north central regional trauma council · north central regional trauma council executive committee...
TRANSCRIPT

North Central Regional Trauma Council Executive Committee Meeting
Mitchell County Hospital, Beloit
August 9, 2017 1:00pm
Agenda Call to Order Dr. Goertzen
Approval of the minutes from the May 10, 2017 meeting
System Finance James Buller, Treasurer Treasurer’s Report
Education Executive Committee
2017 Education Requests
Recap of 2017 Symposium
Acute Hospital Rachelle Giroux / Mary Gray Injury Prevention Tammy Ware / Dana Rickley Prehospital James Buller / Rocky Cramer Emergency Preparedness Sue Cooper Special Populations Tracy Cleary
Old Business Dr. Goertzen
New Business Dr. Goertzen
Announcements (Sharing)
Adjournment Dr. Goertzen
2017 Executive Committee Meetings October 10 6:00pm-8:00pm Location TBD October 11 Statewide Trauma Symposium Via Christi, Wichita
2017 ACT Meetings August 16 10:00am – 3:00pm Kansas Medical Society, Topeka November 1 10:00am – 3:00pm Kansas Medical Society, Topeka
If you are unable to attend in person, conference call will be available. Conference Phone Number: 866-620-7326 Conference Code: 958 411 6860

DRAFT Minutes May 15, 2017 To Be Approved: 8/9/2017
Agenda Minutes Follow up
In Attendance Dr. Cayle Goertzen, James Buller, Justin Overmiller,
Allen Van Driel, Tim Korbe, Dana Rickley, Eric Voss, Dr.
Jake Breeding, Rachelle Giroux, Mary Gray, Rocky
Cramer, Todd Turner, Carman Allen, Tracy Cleary,
Wendy Gronau
General
Membership
Meeting
The members of the trauma region voted to approve
the bylaws as written.
Elections were held. Those elected to the executive
committee were:
Hospital Administrator: Open Physician: Dr. Jake Breeding Nurse: Rachelle Giroux EMS: Rocky Cramer Health Department: Tammy Ware
Call to Order Dr. Goertzen called the meeting to order at 2:25 p.m.
There was no opposition voiced to the minutes from
February 8, 2017.
Dr. Goertzen
Executive Officer
Elections
The executive committee elected their officers to serve a one-year term as follows:
Chairperson: Dr. Goertzen Vice-Chairperson: Mary Gray Secretary: Rachelle Giroux Treasurer: James Buller
Blaine Miller did not seek re-election to the executive
committee. No nominations were received. The
general membership did write in several names: Allen
Van Driel, Dr. Breeding, James Buller, and Austin
Gilliard. Austin is the only one not currently serving.
Allen will make contact with Austin to gauge his
interest.
Allen Van Driel:
Contact Austin
Gilliard
North Central Kansas Regional Trauma Council Executive Committee Meeting Minutes
Salina Regional Health Center, Salina Meeting Minutes
May 10, 2017, After the Regional Trauma Symposium

DRAFT Minutes May 15, 2017 To Be Approved: 8/9/2017
Agenda Minutes Follow up
System Finance The budget spreadsheet was included in the meeting packet and was accepted as presented by the committee with no opposition voiced.
James Buller
Acute Hospital Education requests received to date were discussed.
Those are:
RTTDC~Memorial~$1500 (No dates yet)
TNCC~Mitchell~$1200
ATLS~Black~$850 (No dates yet)
ATLS~Beavers~$275
ATLS~Holmes~$850 (No dates yet)
ATLS~Sheern~$850 (No dates yet)
ATLS~Walker~$275
ATLS~Winegardner~$850
ATLS~Huggans~$850
ATLS~Niles~$695
ATLS~Poore~$695
ATLS~Simesen~$695
James moved to approve these education requests.
Rocky seconded. Motion passed.
Committee Chair ~
Open
Old Business Nothing to report.
New Business Eric Voss reported he is now affiliate faculty for the
National Association of EMTs for PHTLS and all the
tactical courses.
Tracy Cleary is seeking someone from the region to
serve as a pediatric advocate for the EMSC Advisory
Board. This person would serve as a liaison from
EMSC to the region. Rachelle Giroux and Mary Gray
will speak to Tracy more about this.
Due to budget constraints within the trauma
program, Wendy will not be attending the region’s
face-to-face meetings in person for the remainder of
2017 (except the one in conjunction with the
statewide symposium) but will be attending via
conference call.

DRAFT Minutes May 15, 2017 To Be Approved: 8/9/2017
Agenda Minutes Follow up
Announcements /
Each Facility /
Agency
Dr. Goertzen announced he will not be seeking re-
election to the executive committee when his term
expires in 2018. He encouraged everyone to seek out
their local physicians over the next year to be placed
on the ballot.
