Neglect • Missing Children • Domestic Abuse
21

• Bullying • Fewer Children are killed or seriously injured in road traffic accidents • Children who sexually offend
How do these reflect learning and developments from the previous year? Neglect Following the report on the Safeguarding Quality Assurance Framework on Neglect brought to the group and an audit to take place on 65-70 case files in May 2012, it was agreed that some actions and outcomes should be added to the 2012/2013 action plan Missing Children It was agreed that the outcome relating to this priority should remain with the group as it is a high profile area of work Domestic Abuse After discussion of a pilot perpetrator programme in Blackpool the group agreed that focus needs to be on what support is given to children pre CP plan threshold as per the safeguarding and looked after children inspection report. A sub group will be set up to look at what support is available and where there are gaps to ensure consistency of provision. The outcomes will inform the action plan. Bullying Following discussions on cyber bullying and the problem of bullying which occurs outside of school where perpetrators attend the same school further developmental work will be carried out and will therefore remain a priority for the coming year Road Traffic The strategy is being revised and the outcomes will inform the action plan
Children who sexually offend A thematic inspection will take place in June 2012 and links have been made to identify four young people who meet the criteria. It was appropriate therefore that this should remain on the action plan Were the priorities achieved effectively
• Pupil Attitude Questionnaire shows an improving picture of bullying. An anti bullying charter has been developed
• There has been a significant reduction in children killed or seriously injured on Lancashire roads • The number of incidents of domestic violence involving children has reduced • Good feedback was received around the Neglect conference • Where signs have been installed on the 20's project and there is still a speeding issue, a number of systems
have been put in place, these include smiley faces, banners for school gates and school road watch where those caught speeding have been asked to attend a Q & A session with the schoolchildren
• A flowchart around protocols for children missing from care, missing from home and missing education was drawn up to look at any duplication across the services, this shows that there is good partnership working and minimal duplication and overlap
How has the work of the sub-group contributed to the LSCB's priorities in 2013/14 Informative presentation of the statistical data for Children Missing (previous concern of disparity between CSC and Police Data) The anomaly addressed and further work now planned to review arrangements for conducting "return home interviews" will be picked up by the LSCB Task and Finish Group. Work streams around domestic abuse or substance abuse links into the LSCB neglect strategy, which will be linked to the toxic trio as well as workforce development. Key Successes and Achievements for 2012/13
• Development of the anti bullying strategy and charter • Development of a multi-agency neglect strategy and successful conference
22

• 108 schools using the road safety products on Moodle • Successful campaign on the 20's speed limit across Lancashire • Reduction in the number of children and young people being seriously injured in road traffic collisions • Implementation of a Pan Lancashire procedure for children/young people who display sexually harmful
behaviour • Missing from home strategy finalised • The initial feedback from the YOT inspection around young people who sexually offend showed a strong and
overarching strategy and good communication between services alongside excellent multi-agency working
Update from Local Safeguarding Children Sub-Groups (LSCGs)
The LSCB has 3 Local Safeguarding Children Sub-groups which cover the following districts of Lancashire
• Lancaster, Fylde and Wyre • East Lancashire (Hyndburn, Rossendale, Burnley, Pendle and Ribble Valley) • Central & South Lancashire (Preston, Chorley, West Lancashire and South Ribble)
The LSCGs discharge LSCB functions at a local level and advise the LSCB of local issues and developments to ensure the LSCB reflects the diversity of need across the whole of Lancashire.
East Chair: Paul Armitage Central Chair: Jean Rollinson LFW Chair: Paul Hegarty Summary of Key Functions
a. Develop a work programme to ensure effective delivery of specified Strategic Objectives in LSCB annual plan b. Build and sustain local partnerships within LSCGs to ensure the effective delivery of that programme c. Report as required to LSCB, on progress on all aspects of the LSCG work programme, identifying any risks or
barriers which may impact on the achievement of identified objectives d. Assist and contribute to the production of the LSCB annual report on the effectiveness of safeguarding in
Lancashire by giving a local perspective on operational issues and emerging themes. e. Provide a named person to link with each of the District Trusts in their area and ensure regular reporting
and discussion around safeguarding issues f. Participate in discussions around the local planning and commissioning of children’s services to ensure that
they take safeguarding and promoting the welfare of children into account g. Ensure that lessons emerging from any local or county case reviews are well disseminated and partner
agencies are implementing actions plans effectively h. Undertake local multi-agency audits and peer reviews of child protection processes to ensure practice is
effective and improving outcomes for children i. To scrutinise Performance Management and Quality Assurance data at a local level to identify good practice
and areas for further development
Key Priorities for 2012/13 • Identify local consultation channels and mechanisms • Develop and implement consultation plan at county and local level • Review of thresholds re: Child Protection & Common Assessment Framework • Review the understanding of thresholds across agencies • Review the implementation of thresholds across agencies • Reporting arrangements between LSCGs and DCTs are agreed and implemented • LSCGs to create a local communications strategy to include:
- Serious Case Review Learning - CDOP Case Reviews and learning - Improve and update Website - Scope new communication mechanisms / social networking
23

- Publicising LSCB and Safeguarding - Specific Campaigns - Engaging with diverse communities - Ensure themes inform single and multi-agency planning
• Improve governance and function of LSCGS • Assurance that local arrangement for private fostering are effective • Develop methods of learning from best practice
How do these reflect learning and developments from the previous year? LSCGs were re-launched in the previous year to bring activity into line with the new strategy and business planning framework. Learning and activity was collated into the production of the new business plan and a more focused SMART work programme developed for this year with priorities informing and being informed by the LSCB Business Plan. Were these priorities Effectively Achieved A review of the work programmes for each sub-group has provided evidence that each LSCG has largely achieved most of the priorities specified. There has been some local variation in how these have been implemented, especially around learning from best practice, which continues to be developed in 2013/14. The Local Authority has provided a wealth of locally reflective performance information and data which has informed a number of discussions and provided assurance around the application of thresholds and CP processes. How has the work of the sub-groups contributed to the LSCB's priorities in 2013/14 As stated above the sub-groups report bi-monthly to the LSCB on progress with their work programmes which are reviewed annually in line with the business planning cycle to inform priorities for the next year. Key Successes and Achievements for 2012/13
• Completion of local audit in relation to private fostering • Completion of local audit of CP referrals (Central Lancashire) • CDOP annual report presented and discussed at all LSCGs • Case reviews considered at a local level and learning disseminated • Best practice panels successfully established at North and East LSCGs • Membership refreshed • Regular updates and assurance provided from CART Manager re thresholds and referral process
Engagement with and participation of children and young people The LSCB identified participation and engagement with young people as a priority for 2012/13 and has now established effective links with the local Children and Young People's Participation Officer who meets regularly with the LSCB Coordinator to identify where the LSCB can be involved in planned activity and vice versa. The LSCB has involved young people in a number of initiatives throughout 2012/13 as follows: Engagement in national 'take over day' via Lancaster Young Advisors - a young person co-chaired the LSCB meeting which proved a rewarding and useful experience and challenged LSCB members to ensure dialogue is meaningful and accessible to young people. Inclusion of 2 young people, via Chorley Youth Council, on the 'Cover it Live' panel which was established by the eSafety sub-group to answer live questions (via Twitter) regarding cyber-bullying and acceptable behaviour on line. Commissioning Lancaster Young Advisors to complete a research project and produce a suite of resources for gaining the views of primary school age children with regard to safeguarding issues. This work is currently ongoing and a full report will be available for the next annual report.
24

Involvement of a group of young people in the Neglect Managers Conference to raise awareness of the impact on children and young people. This presentation was particularly well received by participants. Completed a survey involving over 100 young people through district youth councils to ascertain their views on safeguarding and what they feel LSCB priorities should be. The results of this informed the review of the LSCB strategy and were shared with locality groups so locally specific issues could be addressed – for example the district councils in East Lancashire noted the number of young people who did not feel safe in parks or leisure centres and this will inform future service planning and development. The report can be viewed at the following link: http://www.lancashire.gov.uk/corporate/web/view.asp?siteid=3829&pageid=31195&e=e
Equality and diversity The LSCB and it members recognise that Lancashire is a large and diverse county with huge local variation in need and the composition of local populations. The LSCB has a lay-member who also provides a BME perspective to the business of the Board and all members are required to comply with equality requirements as laid out in statutory guidance and legislation. Recognition of the diverse needs of different groups of children is central to all areas of LSCB business. Every effort is made to ensure the views of all groups are gathered to inform service developments and business planning.
Priority groups of children
The following groups of children are recognised by the LSCB as potentially experiencing greater vulnerability:
• Children in Custody • Children who are privately fostered • Children experiencing neglect (see QA sub-group update) • Children who are sexually exploited (see QA sub-group update) • Children with disabilities • Children Looked After, particularly those moving out of or into Lancashire
The LSCB receives an annual report from the County Youth Justice manager to be assured that young people in custody are being effectively safeguarded. This report was considered and accepted by the LSCB in May 2012. The report assured the LSCB that 100% of YOT assessments were completed within timescales for young people prior to detention, during and post release. The LSCB was also assured that effective arrangements were in place to identify and respond to any safeguarding issues within the secure estate. The LSCB also receives an annual report from the Local Authority on privately fostered children. This was received in July 2012 and accepted by the LSCB. The following key points were noted:
• All cases related to social care issues • Publicity activity continues to raise awareness effectively • There has been an increase in notifications • All statutory visits have taken place in line with national standards • There were no disqualifications or significant concerns with regard to carers suitability
With regard to children with disabilities (CWD), a report from the local authority CWD Service Manager was presented to the LSCB in January 2013 which concluded that that arrangements for safeguarding Children with Disabilities are robust and effective which was supported through key findings from the recent Ofsted inspection. It was agreed an audit of cases should be carried out in relation to the current practice guidance recommendations which is progressing through the QA Sub-group due for completion in 2013/14.
25

In addition to these priority groups the LSCB receives an annual report from the Local Authority Designated Officer (LADO) with regard to the management of allegations against people working with children and young people. The report was presented to the LSCB in November 2012 and the following key points noted:
• More initial considerations and requests from the Police were impacting on capacity • Health referrals are very low – the LADO is looking into this to establish why • Little change in referrals from other agencies
Overall it was felt the service is effective and robust and there were no concerns expressed.
LSCB effectiveness, contribution and challenge The LSCB determines its own effectiveness largely through the business planning cycle referred to above. The business plan is developed and monitored by the LSCB Management Team and presented to each LSCB Executive and Board meeting for scrutiny and challenge and to agree any corrective action where tasks or activities are not progressing as planned. The LSCB business plan showing the end of year position for 2012/13 can be viewed at appendix 4. In addition the LSCB also has a basket of performance indicators which are monitored by the LSCB through a quarterly performance report. The indicators which relate to the effectiveness of the LSCB, with the year end returns, are as follow: Indicator EoY
2011/12 Q1 Actual
Q2 Actual
Q3 Actual
Q4 Actual
Target Direction of Travel (at Q4)
Number of cases reviewed by CDOP Not Available
30 33 31 30 26 Worse
SCRs referrals considered within timescale 100% 100% 100% 100% 100% 100% Same
Attendance at LSCB Meetings 73% 80% 75% 68% 79% 80% Improved
Percentage of Business Plan Actions completed within timescales
90% 90% 80% 90% 90% 90% Improved
The LSCB also has in place, a risk management framework and risk register which is reviewed twice a year to ensure the appropriate controls are in place to mitigate against key risks to the delivery of LSCB business and the effectiveness of the partnership. There are currently no risks that are felt to be 'high' given the controls in place at present. The full register can be viewed at appendix 5. All LSCB members are required to sign a 'Compact' setting out their responsibilities as a Board member and highlighting the expectation that LSCB work should take priority over single agency responsibilities when acting on Board business. All members are provided with an induction pack containing all necessary information. LSCB Attendance Attendance by agency for all Board meetings in 2012/13 is shown below
Agency % Attended No Attended No Invited East Lancashire LSCG Chair 100 6 6 LCC (Adult SB) 67 4 6 North Lancashire PCT (Chair QA) 83 5 6 East Lancashire PCT 67 4 6 LCC (member) 83 5 6 LCC (DCS) 83 5 6 Designated Doctor 33 2 6 Probation 83 5 6 Police 83 5 6
26

Central Lancashire PCT (Vice Chair & LSCG Chair) 100 6 6 Preston City Council 67 4 6 LCC (Director of Specialist Services) 67 4 6 Independent Chair 100 6 6 LCFT NHS 67 4 6 VCFS 67 4 6 VCFS 100 6 6 North Lancashire LSCG Chair 83 5 6 Cafcass 83 5 6 LTHT NHS 83 5 6 LCC (SCR Group Chair) 83 5 6 Schools Rep 33 2 6 Lay Member 50 3 6 OVERALL 79
LSCB Management Team The LSCB Management Team coordinates and drives forward the work of the LSCB and is currently structured as follows: All posts are hosted by the local authority and individual performance appraisal is in line with the Local Authority procedure. Individual performance plans are in place for all members of the team which are based on the business plan of the LSCB and monitored on a monthly basis through formal supervision. An independent review of the team has taken place in 2011/12 in order to identify any efficiency savings or improved ways of working. The recommendations of this review are currently being finalised and further capacity for the team in light of the new guidance is being considered, especially around the Case Review function. Any changes from this will be reported in next year's Annual Report. LSCB Budget The LSCB is funded from a pooled partnership budget which is monitored via a bi-monthly report to the LSCB and Executive Group. Accountancy assistance is provided through the Local Authority finance team and expenditure is administered through the Local Authority electronic financial management system (Oracle). A scheme of delegation is also in place which determines the level of expenditure that can be authorised at different levels of seniority. The LSCBs statement of account for end of year 2012/13 is as follows:
LSCB Manager
LSCB Strategic Training Coordinator
LSCB Business Coordinator
LSCB Child Death Overview Panel Coordinator
LSCB Training Administrator
LSCB Support Officer
CDOP Administrator
LSCB Administrator
27

