no slide title ent.pdf• we can not treat these patients differently just because they are bleeding...
TRANSCRIPT

CRITICAL ENT!!
Roger Boles, M.D., Endowed Chair in Otolaryngology EducationDepartment of Otolaryngology-Head and Neck Surgery
University of California-San FranciscoSchool of Medicine
Andrew H. Murr, M.D. FACSProfessor of Clinical Otolaryngology
Chief of ServiceSan Francisco General Hospital

Outline
• SINUSITIS
• NOSEBLEED
• THE SURGICAL AIRWAY
• NASAL TRAUMA
• OTOLOGIC EMERGENCIES
SINUSITIS
• 30 MILLION PATIENT VISITS PER YEAR• THE MOST COMMON CHRONIC
COMPLAINT FOR WHICH A PATIENT SEEKS ADVICE FROM A PHYSICIAN IN THE USA
• MULTI-BILLION $$$$$ PHARMACEUTICAL INDUSTRY

Common Perception: NY TIMES

Acute v. Chronic
• Acute– Classic picture: fever, pain,
WBC, pus, “sick”

History
• Frequency, duration, past intervention, effectiveness of intervention
• Symptoms– Nasal congestion, facial pressure, PND, cough– Facial Pain~ relatively UNCOMMON!!!!– PMH: childhood sinusitis, immunocompromise,
triggering events (time of year)– PSH: sinus or nasal surgery, dental surgery– Medications: Beta blockers, BCP

HISTORY
COMMON• URI• “FLU”• SEASONAL ALLERGIC
RHINITIS• PERENNIAL ALLERGIC
RHINITIS• VASOMOTOR RHINITIS• BACTERIAL
RHINOSINUSITIS• PREGNANCY• SIDE EFFECT OF
MEDICATION• MIGRAINE• TOOTH ABSCESS
LESS COMMON• SARCOID• WEGENERS• T CELL LYMPHOMA• AML, ETC.• SAMTER’S• NASAL POLYPOSIS• FOREIGN BODY• IMMUNOCOMPROMISE• CYSTIC FIBROSIS• ALLERGIC FUNGAL
SINUSISTIS• CILIARY DYSKINESIA• ILLICIT SUBSTANCE USE
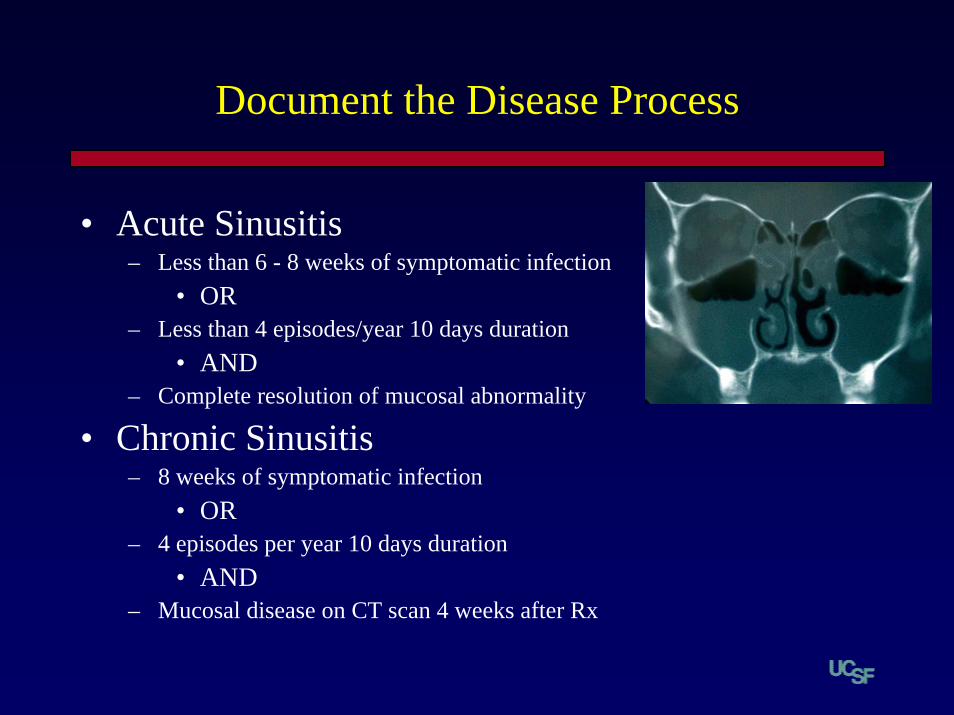
Document the Disease Process
• Acute Sinusitis– Less than 6 - 8 weeks of symptomatic infection
• OR– Less than 4 episodes/year 10 days duration
• AND– Complete resolution of mucosal abnormality
• Chronic Sinusitis– 8 weeks of symptomatic infection
• OR– 4 episodes per year 10 days duration
• AND– Mucosal disease on CT scan 4 weeks after Rx
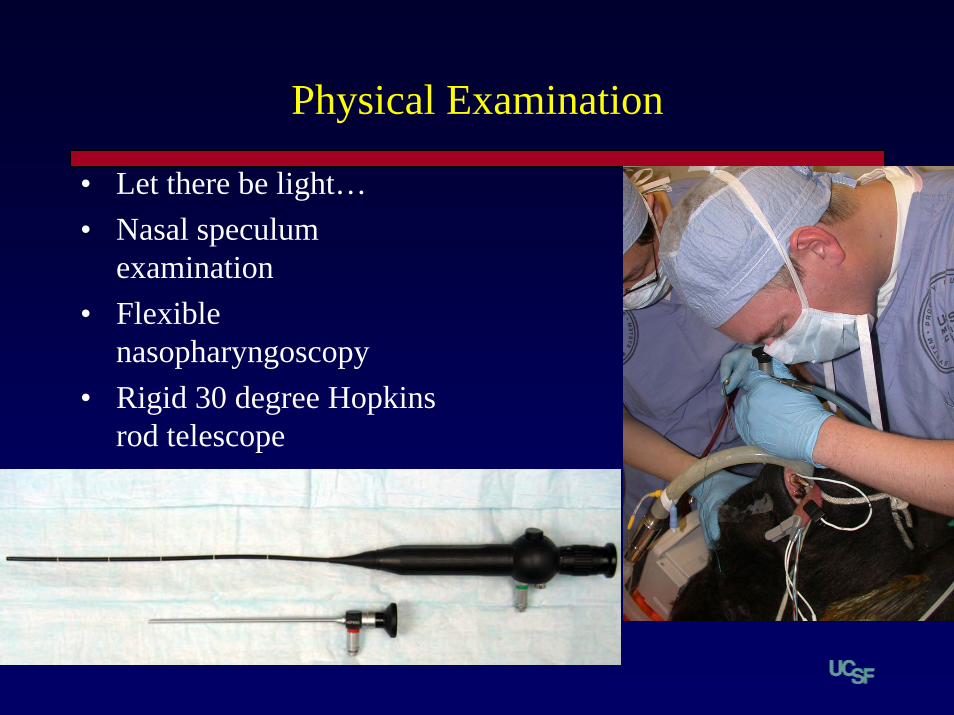
Physical Examination
• Let there be light…• Nasal speculum
examination• Flexible
nasopharyngoscopy• Rigid 30 degree Hopkins
rod telescope


Approach to the patient
Acuteyes no
Rx abi Rx symptoms
improved not improved improved
stop CT scan appropriate management
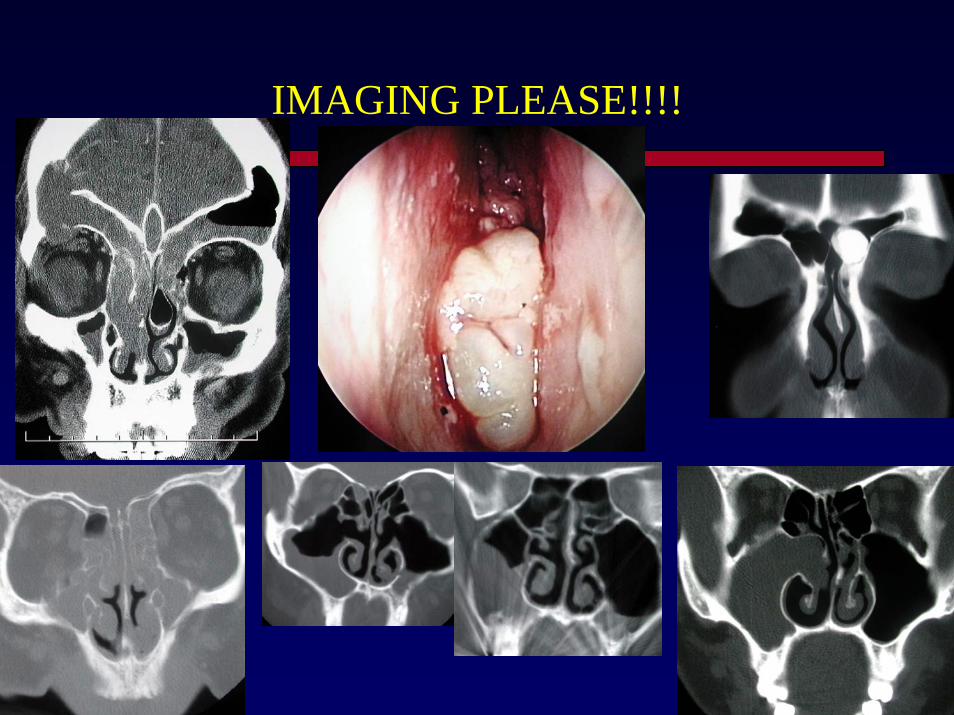
IMAGING PLEASE!!!!

EFFICACY OF PLAIN FILMS
• OFFICE CT SCAN??

