north bristol nhs trust orthotic service protocol bristol nhs nhs trust north bristol nhs trust...
TRANSCRIPT
North Bristol NHS
NHS Trust
North Bristol NHS Trust
Orthotic Services
Good Practice Guidance
North Bristol NHS Trust
Royal United Hospital NHS Trust
Mendip Primary Care Trust
Bath & North East Somerset Primary Care Trust
South Gloucestershire Primary Care Trust
Bristol North Primary Care Trust
North Somerset Primary Care Trust
Version 1.2 : August 2004
Version 1.2 – August 2004
Contents
Section A
Statement Orthotic Service Standards Fitting and footwear Developments Activity Communication Appointment times
Section B
Record keeping Essential information Legal implications Referral for assessment and advice Information required Multi-disciplinary clinics record Access legal implications Ownership Patient held record Computer held records
Section C
The Patient
Section D
Orthotist Clinician guidelines Individualised approach Informed consent Assessment Transfer of core Communication with patients and carers Patient and Clinician safety Equipment safety
Section E
Patient core information
Page 1
Version 1.2 – August 2004
Section A
Statement The following guidelines represent the aims of the service and will require the help and support of the service providers clinicians, referrers and product suppliers if they are to be achieved. They are intended to reflect good practice to ensure that the practitioners involved with delivering orthotic care within the North Bristol Orthotics Service achieve and maintain the highest standards of professionalism and effectiveness in patient care whilst achieving best value for money
Orthotic Service Standards The National Agreement for the Provision of Orthoses and the supporting agreements, provide national standards for maximum delivery times for the provision of orthoses, however the service has established the following minimum standards for other core product ranges.
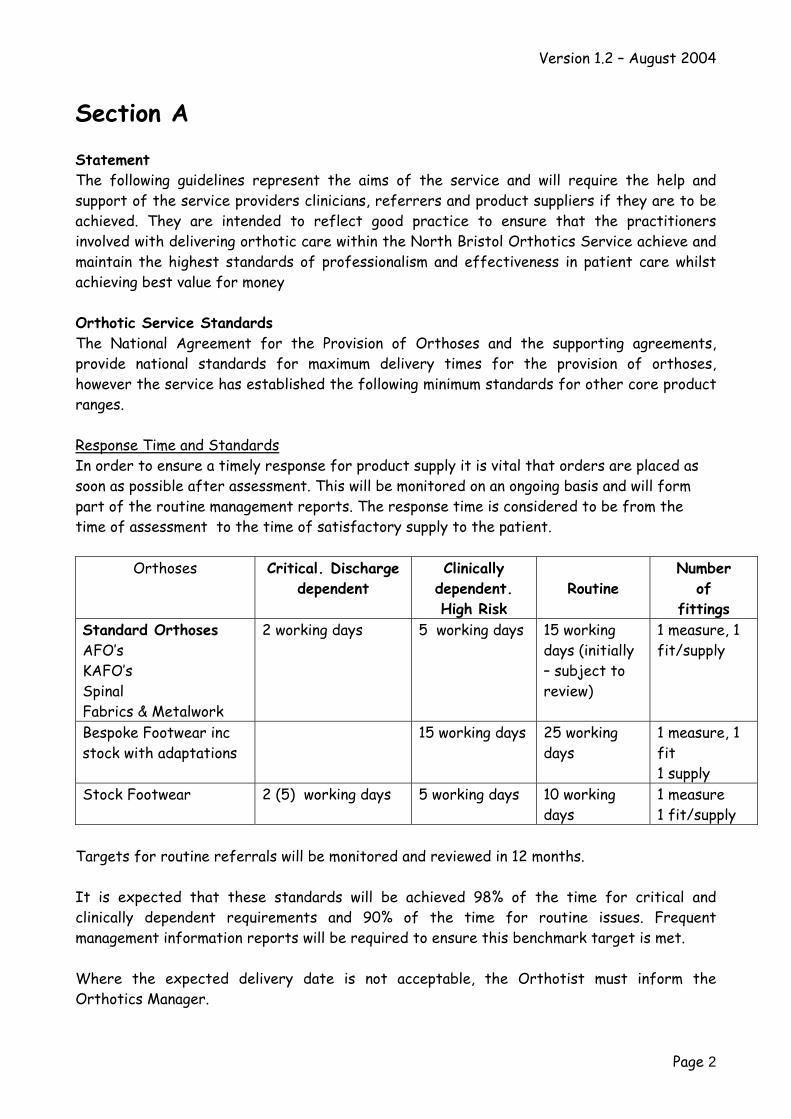
Response Time and Standards In order to ensure a timely response for product supply it is vital that orders are placed as soon as possible after assessment. This will be monitored on an ongoing basis and will form part of the routine management reports. The response time is considered to be from the time of assessment to the time of satisfactory supply to the patient.
Orthoses Critical. Discharge dependent
Clinically dependent. High Risk
Routine Number
of fittings
Standard Orthoses AFO’s KAFO’s Spinal Fabrics & Metalwork
2 working days 5 working days 15 working days (initially – subject to review)
1 measure, 1 fit/supply
Bespoke Footwear inc stock with adaptations
15 working days 25 working days
1 measure, 1 fit 1 supply
Stock Footwear 2 (5) working days 5 working days 10 working days
1 measure 1 fit/supply
Targets for routine referrals will be monitored and reviewed in 12 months.
