non-motor symptoms of parkinson’s disease · obstructive sleep apnea (osa) •~40% pd patients...
TRANSCRIPT
NON-MOTOR SYMPTOMS OF PARKINSON’S DISEASECHRISTINA L. VAUGHAN, MD, MHS
ASSISTANT PROFESSOR OF NEUROLOGY, UNIVERSITY OF COLORADO, ANSCHUTZ MEDICAL CAMPUS
OCTOBER 6, 2018
GOALS
• To provide a comprehensive overview of key non-motor
features of PD
• To provide practical tips regarding management of some
non-motor symptoms
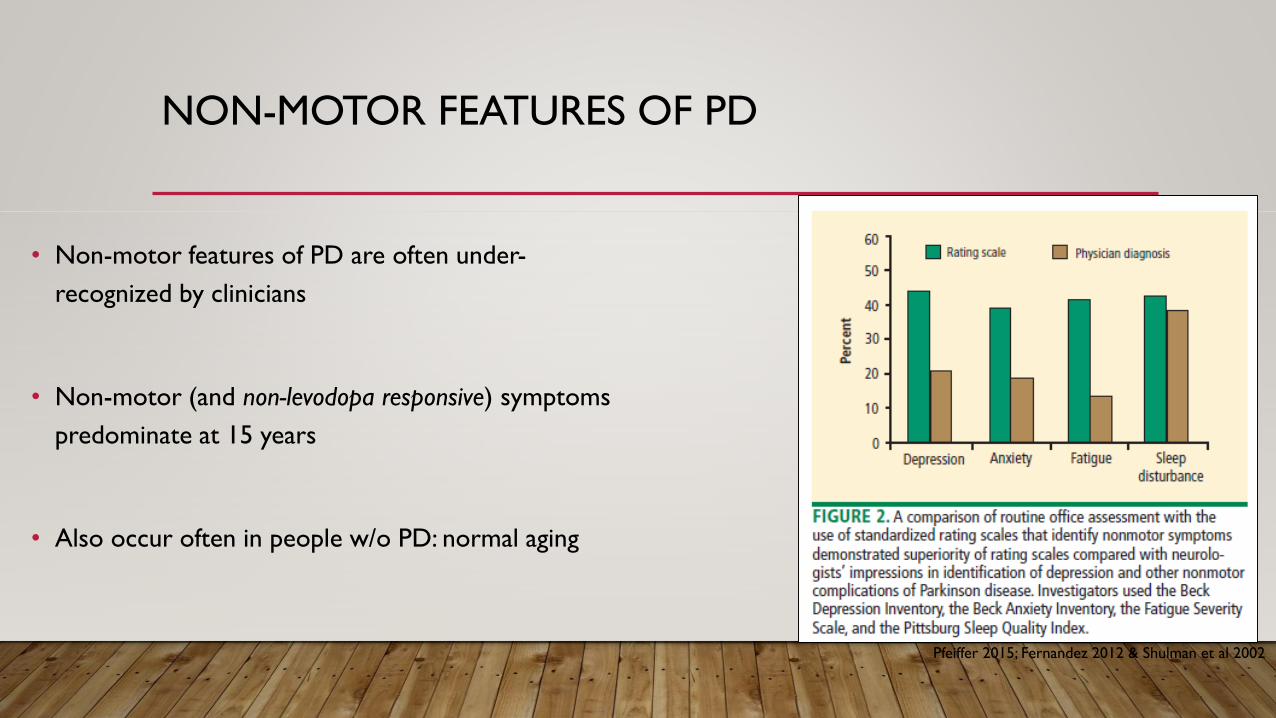
NON-MOTOR FEATURES OF PD
• Non-motor features of PD are often under-
recognized by clinicians
• Non-motor (and non-levodopa responsive) symptoms
predominate at 15 years
• Also occur often in people w/o PD: normal aging
Pfeiffer 2015; Fernandez 2012 & Shulman et al 2002
LOST SENSE OF SMELL
• most common pre-motor symptom
• ~85% early PD
• can precede onset of motor symptoms
by years
• multifactorial
• also common in Alzheimer’s and Lewy
Body Disease
• disease may start in GI tract and/or
olfactory bulb
LOST SENSE OF SMELL: PRACTICAL
• No treatments for lost sense of smell
• Reduced ability to smell might affect your appetite, since taste is linked to smell
1. Adequate provision of fire and/or smoke alarms
2. Specific food and nutritional advice if you also have a reduced taste sensation
3. Labels to ensure food safety as you may not be able to smell degraded food
SLEEP DISORDERS
• ~90%
• ↑ with advanced PD
• Most common sleep complaints:
• Difficulty falling and staying asleep
• Sleep fragmentation*
• Excessive daytime sleepiness
• Talking or yelling out while asleep
• Vivid dreaming
• Leg movements, jerking, cramping
• Difficulty turning over in bed
• Waking up to go to the bathroom
SLEEP DISORDERS: EXCESSIVE DAYTIME SLEEPINESS
• 30-50% of patients with PD
• Common causes:
• Poor night’s sleep
• Dopaminergic medications, especially dopamine agonists:
• Mirapex (pramipexole)
• Requip (ropinirole)
• Neupro patch (rotigotine)
• Apokyn (apomorphine)
SLEEP DISORDERS:EXCESSIVE DAYTIME SLEEPINESS: PRACTICAL
Do not drive while sleepy.