Pt. presents with acute sinusitis and swollen eye. You should ….
A. S
ign out im
mediat
ely
B. P
rescri
be oral
antib
...
C. P
rescri
be IV
antib
i...
D. O
btain a
CT w
ith c.
..
E. Plai
n films a
re bes
t
1% 4% 1%
81%
13%
1. A. Sign out immediately2. B. Prescribe oral antibiotics3. C. Prescribe IV antibiotics4. D. Obtain a CT with contrast5. E. Plain films are best
Just another weekend on top of the Golden Gate Bridge…
EPISTAXIS
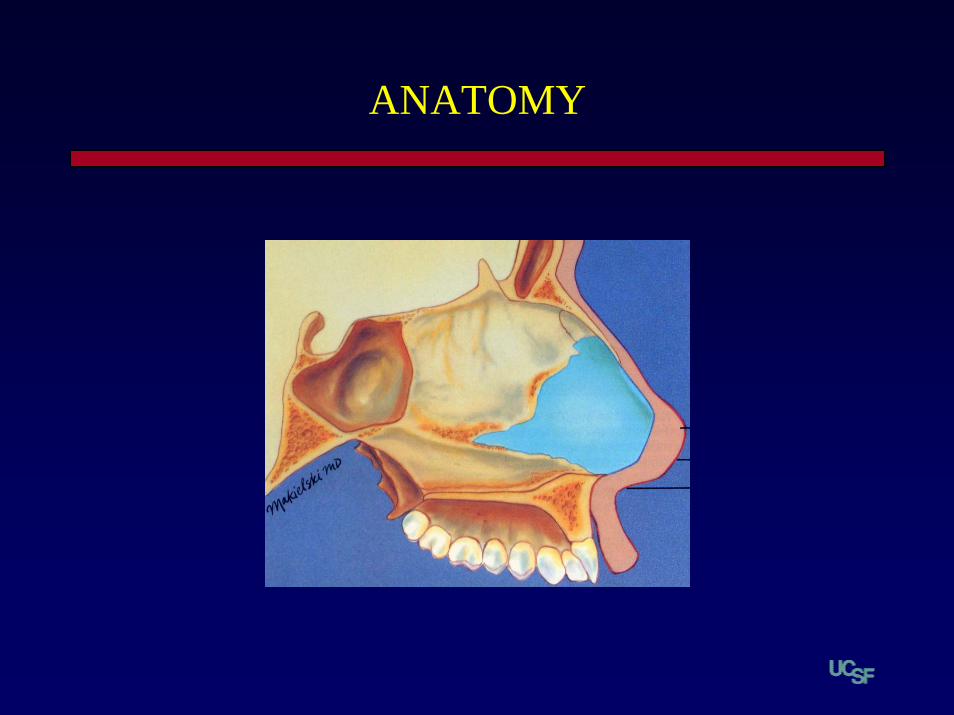
ANATOMY
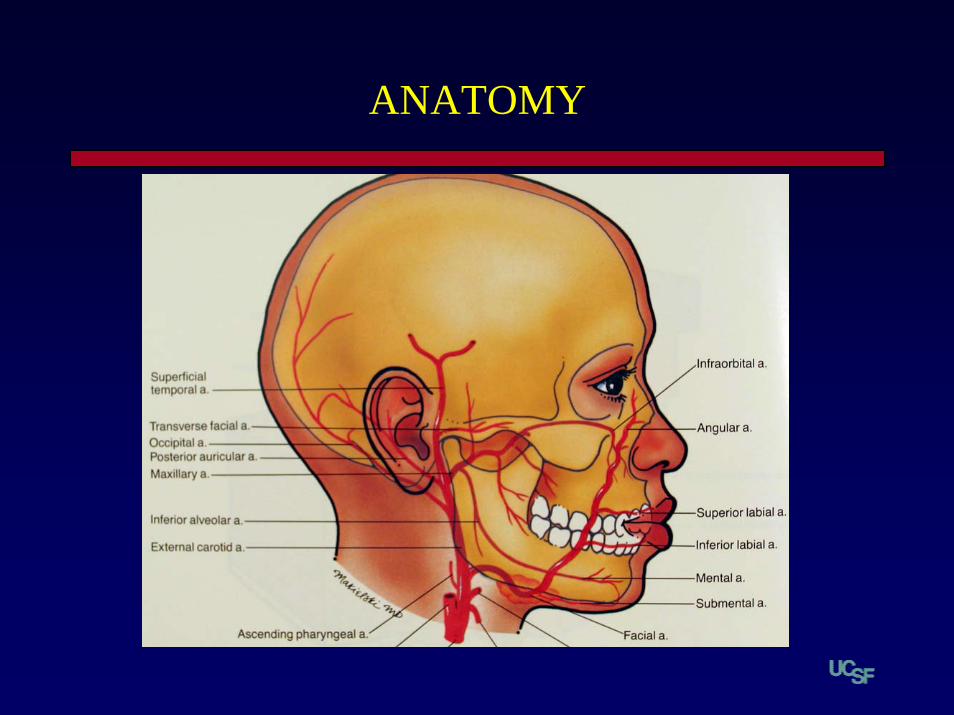
ANATOMY

DON’T FORGET YOUR ABC’S
• AIRWAY • BREATHING • CIRCULATION
– IV– H/H– Type and Cross– Platelet Count– History!!!
• Aspirin• Coumadin• Bruising• Family history
• We can not treat these patients differently just because they are bleeding from their nose!!
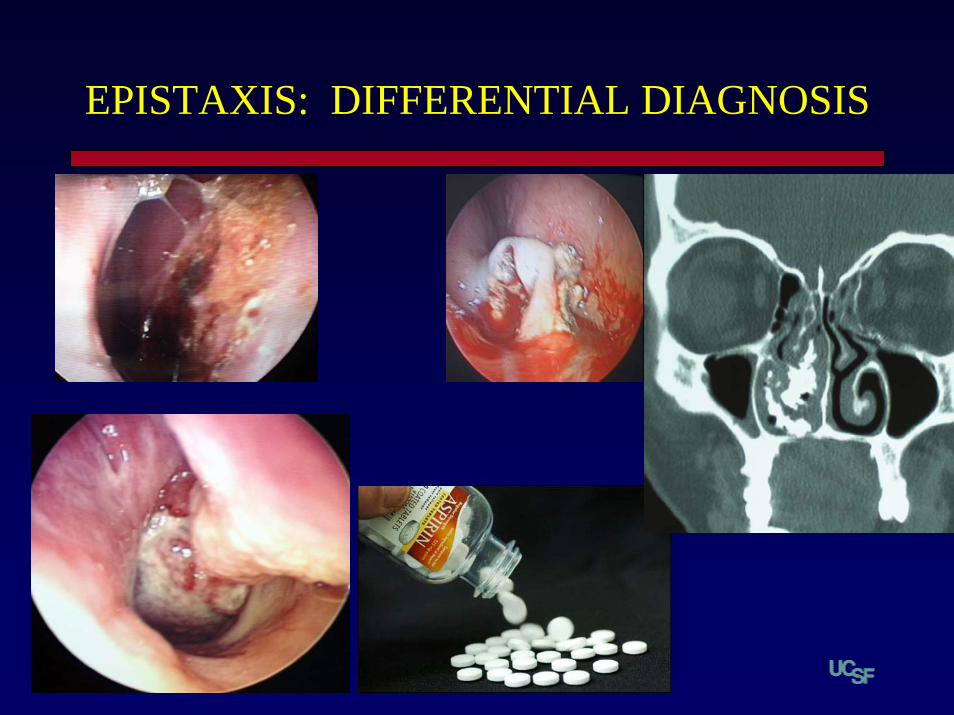
EPISTAXIS: DIFFERENTIAL DIAGNOSIS

TOOLS
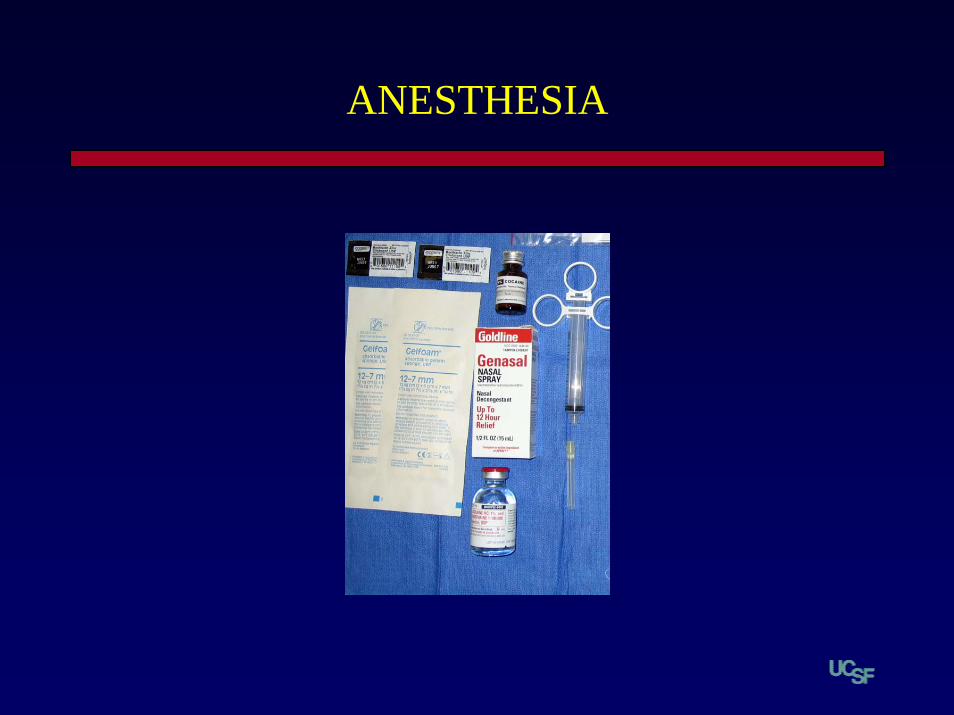
ANESTHESIA
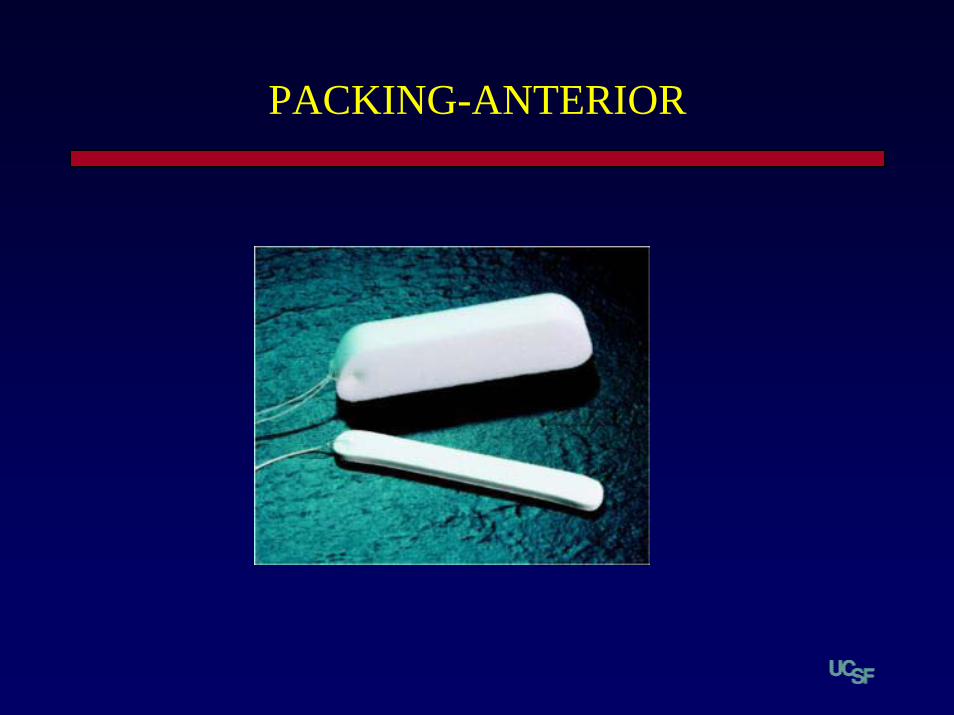
PACKING-ANTERIOR