It is expected that these standards will be achieved 98% of the time for critical and clinically dependent requirements and 90% of the time for routine issues. Frequent management information reports will be required to ensure this benchmark target is met.
Where the expected delivery date is not acceptable, the Orthotist must inform the Orthotics Manager.
Page 2
Version 1.2 – August 2004
For some Critical Discharge Dependant patients temporary arrangements would be acceptable.
Fitting of footwear It is expected that 75% of patients receiving stock footwear be fitted successfully with 1 fitting and 1 initial assessment (i.e. two appointments) and 60% of patients to be fitted with bespoke footwear within 2 fittings plus initial assessment. This will be reviewed in 12 months
In the exceptional circumstances where the quality of an orthosis is not acceptable to the Orthotist or the patient within 2 fittings, the Orthotist must bring this to the attention of the Orthotics Manager.
Individual patients who present with complex conditions or multifaceted problems that may take some time to resolve should be discussed with clinical team members and specific proposal for action to be agreed with the patient/team prior to commencing work on the orthoses. This should be indicated on the referral sheet (Orthotist’s comment).
Developments In partnership with Trusts for whom orthotic services are provided, the orthotic team will look to promote a number of developments. These will be agreed with all parties and may be added to this Guide as they evolve.
1. Development of outcome measurement and quality reviews
Activity Most of the patients are seen as outpatients, usually by appointment.
In addition, there is demand from consultant outpatient clinics, referrals from wards, frequently to facilitate discharge. Domiciliary visits may, from time to time, be required but will be infrequent and determined on a case by case basis.
Page 3
Version 1.2 – August 2004
Communication The Orthotics personnel that are employed by the service meet regularly as a team as agreed. All Orthotists and a relevant Manager, if appropriate, as well as representatives from the relevant clinical areas are invited to regular meetings (Trust specific) in order to promote professional practice and discuss issues pertinent to the group. This forum assists with the on-going development of the service.
Appointment Times Each service will have its own appointment booking system, however members aim to provide the following appointment times in order to provide adequate time for patient assessment and clinical record keeping.
Standard Appointment: CastingAssessment Multi Disciplinary Team Clinics
20minutes 40 minutes
20minutes 40minutes
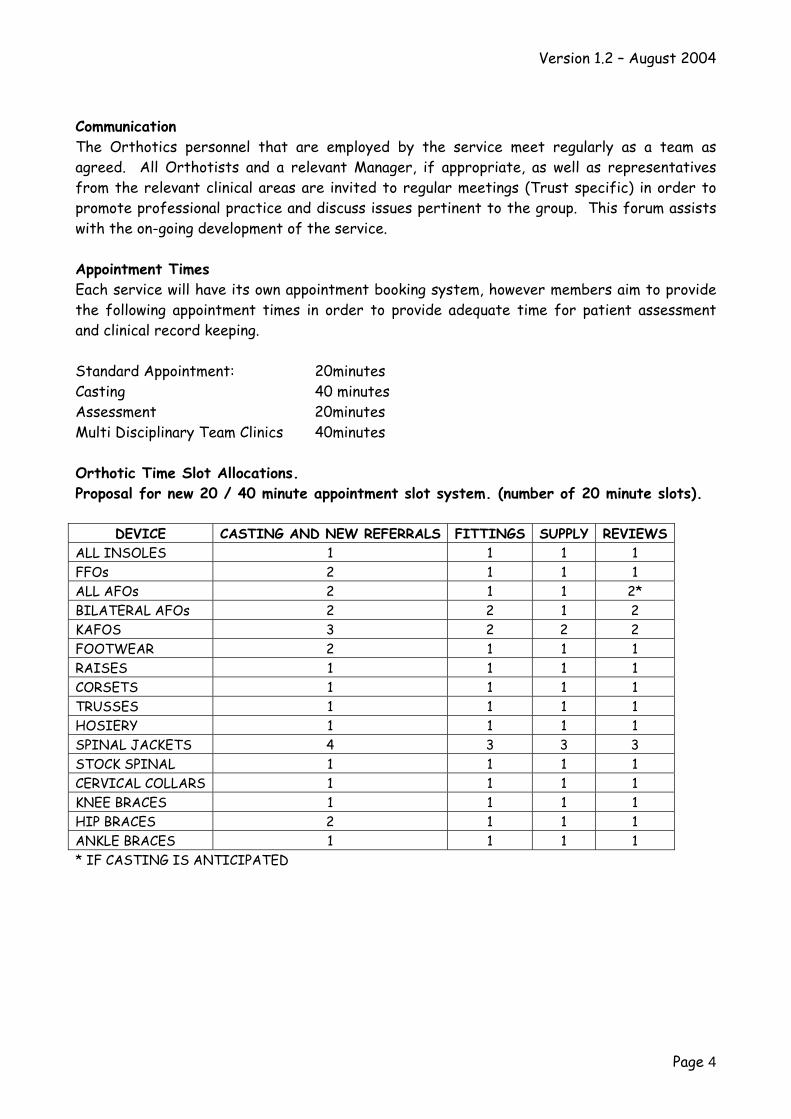
Orthotic Time Slot Allocations. Proposal for new 20 / 40 minute appointment slot system. (number of 20 minute slots).