1. Good sleep hygiene, includes a set bedtime and wake-up time.
2. Exposure to adequate light during the day and darkness at night.
3. Avoid sedentary activities during the day.
4. Participate in activities outside the home, as they may be helpful in providing stimulation to prevent
daytime dozing.
5. Get physical exercise appropriate to your level of functioning, which may also promote daytime
wakefulness.
6. Strenuous exercise, however, should be avoided for 3 - 4 hrs before sleep.
7. If you are on a dopamine agonist and you experience daytime sleepiness or sleep attacks talk to your
doctor about possibly decreasing the dose.
http://www.parkinson.org
SLEEP DISORDERS: NIGHT
• Obstructive sleep apnea (OSA)
• Restless legs syndrome (RLS)
• REM sleep behavior disorder (RBD)
• Sleep fragmentation
• Patients may have a combination of a few sleep problems
http://www.parkinson.org
SLEEP DISORDERS:OBSTRUCTIVE SLEEP APNEA (OSA)
• ~40% PD patients
• Loud snoring
• Restless sleep
• Sleepiness during the daytime
• Pauses in breathing during night sleep
• Diagnose: sleep study
• Treat: Continuous positive airway
pressure (CPAP)
• Associated with many bad health
consequences:
• stroke
• high blood pressure
• heart arrhythmias
• heart attack
• insulin resistance
• depression
• worsening cognition
SLEEP DISORDERS:RESTLESS LEGS SYNDROME (RLS)
• Irresistible urge to move the legs, which interferes with rest
and sleep
• Usually at night, or sometimes daytime when sitting for long
periods
• Creeping, crawling, aching, pulling, searing, tingling, bubbling
• Sometimes also in upper leg, feet, or arms
• 5 -15% of adults; ~2x as likely in PD
SLEEP DISORDERS: RLS
• Treatment:
• Iron replacement (in those
who are deficient)
• Pramipexole (Mirapex)
• Ropinirole (Requip)
• Rotigotine (Neupro)
• Gabapentin (Neurontin)
• (Pain medication)
SLEEP DISORDERS:REM SLEEP BEHAVIOR DISORDER (RBD)
• ~ 50% PD patients
• = continued ability to move
during REM sleep
• “thrashing about” in sleep or “acting
out” of dreams
• often precedes the PD diagnosis
by 5-10 years
• people with RBD may have 80-
90% risk of later developing PD
• Treat:
• clonazepam (effective in 75-
90%)
• melatonin may help
SLEEP DISORDERS:FRAGMENTATION
• interrupted sleep
• significantly less time spent in slow-wave
and REM sleep (the deepest and most
restorative phases of sleep)
• may worsen daytime sleepiness and
predispose to later hallucinations
• Treatment:
• Clonazepam
• tends to help regulate sleep and allow
for a more normal nighttime sleeping
pattern
• adjust anti-PD drugs
• daytime stimulant (ex: Provigil, Ritalin)
• treat nighttime urinary frequency
MOOD DISORDERS
• maintaining emotional health is essential to your physical health
• stress can make PD symptoms worse
• depression and anxiety affect up to 50% of people living with PD