INCOME Actual
£ Contributions to Board Central Lancs PCT 37,835 East Lancs PCT 37,835 North Lancs PCT 37,835 Police 43,938 Probation Service 13,488 CAFCAS 550 LCC - CYP Directorate Funding 112,000 LCC - CYP Directorate Funding -3,181 280,300 Child Death Overview Panel
Lancashire Safeguarding Children Board 55,000 Blackpool 11,500 Blackburn with Darwen 11,500
Miscellaneous Income 265
Funding from Reserves 29,596 107,861 Serious Case Review Funding from LCC CDOP 20,000 Funding from LCC 51,000 Funding from Main Contributions 3,181 Funding from Reserves 36,319 110,500 Other income 12,332
TOTAL LSCB INCOME 510,993
EXPENDITURE £
LSCB General 143,129 Child Death Overview 87,248 Serious Case Review 34,807 Training 134,520
TOTAL LSCB EXPENDITURE 399,704
Carry Forward to 2013/14 (111,289)
28

Safeguarding and Looked After Children Inspection During 2011/12 Lancashire was inspected by Ofsted under the framework for Safeguarding and Looked After Children. Within the inspection the role and effectiveness of the LSCB was assessed as follows: "The performance of the LSCB is good. The independent chair provides good leadership and partners effectively support the board. Partner agencies are challenged and held to account and performance is closely monitored." In addition to the effectiveness of the LSCB a number of recommendations for improvement were made for partner agencies and an action plan developed. The high priority actions which the LSCB maintained a close scrutiny over (see business plan at appendix 4) are as follow:
a. LSCB is assured that gaps in Designated Health roles are effectively addressed b. LSCB is assured that CAMHS resources for ADHD, ASD and 16-18yr olds are adequate c. LSCB is assured that substance misuse services are accessible and effectively commissioned d. LSCB is assured that safeguarding arrangements across out of hours, walk-in and accident and
emergency health services across Lancashire to ensure children are effectively safeguarded
The inspection also highlighted a number of concerns about the effectiveness of safeguarding arrangements at University Hospitals Morecambe Bay NHS Trust. In response to this a multi-agency 'expert panel' was convened, involving a number of LSCB members, and an action plan developed. The LSCB maintained a regular dialogue with the panel through its members and was provided with regular progress reports with implementation of the action plans which is continuing into 2013/14. At the end of year it was felt all improvement plans were established and corrective action progressing. The LSCB will continue to maintain oversight of this action plan both directly and through the North Lancashire Local Safeguarding sub-group.
Issues and challenges facing safeguarding – statement of effectiveness of safeguarding arrangements in local area
The LSCB has faced additional challenges in 2012/13 due to a number of significant external factors and developments as follows:
• Emerging revision of statutory Guidance (Working Together 2013) • The Munro Review of Child Protection • High profile media interest in local Child Sexual Exploitation cases • Reconfiguration of the Health Economy • Ofsted inspection of Safeguarding and Looked After Children • Organisational restructuring in response to austerity measures
The LSCB's robust business planning cycle has enabled the LSCB to regularly review its business plan and priorities in response to these emerging and issues and developments, as can be evidenced at appendix 4. In summary the LSCB has responded to these effectively through the following actions and initiatives:
• Consideration of the draft Working Together guidance and collation of a comprehensive LSCB response to the consultation
• Piloting the systems methodology for the completion of SCRs using the SCIE model on a live case (See Case review Sub-group Update)
• Recognising Child Sexual Exploitation as a priority area for quality assurance and receiving regular reports from the Constabulary and Child Sexual Exploitation sub-group re operational and strategic activity
• Requesting regular updates from key health personnel with regard to ongoing reconfiguration of health services
• Inviting all CCG leads to a special extended LSCB to agree how safeguarding will be embedded across the 6 CCGs and how they will be represented through the LSCB and its sub-groups
• Providing all necessary support, information and engagement for the SLAC inspection and taking an active role in implementing and overseeing subsequent improvements
29

• Requesting all organisations to provide assurance that service re-structuring will not compromise the safeguarding of children and young people
Most of these issues and developments are ongoing into the next financial year and can be clearly evidenced through the 2013/14 business plan and subsequent sub-group work programmes.
Conclusion and recommendations for future priorities and Business Plan 2012/13 has been an extremely challenging year for the LSCB. The pace of organisational change as a result of continuing national and local governmental austerity measures and wholesale revisions to national guidance has required careful planning and horizon scanning to enable the LSCB to meet these challenges head on. In addition to this, the area inspection by Ofsted of Safeguarding and Looked After Children services, while recognising much good and excellent practice has also raised a number of issues and gaps in services resulting in substantial national media interest around issues at University Hospital Morecambe Bay Hospital Trust. There has also been significant challenges in responding to the threat of Child Sexual Exploitation, which has also been widely reported in the media and Lancashire has now been recognised as a beacon of excellent practice for its response. The LSCB has taken an active role in addressing and overseeing many of these improvements and recognising the wealth of good practice and innovative developments. The robust business planning cycle will ensure key issues and areas for further development are continued into next year's business plan. A brief summary of these are as follows :
• Implementing Working Together 2013 • Relationships with the new:
o Health Economy & CCGs o Health & Well Being Board o Police and Crime Commissioner
• Revised Case Review Methodology (systems model) • Quality Assurance around the 'Toxic Trio' • Implementing the new Learning and Improvement Framework • Revision of LSCB Performance Information • Responding to increased risks from the use of Social Media and online behaviour • Continued evaluation of practice through Audits/Mock Inspection • Continued activity to support the victims of Child Sexual Exploitation and bring offenders to justice
30

Appendices
Appendix 1: Learning and Development Plan
LSCB Business Plan Objective
LSCB Business Plan Task
Actions Sub-group will take to deliver this:
Lead Person/Agency
Completion Date
Progress since last meeting
3e. A Multi-agency training programme is in place which meets the identified priorities of the LSCB.
- Conduct Gap / Fit analysis to ensure training programme meets LSCB priorities
Liaise with LSCB and all LSCB sub-groups to ascertain training needs Consult within own agency to ascertain training needs
Training sub members
September 2012
completed
To establish, via employing organisations, who in the workforce requires multi-agency training to safeguard children
Training sub-group members
Ongoing Review done
Plan the training programme to meet the needs, within the resources given
Training sub group
September 2012
completed
To have the training programme agreed by LSCB to ensure it meets LSCB priorities
Jane Carwardine & LSCB
January 2012
completed
Work towards the inclusion of all agencies (statutory, voluntary & independent) in LSCB training programme
Training sub-group, Ane Freed-Kernis
Ongoing Places to Vol. Orgs. On each event
- Provide regular progress reports to Executive
Provide a report to each Executive meeting
Jane Carwardine & Ane Freed-Kernis
Ongoing completed
3f. Single agency training being delivered across the county can be evidenced as complying with Working Together
- Develop and implement programme of audit
To ensure standards are set for single agency basic training/learning and evaluate and review single agency provision
Training sub Standards set. S.11 used to QA
To plan and execute a programme of quality assurance of single agency training
Ane Freed-Kernis
Ongoing s.11
Provide regular progress reports to Executive
To provide half-yearly reports
Jane Carwardine
Ongoing Done
Providing limited children’s safeguarding training consultancy service
Ane Freed-Kernis
Ongoing 58 requests done
6c. LSCB member's can effectively
Identify suitable training for
Questionnaire designed for LSCB members regarding
Ane Freed-Kernis
November 2011
Done
31

LSCB Business Plan Objective
LSCB Business Plan Task
Actions Sub-group will take to deliver this:
Lead Person/Agency
Completion Date
Progress since last meeting
challenge each other.
members with regard to challenge
their needs/wishes for training
Questionnaire distributed and returned for analysis
LSCB members February 2012
Done
Suitable facilitator identified and date booked
Nigel Burke/Ane Freed-Kernis
April 2012 Not needed, LSCB
Ensure training sub-group is will informed about practice issues in the LSCB
To maintain links with Quality Assurance subgroup, child death overview panel and serious case review panel
Have overlapping members of all the sub-groups
Training sub-group
Ongoing Done
To ensure membership of training sub group is in accordance with LSCB guidance
Update terms of reference for training sub-group
Have terms of reference agreed by LSCB annually
Jane Carwardine
April 2012 Done
To commission the design, planning, organisation and implementation of the training/learning programme via the LSCB strategic training co-ordinator, based on inter-agency priorities and learning from SCRs and reviews of child deaths.
Run a core training programme of approximately 75 events covering at least 20 topics, potentially adding further events required by the LSCB
Create a training plan for the year Manage the plan responding to feedback from LSCB should priorities change
Ane Freed-Kernis And Freed-Kernis
October 2011 March 2013
Done. 77 events were planned. 56 ran, 21 were cancelled
To recruit, support, develop and monitor the training pool.
Request trainers from individual agencies Devise and run a development programme for the training pool development
Training sub-group, Ane Freed-Kernis
Ongoing Done
Ensure the programme that is run reflects national and local policy and research
Keep abreast of national research Develop the training pool members Use experts to keep us updated
Ane Freed-Kernis, training pool members, Training sub-group
Ongoing Done
To implement quality assurance measures across
Monitor and evaluate the quality and
Training sub-group members to observe a LSCB course each year
Training sub-group members
Ongoing Method changed, will
32

LSCB Business Plan Objective
LSCB Business Plan Task
Actions Sub-group will take to deliver this:
Lead Person/Agency
Completion Date
Progress since last meeting
the learning programme
effectiveness of the LSCB learning programme
happen in 2013-14
To support the LSCB by providing up to date information in relation to the learning programme
Maintaining records of all delegates and trainers on courses, for statistical use
Maintain and update training database to keep this information and provide statistical information to the LSCB and others on request
Louise Wilson Ongoing done
33

Appendix 2
LSCB Section 11 Audit Tool 2012
Section 11 of the Children Act 2004 places a duty on key people and bodies to make arrangements to ensure that their functions are discharged with regard to the need to safeguard and promote the welfare of children. The application of this duty will vary according to the nature of each agency and its functions.
Agency Name & Designation of Person Completing (include email address) Date Completed
1 - LEADERSHIP Senior managers will need to demonstrate leadership, be informed about, and take responsibility for the actions of their staff who are providing services to children and their families. Minimum Requirements
• Designated Senior Officer for Safeguarding in place and visible • Senior Managers can evidence effective monitoring of service delivery
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
2 – COMMITMENT The agency’s responsibilities towards children is clearly stated in policies and procedures that are available for all staff. Minimum Requirements
• Statement of responsibilities (as per section 11 guidance) is visible in policies & guidance • This is accessible and understood by all staff
34

Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
3 – ACCOUNTABILITY & GOVERNANCE It should be clear who has overall responsibility for the agency’s contribution to safeguarding and promoting the welfare of children and what the lines of accountability are from each staff member up through the organisation to the person with ultimate accountability for children’s welfare. Minimum Requirements
• All staff know who to report concerns about a child to • Staff at all levels know and understand their responsibilities
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
4 – SERVICE DEVELOPMENT/REVIEW In developing local services, those responsible should consider how the delivery of these services will take account of the need to safeguard and promote the welfare of children. Minimum Requirements
• The views of children and families are sought and acted upon when developing services • The need to safeguard children has informed decision making about any developments
Evidence Statement (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant
35

Comments
5 - TRAINING Staff should have an understanding of both their role and responsibilities, and those of other professionals and organisations. Minimum Requirements
• All staff have received level 1 safeguarding training • All appropriate staff have received level 2 and above single agency training (include %) • All appropriate staff have received level 2 and above multi agency training (include %)
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
6 – SUPERVISION Safeguarding Supervision should be effective and available to all Minimum Requirements
• Supervision Policy in place and meets LSCB guidance standards • All staff working with children receive appropriate regular supervision
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
7 – SAFE RECRUITMENT Robust recruitment and vetting procedures should be put in place to prevent unsuitable people from working with children.
36

Minimum Requirements • All recruitment staff are appropriately trained in safe recruitment • All appropriate staff receive a CRB check that is regularly updated • Legal requirements are understood and in place • Role of LADO understood and procedures in place • All staff know who the Named Senior Officer for their agency is
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
8 – INTERAGENCY WORKING Agencies and staff work together to safeguard and promote the welfare of children. Minimum Requirements
• Evidence of leadership to enable joint working • Evidence of practitioners working together effectively • Evidence that CAF is being used appropriately and effectively
Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
9 - INFORMATION SHARING Effective information sharing by professionals is central to safeguarding and promoting the welfare of children. Minimum Requirements
• Evidence of robust single agency protocols and agreements* • Evidence of robust multi agency protocols and agreements*
37