DON’T FORGET TO USE ANTIBIOTICS AND TO REMOVE THE PACKING

PACKING-POSTERIOR
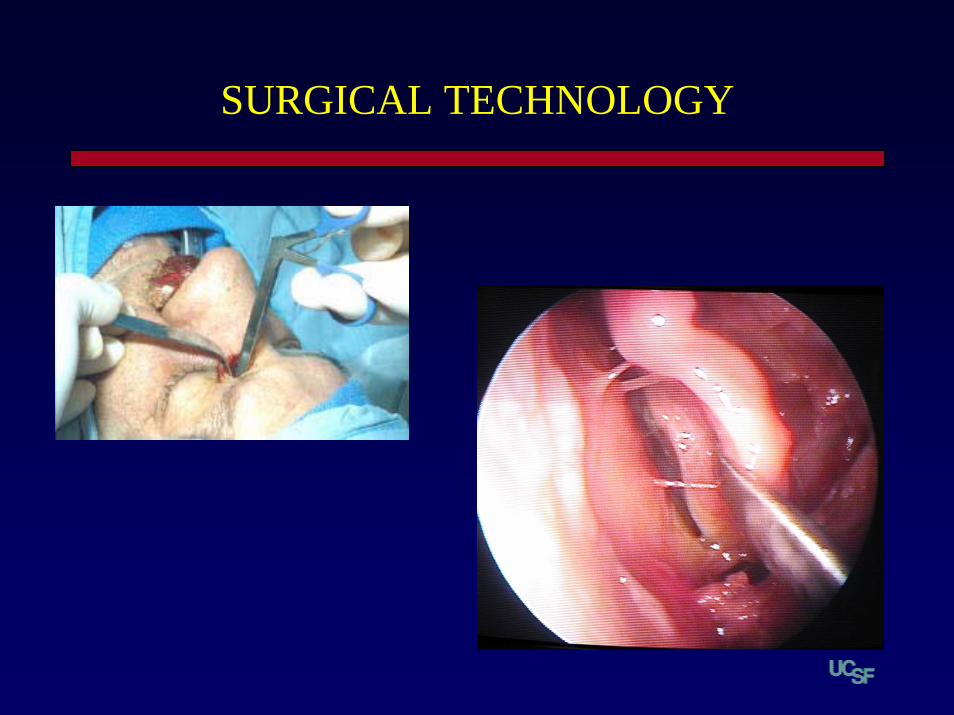
SURGICAL TECHNOLOGY
INTERVENTIONAL TECHNOLOGY
Pt. presents with a nosebleed, you should…
2%
97%
0%1%0%
1. A. Call an immediate ENT consult2. B. Begin an IV, T+C, H+H and ask Pt to blow their
nose3. C. Order a CT with contrast4. D. Call a GI consult5. E. Perform a tracheotomy

SURGICAL AIRWAY

AIRWAY CONTROL PREFERENCE
• 1. INTUBATION• 2. INTUBATION• 3. FIBEROPTIC INTUBATION

SURGICAL AIRWAY CONTROL
• PENETRATING TRAUMA• ANGIOEDEMA• OBSTRUCTING TUMOR
– LARYNGEAL SQUAMOUS CELL CARCINOMA• INFECTION
– LUDWIG’S ANGINA– EPIGLOTTITIS– DEEP NECK INFECTION
• SEPTIC SHOCK
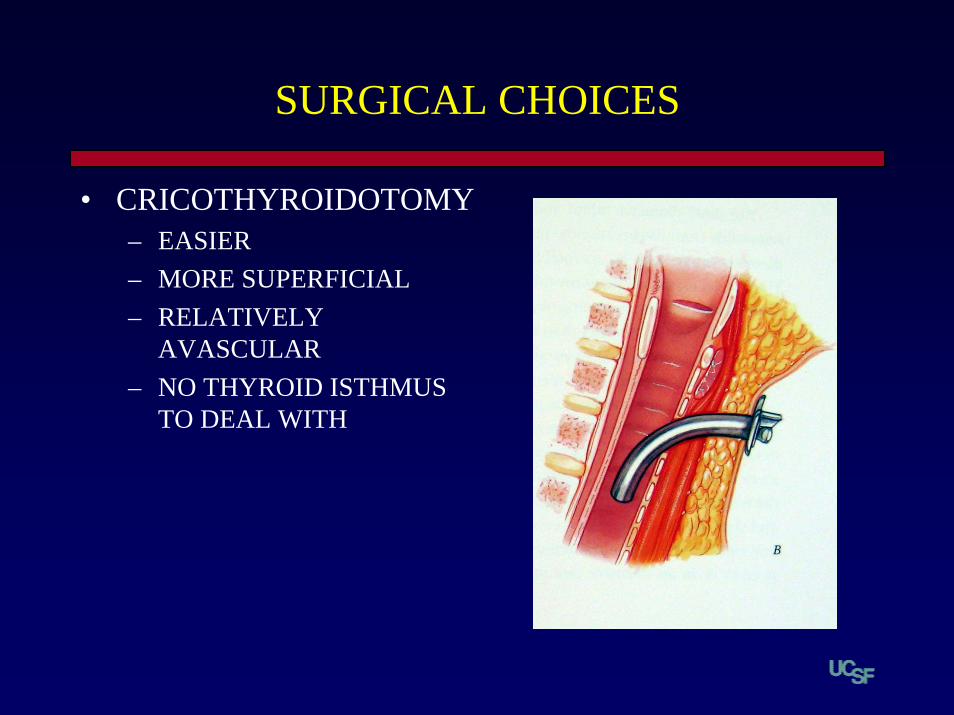
SURGICAL CHOICES
• CRICOTHYROIDOTOMY– EASIER– MORE SUPERFICIAL – RELATIVELY
AVASCULAR– NO THYROID ISTHMUS
TO DEAL WITH

ANATOMY
• ANTERIOR JUGULAR VEINS

PROBLEMS WITH CRICOTHYROIDOTOMY
• ALL OF THE CONTRARY SEQUELAE OF INTUBATION!
– GRANULOMA– PARESIS– STENOSIS– CARTILAGE NECROSIS
• ACCEPTABLE FOR SHORT PERIODS
• ANY AIRWAY IS ACCEPTABLE
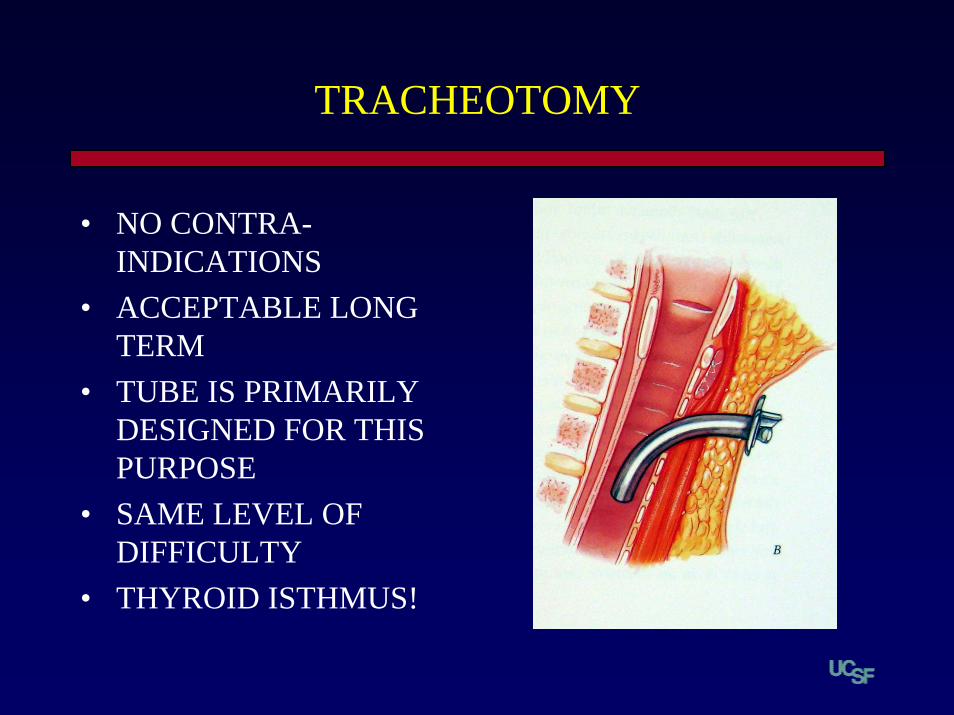
TRACHEOTOMY
• NO CONTRA-INDICATIONS
• ACCEPTABLE LONG TERM
• TUBE IS PRIMARILY DESIGNED FOR THIS PURPOSE
• SAME LEVEL OF DIFFICULTY
• THYROID ISTHMUS!