• mood changes can bring on worsening function, leading to a decreased
quality of life
MOOD DISORDERS: DEPRESSION
• can pre-date other signs
• highly treatable
• Risk factors
• Older age
• Female
• Personal history of depression
• Family history of depression
• Other medical disease(s)
• Severity of PD symptoms
Joseph Hirsch, Lunch Hour (1942)
MOOD DISORDERS: DEPRESSION
• Often present:
• Prominent anxiety
• Dysphoria (low mood)
• Pessimism
• Somatic/physical symptoms
• Less often present:
• Guilt
• Self-blame
• Suicide (low rate despite high
frequency of ideation)
• Delusions/hallucinations
• Especially in advanced PD, it can be
difficult to distinguish between
physical symptoms of depression and
those of PD:
– such as slowness of movement
and thinking, loss of appetite and
weight, or sleep problems

MOOD DISORDERS: DEPRESSION: PRACTICAL
• Treatment is personalized, multidimensional
• Determine whether the symptoms occur only during OFF periods
• Adjust anti-PD medication accordingly
• Assess severity:
• If mild, consider counseling, patient education, or cognitive-behavioral therapy (CBT)
• If moderate-severe, consider:
• Psychotropic medication
• Dopaminergic medication
• Electroconvulsive therapy (ECT)
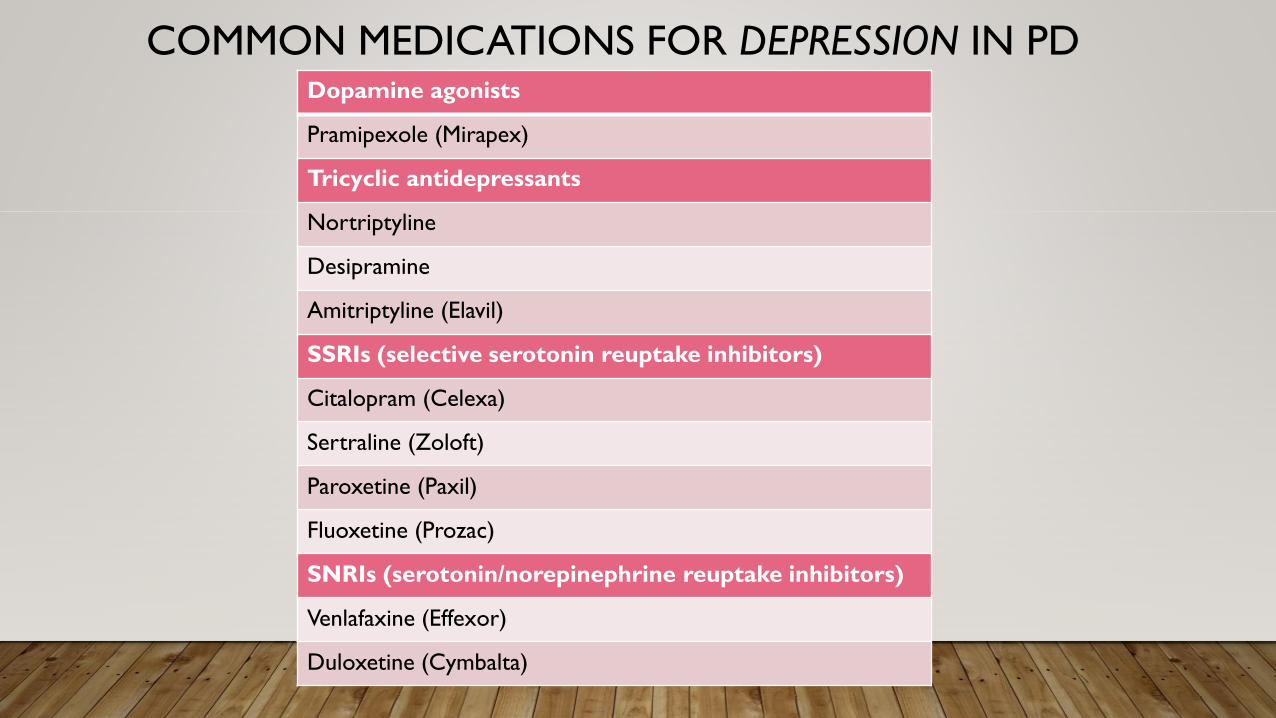
Dopamine agonists
Pramipexole (Mirapex)
Tricyclic antidepressants
Nortriptyline
Desipramine
Amitriptyline (Elavil)
SSRIs (selective serotonin reuptake inhibitors)
Citalopram (Celexa)
Sertraline (Zoloft)
Paroxetine (Paxil)
Fluoxetine (Prozac)
SNRIs (serotonin/norepinephrine reuptake inhibitors)
Venlafaxine (Effexor)
Duloxetine (Cymbalta)
COMMON MEDICATIONS FOR DEPRESSION IN PD
MOOD DISORDERS: ANXIETY
• Panic attacks (often during OFF-periods), generalized anxiety disorder, simple and social
phobias, obsessive-compulsive disorder (OCD)
• Associated with subjective motor symptoms, freezing, more severe gait problems, and
dyskinesiasRelated to anxiety, there is
some evidence of a PD
personality:
lower novelty seeking and
higher harm avoidance; less risky
behavior
MOOD DISORDERS: ANXIETY
• Risk factors:
• Female sex
• Previous history of anxiety disorders
• +/- younger age
• Severity (not duration) of PD
• No tremor > tremor-predominant
• Common fears with anxiety in PD:
• fear of being unable to function,
particularly during a sudden OFF period
• sometimes leads to a need to be with
someone at all times and a fear of being
left alone
• being embarrassed—often related to
having people notice symptoms of PD in
public
MOOD DISORDERS: ANXIETY: PRACTICAL
1. Exercise
2. All basic forms of physical activity can help:
walking, stretching, yoga, tai-chi, dance, etc.
3. Relaxation techniques
4. Massage therapy
5. Acupuncture
6. Aromatherapy
7. Meditation
8. Music therapy
• Newer antidepressants such as SSRIs typically
tried first
• Benzodiazepines (with caution!)