DEVICE CASTING AND NEW REFERRALS FITTINGS SUPPLY REVIEWS ALL INSOLES 1 1 1 1 FFOs 2 1 1 1 ALL AFOs 2 1 1 2* BILATERAL AFOs 2 2 1 2 KAFOS 3 2 2 2 FOOTWEAR 2 1 1 1 RAISES 1 1 1 1 CORSETS 1 1 1 1 TRUSSES 1 1 1 1 HOSIERY 1 1 1 1 SPINAL JACKETS 4 3 3 3 STOCK SPINAL 1 1 1 1 CERVICAL COLLARS 1 1 1 1 KNEE BRACES 1 1 1 1 HIP BRACES 2 1 1 1 ANKLE BRACES 1 1 1 1 * IF CASTING IS ANTICIPATED
Page 4
Version 1.2 – August 2004
Section B
Record Keeping
Record keeping is an integral part of orthotic practice, which should aid the rehabilitation and care process. Protocols on Clinical Records are attached in the Appendix at the end of this guide.
DNAs & FTAs The Trusts will work with Orthotic contractor towards establishing protocols designed to minimise the incidence of missed appointments, in line with Trust-wide practice for other out-patient services.
Multi-disciplinary Clinics records When a patient is to be seen by the Orthotist and at least one other Clinician the content of the clinical record will be jointly decided and agreement will be made as to where the notes should be kept. The appropriate Clinicians will scribe and all Clinicians will sign the record.
Because clinics are held usually to allow multi-disciplinary consideration of complex difficult cases a 45-minute appointment length may be allowed.
Access Legal Implications The Access to Health Records Act 1990 gives patients the right of access to manual health records written about them since 1 November 1991. The Data Protection Act 1998, which conforms to the European Data Protection Directive 95/46/EC, also gives access to their computer held records. The system for dealing with applications for access is explained in the Guide to the Access to Health Records Act 1990.
Ownership The NHS owns patient records, however practitioners (including service providers) have a duty to protect the confidentiality of those records. (Reference to Data Protection Act 1998, and Caldicott)
Patient- Held Records Patients and parents frequently hold their own health care records.
Computer Held Records Computer held records are easier to read, require less clerical input, and reduce the need for duplication and can improve inter-professional communications.
Page 5
Version 1.2 – August 2004
Section C
The Patient
These guidelines have been taken from EmPower’s user charter and the service members, where possible will strive to achieve these recommendations.
Respect for the patient as an individual is central to all aspects of the treatment of care and should be demonstrated at all times.
There should be regular opportunities for users to consult with staff and commissioners. Users should be given information about the equipment available and developments to their local services.
As recommended by emPOWER consideration should be given to 5C’s when prescribing orthoses:
EmPOWER Empower believes that people who use disability equipment have a number of rights. This documents pulls together those rights, published previously in emPOWER’s Prostheses & Orthoses and Wheelchair Charters and emPOWER’s Millennium Agenda for Independence. Users also, of course, have responsibilities.
Rights include: User Involvement There should be regular opportunities for users to consult with staff and commissioners, ideally through a user consultative committee.
Information Users should have a right to information about the equipment available and about developments in their local Trust and Primary Care Trust. If appropriate users should be able to test whether a piece of equipment would meet their needs.
Choice The user should have a freedom of choice with regards to the type and style of equipment.1
This freedom of choice should encompass aspects such as a choice of colour and design. The user should be able to request a second opinion or out of area treatment.
Comfort The equipment prescribed should provide adequate support and comfort to enable the user to achieve optimal function and independence.
1 The NHS endeavours to abide by this within clinical/functional/value for money boundaries.
Page 6
Version 1.2 – August 2004
Capability The equipment must be appropriate to the individual lifestyle and other requirements. It should also be mechanically safe and require relatively little maintenance.
Cosmesis Wherever possible equipment should be cosmetically acceptable to the user and when good cosmesis cannot be achieved, the reasons are fully explained to the user.
Caring Caring professionals provide the catalyst to a good service. Training should be provided for all staff in order that they understand the needs of disabled people.
