nicu protocol
TRANSCRIPT
GENERAL GUIDES TO DAILY NICU PRACTICE
(1) Blood samples from mother, to be kept in plain tube for GXM, to avoid delay of transfusion when necessary.
(2) Name tag to be put on all babies at all time during hospitalisation.
(3) Low birth weight babies < 2kg At 15th day of life to commence Vidalyn drops without iron at 1ml daily and folate 1mg/ml daily. At 28th day of life to commence Vidalyn with iron and continue the folate. Every Tuesday to take Hb/retics, LFT, calcium, phosphate and alkaline phosphatase. To weigh babies on Tuesday and Friday. Plot on the growth chart according to
chronological age. Add human milk fortifier to EBM when feeding established to 6mls per feed.
(1packet to 50mls breast milk or 1/8 packet for 6 mls breast milk).
(4) Ventilated babies 6 hourly ABG if ill no paralysis if rate < 30/min BUSE daily FBC EOD Serum creatinine twice weekly.
(5) Admission: To give IM vitamin K 1mg stat if has not been given. For premature babies, to score gestation age (Dubowitz or Parkin or Ballad). Breast feeding advice must be given to mother and record real time in the note.
(6) Discharge, to do: Full neonatal examination. Discharge summary and reply letter should be written. Babies with NNJ may be reviewed in their respective Child Health Clinic. If immunization is due, to get the vaccine from Postnatal Ward and give baby before discharge. Withold BCG for 3 months if baby has received IVIG. Instruct mother properly about the review.
(7) Strictly handwashing and drying before and after handling baby. No jewellery and long fingernails.
(8) Feeding guideline for premature baby:
Consider to add Polycose 1gm QID alternating with MCT oil 0.5-1.0ml QID after
tolerating orally ½ of total requirement.
1
Birth weight (gm) Age to start feeding (day)<1000 7
1000-1199 51200-1499 3
>1500 1

(9) TPN to be started on day 2 or 3 of life for baby birth weight < 1.2kg, necrotising enterocolitis or surgical cases involving intestine (perforation or obstruction).
Parameters FrequencyCalory assessment
Weight DailyFluid: input and output Every 24 hrsCalorie Every 24 hrsSerum albumin weeklySerum amino acids As indicated
Glucose ToleranceBlood glucose At least daily for 7 days then 2X a weekUrine glucose and ketones Daily
Lipid ToleranceGross lipemia DailySerum cholesterol/ triglycerides
Weekly
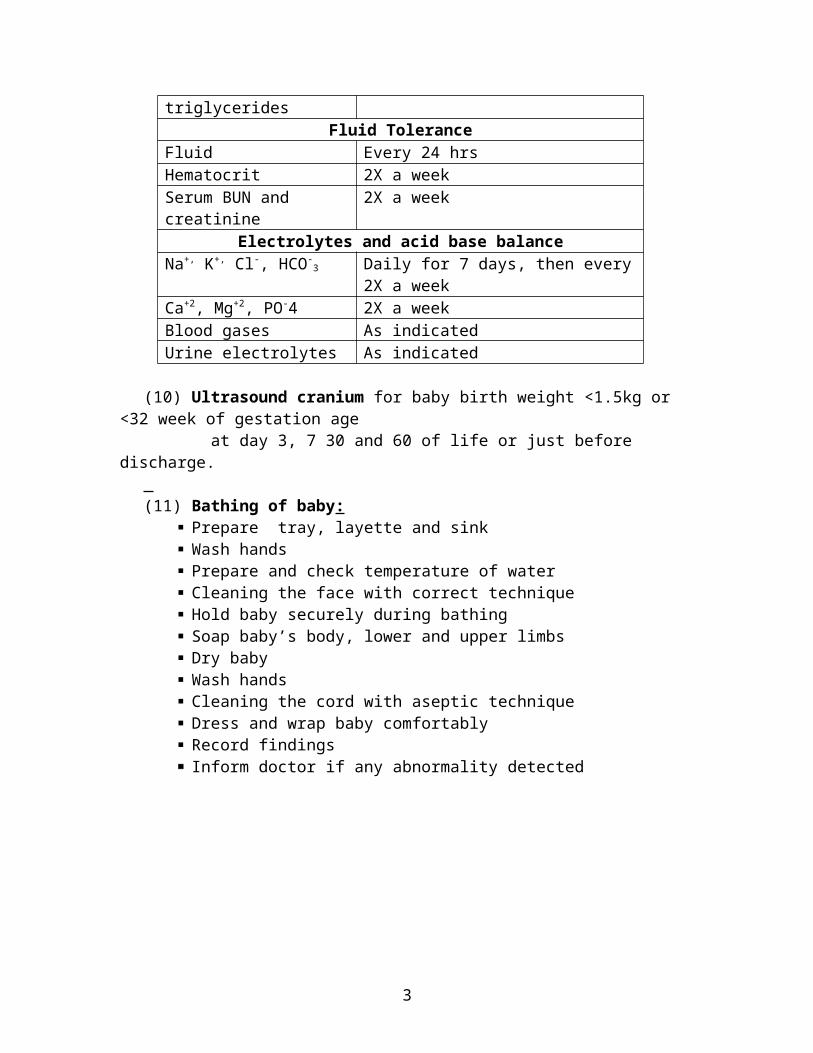
Fluid ToleranceFluid Every 24 hrsHematocrit 2X a weekSerum BUN and creatinine 2X a week
Electrolytes and acid base balanceNa+, K+, Cl-, HCO-
3 Daily for 7 days, then every 2X a weekCa+2, Mg+2, PO-4 2X a weekBlood gases As indicatedUrine electrolytes As indicated
(10) Ultrasound cranium for baby birth weight <1.5kg or <32 week of gestation age at day 3, 7 30 and 60 of life or just before discharge. (11) Bathing of baby:
Prepare tray, layette and sink Wash hands Prepare and check temperature of water Cleaning the face with correct technique Hold baby securely during bathing Soap baby’s body, lower and upper limbs Dry baby Wash hands Cleaning the cord with aseptic technique Dress and wrap baby comfortably Record findings Inform doctor if any abnormality detected
2
(12) Pupils dilation regime for ROP screening (at 2pm appointment): Baby NBM from 1.00pm One drop Amethocaine 0.5% or 1% at 1.99pm. One drop Cyclomydril at 1.05pm, 1.20pm and 1.40pm
3

GUIDELINE FOR VARIOUS LEVELS OF NEONATAL CARE
DefinationsLevel I For uncomplicated maternal and neonatal cases where routine
nursing care is necessary and close observation is not requiredLevel II For neonates with problems requiring close observation and
intervention but not requiring intensive careLevel III For neonates with problems requiring intensive care
Indications for admission to various levels of care
No LEVEL III (Neonatal intensive care)
LEVEL II (Special care)
LEVEL I
1. Respiratory distress Birth weight 1500-2500gm Borderline low birth weight (1.7-2.5kg)
2. Moderate to severe perinatal asphyxia
< 35 weeks gestation Borderline premature (35-37 weeks gestation)
3. Severe birth trauma -subaponeurotic haemorrhage, fractures, intracranial haemorrhage
Large babies ie birth weight > 4.0kg
Neonatal jaundice
4. Congenital heart disease-heart failure, supraventricular tachycardia, arrhythmia
Small for gestational age babies ie <10th centile
G6PD deficient
5. Hypotension, shock Respiratory distress requiring FiO2<40%
Maternal chorioamnionitis or pyrexia > 38% or leaking liquor 18hrs
6. Need for resuscitation and inotropic support
Mecoium below cords during resuscitation
Meconium below cord during resuscitation with no respiratory distress or hyperinflated chest
7. Disseminated intravascular coagulation
Rhesus or ABO incompability Asymptomatic infant of diabetic mother
8. Immediate post-op surgical patients Mild asphyxia or Apgar Score < 7 at 5 mins
Asymptomatic baby with risk of sepsis needing antibiotic therapy
9. Necessity for morphine infusions Sepsis and congenital infection
Social issues eg abandon baby, single parent
10. Necrotising enterolitis (grade 2 and 3)
Symptomatic infant of diabetic mothers
Mother with HIV or VDRL positive
11. Hydrops foetalis Hypoglycaemia (<2.6mmol/L) Maternal thyrotoxicosis12. Neonatal seizures Seizures13. Multiple or major congenital
anomaliesMother drug addict
14. Low birth weight infant < 1.5kg Multiple or serious congenital anomalies
15. Persistent metabolic acidosis Infants requiring surgery and do not require intensive care
16. Intractable hypoglycaemia Unwell baby eg lethargy, poor feeding, vomiting
17. Significant birth trauma
4

NORMAL BLOOD PRESSURE AND HEART RATE FOR CHILDREN
Normal blood pressure of newborn in the first 12 hours of lifeBirth weight (gm) Systolic Diastolic Mean
1000-2000 49-52 26-31 35-402000-3000 57-64 32-38 41-45
>3000 65-70 39-43 50-54
Normal blood pressure in infants and children
Normal heart rates in infants and childrenAge Average
(beats/min)Minimum
(beats/min)Neonate of 1st week 140 100
1-3m 160 1103-6m 150 120
6m-1yr 150 1201-3yr 130 1003-5yr 100 705-10yr 90 60>10yr 80 60
RANGES OF NEUROTHERMAL TEMPERATURE FOR NEONATES
Age Birth weight in gram<1200 1200 - 1500 1501 - 2500 >2500
24 hrs 34.0 - 35.5 33.5 - 34.5 33.0 - 34.0 32.0 - 33.524-48 hrs 34.0 - 35.0 33.0 - 34.0 31.5 - 33.5 30.0 - 33.048-96 hrs 34.0 - 35.0 33.0 - 34.0 31.0 - 33.0 30.0 - 33.04-14 days 33.0 - 34.0 31.0 - 33.0 29.0 - 32.02-3 weeks 32.0 - 34.0 30.5 - 33.53-4 weeks 31.5 - 33.5 30.0 - 32.5
Age Systolic (mmHg) newborn 80 ± 15 6m-1yr 90 ± 30
1-2yr 100 ± 252-4yr 100 ± 205-6yr 100 ± 158-9yr 100 ± 15
11-12yr 100 ± 15
5

BREAST FEEDING AND FORMULA MILK FEEDING PRACTICES
Breast milk is the preferred milk feeding for all neonates in our neonatal units. However under certain circumstances, where breast milk is not readily available, or inconditions where it may be contraindicated in feeding, breast milk is substituted with a suitable formula milk.These formula milks are usually cow’s milk-based; occasionally soy-based or elemental formula milks may be given in special conditions.
Conditions where formula milk may be used in place of breast milk are:(1) Mothers whom have not produced adequate amounts of breast milk. In these mothers, the neonates are encouraged to breastfeed as to stimulate milk production; however, formula milks are given as supplements until adequate amounts of breast milk is produced.
(2) Mothers whom are unable to produce breast milk, or where obtaining breast milk is not feasible, or where breastfeeding may expose the neonate to harm: (a) Mothers whom have passed away post-partum (b) Mothers ventilated in an intensive care setting immediately post-partum (c) Mothers whom have undergone bilateral mastectomy (d) Mothers with specific medical conditions, or on treatment for medical conditions, which may interfere with breast milk production (e) Mothers with untreated aggressive or violent behaviour
(3) Conditions where feeding with breast milk is specifically contraindicated as it may cause harm to the neonate: (a) Maternal human immunodeficiency virus (HIV) infection (b) Maternal consumption of anti-neoplastics or similar chemotherapeutic medications (c) Maternal drug abuse in the immediate peripartum period (d) Neonates with inborn errors of metabolism, e.g. phenylketnouria and galactosaemia
EVALUATION OF BREAST FEEDING TECHNIQUENo Good Positioning Good Attachment1 Baby faces the breast Baby mouth is open wide2 Baby's head and body in a straight line and
close to the mother's bodyBaby's chin touches the breast
3 Support baby's shoulder on the left forearm and buttocks in the left palm
Baby's lower lip is curled outward
4 Move baby towards the breast and not breast towards the baby
More areolar is seen above than below the mouth
6

RESUSCITATION OF NEWBORN INFANT
StatisticsThe greatest mortality in childhood occurs in the first year of life and is highest in the first month; 45% of all childhood (<14 years) death occur in the first 28 days of life.80% of all neonatal deaths, 46% of all infant deaths and 23% of all childhood (<14 years) deaths occur in the first week of life.LBW (<2.5kg) infants comprise 7% of all births but 2/3 of all neonatal deaths; they are 40X more likely to die in the neonatal period compared to those born >2.5kg.VLBW (<1.5kg) infants represent 1% of all births but 50% of all neonatal deaths; 20X more likely to die.1% of all newborns will need vigorous resuscitation involving artificial ventilation.0.5% of term newborns need intubation; 50% of infants born <28 weeks will require resuscitation and intubation.5% of infants born at 35 weeks will need active resuscitation.
Indications For A Paediatrician To Be Present At Delivery
Prematurity: gestation <36 weeks Fetal distress:
thick MSL abnormal CTG/ fetal bradycardia fetal scalp acidosis (pH< 7.2)
Operative delivery: complicated instrumental delivery delivery under GA
Multiple pregnancy Significant antepartum haemorrhage Fetal disease:
known major congenital abnormalities Rhesus disease
Causes Of DeathVary with age
< 1 month: congenital abnormalities (40%) factors associated with prematurity (45%) birth asphyxia (10%) others (5%)
1-12 months: cot death >1 year: trauma
Cardiac arrest in childhood is seldom due to primary/ ischaemic heart disease but to respiratory distress(eg. MAS, IRDS, FB, asthma, croup; depression: eg. convulsion, raised ICP, poisoning, drugs) or circulatory (fluids loss: eg. bleeding, AGE, burns; fluid maldistribution: eg. septic shock, congenital heart disease, anaphylaxis)
7
Recognition Of Seriously Ill ChildThe earlier recognition and management of potential respiratory, circulatory or central neurological failure will decrease mortality and secondary morbidity.
RespiratoryTachypnoea (N< 60/min)RecessionGruntingFlaring
CirculatoryHeart rate (N 110-160)Pulse volume: absent peripheral pulses and weak central pulses are serious signs of advance shock and indicates that hypotension is already present.Capillary refill: digital pressure x 5 sec, N < 2 sec.BP: hypotension is a late and pre-terminal sign (SBP = 80 + [age in year x 2])
Central NeurologicalAlways assess ABC before neurological assessmentConscious level:
A= AlertV= responds to voiceP= responds to painU= unresponsive
Posture: HypotonicDecorticate (flexed upper limbs, extended lower limbs)Decerebrate (extended upper and lower limbs)
Pupils: DilatationUnreactivityInequality
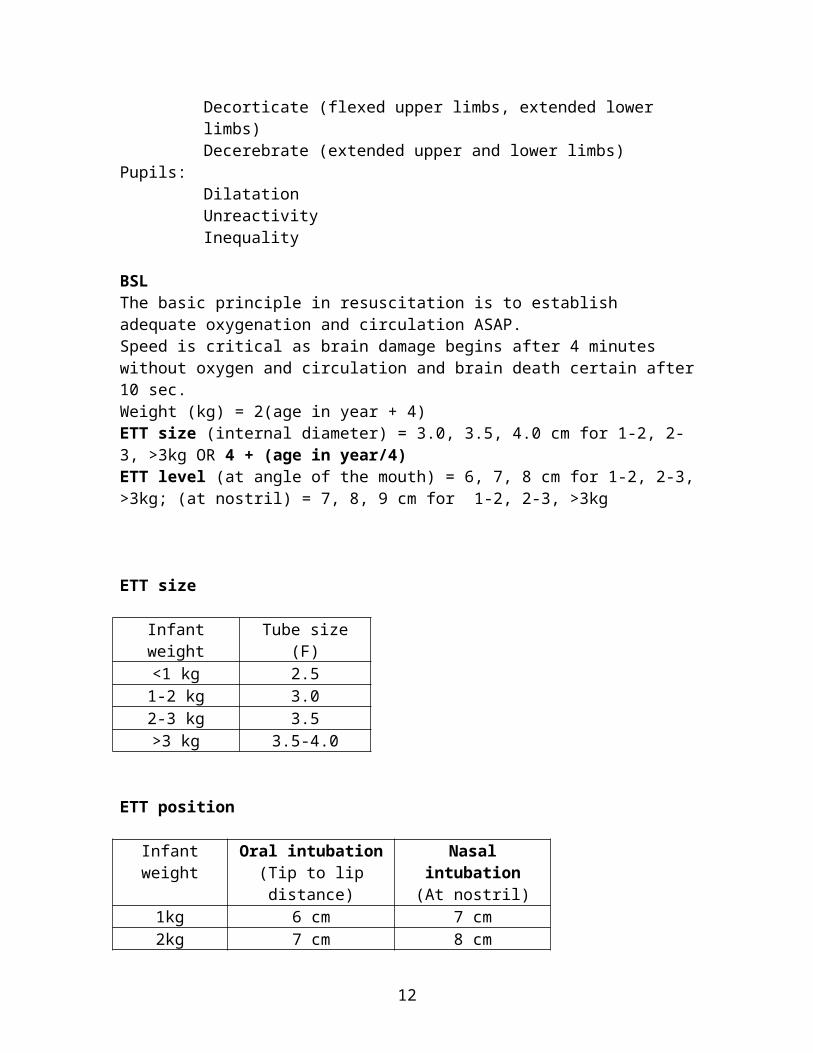
BSLThe basic principle in resuscitation is to establish adequate oxygenation and circulation ASAP.Speed is critical as brain damage begins after 4 minutes without oxygen and circulation and brain death certain after 10 sec.Weight (kg) = 2(age in year + 4)ETT size (internal diameter) = 3.0, 3.5, 4.0 cm for 1-2, 2-3, >3kg OR 4 + (age in year/4)ETT level (at angle of the mouth) = 6, 7, 8 cm for 1-2, 2-3, >3kg; (at nostril) = 7, 8, 9 cm for 1-2, 2-3, >3kg
8