• diazepam (Valium)
• lorazepam (Ativan)
• clonazepam (Klonopin)
• alprazolam (Xanax)
• can cause: memory difficulties, confusion,
increase in balance problems and tiredness
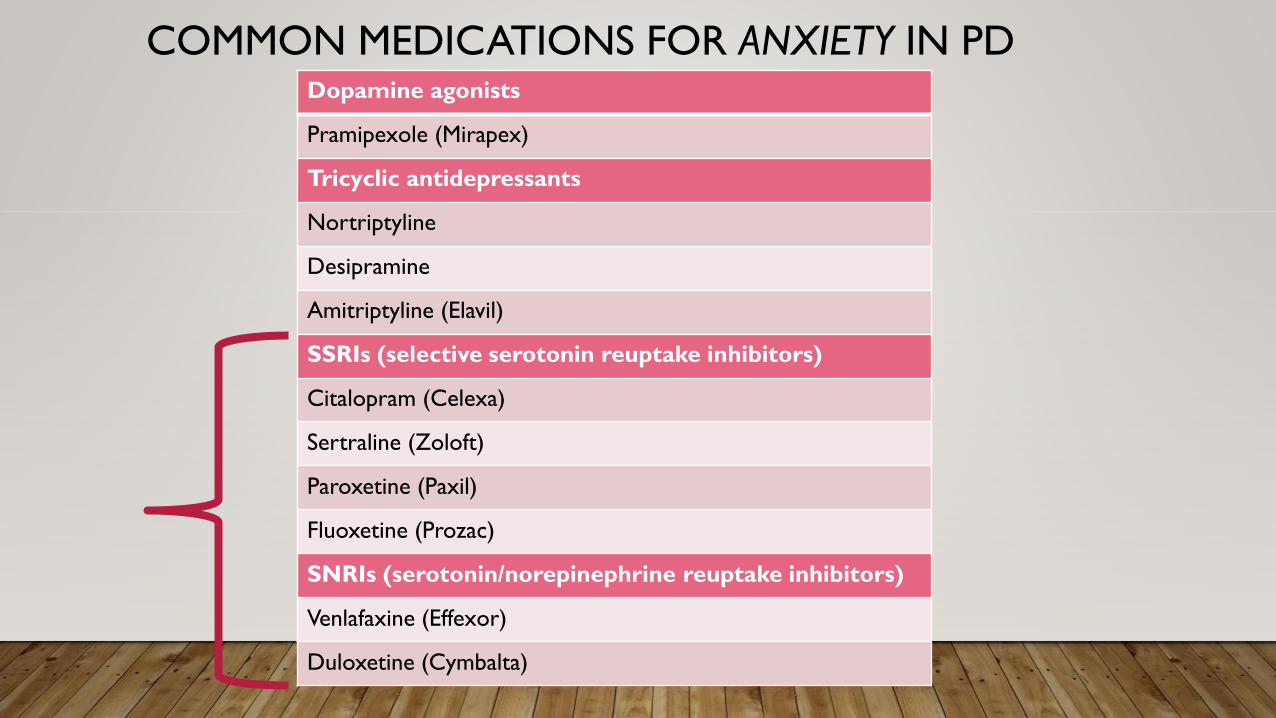
Dopamine agonists
Pramipexole (Mirapex)
Tricyclic antidepressants
Nortriptyline
Desipramine
Amitriptyline (Elavil)
SSRIs (selective serotonin reuptake inhibitors)
Citalopram (Celexa)
Sertraline (Zoloft)
Paroxetine (Paxil)
Fluoxetine (Prozac)
SNRIs (serotonin/norepinephrine reuptake inhibitors)
Venlafaxine (Effexor)
Duloxetine (Cymbalta)
COMMON MEDICATIONS FOR ANXIETY IN PD
MOOD DISORDERS: APATHY/AMOTIVATION
• general lack of motivation and interest,
dampening of emotional expression
• prevalence up to ~40%
• can be misinterpreted as laziness, poor
initiative or depression
• not explained by cognitive impairment,
emotional distress, or decreased
consciousness
• higher risk: older age, severe motor
impairment
• Can cause:
• less physical activity (which can
worsen already impaired mobility)
• fewer social interactions (which
could lead to depressive
symptoms)
• poorer adherence to medication
regimens
MOOD DISORDERS: APATHY/AMOTIVATION: PRACTICAL
1. Maintain a regular sleep and wake
schedule
2. Create a schedule that incorporates
physical, social and cognitive (memory
and thinking) activities. List what you
will do each day and at what time
3. Set personal goals
4. Exercise
• Possible treatments:
• dopamine agonists
• rivastigmine (Exelon)
• memantine (Namenda)
• mood medication
• stimulants
• Cognitive behavioral therapy
FATIGUE
• a feeling of deep tiredness that does not
improve with rest
• may predate onset of motor symptoms
• single most disabling symptom for up to
1/3 PD patients
• associated frequently with depression,
cognitive deficits, and daytime sleepiness
FATIGUE: PRACTICAL
1. Eat well.
2. Stay hydrated.
3. Exercise. Fatigue may make it hard to start exercising, but it may make you feel more energetic
afterward. If you find it difficult to get going, consider exercising with another person or a group.
4. Keep a regular sleep schedule.
5. Take a short nap (10-30 minutes) after lunch. Avoid frequent naps or napping after 3:00 p.m.
6. Stay socially connected.
7. Pace yourself: plan your day so that you are active at times when you feel most energetic and have a
chance to rest when you need to.
8. Do something fun: visit with an upbeat friend or pursue a hobby.
9. At work, take regular short breaks.http://www.parkinson.org
FATIGUE: PRACTICAL
• Adjusting PD medications
• Possible treatments: stimulant (low dose), levodopa, dopamine agonists
• Investigate for other causes (ex: anemia, hypothyroidism, nutritional deficiencies)
CONSTIPATION
• Fewer than 3 bowel movements/week
• Can predate motor symptoms – by years
• Up to 60% in PD patients compared to 6-33% in controls
• Contributes to symptoms: nausea, bloating, feeling full, and weight loss
• Contributes to irregular absorption of medications motor fluctuations
• PD medications can contribute to constipation
CONSTIPATION: PRACTICAL
1. Eat a well-balanced diet with plenty of fiber. Good sources of fiber include fruits, vegetables, legumes,
bran, and whole grain bread.
2. Drink 48 to 64 ounces of water each day.
3. Exercise daily.
4. Drink warm liquids, especially in the morning. Consider warming your prune juice instead of drinking
it cold.