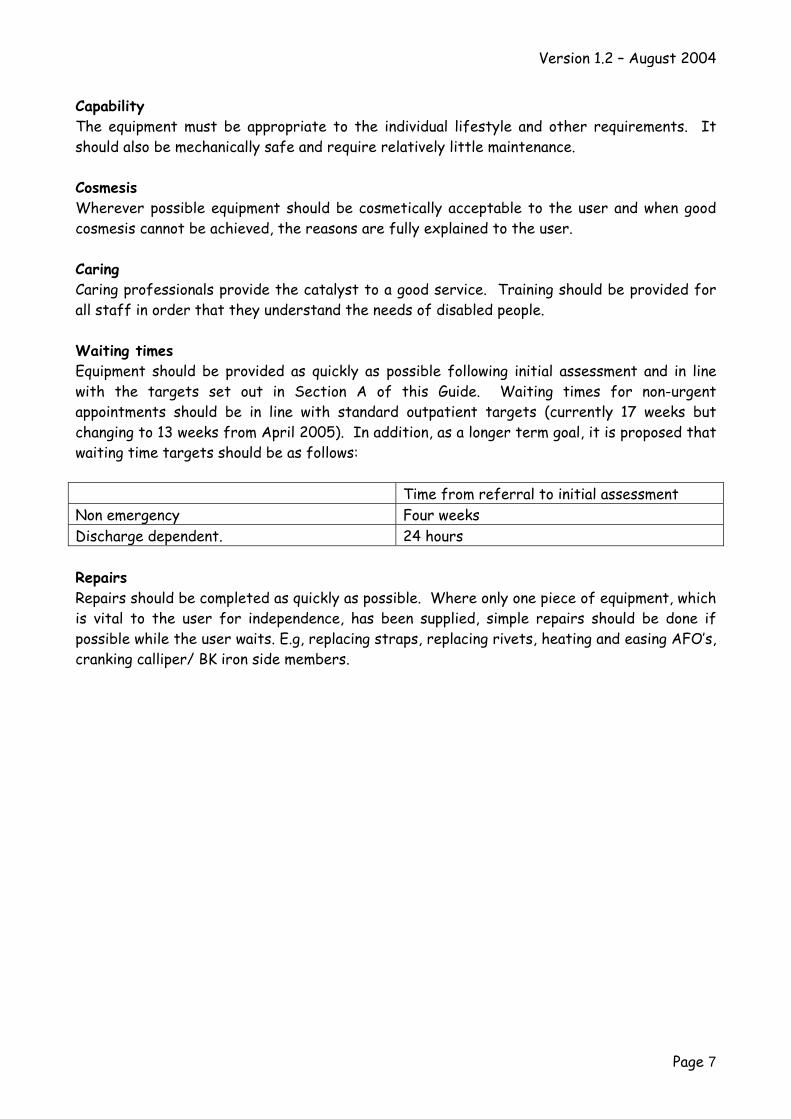
Waiting times Equipment should be provided as quickly as possible following initial assessment and in line with the targets set out in Section A of this Guide. Waiting times for non-urgent appointments should be in line with standard outpatient targets (currently 17 weeks but changing to 13 weeks from April 2005). In addition, as a longer term goal, it is proposed that waiting time targets should be as follows:
Time from referral to initial assessment Non emergency Four weeks Discharge dependent. 24 hours
Repairs Repairs should be completed as quickly as possible. Where only one piece of equipment, which is vital to the user for independence, has been supplied, simple repairs should be done if possible while the user waits. E.g, replacing straps, replacing rivets, heating and easing AFO’s, cranking calliper/ BK iron side members.
Page 7
Version 1.2 – August 2004
Section D
Orthotist / Clinician Guidelines
Individualised approach Respect for the patient as an individual is central to all aspects of the orthotic relationship and is demonstrated at all times.
The Clinician responds to individuals’ lifestyle, cultural beliefs and practices. Guidance: This criterion reflects the need for Clinicians to respect and respond actively to every patient as an individual. Factors affecting this include social, occupational, recreational and economic commitments and are regardless of background or beliefs. For example, to respect the Muslim holy day Friday appointments could be avoided. Single sex treatment facilities should be offered where possible.
The Clinician is courteous and considerate.
The patient is addressed by the name of their choice.
The patient is informed of the name of the Clinician responsible for their episode of care.
The patient is made aware of the role of any Clinician involved in their care. Guidance: It is important that patients are aware if an orthotic assistant or student is treating them.
Informed consent National guidelines laid down in Consent to Treatment and all Trust guidelines must be adhered to.
The patient’s consent is obtained before starting any examination/treatment.
Treatment options, including significant benefits, risks and side effects, are discussed with the patient.
The patient is given the opportunity to ask questions whenever required.
Guidance: patients may need time to digest information and be given opportunities to ask questions on a number of occasions.
The patient is informed of their right to decline an Orthoses at the start without it prejudicing their future care.
Page 8
Version 1.2 – August 2004
If the patient declines orthotic treatment, this is documented in the patient’s record, together with the reasons, if these are known and the referrer should be informed.
The patient is informed that they may be treated by a student and given the right to decline and to be treated by a qualified Clinician. Adherence of appropriate trust guidelines, which relate to treatment by a student, will be required.
The patient’s consent to the treatment plan is documented in the patient’s record.
Opcare draft policy on Right to Privacy is attached at the end of this policy document
Assessment In order to deliver effective care, information relating to treatment options is identified, based on the best available evidence using a range of different sources. Guidance: there will be a range of different sources for obtaining this information including the patient, relatives / carers, other healthcare professionals, library facilities, electronic sources, journals, Trust policies.
The Clinician considers and critically evaluates information about effective interventions relating to the patient’s condition. Sources may include:
a research b clinical guidelines, effectiveness bulletins and other summaries of evidence of
effectiveness c clinical interest and occupational groups d national guidance e.g. National Service Frameworks e Trust standards and protocols f information derived from the use of outcome measures g patient organisations / groups e.g. The Stroke Association h expert opinion
The service will develop a basis for auditable outcome measurement.
Communication with patients and carers
Clinicians communicate effectively with patients and/or their carers/relatives. The Clinician uses active listening skills, providing opportunities for the patient to
communicate effectively. Clinicians shall respect the rights, dignity and individual sensibilities of every patient Clinicians communicate openly and honestly with patients. Guidance: in some circumstances, for example terminal care, an approach to
communication may need to be agreed within the team.
Page 9
Version 1.2 – August 2004
All communication, written and verbal, is clear, unambiguous and easily understood by the recipient.
Methods of communication are modified to meet the needs of the patient. Guidance: communication should take account of an individual’s culture and language. The use of alternative forms of communication such as signing, video/audio cassettes and pictures should be considered.
The Clinician assesses the recipient’s understanding of the information given. Communication of a sensitive nature is undertaken in a private environment. Information is available on condition-specific support groups and networks
Guidance: the Clinician should know how the information could be obtained if it is not readily available.