• Evidence that practitioners understand their responsibilities and when to share information * The lack of an information sharing agreement between agencies should never be a reason for not sharing information that could help a practitioner deliver services to a child. Evidence Statement: (max 200 words, please attach / embed appropriate policies or documents)
Quality Assurance (office use only) Red – Not Compliant Amber – Partially Compliant Green – Fully Compliant Comments
38

Appendix 3
CDOP Work Plan
Priority Status (RAG rating)
Comments
1. The Panel will review cases and make recommendations regarding themes to the Board
The Panel has an ongoing responsibility to review cases and make recommendations as appropriate; the CDOP reports to the Boards bimonthly, quarterly (with statistics) and annually.
2. CDOP will develop links with other Local Safeguarding Children Board Sub-Groups particularly the Safe from Harm Group
The CDOP Coordinator sits on the pan-Lancashire Infant Mortality Group, has presented the Annual Report and Suicide Thematic Report to the Safe from Harm Group, the annual report has also been shared with the CYPT Chairs Meeting, the LSCB locality groups and the JSNA manager.
3. With Public Health department investigate apparent mis-match in numbers of deaths between CDOP and ONS data.
Mismatch of data identified inherent problems with the comparison of the two datasets because they work on different parameters – gestation viability, pending inquest/ criminal investigation.
3b. Further detailed review work to identify themes / trends in deaths categorised as caused by perinatal / neonatal events.
The initial findings have been presented to CDOP the final report is awaited.
4. The Panel will monitor the re-launch of the Give Me room to Breathe (GMRTB) Campaign
The SUDI Prevention Group have updated and re-launched the Campaign; the Boards have approved funding for the second/ third phase of the Campaign.
5. CDOP will ensure the Safer Sleeping Guidance is reviewed
The Guidance was approved by the Board in March 2013 and is being widely disseminated to all frontline professionals.
6. Ensure and monitor the review of the SUDC Protocol
The review of the Protocol was delayed pending the release of the new statutory guidance. This is a priority for 2013/14.
7. Finalise the multi-agency e-learning and make available to front line multi-agency professionals
The e-learning has been re-written to be more user friendly; this remains a priority for 2013/14.
8. Develop a Pan-Lancashire communications strategy for disseminating messages and information on a multi-agency basis
The CDOP developed a task and finish group to look at this; however, it was decided a specific sub-group/ strategy was not required and the CDOP would develop an 'events calendar' to enable CDOP to recommend to the Boards time press releases.
9. Monitor Multi-Board CDOP Budget and develop action plan for utilising the under spend. (suggested ideas: CDOP database, Give Me Room To Breathe Campaign, commissioning a piece of research into Neonatal/ Perinatal deaths and/ or deaths due to genetic, chromosomal and congenital abnormalities)
The Boards approved funding for the safer Sleep campaign. The CDOP still has a budget for 2013/14 which has some under spend from 2012/13 but the under spend from 2011/12 has been utilised. The CDOP now monitor their budget at each bi-monthly Business Meeting.
39

10. Update the data recording/ analysis systems to improve reporting on specific modifiable factors identified by the Panel
The current reporting spreadsheet has been updated to enable some reporting on modifiable factors while a CDOP database is scoped out.
40

Appendix 4
LSCB Business Plan 2012/13
Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
Strategic Priority 1. We will improve the way we work by listening to and responding to the views and experiences of children and young people
a. All existing channels and forums for consulting with children and young people have been identified
- Identify countywide consultation channels and mechanisms
- Identify local consultation channels and mechanisms
LSCB Business Team
LSCGs
October 2012
October 2012
Completed.
Discussed at LSCGs and identified where appropriate
b. Key business priorities incorporate the views of children and young people
- Develop and implement consultation plan at county and local level
- Facilitate safeguarding events (x2) with Youth Councils and/or existing groups (11 – 18 year olds. Possibly use North West regional group)
LSCB Business Team
LSCB Business Team
December 2012
December 2012
Completed
To be considered as part of YP involvement plan 2013-14
c. All agencies can evidence that they consult with children and young people as appropriate
Continued section 11 activity to confirm agency engagement with young people
QA Group March 2013 Completed. New audit tool now gone out including this criteria.
41
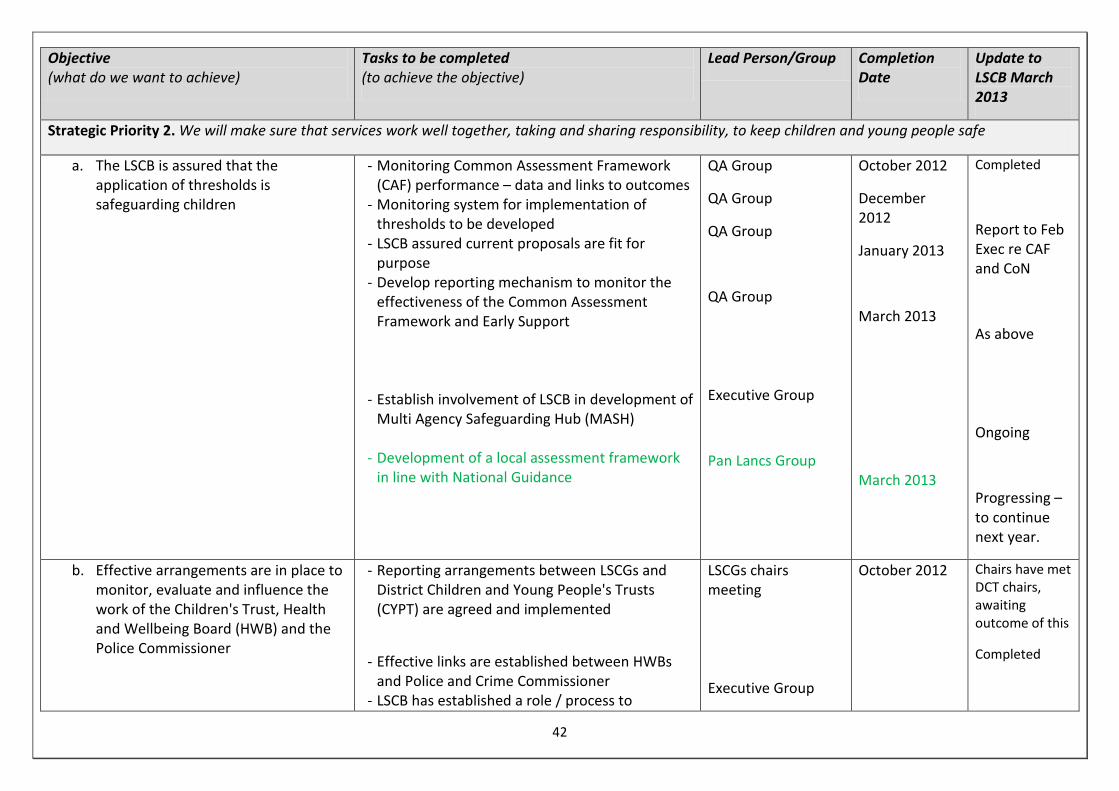
Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
Strategic Priority 2. We will make sure that services work well together, taking and sharing responsibility, to keep children and young people safe
a. The LSCB is assured that the application of thresholds is safeguarding children
- Monitoring Common Assessment Framework (CAF) performance – data and links to outcomes
- Monitoring system for implementation of thresholds to be developed
- LSCB assured current proposals are fit for purpose
- Develop reporting mechanism to monitor the effectiveness of the Common Assessment Framework and Early Support
- Establish involvement of LSCB in development of
Multi Agency Safeguarding Hub (MASH) - Development of a local assessment framework
in line with National Guidance
QA Group
QA Group
QA Group
QA Group
Executive Group
Pan Lancs Group
October 2012
December 2012
January 2013
March 2013
March 2013
Completed
Report to Feb Exec re CAF and CoN
As above
Ongoing
Progressing – to continue next year.
b. Effective arrangements are in place to monitor, evaluate and influence the work of the Children's Trust, Health and Wellbeing Board (HWB) and the Police Commissioner
- Reporting arrangements between LSCGs and District Children and Young People's Trusts (CYPT) are agreed and implemented
- Effective links are established between HWBs and Police and Crime Commissioner
- LSCB has established a role / process to
LSCGs chairs meeting
Executive Group
October 2012
Chairs have met DCT chairs, awaiting outcome of this
Completed
42

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
influence/monitor commissioning
- Annual report to CYPT Partnership Board, Lancashire County Council (LCC) Chief Executive and Leader
Executive Group
LSCB
March 2013
October 2012
July 2012
KG attending commissioning groups
Completed
c. Effective strategies are in place regarding the issues of: - Bullying - Domestic Abuse - Neglect - Child Sexual Exploitation/missing persons - E safety - Child and Adolescent Mental Health
- Rape
- Review current provision regarding these issues and conduct gap analysis
- Commission development of any new strategy and ensure monitoring arrangements are in place
- Hold a conference on neglect to raise awareness of recognition and how to deal with it
- Rape group to report into LSCB regarding development of strategies and work
Specific sub groups
Specific sub groups
Business Team
Strategic Rape group
October 2012
December 2012
July 2012
October 2012
Ongoing activity.
Ongoing
Completed
Completed
43

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
d. LSCB is assured that the refreshed continuum of need is widely understood by practitioners and families and is working well. The LSCB is also assured that the approach to working together with families is making a difference
- Work with CYPT to progress implementation of new continuum of need and the approach to working together with families.
- Attend and participate in all workshops with CYPT regarding these issues
- Complete any actions for the LSCB from these workshops
LSCB
LSCB
LSCB Business Team and LSCB
September 2012
As and when required
As and when required
Work progressing through strategic group, regular updates to Exec.
e. LSCB is assured that multi-agency assessments are effective and robust
Quality Assurance framework to be progressed, to ensure findings from audits are acted upon
QA Group March 2013 Planned
f. The LSCB is assured that arrangements for the safeguarding of privately fostered children are effective
- Annual Report to be presented by LCC - Audit findings to be presented to LSCB and
necessary actions undertaken
Paul Armitage/LSCGs
Paul Armitage
July 2012
July 2012
Completed
Completed
g. Develop effective relationships with the 'new' Health Economy
- Establish connectivity to Clinical Commissioning Groups and Health and Well Being Board
- Re-establish Health sub-group
Executive Group
Health leads
March 2013
October 2012
Completed,
Ongoing
44

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
h. LSCB to receive assurance that issues identified through Safeguarding and Looked After Children Inspection are being/have been addressed effectively
- Full action plan in place which will be monitored by 'continuous improvement' multi-agency group
- LSCB will monitor progress of action plan via QA group
QA Group
QA Group and LSCB
July 2012
Ongoing
Regular update reports now being provided.
i. LSCB is assured that all single agency areas for improvement identified through Safeguarding and Looked After Children Inspection have been addressed effectively
Multi-agency 'Continuous improvement group' to monitor progress of Inspection Action Plan Business Manager to keep the LSCB informed
Jane Higgs Update to every Exec
Group continuing to meet and action plan update can be provided at the Exec if required.
j. LSCGs are well attended by all key local agencies and services and are effectively identifying local issues and needs
- LSCGs to report to LSCB what local needs and priorities are in line with Board priorities and act upon them through their action plans
- Annual report on attendance from LSCGs
LSCGs
LSCGs
October 2012
March 2013
Ongoing
Attendance reported at every meeting
Strategic Priority 3. We will make sure that the way we recruit, train and supervise those who work with children and young people will keep children and young people as safe as possible
a. Multi-agency supervision standards are in place
Develop multi-agency safeguarding supervision standards
LSCB Business Team October 2012 Completed
b. Effective supervision policies are implemented across all agencies and compliance evidenced
Seek assurance from agencies on concerns identified in 2010 section 11 audit in relation to
QA Sub-group March 2013 Completed
45

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
this issue
c. LADO role has been reviewed with regard to function and capacity
- Improve awareness of LADO, including regular newsletters and increased access to website
- Review effectiveness of LADO role - LSCGs to assure all members know about LADO
and LSCB
LADO
LADO and Executive
LSCG chairs
October 2012
March 2013
October 2013
Completed
??
Completed
d. Recruitment practices of LSCB agencies are demonstrably effective and robust
Seek assurance from agencies on concerns identified in 2010 section 11 audit in relation to this issue
QA Sub-group March 2013
Completed
e. A Multi-agency training programme is in place which meets the identified priorities of the LSCB
- Implement revised programme - Commission specific programmes in response to
Munro review using funding provided
Training Sub-group
Training Sub-group
July 2012
October 2012
Completed
Completed
f. Single agency training being delivered across the County can be evidenced as complying with Working Together
- Develop and implement programme of audit
- Provide regular progress reports to Executive
Training Sub-group
Training Sub-group
October 2012
Ongoing
Currently being developed.
As and when required
g. LSCB Members have a suitable pack of induction material
Keep induction pack updated as required LSCB Business Team
Ongoing Completed
46