TRACHEOTOMY TECHNIQUE
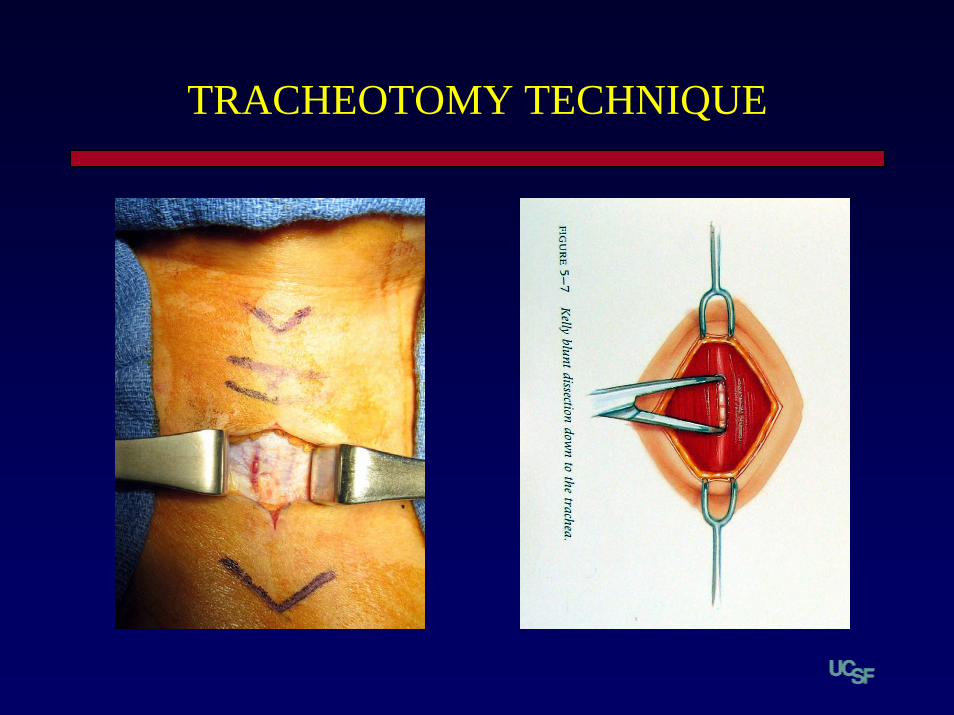
TRACHEOTOMY TECHNIQUE

TRACHEOTOMY TECHNIQUE
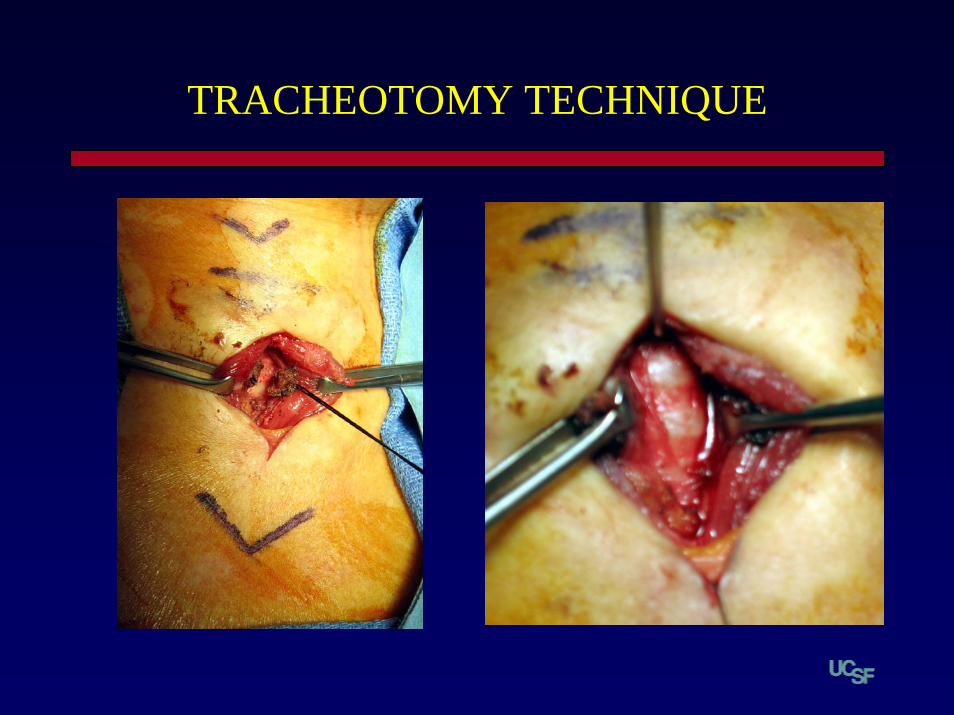
TRACHEOTOMY TECHNIQUE

TRACHEOTOMY TECHNIQUE
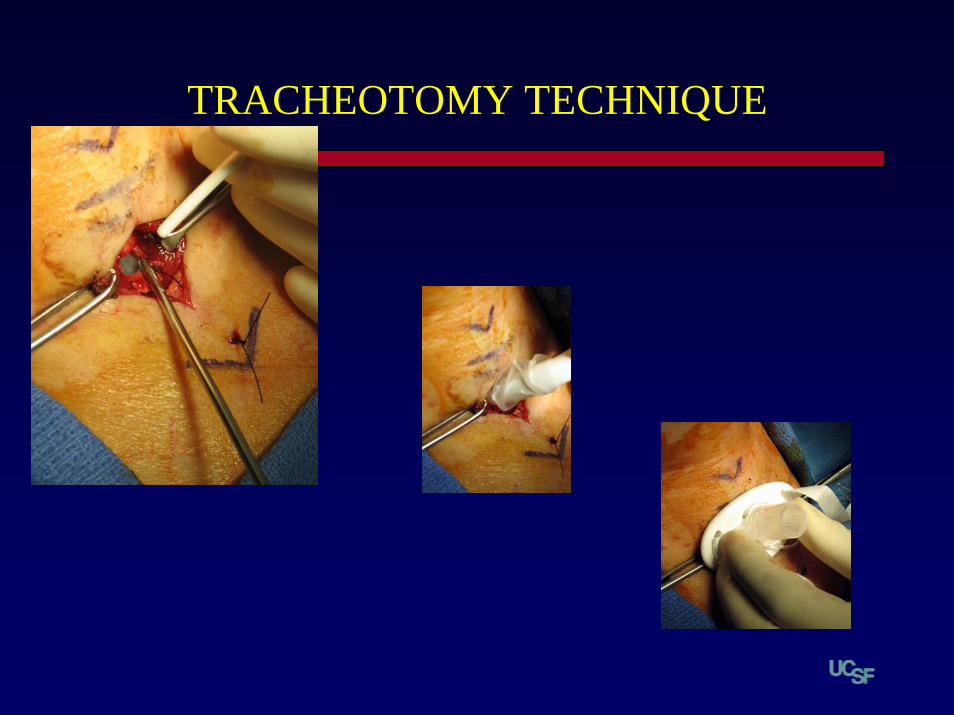
TRACHEOTOMY TECHNIQUE
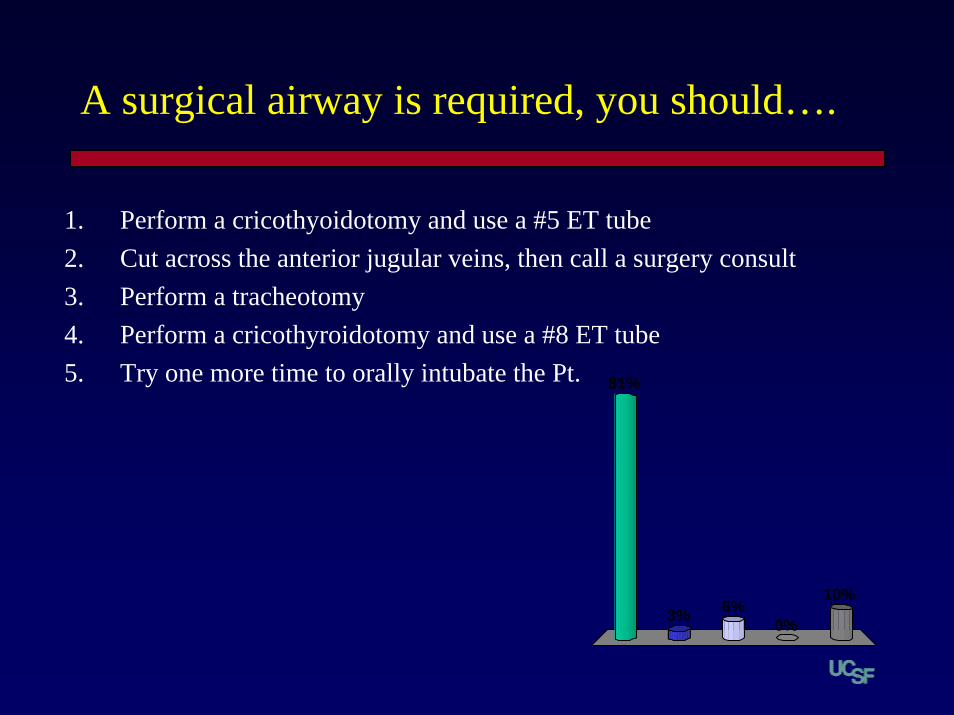
A surgical airway is required, you should….
81%
3%10%
0%6%
1. Perform a cricothyoidotomy and use a #5 ET tube2. Cut across the anterior jugular veins, then call a surgery consult3. Perform a tracheotomy4. Perform a cricothyroidotomy and use a #8 ET tube5. Try one more time to orally intubate the Pt.
Enter question text...
Enter an
swer
text...
100%1. Enter answer text...
NASAL FRACTURES
The Nose
• Prominent facial feature– Direct line of sight
• Can give an impression of one’s personality– Tough guy– Self image– Confidence in appearance
• Ethnic characteristic• Airway!