ETT size
Infant weight Tube size (F)<1 kg 2.51-2 kg 3.02-3 kg 3.5>3 kg 3.5-4.0
ETT position
Infant weight Oral intubation(Tip to lip distance)
Nasal intubation(At nostril)
1kg 6 cm 7 cm2kg 7 cm 8 cm3kg 8 cm 9 cm
Equipment1. Adequate shelf with overhead heater2. O2 supply up to 10 L/min3. Adequate suction ( ~100mmHg = 136cmH2O)4. Stop clock5. Facemask, ambubag (240ml)6. Oropharyngeal airways7. Laryngoscopes8. Magill forceps9. ETT size 2.5, 3.0, 3.5 cm10. Syringes, needles, specimen bottles11. Adhesive tape, scissors12. Stethoscope13. Equipment for UAC/UVC/IVD, chest tube, etc.14. Warm dry towels
Drugs1. Adrenaline: IV 0.01mg/kg, 1/10,000, 0.1ml/kg (max 10ml), repeat dose 0.1mg/kg;
ETT/ intracardiac 0.1mg/kg of 1/10002. Calcium gluconate (levulaenate) 10% IV 1ml/kg; calcium chloride 10% 0.3ml/kg3. NaHCO3 8.4% IV 1ml/kg; dilute to 4.2% 2ml/kg in infants4. Atropine 1mg/ml, 0.01mg/kg, 1/10 0.1ml/kg IV5. Narcan 20mcg/kg IM6. Lasix 1-2mg/kg IV7. 0.9% N/saline; Dextrose 25% 1-2 ml/kg IV8. Vit K >2kg = 1mg, <2kg = 0.5mg IM
9

The Infant Who Does Not Respond To Resuscitation Poor technique. The infant may not be ventilating because the bag and mask is being
used inappropriately, or the ETT is not sited appropriately. Iatrogenic: hypothermia, pneumothorax due to over-vigorous resuscitation. Underlying disease: consider diaphragmatic hernia, TOF, cyanotic congenital heart
disease, hypoplastic lungs.
When to stop resuscitation?All babies deserved to be considered for active resuscitation unless they are macerated or show an obvious lethal congenital abnormality, eg. Edward, Patau syndromes.In those with no cardiac output after 15min, active resuscitation should be abandoned.If the baby is not breathing by 40min, and particularly if he remains extremely depressed with severe hypotonia, then further active resuscitation should be considered inappropriate.
10
KRAMER’S CHART: CORRELATION BETWEEN LEVELS OF SERUM BILIRUBIN WITH AREA OF SKIN THAT IS JAUNDICED
Jaundice first appears at the face and progress downward as it becomes more severe to the chest, abdomen, thigh and leg and sole of feet. Area of body Ranges of indirect bilirubin
mg/dL (umol/L)Head and trunk 4-8 (68-135)Upper trunk 5-12 (85-204)Lower trunk and thigh 8-16 (136-272)Arms and lower legs 11-18 (187-306)Palms and soles >18 (>306)
It may be difficult to assess jaundice in dark skinned infants.The distance of the light source from the baby is 35-50cm.Light wavelength 425-475nm.Light intensity 6-12 uW/cm2/nm.
Intensified phototherapy 26-40uW/cm2/nm.
11
EXCHANGE TRANSFUSION
Indications:(1) Failure of phototherapy: serum bilirubin continues to rise and remains > 340 umol/L in healthy term infant or 310 umol/L in sick babies.(2) Acute neurological changes present with severe jaundice when first diagnosed or during phototherapy.(3) Severe anaemia (<10g%) together with severe jaundice.Blood group:(1) If Rh incompatible, the donor blood should be of the same blood type of the baby BUT Rh negative.(2) In the case of ABO incompatibility, the donor blood is of type O and Rh type of the baby. (3) In other causes of severe jaundice, the donor blood is of the blood and Rh type of the baby. The blood should be preserved with citrate-phosphate-dextrose and preferably be less
than 72 hours and in any case not more than 5 days old. Volume of blood to be exchanged is 160 ml/kg (twice the body volume) and not more
than 500ml. Ensure that the tip of the umbilical venous catheter is not in the portal circulation by
limiting entry of the catheter not more than 5 cm (or less, once free flow of blood can be established).
The procedure must be done aseptically and be accurately timed, regulated and recorded.
Monitor continuously the heart rate, blood pressure, oxygen oxymetry and preferably ECG.
Aliquots usually used in neonatal exchange transfusion: (5ml/kg)Volume (ml)Body weight (kg)
5<1101-2152-320>3
The first aliquot should be of the desired volume and no need a step up increment. The rate of exchange in each cycle:
1 min withdrawal1 min interval1 min infusion Drugs used:
1ml for every 100mls outIV Sodium Bicarbonate0.1ml for every 160mls outIV Calcium Gluconate
Prewarm the blood and agitate it periodically to prevent settling of red cells. Maintain the baby in a neutral thermal environment under a radiant warmer and
restrain the extremities. The whole procedure should not be less than 1 hour. Usually lasts 1-2 hours. Limit rise in bilirubin by resuming phototherapy immediately after the exchange is
completed. Monitor vital sign hourly and serum bilirubin 6 hourly for at least next 24hrs.
12

Keep NBM and the umbilical vein catheter until at a SB level that can convincingly avoid another exchange transfusion.
Antibiotic prophylaxis: IV Ampicillin 50mg/kg/dose BD IV Gentamicin 5mg/kg daily Beware of complications: infection, vascular complications, coagulopathies,
electrolytes abnormalities, hypoglycaemia, metabolic acidosis, metabolic alkalosis, necrotising enterocolitis.
Exchange transfusion investigations:Post-ETPre-ET
FBC/pltBUSE/RBSSB-direct and indirectBlood C+SVBGCa2+/albumin
FBC/plt/reticBUSE/RBSSB-direct and indirectBlood C+SCoombs-direct indirectG6PDPBFHBsAg/VDRL
13

INTRAVENOUS IMMUNOGLOBULIN IN NEONATES
Indications:(1) Clinical sepsis in premature infants, term infants, 1st 4weeks of life.(2) Neonatal jaundice due to ABO incompatibility
Dose: IVIG 1g/kg Giving over 4 1/2 hours Start infusion with 1ml/hr for 30 min, if no reaction to increase to maximal dose for 4 hours Repeat IVIG after 24 hours of the 1st dose
Adverse reactions: (1) Hypotension(2) Hypoglycaemia(3) Anaphylaxis
Caution: All baby received IVIG (high dose), the immunization schedule (including BCG) must be deferred for 3/12.
Reference: Cochrane neonatal review 25th Nov 2003
14

IVIG THERAPY FOR NEONATAL JAUNDICE SECONDARY TO ABO INCOMPABILITY
HYDROPS FETALIS
15
No admissionif SB < photo level
If SB > photo level
Make decision on admission based on the SB result
Admission to level 1
Start phototherapy
Repeat SB after 4 hours together with maternal and blood group
If SB rising more than 10umol/L/H or SB near ET level and confirm ABO incompatibility(discussion with specialist)
To start IVIG – dose 0.5gm/kg over 41/2hours
Monitor SB 4 hourly and continue phototherapy
If discharged – TCA 3 months to repeat FBC (late onset anaemia)
All baby jaundice at D1 of life
Take SB
Inform Paed MO SB result
Repeat SB 6 hourly

Defination: newborn infant with gross subcutaneous oedema, commonly associated with ascites, pleural effusions and nearly always has an enlarged oedematous placenta.
Causes:Fetal Haematological Homozygous alpha-thalassemia,
fetimaternal haemorrhage, twin to twin transfusion
CVS Cardiac malformation, fetal arrhythmias, AV shunts
Pulmonary Diaphragmatic hernia,cystic adenomatoid malformation
Renal Congenital nephrosis, Wilm tumourInfection Syphilis, Parvovirus, Toxoplasmosis,
CMVChromosomal Turner syndrom, Trisomies 18 and 21,
triplodyMaternal DM, toxaemia, anaemiaPlacenta Chorioangioma, umbilical vein thrombosisIdiopathic 50% cases of non-immunological hydrops
Investigations:Antenatal Neonatal
Blood Ix: blood group, rhesus, minor Antigens, Antibodies (AB, RH, minor), Betke-Kleihaur, VDRL & TPHA, TORCH, alpha-fetoprotein, Hb, Hb electrophoresis, GTT.
Blood Ix: FBC platlet and retics, PBF, G6PD, Hb electrophoresis, Blood group, Coombs test TORCH, syphilis, BUSEC, LFT, cultures, karyotype.
Ultrasound Placenta histologyAmniocentesis X rays, ECHO, ECG if still alife
Autopsy
16

SURFACTANT THERAPY FOR RDS
Indications: Moderate to severe respiratory distress syndrome
Eligibility Criteria: (1) History of prematurity (2) Birth weight ≥ 1.0kg (3) Age of baby within 24 hours of life (the 2nd dose < 12 hours apart) (4) No gross congenital anomalies (5) Baby is stabilized without severe complications eg pneumothorax, severe birth asphyxia and frank sepsis. (6) IRDS required ventilation support (a) on mechanical ventilation (b) if on nasal CPAP, PEEpressure 5 mmHg for wt < 1.5kg and FiO2 > 50% wt > 1.5kg and FiO2 > 70% indication for intubation, ventilation and surfactant (7) Clinical evidence of moderate to severe IRDS: (a) respiratory rate > 80/min (b) marked subcostal / intercostals / sternal recessions (c) CXR reveals a white-out lungs (8) a-A ratio < 0.22 (9) Early surfactant rescue for moderate RDS Criteria for early surfactant rescue therapy for RDS: (a) premature baby age <6 hours of life
(b) on nasal CPAP requires O2 of 50% or more Then to intubate baby for administration of surfactant.
Calculation of a-A ratio: (1) From chart by plotting Pa O2 vs PaCO2, check against FiO2
To the left of line ie <0.22 : for surfactant To the right of line ie >0.22 : not for surfactant (2) By calculation:
a-A ratio =
713 x FiO2 (%)
100PaCO2(mmHg)
_
NB: mmHg = 7.5 x kPA
17
PaO2 (mmHg)

Surfactant dosageName : SurvantaDosage : 4ml/kgFirst dose to be given as soon as eligibility criteria has been metSecond dose should be given 8 hours after the first dose (no less than 6 hours apart)
Equipment Vial of Survanta 10 ml syringe Alcohol swab 19 gauge needle ET tube with side tubing or Ryle’s tube
Preparation
Warm Survanta at room temperature for 20 minutes before administration or 8 minutes if warmed in the hand
Ensure the following are in place : arterial line for ABG and intraarterial BP monitoring, pulse oxymetry and ECG monitor.
Ventilated infant Intubate infant with appropriate size ETT and ventilate using IMV or AC mode Baseline ABG Suction of ETT Administer ½ of the dose with the head and body inclined slightly up and administer
½ of the dose with the head and body inclined slightly down Total duration of administration : 15-20 minutes After surfactant administration, ventilation mode for:
Wt 1.0-1.2kg, high frequency ventilation Wt >1.2kg, continue IMV
Monitoring As response is rapid, be ready to decrease the ventilatory pressure and FiO2
quickly Repeat CXR after surfactant Hourly ABG for 4 hours followed by 4-6 hourly Continuos ECG and SaO2 monitoring Keep infant in supine position. No physiotherapy or suctioning for at least 4 hours Be aware of blockage of ETT may occur especially with ETT size < 3.0F
18

RADIOLOGICAL GRADING OF SEVERITY OF RESPIRATORY DISTRESS SYNDROME
Grading SeverityGrade I Fine reticulogranular mottling, good lung expansionGrade II Mottling with air bronchogramsGrade III Diffuse mottling, heart borders just discernible, prominent air
bronchogramsGrade IV Bilateral confluent opacication of lungs (‘whiteout’)
19

MECONIUM ASPIRATION SYNDROME
Incidence 9% of all term neonates have meconium-stained liquor (MSL). 56% of neonates with MSL have meconium in their trachea. 20% of neonates with MSL develop MAS.
Pathogenesis Fetal distress prior to birth stimulates intestinal peristalsis and relaxation of the anal sphincter. Fetus < 34 weeks gestation does not relax its anal sphinter even with severe distress. Therefore, MSL/MAS in preterm babies, always consider congenital infections. Aspiration may occur in utero in a distress, gasping fetus, or more usually, meconium is aspirated into a lung immediately after delivery. Meconium in the small airways causes obstruction and air trapping and atelectasis. Surfactant dysfunction contributes to MAS.
Complications Pneumothorax is common (up to 30% of severe MAS). Chemical pneumonitis. Secondary bacterial infection is common. PPHN. Abnormal pulmonary vascular spasm with arteriolar thickening causes pulmonary hypertension leading to PPHN.
Clinical Features Babies are term or post-term or IUGR. Meconium staining of the skin, nails and umbilical cord. Respiratory distress may present soon after birth or more usually, over the first 12 hours with tachypnoea, recession, grunting, flaring, cyanosis, and a hyperinflated chest. Metabolic acidosis, hypoglycaemia, and signs of birth asphyxia and pneumothorax are common.
Diagnosis Diagnosis is based on a combination of meconium stained liqour, meconium in the
trachea and CXR changes. CXR: hyperinflated with coarse fluffy opacities, pneumothorax, pneumomediastinum, and cardiomegaly.
Differential diagnosis IRDS. Congenital pneumonia. Aspiration pneumonia. Birth asphyxia with raised ICP. Diaphragmatic hernia. TTN.
20

