“non“non--invasive positive pressure invasive … · 3.02.2010 1 “non“non--invasive...
TRANSCRIPT
3.02.2010
1
“Non“Non--Invasive Positive Pressure Invasive Positive Pressure Ventilation”Ventilation”
Robert M. Kacmarek PhD, RRTRobert M. Kacmarek PhD, RRTHarvard Medical SchoolHarvard Medical SchoolHarvard Medical SchoolHarvard Medical School
Massachusetts General HospitalMassachusetts General HospitalBoston, MassachusettsBoston, Massachusetts
66--99--08 Estonia08 Estonia
Who Who –– Indications for NPPVIndications for NPPVUndisputed indications Undisputed indications
Acute Exacerbation of COPDAcute Exacerbation of COPDAcute Cardiogenic Pulmonary EdemaAcute Cardiogenic Pulmonary Edema
General Indications for UseGeneral Indications for UseP b i H bi R i F ilP b i H bi R i F ilPost extubation Hypercarbic Respiratory FailurePost extubation Hypercarbic Respiratory FailureHypoxemic Respiratory Failure in :Hypoxemic Respiratory Failure in :
-- Immunosurpressed PatientsImmunosurpressed Patients-- Patients Awaiting TransplantationPatients Awaiting Transplantation-- Patients Post Lung ResectionPatients Post Lung Resection
Patients with DNI StatusPatients with DNI StatusAcute Hypercapnic Respiratory Failure as a Result ofAcute Hypercapnic Respiratory Failure as a Result ofAcute Hypercapnic Respiratory Failure as a Result of Acute Hypercapnic Respiratory Failure as a Result of
Neurological or Neuromuscular DiseaseNeurological or Neuromuscular DiseaseControversial IndicationsControversial Indications
Post Post ––Extubation Hypoxemic Respiratory FailureExtubation Hypoxemic Respiratory FailureAcute Lung InjuryAcute Lung InjuryAcute Respiratory Distress SyndromeAcute Respiratory Distress SyndromeAsthmaAsthma
3.02.2010
2
Brochard NEJM 1995; 333:817Brochard NEJM 1995; 333:817Acute exacerbation COPDAcute exacerbation COPD
NPPV (n = 43) vs control (n = 42)NPPV (n = 43) vs control (n = 42)Five centers in EuropeFive centers in EuropeFive centers in EuropeFive centers in Europe
NPPVNPPV ControlControlIntubatedIntubated 11 (26%)11 (26%) 31 (74%)*31 (74%)*Hospital StayHospital Stay 23 23 ++ 1717 35 35 ++ 33 days*33 days*MortalityMortality 4 (9%)4 (9%) 12 (29%)*12 (29%)*MortalityMortality 4 (9%)4 (9%) 12 (29%)12 (29%)
*p < 0.01*p < 0.0110/12 control and 3/4 NPPV10/12 control and 3/4 NPPVDeaths in intubated patientsDeaths in intubated patients
NPPV Acute Exacerbation of NPPV Acute Exacerbation of COPDCOPD
I5 RCT’s NPPV in COPDI5 RCT’s NPPV in COPDI5 RCT s NPPV in COPDI5 RCT s NPPV in COPDNPPV:NPPV:
Prevents intubationPrevents intubationDecreases length of MVDecreases length of MVDecreases ICU and Hosp stayDecreases ICU and Hosp stayDecreases cost Decreases cost Decreases mortalityDecreases mortality
Keenen JAMA 2002 Keenen JAMA 2002

3.02.2010
3
NPPV Acute Exacerbation of NPPV Acute Exacerbation of COPDCOPD
Standard of CareStandard of CareShould be available as first line Should be available as first line therapy in all setting caring for therapy in all setting caring for COPD ti tCOPD ti tCOPD patientsCOPD patients
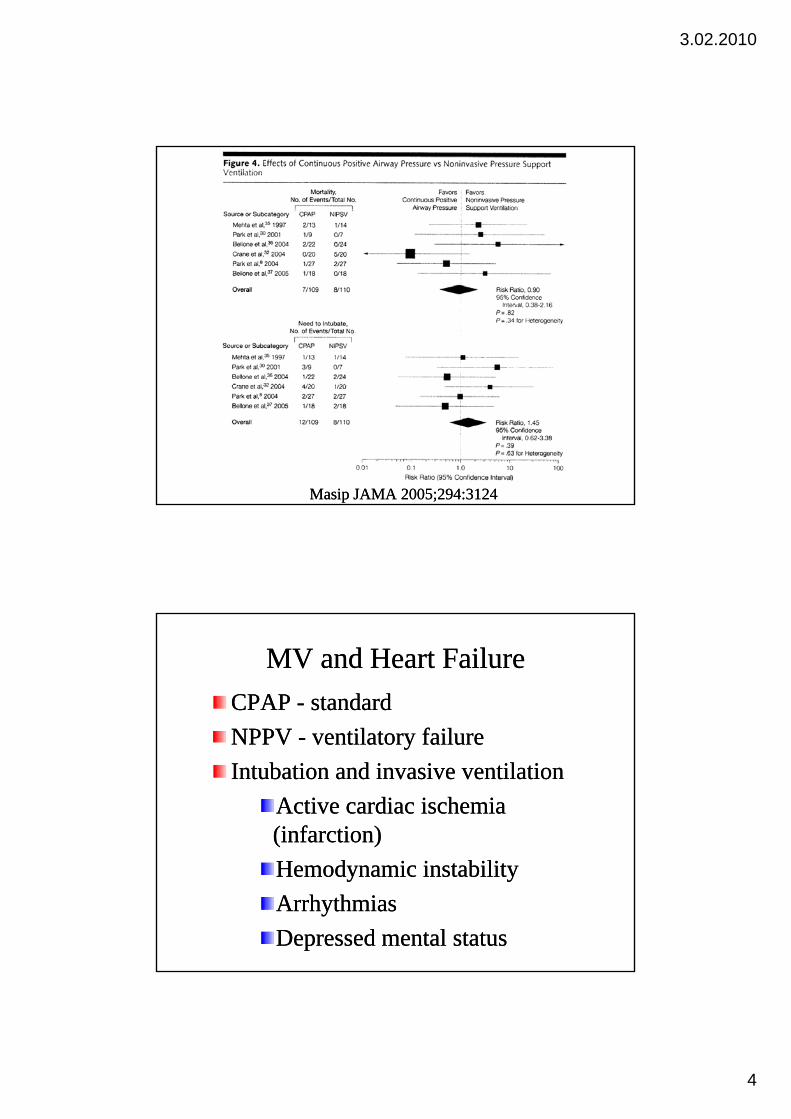
Masip JAMA 2005;294:3124Masip JAMA 2005;294:3124
3.02.2010
4
Masip JAMA 2005;294:3124Masip JAMA 2005;294:3124
MV and Heart FailureMV and Heart FailureCPAP CPAP -- standardstandardNPPVNPPV til t f iltil t f ilNPPV NPPV -- ventilatory failureventilatory failureIntubation and invasive ventilationIntubation and invasive ventilation
Active cardiac ischemia Active cardiac ischemia (infarction)(infarction)Hemodynamic instabilityHemodynamic instabilityArrhythmiasArrhythmiasDepressed mental statusDepressed mental status
3.02.2010
5
NPPV Acute Hypoxemic RFNPPV Acute Hypoxemic RF
Post Operative Respiratory FailurePost Operative Respiratory FailureImmunosurpressed PatientsImmunosurpressed PatientsPatients Awaiting TransplantationPatients Awaiting TransplantationPatients Post Lung Resection Patients Post Lung Resection Acute Lung InjuryAcute Lung InjuryAcute Lung InjuryAcute Lung InjuryAcute Respiratory Distress SyndromeAcute Respiratory Distress Syndrome
Squadrone JAMA 2005;293:589Squadrone JAMA 2005;293:589209 pts developing hypoxemia (P/F < 300 mm 209 pts developing hypoxemia (P/F < 300 mm Hg) post major abdominal elective surgeryHg) post major abdominal elective surgeryRandomized to CPAP vs. simple O2 therapyRandomized to CPAP vs. simple O2 therapyCPAP lower incidence of:CPAP lower incidence of:
Intubation (1% vs. 10%, p = 0.005)Intubation (1% vs. 10%, p = 0.005)Pneumonia (2% vs. 10%, p = 0.02)Pneumonia (2% vs. 10%, p = 0.02)Infection (2% vs. 10%, p = 0.03)Infection (2% vs. 10%, p = 0.03)Sepsis (2% vs. 9%, p = 0.03)Sepsis (2% vs. 9%, p = 0.03)No difference in ICU or Hosp LOS or No difference in ICU or Hosp LOS or mortality (0 vs. 3)mortality (0 vs. 3)
3.02.2010
6
KindgrenKindgren--Milles Chest 2005;128:821Milles Chest 2005;128:821
