nihan kahya eren, md izmir ataturk education and research...
TRANSCRIPT

Nihan Kahya Eren, MDIzmir Ataturk Education and Research Hospital
Cardiology Department

Hypertensive Disorders of Pregnancy
Definition:
Systolic bld pressure ≥
140 mm Hg or
Diastolic bld pressure ≥
90 mm Hg on at least 2
seperate measurements
Prevalance: 6‐10% of all pregnancies
Major cause of maternal, fetal and neonatal
morbidity and mortality
16%of maternal deaths in developed countries

Hemodynamic Changes During Pregnancy
Plasma volume expansion (50%)
Heart rate increase (20%)
Cardiac output increase (50%)
Peripheral vascular resistance decrease
Systemic blood pressure decrease

Hypertensive Disorders of Pregnancy Classification:
Gestational hypertension:
HT w/o proteinuria after 20 weeks of gestation
Preeclampsia
HT and proteinuria after 20 weeks of gestation
Preexisting hypertension (Chronic HT)
HT before 20 weeks of gestation or persisting >12 weeks
postpartum
Preexisting HT with superimposed preeclampsia
Transient HT of pregnancy
Retrospective diagnosis

Preexisting (Chronic) Hypertension
•
HT before 20 weeks of gestation or persisting >12 weeks postpartum
•
Prevelance: 1‐5%
•
Mild‐moderate HT:
Sistolic 140‐159 mm Hg; diastolic 90‐105/109 mmHg
•
Severe HT:
Sistolic ≥
160 mm Hg
Diastolic ≥
105‐110 mm Hg

Preexisting HypertensionAdverse outcomes related to chr. HT in
pregnancy:
Placental abruption
Low birth weight
Premature birth
Perinatal mortality
Preeclampsia

Preexisting Hypertension: Management
Optimal blood pressure during pregnancy?
Medical tx of mild‐moderate HT during pregnancy improves maternal outcomes?
Fall in mean arterial pressure may lead to decreased uteroplacental perfusion?

Preexisting Hypertension:Management Cochrane Metaanalysis
Role of antihypertensive drug therapy in pregnant women with mild‐moderate HT (either chronic or gestational)
28 trials, n=3200
Antihypertensive therapy vs placebo/no therapy:
Decresed the risk of developing severe HT
No effect on the risk of preeclampsia
No improvement in perinatal outcomes (perinatal death, preterm
birth)
No effect on birth weight
Cochrane Database of Systematic Reviews 2007, Issue 1.

Preexisting Hypertension:Management JNC, NHBPEP
Women with stage 1 HT (<160/100): Non‐pharmacologic
treatment:
Limitation of activities
ASA for high risk for preeclampsia
Drug therapy: SBP ≥
160; DBP ≥
100 mm Hg
Medications can be tapered during pregnancy
Reinstitude if systolic BP150‐160; diastolic 100‐110 mm Hg
TOD (+), or a previous requirement of multiple medications: continue therapy
ESC
SBP≥
150, DBP ≥
95 mm Hg: Drug treatment
HT+ subclincal organ damage: drug tx if BP ≥
140/90 mm Hg

Preexisting Hypertension:Management Methyldopa:
Long‐term follow‐up studies supporting
safety
Maintain stable uteroplacental blood flow
Beta blockers:
Labetalol:
Β‐blocking agent with some α‐blocking activity
As effective as methyldopa, less adverse effects
IUGR (atenolol) when used during first trimester
Atenolol and metoprolol safe and effective in late
pregnancy

Preexisting Hypertension:Management Calsium antagonists:
Limited data
No increase in major teratogenicity with exposure
Diuretics:
No increase in adverse fetal events
May potentiate volume depletion in preeclampsia
ACEI and ARB are contraindicated