Epidemiology of Nasal Fracture
• Male 2X female– Sports injury– Assault – Etoh
• 2nd and 3rd decade of life-peak
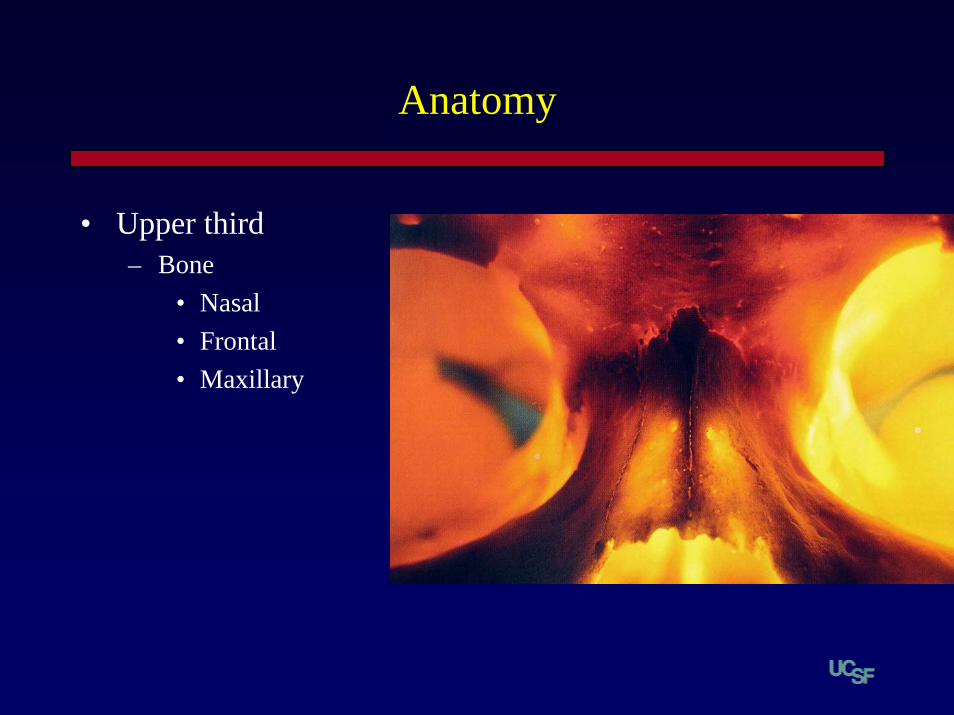
Anatomy
• Upper third– Bone
• Nasal• Frontal• Maxillary
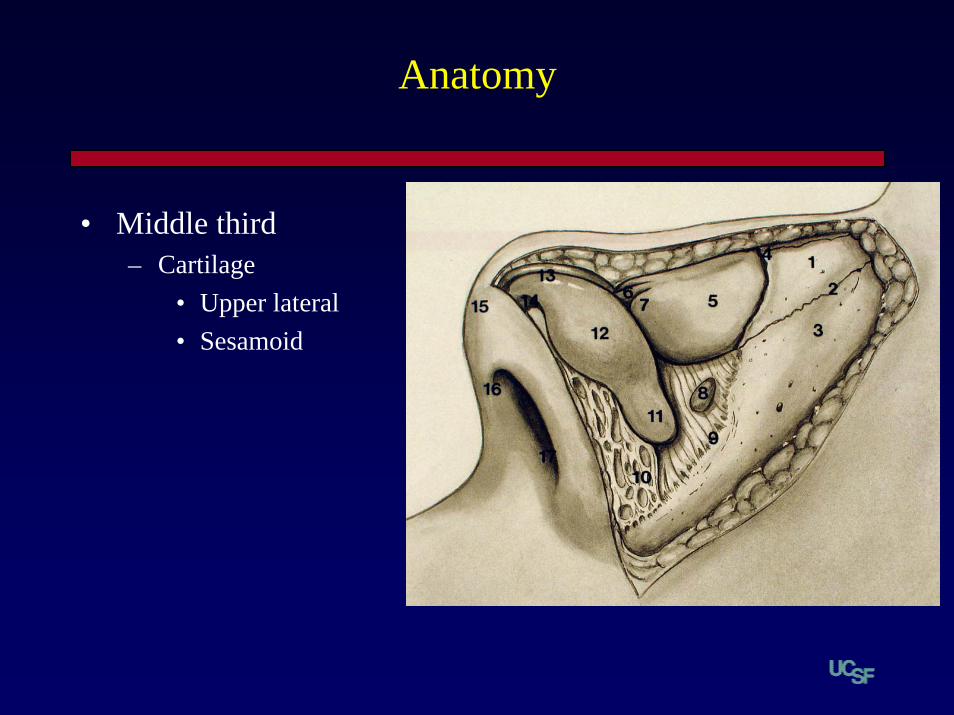
Anatomy
• Middle third– Cartilage
• Upper lateral• Sesamoid
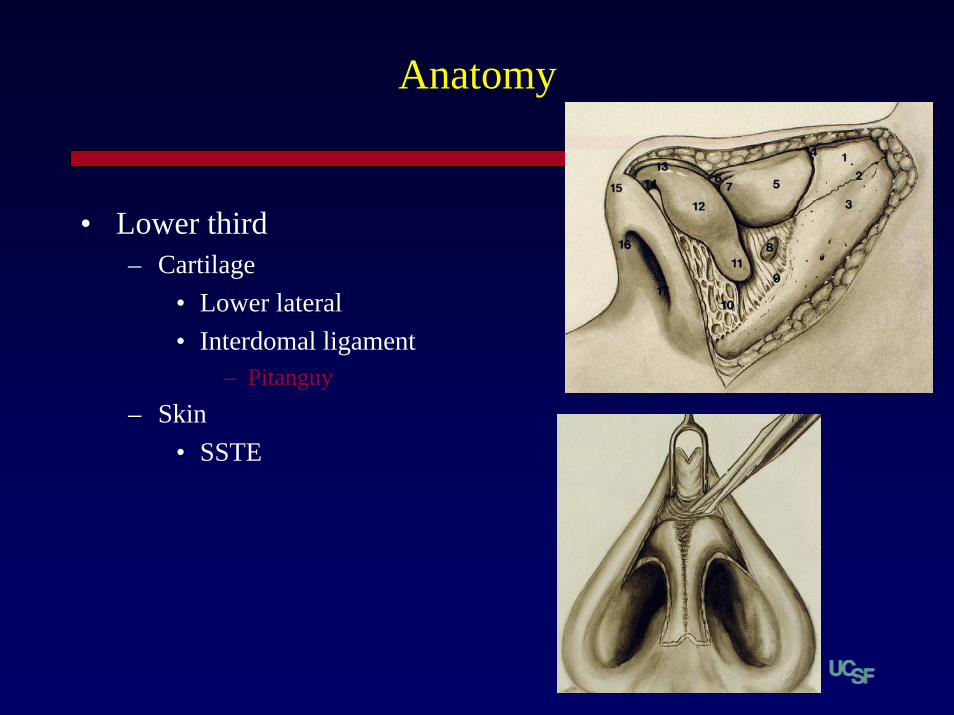
Anatomy
• Lower third– Cartilage
• Lower lateral• Interdomal ligament
– Pitanguy– Skin
• SSTE
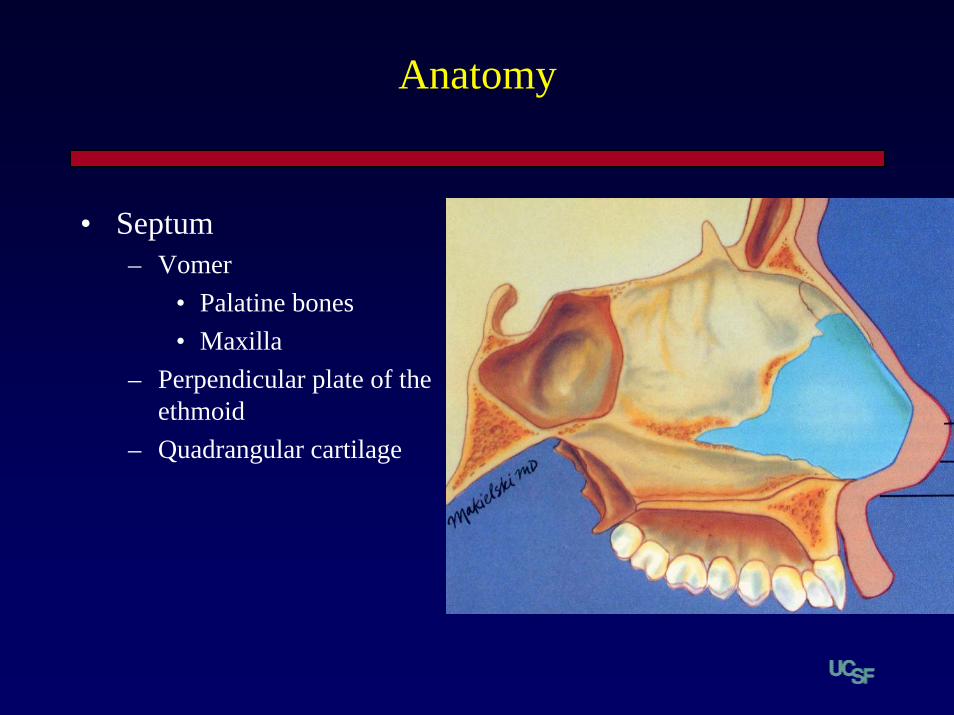
Anatomy
• Septum– Vomer
• Palatine bones• Maxilla
– Perpendicular plate of the ethmoid
– Quadrangular cartilage
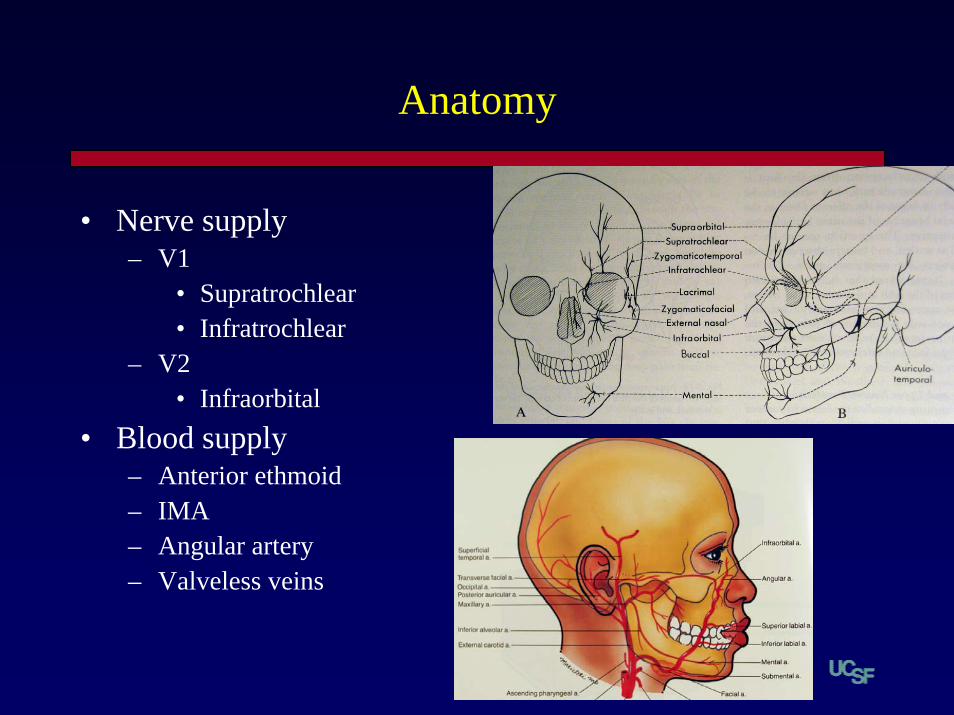
Anatomy
• Nerve supply– V1
• Supratrochlear• Infratrochlear
– V2• Infraorbital
• Blood supply– Anterior ethmoid– IMA– Angular artery– Valveless veins