56 pts following elective prosthetic replacement 56 pts following elective prosthetic replacement f h h bd i lf h h bd i lof the thoracoabdominal aortaof the thoracoabdominal aorta
Post extubation in ICU 10 cmHPost extubation in ICU 10 cmH22O CPAP for 12 O CPAP for 12 to 24h vs. CPAP 10 min Q4hto 24h vs. CPAP 10 min Q4hFewer pulmonary complications (Pneumonia, Fewer pulmonary complications (Pneumonia, atelectasis P/F < 100 reintubations) p < 0 019atelectasis P/F < 100 reintubations) p < 0 019atelectasis, P/F < 100, reintubations), p < 0.019atelectasis, P/F < 100, reintubations), p < 0.019Hosp LOS 22Hosp LOS 22++2 vs. 342 vs. 34++5 days, p < 0.0485 days, p < 0.048
HPPVHPPV--Hypoxemic Respiratory FailureHypoxemic Respiratory FailureHilbert NEJM 2001;344:481Hilbert NEJM 2001;344:481
52 Immunosuppressed patients NPPV vs. St Rx52 Immunosuppressed patients NPPV vs. St RxR i d i b i S i li i Di d i h ICUR i d i b i S i li i Di d i h ICURequired intubation, Serious complications, Died in the ICU: Required intubation, Serious complications, Died in the ICU: better with NPPV p < 0.05better with NPPV p < 0.05
Antonelli JAMA 2000; 283:235Antonelli JAMA 2000; 283:23540 Patients awaiting transplantation NPPV vs. St Rx40 Patients awaiting transplantation NPPV vs. St RxIntubation, Length of hospitalization, Complications, ICU Intubation, Length of hospitalization, Complications, ICU mortality: better with NPPV p < 0 05mortality: better with NPPV p < 0 05mortality: better with NPPV p < 0.05mortality: better with NPPV p < 0.05
Auriant AJRCCM 2001;164:1231Auriant AJRCCM 2001;164:123148 patients post lung resection48 patients post lung resectionIntubation, Hospital mortality: better with NPPV p <0.05 Intubation, Hospital mortality: better with NPPV p <0.05

3.02.2010
7
Antonelli NEJM 1998; 339:429Antonelli NEJM 1998; 339:429Hypoxemic ARF, nonHypoxemic ARF, non--immunosuppressed immunosuppressed NPPV n = 32 CMV n = 32NPPV n = 32 CMV n = 32NPPV n 32, CMV n 32NPPV n 32, CMV n 32Survival: 50% CMV, 69% NPPVSurvival: 50% CMV, 69% NPPVComplications: 66% CMV, 38% NPPV Complications: 66% CMV, 38% NPPV (P=0.02)(P=0.02)Pneumonia/sinusitis:Pneumonia/sinusitis:Pneumonia/sinusitis: Pneumonia/sinusitis:
31% CMV, 3% NPPV (p=0.003)31% CMV, 3% NPPV (p=0.003)MV shorter NPPV (p=0.006)MV shorter NPPV (p=0.006)ICU stay shorter NPPV (p=0.002)ICU stay shorter NPPV (p=0.002)
Ferrer AJRCCM 2003;168:1444Ferrer AJRCCM 2003;168:1444
105 pts PO105 pts PO22 < 60 mmHg or SpO< 60 mmHg or SpO22 < 90% for > < 90% for > 6 hr with maximal O6 hr with maximal O22 50% by venturi mask50% by venturi mask22
RCT: ORCT: O22 vs. NPPV, PEEP 7 vs. NPPV, PEEP 7 ++ 2, ventilating 2, ventilating press 16 press 16 ++ 3 cmH3 cmH22O for 3.5 O for 3.5 ++ 2.6 days2.6 daysNPPV decreased :NPPV decreased :•• Intubation 13(25%) vs 28(52%) p = 0 01Intubation 13(25%) vs 28(52%) p = 0 01•• Intubation 13(25%) vs. 28(52%) p = 0.01Intubation 13(25%) vs. 28(52%) p = 0.01•• Septic shock 6(12%) vs. 17(31%) p = 0.028Septic shock 6(12%) vs. 17(31%) p = 0.028•• ICU mortality 9(18%) vs 20(39%) p = 0.028ICU mortality 9(18%) vs 20(39%) p = 0.028
3.02.2010
8
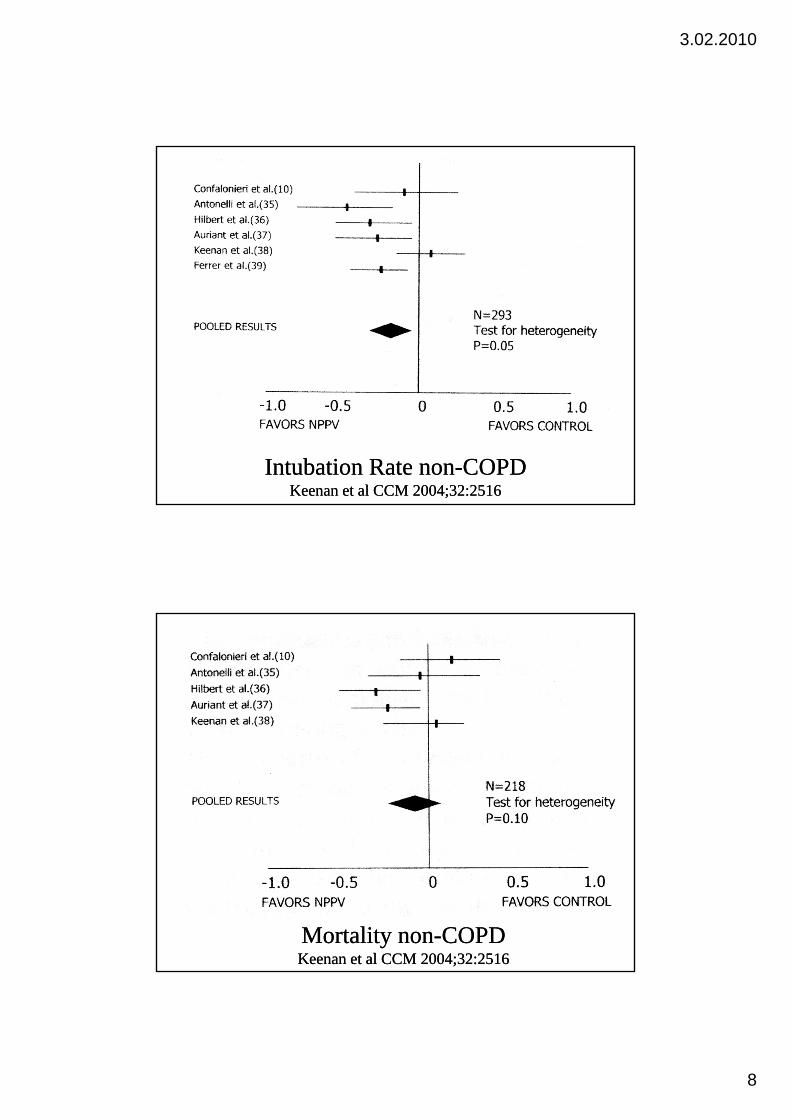
Intubation Rate nonIntubation Rate non--COPDCOPDKeenan et al CCM 2004;32:2516Keenan et al CCM 2004;32:2516
Mortality nonMortality non--COPDCOPDKeenan et al CCM 2004;32:2516Keenan et al CCM 2004;32:2516
3.02.2010
9
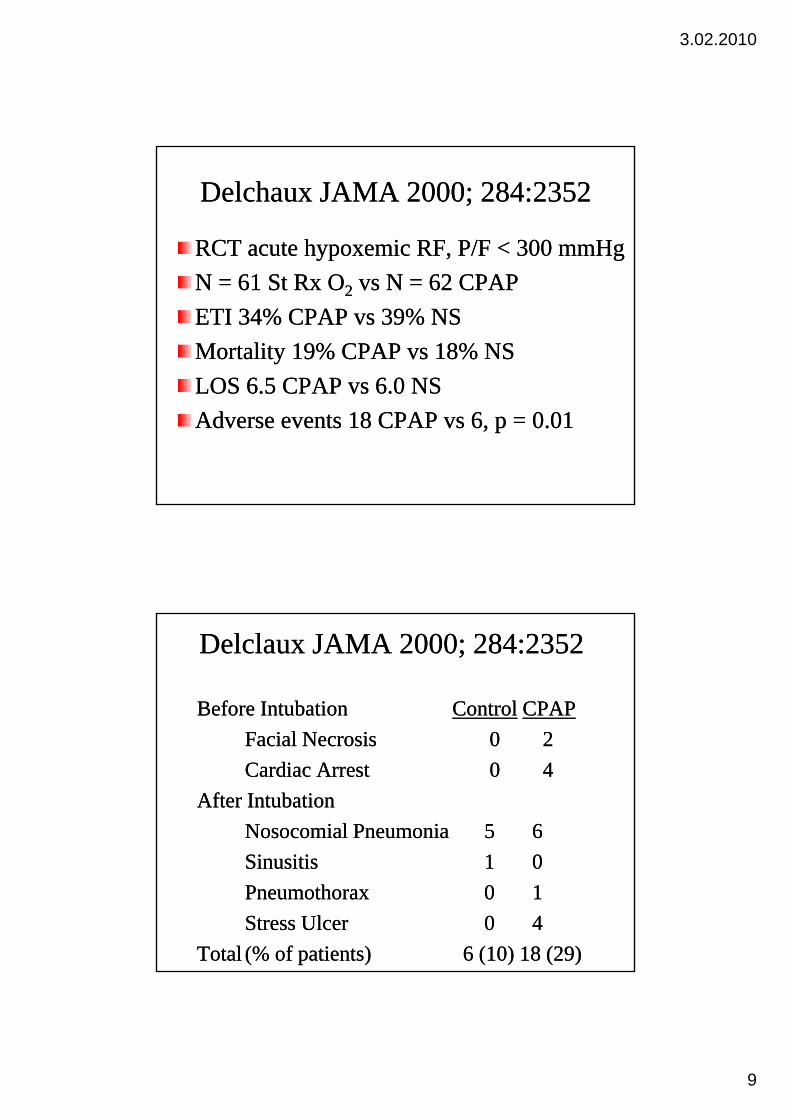
Delchaux JAMA 2000; 284:2352Delchaux JAMA 2000; 284:2352
RCT acute hypoxemic RF, P/F < 300 mmHgRCT acute hypoxemic RF, P/F < 300 mmHgN = 61 St Rx ON = 61 St Rx O22 vs N = 62 CPAP vs N = 62 CPAP ETI 34% CPAP vs 39% NSETI 34% CPAP vs 39% NSMortality 19% CPAP vs 18% NSMortality 19% CPAP vs 18% NSLOS 6 5 CPAP vs 6 0 NSLOS 6 5 CPAP vs 6 0 NSLOS 6.5 CPAP vs 6.0 NSLOS 6.5 CPAP vs 6.0 NSAdverse events 18 CPAP vs 6, p = 0.01Adverse events 18 CPAP vs 6, p = 0.01
Delclaux JAMA 2000; 284:2352Delclaux JAMA 2000; 284:2352
Before IntubationBefore Intubation ControlControl CPAPCPAPF i l N iF i l N i 00 22Facial NecrosisFacial Necrosis 00 22Cardiac ArrestCardiac Arrest 00 44
After IntubationAfter IntubationNosocomial PneumoniaNosocomial Pneumonia 55 66SinusitisSinusitis 11 00PneumothoraxPneumothorax 00 11Stress UlcerStress Ulcer 00 44
TotalTotal (% of patients)(% of patients) 6 (10) 18 (29)6 (10) 18 (29)
3.02.2010
10
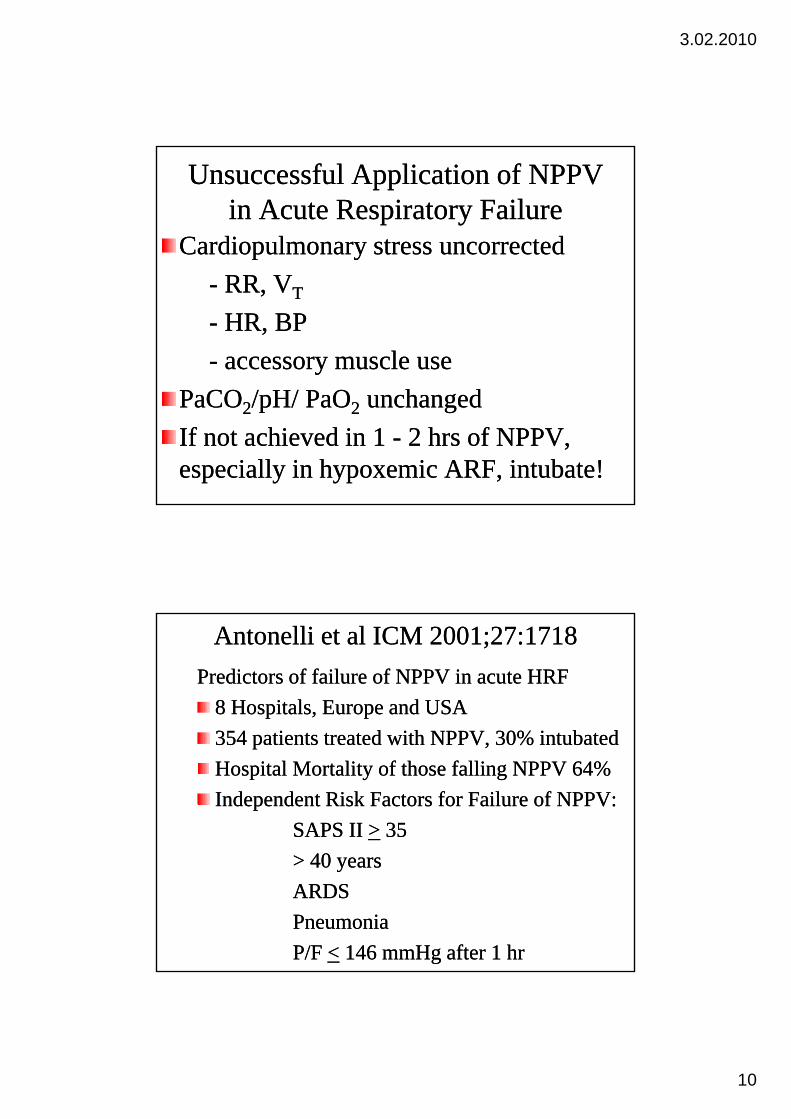
Unsuccessful Application of NPPV Unsuccessful Application of NPPV in Acute Respiratory Failurein Acute Respiratory Failure
Cardiopulmonary stress uncorrectedCardiopulmonary stress uncorrected-- RR, VRR, VTT
-- HR, BPHR, BP-- accessory muscle useaccessory muscle use
PaCOPaCO22/pH/ PaO/pH/ PaO22 unchangedunchangedIf not achieved in 1 If not achieved in 1 -- 2 hrs of NPPV, 2 hrs of NPPV, especially in hypoxemic ARF, intubate!especially in hypoxemic ARF, intubate!