Medications in Hypertension of Pregnancy
Drug Dose Adverse events in pregnancyMethlydopa 500 mg–3 g in 2
divided dosesPeripheral edema, anxiety, nightmares, drowsiness, dry-mounth, maternal hepatitis
Labetalol 200-1200 mg/dayİn 2-3 divided doses
Persistent fetal bradycardia, hypotension, neonatal hypoglycemia
Hydrochlorothiazide 12,5-25 mg/day Fetal malformations, electrolyte abnormalities,
volume depletion
Nifedipine 30-120 mg/day Inhibition of labor particularly if used with Mg sulphate
Metoprolol 25-200 mg/day Possible association with fetal growth restriction
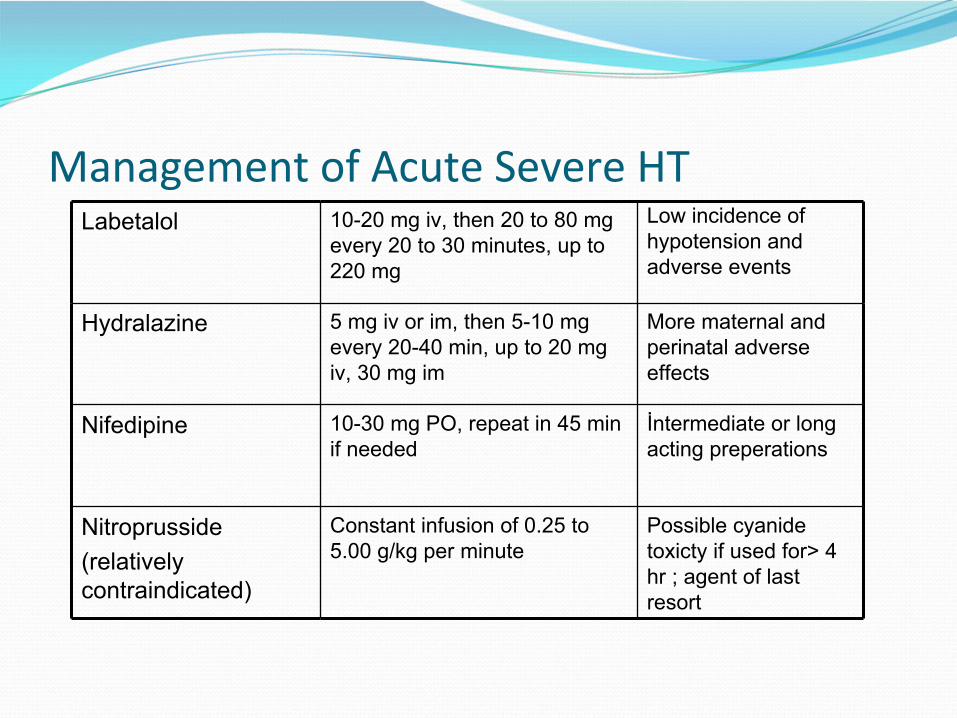
Management of Acute Severe HT Labetalol 10-20 mg iv, then 20 to 80 mg
every 20 to 30 minutes, up to 220 mg
Low incidence ofhypotension andadverse events
Hydralazine 5 mg iv or im, then 5-10 mg every 20-40 min, up to 20 mg iv, 30 mg im
More maternal and perinatal adverse effects
Nifedipine 10-30 mg PO, repeat in 45 min if needed
İntermediate or long acting preperations
Nitroprusside(relatively contraindicated)
Constant infusion of 0.25 to 5.00 g/kg per minute
Possible cyanide toxicty if used for> 4 hr ; agent of last resort

Preeclampsia Superimposed on Preexisting HT
20‐25% of women with preexisting HT
New onset proteinuria after 20 weeks in a woman with chronic hypertension
In a woman with hypertension and proteinuria prior to 20 weeks gestation:
Sudden 2‐
to 3‐fold increase in proteinuria
Sudden increase in BP
Thrombocytopenia
Elevated AST or ALT

Hypertensive Disorders of Pregnancy
Gestational HT:
HT w/o proteinuria after 20 weeks of gestation
Preeclampsia:
Multiorgan disease process characterized by the
development of hypertension and proteinuria (>300mg/day) after 20 weeks of gestation
Up to 50% of women with gestational HT develop
preeclampsia

Hemodynamics in Preeclampsia
Plasma volume and CO decrease
İncrease in systemic vascular resistance

Preeclampsia : Pathophysiology
Abnormal placentation•Abnormal trophoblast invasion
•Inadequate vascular remodelling of spiral arteries into low resistance vessels
•Reduced blood flow to the feto-placental unit
Poor placental perfusion
Circulating factors triggering endothelial dysfunction and generalised hyperinflammatory
state
Altered placental angiogenesisAngiogenic factors: Decreased placental GF,VEGFIncreased anti-angiogenic factors
Maternal
sx of preeclampsia

Multiorgan System Involvement in Preeclampsia
Preeclampsia
CNS:Severe headache
Visual disturbances,Hyperreflexia
Cerebral hemorhageKidney:Decreased filtration rate
ARF
Lung:Pulmonary edema
ARDS
Liver: Elevated transaminase levels
Subcapsular hemorrhage
Hematological:Trobocytopenia
HemolysisDIC
Placental abruptionIUGR