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
h. LSCB has a Learning and Improvement Framework
Develop Framework LSCB Business Team
March 2012 Completed
Strategic Priority 4. We will make sure that everybody who works with children and young people knows that keeping them safe is an important part of their job
a. LSCB Safeguarding policies and procedures are up to date and effective
- Existing pan-Lancashire group to continue to meet regularly and consider priorities
- Set task and finish groups to develop specific procedures as and when required
- Monitor Tri-X updates and improvements to procedures and ensure they are completed
Pan-Lancs & Cumbria procedures group
Pan-Lancs & Cumbria procedures group
Pan-Lancs & Cumbria procedures group
Ongoing
Ongoing
Ongoing, new procedures being developed as and when required.
b. The LSCB is assured that all agencies are meeting their requirements under section 11
- Section 11 Audit has been completed by all member agencies, quality assured and key findings acted upon
- Seek assurance from agencies that areas for improvement are progressing as planned
- Revise S11 Tool to ensure effectiveness
QA Sub-group
QA sub-group
QA sub-group
March 2013
March 2013
October 2013
Progressing as planned
Completed
Completed
Strategic Priority 5. We will assist children, young people, their families and communities to keep themselves safe and know how to get help
LSCB have an effective communications strategy
To include:
- Serious Case Review Learning - CDOP Case Reviews and learning – especially
around overlay
Specific sub-groups to manage specific
July 2012
47

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
- Improve and update Website - Scope new communication mechanisms (Social -
Networking etc) - Publicising LSCB and Safeguarding - Specific Campaigns - Engaging with diverse communities - Rapid response to increase incidence of overlay
issues
LSCB Business team to develop overarching communications strategy
Completed
Strategic Priority 6. We will continue to make sure that people who work with children and young people are doing their jobs well, and will challenge them when they don't
a. The LSCB is robust in its challenges of agencies that are not safeguarding children in the way they should do
- LSCB member's can effectively challenge - Review responses to challenge questionnaire
and develop action plan - Offer individual training sessions to individuals
that want it
Training sub
October 2012 Training offered questionnaire completed
b. The LSCB be assured that all agencies are meeting the needs of children and young people across Lancashire, specifically with regards to neglect and Child Sexual Exploitation
- Embed Quality Assurance Framework and feedback to the LSCB
- Deliver priorities as specified in Quality Assurance Framework for this year
QA Sub-group March 2013
Largely completed, some activity to continue into next year.
c. The LSCB is assured that health agencies are meeting the needs of children and young people across Lancashire
Review of Health performance data : existing and provision of data as per example from Manchester LSCB (include acute trusts and safeguarding standards)
QA sub group July 2012 Completed. End of year data to be requested as agreed.
48

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
d. LSCB is assured that gaps in Designated Health roles are effectively addressed 1
Health action plan to be progressed and monitored by QA sub-group
QA sub group October 2012 Expert Panel now in place and update reports provided.
e. LSCB is assured that CAMHS resources for ADHD, ASD and 16-18yr olds are adequate 1
Health action plan to be progressed and monitored
QA sub group October 2012 Progressing through inspection improvement group.
f. LSCB is assured that substance misuse services are accessible and effectively commissioned 1
Health action plan to be progressed and monitored
QA sub group Update to every Exec
Progressing through inspection improvement group.
g. LSCB is assured that safeguarding arrangements across out of hours, walk-in and accident and emergency health services across Lancashire to ensure children are effectively safeguarded 1
Health action plan to be progressed and monitored
QA sub group
Update to every Exec
Progressing through inspection improvement group.
1 Relates to Inspection findings
49

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
h. LSCB has a robust plan and is prepared for any future inspection
Plan and arrangements to be developed and scrutinised.
QA Sub-group March 2013 Carried over to next year.
Strategic Priority 7. We will make sure that we use our money and staff to give the best results for children and young people
a. LSCB Business Team is effective, efficient and provides value for money
Review of establishment to be completed through LCC Business Analysts
Executive Group October 2012 Progressing but significant slippage.
b. LSCB has effective and efficient ways of working
- Budget management process to be further refined and improved
- Review training function and all sub-groups for efficiency savings
Executive Group
October 2012 Completed
Largely completed
c. Ensure closer joined up working with other LSCBs on cross cutting / Sub-regional issues
LSCB Business Teams and Chairs to develop cross boundary working when possible
Pan –Lancs and Cumbria Chairs group
Ongoing Ongoing meetings and developments.
d. LSCB Membership has the right representation from all necessary agencies
Review membership to ensure the following are linked in:
Executive March 2012 Discussed at Nov LSCB and felt to be
50

Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
- Faith Community - Armed Forces - Transport Police - Another lay-member?
adequate.
Strategic Priority 8. We will make changes that come from research, serious case reviews and any national policy guidelines.
a. Serious Case Reviews and Critical Incident Reviews are undertaken where appropriate
- Consider referrals against criteria for Serious Case Reviews
- Commission Serious Case Reviews as appropriate
- Commission Critical Incident Reviews as appropriate
- Complete Critical Incident Reviews and feedback learning to SCR Group and local agencies
SCR Group
SCR Group
SCR Group
LSCGs
Ongoing
Systems in place and effective.
b. An effective system is in place for the monitoring of action plans and dissemination of learning from case reviews
- Maintain system to monitor action plans - Ensure messages from case reviews are widely
disseminated within all agencies
SCR Group
SCR Group
Ongoing Systems in place and effective.
c. That good practice is recognised and disseminated
- Learning from best practice cases in the north and the east be shared and any learning is acted upon
LSCGs Ongoing Systems in place and effective.
51
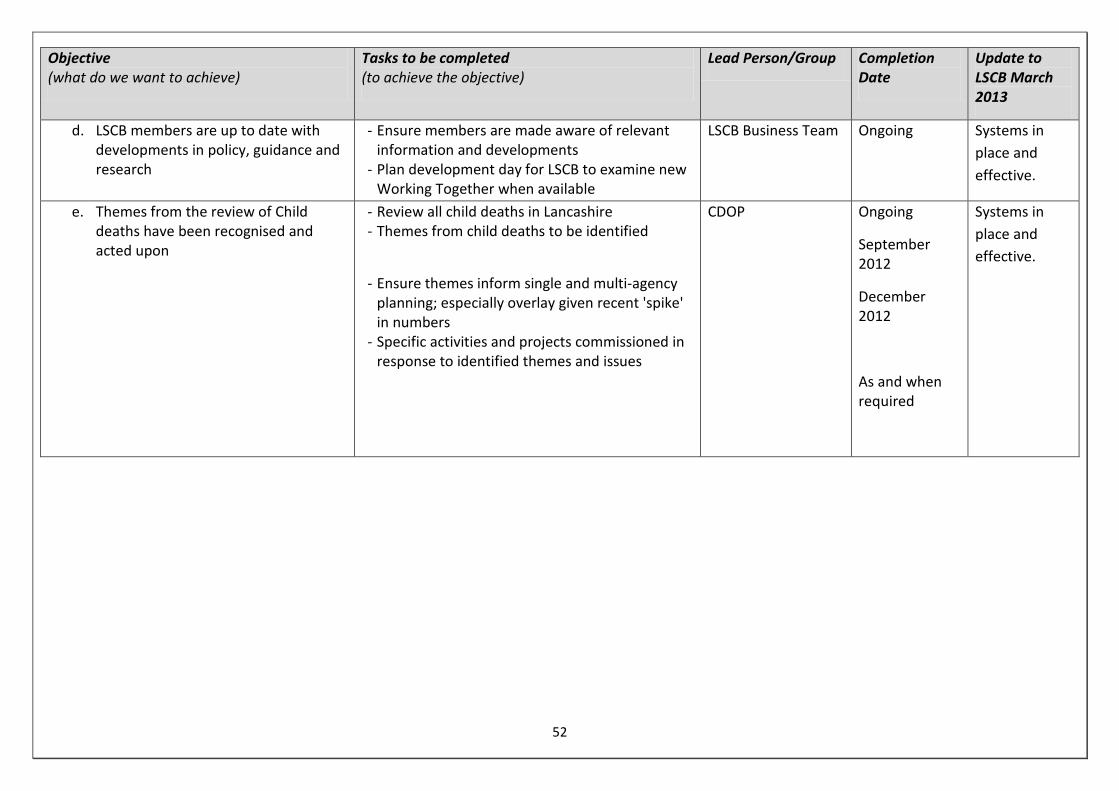
Objective (what do we want to achieve)
Tasks to be completed (to achieve the objective)
Lead Person/Group Completion Date
Update to LSCB March 2013
d. LSCB members are up to date with developments in policy, guidance and research
- Ensure members are made aware of relevant information and developments
- Plan development day for LSCB to examine new Working Together when available
LSCB Business Team Ongoing Systems in place and effective.
e. Themes from the review of Child deaths have been recognised and acted upon
- Review all child deaths in Lancashire - Themes from child deaths to be identified
- Ensure themes inform single and multi-agency planning; especially overlay given recent 'spike' in numbers
- Specific activities and projects commissioned in response to identified themes and issues
CDOP
Ongoing
September 2012
December 2012
As and when required
Systems in place and effective.
52

Appendix 5
Risk Register
Theme 1 – Integrity & Reputational Risks
No Description of Risk
Inherent Risk
Rating Current Controls Residual
Risk Rating
Further Controls Required By When By Whom
Retained Risk
Current Status
Review Date
1a
Inability to evidence improved outcomes for children and families
12
Performance Reports, QA framework, scrutiny of single agency inspections / evidence, Mock Inspections
8 None NA NA 8 September 2013
2a Negative media exposure
9
Media planning around key issues and SCRs. Scrutiny of key reports and info. Communication with agency media liaison staff
6 None NA NA 6
September 2013
3a Information security breaches.
8 Robust procedures and governance. Training and supervision.
6 None NA NA 6 September 2013
4a Poor inspection judgement – of LSCB or key partner
9
Peer review feedback, business planning, intelligence gathering from other areas, links to inspection planning groups, assurance from partners
6 None NA NA 6
September 2013
Theme 2 – Risks to Partnership & Engagement
53

No Description of Risk Inherent Risk Rating
Current Controls Residual Risk Rating
Further Controls Required
By When By Whom Retained Risk
Current Status
Review Date
1b
Insufficient contribution from partners - financial or in kind (Failure of duty to cooperate)
9
Review at regular intervals, operation of Compact, regular reports, accountability and governance arrangements,
6 None NA NA 6
September 2013
2b Failure to effectively hold a partner agency to account who is failing
8
Publish attendance stats, quality assurance of sec 11, peer review, chair has a clear mandate, LSCB compact , calendar of peer reviews
6 None NA NA 6
September 2013
3b Disengagement of key partners from the LSCB
8
Governance arrangements, secured commitment, LSCB Compact, shared priorities
3 None NA NA 3
September 2013
4b
Impact of Health reforms resulting in potential loss of focus and leadership around safeguarding
9 Regular updates from Health members, engagement with CCGs
6 ? 6
September 2013
Theme 3 – Risks to Delivery of LSCB Business Objectives
No Description of Risk
Inherent Risk
Rating Current Controls Residual
Risk Rating
Further Controls Required By When By Whom
Retained Risk
Current Status
Review Date
1c Insufficient resources to deliver key business priorities.
12 Financial monitoring, review of team structure, Effective business planning
8 Establish long term capacity in LSCB Team
September 2013?
Exec 8 September 2013
2c Changes in government policy impacting upon resources and priorities
12
Regular updates from members on policy issues, forward planning and horizon scanning
9 Response to finalised revised WT
September 2013? Exec 9
September 2013
3c Severe staff absence in 8 Formal absence 8 Contingency September LSCB 8 No September
54

management team – business continuity
management procedure. planning for additional resources if required
2013 Manager business continuity plan in place
2013
4c Severe weather restricting business activity
9 Electronic information systems, forward planning
6 None NA NA 6 September 2013
5c Legal challenge or substantial liability claim
8 Close links with legal team, scrutiny of key business.
6 None NA NA 6 September 2013
6c Very high profile and complex SCR, or several required simultaneously
8
Close scrutiny of referrals, improved processes, additional staff resources to support SCRs
6
Establish long term capacity to support SCRs
September 2013 Exec 6
September 2013
7c Competing Priorities from supporting LASB?
9?
Being developed – clear mandate for resource allocation / level of support
? ?
September 2013
8c Failure to evidence effective monitoring of single agency training
9 Process being developed through L&D Group
9
Assurance from all key agencies that processes are in place
September 2013
L&D Sub Chair
9
September 2013
55
Page 1 of 4
Minutes
Quality Improvement Committee
Venue: Committee Room, NHS West Lancashire CCG offices, Ormskirk
Date & Time: Tuesday 20 August 2013 at 1.00 pm – 3.10 pm
Attendees: Mr G Mitten – Chair Dr J Kinsey – Clinical lead for clinical engagement Dr A Bisarya – Clinical lead for quality Mrs J Worswick – Deputy chief officer Mrs J Moran – Head of quality, performance & contracting Mrs J DeBacker – Practice manager In attendance: Dr R Bonsor – Interim clinical lead Mrs J Rollinson – Associated director safeguarding Miss C Ashcroft – Executive assistant
Apologies: Mrs D Dobson – Practice manager Mrs H Clarke – Chief nurse
Agenda
Item CCGQIC/
Summary of Discussion Lead
08/13/1 Welcome and apologies for absence The Chair welcomed the members of the Quality Improvement Committee to the meeting.
08/13/2 Minutes from the previous meeting on 25 June 2013 The notes from the previous meeting were approved as an accurate record.
08/13/3 Matters arising – action sheet The action sheet was updated.
08/13/4 Quality workplan Jackie Moran presented the quality workplan which had been produced with input from Helen Clarke, Jo Worswick and Jean Rollinson. The workplan covered areas recommended by Helen Clark in an earlier document and reflected the Southport & Formby CCG workplan. The papers listed within the workplan cover all the areas and will be included on the committee agenda or within the Integrated Business Report. All committee members were requested to look at the areas in the workplan and comment to Jackie Moran by cop on Friday 30 August 2013.
All / JM
08/13/5 Integrated business report – Month 3 The integrated business (IBR) report for month 3 was presented by Jackie Moran. An overview of the quality and performance section of the IBR report was provided with discussion on the following key areas:
The CCG is currently meeting its financial performance statutory requirements
GP referrals are on a downward trend, whereas other referrals are increasing. A breakdown of numbers for individual areas is required.