Fracture Patterns

History
• Time, date, associated factors– MVA
• Restraints, airbags– Assault
• Subpoena- photos• Domestic violence
– 30 – 60% of women with facial trauma
– Substance abuse• Withdrawal issues
History
• Epistaxis– Blood loss- H/H, T&C
• Airway obstruction• Anosmia• Clear rhinorrhea• Numbness
– Incisors• Occlusion• Vision• Past nasal surgical history
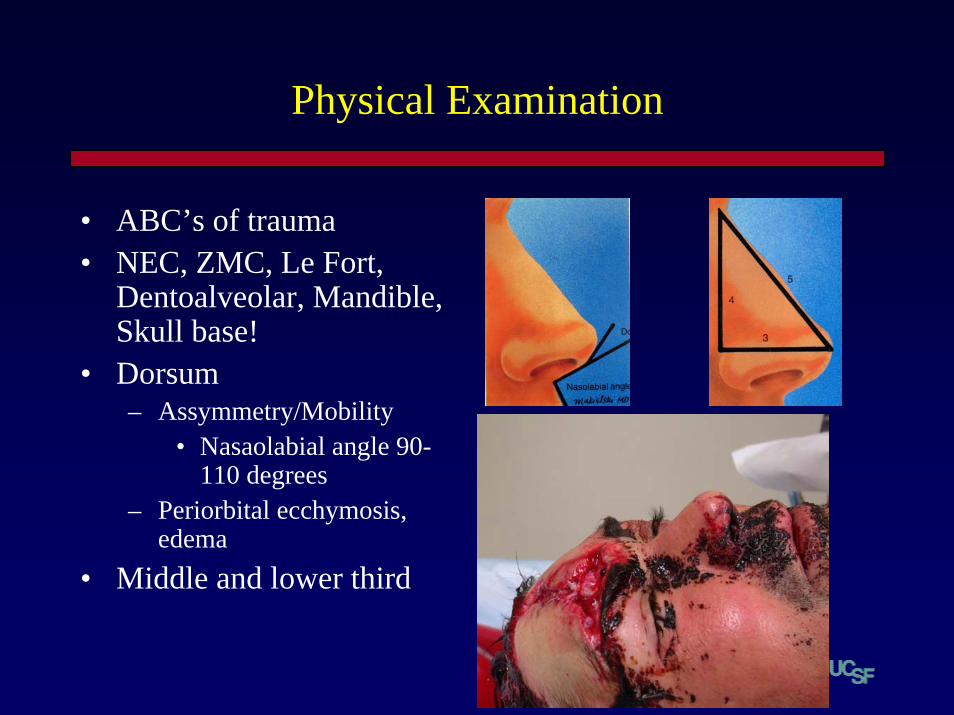
Physical Examination
• ABC’s of trauma• NEC, ZMC, Le Fort,
Dentoalveolar, Mandible, Skull base!
• Dorsum– Assymmetry/Mobility
• Nasaolabial angle 90-110 degrees
– Periorbital ecchymosis, edema
• Middle and lower third

Septal Examination
• Equipment– Suction, speculum,
headlight, vasoconstrictor, anesthetic
– r/o Septal Hematoma
• Internal exam– 30 degree Hopkins rod– Flexible
nasopharyngoscope
• Brown-Gruss analysis– Upper, middle, and lower
thirds
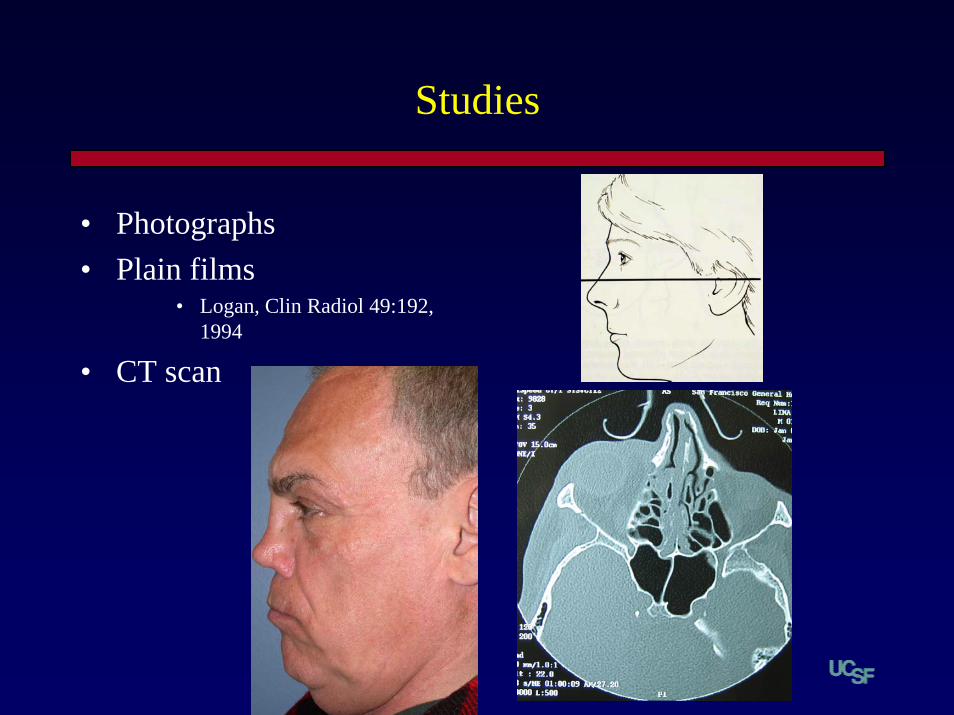
Studies
• Photographs• Plain films
• Logan, Clin Radiol 49:192, 1994
• CT scan
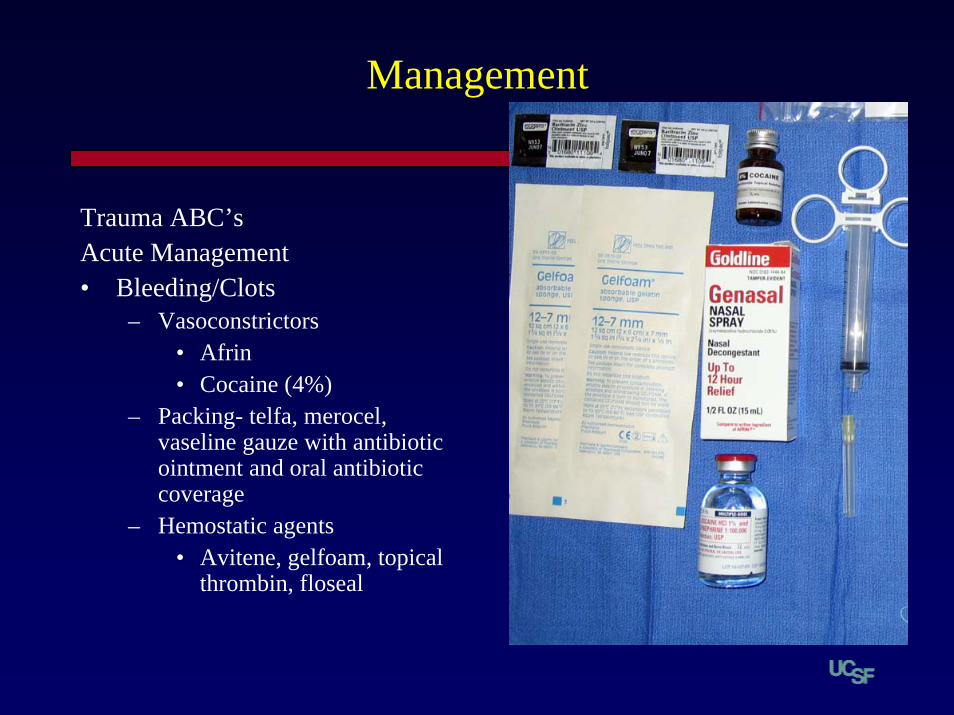
Management
Trauma ABC’sAcute Management• Bleeding/Clots
– Vasoconstrictors• Afrin• Cocaine (4%)
– Packing- telfa, merocel, vaseline gauze with antibiotic ointment and oral antibiotic coverage
– Hemostatic agents• Avitene, gelfoam, topical
thrombin, floseal

Management
• Immediate v. Delayed reduction– Accurate reduction– Patient expectations and
psychology
• Timing of Delayed reduction– 7- 10 Days

Algorithm
Nasal TraumaStabilize
No deformity Deformity NOE
CRNF ORIF
F/UHigh Satisfaction Persisting Issues
NSR v. Open Septorhinoplasty

Sequelae
• Persisting or noticeable nasal deformity
• Nasal obstruction• Synechiae• Septal perforation• Sinusitis• Epiphora
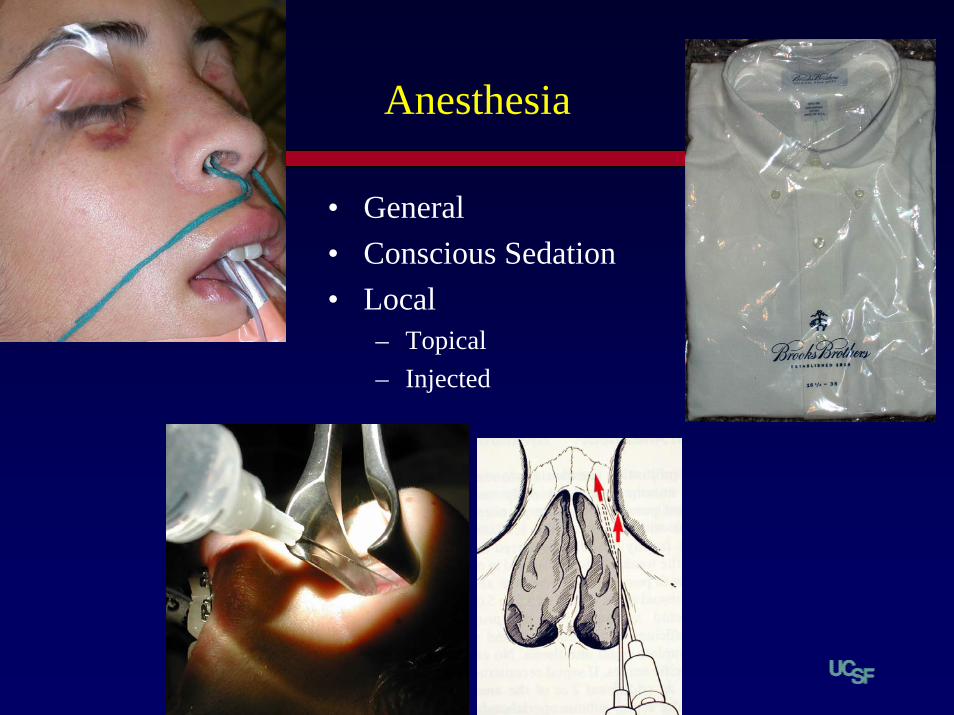
Anesthesia
• General• Conscious Sedation• Local
– Topical– Injected