5. Add fruits and vegetables to your diet.
6. Eat prunes and/or bran cereal.
7. If needed, use a very mild laxative or stool softener.
CONSTIPATION: PRACTICAL
• Senna/Senokot
• Stool softener(s)
• Polyethylene glycol electrolyte solution
(Miralax)
• Enemas
• Note: bulking agents like Metamucil may
make it worse (“cement block”)
• Recipe 1:
• Equal parts bran cereal, applesauce, and
prune juice (example: 1 cup of each)
• Mix into a container with a lid; store in
the refrigerator
• Eat two tablespoons a day (preferable
the same time each day)
• Recipe II:
• Yakima Fruit paste, 1 Tb/day

OVERVIEW OF NON-MOTOR SYMPTOMS
EARLIER SYMPTOMS
• ↓Taste/sense of smell
• Sleep disorders
• Mood disorders
• Fatigue
• Constipation
The importance
of EXERCISE!
WHAT DO MOST HAVE IN COMMON?
COGNITIVE CHANGES
• Mild cognitive impairment ~25% in early
PD
• Dementia ~80% for those with >20 yrs of
PD
• while approximately 50 percent of people with
PD will experience some form of cognitive
impairment, not all lead to dementia
• Note: if dementia precedes parkinsonism,
consider Lewy Body Disease
COGNITIVE CHANGES
• Executive dysfunction: problem solving, making plans, formulating goals, anticipating
consequences
• Attention difficulties
• Slowed thinking
• Word-finding trouble
• Difficulty learning and remembering information
• Visuospatial trouble: where things are in space
COGNITIVE CHANGES: DEMENTIA
• Not a specific disease
• An overall term: wide range of symptoms
associated with ↓memory or other
thinking skills severe enough to reduce a
person's ability to perform everyday
activities
• Progressive
• Multiple types: Alzheimer’s (60-80%),
Parkinson’s-type, vascular,
frontotemporal,…
• At least 2 are impaired with
dementia:
1. Memory
2. Communication and language
3. Ability to focus and pay attention
4. Reasoning and judgment
5. Visual perception
http://www.alz.org/what-is-dementia.asp
COGNITIVE CHANGES
• Risk factors for PD Dementia
• Age
• Motor severity
• Older age at PD onset
• Longer PD duration
• No tremor > tremor
• Hallucinations
• Depression +/-
• Genetic forms of PD +/-
COGNITIVE CHANGES
• Treatment
• Exclude other medical causes of
cognitive problems, especially if sudden
onset
• Address safety and care-giver issues
• Driving evaluations
• Cognitive remediation therapy
• alternative ways to compensate for
memory or thinking problems
• Cholinesterase inhibitors:
1. donepezil (Aricept)
2. galantamine (Razadyne)
3. rivastigmine (Exelon)*
• NMDA antagonists:
1. memantine (Namenda)
COGNITIVE CHANGES: PRACTICAL
• Offer help only when asked.
• Prompt the person — for example, instead of asking, “Did anyone call?” ask, “Did Linda call?”
• Say the name of the person and make eye contact when speaking to gain and hold attention.
• Put reminder notes and lists in a prominent place.
• Keep things in routine places.
• To ensure medications are taken on time, provide a dispenser, perhaps with a built-in alarm.
• Use photos on cell phone contact entries to prompt face-name association.
• If the person is searching for a word, provide a cue, such as, “the word you are looking for probably begins with ‘d’.”
• Do not finish the sentences of a person who needs more time to put them together.
• When presenting the person with a list of actions, first verbalize them, then write them down.
• Ask questions to moderate the conversation pace and allow catch up and reinforcement.
http://www.parkinson.org
COGNITIVE CHANGES: PRACTICAL
• Get adequate rest
• Eat a healthy diet
• A Mediterranean diet, for example, has been associated with improved cognitive function
• Do not multitask
• Focus on your abilities
• Introduce novelty - learn something new
• Exercise
• SOCIALIZE!