Air leak syndrome – pneumothorax, pneumomediastinum, PIE. Lobar emphysema, heart failure, PPHN, pulmonary hypoplasia, choanal atresia, and metabolic acidosis. Congenital muscular disorders, anaemia, and hypovolaemia.
ManagementPrevention MAS is preventable by careful antenatal monitoring, rapid delivery for fetal distress and rapid resuscitation and tracheal suctioning at birth. Clear the mouth and pharynx as soon as the head has been delivered. At birth, larynx should be inspected directly and trachea sucked below the cords of any meconium. Nine percent of neonates have meconium in the trachea despite it being absent from the mouth and pharynx.
Treament All babies with meconium below the cords should be admitted to the NICU for
observation and further management.
Mild Moderate SevereNBMRT free flow and 4H aspirationBM 6HIVDIV C Penicillin + GentamicinHead box O2
SpO2 hourlyVital signs
NBMRT free flow and 4H aspirationBM 6HIVDIV C Penicillin + GentamicinHead box O2
Continuous SpO2 + cardiac monitoringVital signsInotropic supportConsider treatment for associated birth asphyxia.
NBMRT free flow and 4H aspirationBM 6HIVD + UACIV C Penicillin + GentamicinMechanical ventilation/sedation/paralysis Equipment for tension pneumothorax.Continuous SpO2 + cardiac monitoringVital signsInotropic supportTreat associated birth asphyxia.
FBCBlood C+SBUSECRBSABGCXR
FBCBlood C+SBUSECRBSCa/albuminABGCXR
FBCBlood C+SBUSECRBSCa/albuminABGGXMCXR
21

Advances HFOV ECMO Surfactant Amnioinfusion
Outcome Mild to moderate MAS requiring no assisted ventilation usually recover within a few days. Overall mortality rates is 25%, up to 50% in those needed assisted ventilation. Both the mortality and long term developmental sequelae are related to the severity of the underlying perinatal asphyxia.
22

SURFACTANT LAVAGE FOR MAS
Criteria Term newborn with MAS Baby requires ventilator support within 6 hours of life
Surfactant lavage Dilute 8ml of surfactant with 32ml of normal saline Choose one position: right lateral or left lateral Administer 2ml of diluted surfactant into the distal ETT Manual bagging to keep SpO2>90% ETT suction to clear up the administered surfactant In between suctioning, to manual bagging and keep SpO2>90% Repeat the same position once more Repeat the same step twice consecutively on the same position (total 5 cycles) Perform until the 40ml diluted surfactant finish
Monitoring Continuous SpO2 (preductal and postductal) Blood pressure Heart rate ABG and ventilator settings at 0, 60, 120 min, 4 hourly after starting surfactant
lavage
23

VENTILATION STRATEGY IN NEONATE WITHOUT PPHN
Pneumonia, sepsis, asphyxia
Respiratory distress needed FiO2 ≥ 70% or poor effort/apnoea
MAS < 6h,surfactant lavage, 8ml in 40ml
Intubate and for conventional ventilatory support
RDS < 24h,surfactant 4ml/kg
Hypoxia persists,*ruled out PPHN/cyanotic CHD
Increase conventional setting, lung recruitment strategy
Concurrent management of hypotension, acidosis and hypercarbia
Hypoxia persists even with MAP ≥15cmH2O and FiO2 100%.*
For HFOV,Entry MAP at 2cmH2O above the conventional.
Hypoxia persists*
Optimize HFOV setting CXR, keep diaphragm at 9th posterior rib
Response
Maintain or wean setting according to SaO2
Hypoxia persists
Presumed PPHNKiv start MgSO4, iNO
History, clinical ± CXR
24
*Check for evidence of PPHN frequently. Evidences of PPHN:
(1) Preductal SpO2 ≥ 5% than postductal(2) Preductal SaO2 ≥ 10% than postductal(3) ECHO: increase PA pressure(4) Persistent hypoxaemia can not be explained by lungs condition

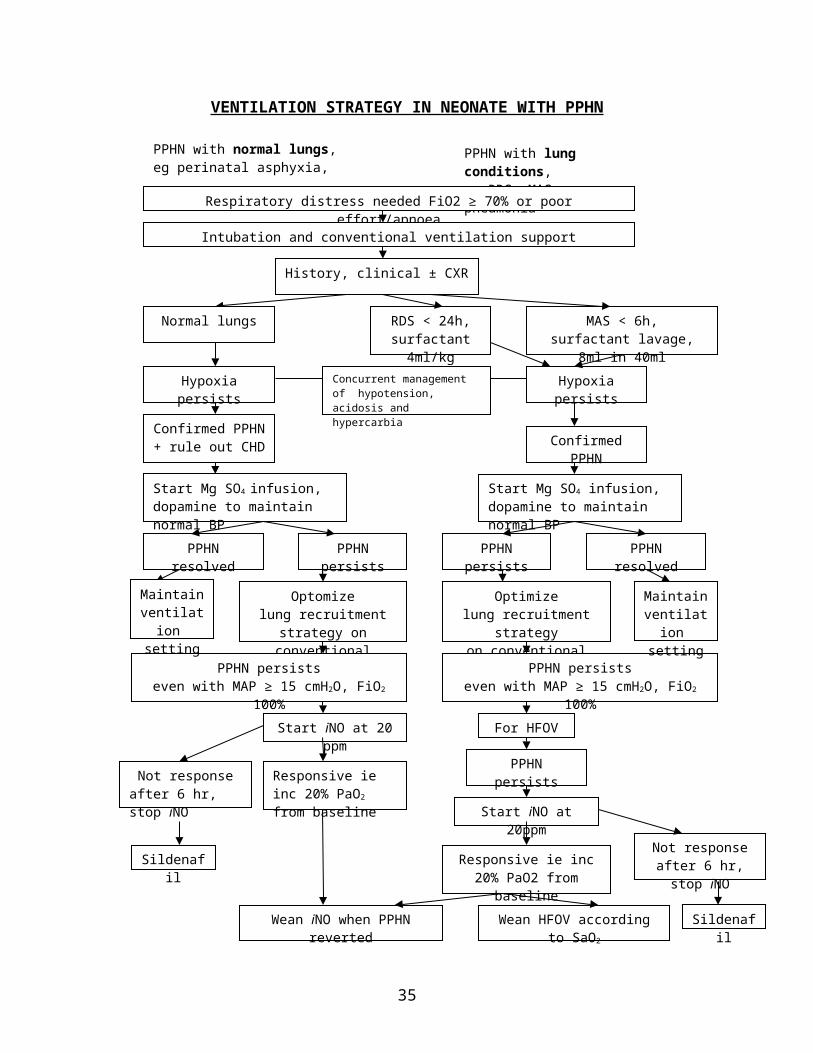
VENTILATION STRATEGY IN NEONATE WITH PPHN
PPHN with lung conditions,eg RDS, MAS, pneumonia
Respiratory distress needed FiO2 ≥ 70% or poor effort/apnoea
Intubation and conventional ventilation support
RDS < 24h,surfactant 4ml/kg
MAS < 6h,surfactant lavage, 8ml in 40ml
Hypoxia persistsHypoxia persists
Confirmed PPHN+ rule out CHD Confirmed PPHN
Concurrent management of hypotension, acidosis and hypercarbia
Start Mg SO4 infusion, dopamine to maintain normal BP
Start Mg SO4 infusion, dopamine to maintain normal BP
PPHN resolved PPHN persists PPHN persists PPHN resolved
Optimizelung recruitment strategyon conventional ventilator
Optomizelung recruitment strategy on conventional ventilator
PPHN persistseven with MAP ≥ 15 cmH2O, FiO2 100%
PPHN persistseven with MAP ≥ 15 cmH2O, FiO2 100%
Start iNO at 20 ppm For HFOV
PPHN persists
Start iNO at 20ppm
Responsive ie inc 20% PaO2 from baseline
Responsive ie inc 20% PaO2 from baseline
Wean iNO when PPHN reverted Wean HFOV according to SaO2
Maintainventilation
setting
Not responseafter 6 hr, stop iNO
Not responseafter 6 hr, stop iNO
Sildenafil
History, clinical ± CXR
Normal lungs
Sildenafil
Maintainventilation
setting
25
PPHN with normal lungs,eg perinatal asphyxia, acidosis

INHALED NITRIC OXIDE ( i NO) IN NEONATES
Indication
Neonates with evidence of persistent pulmonary hypertension of newborn (PPHN) who has persistent severe hypoxaemia (PaO2 <80 mmHg with FiO2 > 80%) after 1 hour of mechanical ventilation (IPPV or HFOV) with appropriate lung recruitment strategies.
Evidence of PPHN Clinical evidence of right-to-left extra-pulmonary shunting
The degree of hypoxaemia cannot be explained by the underlying lung parenchymal disease alone or
Post-ductal oxygen saturation (SpO2) is 5% lower than preductal oxygen saturation (persistently or intermittently) or
Post-ductal arterial oxygen SaO2 is 10mmHg lower than preductal SaO2 Echocardiogram is not mandatory but is useful in confirming the diagnosis and
excluding congenital cyanotic heart disease. Measure pulmonary artery pressure by adding 10mmHg to tricuspid valve
pressure gradient. PA pressure is considered high (PPHN) if ≥ ½ of systemic mean blood pressure or ≥ 50mmHg.
Dilated pulmonary trunk. Ventricular septum pushed to the left.
Precipitating cause is usually present (eg meconium aspiration syndrome, congenital pneumonia, diaphragmatic hernia, hyaline membrane disease).
Initial dose: 20 ppm
Clinical Response Improvement in oxygenation (PaO2) of 20% or more over baseline, usually
within 30-60 min. If no improvement is observed after 6 hours, discontinuing iNO therapy should be
considered as late response is unlikely.
Continuation of iNO TherapyOnce clinical response is achieved, the dosage of iNO is reduced and to be kept at lowest possible dose that prevents the right to left shunt. The method employed should be individualized. The recommendations below are served as general guideline.
Decrease the nitric oxide at 2 ppm decrement every ½ - 1 hour, as long as the PaO2 is 80 to 100 mm Hg and the pulse oximetry reading (SpO2) is more than 94%.
To maintain the iNO at minimal dose (not lower than 5 ppm) which prevents the right to left shunt.
FiO2 is reduced with 5% decrement every 1 hour if PaO2 is persistently >100 mmHg. To avoid confusion, try not to reduce iNO and FiO2 simultaneously since reduction
of either one may be attributed to clinical deterioration.
26

In the process of deceasing the iNO and FiO2, ensure that the PaO2 remains at 80-100 mm Hg and oxygen saturation determined using pulse oximetry is more than 94%.
Weaning off iNOOnce the FiO2 reaches 40-50%, iNO 5 ppm and clinically there is no more right to left shunt, to reduce the iNO further with 1 ppm decrement every ½-1 hour.If rebound effect occurs, to keep iNO at lowest possible level that controls the PPHN.
Duration of therapy Total duration of iNO therapy should not exceed 5 days.
Monitoring Keep NO2 level < 0.5 ppm methaemoglobinaemia
27

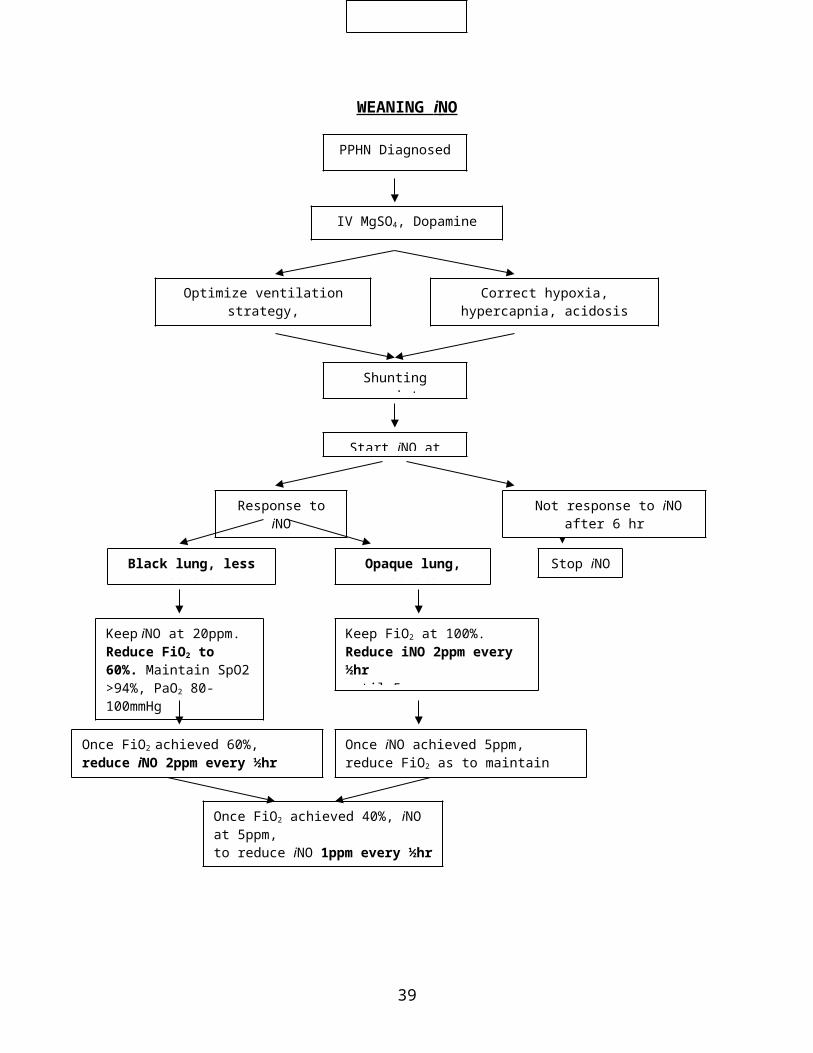
WEANING i NO
28
PPHN Diagnosed
Start iNO at 20ppm
Correct hypoxia, hypercapnia, acidosis
Shunting persists
Optimize ventilation strategy, Conventional or HFOV
IV MgSO4, Dopamine
Opaque lung, severeBlack lung, less severe Stop iNO
Response to iNO
Once FiO2 achieved 60%, reduce iNO 2ppm every ½hr until 5ppm
Keep iNO at 20ppm. Reduce FiO2 to 60%. Maintain SpO2 >94%, PaO2 80-100mmHg
Once FiO2 achieved 40%, iNO at 5ppm, to reduce iNO 1ppm every ½hr
Once iNO achieved 5ppm, reduce FiO2 as to maintain SpO2 > 94%.
Keep FiO2 at 100%.Reduce iNO 2ppm every ½hr until 5ppm
Not response to iNO after 6 hr
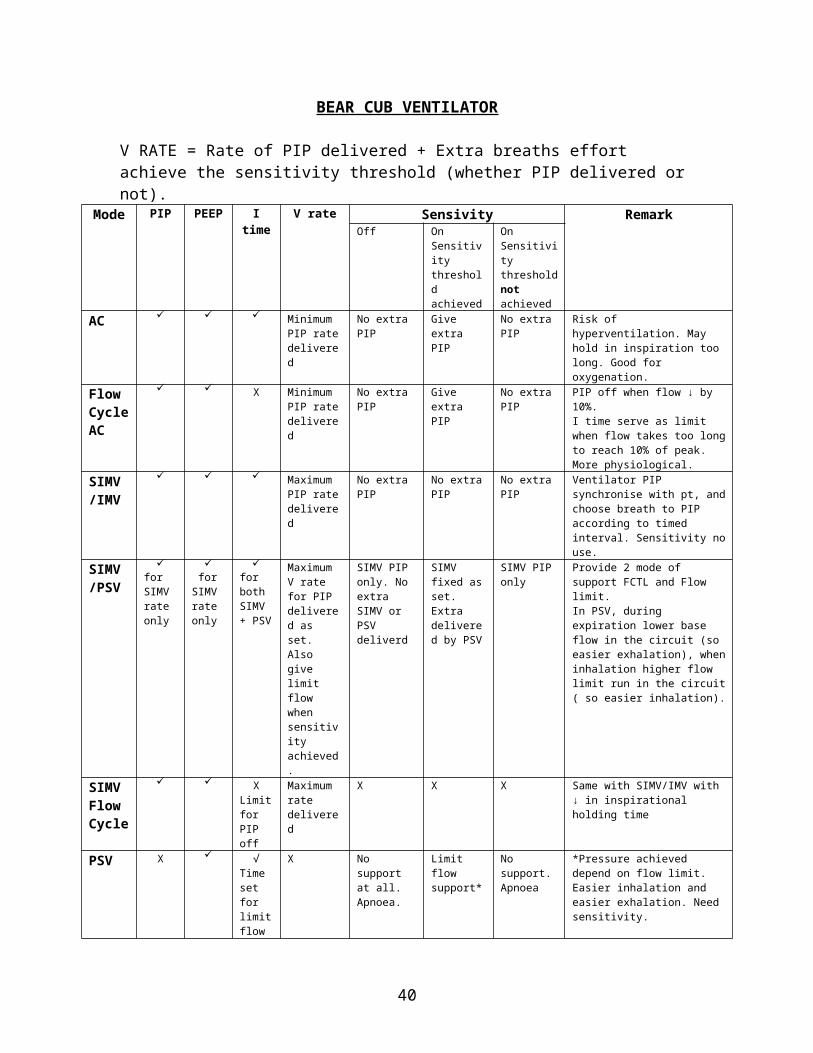
BEAR CUB VENTILATOR
V RATE = Rate of PIP delivered + Extra breaths effort achieve the sensitivity threshold (whether PIP delivered or not).
Mode PIP PEEP I time V rate Sensivity RemarkOff On
Sensitivity threshold achieved
On Sensitivity threshold not achieved
AC Minimum PIP rate delivered
No extra PIP Give extra PIP
No extra PIP Risk of hyperventilation. May hold in inspiration too long. Good for oxygenation.
FlowCycle AC
X Minimum PIP rate delivered
No extra PIP Give extra PIP
No extra PIP PIP off when flow ↓ by 10%.I time serve as limit when flow takes too long to reach 10% of peak.More physiological.
SIMV/IMV
Maximum PIP rate delivered
No extra PIP No extra PIP No extra PIP Ventilator PIP synchronise with pt, and choose breath to PIP according to timed interval. Sensitivity no use.
SIMV/PSV
for SIMV rate only
for SIMV rate only
for both SIMV + PSV
Maximum V rate for PIP delivered as set.Also give limit flow when sensitivity achieved.
SIMV PIP only. No extra SIMV or PSV deliverd
SIMV fixed as set. Extra delivered by PSV
SIMV PIP only
Provide 2 mode of support FCTL and Flow limit.In PSV, during expiration lower base flow in the circuit (so easier exhalation), when inhalation higher flow limit run in the circuit ( so easier inhalation).
SIMV FlowCycle
XLimit for PIP off
Maximum rate delivered
X X X Same with SIMV/IMV with ↓ in inspirational holding time
PSV X √ Time set for limit flow
X No support at all. Apnoea.
Limit flow support*
No support. Apnoea
*Pressure achieved depend on flow limit. Easier inhalation and easier exhalation. Need sensitivity.
CPAP X X X X X X Base flow to maintain PEEP. No change in flow rate both inspiration and expiration.
Suggested weaning mode: Flow cycle AC SIMV/PSV PSV Off
29