All Members
Adjournment Dr. Goertzen adjourned the meeting at 2:40 p.m.
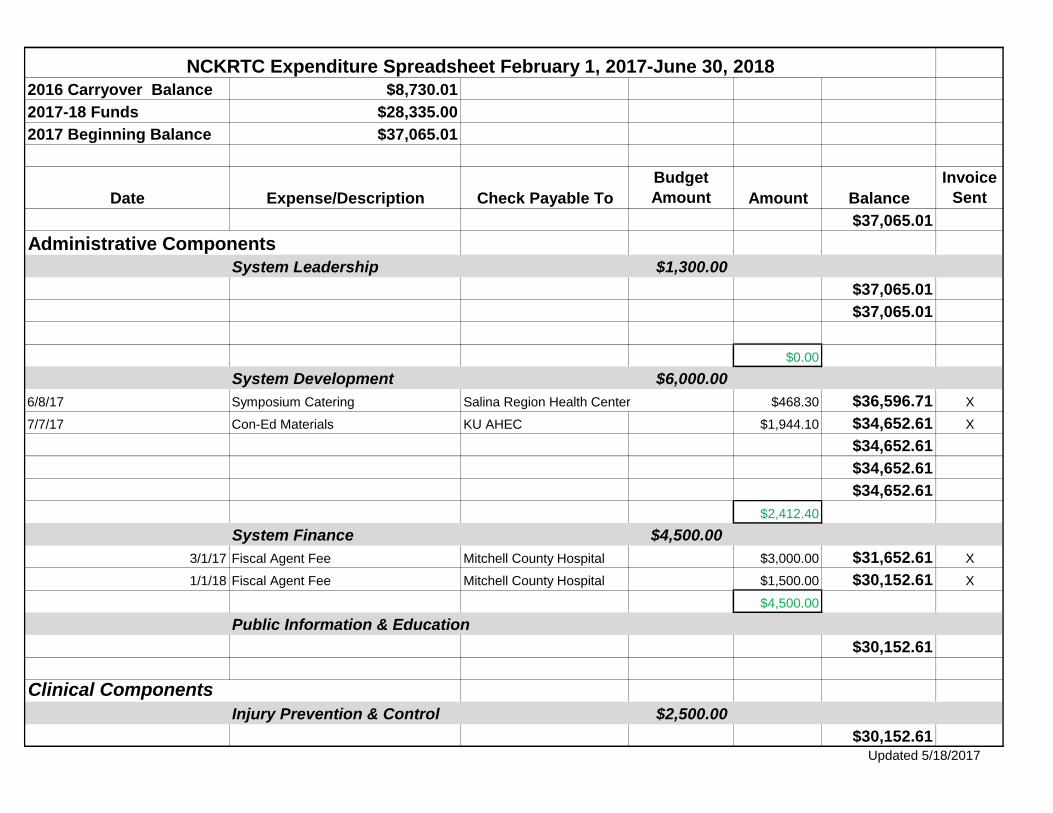
2016 Carryover Balance $8,730.01
2017-18 Funds $28,335.00
2017 Beginning Balance $37,065.01
Date Expense/Description Check Payable To
Budget
Amount Amount Balance
Invoice
Sent
$37,065.01
System Leadership $1,300.00
$37,065.01
$37,065.01
$0.00
System Development $6,000.00
6/8/17 Symposium Catering Salina Region Health Center $468.30 $36,596.71 X
7/7/17 Con-Ed Materials KU AHEC $1,944.10 $34,652.61 X
$34,652.61
$34,652.61
$34,652.61
$2,412.40
System Finance $4,500.00
3/1/17 Fiscal Agent Fee Mitchell County Hospital $3,000.00 $31,652.61 X
1/1/18 Fiscal Agent Fee Mitchell County Hospital $1,500.00 $30,152.61 X
$4,500.00
Public Information & Education
$30,152.61
Injury Prevention & Control $2,500.00
$30,152.61
Clinical Components
NCKRTC Expenditure Spreadsheet February 1, 2017-June 30, 2018
Administrative Components
Updated 5/18/2017
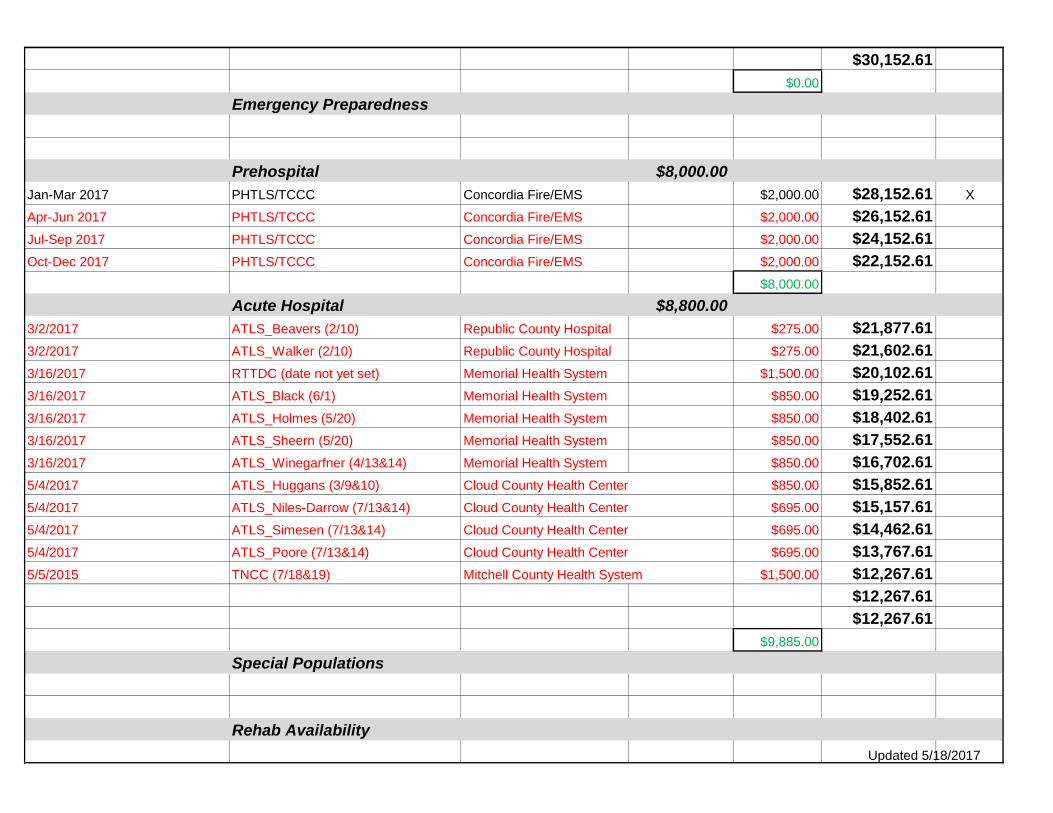
$30,152.61
$0.00
Emergency Preparedness
Prehospital $8,000.00
Jan-Mar 2017 PHTLS/TCCC Concordia Fire/EMS $2,000.00 $28,152.61 X
Apr-Jun 2017 PHTLS/TCCC Concordia Fire/EMS $2,000.00 $26,152.61
Jul-Sep 2017 PHTLS/TCCC Concordia Fire/EMS $2,000.00 $24,152.61