Permission is sought from the patient before discussing confidential details with carers, friends or relatives.
Patient and Clinician safety
Patients are treated in an environment that is safe for patients, Clinicians and carers. A risk assessment to be carried out in line with trust policy. Action is taken on the results of the risk assessment; to minimise any hazards
identified. Patients receiving treatment are made aware of how to summon assistance. The Clinician is able to summon urgent assistance when required as per agreed
procedure. Infection control procedures are followed in accordance with Trust policy
Adverse events are reported in accordance with Trust policy.
Equipment safety
All equipment is safe, fit for purpose and ensures patient, carer and Clinician safety. Visual and physical safety checks are made of equipment prior to its use or issuing to
patients. Equipment is used according to manufacturers’ instructions Equipment is cleaned according to manufacturers’ instructions and infection control
policies. Any equipment faults identified are reported Faulty equipment is taken out of use immediately The Clinician acts on new guidance about equipment safety The risks associated with using electrical equipment in a patient’s home are minimised. The patient is given instructions on the safe use of any equipment issued.
Page 10
Version 1.2 – August 2004
Section E
Advice to Professionals and Entitlement Of Patient for Orthotic Equipment Provision
This guidance will be reviewed on a bi-annual basis or as and when local or national guidance is issued. The North Bristol Orthotics Service continually develop and review the information ensuring it is relevant and user friendly.
PROTOCOL FOR SUPPLY OF ORTHOSES
Orthotic Referral
Referral is made to the Orthotic Service on the new Referral form (attached in the appendix to this Guide) and should include all details as requested. The information will assist the orthotist in his assessment of the patient and in the decision of the most appropriate orthoses for the patients need. This may be different to that suggested by the clinician or visualised by the patient.
Stabilisation/Orthotic intervention
Requests for orthoses can be a one off for an acute episode or before or after surgery. It may be for long term use with a period of time specified for repair and replacement. It is the responsibility of the orthotist to ensure the product supplied is appropriate and best value. If the orthotist feels that the previous provision is now not appropriate or there has been a change in the condition of the patient, this will be referred back to the original referrer for a re-assessment by them. If the original referrer in the case of a consultant, has discharged the patient, then the request for re-assessment or up to date information will be requested from the patients G.P.
Orthoses will not be supplied where:
There is no specific clinical or biomechanical need
The need has passed and the patient no longer requires replacements
The orthoses is being supplied as a placebo
They are being supplied for only socio-economic reasons
No orthoses should be supplied because of historical practice.
Page 11
Version 1.2 – August 2004
If the need for the orthoses is solely for sporting purposes, the patient will be invoiced for the product.
It is a product that is readily available from retail outlets.
Private Patients
Consultants must make it clear on all correspondence if the patient they are seeing is a private patient. The designated person within each Trust with responsibility for private patients, should be contacted to clarify the situation. Local policies and procedures should be adhered to in respect of private patients.
FOOTWEAR
The footwear provided may be made to measure or ready made/stock footwear, depending upon the particular foot problems of the patient. While every effort is made to supply shoes or boots that are cosmetically acceptable, this is not fashion footwear and must always be suitable for the patient’s foot shape and condition and meet the medical needs.
Where standard footwear is required for adaptation, the patient will be required to provide their own shoes which will then be adapted free of charge by the service.
Entitlement
Adults
The usual allocation is to have two pairs of boots or shoes, which are kept in good repair.
Children
When footwear is provided for children it is usually impractical to provide two pairs of shoes when a child is growing quickly. In these circumstances shoes, which are in good condition, but are too small, will be replaced without question, provided the Clinician agrees. The Orthotist or physiotherapist will check the fit of shoes whenever it is necessary.
Footwear for children will only be provided when there is a clinical need for non standard shoes. Where standard footwear is required for adaptation, the patient will be required to provide their own shoes which will then be adapted free of charge by the service.
Repair and Replacement
There is no fixed time for renewing footwear. We do not replace boots and shoes every year. They will be replaced when they are no longer economical to repair, for growth, or if
Page 12
Version 1.2 – August 2004
the Clinician feels they are no longer suitable due to a change in foot condition, and there remains a clinical need for bespoke footwear
Please advise patients not to throw their shoes away, even if they think they are worn out. The orthotic service co-ordinator/orthotist will need to see them before they can be replaced.
Patients must inform/ring the orthotic service to advise them when their shoes/boots need repair or possible replacement and an appointment will be made for them. They do not need to come back to the professional each time.
Adapting Footwear
Patients will provide their own appropriate boots or shoes for normal adaptations, including the following:
Addition of raises to compensate for a difference in leg length Flaring out or wedging of heels to correct foot posture Sockets and t-straps for callipers
The orthotist can give advice on appropriate footwear to be adapted. It is usual to adapt up to 3 pairs of shoes in a year and keep them in good repair. If more are requested by the patient, we will ask them to pay for them, unless there are very special circumstances.
Calliper sockets
Shoes must have a broad based and solid heel, such as leather or microcellular rubber, which is at least 2.5cm (1”) high. To make sure they are stable the shoes must have a full back. Sling back styles are unsuitable.
T-straps
The shoe must have a full back. Sling back styles are unsuitable.
Flared out or wedged heels
Heels should be solid and no higher than 5cm (2”) Ladies shoes should have straight-sided broad based heels. Tapered Cuban heel shape is
unsuitable.