CRNF
• Office v. O.R.• Tools of the Trade• Technical tips
– Gelfoam roll– Asch forceps– External splint– Telfa
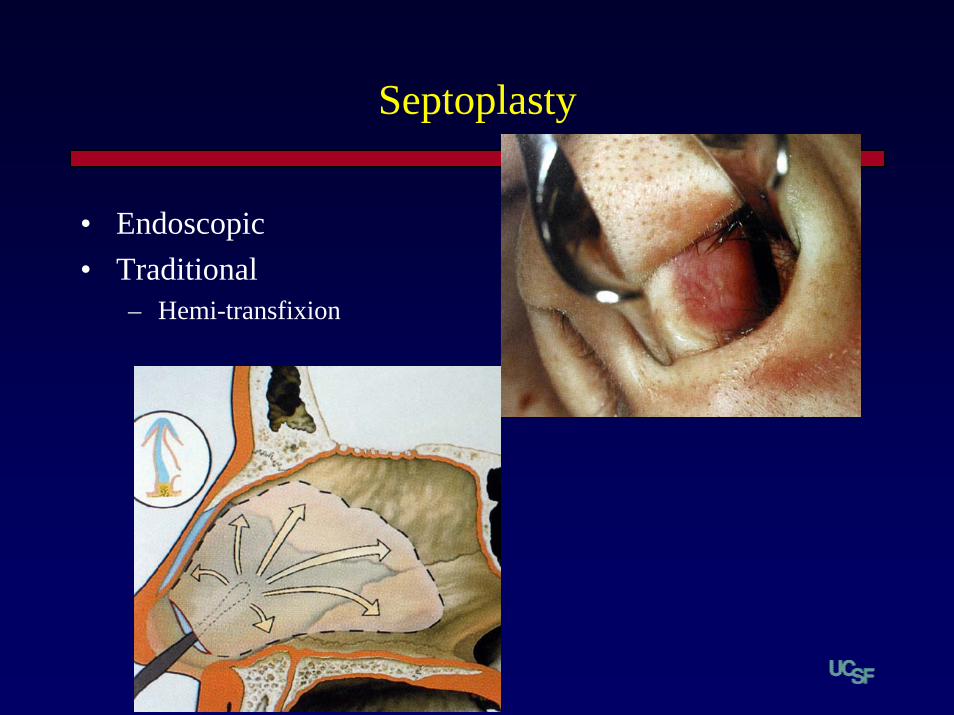
Septoplasty
• Endoscopic• Traditional
– Hemi-transfixion

NSR
Severe septal deviationDorsal deviation• Septoplasty• IC incisions• Deglove• UL separation• +/- osteotomies

Septorhinoplasty
• Extremely severe septaldeformity
• Septal perforation• Severe dorsal
deformity/grafting• Tip work• Open- grafting, tip work

Satisfaction
• 80% of patients will be satisfied with CRNF
• 10% of patients will request revision after Rhinoplasty
• Taking care of nasal trauma skillfully can be the best entre into a cosmetic practice

Nasal Fractures
• Taking care of nasal fractures can be an entre to a cosmetic practice!

Otologic Emergencies
• Otologic conditions the ER staff will torture you with for no apparent reason
• Calls that you can blow off at 3am
Alternate Titles:


When In Doubt
Check It Out

Case 1
• 10 yo Boy
• Slapped on Ear by Older Brother
• Intense ear pain, bleeding from canal, hearing loss
Dr. M. Green


Traumatic TM Perforation
• Conservative Management
• Antibiotic Ear Drops (eg Cipro)
• Dry Ear Precautions
• F/U with Audiogram

Case 2
• US Wrestling Champ
• Lost in a Head Lock
• Swollen, painful Auricle
Dr. Del Amico

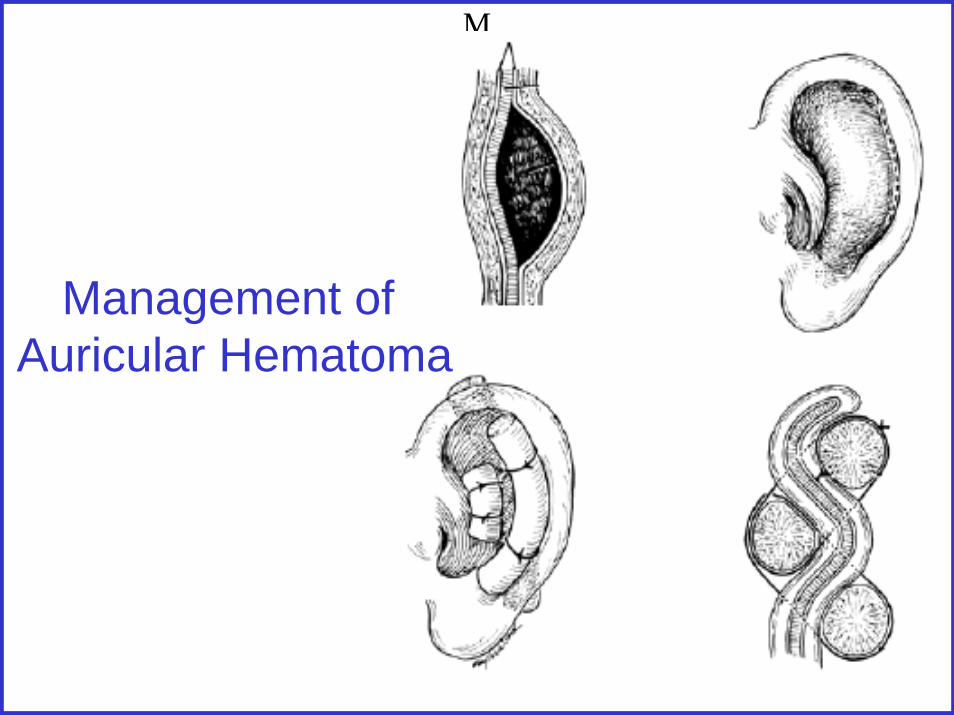
M
Management of Auricular Hematoma
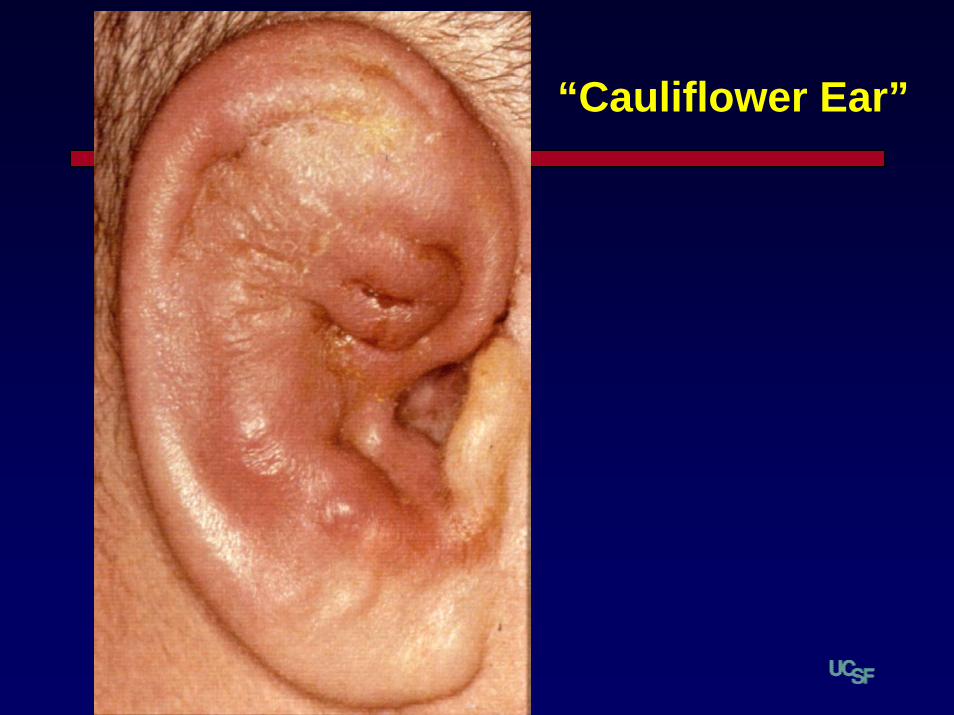
“Cauliflower Ear”

Case 3 • “Standing on a street corner, minding my own business”
• “I swear to God, doc, I didn’t do Nuthin’ to that @#!$$%^& SOB!”
• Assaulated to head w/ Baseball Bat
• Temporary LOC• Headache, bloody otorrhea,
hearing loss
Dr. Doug Ross

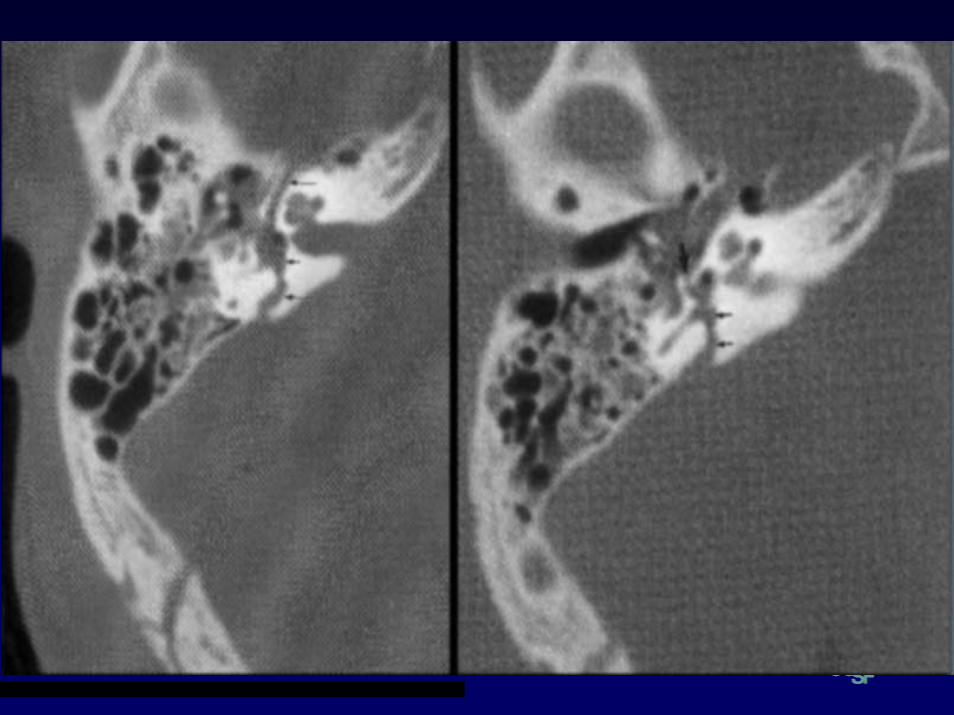
Longitudinal T-Bone Fx
• Common structures involved:– Tympanic Membrane– Roof of Middle Ear– Anterior Petrous Apex– Tympanic portion of FN most common