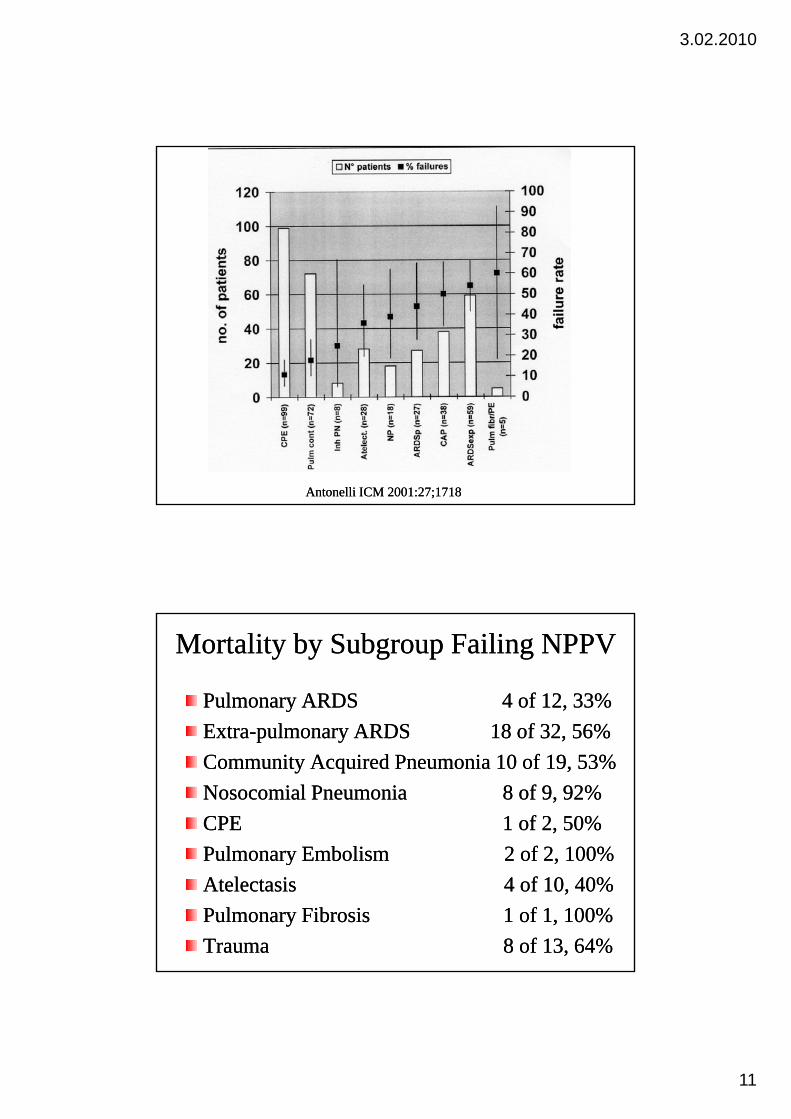
Antonelli et al ICM 2001;27:1718Antonelli et al ICM 2001;27:1718Predictors of failure of NPPV in acute HRFPredictors of failure of NPPV in acute HRF
8 Hospitals, Europe and USA8 Hospitals, Europe and USA354 ti t t t d ith NPPV 30% i t b t d354 ti t t t d ith NPPV 30% i t b t d354 patients treated with NPPV, 30% intubated354 patients treated with NPPV, 30% intubatedHospital Mortality of those falling NPPV 64%Hospital Mortality of those falling NPPV 64%Independent Risk Factors for Failure of NPPV:Independent Risk Factors for Failure of NPPV:
SAPS II SAPS II >> 3535> 40 years> 40 yearsARDS ARDS PneumoniaPneumoniaP/F P/F << 146 mmHg after 1 hr146 mmHg after 1 hr
3.02.2010
11
Antonelli ICM 2001:27;1718Antonelli ICM 2001:27;1718
Mortality by Subgroup Failing NPPVMortality by Subgroup Failing NPPV
Pulmonary ARDS 4 of 12, 33%Pulmonary ARDS 4 of 12, 33%ExtraExtra pulmonary ARDS 18 of 32 56%pulmonary ARDS 18 of 32 56%ExtraExtra--pulmonary ARDS 18 of 32, 56%pulmonary ARDS 18 of 32, 56%Community Acquired Pneumonia 10 of 19, 53%Community Acquired Pneumonia 10 of 19, 53%Nosocomial Pneumonia 8 of 9, 92%Nosocomial Pneumonia 8 of 9, 92%CPE 1 of 2, 50%CPE 1 of 2, 50%Pulmonary EmbolismPulmonary Embolism 2 of 2 100%2 of 2 100%Pulmonary Embolism Pulmonary Embolism 2 of 2, 100%2 of 2, 100%Atelectasis 4 of 10, 40%Atelectasis 4 of 10, 40%Pulmonary Fibrosis 1 of 1, 100%Pulmonary Fibrosis 1 of 1, 100%Trauma 8 of 13, 64%Trauma 8 of 13, 64%
3.02.2010
12
Schettino CCM 2008 Schettino CCM 2008
About 1000 patients received NPPV over About 1000 patients received NPPV over h fh fthe course of one yearthe course of one year
Three groups: Chronic use, ARF, DNI/DNRThree groups: Chronic use, ARF, DNI/DNR144 with hypoxemic ARF (none acute heart 144 with hypoxemic ARF (none acute heart failure or post extubation)failure or post extubation)60% failed NPPV and were intubated60% failed NPPV and were intubatedOf these 64% (55) diedOf these 64% (55) died
Schettino CCM 2008Schettino CCM 2008Acute RF 458 patients managed with NPPVAcute RF 458 patients managed with NPPV38% failed NPPV and required intubation38% failed NPPV and required intubation38% failed NPPV and required intubation38% failed NPPV and required intubationMortality failing 47% vs. 5.4%, p < 0.0001Mortality failing 47% vs. 5.4%, p < 0.0001CPE 18% intubated, mortality 39%CPE 18% intubated, mortality 39%COPD 24% intubated, mortality 33%COPD 24% intubated, mortality 33%NonNon COPD hypercapnia 38% intubated mortalityCOPD hypercapnia 38% intubated mortalityNonNon--COPD hypercapnia 38% intubated, mortality COPD hypercapnia 38% intubated, mortality 0.0%0.0%Post extubation failure 40% intubated, mortality Post extubation failure 40% intubated, mortality 32%32%
3.02.2010
13
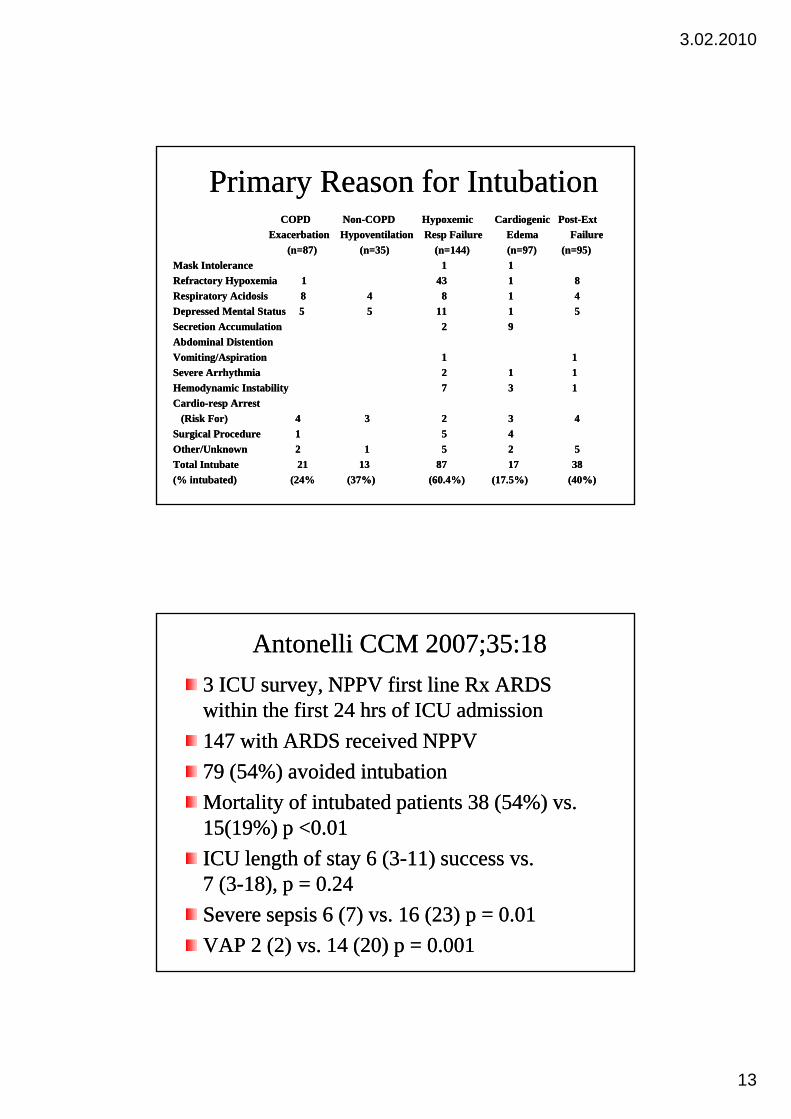
Primary Reason for IntubationPrimary Reason for IntubationCOPD NonCOPD Non--COPD Hypoxemic Cardiogenic PostCOPD Hypoxemic Cardiogenic Post--ExtExt
Exacerbation Hypoventilation Resp Failure Edema FailureExacerbation Hypoventilation Resp Failure Edema Failure(n=87) (n=35) (n=144) (n=97)(n=87) (n=35) (n=144) (n=97) (n=95)(n=95)
Mask IntoleranceMask Intolerance 11 11Mask IntoleranceMask Intolerance 11 11Refractory Hypoxemia 1Refractory Hypoxemia 1 4343 11 88Respiratory AcidosisRespiratory Acidosis 88 44 88 11 44Depressed Mental Status 5Depressed Mental Status 5 55 11 11 11 55Secretion AccumulationSecretion Accumulation 22 99Abdominal DistentionAbdominal DistentionVomiting/AspirationVomiting/Aspiration 11 11Severe ArrhythmiaSevere Arrhythmia 22 11 11H d i I t bilitH d i I t bilit 77 33 11Hemodynamic InstabilityHemodynamic Instability 77 33 11CardioCardio--resp Arrestresp Arrest
(Risk For) (Risk For) 44 33 22 33 44Surgical ProcedureSurgical Procedure 11 55 44Other/UnknownOther/Unknown 22 11 55 22 55Total Intubate 21Total Intubate 21 1313 8787 1717 3838(% intubated) (24% (37%) (60.4%) (17.5%) (40%)(% intubated) (24% (37%) (60.4%) (17.5%) (40%)