Page 2 of 4
Agenda Item
CCGQIC/
Summary of Discussion Lead
Planned care – o A meeting around the reporting elements of the integrated
referral gateway will take place. o Cancer screening 62-day waiters is still at red and an
explanation of how the numbers are being counted is required. Further analysis is being carried out by Sally Jones. Dr Jack Kinsey will discuss this before the next committee meeting.
o Diagnostics by speciality data are required (JDeB to send letter)
Mortality rates are still forecast to be red at end of year. TIA – an explanation as to why this is slipping is required. A&E underperformance - Pressure sores levels are a concern.
Jackie Moran will circulate report on pressure sores data. Data is needed from community to demonstrate the concerns from the district nursing service. Dr Ros Bonsor to investigate further with Jean Rollinson.
The quality email address will be provided to Dr Bisarya, as no response had been received from Dr Gary Simpson to date. A letter to be sent to Dr Rob Gillies, Medical Director, requesting a meeting and to establish vision of how work previously undertaken by the abolished clinical senate and GP Operational Group will progress. Dr Bisarya raised an issue of the communication arrangements between GPs and consultants, who are not contactable directly. The only option open to GPs is to contact the medical secretaries and leave a message for the consultant. Jo Worswick will ask Mike Maguire to raise this in his next meeting with Jonathan Parry. Greg Mitten complimented the quality team who had worked hard on the IBR.
SJ / JK
JM
RB/JR
JM
JW
08/13/6
Serious untoward incidents (SUIs) a. SUI report – Merseyside – The committee expressed concern over
the never event regarding a retained swab. Meetings have been arranged by the trust to investigate. Debbie Fagan and Jo Worswick / Jackie Moran will look at the lessons learned and the prevention steps put in place following the meetings. The outcomes will be shared at an internal follow-up meeting. The process of closing a SUI was discussed and Jackie Moran will contact the local area team (LAT) regarding a SUI still open from November 2012 with concerns that an action plan has not been agreed, but the service is continuing.
b. SUI report – Lancashire – Seven SUIs remain open, including
unexpected deaths and attempted suicide for Lancashire Care Foundation Trust. Concern was raised as to the mental health day centres being closed in Lancashire with no alternative service available. The agenda for the mental health contract meetings are long and items is not discussed in depth. Jo Worswick will require benchmarking information and is attending a LCFT quality and performance meeting tomorrow. Jean Rollinson will provide details of a Lancashire suicide group which could provide the benchmark information. Jo Worswick to feedback to the next committee meeting.
JM
JR/ JW

Page 3 of 4
Agenda Item
CCGQIC/
Summary of Discussion Lead
08/13/7
Safeguarding / Individual patient activity (IPA) a. IPA numbers – this item was not discussed.
Safeguarding action plan update - Jean Rollinson outlined the report which provided assurance to the committee that progress was being made towards full compliance with the revised statutory guidance for safeguarding children and the accountability and assurance framework for safeguarding within the NHS. Two new safeguarding posts will commence work across Lancashire with funding from Greater Preston and Chorley & South Ribble CCGs. Links for websites and reports are provided in paper. The self-assessment report was amended with input from the committee to enable sign off. Once changes are made the report will be sent to the LAT to include explanations for the areas which remain amber. GPs are being trained in safeguarding on 17 September 2013. Katie Wightman is looking at on-line mandatory safeguard training to roll out to CCG staff. Jean Rollinson and Dr Jack Kinsey will discuss the designated doctors.
b. Lancashire Safeguarding Children Board annual report 2012-13
The annual report was presented for information. The child exploitation awareness week at end of September, will be communicated in the weekly briefing. A summary document highlighting the various challenges within the annual report will be emailed out with notes and presented to governing body in September.
The quality improvement committee: Noted the content of the report, including the self-assessment of the CCGs current safeguarding arrangements.
JK/JR
JR
08/13/8
Acute Hospital Quality Issues
a. North West Ambulance Service targets – A board has been set up to look at the NWAS performance by Dr Amanda Doyle. Dr John Caine attends the board and will take this work forward.
b. Diabetes mortality – The status remains red and will be mentioned in the letter to Dr Rob Gillies and Liz Yates.
08/13/9 Child and adolescent mental health services (CAMHS) A national-wide shortage of mental health inpatient beds has resulted in children and young people being accommodated on paediatric wards until a bed becomes available. There is also limited access at weekends to CAMHS face to face assessments. This issue is heightened in Lancashire and Dr Ng has raised the issue with the Lancashire Commissioning Support Unit. This is a specialist commissioning responsibility which causes disruption on the paediatric wards, with staff being taken away to deal with the mental health patients. There is a gap in provision as it is managed by different bodies and ownership is an issue. Tim Mansfield is looking into this matter as a pan-Lancashire issue.

Page 4 of 4
Agenda Item
CCGQIC/
Summary of Discussion Lead
Jo Worswick will contact Tim to share the content of a report for Southport & Ormskirk Hospital NHS Trust and the gaps in safeguarding assessments.
JW
08/13/10 Friends and family test The summary of friends and family test results for June at Southport & Ormskirk Hospital NHS Trust were discussed. Ward 9B is a concern and we are continuing to monitor this. As the test is due to commence in maternity wards, the LAT have been asked which trusts have a good uptake and why.
08/13/11 Learning disability self-assessment framework This item has moved on as the self-assessment submission date have been deferred to the end of November. The item will be raised at the next meeting.
JW
08/13/12 Alternative quality contract (AQC) – update Sally Jones reported that the AQC is nearly ready for sign off. The indicators have been trimmed down to focus on those which provide a benefit to the trust. No feedback had been received from Sheilah Finnegan on electronic discharges, which will result in funding not being received by the trust. Sally Jones reported on the incentives which have a direct impact on improving the quality of the service. There are many areas in the AQC which mirror the organisation’s priorities and there is a need to look at the culture. Carole Panteli is involved and will bring in patient and public involvement to the AQC next year. Greg Mitten summarised that there are concerns about recent changes and delayed data provision at Southport & Ormskirk Hospital NHS Trust. If targets are not met funding will not be provided. Mike Maguire will relay the achieved delivery of the AQC to the Executive Committee and the Quality Improvement Committee. Dr Bisarya requested that a letter be sent to a GP when a patient DNAs. This will be added to next year’s AQC.
08/13/13 Quality in primary care Primary care dataset Letter from NHS England on the national approach to improve quality and outcomes in general practice was discussed. This will be addressed at the board development day on 27 August. This request needs to be completed at a GP practice, before being shared with the Membership Committee, to demonstrate how the seven areas have been addressed and to ensure membership engagement. There is however no contractual obligation to complete the proforma. Look at outliers and take forward with support offered.
08/13/14 Business matters Committee meetings dates for 2013-14 were agreed and will be circulated.
CA
08/13/15 Any other business None.
08/13/16 Date and time of the next meeting Tuesday 22 October, 1 – 2.30 pm, venue to be confirmed, Ormskirk

CCG meeting, 27 June 2013 Page 1 of 2
Network of Lancashire Clinical Commissioning Groups held on Thursday 27 June 2013, 2 pm
Meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY
Present: In attendance: Chris Clayton (Chair) - Bwd Gora Bangi – Chorley & South Ribble John Caine – West Lancashire Alex Gaw – Lancashire North Tony Naughton – Fylde & Wyre
Ian Fletcher - Bwd Mike Maguire – West Lancashire Andrew Bennett – Lancashire North Peter Tinson – Fylde & Wyre David Bonson – Blackpool
Mike Ions – East Lancashire
Tim Mansfield – East Lancashire Jill Truby - support
Carl Ashworth (item 6) Samantha Ruthven-Hill (item 6)
1. Apologies for absence Apologies for absence had been received from Ann Bowman, Amanda Doyle, Debbie Nixon, Jan Ledward and Mike Barker. 2. Declarations of interests There were no declarations of interests in relation to agenda items. 3. Minutes of meeting held on 30 May 2013 The minutes of the meeting held on the 30 May 2013 were agreed as an accurate record. 4. Matters arising – action sheet 3.1 Strategic – clinicians still to be identified to join core group to take forward Better Value Healthcare – deferred. 3.2 Governance - on-going 3.3 Legacy issues – no further issues reported 3.4 Scheme of delegation – still waiting final document for signing off The action sheet was updated. 5. Minutes from other meetings 5.1 Members noted the minutes from the Collaborative Arrangements Group meeting held on 11 June 2013. 6. Summary of appraisal methodology Carl Ashworth explained that a joint CCG specialist dementia committee has been established for CCGs to work in collaboration with each other and with the Local Authorities and key stakeholder representatives. Staffordshire and Lancashire CSU is supporting the appraisal process and has developed an appraisal methodology as a technical tool to enable the parties involved to reach a decision ideally on the basis of a consensus. In response to a query Carl confirmed that there was consistency in relation to the papers being presented to each governing body. A question around transport was raised and it was confirmed that this would be considered in the overall deliberation. Members noted the appraisal methodology and that a further report including the recommended “Appraisal Decision” will be provided to the network in August.

CCG meeting, 27 June 2013 Page 2 of 2
9. High risk issues requiring urgent attention Andrew Bennett informed members that he had been contacted by Janet Soo-Chung who had been commissioned as an adviser around the Lancashire Health and Wellbeing Board. Janet had asked if she could meet Lancashire CCGs representatives to explain her brief and it had been suggested that she used the first hour of the July Collaborative Arrangement Group. Following this meeting Janet would then present her findings in an interim report. Members agreed to this request. 12. Any Other Business LWEG (Lancashire Workforce Education Group) – Gora Bangi reported that he was no longer able to attend these meetings following a change of meeting day to Tuesdays. A nominee was sought. 13. Next meeting Next meeting 25 July 2013, meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY. The remainder of the meeting was dedicated to development.

CCG meeting, 25 July 2013 ratified Page 1 of 2
Network of Lancashire Clinical Commissioning Groups held on Thursday 25 July 2013, 9 am
Meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY
Present: In attendance Chris Clayton (Chair) – Bwd Debbie Nixon – Bwd Gora Bangi – Chorley & South Ribble Jan Ledward – Greater Preston/C&SR John Caine – West Lancashire Jo Worswick – West Lancashire Alex Gaw – Lancashire North Andrew Bennett – Lancashire North Ann Bowman – Greater Preston Peter Tinson – Fylde & Wyre Mike Ions – East Lancashire Tim Mansfield – East Lancashire Amanda Doyle – Blackpool David Bonson – Blackpool Iain Fletcher – Bwd Finance Officers in attendance Jill Truby - support Kevin Parkinson – Lancashire North Gary Raphael – Blackpool Iain Stoddart – Fylde & Wyre Mark Youlton – East Lancashire Dr Julia Reynolds/Nicky Dooley – LTH (item 5) Yvonne Rispin/Graham Rose – Blackpool – (item 6) 1. Apologies for absence Apologies for absence had been received from Tony Naughton, Mike Maguire, Paul Kingan, Roger Parr and Mike Barker. 2. Declarations of interests There were no declarations of interests in relation to agenda items. 3. Minutes of meeting held on 27 June 2013 The minutes of the meeting held on the 27 June 2013 were agreed as an accurate record. 4. Matters arising – action sheet Strategy development action sheet updated Lancashire CCGs network action sheet updated The chair informed members of the formation of a subcommittee of the network involving lay member chairs/vice chairs. 5. Clinical research Dr Julia Reynolds and Nicky Dooley of the primary care research business support unit for Cumbria and Lancashire attended the meeting to inform members of the activities of the unit. Members noted the material provided and asked for further information with regards to the GP champions and their role. CCGs were asked to identify a relevant reporting structure for research activity being undertaken in the CCG and to provide a named contact for the network. It was agreed to create a CCG network contact list. ACTION JT 6. NHS 111 Members discussed proposals for working with a stability partner to ensure continued safe provision of NHS 111 service across Lancashire pending a re-procurement, and had further detailed discussions about the proposed future clinical model and ‘footprints’ for the new service. 7. Risk sharing A lengthy discussion took place covering risk sharing and allocations. A number of meetings were being held across the Lancashire patch to discuss the issue of allocation in more detail. Jan Ledward informed members that she, Gora and Ann had met with Richard Barker, NHS North to discuss the issue in detail, following which they had taken revised plans to their governing bodies.