MILLENIUM SECHRIST
V rate, RR = PIP rate + extra breaths effort achieve the sensitivity threshold.Pressuregraph - pressure change does not show whether ventilator delivers PIP or extra breath.Mode PIP PEEP I time V rate Sensivity Remark
Off On Sensitivity threshold achieved
On Sensitivity threshold not achieved
AC Minimum PIP rate delivered
No extra PIP
Extra PIP delivered
No extra PIP Risk of hyperventilation. May hold in inspiration too long
SIMV Maximum rate delivered
PIP not synchronize
PIP synchronize
PIP not synchronize
Sensitivity is for synchronization. RR will record extra breath rate if sensitivity is on.Same with SIMV/IMV of BEAR CUB
CPAP backup(sensitivity on)
X. V rate has no function.A backup PIP given if apnoea for duration as set at Alarm Delay
- No extra PIP Ventilator detect apnoea. Give PIP as set by Delay Alarm
RR recorded if achieving sensitivity threshold.
CPAP no backup (sensitivity off)
X X X X. No PIP delivered.
No extra PIP
- - No RR recorded.
30

HIGH FREQUENCY OSCILLATORY VENTILATION (HFOV)
The HFOV generates tidal volume less than or equal to dead space by means of an oscillating piston or diaphragm. This mechanism creates active exhalation and inhalation. Lung recruitment can be achieved with relatively less barotrauma.
IndicationsAs a rescue therapy in the following conditions when conventional mechanical ventilation does not result in adequate oxygenation or ventilation or requires the use of very high airway pressures:
(1) PPHN associated with parenchymal lung diseases(2) Meconium aspiration syndrome(3) Hyaline membrane disease(4) Pneumonia(5) Diaphragmatic hernia(6) Pulmonary interstitial emphysema
Management Strategies(A) Initiation
(1) To calibrate the ventilator following the instruction attached to the machine.(2) Settings.
The user-defined parameters are FiO2, frequency, mean airway pressure (Paw), and amplitude.
As a general rule, the bias flow rate is set at 20 L/min, and inspiratory % time at 33% (I:E ratio=1:2).
(a) FiO2 is started on 100% and wean as tolerated.
(b) Paw controls oxygenation of the patient. Start at 2 cmH2O higher than MAP on conventional ventilator (at least 10-12
cmH2O). If over-distention or air leak (PIE, pneumothorax) were present prior to initiation of HFOV, a lower Paw should be considered.
If patient desaturates, increase 1-2 cmH2O increments every 5 minutes until optimal lung volume and SaO2 are reached.
Optimal lung volume is reached once there is good chest expansion on CXR (right diaphragm at the 8- 9th rib level posteriorly).
Over expansion (hyperinflation on chest X-ray) may lead to a paradoxical decrease in SaO2 and low blood pressure (compromised venous return).
31

(c) Frequency affects mainly the ventilation of the patient. The smaller the Hz number, the larger the tidal volume for a given amplitude.
The initial frequency setting is based on baby’s weight (table below) and disease process.
Body weight FrequencyNeonates < 1000 gms 15 Hz
1000 – 2000 gms 12 Hz2.0 – 10 kg 10 Hz
Children 11 – 20 kg 8 Hz21 – 30 kg 7 Hz
> 30 kg 6 Hz
For baby with significant component of increased airway resistance (e.g. meconuim aspiration), lower frequency (6-8 Hz) is required.
*Some protocol recommends an initial frequency of 3-6 Hz for meconium aspiration syndrome.
(d) Amplitude (Delta P, ∆P) affects tidal volume delivered to patient. It is set at the level where there is adequate chest wiggle, which should extend to the level of umbilicus. To start at 20-30 cmH2O and adjust accordingly. Generally, smaller baby requires lower amplitude.
(B) Continual ManagementAfter HFOV has been initiated, careful and frequent assessment of lung expansion and adequate gas exchange are necessary.
(1) Air trapping is a continuous potential threat. Signs of over-distention, such as descended / flat diaphragms and small heart shadow, are monitored with frequent chest X-ray.
Obtain 1 hour after initiation and every 6-12 hours after that for the first 48 hours, and whenever clinically indicated.
(2) Gas exchange.
Assess ABG ½ hourly until both oxygenation (PaO2) and ventilation (PCO2) are optimized, than 2 -6 hourly subsequently.
If PaO2 is low on FiO2 100%, an increase in Paw may be necessary. CXR is helpful in determining the adequacy of lung expansion.
If PaCO2 is high:(i) If oxygenation is poor, the Paw may be too high or too low, result in either hyperinflation or widespread collapse, respectively. Again, CXRs are necessary to differentiate between the two conditions.
32

(ii) If oxygenation is adequate, the amplitude should be increased (change in 2-4 cmH2O FiO2 increments). (iii) Reduce the frequency will allow better tidal volume, hence reduce the PaCO2.
Summary of adjustments of HFOV settings:Low PaO2 High PaCO2
↑FiO2↑Paw
↑Amplitude↓Frequency
High PaO2 Low PaCO2↓FiO2↓Paw
↓Amplitude↑Frequency
(C) Weaning
In the absence of hyperinflation, FiO2 is weaned prior to Paw for adequate PaO2. When FiO2 below 40%, wean Paw exclusively. Aim to achieve Paw of 10-12 cmH2O. Paw of 8 cmH2O is essentially CPAP.
Paw should be weaned as the lung disease improves with the goal of maintaining optimal lung expansion. Excessively aggressive early weaning of Paw may result in widespread atelectasis and the need for significant increases in FiO2.
Amplitude should be weaned for acceptable PaCO2.
Frequency is usually not adjusted during weaning. A decrease in frequency is necessary when signs of lung over-distention cannot be eliminated by a reduction in Paw.
The neonate may be switched to conventional ventilation at a low level of support or may be extubated directly from an HFOV.
(D) Precautions
Adequate blood pressure is crucial or patient will not oxygenate. May need bolus volume, increase IV maintenance fluid rate or inotropes.
Patients should be well sedated. To paralyse patient only in exceptional case.
Avoid interrupting ventilation with unnecessary ETT suctioning.
33

MAGNESIUM SULPHATE INFUSION
Indication: PPHN
Loading dose: 200mg/kg Or 0.4ml/kg of MgSO4 50% Or 2.0ml/kg of MgSO4 10% Dilute into 10% concentration ie 1:5 Dilute with D 5% or D 10% Intravenous slow bolus over 20-30 minutes.
Maintenance: 20-50mg/kg/hr MgSO4 50% diluted into 10% (same concentration with loading) In a 50ml syring, add 10ml of MgSO4 50% into 40ml D5% = MgSO4 10% To run between 0.2ml/kg/hr (20mg/kg/hr) and 0.5ml/kg/hr (50mg/kg/hr)
Monitor: serum magnesium level: 3.5-5.0 mmol/L
SINGLE PREPARATION: Dilute 10ml of IV MgSO4 50% with 40ml of D10%.Loading: 200mg/kg = 2ml/kg to run over 20-30 min.Maintenance: 20-50mg/kg/hr = to run 0.2-0.5ml/kg/hr.
34
PDA CLOSURE WITH INDOMETHACIN AND IBUPROFEN
NSAIDS SELECTIONChoosing either indomethacin or ibuprofen is based on serum creatinine level. Both are contraindicated if renal impairment (serum creatinine >120umol/L), necrotising enterocolitis and thrombocytopenia (platelet < 100 x 106/uL). Indomethacin is chosen if serum creatinine <80umol/L or ibuprofen if serum creatinine 80-120umol/L.
INDOMETHACINOne vial of indomethacin contains1mg in 1ml. Concentration is 1mg/ml. Dilute it to 0.1mg/ml by adding 9ml of water for injection into the 1mg (or 1ml) of indomethacin. Dosage in mg/kg: daily dose
3rd day2nd day1st dayAge at the 1st dose0.10.10.2< 48 hours of life0.20.20.2*2nd -7th day of life0.250.250.2>7 day of life
Complications: renal impairment, upper GI bleed, NECMonitor: Hb, plt, urea, creatinine, urine specific gravity, urine output
IBUPROFENIndication: PDA in premature baby <34th corrected age after failed indomethacin therapy or has renal impairment (with serum creatinine of 80-120umol/L).Dosage in mg/kg: daily dose
3rd day2nd day1st day5510Dosage
Fail NSAIDs, step up anti-failure therapy and kiv for coil interventional or operative closure.
35
PDA diagnosed clinically or by ECHO
<5 days old
Start IV frusemide if signs of heart failure present
Start NSAIDs
*the usual dose
>5 days old
Fluid restriction Fluid restriction + NSAIDs
Failure of PDA closure after 5 days oldPDA closure
Failure of PDA closure or reopening after 3 days of NSAID
To continue NSAID for 5 days
PDA closure PDA closure
NSAID x 3 days NSAID x 3 days

SUPRAVENTRICULAR TACHYCARDIA
(1) Attempt vagal manoeuvre, ie carotid massage ± apply abdominal pressure gently with the hand.
(2) Illicit “diving reflex”, ie place a pack of ice to the face. Alternatively, wrap the baby up firmly and place the face in a bowl of iced water for a couple of seconds.
(3) Adenosine: stat dose of 0.1mg/kg undiluted adenosine, rapid IV push with saline. Increased dose by 0.05mg/kg every 2 min to maximum of 0.35mg/kg.(4) If baby is in heart failure, to attempt electrical conversion with 1 joule/kg(5) Flecainide: use 2mg/kg stat, slowly over at least 10 min. If there is any widening of the QRS complex during the infusion stop immediately.(6) Amiodarone: use 350mg/m2 loading dose orally once a day and load for 10 days.
Then give 200mg/m2 as oral maintenance (preferred) or IV 5mg/kg.
An ECG during these procedures, particularly to capture the beats at conversion back to sinus rhytm can be diagnostic of an aberrant pathway and should always be attempted.
36
AMINOPHILLINE PROPHYLAXIS FOR APNOEA OF PREMATURE
37