Antonelli CCM 2007;35:18Antonelli CCM 2007;35:183 ICU survey, NPPV first line Rx ARDS 3 ICU survey, NPPV first line Rx ARDS within the first 24 hrs of ICU admissionwithin the first 24 hrs of ICU admission147 with ARDS received NPPV147 with ARDS received NPPV79 (54%) avoided intubation79 (54%) avoided intubationMortality of intubated patients 38 (54%) vs. Mortality of intubated patients 38 (54%) vs. 15(19%) p <0.0115(19%) p <0.01ICU l h f 6 (3ICU l h f 6 (3 11)11)ICU length of stay 6 (3ICU length of stay 6 (3--11) success vs. 11) success vs. 7 (37 (3--18), p = 0.2418), p = 0.24Severe sepsis 6 (7) vs. 16 (23) p = 0.01Severe sepsis 6 (7) vs. 16 (23) p = 0.01VAP 2 (2) vs. 14 (20) p = 0.001VAP 2 (2) vs. 14 (20) p = 0.001
3.02.2010
14
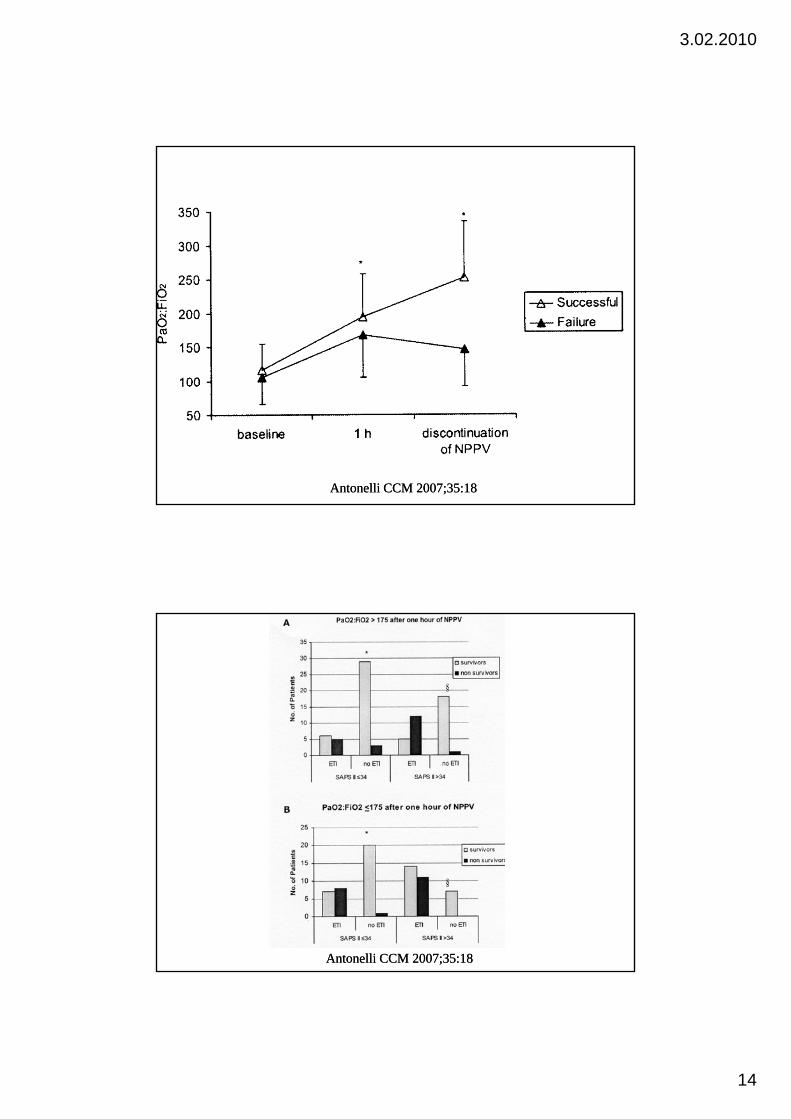
Antonelli CCM 2007;35:18Antonelli CCM 2007;35:18
Antonelli CCM 2007;35:18Antonelli CCM 2007;35:18
3.02.2010
15
NPPVNPPV Hypoxemic RFHypoxemic RFKey word is Key word is Caution!Caution!Hypoxemic Respiratory Failure in :Hypoxemic Respiratory Failure in :
––Post operative Respiratory Failure Post operative Respiratory Failure -- YesYes-- Immunosurpressed Patients Immunosurpressed Patients -- YesYes-- Patients Awaiting TransplantationPatients Awaiting Transplantation-- YesYes-- Patients Post Lung Resection Patients Post Lung Resection -- Yes Yes
Acute Lung Injury Acute Lung Injury –– With CautionWith CautionCommunity Acquired Pneumonia Community Acquired Pneumonia –– With CautionWith CautionAcute Respiratory Distress Syndrome Acute Respiratory Distress Syndrome -- ????????
Elective Extubation to NPPVElective Extubation to NPPVCOPD, failed TCOPD, failed T--piece trial 48piece trial 48--72 hr after 72 hr after intubationintubationR d i d t PSV t b ti t NPPVR d i d t PSV t b ti t NPPVRandomized to PSV vs. extubation to NPPVRandomized to PSV vs. extubation to NPPVBetter outcome NPPV Better outcome NPPV
Nava Ann Intern Med 1998; 128:721Nava Ann Intern Med 1998; 128:721
No difference in outcomeNo difference in outcomeGirault AJRCCM 1999;160:86Girault AJRCCM 1999;160:86Girault AJRCCM 1999;160:86Girault AJRCCM 1999;160:86
Failed weaning trial 3 consecutive days, 50% of Failed weaning trial 3 consecutive days, 50% of patients COPD, better outcome NPPVpatients COPD, better outcome NPPV
Ferrier AJRCCM 2003;168:70Ferrier AJRCCM 2003;168:70
3.02.2010
16
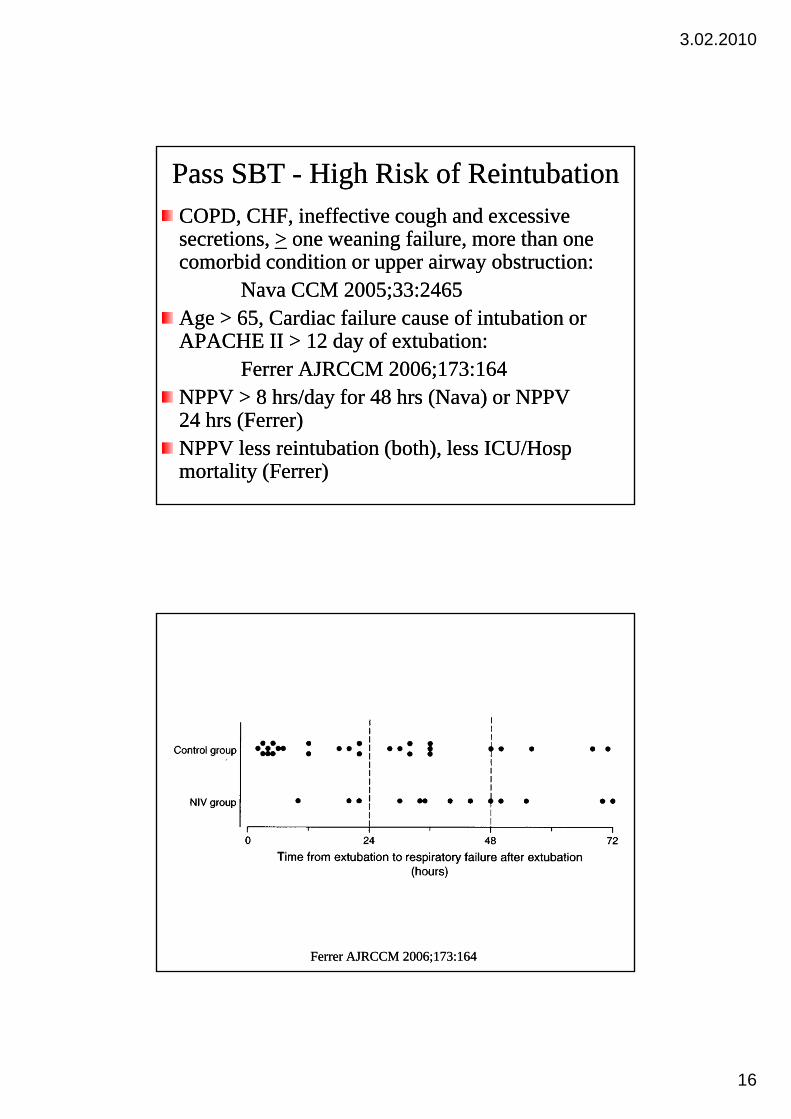
Pass SBT Pass SBT -- High Risk of ReintubationHigh Risk of ReintubationCOPD, CHF, ineffective cough and excessive COPD, CHF, ineffective cough and excessive secretions, secretions, >> one weaning failure, more than one one weaning failure, more than one comorbid condition or upper airway obstruction:comorbid condition or upper airway obstruction:comorbid condition or upper airway obstruction: comorbid condition or upper airway obstruction:
Nava CCM 2005;33:2465Nava CCM 2005;33:2465Age > 65, Cardiac failure cause of intubation or Age > 65, Cardiac failure cause of intubation or APACHE II > 12 day of extubation: APACHE II > 12 day of extubation:
Ferrer AJRCCM 2006;173:164Ferrer AJRCCM 2006;173:164NPPV > 8 hrs/day for 48 hrs (Nava) or NPPV NPPV > 8 hrs/day for 48 hrs (Nava) or NPPV 24 hrs (Ferrer)24 hrs (Ferrer)NPPV less reintubation (both), less ICU/Hosp NPPV less reintubation (both), less ICU/Hosp mortality (Ferrer)mortality (Ferrer)
Ferrer AJRCCM 2006;173:164Ferrer AJRCCM 2006;173:164

3.02.2010
17
NPPV PostNPPV Post--Extubation FailureExtubation Failure•• Weaned nonWeaned non--COPD patients developing acute hypoxemic COPD patients developing acute hypoxemic
respiratory failure < 48 hours after extubation (n=81)respiratory failure < 48 hours after extubation (n=81)Reintubation rate 72 vs. 69%, LOS, mortality no Reintubation rate 72 vs. 69%, LOS, mortality no differencedifference
Keenan JAMA 2002;287:3238Keenan JAMA 2002;287:3238•• Primarily patients developing acute hypoxemic Primarily patients developing acute hypoxemic