• Stay busy and fill your schedule
http://www.pdf.org/pdf/slides_pdexpertbriefing_cognition15_111015.pdf
COGNITIVE CHANGES: PRACTICAL
• An active and socially integrated lifestyle in late life might protect against dementia
• Incidence and progression of dementia increases with isolation
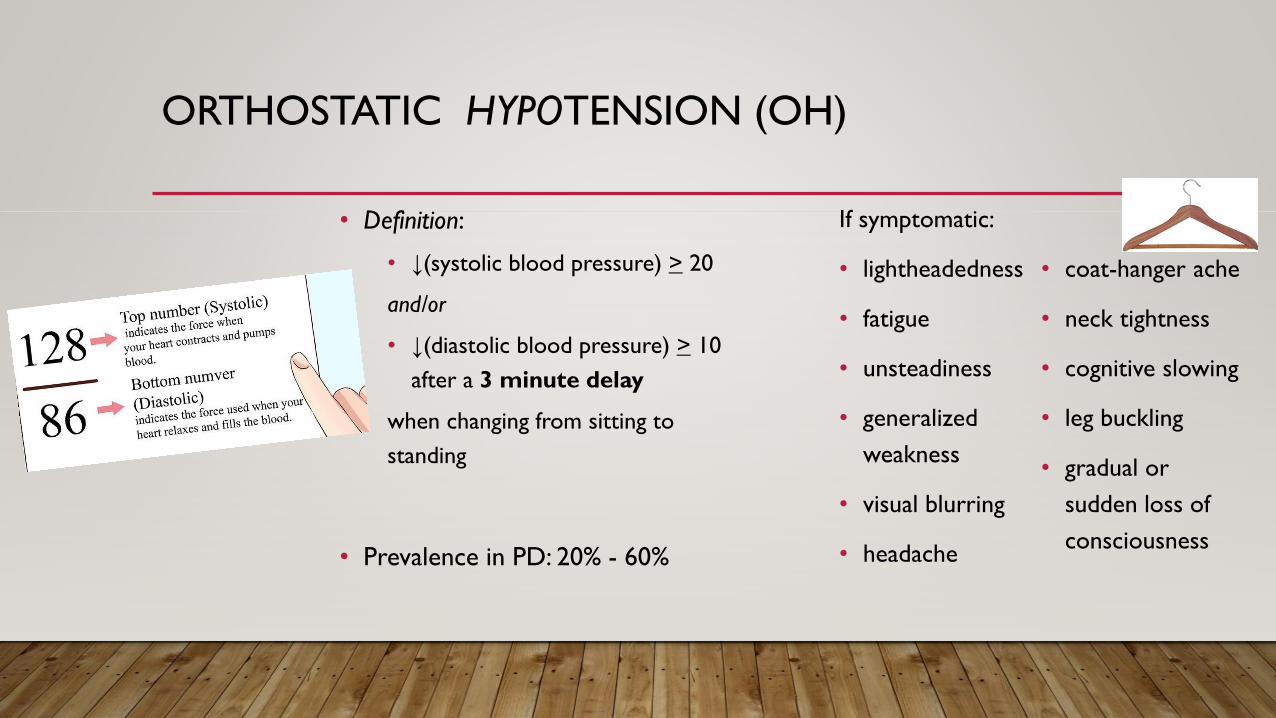
ORTHOSTATIC HYPOTENSION (OH)
If symptomatic:
• lightheadedness
• fatigue
• unsteadiness
• generalized
weakness
• visual blurring
• headache
• coat-hanger ache
• neck tightness
• cognitive slowing
• leg buckling
• gradual or
sudden loss of
consciousness
• Definition:
• ↓(systolic blood pressure) > 20
and/or
• ↓(diastolic blood pressure) > 10
after a 3 minute delay
when changing from sitting to
standing
• Prevalence in PD: 20% - 60%
ORTHOSTATIC HYPOTENSION
• Associated with:
• Disease duration
• Disease severity
• Use of higher daily levodopa doses
• Older age
• Increased risk of falls
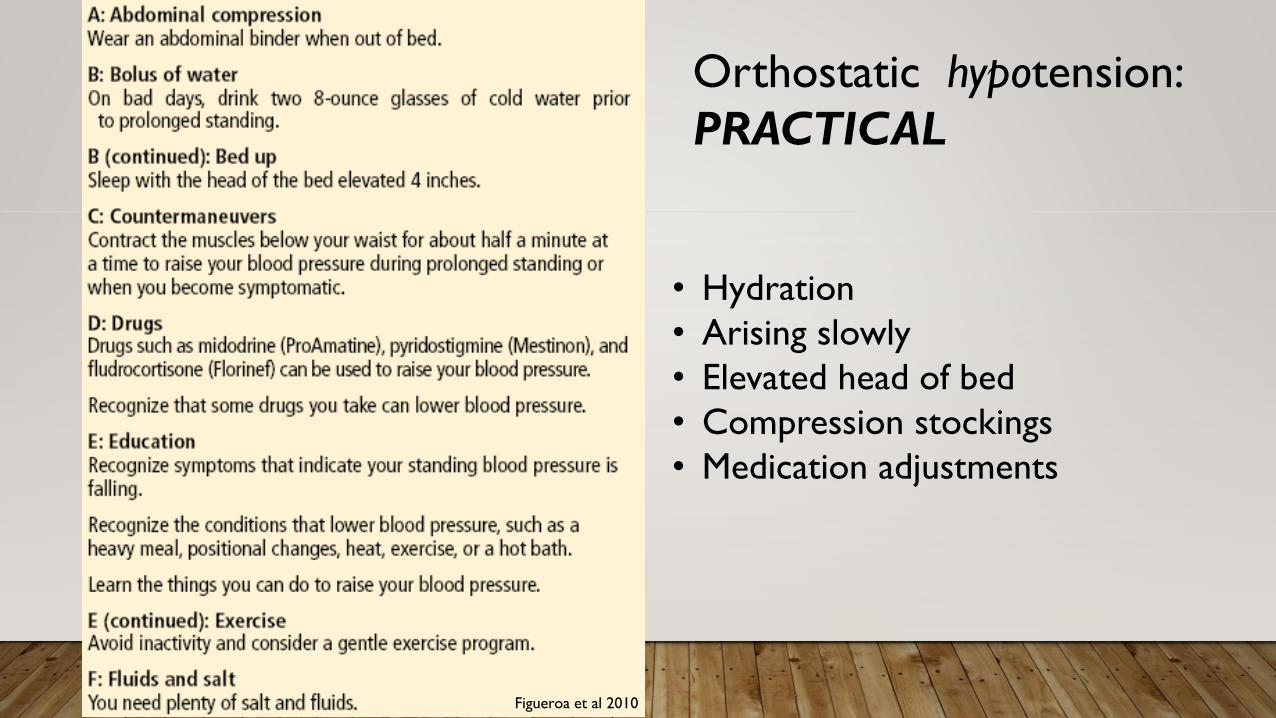
• Hydration
• Arising slowly
• Elevated head of bed
• Compression stockings
• Medication adjustments
Figueroa et al 2010
Orthostatic hypotension:
PRACTICAL