Case 4 • Next day, also minding own business on same corner, the SOB that hit the first guy is hit himself
• Headache, bloody otorrhea, hearing loss, facial nerve palsy, vertigo

Transverse T-Bone Fx
• Common structures involved:– traverse the otic capsule– May lead to deafness, vertigo, facial nerve palsy
T-Bone Fractures-Evaluation
• ABC’s• CN exam, esp Facial Nerve
– Unconscious pts-painful stimulus elicits grimmace
• Vestibular Eval, Vertigo (nystagmus?)• Hearing-Tuning Fork in ER• EAC Eval (usually bloody)• Otic Capsule “sparing” or “involvement”

T-Bone Fx’s-Evaluaton
• Radiology: CT > MRI• Audiogram• Vestibular Studies• FN Studies:
– Evoked EMG-– Direct Stimulation-MST-(Hilger nerve stim)

Indications for Surgical Intervention:– CSF Leak– Persistent PLF– Ossicular Disruption (late)– Non-healing TM Perf (late)– Secondary Cholesteatoma (late): Skin
implosion or canal stenosis
T-Bone Fx’s-Treatment
T-Bone Fx-Facial Nerve Surgery
Indications for Surgical Inervention:
Absolute
Immed FN Paralysis w/ radiograph evidence
Relative
Evoked EMG >95% degeneraton
No recovery after 4-12 months
Case 5
• 8 yo Boy fell while running around with Q-tip in ear
• Pain, Hearing Loss, bloody otorrhea
Nurse Hathaway



Traumatic Ossicular Fracture


Case 6
• Scuba Diver• Had cold but went diving
anyway…• Intense pressure, pain on
descent• Now he is very dizzy and
cannot hear out one ear, and has an intense ringing.
Dr. Carter

Inner Ear Barotrauma
• “Alternobaric” Trauma– Transient vestib/auditory dysfunction
• “Barotrauma”– Extreme fluctuations in ME pressure, causing
labyrinthine concussion, membrane tears, oval or round window fisutae
• “Decompression Sickness”-the bends

Barotrauma-Treatment
• Bed Rest• Head elevation• Close monitoring of hearing and balance• Steroids?• Surgery for progressive HL or perisitent vertigo >
5 days• Avoid diving at least 3 months, forever if
permanent damage has resulted

Decompression Sickness
• Usually dives > 100 m• Formation of gas bubbles in body• Joint Pains and CNS findings present• Permanent auditory/vestibular injury• Rx-IMMEDIATE Recompression

Case 7
• 40 yo Woman• 3 Days s/p Cholesteatoma surgery
@ outside hosp.• Fevers, Headache, myalgias, ear
pain• Otorrhea
Dr. Benton

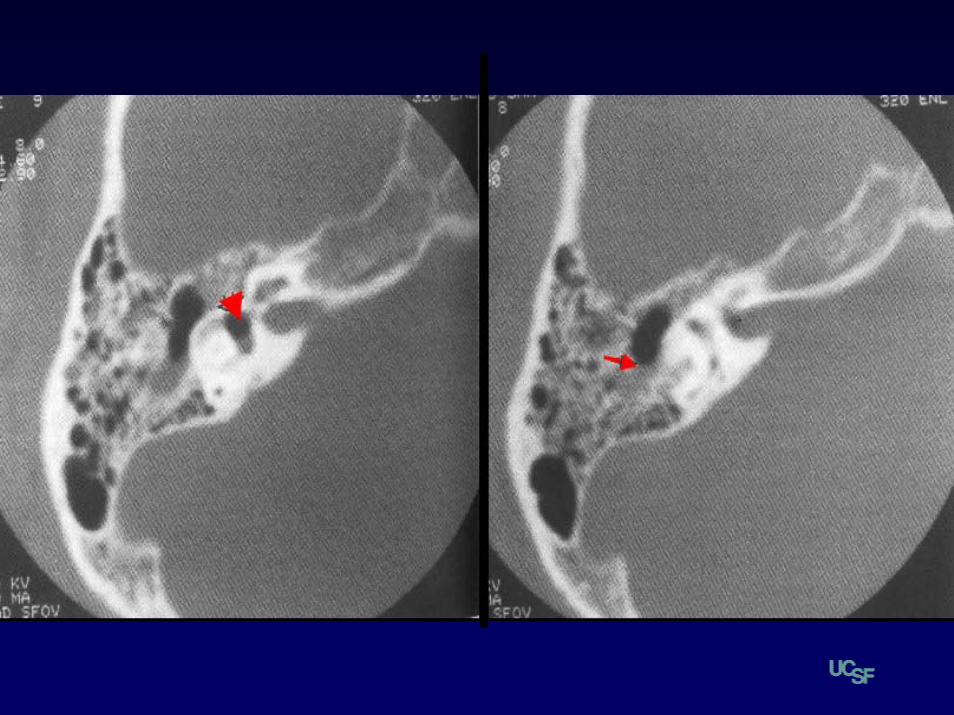
CSF Otorrhea
• Non-traumatic: Tumors, Congenital, Osteo• Traumatic: Trauma vs Surgical
• Dx:– “Halo” Sign, Glucose > 30mg/ml, ß-transferrin– CT-Metrizamide Scan, flourescein, MRI
CSF Otorrhea-Management
• Depends on location & etiology of leak• Decrease CSF Pressure
– Bed rest, HOB elevation, laxatives, diuretics, avoidance of noise-blowing, lifting, etc…
– Serial LP’s vs lumbar drain
• Surgery– Closure of dural defect, closure of bony defect
Case 8
• 38 yo Woman• 1 day h/o inability to
move R side of face• Otalgia
Dr. Weaver


Facial Palsy-DDX
• Polyneuritis-– Bells, HZV, GB, Autoimm, Lyme, HIV, Kawasaki
• Trauma-– TB Fx, Barotrauma, Birth trauma
• Otitis Media- AOM, COM, Chole• Sarcoid• Melkersson-Rosenthal• Neurologic - HIV, CVA• Malignancy - parotid, metastatic• Benign Tumors - schwannoma, glomus
“Bell’s” Palsy
• Dx of Exclusion• Probable viral • Hyperacusis in 30%• MRI-when no recovery in 12 weeks• Rx-Steroids, ?antivirals, • Surgical decompression-controversial• Outcome-if incomplete: 95-100% recover


Herpes Zoster OticusAKA: Ramsay Hunt
Syndrome
Case 9• Screaming 4 year
old• Painful Right Ear• Cochroach in canal
How do I get those ENTresidents to
NOTICE me?!?



Case 10• Screaming 5 year
old• Painful Right Ear• Fevers



Coalescent Mastoiditis + SS Thrombosis
• Emergent mastoidectomy• Myringotomy + Tube• IV Antibiotics
• Controversial: anticoagulation

Dr. Kovak
•65 year old man•Insulin Dependent Diabetic•Chronic external OE•Facial Nerve Palsy x 2 weeks
Case 11

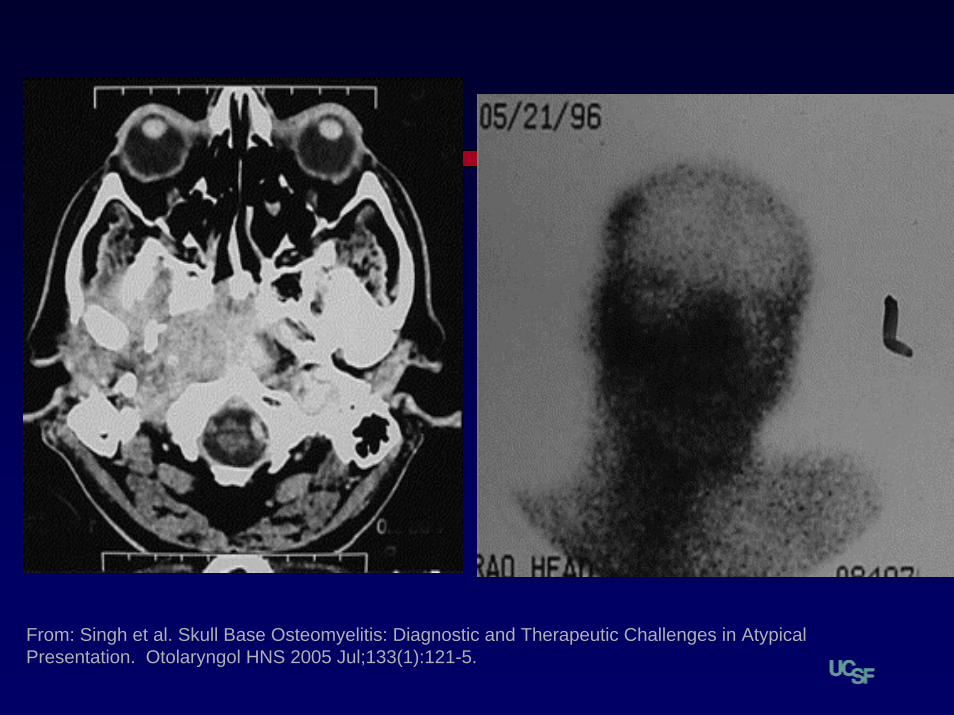
From: Singh et al. Skull Base Osteomyelitis: Diagnostic and Therapeutic Challenges in Atypical Presentation. Otolaryngol HNS 2005 Jul;133(1):121-5.
Malignant Otitis Externa / Skull Base Osteomyelitis
• Immunocompromised or Diabetics• Dx = CT, MRI, Bone Scans• Follow resolution with
– Technetium scans = osteoblastic activity– Gallium 67 scans = granulocytic activity
• 6-8 weeks of IV antipseudomonal ABx
• Controversial: surgical debridement

Pt presents with ear trauma and TM perforation. You should…
3%
11%
22%
2%
62%
1. A. insist that the ENT on call come in immediately to operate on the Pt.
2. B. Reassure the Pt, make an appt to see the ENT in 1 week.3. C. Reassure the Pt. make an appt to see the ENT in 1 week with an
audiogram4. D.Place a hot poker in the ear canal5. E. Obtain a CT scan
Conclusion