respiratory failure (n=244), 37centers, 8 countriesrespiratory failure (n=244), 37centers, 8 countriesReintubation 48% both groupsReintubation 48% both groupsICU mortality 25% NPPV vs. 14% p=0.048ICU mortality 25% NPPV vs. 14% p=0.048Time to intubation 12 hr NPPV vs. 2.5 hr p=0.02Time to intubation 12 hr NPPV vs. 2.5 hr p=0.02
Esteban NEJM 2004;350:2452Esteban NEJM 2004;350:2452
NPPV and WeaningNPPV and WeaningFailed weaning NPPV bridge to spontaneous Failed weaning NPPV bridge to spontaneous breathingbreathingbreathingbreathing
COPD onlyCOPD onlyWeaned successfully but high probability of Weaned successfully but high probability of failurefailure
COPD CHFCOPD CHFCOPD, CHF, etcCOPD, CHF, etcExtubation FailureExtubation Failure
COPD, CHF COPD, CHF --Yes Yes Acute Hypoxemic RF Acute Hypoxemic RF -- NoNo

3.02.2010
18
Categorization of Indications for NPPVCategorization of Indications for NPPV
Life Support Without Preset LimitsLife Support Without Preset LimitsppppLife Support With Preset LimitsLife Support With Preset Limits
DNIDNIComfort Measures OnlyComfort Measures OnlyComfort Measures OnlyComfort Measures Only
DNIDNICurtis CCM 2007;35:932Curtis CCM 2007;35:932
Goals of TherapyGoals of TherapyCategory 1 Category 1 -- Improved oxygenation and Improved oxygenation and ventilation, discomfort outweighed by ventilation, discomfort outweighed by
i l b fi !i l b fi !potential benefit!potential benefit!Category 2 Category 2 -- To restore health without To restore health without using endotracheal intubation and without using endotracheal intubation and without causing unacceptable discomfort!causing unacceptable discomfort!Category 3Category 3 Maximize comfort whileMaximize comfort whileCategory 3 Category 3 -- Maximize comfort while Maximize comfort while minimizing adverse efforts of opiates!minimizing adverse efforts of opiates!
Curtis CCM 2007;35:932Curtis CCM 2007;35:932
3.02.2010
19
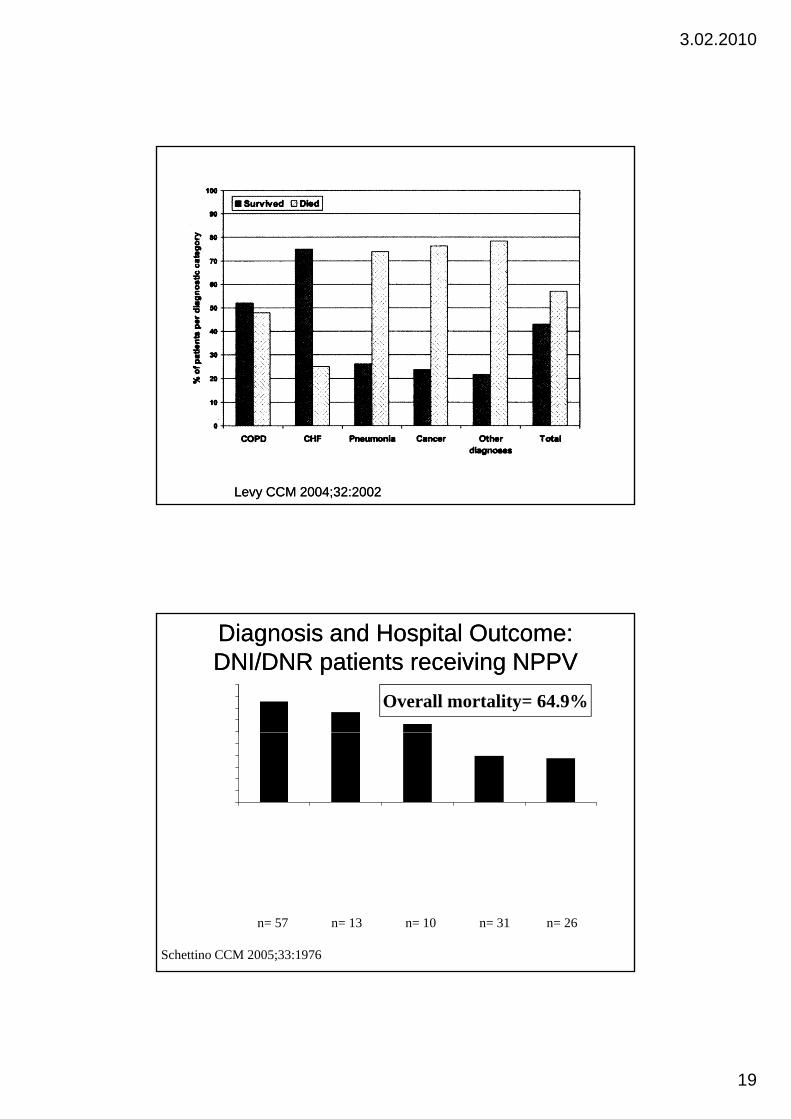
Levy CCM 2004;32:2002Levy CCM 2004;32:2002
Diagnosis and Hospital Outcome:Diagnosis and Hospital Outcome:DNI/DNR patients receiving NPPVDNI/DNR patients receiving NPPV
60708090
100
talit
y (%
)
Overall mortality= 64.9%
0102030405060
poxe
mic
pira
tory
Failu
re
tuba
tion
rato
rylu
re
CO
PDnt
ilatio
n
diog
enic
lmon
ary
Ede
ma
OPD
-er
batio
n
hosp
ital m
ort
Hyp
Res F
Post
-Ex
Res
pir
Fail
Non
-CH
ypov
e
Car Pu
l E CO
Exa
ce
n= 57 n= 13 n= 10 n= 31 n= 26
Schettino CCM 2005;33:1976

3.02.2010
20
What Do Patients Want!What Do Patients Want!
Data on patients perspective of “end of life” Data on patients perspective of “end of life” b d h i f ib d h i f ibased on the experience of cancer patients.based on the experience of cancer patients.Primary concern is “loss of autonomy over the Primary concern is “loss of autonomy over the circumstances of their dying”. circumstances of their dying”. Feeling powerless over decisions about Feeling powerless over decisions about medical treatment prolonging lifemedical treatment prolonging lifemedical treatment prolonging life.medical treatment prolonging life.
Simonds Chron Respir Dis 2004;1:56Simonds Chron Respir Dis 2004;1:56
The fear of death is being replaced by “the fear The fear of death is being replaced by “the fear of dying”.of dying”.
Clark BMJ 2003;327:174Clark BMJ 2003;327:174
A Good vs. Bad DeathA Good vs. Bad DeathAA Bad Death: A lack of opportunity to Bad Death: A lack of opportunity to
Plan aheadPlan aheadArrange personal affairsArrange personal affairsDecrease family burdenDecrease family burdenTo say good bye To say good bye
A Good DeathA Good DeathPain and symptom managementPain and symptom managementClear decision makingClear decision makingPreparation for deathPreparation for deathPreparation for deathPreparation for deathContributing to othersContributing to others
Steinhauser Ann Intern Med 2000;132:825Steinhauser Ann Intern Med 2000;132:825
Quill. “You promised me I would not die like Quill. “You promised me I would not die like this” Arch Intern Med 1995;155:1250this” Arch Intern Med 1995;155:1250
A Bad Death is a Medical Emergency!A Bad Death is a Medical Emergency!