CCG meeting, 25 July 2013 ratified Page 2 of 2
The CFOs reported on a meeting with Jim Hayburn and KPMG. Following discussion it was agreed that the chair would write to Barbara Hakin on behalf of the network. ACTION CC The CFOs were asked to put together a proposal, using examples, for working together and sharing financial risks for discussion at the next joint meeting in October together with integration funding. ACTION CFOs 8. Outbreaks of infectious diseases Iain Fletcher spoke to the two documents issued for consultation by Cumbria and Lancashire Public Health England centre. After discussion members tasked Iain with requesting further validity and a better understanding of the documents. ACTION IF 9. Vascular - latest position The network received an update on the vascular services reconfiguration from Andrew Bennett. Members noted the contents of the report. The chair confirmed that he was happy for Andrew to continue to be the SRO but requested details of exactly what the role and responsibilities were of an SRO. Peter Tinson agreed to write a paper for the next meeting. ACTION PT 10. 12 month plan A draft annual plan was presented for discussion. Members were asked to liaise with Jill around other items for inclusion. 11. JCDS dementia update Debbie Nixon reported that the dementia activity was on-going and progressing well. 12. Collaborative commissioning update Peter Tinson, by way of the collaborative commissioning minutes of the meeting held on 9 July, updated members on the progress of the collaborative commissioning group. In relation to the work around stroke TIA, it was agreed that this would be incorporated in conversations in the clinical strategy steering group and that the collaborative commissioning team would be asked to immediately progress the work. Members noted the minutes of the meeting held on 9 July. 13. Declarations of interests annual update Members noted the annual update of declarations of interests. 14. Feedback / minutes from meetings attended The minutes of the Lancashire Quality Surveillance Group meeting held on 2 May 2013 were noted. 15. Any other business 15.1 A request had been received asking for three CCG representatives to attend the September Overview and Scrutiny Meeting at County Hall to give an overview of the work of CCGs. 15.2 A volunteer was sought to attend the August meeting of the NW Specialist Commissioning Oversight Group. Jan Ledward volunteered if Chris was not available. Gary/Roger/Mark would attend as representatives of the chief finance officers. Jill was asked to co-ordinate meetings. 15.3 A request had been received for the network to nominate a vice chair for the Lancashire Health & Wellbeing Board. Ann Bowman was nominated by the network. 15.4 Military veterans – Debbie Nixon updated members in relation to the military veterans. 16. Next meeting 29 August 2013, meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY - NHS England Lancashire Area Team 31 October 2013, meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY – Finance Officers

25/06/13 NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 10.00 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
Review progress of actions Vs.
weekly action log (45mins)
Review finance and allocation
update, performance and quality
measures (10min)
Month 1 figures available. Reporrting a balanced position.
Fianncial risk was also covered. Spec Comm discussion took place with
KPMG and the work theya re undertaking pan Lancashire. Report from them
is due out 26th June.
Gap between CCGs continues to be discussed with Gtr Preston and C&SR
CCGs. No formal dispute process is in place nationally but there are aother
courses of action availabe. if this si needed.
Month 2 report s have been submitted but due to new guidancde we may
have to chamnge our submission next month.
Rosie Cooper is asking questions on financial positionand needs a brieifn by
the end of June.
Rosie Cooper is asking questions on financial
positionand needs a brieifn by the end of June.
end of June Paul Kingan
10.00 to 10.25 Service redesign / improvement
issues
Update on Mental Health and
Learning Disabilities - J Worswick
(15mins) JW gave an overview of the MH & LD agenda.
Pioneer Integration Bid - S Jeffrey
(10mins) Sharon Jeffreys presented the draft version of the pionering paper. JW noted
that Lacnashire cAre was not an obvious partner to this document and
ntheir profile eed sto be raised.
Connect 4 needs to be raised.
SJ to increase the profile of Lancas Care and
Connect 4.
clinical senate should alos be referenced
by Friday 30th June Sharon Jeffrey
10.25-11.00 AOB / Comfort Break
11.00 to 11.30 Governance issues
Children and Young People - Anna
Bailey (30mins)
AB will link with Lucinda and Jack
AOB / Comfort Break
Jt event with GPs and CVFS 18th July planning meeting taking palce today. Agenda to
be produced by next week. Confirm room
bookings / cancellations.
2nd july Debbie Dobson /
Jodebacker / Greg
Mitten
Health Promotion- Lancashire CC - want to discuss with health promotion
the use of e-cigarettes in Burscough Priory year 11
Jmo to discuss with ANN Bailey who is the best
person to tak ethis up.
It issues MM discussed this with JP Friday 21st June JP to get an update from his IT team and will
come back to us
next weeks meeting with the AT. Joint areas for discussion
12.00pm Wrap up
Summarise actions in action log
after action review
Anna Bailey presented a paper on C&YP Anna Bailey presented a paper on C&YP

16/07/13NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 10.00 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
greg took on the role of patient and pubic voice as Jo DeBacker
has sent apols
Review progress of actions Vs.
weekly action log (45mins)
the health project to engage students in Edge Hill
would benefit from understnadning the results of
work done on the best way to communicate
30.07.13 Lucinda Cawley and
Greg Mitten
there may be a way to support the study by some GPs
into those poatients who would benegfit from the
walking away from diabetes scheme by using CVFS
monies.
30.07.13 Greg Mitten / Ros
Bonsor
Review finance and allocation
update, performance and quality
measures (10min)
PK gave an update on the financial position.
Anticipated allocation now needs to be confirmed as part of the
financial returns to the centre. Our allocation anticipates the
£6.8m coming in from specialist comissioning. The anticpiated
transfer from gtr preston and chorley & SR has not been
anticipated.
Lancashires position re; spec comm has not really change post
the KPMG review. However W Lancs CCG could benefit from
some interntal shifts.
There is therefore a range of anticipated allocations that W
Lancs could expect and these were reflected in PKs discussion.
Key meeting next week with Spec comm and finance officers
pan Lancashire.. Meeting with Gtr Preston and Chorley &SR has
not been forthcoming.
The financial position is now feeling more firm and thus we can
begin to sign some contracts.
10.00 to 11.00 Service redesign / improvement
issues
Planned Care & Procurement
Strategy (30mins)
JM gave a review of the planned care strategy for W Lancs CCG.
Executives agreed that the CCg should continue to use the
referral gateway and that its use should be encouraged across
the Gp practices
Further detail was requested on the reprocurement of Tier2 and
Reinvigourate Referral Gateway project
Paper back to Board for approval
10/09/2013 Jackie Moran
Bridging the dementia diagnosis gap
(10mins)
JW gave an overview of the dementia work underway. Approval
to work with LCFT given by Execs
NHS 111 (10mins) Letter received from Amanda Doyle (Blackpool CCG) for
discussion at the network. There will be a need to reprocure
next year but use a stability partner in the shorterm - NWAS.
Executives were asked to give their views.
Could W Lancs be tagged onto Mersey NHS 111
reprovision rather than Gtr Preston / C&SR - phone
numbers may be the limiting factor.
Jo W bring back obsevations from the network
meeting next week?
30th July Paul Kingan
Jo Worswick
Risk profiling (10mins) info to be sent out to pratices today and discussion to take
place at Peer review on Thursday
execs had discussion about the methodology that was being
undertaken in pactices now and what could be learned.
Bapi to prepare info for Peer Review re: how we might
reduce readmissions or develop medicines
optimisations to influence strategic change from the
risk profiling tool
18th July Bapi Biswas
11.00-11.30 AOB / Comfort Break
11.30 to 12.25 Governance issues
Birleywood health centre (30mins) design is complete for Birleywood. the project has been out to
tender and there is now a temporary and permanent solution in
place. Multiple approvals are being sought for this scheme.
The capital development will leave voids in the space and the
cost of these voids will be picked up by the CCG. Discussion took
place about how to fill the voids in brierley wood. it was agreed
that it might make sense to move the Diabetes centre into this
location
JM to discuss with Dave Walmseley to understand
what the impact of the development at brierley wood
will have for the CCG and whether there are options
to fill the voids
A revised business case is to be received by the
Executives in due course
ASAP Jackie Moran
Safeguarding policy updated policy was discussed. HC took Executives through the
paper and GPs thought this paper was very useful particularly
the flow charts.
Integrated business report Pk took the Executives through the financial and activity
performance in the IBR
it was noted that there was an error in the information re: HCAI
cDiff
12.25pm Wrap up
Summarise actions in action log after
action review

30/07/13NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 10.00 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
Review progress of actions Vs.
weekly action log (45mins) BB raise an issue re; end of life / the link to EMIS web and the ability for sites to have access to EPCCS web
portal.
The IT strategy is to be developed soon. This is a prioity and should be approved as soon as possible. The
financial costs were discussed and Execs agreed this would be prioritised.
risk sharing agreement needs to be completed for this
EPCCS to be rolled out and put in place
the financial allocation will be earmarked for this
Katie
Paul K
Review finance and allocation
update, performance and quality
measures (10min)
CFOs have been discussing this and we have kept our line regarding only being open to discussing financial
budgets in totallity and not just the specialist commissioning element.
Jim Hayburn made the deicison that the agreements made to date need to be the basis of CCGs planning
assumptions.This means our CCG can plan on the baiss of the £6.8m coming back for spec comm for us.
Jo W gave additional feedback from the network. The major issue was the consideration of a risk share
agreement, however the CFOs present at the meeting stated they would prefer an informal risk share
agreemnt rather than a formal agreement.
10.00 to 11.10 Service redesign / improvement
issues
Update on site appraisal for specialist
dementia beds (10mins)
Jo W gave feedback of the meeting that she had attended were the results of the scoring options for the
location of the dementia beds was discussed. LCFT will consider the support services that will be provided
alongside the new build. W Lancs reserved the right to send patients to other providers of dementia beds.
At the next meeting the details will be confirmed and a paper will be prepared for CCGs to take the
decision to their board. A communications strategy will be run alongside the approvals process.
Dialogue with Merseycare re: ability to send our
patient to them if required.
03/09/2013 Jo W
CAMHS access (30mins) Graham Pattinson gave an overview of the issues with regard to CAMHS service and S&O hospitals. Access
to inpatient crisis beds has been an issue. the pathway is working ok but the capacity of beds is not
sufficient both within the NHS and in the independent sector.. The only remaining option as a place of
safety has therefore been a paediatric ward for children under 16 which really is not appropriate for this
type of patient and for those others on the wards. options to alleviate this situation have been considered.
The options are the continued use of paediatric wards perhaps using medication to manage patients,to
use crisis teams from other areas or increase the numbers of inpatient beds in Lancashire. NHS England
specialist commissioning are now responsible for commisisoning inpatient beds.
Executives noted the issues and agreed actions regarding the services in which they had a commisisoning
interest.
CSU to undertake a stocktake of the paediatric ward
GP to work with LCFT to refresh the pathway and to
improve education of staff including paediatric
consultants of what is available .
JoW to Continue link with tim mansfield into specialist
commissioning
QIC to consider this issue and to escalate this to spec
commissioning as necessary
20/08/2013 CSU / Jo W
Graham Pattinson
Jo W
JM
AOB / Comfort Break (20mins)
Time to think proposal (10mins) Terry Mears gave an update as to the new model of "time to think"beds. It was agreed that this discussion
would continue at the nurisng and care home beds event that Sharon is organising
Presentation from Terry Mears to be shared with
Sharon so she is aware of this proposal
06/08/2013 Paul Kingan
11.10 to 11.20 Governance issues
CCG Assurance (10mins) JoW gave an overview of the CCG Assurance process and the meeting that is to take place in August.
Executives were invited to attend this meeting if they were available.
11.20pm Wrap up
Summarise actions in action log after
action review
AOB LC gave an overview of a meeting on healthcheck programme. Certain practices have not yet sigend up to
this with LCC.
LC to present the information to practice managers
meeting tomorrow 31/07/13 31/07/2013
Lucinda/ JO
Debacker

06/08/13 NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 10.00 Assign ADP Roles for the meeting
(5mins)
PK to make amends via Joanna to last week's notes 06.08.13 Paul Kingan
To add to the agenda to agree the notes from the last
meeting by exception only 13.08.13 Mike Maguire
Complex packages of care to come back to exec in
3mths 05.11.13 Paul Kingan
Jean Rollinson to pick up discussion with Katie
Wightman re info sharing from EPACCs and
transferrability to MASH 13.08.13
Jean Rolinson &
Katie Wightman
Assign ADP Roles for the meeting
(5mins)
Review progress of actions Vs.
weekly action log (45mins) See actions noted above
Current discussions about allocations seems relatively positive for the CCG. There is an eagerness within
the system to reach a conclusion on the specialise commissioning issue. There has been agreement and
discussion on this through the DoFs in a series of meetings last week. PK will be meeting with P/C/SR CCGs
for final balances on the allocations. PK and Area Team (AT) have met with regard to their agreement on
the 2% plans - CCG to prepare a risk assessment of the financial position to allow the AT to sign off the 2%
plans which focus around AQC.
Submit business case to AT for 2% sign off 09.08.13 Paul Kingan
Paul noted the request from AQUA to meet to discuss subscription Meeting to be arranged TBC Paul Kingan, Mike
Maguire & John
Caine
10.00 to 10.30 Service redesign / improvement
issues
Armed Forces Community Covenant Simon presented the armed forces covenant and noted that he has been in contact with the lead CCG on
commissioning for armed forces. The Exec agreed to sign up to the Covenant.
Katie to check if this requres a Governing Body
decision.
13.08.13 KW to confirm sign
off
Referral Gateway Simon noted that a nuber of patients referred back to the GP as IRG hadn't been able to contact the
patient. Will be investigated.
To be investigated by Jackie 20.08.13 Jackie Moran
10.30 to 10.50 AOB / Comfort Break (20mins)
10.50 to 11.20 Governance issues
Safeguarding Jean has produced a safeguarding action plan that will be reported to the Quality Cmte. There has been
recruitment into the safeguarding service. Jean is establishing which organisation holds the funding for the
Mental Capacity Act following the reforms. Safeguarding GP will be leaving and needs to be recruited to
which is a Area Team responsibiity but likely CCG will want involvement. Will be discusssed at the Quality
Cmte. CLA Adoption Panel Advisor role - CCGs being asked to contribute despite view that it is LA
responsibility. Meeting due to take place this week on this and Jean to feedback to Katie on this. CLA
health assessments within 4wks - target not met with gap in 16-18yr olds. MASH business case will be
presented to CCGs in Oct '13 - focus on commissioning the health input into MASH going forward. CAMHS
statutory inspection action plan from January being proressed.
Jean to update Katie after meeting to discuss CLA
adoption panel. Jean to attend Exec every month.
Business case on MASH to be presented to Exec
20.08.13
(CLA) and
Oct (MASH
business
case)
Jean Rollinson
Verification of Expected Death
Training
The Exec agreed to support the offer made by Karen Groves with regard to training for verification of
expected death. Noted the need for robust governance for nursing home verification of death. Exec
noted the importance of establishing the policy before the training. Also keen to understand any recurrent
expectations of training
To respond to Karen to say the CCG is happy to be
involved with the development of a policy with
training to follow and would like to understand the
recurrent aspects of the training. To note that OOH
need to be involved
20.08.13 Simon Frampton
Contingency Plan Katie presented the draft busines continuity policy and plan. She noted that as a new organisation the
document is not written on a team by team basis. Katie outlined the action plan (appendix 2) which
incudes templates for ensuring accurate record keeping during times of crisis. Exec agreed the business
continuity plan.
CCG major incident plan to be drafted (cat2
responder)
Mid October
2013
Katie Wightman
11.20pm Wrap up
Summarise actions in action log
PK to make amends to notes from last week via Joanna re alloctions
Review finance and allocation
update, performance and quality
measures (10min)