ORTHOSTATIC HYPOTENSIONTREATMENT
1. Fludrocortisone (Florinef): ↑increases
salt retention ↑blood volume, ↑blood
pressure
2. Midodrine (ProAmatine): causes blood
vessels to constrict ↑blood pressure
3. Droxidopa (Northera® ):
norepinephrine ↑blood pressure

URINARY DYSFUNCTION
• Prevalence 38-71% (57%)
• Nocturia** (overnight)
• Frequency *
• Urgency*
• Urge incontinence
• Hesitancy and bladder retention
• Proper referral to a urologist is
important for guidance in assessment
and treatment
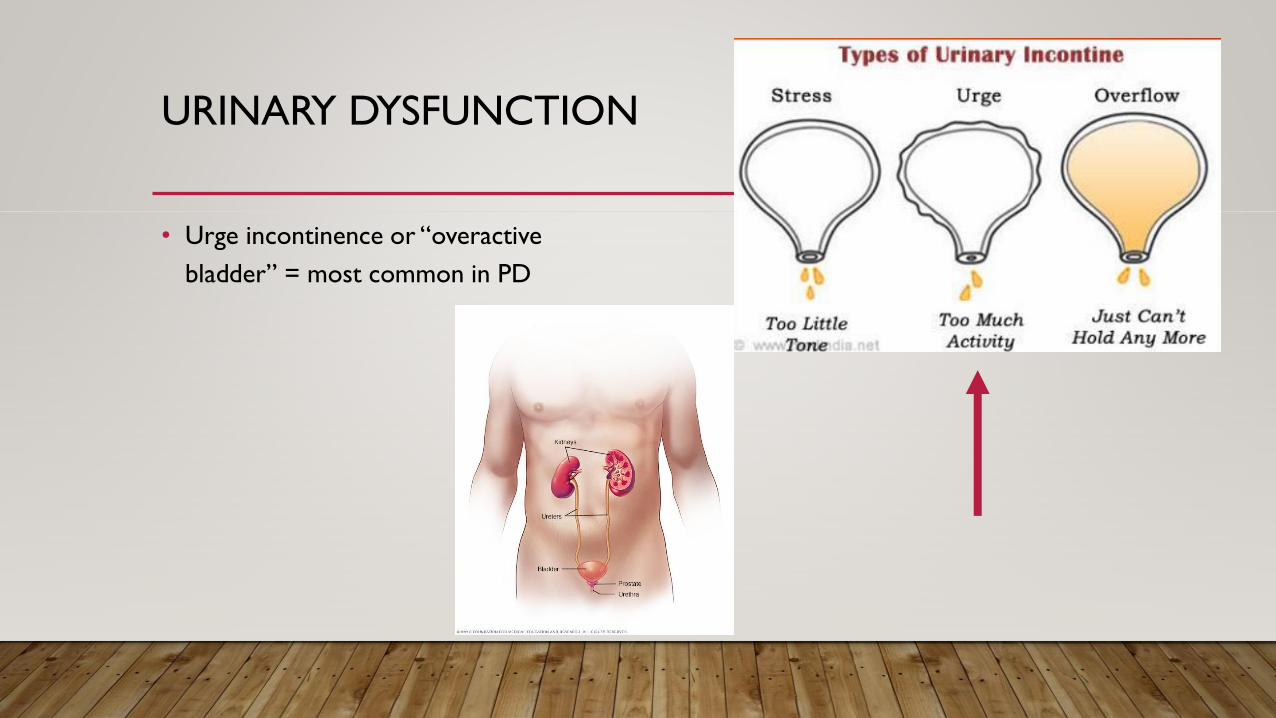
URINARY DYSFUNCTION
• Urge incontinence or “overactive
bladder” = most common in PD
URINARY DYSFUNCTION
• Medications that work to block or reduce bladder over-activity:
OLDER MEDICINES
• oxybutynin (Ditropan)
• tolterodine (Detrol)
NEWER MEDICINES
• solifenacin (Vesicare)
• darifenacin (Enablex)
• trospium (Sanctura)
• mirabegron (Myrbetriq)
• “Botox” injections
URINARY DYSFUNCTION : PRACTICAL
• Examine the medications
• Look for infection (UTI)
• Weight loss
• Dietary changes – cut back on alcohol, caffeine
and carbonated beverages
• Cut back on excessive fluid intake but avoid
dehydration!