3.02.2010
21
Ethical DilemmaEthical Dilemma
Has the patients provided informed consent?Has the patients provided informed consent?Ideally discussions regarding end of lifeIdeally discussions regarding end of lifeIdeally, discussions regarding end of life Ideally, discussions regarding end of life should occur as the patients condition begins should occur as the patients condition begins to change to provide the patient time to to change to provide the patient time to contemplate DNI status and the use of NPPVcontemplate DNI status and the use of NPPVDiscussions should occur long before patientsDiscussions should occur long before patientsDiscussions should occur long before patients Discussions should occur long before patients are admitted in acute failureare admitted in acute failurePatients preferences should be clearly Patients preferences should be clearly documented in the medical recorddocumented in the medical record
NPPV NPPV ––DNI/DNRDNI/DNRDoes reverse acute RF in many patientsDoes reverse acute RF in many patientsDoes allow patient to communicate and make Does allow patient to communicate and make decisionsdecisionsMay decrease use of opioids and improve May decrease use of opioids and improve patient comfort?patient comfort?Does require that patients be fully informed of Does require that patients be fully informed of q p yq p ywhat NPPV is and what it is intended to do!what NPPV is and what it is intended to do!Add “Do Not Noninvasively Ventilate” to the Add “Do Not Noninvasively Ventilate” to the list of status decisions patients make upon list of status decisions patients make upon admissionadmission
3.02.2010
22
3.02.2010
23
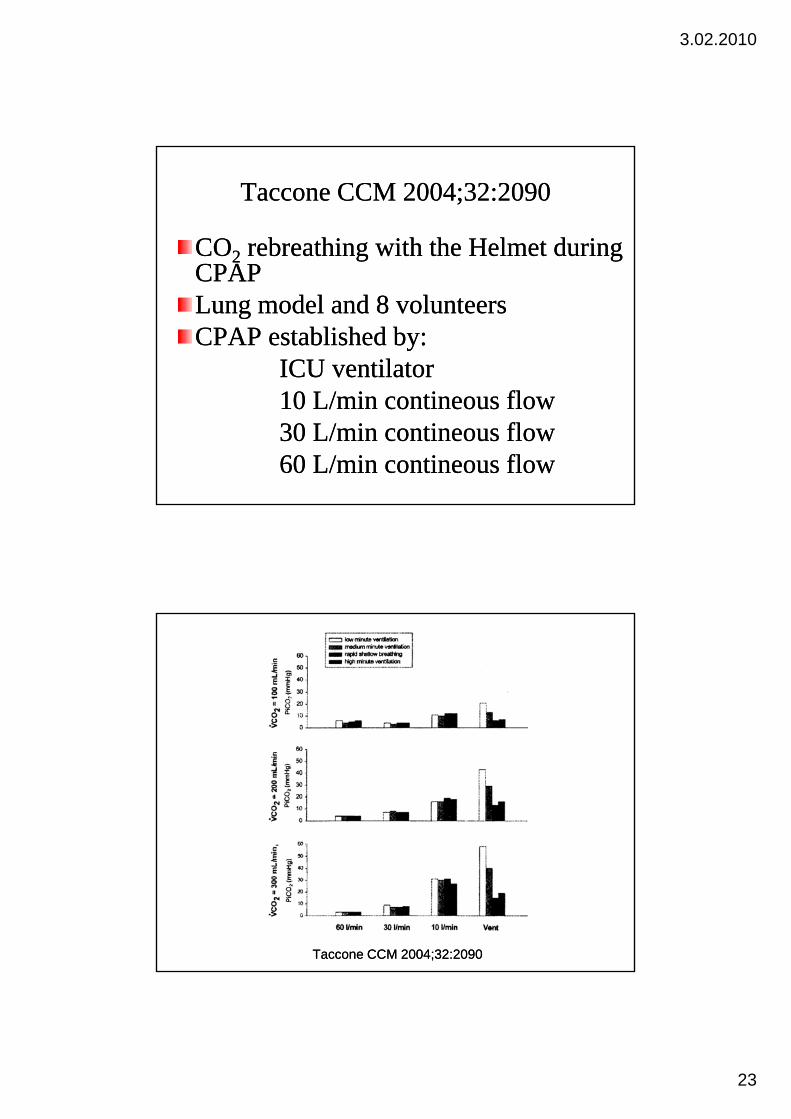
Taccone CCM 2004;32:2090Taccone CCM 2004;32:2090
COCO22 rebreathing with the Helmet during rebreathing with the Helmet during CPAPCPAPCPAPCPAPLung model and 8 volunteers Lung model and 8 volunteers CPAP established by:CPAP established by:
ICU ventilatorICU ventilator10 L/min contineous flow10 L/min contineous flow30 L/min contineous flow30 L/min contineous flow60 L/min contineous flow60 L/min contineous flow
Taccone CCM 2004;32:2090Taccone CCM 2004;32:2090
3.02.2010
24
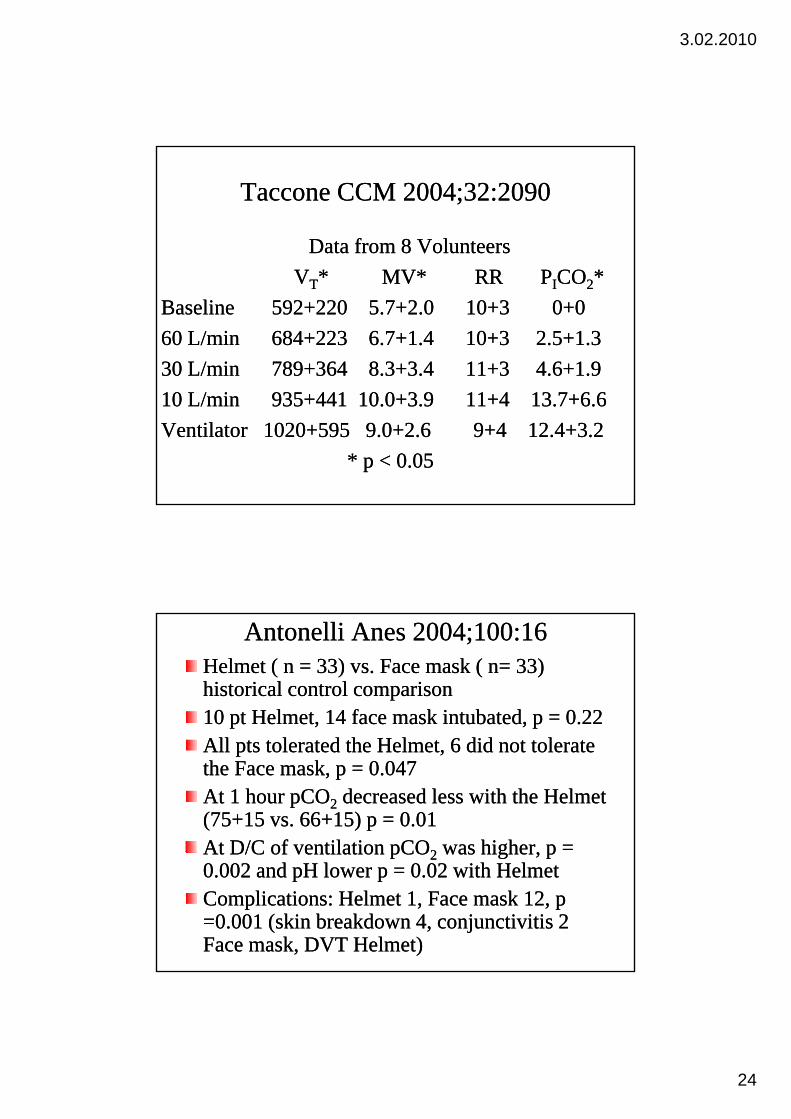
Taccone CCM 2004;32:2090Taccone CCM 2004;32:2090
Data from 8 Volunteers Data from 8 Volunteers VVTT* MV* RR P* MV* RR PIICOCO22**
Baseline 592+220 5.7+2.0 10+3 0+0Baseline 592+220 5.7+2.0 10+3 0+060 L/min 684+223 6.7+1.4 10+3 2.5+1.360 L/min 684+223 6.7+1.4 10+3 2.5+1.330 L/min 789+364 8.3+3.4 11+3 4.6+1.930 L/min 789+364 8.3+3.4 11+3 4.6+1.910 L/min 935+441 10.0+3.9 11+4 13.7+6.610 L/min 935+441 10.0+3.9 11+4 13.7+6.6Ventilator 1020+595 9.0+2.6 9+4 12.4+3.2Ventilator 1020+595 9.0+2.6 9+4 12.4+3.2
* p < 0.05* p < 0.05
Antonelli Anes 2004;100:16Antonelli Anes 2004;100:16Helmet ( n = 33) vs. Face mask ( n= 33) Helmet ( n = 33) vs. Face mask ( n= 33) historical control comparisonhistorical control comparison10 pt Helmet, 14 face mask intubated, p = 0.2210 pt Helmet, 14 face mask intubated, p = 0.22All pts tolerated the Helmet, 6 did not tolerate All pts tolerated the Helmet, 6 did not tolerate the Face mask, p = 0.047the Face mask, p = 0.047At 1 hour pCOAt 1 hour pCO22 decreased less with the Helmet decreased less with the Helmet (75+15 vs. 66+15) p = 0.01(75+15 vs. 66+15) p = 0.01At D/C of ventilation pCOAt D/C of ventilation pCO22 was higher p =was higher p =At D/C of ventilation pCOAt D/C of ventilation pCO22 was higher, p was higher, p 0.002 and pH lower p = 0.02 with Helmet0.002 and pH lower p = 0.02 with HelmetComplications: Helmet 1, Face mask 12, p Complications: Helmet 1, Face mask 12, p =0.001 (skin breakdown 4, conjunctivitis 2 =0.001 (skin breakdown 4, conjunctivitis 2 Face mask, DVT Helmet)Face mask, DVT Helmet)