Raises
A shoe is usually raised to compensate for difference in leg length. The amount of the raise is usually less than the actual difference.
Page 13
Version 1.2 – August 2004
Raises may be made of microcellular rubber, cork or high-density plastazote. The material used will depend on the type of shoes and the height of the raise required. The raise is usually added to the outside of the shoe on the sole and heel.
A raise may be added to the heel of the shoe only to help with tendon problems or where only a very small amount of raise is required.
It is important that the base of the heel is broad enough for stability. The higher the raise needed the broader the base of the heel must be. The Orthotist will be happy to advise.
A raise may be put on an insole inside a shoe. This may be possible where only a very small raise is needed. It depends on the type of shoe, as there is a limit to the amount, which can be placed inside without pushing the heel out of the shoe. Usually the maximum amount of inside raise is 0.50cm (just under ¼ ”), although it is possible to add a little more inside a boot or trainer.
Suitable styles for low raises of under 1.5cm (approx. ½ “)
The raise may be added to the bottom of the sole and the heel or inserted between the upper and the sole and heel, depending upon the height of the raise required and the way the shoe is made.
The raise makes the shoe less flexible so that the foot ‘walks’ out of the shoe. For this reason shoes without fastenings are unsuitable.
Shoes must support the foot and have a heel base not less than 2.5cm square. The higher the raise the broader the heel base needs to be.
Flat shoes which fasten Higher heeled shoes which fasten and have a heel base of not less than 2.5cm Trainers which have solid soles and heels Fabric summer or house shoes with lace or strap fastening
When buying footwear it should be noted that decorative edges or elaborate patterns or inserts on the soles and heels might be lost when adaptations are carried out. If in doubt please check with the Orthotist prior to purchasing shoes. NB. Most shoe shops will allow for sale or return.
INSOLES
There are several types of insoles and materials from which they are manufactured, to cater for different foot problems. They are usually loose and transferable from one shoe of
Page 14
Version 1.2 – August 2004
similar size and shape to another. They may be made from a paper pattern, for which the Orthotist will draw around the foot, or from a cast made from a mould.
Standard insoles available from retail outlets will not be supplied by the service. However, the orthotist will provide advice on suitable products and where they can be purchased.
It may be necessary to purchase new shoes to accommodate the insoles required.
Entitlement - Adults
Two pairs of bespoke insoles will be provided when clinically appropriate which can be moved between footwear of same size and shape. One pair of insoles will be made and fitted. These will be reviewed to ensure they are correct. If the insoles is fitting well at review, a second pair of insoles will be made.
Children
Due to growth, one pair of insoles will be provided and fitted. These will be replaced as the child grows.
Repair and Replacement
The Patient must contact the orthotic department when they think their insoles need repair (in some circumstances, depending on make of insole) or replacement.
There is no fixed time for renewal of insoles. They are replaced when necessary and subject to ongoing clinical need. If a paper pattern or cast is given to the patient on first supply, this should be brought to the orthotic department when a replacement is needed
The patient must bring their insoles with them to their orthotic appointment.
CALLIPERS
Entitlement
Adults
One pair of callipers is provided and fitted. A second pair will be provided on review if the patient has long term mobility needs.
Children
One pair of callipers is provided and fitted.
Page 15
Version 1.2 – August 2004
Patients will be requested to provide suitable shoes for the socket to be added. Please read the section on adaptations to footwear, which will give you advice on the type of shoe you need.
Repair and replacement
Callipers MUST be reviewed every six months.
The orthotic service MUST pre book a review appointment for any patient that is not seen on a regular basis by another professional at the time of the patients fitting. Children are usually reviewed more regularly by the physiotherapist.
SPLINTS
A stock item will be supplied by the referring clinician if this meets the clinical need, otherwise a made to measure orthoses will be provided by the orthotics department.
Entitlement
Adults
One foot splint (AFO) or pair, will be provided. For long term need or where the wearer is particularly heavy, a second splint or pair, can be provided.
Children
These are usually made to measure. One AFO or pair is provided at any one time and reviewed for growth.
Repair and replacement
Patients must contact the orthotic service if their splint needs repair or replacement.
Repairs may be for straps, padding or wedges as appropriate. Patients MUST bring their old splint with them to an orthotic clinic so that the clinician can decide what best meets the patients needs if a new splint is required. Children will be regularly checked and seen by their physiotherapist (if they have one).
Patients can ring the orthotic service to request a repair or replacement.
Page 16
Version 1.2 – August 2004
KNEE BRACES
Entitlement
Whether child or adult, one only is issued.
Repair and Replacement
Knee braces with joints, need to be reviewed at 6 monthly intervals. An appointment MUST be made by the orthotic service at the time of the fitting appointment.
It is the patients responsibility to ensure that they ring the orthotic service at any time that they feel their knee brace needs repairing or replacing above and beyond this 6 monthly interval review.
Long term users will be supplied with a replacement when their current brace is beyond economical repair. The old/existing brace MUST be brought to the orthotic appointment.
WRIST SUPPORTS
Stock wrist supports will be supplied by the referring clinician.
These are usually ready-made but when necessary can be made to measure or to a cast. The service may keep a stock of simple wrist supports.
Entitlement
Children and adults will be provided with one wrist splint. If replacement need is excessive, then two may be provided or alternatively, a longer wearing item will be sought and provided.