• Cut back on night time fluid intake if nocturia
• Smoking cessation
• Pelvic floor (Kegel) exercises
• Bladder training
• voiding diary
• void at regular timed intervals
• urgency episodes are dealt with by distraction
and Kegel movements
• voiding intervals are gradually increased
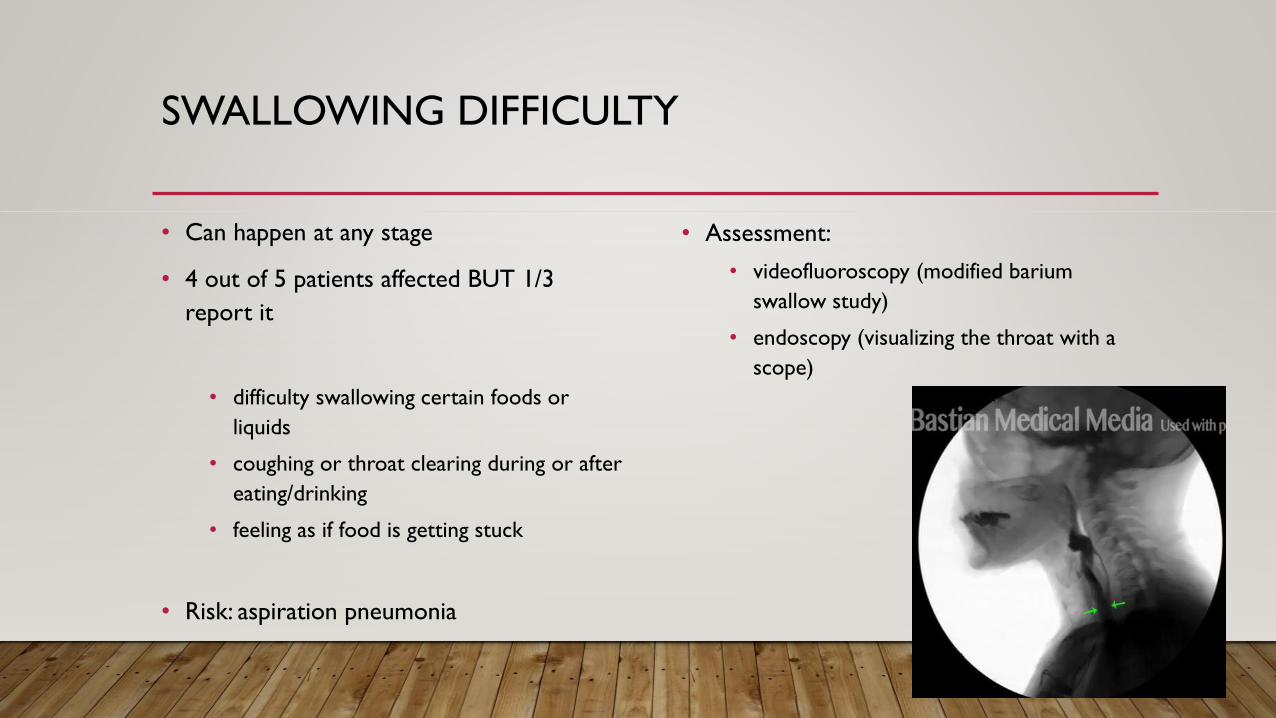
SWALLOWING DIFFICULTY
• Can happen at any stage
• 4 out of 5 patients affected BUT 1/3
report it
• difficulty swallowing certain foods or
liquids
• coughing or throat clearing during or after
eating/drinking
• feeling as if food is getting stuck
• Risk: aspiration pneumonia
• Assessment:
• videofluoroscopy (modified barium
swallow study)
• endoscopy (visualizing the throat with a
scope)
SWALLOWING DIFFICULTY: PRACTICAL
• Strategies to help food or liquid go down
safely
• swallowing hard
• holding breath while swallowing
• tucking the chin while swallowing
• Exercises
• Diet changes
• thickening liquids
• making foods softer
• Ask your doctor to refer you to a
speech/language pathologist for a
swallowing evaluation
CHANGES IN SPEECH
• The voice may get softer, breathy, or hoarse, causing others difficulty hearing
what is said
• Speech may be slurred
• Speech may be mumbled or expressed rapidly
• The tone of the voice may become monotone, lacking the normal ups/downs
• The person may have difficulty finding the right words, causing speech to be
slower
• The person may have difficulty participating in fast-paced conversations
CHANGES IN SPEECH: PRACTICAL
• Assessment and treatment with speech therapist/pathologist
• Lee Silverman Voice Treatment (LSVT) - improvements may last up to 2 years: “LOUD”
• Assistive communication device
• portable voice amplifier
• electronic device for stuttering (Speech Easy)
• Collagen is injected into the vocal folds (only when vocal cords don’t close completely)
PAIN
• 60% prevalence
• Dystonia/dyskinesia: pulsing or aching
• Musculoskeletal pain: aching or burning
• Nerve/nerve root pain: sharp, numbness
or “pins and needles”
• Primary/central pain: sudden, sharp
burning pain that occurs for no known
reason
• Akathisia: restlessness
• Musculoskeletal pain
• Frozen shoulder
• Flexed fingers or toes
• Stooped posture (camptocormia)
• Leaning sideways (Pisa syndrome)
• Scoliosis
• Dropped head (anterocollis)
• Bone fractures
PAIN: PRACTICAL
• Dopamine agonists, carbidopa/levodopa
• Medication for nerve pain
(gabapentin/Neurontin, pregabalin/Lyrica)
• Topical (Lidoderm, capsaicin)
• Medical cannabis? (CBD>THC)
• Physical therapy
• Acupuncture
• Tai chi and yoga
• Exercise

THANK YOU