13/08/13NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 10.05 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
John confirmed that he has resigned from the OWLS Board
Notes from the last meeting were agreed
Sunquest ICE - follow up as part of IT strategy including
potential training issues
20.08.2013 Bapi Biswas, Paul
Kingan
Prepare agenda for membership focussed on urgent
care, acute visiting service and ambulatory care,
ECIST, winter schemes proposed by Trust
01.09.2013 Paul Kingan
Data not been updated in risk profiling tool and this to
be raised wit Derek Kitchen at CSU
20.08.2013 Mike Maguire
AQC indicator summary to be shared with Exec -
agenda for next week
20.08.2013 Mike Maguire
10.05 to 10.45 Service redesign / improvement
issues
Friends and Family test Detail to be provided at quality cmte but overview to Exec given. First published in June with further roll
out planned. Ward 9B (medical) in bottom 10 wards with response rate of >15% (n=10) with neutral
response for recommendation (n=4). Ward 11B also flagged. Action plans are in place.
No actions noted
Demonstration - Performance
Management Dashboard
Sally presented the prototype of the dashboard and the exec agreed for continued development of it No actions noted
ECIST Draft Report Request practcies to undertake a nursing home audit
and for information to be brought to next
membership meeting for discussion related to ECIST
recommendation on nursing homes
Membership
18.09.2013
Paul Kingan (Sharon
Jeffery)
Draft agenda for board development to be brought to
Exec next week
20.08.13 Mike Maguire
10.45 to 11.05 Comfort Break / AOB
11.05 to 11.30 Governance issues
Update on CCG Assurance Katie summarised the Q1 assurance process No actions noted
Need to understand timescales from Jo re the
establishment of the adult ADHD service in LCFT
20.08.2013 Jo Worswick
To include the need to understand number of meds
requests going through IFRs as part of discussion with
CSU about reporting
End August
2013
Jackie Moran & Paul
Kingan
MCA Implementation Lead
Commissioning of post
Katie outlined the duty the CCG has on ensuring the MCA post. The background was explained and the
options for taking this forard - see paper. The Exec agreed to support option "4.2.i"
Katie to feedback to Jean Rollinson 16.08.2013 Katie Wightman
11.30am Wrap up
Summarise actions in action log
Refer to presentation
Notes from the last meeting
Review progress of actions Vs.
weekly action log (45mins)
First cmte met on 21.07.2013. Standing items prescribing moniotring report and final year figures.
Discussion of busget for this year and allocation across practcies (capitation weighted model capped at
either end). No practice saw a decrease on the budget which the cmte saw as fair. ToR agreed minimum
of 4 members including one GP and NB to ensure quoracy. Some potential issues identified coming from
Lancs and Mersey Cmtes - see cmte minutes
Medicine Management Committee
minutes
KPMG review has been concluded. Resolution on allocatons is nearing completion. PK offered again to
meet with P/C/SR CCG to finalise issues. "% money being held by AT - PK has submitted a business case
and discussion with AT as part of Q1 asurance will be to seek sign off. Further discussion about how we
deploy the reaminder of the 2% non rec money. Winter pressures funding is not coming from the 2% but
further clarity awaited re route of funding and allocations. Funding for GP IT delegated from AT to CCG
based on historic spend. Further work ongoing re funding/underwriting IT issues that are critical for
business continuity. One aspect is for GP capital money where there is notification of money coming back
in from the AT to support this (EMIS, kit relacement and wireless). Meeting planned with Stephen Lord for
20.08.2013.
Review finance and allocation
update, performance and quality
measures (10min)
No actions noted

20/08/13 NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 9.50 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
Constitution - this was submitted with minor amends. Letter received back from NHS England to confirm
these changes have been approved. KW to now change conflict of interest policy. Amended constitution
is on the CCG website
KW to change conflict of interest policy 04/09/2013 Katie Wightman
360 degree feedback - KW updated on dual running appraisal process - part of performance against
objectives and 360 degree feedback against the behaviours that are agreed as demonstrating the
organisational values.
Add free text to bottom of the questionnaire. For full
governing body to also undertake the 360 following
completion of that for staff
For staff to
have
feedback
session by
mid Oct. Aim
for governing
body
Katie Wightman
Comfort Break / AOB (30mins)
10.20 to 10.40 Governance issues
Board Development Agenda (10mins)
MMg outlined the proposal for the board development day Ros to be second facilitator
Medicines Optimisation Care Home
Medication Review Service (10mins)
NB presented a business case for additional capacity for conducting regular medicines reviews on nursing
and residential home. Been identified as a priority from the frail elderly ICPG. It was agreed that this
would be approved on a permanent basis
SIP feed to be included within commissioning
intentions end Sep 2013 Nicola Baxter
10.40 to 11.20 Service redesign / improvement
issues
Develop a template for business cases 03/09/2013 Jackie Moran, Karen
and Bapi
Greg to feed into Jackie CVFS organisations at risk 30.08.2013 Greg Mitten
Jackie to ask Joanna to send deadline around to CCG
staff and clinical leads for long list of schemes
20.08.2013 Jackie Moran
High level principles for screening long list to be agreed
at weekly senior team meeting
27.08.2013 Senior Manager
Paul to exec long list of schemes to be filtered,
headline principles and draft business case
03.09.2013 Paul Kingan
Agreed list of schemes to be worked up into the
agreed business case template
13.09.2013 All
Headline principles to be further refined to be used to
prioritise the business cases (by 13th Sep)
13.09.2013 all
Decision taken at exec on which schemes to be taken
forward
01.10.13 all
Karen Thompson to seek further information and
assurance from Gulab Singh re affordable warmth
work via WLHWB Group
Karen Thompson
11.20am Wrap up
Summarise actions in action log
Discussion about how we might need
to change our plans in light of:
- Health and social care integration
(top slice)
- Care closer to home
- ECIST review
- Winter planning
- Possible use of in year non
recurrent (one off) money
(40mins)
Agreed as an accurate record
Notes from the last meeting (5mins)
Review progress of actions Vs.
weekly action log (30mins)
Review finance and allocation
update, performance and quality
measures (10min)
PK has met with Iain Crossley at P/C/SR CCG. ToR agreed for the joint work which will start 9th Sep. ToR
state to work within the existing numbers within all budgets, not just specialist. Key meeting on Wed with
CFOs in Lancashire to discuss letter from specialist commissioning re process for rest of the year and
managing any outstanding issues. PK to update at next meeting. Whilst this seems positive there are still
risks that the CCG needs to be aware of and manage. Draft working papers have been released re
allocations formula for next year which would be positive for our CCG. Need to plan for a flat settlement.
Allocation confirmed for GP IT capital - upgrade to EMIS web confirmed along with replacement kit but
wireless developments not approved as yet. PK & BB have meeting with Stephen Lord. LASCA have to
make efficiency savings reflecting national consolidation of these services which may pose a potential risk -
the CCG will continue to monitor this.
Any headline items for AOB
Paul Kingan
PK introduced a debate about how we prioritise financial monies that may be available this year - whilst
may change working on an assumption of 1-2m. Areas discussed included - preventing readmissions
related to COPD. Need to clarify conflict of interest in terms of arguable investment required in primary
care. Need to be aware that CCtH does not cover all of our 11 programmes of work. Prescribing central.
Principles should include our duty on health inequalities. Role of rescue packs for improving outcomes -
example of rescue packs for COPD - seems to be an enabler. Need a realistic assessment of what can be
delivered by year end. Opportunities for working with other partners to lead such developments but
needs balancing against building internal capability. Need to build in seasonality of CCG staff roles
.ie.planning guidance at xmas and contracting. Question about how to ensure participation of the
Membership in agreeing priorities for the spend. Need to agree a timescale for business cases for
intentions. COPD - Practices identifying vulnerable patients - staffing for winter - pilot for social support for
discharge - visiting service for nursing homes - backfill staff in CCG
PK to check text in discussion notes before circulation 20/08/2013

03/09/13 NOTES OF THE MEETING
Discussion and Decisions This weeks actions Due DateResponsible
officerRAG
9.00 to 9.50 Assign ADP Roles for the meeting
(5mins)
Assign ADP Roles for the meeting
(5mins)
Notes from the last meeting (5mins)Agreedas accurate record
Any headline items for AOB Tri board agenda, ipad training, personal healthcare budgets
9.50 to 10.20 Service redesign / improvement
issues
Care Closer to Home Programme
(20mins)
Janice Horrocks, Programme Sponsor for Care Closer to Home introduced herself. Jancie gave an update
of where the programme is currently up to outlined the aim to identify any areas which may need
strengtheing. She is reporting back to the Strategic Partnerhips Board on 11 Sept.
It was noted that public engagement is key to transformational change.
Agreed that programme needs to refocus back on to community care in local areas which was one of the
main aims of the programme.
Noted that communications plan begin developed across the 3 organisations for the programme.
Standardisation of community nurse service provision would be beneficial. Need to establish a baseline of
what is being provided currently by community staff.
Proposed addtional worsktreams - workforce, IT
Janice to attend Exec to feedback.
Janice to meet with Greg re CVFS sector.
Ensure LCC are represented at SPB.
end Sept JH
JH
MM
111 Interim Arrangements (10mins)
Letter noted.
JM to review OOH contract to esnure still robust
end Sept JM
10.20 to 10.40 Comfort Break / AOB (20mins)
ipad training ipad training training arranged for 22 Oct after board development session 22/10/2013 KW
Tri board meeting on 18 sept. Any additional agenda items to be sent to Mike today. 04/09/2013 MM
Personal health budget broker
Personal budget pilot being undertaken across the country and may be featuring in the media in the
coming months
Need to develop local strategy. Discuss at next board
development session. 22/10/2013 MM
Quality committee letter
Quality issues - letter sent to new medical director re enagement mechanisms and mortality info - no
repsonse as yet.
Add letter to tri board agenda 04/09/2013 MM
10.40 to 12.25 Governance issues
AQC scheme and the associated
indicators (25mins)
Sally Jones presented an update of the current position of the AQC indicators and the data to be collected .
All indicators are agreedby the Trust and monitoring will begin.
Staffing levels - some hospitals publish staffing levels eg. Hope
AQC indicators agreed.
Monitoring to be lead by clinical leads and to form part of IBR
Sense check audits to be carried out for some
indicators eg. Cancleled outpatients.
Sally to follow up publishing of staffing levels with
Adam Robinson.
MM to check with PK over any possible unspent AQC
money as result of not meeting indicators
Establish finncial position for AQC informing trust of
funds achieved and funds that are at risk.
AQC indicators to be discussed at Membership
Dec 13
Nov 13
17.9.13
1.10.13
Nov 13
SJ
SJ
MM
SJ/PJ
JC
Safeguarding Training and Prevent
(45mins)
Jean Rollinson, Head of safeguarding gave a presentation on safeguarding in the new NHS and on Prevent
which is aimed at stopping people becoming terrorists
Escalation Procedure For Monitoring
Compliance With Safeguarding
Standards Via Provider Contracts
(5mins)
Procedure has been updated to include sanctions for providers. Lead commissioner will notify assocaite
commissioner of any issues.
Procedure approved
Peer Review Agenda (15mins) Agenda discussed. Peer review to be held first and then split into 3 groups to discuss solutions re urgent
care systems and processes.
Add ambulatroy primary care, whole systems review, EISS review to agenda
Send reminder to practices to look at urgent care data
and to have had a practice meeting to discuss.
A&E info sharing agreeement to be checked.
Book venue for March Peer Review
JD
JD
JD
Update on Quarter 1 CCG Assurance
(5mins)
Update provided on final dashboard results following quarter 1 assurance process. Postive results gained
with no red areas on high level summary report and just 1 red indicator relating to cancer waits.
Action plan for the 1 red indicator to be submitted by
4 Sept
4.9.13 JW
Balancing the Budget 2014/15
(5mins)
Response discussed with suggestions additions to the response - any costs that would result in increase in
costs that would result in reduced access to healthcare services eg. Car park charges at or near to
healthcare facilities and use of reserves as long as not resulting in issue next year.
Amends to be made to letter which can then be sent
to WLBC
11.9.13 KW
Governing Body, Board
Development Days and Quality
Improvement Committee dates for
2014-15 (5mins)
Dates for future meetings discussed. Approved. Need to amend 17 Sept to be Dev day.
Feedback any issues over dates to Cathy
24.9.13 KW
12.25am Wrap up
Summarise actions in action log after
action review / Any Items Discussed
for Membership Committeee Suggestion would be both Chair's netwotk, IM&T group, IG Sterring Group, One West Lancashire, HWB
Board, SPB, 111,. Membership goes to GB,
Consider what meeting minutes need to be brought
for info the Exec
10/09/2013 KW
Review finance and allocation
update, performance and quality
Allocation issues with former PCT CCG split on going. Meeting taken place with Preston & Chorley CCGs.
Further meeting on 12 Sept.
03/09/2013
Review progress of actions Vs.
weekly action log (30mins)