Repair and Replacement
For patients who require their wrist splint for long term use, they will be repaired where straps or linings are worn. They will be replaced as required on production of the old splint to the orthotic service.
COLLARS
Soft collars are not provided through orthotic services (in some Trusts). Patients will be provided with one collar. Where a patient has a chronic disease and a long term need, they may be supplied with a second one for repair purposes and to help prolong the life of the collar.
Page 17
Version 1.2 – August 2004
FABRIC SUPPORTS
Fabric abdominal or spinal support and spinal braces
THERE IS A STATUTORY PRESCRIPTION CHARGE PAYABLE FOR THIS TYPE OF SUPPORT
These are usually made to measure but could be ready-made if appropriate
Entitlement
Children and adults are usually provided with two.
Repair and Replacement
These are repaired or replaced as necessary. Replacement is given when the support is no longer economical for repair. It must be taken to the orthotic appointment.
ELASTIC HOSIERY
THERE IS A STATUTORY PRESCRIPTION CHARGE PAYABLE FOR HOSIERY SUPPORT.
Entitlement
One pair of elastic stocking or tights will be supplied (from stock if available) and if an appropriate prescription is provided. A second pair of stockings or tights will be provided so they can be washed, but the prescription charge still applies.
Replacement
If the item is on an FP10 prescription form, the patient should go back to their GP for further pairs.
WIGS
THERE IS A STATUTORY PRESCRIPTION CHARGE PAYABLE FOR WIGS. PRESCRIPTION CHARGES WILL NOT BE APPLICABLE FOR IN PATIENT EPISODES.
Wigs are usually made from washable mono-acrylic material. Wigs may be fitted at the hospital or supplied by a wig Consultant or hairdresser from outside the hospital.
Page 18
Version 1.2 – August 2004
Entitlement
Wigs are provided for patients undergoing cancer treatments. Wigs are also provided for hair loss due to a medical condition or treatment or following surgery but cannot be provided for normal hair loss due to age.
Patients undergoing chemotherapy treatment will be supplied with one wig initially and will be reviewed after 6 months when a second wig can be ordered if required. Other patients requiring wigs are also entitled to two per year (the prescription charge is applicable to both wigs). Should a patient want a more expensive wig than that provided by the NHS, the patient will be required to pay the difference in cost.
Page 19

Version 1.2 – August 2004
Section F Appendices
Opcare - Policy on chaperoning Opcare - Consensus Policy – Right to Privacy Opcare - Consensus Policy – Clinical Records
Page 20
Version 1.2 – August 2004
Opcare
POLICY ON CHAPERONING
Unaccompanied Consultation / Examination Guidelines
INTRODUCTION
These guidelines have been developed to ensure that all patients are treated with dignity and respect at all times and to support healthcare staff in avoidance of the risk of unjustified complaints from patients following consultation or examination.
A common factor in many patient complaints about inappropriate behaviour (particularly inappropriate touching) by healthcare staff is that patients were not told in advance precisely what would be involved in the examination or procedure. To a person who is not a healthcare professional it may seem inappropriate to examine one part of the body when the patient has identified the problem as being elsewhere. For example, a trivial problem such as a sore throat may require a doctor to examine the patient’s chest.
GUIDELINES
(Taken from Chief Medical Officer, Professor Liam Donaldson, letter ‘Patient Dignity and Privacy – Intimate Examinations, 2003)
1. Patients should be allowed to undress in private and be offered a suitable covering for the examination or procedure. Do not assist the patient in removing clothing unless you have clarified with them that your assistance is required.
2. Explain to the patient why the examination or procedure is necessary and give the patient the opportunity to ask questions. Ensure the patient understands exactly what the examination or procedure will involve, in a way that the patient can understand, so that the patient has a clear idea of what to expect, including any potential pain or discomfort.
3. Seek the patient’s permission before any examination. Consider the need to record that permission has been obtained. Be prepared to discontinue the examination or procedure if the patient asks you to.
4. Keep discussion relevant and avoid unnecessary personal comments. 5. Seek permission from the patient for any students (or others) to be present and / or
to participate in the examination or procedure. Always introduce students or others, to the patient.
Use of Chaperones
The use of chaperones raises a number of issues and concerns including:
Page 21
Version 1.2 – August 2004
Who should undertake the role – relative, friend, healthcare professional, other The practicalities and cost of providing chaperones (if they are healthcare
professionals) The potential that the presence of a third party may inhibit the patients’ willingness
to discuss personal matters The issues of confidentiality
Therefore the Healthcare professional carrying out the consultation, examination or procedure should use their professional judgement to make an assessment in each individual case to determine if a chaperone is required.
Guidelines for the use of Chaperones:
1. When an intimate examination or procedure is required a chaperone should always be offered. If the patient refuses, it should be recorded that the offer was made and declined. It may be necessary to advise the patient that the procedure or examination cannot be carried out without the presence of a chaperone.
2. If a chaperone is present, this should also be recorded and note made of the chaperone’s identity .
3. If a patient asks for a chaperone to be present, one should always be provided. If, for justifiable practical reasons a chaperone cannot be provided, an explanation should be given to the patient and, if possible the examination or procedure delayed to a later time. Always document these discussions.
4. Reference to the Trust approach to the use of chaperones - how patients can request, should be made within appropriate patient information. Notices should be present in patient areas, which make patients aware how they can request a chaperone.