MANAGEMENT OF HYPERKALEMIA
Hyperkalemia – Ensure the blood is not lysed, withhold KCl in IVD or oral KCl
K+>5.6K+>6 in nepnates
Salbutamol neb 0.5ml x 2 apart
K+>6.5K+>7.0 in neonates or ECG shows arrhythmia
Ca gluconate 0.5ml/kgNaHCO3 4.2 % 2ml/kgSalbutamol neb 0.5ml x 2Rectal resonium 1g/kg 6Hly
Repeat K+ level½ hour after 2nd neb
K+<5.6 5.6<K+<6.5 K+>6.5
(1) Salbutamol neb 0.5ml x 2(2) Rectal resonium 1g/kg 6Hly
Stop Tx (1) Ca gluconate 0.5ml/kg(2) NaHCO3 4.2% 2ml/kg(3) Salbutamol neb 0.5ml x 2(4) Dextrose 10% 0.5g/kg or 5ml/kg(5) Insulin IV bolus 0.1u/kg
Repeat serum K+ level ½ hour after 2nd neb
K+<5.6 5.6<K+<6.5 K+>6.5
Stop Tx (1) IVI salbutamol 30-50ug/kg/hr(2) Continue rectal resonium
Peritoneal dialysis
K+<5.6 5.6<K+<6.5 K+>6.5
Repeat serum K+ level
38
Stop Tx Continue IVI salbutamol till K+ 5.6, 4Hly K+ Peritoneal dialysis
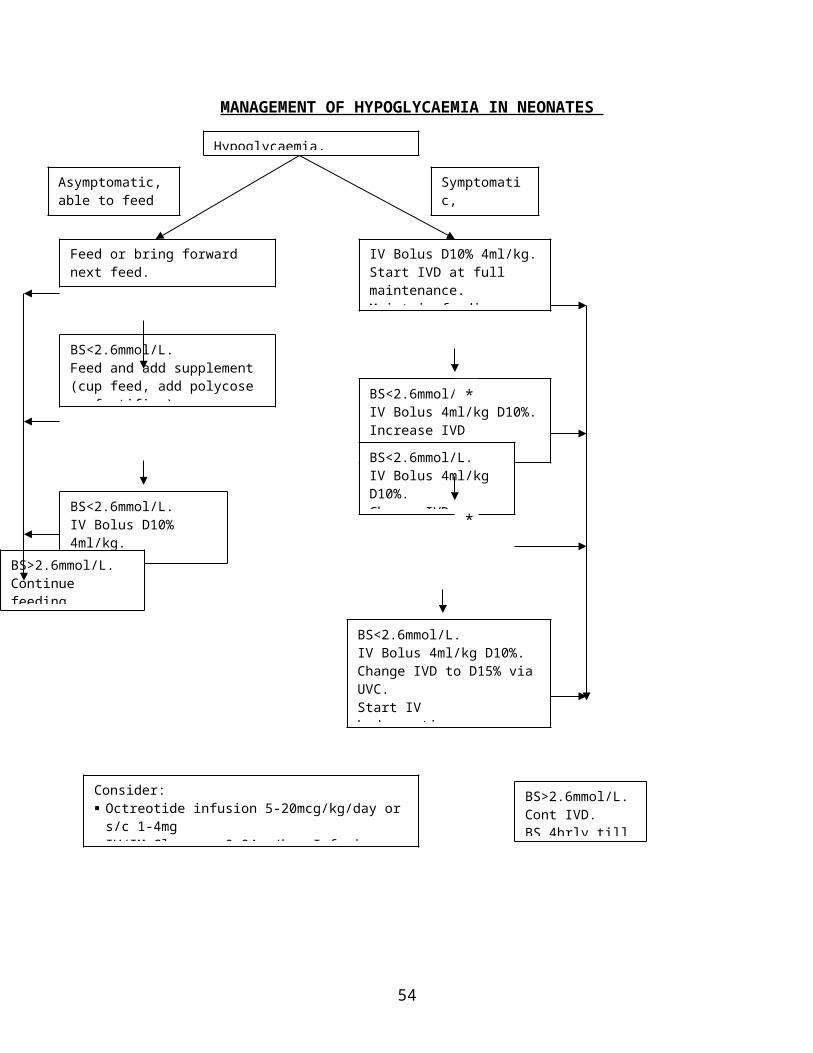
MANAGEMENT OF HYPOGLYCAEMIA IN NEONATES
Infusion rate of glucose is 4-6mg/kg/min and can be increased up to 15-20mg/kg/min.Breast feeding should be encouraged where possible.Milk formula provides more energy/ml than D10%.Milk feed must not be discontinued or reduced when on IVD unless NEC is suspected.*For term baby. In premature baby or baby required fluid restriction, may increase concentration of glucose before volume increment.
39
Hypoglycaemia, BS<2.6mmol/L
Asymptomatic, able to feed
Symptomatic,persistent
Feed or bring forward next feed. Rpt BS in 30min.
IV Bolus D10% 4ml/kg. Start IVD at full maintenance. Maintain feeding. Rpt BS in 30min.
BS<2.6mmol/L.Feed and add supplement(cup feed, add polycose or fortifier)Rpt BS in 30min.
BS<2.6mmol/L.IV Bolus D10% 4ml/kg. Start IVD.
BS<2.6mmol/LIV Bolus 4ml/kg D10%.Increase IVDto the next day's requirement. Rpt BS in 30 min.
BS<2.6mmol/L.IV Bolus 4ml/kg D10%.Change IVD to D12.5%.Rpt BS in 30min.
BS<2.6mmol/L.IV Bolus 4ml/kg D10%.Change IVD to D15% via UVC.Start IV hydrocortisone (2-4mg/kg/dose QID) if glucose requirement > 20mg/kg/min.
Consider: Octreotide infusion 5-20mcg/kg/day or s/c 1-4mg IV/IM Glucagon 0.04mg/kg. Infusion: 10-50mcg/kg/hr Ix for sepsis, hyperinsulinism and metabolic diseases.
BS>2.6mmol/L. Continue feeding. BS 4hrly till stable.
BS>2.6mmol/L.Cont IVD.BS 4hrly till stable.
*
*
For cases with persistent hypoglycaemia, investigations to be taken during hypoglycaemia.
Blood UrineRandom glucoseLactate/pyruvateKetone bodiesFFAAminoacidsInsulin/C-peptideCortisol/growth hormone
KetonesReducing substanceOrganic acids
Hyperinsulinism state can occur in infant of diabetic mother or persistent hyperinsulinism of infancy.Diagnostic criteria for hyperinsulinism are:Glucose requirement >6-8mg/kg/min to maintain BS above 3mmol/LRandom BS <2.6mmol/L.Detectable insulin with raised C-peptide when hypoglycaemia.Low blood FFA and ketone body when hypoglycaemia.Glycaemic response after the administration of glucagons when hypoglycaemia.Absence of ketonuria.
40

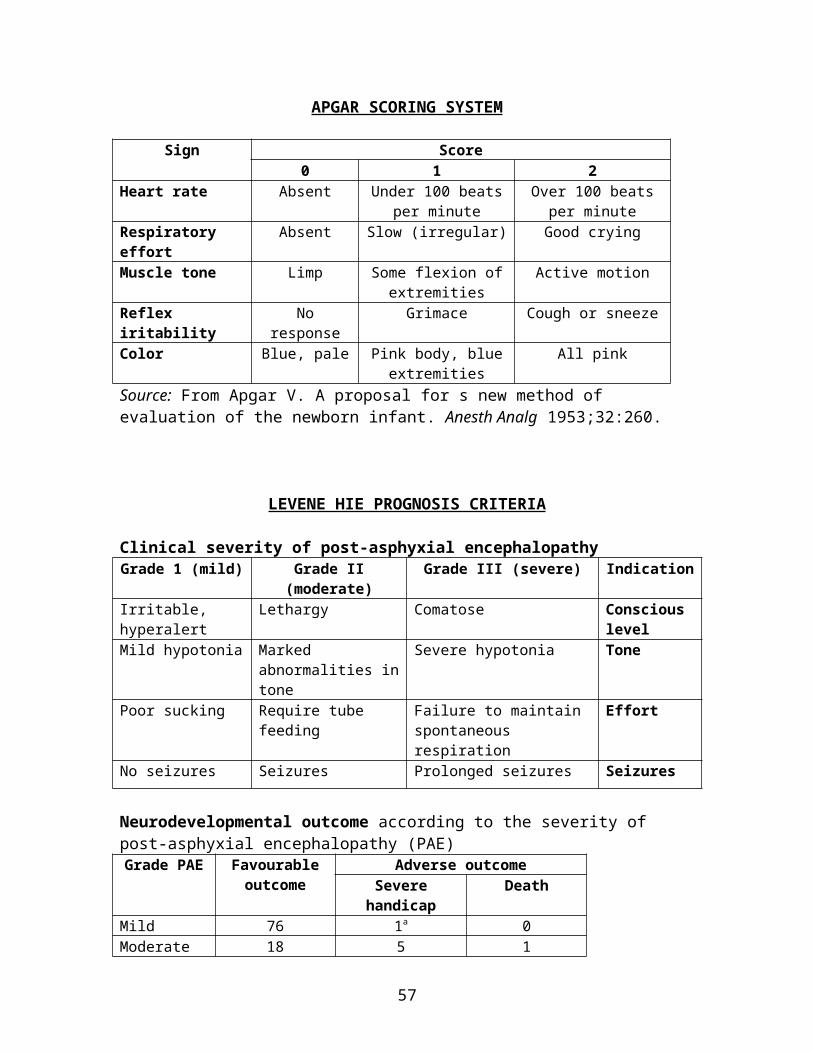
APGAR SCORING SYSTEM
Sign Score0 1 2
Heart rate Absent Under 100 beats per minute
Over 100 beats per minute
Respiratory effort Absent Slow (irregular) Good cryingMuscle tone Limp Some flexion of
extremitiesActive motion
Reflex iritability No response Grimace Cough or sneezeColor Blue, pale Pink body, blue
extremitiesAll pink
Source: From Apgar V. A proposal for s new method of evaluation of the newborn infant. Anesth Analg 1953;32:260.
LEVENE HIE PROGNOSIS CRITERIA
Clinical severity of post-asphyxial encephalopathyGrade 1 (mild) Grade II (moderate) Grade III (severe) Indication
Irritable, hyperalert Lethargy Comatose Conscious level
Mild hypotonia Marked abnormalities in tone
Severe hypotonia Tone
Poor sucking Require tube feeding Failure to maintain spontaneous respiration
Effort
No seizures Seizures Prolonged seizures Seizures
Neurodevelopmental outcome according to the severity of post-asphyxial encephalopathy (PAE)
Grade PAE Favourable outcome
Adverse outcomeSevere handicap Death
Mild 76 1a 0Moderate 18 5 1Severe 5 3 13a An infant with weakness due to congenital myopathy.Source: Levene et al., 1986
41

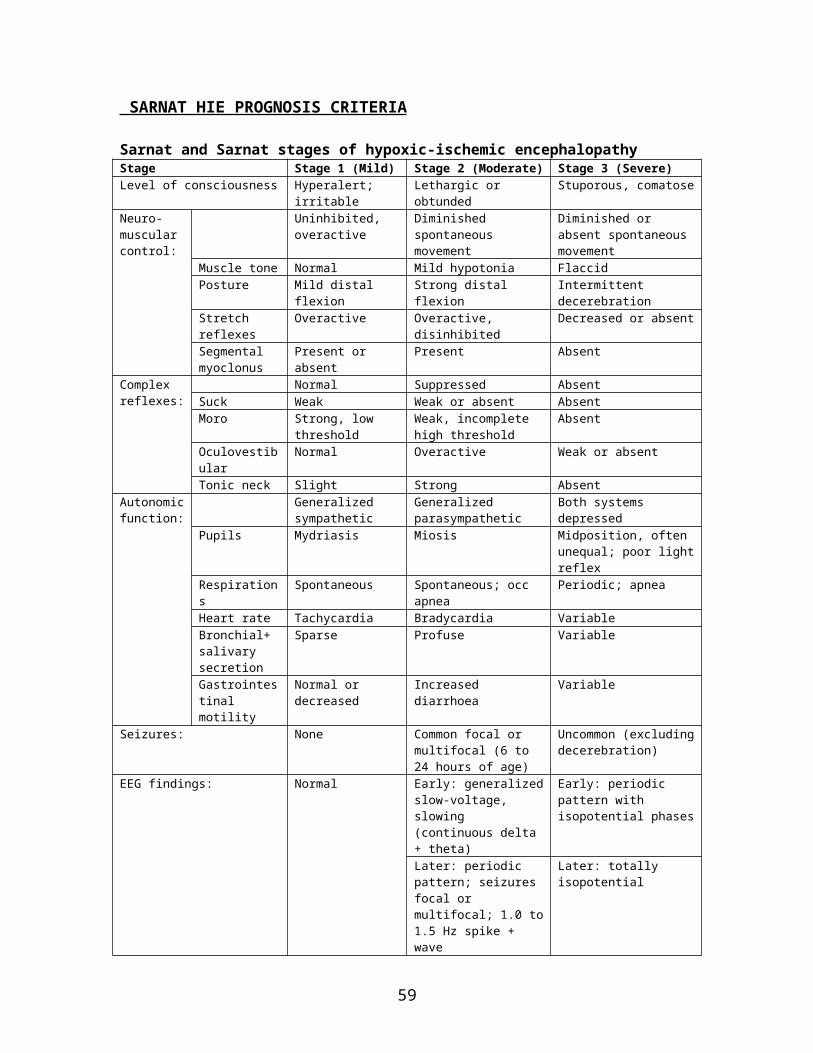
SARNAT HIE PROGNOSIS CRITERIA
Sarnat and Sarnat stages of hypoxic-ischemic encephalopathyStage Stage 1 (Mild) Stage 2 (Moderate) Stage 3 (Severe)Level of consciousness Hyperalert; irritable Lethargic or obtunded Stuporous, comatoseNeuro-muscular control:
Uninhibited, overactive
Diminished spontaneous movement
Diminished or absent spontaneous movement
Muscle tone Normal Mild hypotonia FlaccidPosture Mild distal flexion Strong distal flexion Intermittent decerebrationStretch reflexes Overactive Overactive, disinhibited Decreased or absentSegmental myoclonus
Present or absent Present Absent
Complex reflexes:
Normal Suppressed AbsentSuck Weak Weak or absent AbsentMoro Strong, low threshold Weak, incomplete high
thresholdAbsent
Oculovestibular Normal Overactive Weak or absentTonic neck Slight Strong Absent
Autonomic function:
Generalized sympathetic
Generalized parasympathetic
Both systems depressed
Pupils Mydriasis Miosis Midposition, often unequal; poor light reflex
Respirations Spontaneous Spontaneous; occ apnea Periodic; apneaHeart rate Tachycardia Bradycardia VariableBronchial+salivary secretion
Sparse Profuse Variable
Gastrointestinal motility
Normal or decreased Increased diarrhoea Variable
Seizures: None Common focal or multifocal (6 to 24 hours of age)
Uncommon (excluding decerebration)
EEG findings: Normal Early: generalized slow-voltage, slowing (continuous delta + theta)
Early: periodic pattern with isopotential phases
Later: periodic pattern; seizures focal or multifocal; 1.0 to 1.5 Hz spike + wave
Later: totally isopotential
Duration of symptoms: <24 hours 2 to 14 days Hours to weeksOutcome: About 100% normal 80% normal; abnormal if
symptoms more than 5 to 7 days
About 50% die; remainder with severe sequelae
Sarnat H.B., Sarnat M.S. Neonatal encephalopathy following fetal distress: A clinical and electroencephalographic study. Arch Neurol 1976;33:696.Summary of Sarnat HIE prognosis criteria
Factor Stage I Stage II Stage IIILevel of consciousness Alert Lethargy ComaMuscle tone Normal Hypoyonia FlaccidityTendon reflexes Normal/increased Increased Depressed/absentMyoclonus Present Present AbsentComplex reflexes
Sucking Active Weak AbsentMoro Exaggerated Incomplete AbsentGrasping Normal/exaggerated Exaggerated absent
Oculocephalic (doll’s eye) Normal Overreactive Reduced/absent
Seizure None Common focal or multifocal
Uncommon
42

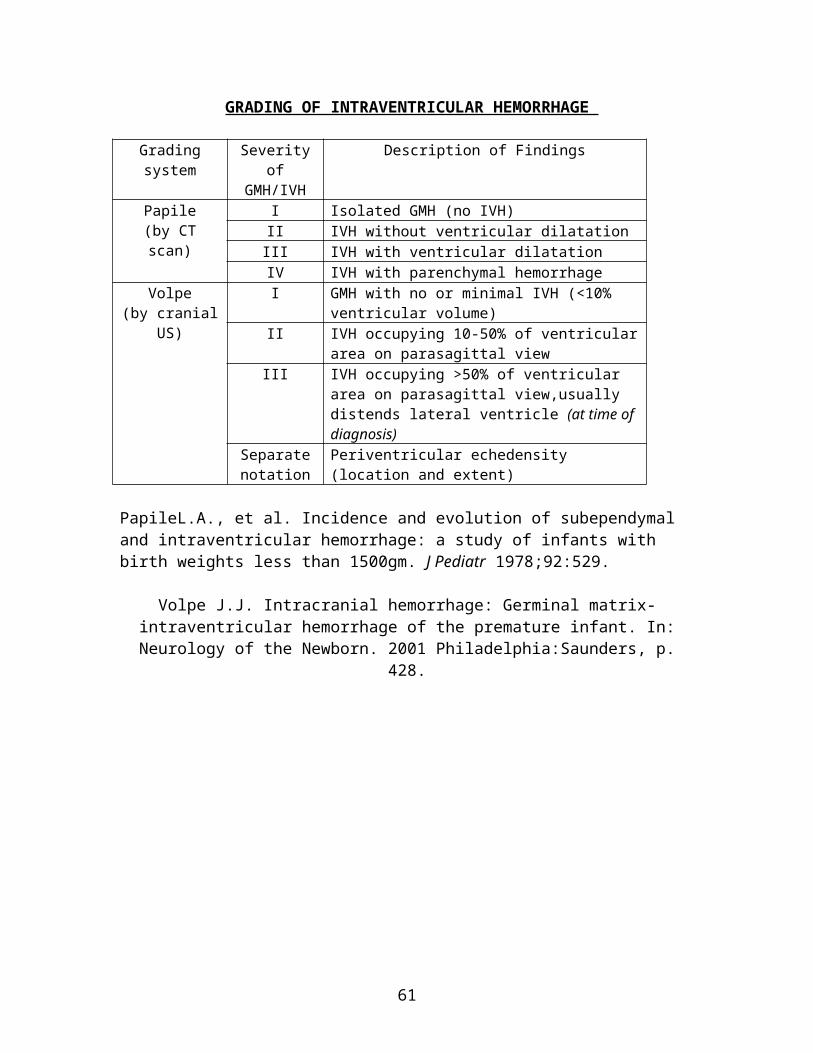
GRADING OF INTRAVENTRICULAR HEMORRHAGE
Grading system Severity of GMH/IVH
Description of Findings
Papile (by CT scan)
I Isolated GMH (no IVH)II IVH without ventricular dilatationIII IVH with ventricular dilatationIV IVH with parenchymal hemorrhage
Volpe (by cranial US)
I GMH with no or minimal IVH (<10% ventricular volume)
II IVH occupying 10-50% of ventricular area on parasagittal view
III IVH occupying >50% of ventricular area on parasagittal view,usually distends lateral ventricle (at time of diagnosis)
Separate notation
Periventricular echedensity (location and extent)
PapileL.A., et al. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1500gm. J Pediatr 1978;92:529.
Volpe J.J. Intracranial hemorrhage: Germinal matrix-intraventricular hemorrhage of the premature infant. In: Neurology of the Newborn. 2001 Philadelphia:Saunders, p. 428.
43