3.02.2010
25
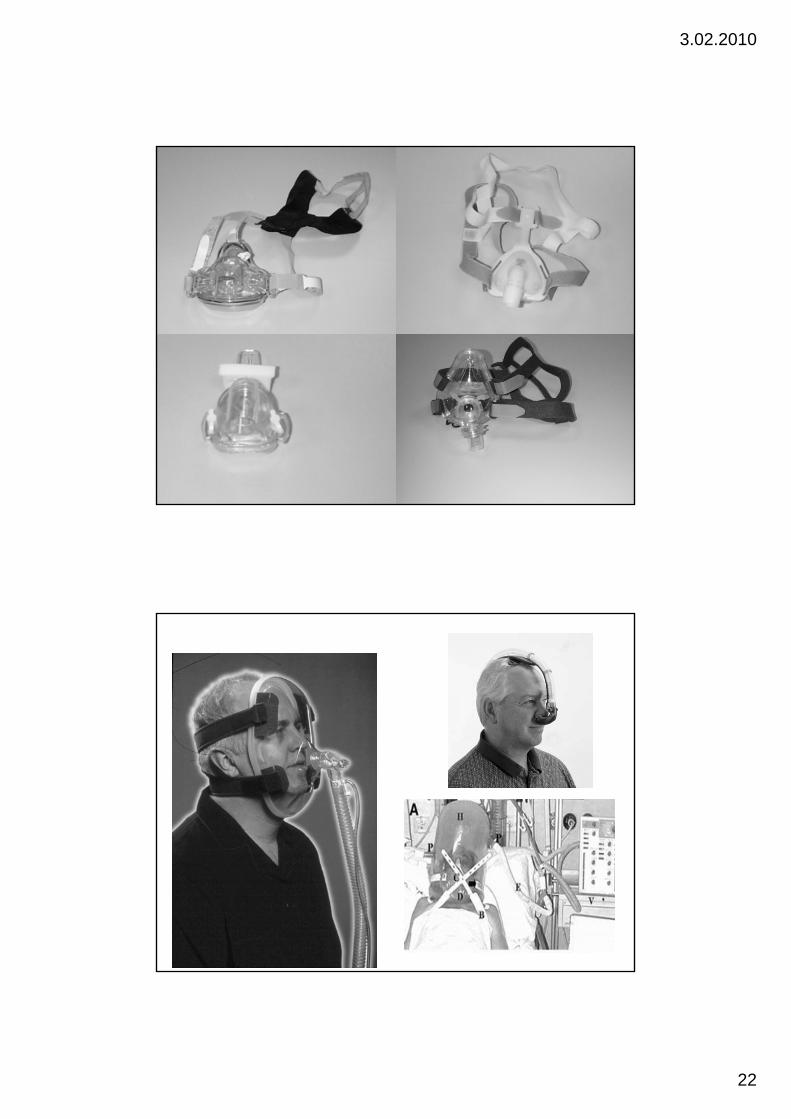
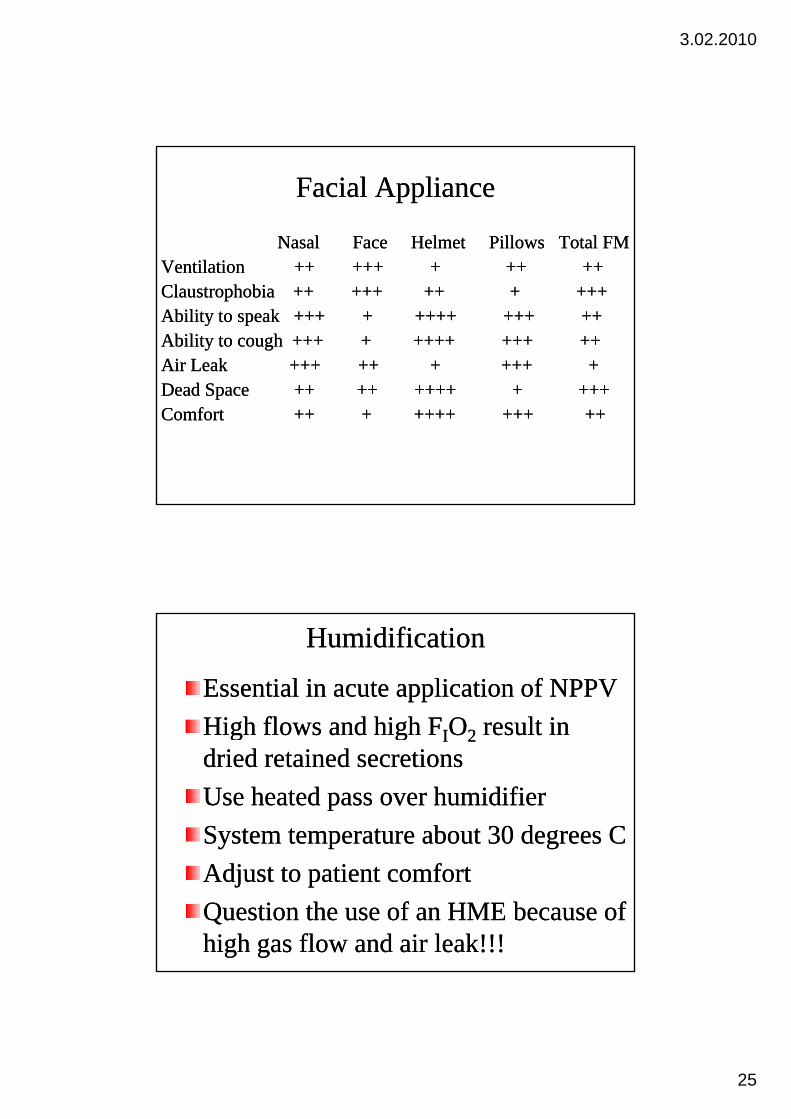
Facial ApplianceFacial Appliance
NasalNasal Face Helmet Pillows Total FMFace Helmet Pillows Total FMVentilationVentilation ++ +++ + ++ ++++ +++ + ++ ++VentilationVentilation ++ +++ + ++ ++++ +++ + ++ ++Claustrophobia ++ +++Claustrophobia ++ +++ ++ + +++ ++ + +++ Ability to speak +++ + ++++ +++ ++Ability to speak +++ + ++++ +++ ++Ability to cough +++ + ++++ +++ ++Ability to cough +++ + ++++ +++ ++Air LeakAir Leak +++ ++ + +++ ++++ ++ + +++ +D d SD d S ++ ++++ ++ ++++ + +++++++ + +++Dead Space Dead Space ++ ++++ ++ ++++ + +++++++ + +++Comfort ++ + ++++ +++ ++Comfort ++ + ++++ +++ ++
HumidificationHumidification
Essential in acute application of NPPVEssential in acute application of NPPVHigh flows and high FHigh flows and high FIIOO22 result inresult inHigh flows and high FHigh flows and high FIIOO22 result in result in dried retained secretionsdried retained secretionsUse heated pass over humidifierUse heated pass over humidifierSystem temperature about 30 degrees CSystem temperature about 30 degrees CAdjust to patient comfortAdjust to patient comfortQuestion the use of an HME because of Question the use of an HME because of high gas flow and air leak!!!high gas flow and air leak!!!
3.02.2010
26
Ventilator SettingsVentilator Settings
PEEP PEEP -- initially zeroinitially zeroPeak pressurePeak pressure -- 5 cmH5 cmH OOPeak pressure Peak pressure -- 5 cmH5 cmH22O O Volume Volume -- 100100--200 mL200 mLAdjust the ventilator from these Adjust the ventilator from these basic settings based on the patients basic settings based on the patients g pg presponse and the goals of therapy!response and the goals of therapy!Strap the mask only when the Strap the mask only when the patient is comfortable!patient is comfortable!
Ventilator SettingsVentilator Settings
PEEP 3PEEP 3--8 cmH8 cmH22O to offset autoO to offset auto--PEEPPEEPPeak pressure Peak pressure << 20 cmH20 cmH22OOTidal Volume 300Tidal Volume 300--500 mL500 mLInspiratory time < 1.0 secInspiratory time < 1.0 sec
Gastric opening pressure 20Gastric opening pressure 20--25 cmH25 cmH22OO
3.02.2010
27
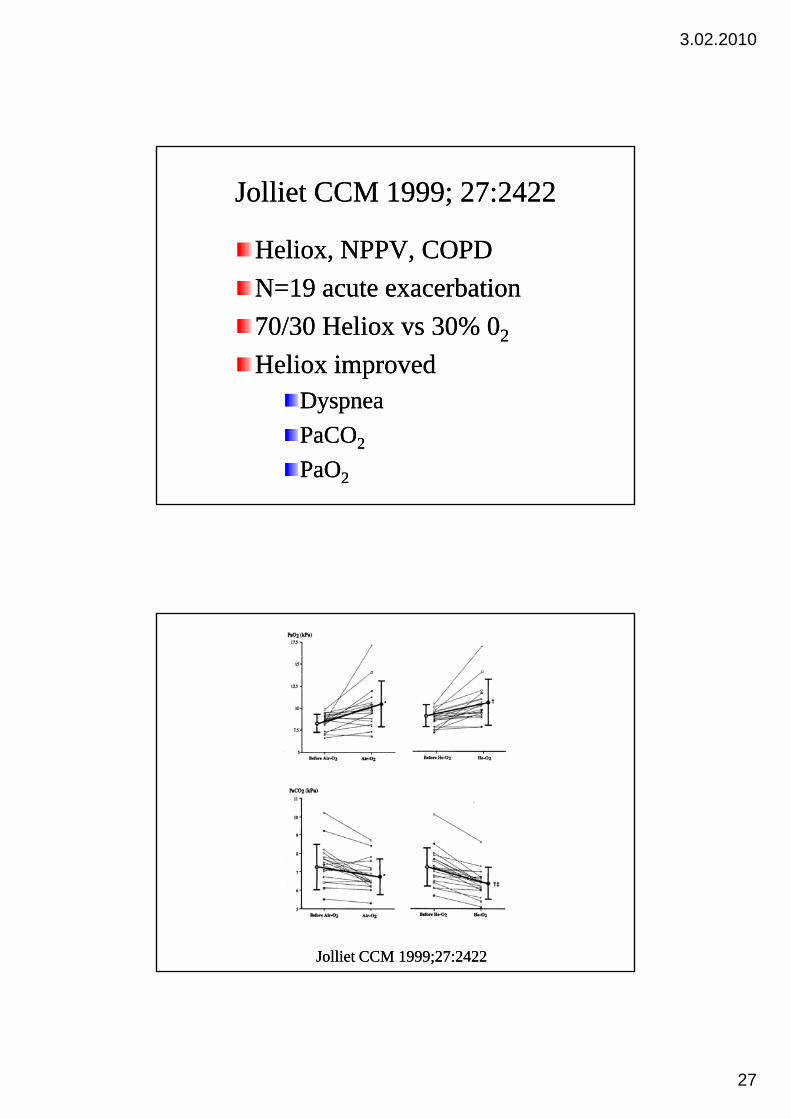
Jolliet CCM 1999; 27:2422Jolliet CCM 1999; 27:2422
Heliox, NPPV, COPDHeliox, NPPV, COPDN=19 acute exacerbationN=19 acute exacerbation70/30 Heliox vs 30% 070/30 Heliox vs 30% 022
Heliox improvedHeliox improvedDyspnea Dyspnea PaCOPaCO22
PaOPaO22
Jolliet CCM 1999;27:2422Jolliet CCM 1999;27:2422
3.02.2010
28
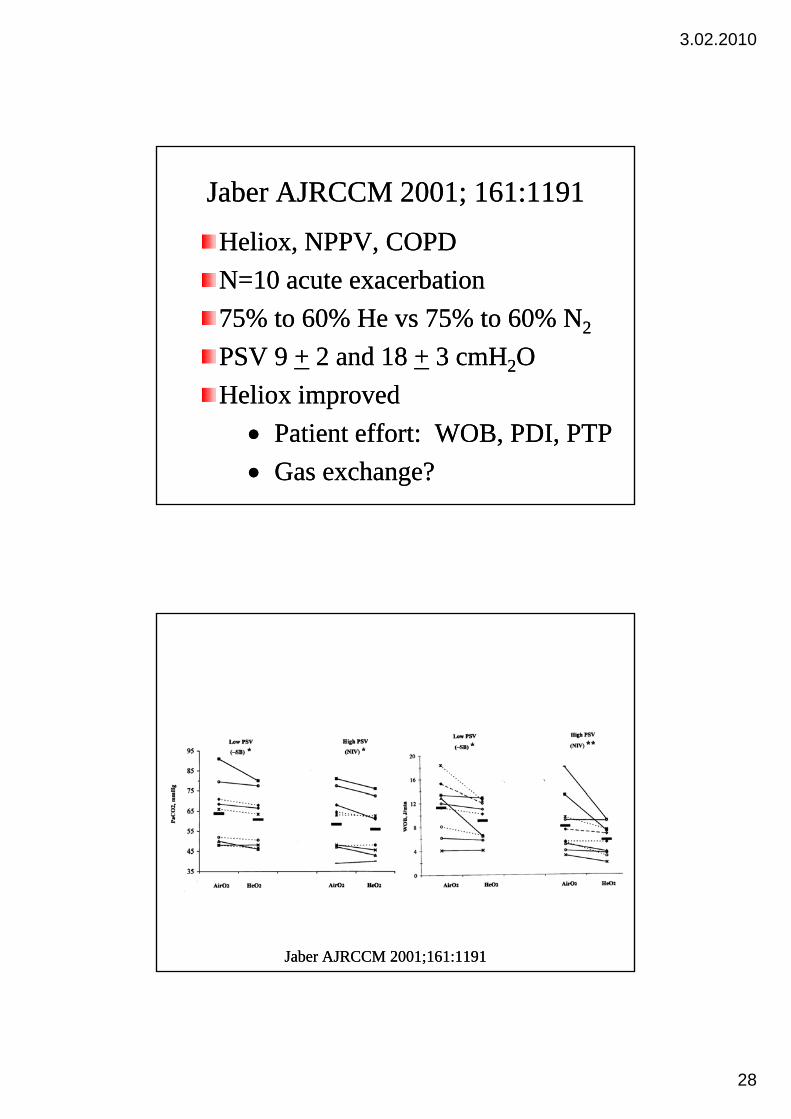
Jaber AJRCCM 2001; 161:1191Jaber AJRCCM 2001; 161:1191
Heliox, NPPV, COPDHeliox, NPPV, COPDN=10 acute exacerbationN=10 acute exacerbation75% to 60% He vs 75% to 60% N75% to 60% He vs 75% to 60% N22
PSV 9 PSV 9 ++ 2 and 18 2 and 18 ++ 3 cmH3 cmH22OOli i dli i dHeliox improvedHeliox improved•• Patient effort: WOB, PDI, PTPPatient effort: WOB, PDI, PTP•• Gas exchange?Gas exchange?