Page 1 of 2 West Lancashire Clinical Commissioning Group Remuneration Committee – 20 August 2013
Minutes D R A F T
Meeting Title: West Lancashire Clinical Commissioning Remuneration Committee
Date: 20 August 2013
Time: 12.30 – 1.00 pm Venue: Boardroom, NHS Central Lancashire, Ormskirk
Present: Douglas Soper, Lay Member (Chair) Greg Mitten, Lay Member Dr Adam Robinson, Secondary Care Doctor In attendance Carol Sheard, Associate Director of Workforce CSU Cathy Ashcroft, Executive Assistant Paul Kingan, Chief Finance Officer (part of item 4)
Apologies: Helen Clarke, Chief Nurse
Agenda
Item Summary of Discussion Action
1. Welcome, Introductions and apologies for absence Doug Soper welcomed all present to the meeting of the Remuneration Committee and introductions were made. Apologies were noted.
2. Minutes of the previous meeting The minutes of the meeting held on 9 April were approved as an accurate record of the meeting.
3. Declarations of interests No declarations of interests pertinent to agenda items were raised.
4. Agreeing recommendation to governing body on terms and conditions of: GPs Paul Kingan, Chief Finance Officer, stated that in the absence of any national guidance for GP payment, CCGs in Lancashire commissioned Price Waterhouse Cooper LLP to undertake a benchmark exercise across Lancashire and to recommend rates of pay for GPs undertaking work for CCG’s. The paper recommends that a specialty lead should be paid within a range from £260 – £350 gross per session. The employment status recommended in this case is either Contracted or Employed. Doug Soper highlighted that the rate for governing body GPs is £350 gross per session, plus travel with no backfill locum payment required. The membership of the monthly Prescribing Committee includes two non-governing body GPs who require payment for attendance. As attendance is on a regular basis, the employment status and payment method will be discussed between Paul Kingan and Carol Sheard separately. The committee agreed that a rate of pay of £300 per session should be recommended. The Remuneration Committee recommend to the Governing Body:
The rate of pay for a non-governing body GP with membership on the Prescribing Committee to be £300 gross per session.

Page 2 of 2 West Lancashire Clinical Commissioning Group Remuneration Committee – 20 August 2013
Travel expenses will continue to be paid at standard rates, with no backfill payment provided.
The Chief Finance Officer will determine the Employment Status taking appropriate advice as required.
Doug Soper added that the Prescribing Committee membership also includes a practice nurse. Discussion ensued to determine the appropriate rate of pay for the practice nurse. It was suggested that this role maybe similar to that undertaken by the practice managers who attend the Clinical Executive. Following discussion it was agreed that the same rate £30 per hour gross would be recommended with no back fill costs. The Remuneration Committee recommend to the Governing Body:
The rate of pay for the practice nurse attending the Prescribing Committee should be £30 gross per session, for a maximum of four hours (including preparation)
Travel expenses will continue to be paid at standard rates, with no backfill payment provided.
The Chief Finance Officer will determine the Employment Status taking appropriate advice as required.
5. Any other business
None.
6. Date and time of next meeting To take place when required.

Page 1 of 5 West Lancashire Clinical Commissioning Group Audit Committee – 16 July 2013
Minutes D R A F T
Meeting Title: West Lancashire Clinical Commissioning Audit Committee
Date: 16 July 2013
Time: 1.30 – 3.30 pm Venue: Boardroom, NHS Central Lancashire, Ormskirk
Present: Douglas Soper, Lay Member (Chair) Dr Adam Robinson, Secondary Care Doctor Dr Jack Kinsey, Clinical Lead In attendance Paul Kingan, Chief Financial Officer Katie Wightman, Head of Corporate Affairs Fiona Blatcher, External Audit (Grant Thornton) Tommy Rooney, External Audit (Grant Thornton) Liz Squires, Internal Audit (Audit North West) Chris Morris, Head of Fraud, Counter Fraud Claire Ward, Counter Fraud Cathy Ashcroft, Executive Assistant
Apologies: Greg Mitten, Lay Member Dr Bapi Biswas, Clinical Lead Helen Clarke, Chief Nurse
Agenda
Item Summary of Discussion Action
1. Welcome, Introductions and apologies for absence Doug Soper welcomed all present to the meeting of the Audit Committee and introductions were made. Apologies were noted as above.
2. Minutes, matters arising and Chair’s action The minutes of the meeting held on 9 April 2013 were approved as a correct representation of the discussion. Matters arising from the previous minutes included: Page 1, 1. The Audit Committee terms of reference, within the Constitution, had been amended to reflect the addition of two clinical leads as voting members of the committee. The decision had been approved at the Membership Committee and the amended Constitution had been submitted to NHS England for approval. Page 3, 7. A recommendation to the Governing Body to contract Internal Audit for a period of three years was pending, due to the possible merger of Audit North West (ANW) with Mersey Internal Audit Agency (MIAA). Once the decision and detail of the merger is known, at the end of September, the recommendation would return to the Governing Body. If the merger proceeds Tim Crowley may be approaching organisations regarding the terms of contract. The action sheet was updated.
3. Declarations of interests No declarations of interests pertinent to agenda items were raised.

Page 2 of 5 West Lancashire Clinical Commissioning Group Audit Committee – 16 July 2013
4. Risk register and board assurance framework (BAF) The Audit Committee’s role is to provide assurance to the Governing Body that risks are being managed effectively. The key areas were highlighted as follows:
One new risk has been added around a legacy issue of an apparent lack of governance in relation to the brief therapy support services. This is being investigated by all three former central Lancashire CCGs. The Executive Committee will be updated accordingly.
The two risks with a risk score of 12 are being managed or have action plans in place.
One risk has been removed from the register – Access is now available to historical datix reported incidents and a new reporting system is in place.
The risk register is a live document which will be shared at each Audit Committee, informally at the Executive Committee two weeks prior to its presentation at the Governing Body meeting in September.
- The members noted the risk register and board assurance framework.
Katie Wightman
5. Fire, health and safety and first aid The CCG has a statutory obligation in relation to fire, security and health and safety. Following recent assessments at the CCG premises, no significant issues had been identified. Fire – rated tolerable – another inspection will take place on the new Hilldale accommodation Security – IT recommendations are being actioned Health and safety – very few minor issues were identified with all being resolved.
- The members noted the report and action to date and that planned.
6. New arrangements for dealing with suspected fraud Chris Morris stated that NHS Protect had written to Chief Financial Officers outlining the new arrangements for dealing with suspected fraud. NHS Protect are asking CCGs to nominate a Local Counter Fraud specialist. The paper proposes that Audit North West Counter Fraud lead is nominated as the CCG Local Counter Fraud Specialist. NHS England will determine if the CCGs will abide by the same standards as those adopted by their organisation.
- The members agreed to the proposal to nominate Claire Ward as the CCG Local Counter Fraud Specialist.
Katie Wightman
INTERNAL CONTROL
7. Internal audit
Progress report Liz Squires provided a verbal update on current progress. A formal audit report with progress against plan will be presented in future. Work has commenced on the plan.

Page 3 of 5 West Lancashire Clinical Commissioning Group Audit Committee – 16 July 2013
Central Lancashire PCT and transfer of recommendations The report lists the audit providers appointed to the successor organisations. As the PCT addressed many audit recommendations prior to abolition, the report was for information to help inform CCG processes going forward. External Quality Assessment The External Quality Assessment (EQA) has assessed the ANW’s in the context of internal auditing standards. The EQA overall opinion concluded that ANW meets the highest grading available to the latest release of the International Standards of the Institute of Internal Auditors. Recommendations are being addressed within the merger with MIAA. - The members thanked the internal auditors for the update.
8. External Audit Central Lancashire PCT 2012/13 audit findings report Fiona Blatcher provided an outline of the report, which highlights the key findings from the 2012/13 audit of Central Lancashire PCT including an unqualified opinion of the annual accounts. The following points were highlighted for awareness: Continuing care provision – the value of the provision is recognised as
an estimate. The Chief Financial Officer reported that the CSU have a team dealing with the claims, but the full impact will not be known for 2 – 3 years.
A payment in advance made to a provider. VFM section – in preparation for the Commissioning Support Unit,
consultancy support was engaged at short notice and the proper procurement process was not followed.
There were no issues specific to West Lancashire CCG. Planning fee letter The planned audit fee letter for 2013/14 was presented. The scale fee had been set by the Audit Commission at the lowest charge for a small organisation. Tommy Rooney was introduced as the Audit Manager appointed to West Lancashire CCG. A detailed audit plan will be produced in March 2014. The VFM section will be returned when the detail is available. - The members thanked the external auditors for the update.
9. Counter Fraud Annual workplan 2013/14 Claire Ward presented the annual workplan in which the Governing Body’s responsibilities are outlined. The CCG will receive fraud notices to raise awareness of current issues. The plan will reflect risk areas from other NHS organisations. A risk assessment of the CCG will result in a revised plan. There are no outstanding legacy issues to be transferred to the CCG.
- The committee accepted the workplan

Page 4 of 5 West Lancashire Clinical Commissioning Group Audit Committee – 16 July 2013
Bribery Act Guidance The Bribery Act 2010, which came into effect from 1 July 2011, makes it a criminal offence to give promise or offer a bribe, and to request agreed to receive or accept a bribe, either at home or abroad. This paper is for information to raise awareness for all CCG staff using a survey and a presentation. Katie Wightman confirmed the Bribery Act is referenced in the CCG’s conflict of interest policy. It was agreed that presentation will be delivered at the Executive Committee, followed by the Governing Body on 24 September, with information to be shared with the Membership Committee. NHS Protect update The NHS Protect Information and Intelligence Unit’s (IIU) third report to Local Counter Fraud Specialists was presented for information. Invoice Fraud Claire Ward explained that following the NHS Protect ‘Strategic Intelligence Assessment for 2011-12, identifying invoice fraud as a risk area with potential for growth, the guidance document was developed to provide an understanding of the invoice fraud threat facing the NHS. This includes procedures to put in place to ensure this does not occur. Pre Contract Procurement Fraud Corruption The guidance can be used to support work to prevent and detect procurement fraud and corruption at a local level. The processes within the document can protect an organisation in terms of payment of fraudulent invoices. - The members thanked the external auditors for the update.
Claire Ward
10. Financial position Paul Kingan highlighted the key areas for information:
A balanced plan for the CCG had been set with a required 1% surplus and 1% contingency.
The CCG has a small underspend at month 2 Risk around the national allocations is being discussed with
specialist commissioning and other CCG’s. It is expected that the funding allocation being returned to the CCG is currently sufficient, however, until the allocations solution has been finalised the CCG is declaring a £2 million financial risk which is preventing contracts from being signed.
The full QIPP is £2.9 million and has been applied to commission budgets.
Working with the CSU and Area Teams to develop the use of the single ledger
Liz Squires will provide a support tool which alleviates duplications in payments.
- The members noted the financial position
11. Losses and special payments Paul Kingan confirmed that there were no losses and special payments to report.

Page 5 of 5 West Lancashire Clinical Commissioning Group Audit Committee – 16 July 2013
12. Single tender waivers Paul Kingan confirmed that there were no single tender waivers to report.
TRANSITION /LEGAL ARRANGEMENTS
13. Progress report Paul Kingan raised the following key issues: The CCG had received guidance on which balances would transfer to
CCGs. Continuing care provision is the key balance for the CCG. The CSU provision has improved and service is good, with support from
a relationship manager. Staff are getting used to new ways of working and systems including
single ledger. Work with the CSU continues around high cost packages with clinical
input. All critical and hospital payments are being paid on time, although it is
unlikely that the CCG will achieve its better payments practice targets this year.
Legacy and transition issues are discussed regularly at the Lancashire Chief Financial Officer communication meeting.
REPORTS OF SUB-COMMITTEES / MINUTES OF MEETINGS
14. Formal Local Assurance Group minutes – 18 March 2013 NHS Audit Committee minutes – 18 March 2013 - The minutes were noted.
ANY OTHER BUSINESS
15. Any other business No other business was raised.
16. Date and time of next meetings Tuesday 12 November at 1.30 pm, to be confirmed
Meeting closed at 2.45 pm