STAGING OF NECROTIZING ENTEROCOLITIS
Defination: Necrotizing enterocolitis is an acquired neonatal disorder representing an end expression of serious intestinal injury following a combination of vascular, mucosal, and toxic insults to a relatively immature gut.
Staging
Stage Systemic Intestinal RadiographicStage I:Suspected
Nonspecific, apnea, bradycardia, lethargy, temperature instability
Gastric residual Normal
Stage IIA:Mild NEC
Signs similar to Stage I Abdominal distention, absent bowel sound, gross blood in stool
Ileus, dilated loops with focal areas of pneumatosis intestinalis
Stage IIB:Moderate NEC
Mild acidosis and thrombocytopenia
Abdominal wall edema and tenderness
Extensive pneumatosis, early ascites, intrahepatic portal venous gas
Stage IIIA:Advanced NEC
Respiratory and metabolic acidosis, assisted ventilation for apnea, hypotension, reduced PU, neutropenia, DIVC
Spreading edema, erythema, induration of abdomen
Prominent ascites, persistent sentinel loop, no perforation
Stage IIIB:Advanced
Deteriorating vital signs, shock, electrolyte imbalance
Evidence of perforation
Clinical diagnosis: Triad of feed intolerance, abdominal distention and bloody stools.
Bell’s Criteria
Stage Clinical featuresStage 1 - Suspect History of perinatal stress, systemic signs of ill health ie
temperature instability, lethargy, apnoea, GIT manifestations ie poor feeding, increased volume of gastric aspirate, vomiting, mild abdominal distension, fecal occult blood with no anal fissure
Stage 2 - Confirmed Any of features of stage 1 plus persistent occult, or gastrointestinal bleeding, marked abdominal distension, abdominal radiograph; intestinal distension, bowel wall oedema, unchanged bowel loops, pneumatosis intestinalis, portal vein gas
Stage 3 - Advanced Any of features of stages 1 or 2 plus: deterioration in vital signs, evidence of shock or severe sepsis, or marked gastrointestinal hemorrhage, or abdominal radiograph shows any of features of stage 2 plus pneumoperitonium
44

PROGNOSIS SCORING FOR NEONATAL TETANUS
Score 0 1 2 3 Indication
Age of symptom onset in days
1-4 5-8 9-12 >12 Incubation period
Interval between onset of symptom and spasm (hours)
<24 24-48 >48 No spontaneous
spasm
Severity of spasm
Duration of spasm (minutes)
Persistent/ prolonged
>2 <2 Transient on stimulation
Severity of spasm
Temperature variation from normal (oC)
>3 2 to 3 1 to 2 Normal or ±1
Autonomic involvement
Pneumonia and/or atelectasis
Definite widespread
Definite limited
Suspected or mild
Nil Complication
Score Prognosis0 Recovery improbable15 Recovery expected
Assessment should be done 24 hourly. If the score is unchanged or lower at subsequent assessments signifies ineffective management or complications.
45

VENTRICULAR TAP
Indications: (1) Ventriculitis(2) Administration of intraventricular antibiotics(3) Emergencyrelief of raised intracerebral pressure in non-communicating hydrocephalus(4) Management of progressive non-communicating hydrocephalus when the baby's
condition precludes as immediate ventricular shunt procedure.
Procedure:(1) Shave the anterior part of the head wall behind the posterior angle of the anterior fontanelle (AF).(2) Wrap the baby well and to avoid movement as assistant must hold the head firmly with the baby supine.(3) Identify the coronal suture and the lateral angle of the anterior fontanelle.(4) Insert the needle* through the lateral angle of the AF. Advance slowly in the direction of the inner canthus of the eye on the ipsilateral side.(5) The lateral ventricle is usually entered 2-4cm from the surface, sooner if the ventricles are dilated. The CSF will fill the needle.(6) Collect the CSF by allowing it to drip from the needle.(7) Remove needle, seal the puncture site with plastic aerosol dressing and cover with small adhesive tape (or cover with flavin dressing). Keep baby supine for approximately 15 min after procedure.*Usually use a butterfly needle 23 gauge.
Precautions:(1) Once into the brain tissue, do not change the direction of the insertion of the needle as this cause unnecessary damage.(2) After 2 unsuccesful attemps inserting the needle to a depth of 4.5cm, do not persist with the procedure.(3) In the presence of cerebral oedema and slit-like ventricles, it is doubtful if any attempt is justified.(4) Limit total volume of CSF removed at each tapping to no more than 30mls. (The initial puncture should not exceed 10ml in volume and can be increased as sequential taps at a rate of not more than 5ml/day).
Reference: Textbook of Neonatology, NRC Roberton, page 1186.
46

APT TEST
Apt test is to differentiate maternal blood from fetal blood.
Methods: (1) Mix equal parts of bloody SAMPLE (from baby’s vomitus or BO) with water and centrifuge it. (2) Add 1 part of 0.25 molar sodium hydroxide to parts of pink supernatant.
Results: If the fluid remain pink – blood is fetal in origin. If the colour changes pink to yellow brown – it is mother’s blood.
Fetal blood has high level of HbF which is resistant to hydrolysis by NaOH compared to maternal blood which high in HbA2.
47

CENTRAL VENOUS LINESNURSING CARE & MAINTENANCE
Indications of a central line1. Prolonged central venous access is necessary in the very low birth weight infant to facilitate adequate nutrition prior to the establishment of full enteral feeds. 2. To enable the safe and uninterrupted administration of clinically essential or locally toxic solutions (eg inotropes or concentrated dextrose solution).
Types of CV lines Umbilical venous catheters (UVC) Peripherally inserted central catheters (PICC) Central lines inserted over a guide wire at puncture of a large superficial vein Surgically inserted central lines.
48

Catheter placement Zone A (low SVC/upper right atrium). This is a suitable tip site from any access
point in the upper body. Catheter tips can be sited safely within the upper right atrium provided they do not abut the atrial wall end-on or pass through the tricuspid valve or into the coronary sinus.
Zone B (upper SVC). Suitable site for tips of catheters placed via the right internal jugular route.
Zone C (mid-point, left innominate vein). This is a suitable site for the tip when the catheter is introduced from the left internal jugular or subclavian vein, and reduces the risk of SVC perforation.
Post-insertion Following catheter insertion, placement must be confirmed by a chest x-ray. This
should be done stat as a central catheter will occlude if no heparin is injected, or an IV is not infusing to maintain patency.
The infant should be left clean and dry, check temperature There is no need to immobilize the arm PICC catheter - a phlebitis may occur immediately following insertion and may last
for 48 hours post-insertion. This usually resolves on its own within 48 hours and may be alleviated by application of warm compresses intermittently to the upper arm. Look out for any elevation of temperature, redness around the insertion site or purulent drainage.
Document in case notes type, size, and location of central catheter placed. Insertion site to be observed 1 hrly for:
• signs of superior vena cava obstruction (neck / arm swelling)
49

• extravasation • bleeding • signs of infection • leaking of infusate • security of catheter and occlusive dressing – hub must be adequately secured
Ensure lumens are either heparinized or run IV to keep the vein open until placement is confirmed by x-ray.
For a PICC catheter – sterile gauze dressing should be applied over the insertion site and PICC line well secured following insertion. A small amount of sanguineous ooze is expected within the first 24 hours post-insertion. Reinforce with gauze if necessary. The gauze dressing is replaced with a transparent dressing 24hr post-insertion.
Precautions No blood pressure assessment Do not attempt venipuncture No scissors or sharp instruments near or on the tubing or catheter of a central venous
access device except for suture removal Do not attempt blood sampling from a 3.0 Fr PICC or smaller Do not use acetone or adhesive removers as these may cause damage to the catheter
material Do not use a syringe size smaller than 10 ml volume (smaller syringes exert
excessive pressure on the central venous access device) Blood or blood products should not be routinely infused through these small lumens. The Premicaths should not have blood, blood products or lipid infusions. The catheter hub (the external female end of the catheter to which infusion tubing
connects) plays a major role as a source for catheter related sepsis especially in long term catheter use
Rupture of catheters under high pressure is a potential serious problem. The Vygon corporation states their neonatal catheter:
• has a continuous working pressure limit of 14.5 psi (750 mmHg) • has a bolus pressure limit of 17.4 psi (900 mmHg) • may rupture between 58 – 72 psi (3000-3700 mmHg) but:• 1ml tuberculin syringes will generate 150 psi (7800 mmHg) • 3ml syringe will generate 120 psi (6200mmHg) • 5ml syringe will generate 90 psi (4608 mmHg) therefore:• 1 ml and 3ml syringes should not be used under any circumstances • retrograde infusions are preferable when administering medications
MaintenanceNon-tunnelled central catheter, including a PICC line must be flushed q. 24 hours or after each intermittent use, if there is not a continuous IV maintaining the patency of each lumen.
50
Prophylactic heparin in central venous catheters reduces the incidence of catheter occlusion thus increasing usable life span of the catheter.
PICCs may not be heparin locked – continuous infusion of at least 0.5ml/hour needed to maintain patency.
Plan line changes and administration of medications to reduce the number of line violations.
Prepare IV solutions using sterile technique – sterile drape & gloves and the assistance of a second nurse.
Prior to breaking the line swab the connection with alcohol chlorhexidine 0.5% and leave until dry.
Replace all infusions given through PICC every 24 hours. Do not use 1ml or 3 ml syringe. Use peripheral lines in infants > 27 weeks gestation
Dressing change Wash hands. Assemble necessary equipment. For a PICC line, position patient’s arm extended
away from his/her body at a 45°- 90° angle so that insertion site is below level of the heart.
Put on mask. Open sterile towel. Open sterile supplies onto sterile field. All neonatal lines to be dressed by 2 staff nurses Don clean gloves and remove old dressing. Working from the edges to the insertion
site carefully remove the dressing in direction towards the centre careful not to cause catheter movement.
NOTE and document: how many cms of catheter are external to the skin at each dressing change. If the catheter has migrated in or out by 2 cm notify the doctor. Remove soiled gloves. ( Ensure all lumens are clamped.)
Cleanse the insertion site with appropriate solution. Cleanse in a circular fashion starting at the insertion site working outward from the site. Contact time with the cleansing solution should be 30 seconds. Allow area to dry before placing transparent dressing.
Apply Tegaderm IV transparent dressing. It is not necessary to secure the edges of the dressing with additional tape.
Routine dressing changes are contra indicated due to risk of contamination and accidental catheter dislodgment. Dressings should be changed only when:
the dressing lifts the catheter is inadequately secured or kinked the site requires closer observation due to inflammation, oedema or
leaking of infusion Requires 2 registered nurses with suitable instruction in the technique. It is a sterile
procedure and the area is to be cleaned with povodine-iodine & aqueous chlorhexidine prior to reapplication of dressing. Document management.
The goal of nursing care is to minimise the number of connections and line violations
51

Removal Wash hands. Put on clean gloves; remove dressing securing the PICC line while stabilizing the
catheter hub with one hand. Without dislodging the catheter, use your other hand to gently remove the dressing.
Cleanse site and any sutures with appropriate solution. Allow to dry. Do not apply pressure over the insertion site during catheter removal. Gently remove
the PICC; pull in short increments. After each increment is removed, begin pulling again near the insertion site. Remove 2 –3 cm at a time until the full length of catheter has been removed. The removal process should take 30sec. - 1 minute.
If resistance is felt stop and place a sterile dressing over the site. Apply a warm blanket or warm compress to the upper arm and attempt removal again in 15 – 20 minutes. Resistance may be due to
vasospasm. If resistance is felt on second attempt of removal stop, redress the catheter and inform doctor.
Once the catheter has been successfully removed, apply manual pressure to the site for 2 -3 minutes with gauze. There should be no oozing at the site. Hemostasis should be achieved.
Apply a sterile gauze dressing to the site and secure well. Dressing to remain in place for 24 hours following removal.
NOTE: If a portion of the catheter breaks during removal, immediately apply a tourniquet to the upper arm, close to the axilla, to prevent advancement of the catheter piece into the right atrium. Then check the patient’s radial pulse. If you don’t detect a radial pulse, the tourniquet is too tight. Do not leave patient with tourniquet in place unattended. Vital signs and pulses should be checked q. 5 minutes while tourniquet is in place.
Measure and inspect the PICC catheter. If any part has broken off during removal, place a tourniquet on affected arm immediately, monitor patient for signs of distress. The insertion length should be documented on the patient’s case note. Measure the length and compare to documented insertion length.
If there is a discrepancy in length notify doctor. Catheter should be removed as soon as its use is no longer clinically indicated.
Other indications for catheter removal include: 1. bacteremia and/or clinical symptoms persisting beyond 48-72 hrs despite appropriate IV antibiotic therapy through the catheter 2. progressive insertion site infection especially pseudomonas septicaemia or fungaemia 3. clinically unstable condition of infant and/or development of hypotension due to sepsis 4. evidence of septic emboli or endocarditis
Risks Direct tissue injury Intravascular thrombosis Embolism
52

Risks of parenteral nutrition Line related sepsis Delayed effusion PCE with tamponade
53
CRITERIA FOR ANTIBIOTIC THERAPYFOR NEONATE AT RISK OF SEPSIS
RISKS OF SEPSISAll neonates with the following risk factors for sepsis should be reviewed:(1) Prolonged rupture of membranes >24 hours(2) Maternal chorioamnionitis
(a) obstetrician-defined criteria or,(b) foul-smelling liquor
(3) Maternal urinary tract infection (a) urine microscopic examination with WBC >10 per hpf or, (b) urine microscopic examination showing bacteriuria >3+ or, (c) significant positive urine cultures(4) Maternal fever
(a) fever >38°C (excluding intrapartum),(b) all episodes of intrapartum fever
CRITERIA FOR ANTIBIOTIC THERAPY for neonates at risk for sepsisAntibiotic therapy is commenced for:(1) Premature baby with one or more risk of sepsis.(2) Term baby who have two or more points as listed below:
Risks ScoreProlonged rupture of membranes >24 hours 1 point
Maternal chorioamnionitis 2 points
Maternal urinary tract infection 1 point
Maternal fever 1 point
(3) Therapy also started for those with one point (as listed above) if associated with one of the below: (a) Abnormal total white cell count (<5,000/L, >25,000/L) (b)C-reactive protein levels >1.0 ng/dL (c) Immature to total white cell ratio (I:T ratio) >0.2
(4) As for those who are started on antibiotic the antibiotic may be discontinued if blood culture is negative. (5) Neonate who did not fulfil the above criteria and the score are < 2 points, no therapy is started. Blood must be taken for FBC and culture and the baby will be observed for 24 hours without antibiotic therapy. Child may then be discharged after the observation period if there is no clinical evidence of sepsis.
54