Jaber AJRCCM 2001;161:1191Jaber AJRCCM 2001;161:1191
3.02.2010
29
Jolliet CCM 2003;31:878Jolliet CCM 2003;31:878
RCT RCT -- COPD ICU patients receiving COPD ICU patients receiving NPPV ith ith t H li llNPPV ith ith t H li llNPPV with or without Heliox all NPPV with or without Heliox all ventilator settings sameventilator settings same123 pts, 71+10 yrs,123 pts, 71+10 yrs,Intubation rate 20% vs 13% HelioxIntubation rate 20% vs 13% HelioxLOS ICU 6.2LOS ICU 6.2++5.6 vs 5.15.6 vs 5.1++4 Heliox4 HelioxLOS Hosp 19+12 vs 13+6 Heliox p<0.5LOS Hosp 19+12 vs 13+6 Heliox p<0.5Hosp cost lower by $3,348/pt with HelioxHosp cost lower by $3,348/pt with Heliox
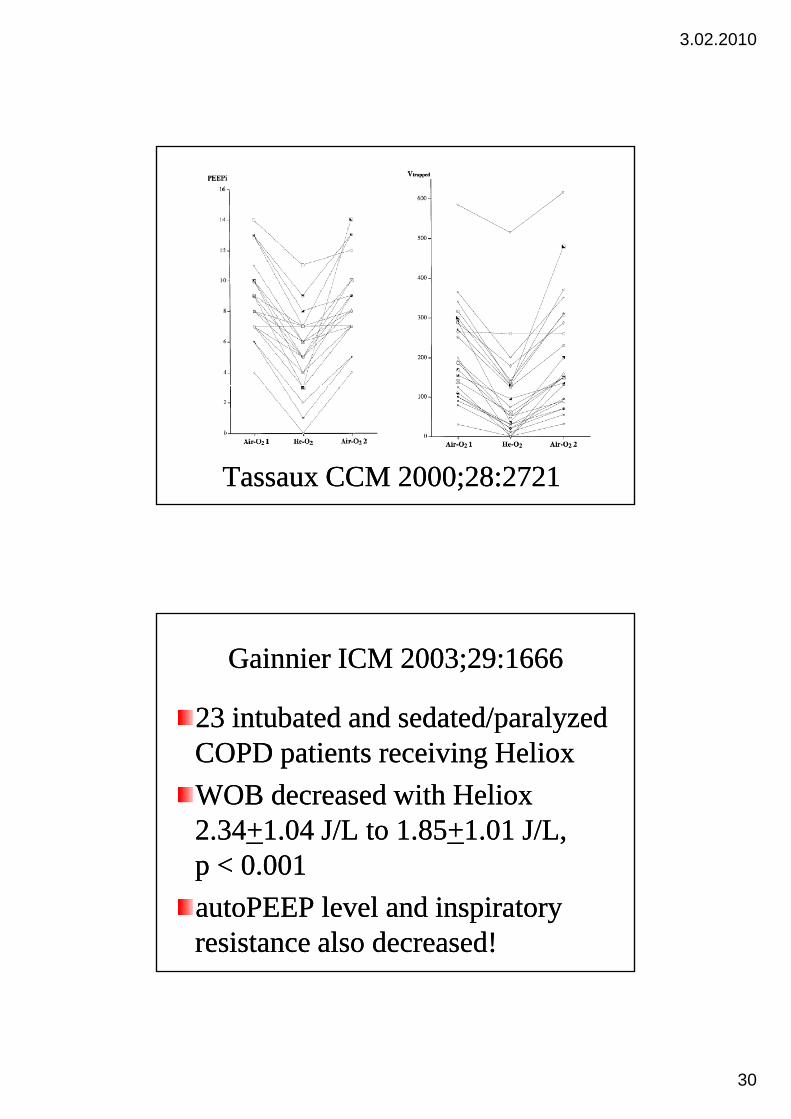
Tassaux CCM 2000;28:2721Tassaux CCM 2000;28:2721
Heliox enhanced lung empting in 23 Heliox enhanced lung empting in 23 i b di b d l b hil b hiintubated nonintubated non--spontaneously breathing spontaneously breathing COPD patientsCOPD patientsTrapped lung volume decreased 116 ml Trapped lung volume decreased 116 ml (54%)(54%)autoPEEP decreased 4 cm HautoPEEP decreased 4 cm H22O (45%)O (45%)Peak airway pressure decreased 5 Peak airway pressure decreased 5 cmHcmH22O (17%)O (17%)
3.02.2010
30
Tassaux CCM 2000;28:2721Tassaux CCM 2000;28:2721
Gainnier ICM 2003;29:1666Gainnier ICM 2003;29:1666
23 intubated and sedated/paralyzed 23 intubated and sedated/paralyzed p yp yCOPD patients receiving HelioxCOPD patients receiving HelioxWOB decreased with Heliox WOB decreased with Heliox 2.342.34++1.04 J/L to 1.851.04 J/L to 1.85++1.01 J/L, 1.01 J/L, p < 0.001p < 0.001autoPEEP level and inspiratory autoPEEP level and inspiratory resistance also decreased!resistance also decreased!
3.02.2010
31
Jolliet ICM 2003;29:1442Jolliet ICM 2003;29:1442
10 patients with COPD, invasively 10 patients with COPD, invasively ventilated sedated/paralyzedventilated sedated/paralyzedventilated, sedated/paralyzedventilated, sedated/paralyzedStudied the effect of Heliox and PEEP on Studied the effect of Heliox and PEEP on autoPEEPautoPEEPHeliox and PEEP equally reduced trapped Heliox and PEEP equally reduced trapped gas (215 ml) and autoPEEP (4.4 cmHgas (215 ml) and autoPEEP (4.4 cmH22O)O)Heliox also reduced inspiratory and Heliox also reduced inspiratory and expiratory resistance and plateau pressureexpiratory resistance and plateau pressure
Diehl CCM 2003;31:1415Diehl CCM 2003;31:1415
COPD patients weaningCOPD patients weaningHeliox vs OHeliox vs O22/N/N22 for 20 min before extubationfor 20 min before extubationHeliox vs OHeliox vs O22/N/N22 for 20 min before extubation, for 20 min before extubation, effect on Work of breathingeffect on Work of breathingIn both situation 29+4% OIn both situation 29+4% O22 administeredadministeredNo modification of the ventilatory patternNo modification of the ventilatory patternBut Heliox reduced:But Heliox reduced:–– WOB 1.44WOB 1.44++0.72 vs 1.130.72 vs 1.13++0.50 J/L0.50 J/L–– PEEPPEEPA A 2.92.9++2.1 vs 2.2 2.1 vs 2.2 ++1.81.8
3.02.2010
32
Who Who –– Indications for NPPVIndications for NPPVUndisputed indications Undisputed indications
Acute Exacerbation of COPDAcute Exacerbation of COPDAcute Cardiogenic Pulmonary EdemaAcute Cardiogenic Pulmonary Edema
General Indications for UseGeneral Indications for UseP b i H bi R i F ilP b i H bi R i F ilPost extubation Hypercarbic Respiratory FailurePost extubation Hypercarbic Respiratory FailureHypoxemic Respiratory Failure in :Hypoxemic Respiratory Failure in :
-- Immunosurpressed PatientsImmunosurpressed Patients-- Patients Awaiting TransplantationPatients Awaiting Transplantation-- Patients Post Lung ResectionPatients Post Lung Resection
Patients with DNI StatusPatients with DNI StatusAcute Hypercapnic Respiratory Failure as a Result ofAcute Hypercapnic Respiratory Failure as a Result ofAcute Hypercapnic Respiratory Failure as a Result of Acute Hypercapnic Respiratory Failure as a Result of
Neurological or Neuromuscular DiseaseNeurological or Neuromuscular DiseaseControversial IndicationsControversial Indications
Post Post ––Extubation Hypoxemic Respiratory FailureExtubation Hypoxemic Respiratory FailureAcute Lung InjuryAcute Lung InjuryAcute Respiratory Distress SyndromeAcute Respiratory Distress SyndromeAsthmaAsthma
Thank YouThank YouThank YouThank You