March 2004
Page 22
Version 1.2 – August 2004
OPCARE CONSENSUS POLICY – RIGHT TO PRIVACY
1. SCOPE
This document states the policy regarding a patient’s right to privacy.
2. PURPOSE
To ensure a consistent and professional approach is adopted.
3. RELATED DOCUMENTS
BAPO Guidelines for Best Practice No. 5 “The Clinical Environment” HPC: Standards of coduct, performance and ethics Professor Liam Donaldson Chief Medical Officer, ”Patient Dignity and Privacy – Intimate Examinations, 2003” Consensus Policies: Consent To Treatment, Chaperoning, Intimate Examinations
4. RESPONSIBILITIES
The clinician treating the patient should adopt this policy
5. POLICY
5.1.1 Patients should be allowed to undress in private and be offered a suitable covering for the examination or procedure. Do not assist the patient in removing clothing unless you have clarified with them that your assistance is required.
5.1.2 Explain to the patient why the examination or procedure is necessary and give the patient the opportunity to ask questions. Ensure the patient understands exactly what the examination or procedure will involve, in a way that the patient can understand, so that the patient has a clear idea of what to expect, including any potential pain or discomfort.
5.1.3 Seek the patient’s permission before any examination. Consider the need to record that permission has been obtained. Be prepared to discontinue the examination or procedure if the patient asks you to.
5.1.4 Keep discussion relevant and avoid unnecessary personal comments.
Page 23

Version 1.2 – August 2004
Seek permission from the patient for any students (or others) to be present and / or to participate in the examination or procedure. Always introduce students or others, to the patient.
Page 24
Version 1.2 – August 2004
OPCARE CONSENSUS POLICY – CLINICAL RECORDS
1. SCOPE
This document states the policy regarding clinical records.
2. PURPOSE
To ensure a consistent and professional approach is adopted.
3. RELATED DOCUMENTS
None
4. RESPONSIBILITIES
The clinician treating the patient should adopt this policy
5. POLICY
5.1 CLINICAL RECORDS
Note keeping is an integral part of Prosthetic and Orthotic practice, and indeed adherence to minimum standards for note keeping is mandatory for all state registered members.
5.2 CORE STANDARDS
Clinical records will be legible. All entries will be in permanent black ink. All entries will be signed and fully dated When a practitioner is writing in a file for the first time, they will also print their name and designation under their signature for their first entry. Mistakes will be crossed through with a single line – initialed and dated. Correction fluid must not be used. All entries should be in full handwriting. However, and agreed list of approved abbreviations can be used. All entries should be recorded contemporaneously or within 24hrs of treatment/care. All entries should be made sequentially with a line through any spaces and sign it. Ruling through of any unnecessary gaps or spaces.
Page 25
Version 1.2 – August 2004
Judgments beyond the scope of professional ability, should not be used in clinical records.
Each episode of care/ Patient contact should be recorded in a clinical record, based on the following criteria: Where appropriate, telephone conversations should be minuted at the discretion of the clinician. (Emails from patients – are now classed as correspondence with a patient and therefore do form part of a patients clinical record. They should be printed off and a copy enclosed within the patients clinical records)
5.2.1 CLINICAL CONTENT.
Each record should have a unique number to identify the patient. Each continuation sheet within the clinical record should bear the full name of the patient and his identification number. Each record will include the following patient core data: - The hospital registration number/centre registration number
NHS number where appropriate Address Telephone number Date of birth Sex Emergency contact name General medical practitioners details
Local Trust policy should be referred to and incorporated as a local procedure supplementary to this document.
All clinical notes should be recorded based on the following SOAP note format: -Subjective – Subjective analysis from the patient. – EG what they are stating they feel the problem is.
Objective – Objective assessment – what a clinician sees the problem or issue to be. Specific areas of risk (including staff personal risk) should be recorded EG over weight limit for a device or aggressive patients risk
Analysis/Action - What treatment or steps were taken in overcoming the problem. Patient goals should be recorded
Page 26
Version 1.2 – August 2004
There should be evidence detailing consent to treatment has been obtained, a chaparone has been used, or the patient’s right to privacy has been addressed. ( NB paediatrics – Gillick competence).
Plan: What the planned outcome is IE recalled for further review in 3/12
5.2.2 LEGAL IMPLICATIONS.
Patient records can be called in evidence before a court of law, by a health service commissioner or in order to investigate a complaint at local level. You must respond to all written requests for information within 20 working days. As a state registered Health Care Professional, we have both a professional and legal duty of care. Our Clinical record keeping should therefore be able to demonstrate: - A full account of your assessment, treatment planned and treatment
provided. Relevant information about the condition of the patient. The measures you have taken to respond to the patients needs. Evidence that you have understood and honoured your duty of care and
that any actions or omissions on your part have not compromised their safety in any way.
A record of any arrangements you have made for the continuing care of the Patient.
If record keeping is delegated to pre–registration students, you must ensure
that they are competent and are supervised, and that their entries are countersigned. Do not use initials only as a signature.
Associated documentation to view:
1. Access to Health Records Act 1990. 2. The Data Protection Act 1984 and 1998. 3. The Guide to the Access to Health Records Act 1990. 4. Human rights Act 1998. 5. Access to Medical Reports Act 1988. 6. BAPO Guidelines for Best Practice No.3 – Clinical Records. 7. Freedom Of Information Act 2000
Page 27