ANTIBIOTIC GUIDE FOR NEONATES
Presumed sepsisAge 1st line antibiotics Dose Duration
Premature baby IV C Penicillin +IV Gentamicin*
100,000u/kg/d div 12h 5-7 days
Term newborn IV Ampicillin + IV Gentamicin*
25-50mg/kg/dose 12h 5-7 days
Term newborn after day 5 of life
IV Ampicillin+ IV Gentamicin*
25-50mg/kg/dose 12h 5-7 days
If renal impairment to change to IV gentamicin with IV cefuroxime.*See Gentamicin dose
Severe infectionStep up Antibiotic Dose
2nd line of antibiotic Augmentin 20-50mg/kg/dose. <7d 12h, >7d 8h
3rd line of antibiotic Cefepime 100/kg/d div 12h
Amikacin 15mg/kg stat then Prem 7.5mg/kg/24h Term 15mg/kg/24h
4th line of antibiotic Imipenem 10-25mg/kg/dose 12h <7d. If >7d 8h
Meropenem 10-20mg/kg/dose. <7d 12h, >7d 8h.
Vancomycin Term 10mg 6hPrem<1200gm 15mg/kg/24h, 1200-2000gm 15mg/kg/12h, >2000gm <7d 15mg/kg/12h.> 7d 15mg/kg/8h
Neonatal meningitis Organism Antibiotics Dose Duration
Group B Streptococcus IV C Penicillin + IV Cefotaxime
400 000u/kg/d div 6h200mg/kg/d div 12h
14 days
Gram negative organism IV C penicillin + IV Cefotaxime
400 000u/kg/d div 6h200mg/kg/d div 12h
21 days
Subdural empyema IV C penicillin + IV Cefotaxime
400 000u/kg/d div 6h200mg/kg/d div 12h
4-12 weeks
Salmonella sp IV Ceftriaxone + IV Amikacin
100mg/kg/24h15mg/kg/24h
6-12 weeks(at least 1/12)
55

Other conditionsConditions Antibiotics Dose Duration
Septic spot Chlorhexidine BD
LA
Umbilical sepsis
IV Cloxacillin +IV Gentamicin
Prem (<2.5kg): 100mg/kg/d 7 days
Term: 200mg/kg/d <10d: div8h >10d: div6h
UTI prophylaxis
Trimethorprim 2mg/kg/nocte Until confirmed radiologically normal urological tract
Necrotizing enterocolitis
MetronidazoleAmpicillin+ Gentamicin
15mg/kg loading dose, then 15mg/kg div 12h
7-10 days
Neonatal tetanus
Metronidazole 15mg/kg loading dose, then 15mg/kg div 12h
10 days
Congenital toxoplasmosis
Pyrimethamine + Clindamycin + Folinic acid
Pyrimethamine:1mg/kg daily for 2-6 mths, then 1mg EOD to complete 1 yr.Folinic acid 10mg 3 times /week (dose increased as pyrimethamine toxicity)
1 year
Candida sepsis Fluconazole Loading 12mg/kg, maintenance 6mg/kg/dose.<30wk till 2wk 72h, then 48h<36wk till 2wk 48h, then 24h37-44 till 1wk 48h, then 24h>45wk 24h
10-14 days
*Gentamicin dosing and monitorAge Dose
<30 week 2.5mg/kg/24h30-35 week 3.5mg/kg/24hTerm 5mg/kg/24hMonitor BUSE and serum creatinine on day 3 of IV Gentamicin.
Drug levelDrug Trough Peak
Gentamicin <2ug/mL 5-10ug/mLAmikacin 3-5ug/mL 10-25ug/mLVancomycin 5-10ug/mL 25-40ug/mL
56
Criteria for consideration for systemic antifungal thaerapyA Babies who have been admitted to NICU for more
than two weeks with any of below:1. History of receiving TPN2. History of central venous catheter/ long line3. History of prolonged ventilation for more than 1 week4. Had been receiving Cefepime/ Carbapenem5. Unresolved signs of infection eg fever, thrombocytopenia6. Evidence of immunodeficiency7. Evidence of fungal colonization (cutaneous/ oral
candidiasis, tracheal secretion)8. Immunosupression states eg cytotoxic chemotherapy,
neutropeniaB Post-intraabdominal surgery
Strategy for antifungal: suspect fungal infection, obtain fungal cultures, initiate antifungal treatment, even before culture results are known, adjust antimicrobial therapy accordingly, once results have been obtained.
57

MANAGEMENT OF INFANT BORN TO RETROVIRAL POSITIVE MOTHER
(1) No need to take HIV PCR in the ward. It will be ordered during follow-up in Dr Fong's clinic review.(2) In certain cases where social background and compliance to follow-up is suspect, may consider to take HIV PCR in the ward before discharge at 48 hours life.
Updated on 26th Feb 2005
O&G to inform Paediatric MO upon delivery
Admission to NICU
Initiate bottle feeding Breast feeding is strictly contraindicated Start oral zidovudine as soon as possible (within 12 hours of life: dose 2mg/kg/dose 6 hourly)
Investigations to take: FBC, renal profile
Upon discharge, to ensure: Hepatitis B and BCG are given Counselling for mother: compliance to medication and follow-up
Get an appointment under Dr. Fong's clinic
at 2 weeks of life
58
PAEDIATRIC HIV DIAGNOSTIC TEST PROTOCOL
Indication: for infant age 0-18 months of HIV seropsitive mothers.
59
Paediatrician collects 2.5ml EDTA blood for baby and 2.5ml EDTA blood for mother.IMR/Virus/NARL 2 form to be filled in duplicate with Paediatrician’s name and telephone number.
Transport at room temperature to arrive in NARL on the same day
Tests done at NARL: Anti-HIV
HIV-AntigenHIV-PCR
Positive Negative
Fresh sample require for verification of results within 3 months
Positive Negative Serial testing 3 monthly till 18 months (Anti-HIV, HIV Antigen, HIV-PCR)
NegativePositive
HIV infectedNot infected
Repeated at 18 months of age for verification of true HIV status.
Ref: (55) dlm.KKM-97(467)Bhg 18Issued on: 27 Feb 1995

PAEDIATRIC HIV MANAGEMENT PROTOCOL
Prenatal CounsellingAll HIV positive mothers should meet the paediatrician once before delivery for prenatal counselling. In situations where this is not possible, the counselling can be done by family medicine specialist (FMS). The information given during the prenatal counselling should include:(1) The risk of having an infected baby is between 25-30% without any intervention.(2) The highest risk of vertical transmission is during the intrapartum period.(3) Zidovudine and caesarean section can reduce the risk of maternal-fetal transmission
to less than 2%.(4) A series of blood tests will be carried out on her baby following delivery.(5) Breast feeding must be avoided because it contributes to another 14% transmission to
the baby.
Labour and Delivery(1) The baby must be delivered in a hospital setting where there are doctors available,
irrespective of the mode of delivery.(2) The paediatric team must be informed about the impending delivery.(3) Zidovudine must be made available.(4) The fisrt dose of Zidovudine must be given within 12 hours of life.
Postnatal(1) Routine postnatal screening must be performed in the usual manner. If any neonatal
problems present, refer to paediatric team.(2) Zidovudine prophylaxis for 6 weeks: This could be initiated by Medical Officer.(3) Zidovudine dosage: Term: syrip zidovudine 2mg/kg/dose 6 hourly Premature baby: 1.5mg/kg/dose 6 hourly.If unable to take orally, use IV zidovudine. The baby must be seen by paediatrician at 2 weeks of age for follow up.
Diagnosis of HIV infectionA. In Infant (< 18 months) (1) Confirmation of the diagnosis is by virological tests only.
(2) Needs at least 2 consecutive positive HIV DNA PCR, performed at not less than one month apart.(3) Recommended schedule for testing is as follows: HIV DNA PCR at 2 weeks old, 3 months and 6 months. The first PCR may be performed anytime after 48 hours, should there be a possibility that the baby may not returned for the 2 week follow up. If the first PCR is positive, repeat as soon as possible.
(4) Interpretation of the PCR results: Infected: Two positive HIV DNA PCR performed on separate blood samples, regardless of age.
60
Not infected: HIV infection can be reasonably excluded in non-breast fed infants with 2 or more negative virologic tests performed at 1 months, with one of those performed at age 4 months. In such situation the infant needs to be followed up till 1 months old and the anti-HIV antibody test performed to document its disappearance.
B. Children (18 months or older)(1) Diagnosis may be based on serological tests (ELIZA) and confirmed by
immunoblot assay.(2) Needs at least 2 consecutive positive HIV antibody tests.
Follow up and MonitoringPaediatricians or FMS should follow up these babies.
(1) Monitor for the following:- Zidovudine tolerance- Adverse effects of zidovudine- Compliance- Growth and development- Symptoms and signs related to HIV infection
(2) Ensure appropriate investigations are carried out and results reviewed. Screen for other infectious diseases – VDRL, HBsAg and AntiHCV at birth:
Age At birth 2 weeks 6 weeks 3 months 6 monthsFBC √ √ √Renal profile1 √Liver function test √ √Creatinine kinase2 √ √HIV DNA PCR3 √ √ √
1In premature babies only, perform after 24 hours of life. Adjust dosage of zidovudine in renal impairment.2Where available.3If any PCR is positive, repeat as soon as possible.
(3) Ensure appropriate immunizations are given.(4) PCP prophylaxis should be given at 6 weeks of age. Dose: 4mg per kg per dose of
TMP 12 hourly given on alternate days. Stop if infant subsequently confirmed not infected (HIV).
(5) For those infants found subsequently not infected must be followed up annually till at least adolescent and refer to gynaecologist for screening of genital cancer.
Adverse effects of ZidovudineGeneral – fever, vomiting
GIT – transient elevation of hepatic transaminases Musculoskeletal – myopathy Haematological – anaemia (maximal effect at 6 wks), neutropenia, thrombocytopenia
61
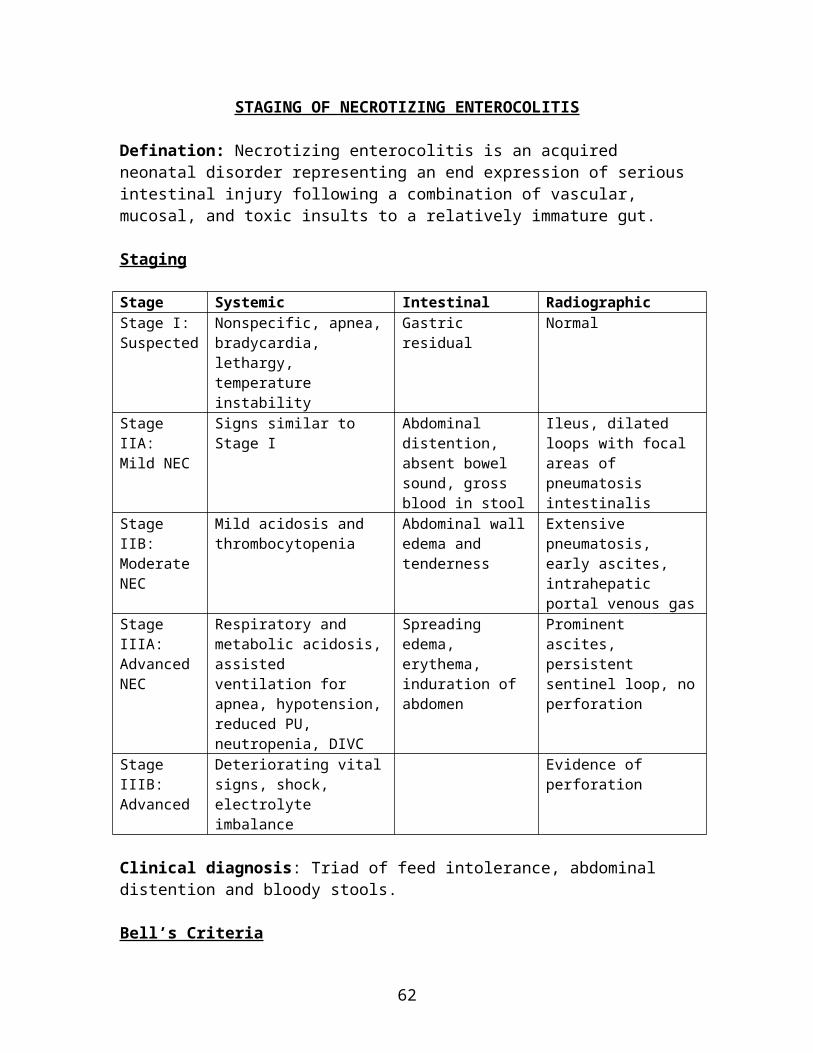
Immunisation ScheduleFollow the normal immunization schedule.The exceptions to the above are
Do not give oral polio vaccine (OPV) Replace OPV with injectable polio vaccine (IPV)
Polysaccharide pneumococcal vaccine is recommended at 2 years of age. If conjugated pneumococcal vaccine is available, this can be given at an earlier age.
Special ConsiderationsAbandoned babies:Initiation of postexposure prophylaxis with zidovudine after age 2 days is not likely to be efficacious in preventing transmission, and by the age of 14 days, infection would already be established in most infants. Abandoned babies pose a special problem because the HIV status of the mother and the age of the baby are unknown.
Rapid HIV screening and ELIZA HIV antibody tests must be done immediately on the baby's blood. The results can be used as a marker of maternal HIV status.
The presence of an attached umbilical cord stump may be used as a crude estimation of the age of the baby. A fresh (moist) umbilical cord stump indicates an age of less than 24 hours. In this group of babies zidovudine prophylaxis may be given if the above tests are positive.
62