Preeclampsia : Risk Factors
•Nulliparity•Preeclampsia in a previous pregnancy•Elevated BMI (>30)•Multiple gestation•Maternal age > 40 years•Antiphospholipid antibody syndrome•Chronic renal disease•Diabetes mellitus•Chronic hypertension

Diagnostic Criteria for Severe Preeclamsia:
Blood pressure ≥
160 mm Hg systolic or 110 mm Hg
diastolic (during bed rest) or
Proteinuria ≥
5g/day or
Any of the following associated signs and symptoms:
Cerebral or visual disturbances
Epigastric or right upper quadrant pain
Impaired liver function
Oliguria < 500 mL in 24 hours
Pulmonary edema
Thrombocytopenia
Fetal growth restriction

HELLP Syndrome
A variant of severe preeclampsia
Hemolysis + Elevated Liver enzymes + Low Platelet count
Occurs in 20%of pregnancies with severe preeclampsia

Management of Preeclampsia:
Delivery is the only cure for preeclampsia
Decion to deliver:
Risk of worsening preeclamsia
Risk of prematurity

Treatment of Mild Preeclampsia
Delivery is generally not indicated until 37 to 38
weeks of gestation
Maternal monitoring:
Measure BP twice/week
CBC, platelet count, ALT, AST, LDH, uric acid, creatinine (1/week)
Assess for proteinuria: screen with dipstick or spot
protein/creatinine ratio and obtain periodic 24‐hour urine collections
Fetal monitoring
Nonstress test (2/week)
Measure amniotic fluid index (1‐2/ week)
Perform ultrasonography for fetal growth every 3‐4 weeks

Management of Mild Gestational Hypertension or Preeclampsia
Maternal and fetal evaluation:
•≥
40 weeks of gestation•≥37 weeks and
•Bishop score ≥
6•Noncompliant patient
•<37 weeks and•Worsening maternal and fetal condition
•≥
34 weeks •Labor or rupture of membranes•Abnormal fetal testing results•Intrauterine growth restriction?
Delivery

Management of Severe Preeclampsia
Hospital admission, bed rest
Maternal and fetal evaluation for 24 hours
Magnesium sulphate for 24 hours
Antihypertensive tx if:
Sistolic BP ≥160 mm Hg
Diastolic BP ≥110 mm Hg
Mean arterial pressure > 125 mm Hg

Management of Severe Preeclampsia: Antihypertensive treatment:
BP >160/110 mm Hg
Goal of tx: sistolic 140‐155 mm Hg,
diastolic 90‐105 mm Hg
Acute management:
İv. hydralazine :
5 mg IV, 5–10mg every 20–40 min up to 30 mg
iv. labetalol:
20 mg IV, 40‐80 mg every 10‐15 min. up to 220 mg
For patients undergoing expectent management remote from term oral labetalol and nifedipine acceptable

Management of Severe Preeclampsia
•≥34 weeks of gestation or
•Maternal distress (Ecclampsia, trombocytopenia,pulmary edema, hemolysis and elevated liver enzymes)
•Nonreassuring fetal status
•Severe IUGR•Labor or rupture of membranes
Maternal and fetal evaluation:
DeliveryWithin 24 hours
<23 weeks of gestation
Termination of pregnancy
24-33 weeks of gestation
SteroidsAntihypertensives if neededDelivery

Preeclampsia: Postpartum Management
Most patients respond promptly to delivery with decreased BP and clinical improvement
Eclampsia may occur postpartum
greatest risk within 48 hours
Mg sulphate continued for 12‐24 hours

Postpartum Management:
Antihypertensive treatment during lactation:
Methyldopa, labetolol, nifedipine, captopril, enalapril, quinapril
Atenolol may cause bradycardia and lethargy in newborns
Diuretics may reduce milk volume
Thank You


HELLP Syndrome
A variant of severe preeclampsia
Hemolysis + Elevated Liver enzymes + Low Platelet count
Occurs in 20%of pregnancies with severe
preeclampsia
Clinical presentation is variable:12‐18% are normotensive13% proteinuria (‐)At diagnosis 30% postpartum, 18% term, 52% preterm
Common presenting sx: Right upper quadrant pain or epigastric pain, nausea, vomitting,
non
spesific sxSigns and sx: CBC, plt count and liver enzyme should be evaluated

Management of Mild Gestational Hypertension or Mild Preeclampsia
Antihypertensive treatment:
No compelling studies showing prolonged gestational
age or improved outcomes with antihypertensive tx
ESC Antihypertensive tx >140/90 mm Hg
NHBPEP Antihypertensive tx >160/105-110 mm Hg