MANAGEMENT OF BABY BORN TO VDRL POSITIVE MOTHER
(1) Mother was detected during antenatal period, more than one month before delivery and with treatment (very sure or documented):
(2) VDRL positive mothers who are not treated, inadequately treated, treated with drugs other than penicillin, received treatment in late pregnancy (ie less than one month before delivery) and where treatment is not known or documented:
(3) Treatment for VDRL positive mother: Early latent phase: IM Benzathine Penicillin weekly x 2 doses. Late latent phase: IM Benzathine Penicillin weekly x 3 doses.
Investigations in congenital syphilis:VDRL (Venereal Disease Research Laboratory)
Non-specific for syphilis
63
No clinical manifestation
No need admission
Send baby’s VDRL & TPHA &f/u in Paed clinic 2/52
VDRL titre increasingVDRL titre not increasing
F/u monthly and monitor VDRL titre
VDRL –ve / TPHA +ve or VDRL < mother’s
Baby’s VDRL > mother’s
No treatmentF/u 3/12, 6/12 with VDRL/TPHA
Admit for treatment
VDRL & TPHA negative
Admit, send baby’s VDRL/TPHA/FTA IgM& commence treatment
VDRL/TPHA negative With manifestation or VDRL/TPHA positive
LP
CSF abnormalCSF normal
IV C Penicillin 100,000/kg/day x10 days. BDx 1/52 then TDS.Or Procaine Penicillin G 50,000 u/kg/day IM for 10days.
IV C Penicillin 300-400000u/kg/day for 14 days. BD x 1/52 then TDS.
Discontinue Rx and d/cF/u 3/12, 6/12 with VDRL/TPHA
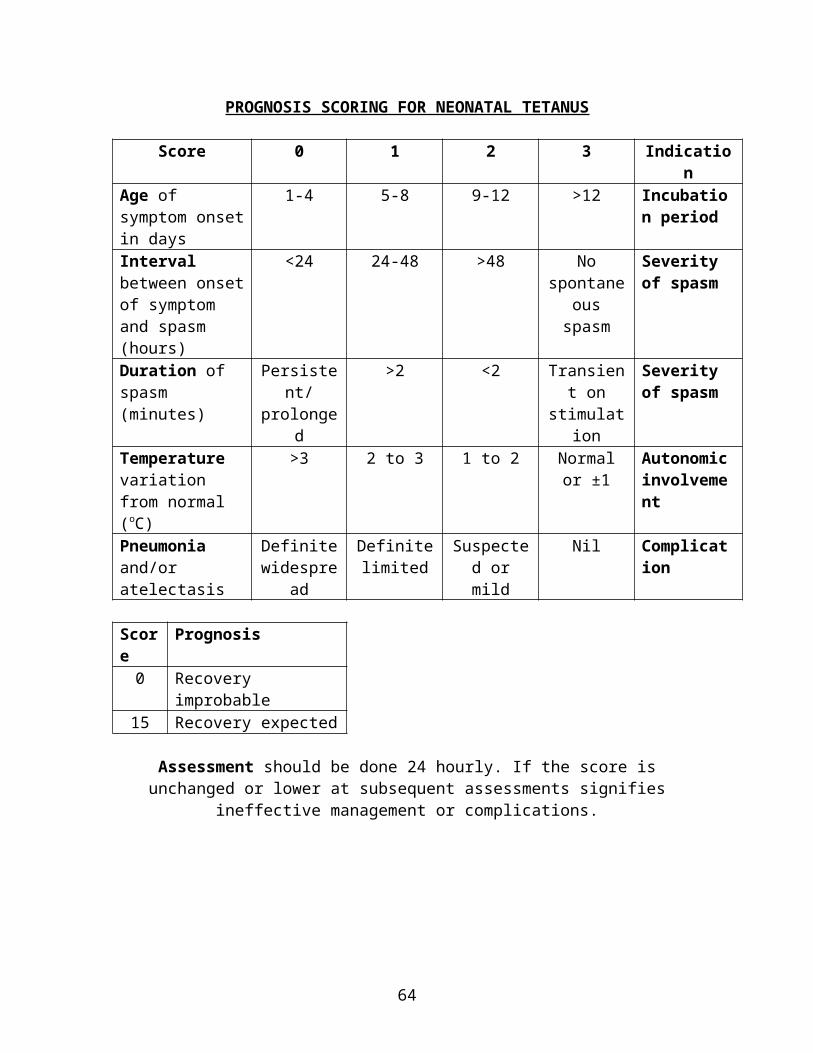
Titers rise when disease is active and fall when treatment is adequate (in congenital syphilis, this test becomes non-reactive within a few months after adequate treatment). False-positive VDRL can occur in an uninfected infant delivered to a VDRL mother because it detects maternal IgG that crosses the placenta. This is suggested when neonatal titers are significantly less (at least 4 fold) than the maternal titers and can be verified when Ab is no longer demonstrable by 3 month of age. False-negative VDRL may occur in patients who acquire infections late in pregnancy;
such infants become seropositive in the postnatal period.
TPHA (Treponemal Pallidum Haemagglutination) TPHA measures Ab specific for Treponema Pallidum. The test is not quantified; they are reported only as ‘reactive’ or non-reactive’. Once positive, the test remains positive for life, even when therapy is adequate. TPHA can be positive in an uninfected newborn; whose mother is TPHA positive
even if she has been adequately treated. This will become negative after the 6th month of life.
FTA (IgM) done in IMR, results may take months to come back. measures IgM antibodies that do not cross the placenta.
64

MANAGEMENT OF BABY OF MOTHER WITH CHICKEN POX
65
Time of the maternal chicken pox
5 days before & 28 days after delivery
More than last 28 days of life
To treat baby with: Varicella –zoster 125 units ASAP (not more than 48 hours) or IM Immunoglobulin 0.4ml/kg or IV Immunoglobulin 1.0ml/kg single dose. IV Acyclovir if baby symptomatic Chicken pox dose: 10mg/kg/dose 8h for 1/52. Varicella encephalitis dose: 20mg/kg/dose 8h x 10/7 Breast feeding only when maternal lesions dry Skin lesions developed to keep isolation for 3/52 If baby asymptomatic, to observe for 1/52 in the ward 30% mortality esp the 1st 10 days of life Once baby received immunoglobulin for chicken pox,
to give only BCG and defer other immunization schedule for 3/12
No treatment

NATIONAL SCREENING FOR CONGENITAL HYPOTHYROIDISM
RETINOPATHY OF PREMATURITY
Cord blood sample collected at birth in labour room1
Babies not discharged
Recall babies urgently by phoneor through nearest clinic/office
T4 Low3 (<100nmol/L)
T4 Normal (>100nmol/L)
Total T4 analysis (on cord blood)
Normal2
(<25mU/L)
Babies discharged
Send to lab for IX of TSH
Missed cases
High2,3
(>60mU/L)Borderline2,3
(25-60mU/L)
Result to Paediatric Clinic
Blood to lab for Ix of serum T4/TSH
Take blood for Ix. of T4/TSH6
Refer baby to Paediatric Clinic5
Further management by Paediatrician
1Blood taken by staff who conducts the delivery. Investigation form for screening of TSH to be filled up by attending staff.2Result to be sent to paediatric clinic and compiled by staff.3Lab to inform relevant officer/staff at paediatric clinic to recall for cases either by phone or to inform sisters/PHN at health districts/clinics.4Sister/PHN to recall babies.5Urgent referral and appointment to paediatric clinic after 3 days of life.6Blood to be taken at paediatric
clinic after 3 days of life.For asphyxiated neonates, repeat screening test should be done after 3rd day of life when hemodynamically stable.
66

Retinopathy of prematurity (ROP) is a disorder of immature retinal vasculature affecting the eyes of premature babies. It can be mild with no residual defects, or it may become aggressive with new vessel formation (neovascularisation) and progress to retinal detachment and blindness. The stimulus for this abnormal growth of blood vessels comes from the peripheral yet to be vascularised retina. Early detection and effective management of this condition can prevent blindness.
Indications for ROP screening(4) Birth weight < 1500gm(5) Gestational age < 32weeks(6) Selected infants with an unstable clinical course who are at high risk
Classification of ROPThe International Classification of ROP grades severity of the disease by stages (0-5), location of the disease into zones (1-3) and the extent of the disease based on the clock hours (1-12).StagesStage 0 Mildest form of ROP, with immature retinal vasculature and no clear demarcation of
vascularized and nonvascularized retinaStage 1 Fine , thin demarcation line with no height and thickness appears between the vascular
and avascular retina Stage 2 This white line widens into a broad, thick ridge clearly separating the vascular and
avascular retina Stage 3 Neovascularization grows into the vitreous on the ridge, on the posterior surface of the
ridge or anteriorly toward the vitreous cavity, so that the ridge has a velvety appearance with a ragged border
Stage 4 Sub-total retinal detachment beginning at the ridge where the retina is pulled anteriorly into the vitreous by the fibrovascular ridge
Stage 4A Partial retinal detachment does not involves the foveaStage 4B Partial retinal detachment involves the foveaStage 5 Total retinal detachment occurs in the shape of a funnelStage 5A Open funnelStage 5B Closed funnel
Plus disease is an indication of activity and is characterised by the appearance of dilatation and turtuosity of the peripheral retinal vessels, iris vascular engorgement, papillary rigidity, and vitreous haze.
ZonesZone 1 Extent from the optic dick to a point double the distance from the disc to the fovea, a
radius of 30o
Zone 2 Is a circle surrounding the zone 1 circle with nasal ora serrata as its nasal borderZone 3 The crescent that circle of zone 2 did not encompass temporally, inferiorly and
superiorly, but not nasally.
Clock hoursThe extent of ROP is recorded as clock hours in each eye according to the relevant zone.
67

Regressed ROPRegressed early phase ROP results in vitreoretinal sequelae producing vascular and retinal peripheral changes in both the posterior and peripheral retina.
When to screen(1) The 1st examination should be performed 4 to 6 weeks after birth(2) Weekly eye examination should be carried out for the following threshold disease:
(a) ROP zone 1, less than threshold(b) ROP zone 2, stage 2 with plus disease(c) ROP stage 3 without plus disease(d) ROP stage 3 with plus disease but less than threshold
(3) If there is no ROP, subsequent examinations should be carried out at least every 2 weeks.
(4) Screening should be discontinued in the following situations:(a) infant has reached 45 weeks postmenstrual age without developing pre- threshold ROP(b) vascularisation has progressed into zone 3 without previous zone 1 or 2 ROP(c) full vascularisation
Complications of ROPComplications Percentage
Myopia 80%Strabismus and amblyopia 20%Retinal detachment 22%Acute angle closure glaucoma
Follow upPost screening Assessment of vision throughout the 1st year and periodic monitoring of
the visual acuityChildren treated for ROP Pre-school years-monitor development of vision, refractive status and
motilityPatients with threshold ROP Tailored individually, 3 months after adequate laser or cryotherapy, then
yearly or more frequently depending on clinical findingsPatients with complications Follow up over long period
Clinical Practice Guidelines on retinopathy of prematurity by Academy of Medicine and Ministry of Health of Malaysia, 2005.
68

APPENDIX 1HOW TO REFER TO PAEDIATRIC MO IN HOSPITAL LIKAS
1. Refer cases to 2nd MO on call, even during office hours. 2. All cases must refer on the same day (with referral form).3. Keep NICU clerking sheet in OT, LR and Obst. wards.4. Referral to stand by for Em. LSCS must discuss with O&G MO before referral.5. Indications for referral:Maternal history mother with bad obstetric historyBaby whose mother has
chicken poxherpes simples type 2 for SVDPTB if untreated/sputum +veHBsAg +veVDRL +veretrovirus +veRh –veimpaired GTT/diabetes
Maternal risk of sepsis
prolonged rupture membranes >24 hoursmaternal chorioamnionitis
obstetrician defined criteria foul smelling liquor
maternal UTI ufeme wbc>10 ufeme bacteria>3 significant positive urine C&S
maternal fever fever >38’C (excluding intrapartum) all episodes of intrapartum fever
Delivery instrumental delivery refer at/pending delivery if fetal distress refer during office hours if baby is otherwise OK
emergency LSCS for fetal distresscord prolapseall meconium stained liquor (except light)twin or multiple pregnancy
Baby prematurity <36 weeksbirth wt <1.7kg or >4.0kggrunting/flat babiesbaby with 5 minute Apgar score < 7congenital abnormalitiessick baby: fever, poor feeding, cyanosed, tachypnoea, tachycardia, bradycardia, desaturate, lethargy and etc.baby with G6PD deficiencybaby with SB > PL with reference to bilirubin chart
69

APPENDIX 2FLOW CHART OF NEONATAL JAUNDICE REFERRAL
FROM HEALTH CLINICS TO HOSPITAL LIKAS
N
otes:1. *Health clinics are Klinik Kesihatan Ibu dan Anak, Klinik Kesihatan and Klinik Desa. 2. The ward staff nurse who converse with the health nurse must inform the 2nd Paediatric MO on call regarding the case.
3.**If the second medical officer not available in the ward, he/she should be contacted via his/her handphone. The ward staff nurse should provide the handphone number of the 2nd Paediatric MO oncall to the health nurse.
HL=Hospital Likas
HEALTH CLINICS*
MEDICAL OFFICERAvailable on-site
MEDICAL OFFICERNot available on-site
Direct referral by HEALTH MO to
HL’s 2nd Paediatric MO on call**
Direct referral by HEALTH CLINIC NURSE to
HL’s 2nd Paediatric MO on call**
HL’s 2nd Paediatric MO on call** to accept referral
70
APPENDIX 3IMPORTANT FORMULA
Anion gap = (Na+K) – (Cl+HCO3)Bicarb correction = 1/3 x BW X BE in ml of 8.4% bicarbBicarb deficit = 0.4 x BW x (desired HCO3-actual HCO3)Blood volume, neonate 80ml/kg ___________________Body surface area, BSA(m2)=√ht(cm) x wt(kg) ÷ 3600Creatinine clearance (ml/min/1.73m2) = UV x 1.73___ P BSA(m2) = K x Ht(cm) P(mg/dL) U=urine creat(mg/dL) P=plasma creat(mg/dL) V=urine volume(ml/min) K=constant; children 0.55, adolescent 0.70, infant 0.45 Normal: NB=40-65ml/min/1.73m2
1.5yr: M=125, F=109 adult: M=105,F=95 Creat, mg/dL x 88.4 = umol/LFraction excretion, Na FE= urine Na ÷ urine creat x 100% plasma Na plasma creat <1% prerenal failure >2% ATNInsensible water loss=400mL/m2/24H, neonate <1.5kg=40ml/kg, >1.5kg=30ml/kgOxygen content=[SaO2% x Hb(g/dL)] + [0.003 x PaO2mmHg]PaO2/FiO2 > 200mmHg (N)PEFR(L/min)=5 x ht(cm) – 400 pH probe catheter distance=[ 5+(0.252xht)] x 0.87Protein/creatinine ratio (urine) <200mg/mmolProteinuria (nephritic) >3.5gm/24H, >40mg/m2/H QTc= QT(s) infant<0.45, children<0.44, adult<0.53 √RR(s)Renal failure index = Urine Na X Plasma Creatinine Urine creatinine Resistive index N=0.65-0.85 >0.85 ICP, <0.65 loss of autoregulationSerum osmolality=2(Na)+Glu+BUN, N=285-295mOsm/LUAC=base of umbilicus to tip of shoulder =3 x BW + 9 (cm)UVC=½ of UAC, high UVC +2cm
In CAH, HCT suppression dose =15mg/m2/d ÷3 doses
Anti-TB:Drugs Intensive
(usual daily)Maintenance (Biweekly)
INH 5-10 (10) 5RIF 10-20 (15) 10PZA 20-40(25) 50SM 20-40EMB 15-25Extrapulm Add amikacin
71
APPENDIX 4WHO DEFINITIONS
Live birth The complete expulsion or extraction from its mother of a product of conception, irrespective of the duration of the pregnancy, which, after such separation, breathes or shows any other evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, whether or not the umbilical cord has been cut or the placenta is attached; each product of such a birth is considered live-born.
Fetal death The death prior to the complete expulsion or extraction from its mother of a product of conception, irrespective of the duration of pregnancy; death is indicated by the fact that after such separation the fetus dose not breathe or show any other evidence of life, such as beating of the heart, pulsation of the cord, or definite movement of voluntary muscles.
Birth weight The first weight of the fetus or newborn obtained after birth. This weight should be measured preferably within the first hour of life before significant postnatal weight loss has occurred.
Low birth weight <2500gm (up to and include 2499gm)Very low birth weight <1500gmExtreme low birth weight <1000gmGestation age The duration of gestation is measured from the first day of the last
menstrual period. Gestational age is expressed in completed days or in completed weeks (eg events occurring 280-286 days after the onset of the last normal menstrual period are considered to have occurred at 40 weeks gestation). Measurements of fetal growth, as they represent continuous variables, are expressed inrelation to a specific week of gestational age (eg the mean birth weight for 40 weeks is that obtained at 280-286 days of gestation on a weight for gestaional age curve).
Preterm <37 completed weeks (<258 days).Term From 37 to < 42 weeks (259-293 days).Post-term 42 completed weeks or more (294 days or more).Stillbirth rate Stillbirths x 1000
Live births + StillbirthsPerinatal mortality rate (Stillbirths + Deaths at 0-6 days after live birth) x 1000
Live births + StillbirthsEarly neonatal mortality rate
Deaths at 0-6 days after live birth x 1000Live births
Late neonatal mortality rate
Deaths at 7-27 days after live birth x 1000Live births
Neonatal mortality rate Deaths at 0-27 days after live births x 1000Live births
Postneonatal mortality rate Deaths at 1-11 months after live birth x 1000Live birth
Infant mortality rate Deaths under the age of 1 year after live birth x 1000Live births
72