Oct-Dec 2017 PHTLS/TCCC Concordia Fire/EMS $2,000.00 $22,152.61
$8,000.00
Acute Hospital $8,800.00
3/2/2017 ATLS_Beavers (2/10) Republic County Hospital $275.00 $21,877.61
3/2/2017 ATLS_Walker (2/10) Republic County Hospital $275.00 $21,602.61
3/16/2017 RTTDC (date not yet set) Memorial Health System $1,500.00 $20,102.61
3/16/2017 ATLS_Black (6/1) Memorial Health System $850.00 $19,252.61
3/16/2017 ATLS_Holmes (5/20) Memorial Health System $850.00 $18,402.61
3/16/2017 ATLS_Sheern (5/20) Memorial Health System $850.00 $17,552.61
3/16/2017 ATLS_Winegarfner (4/13&14) Memorial Health System $850.00 $16,702.61
5/4/2017 ATLS_Huggans (3/9&10) Cloud County Health Center $850.00 $15,852.61
5/4/2017 ATLS_Niles-Darrow (7/13&14) Cloud County Health Center $695.00 $15,157.61
5/4/2017 ATLS_Simesen (7/13&14) Cloud County Health Center $695.00 $14,462.61
5/4/2017 ATLS_Poore (7/13&14) Cloud County Health Center $695.00 $13,767.61
5/5/2015 TNCC (7/18&19) Mitchell County Health System $1,500.00 $12,267.61
$12,267.61
$12,267.61
$9,885.00
Special Populations
Rehab Availability
Updated 5/18/2017
System Evaluation
Balance $12,267.61
Note-Red text is encumbered funds.
Note-Green text is running total for that line item.
Updated 5/18/2017
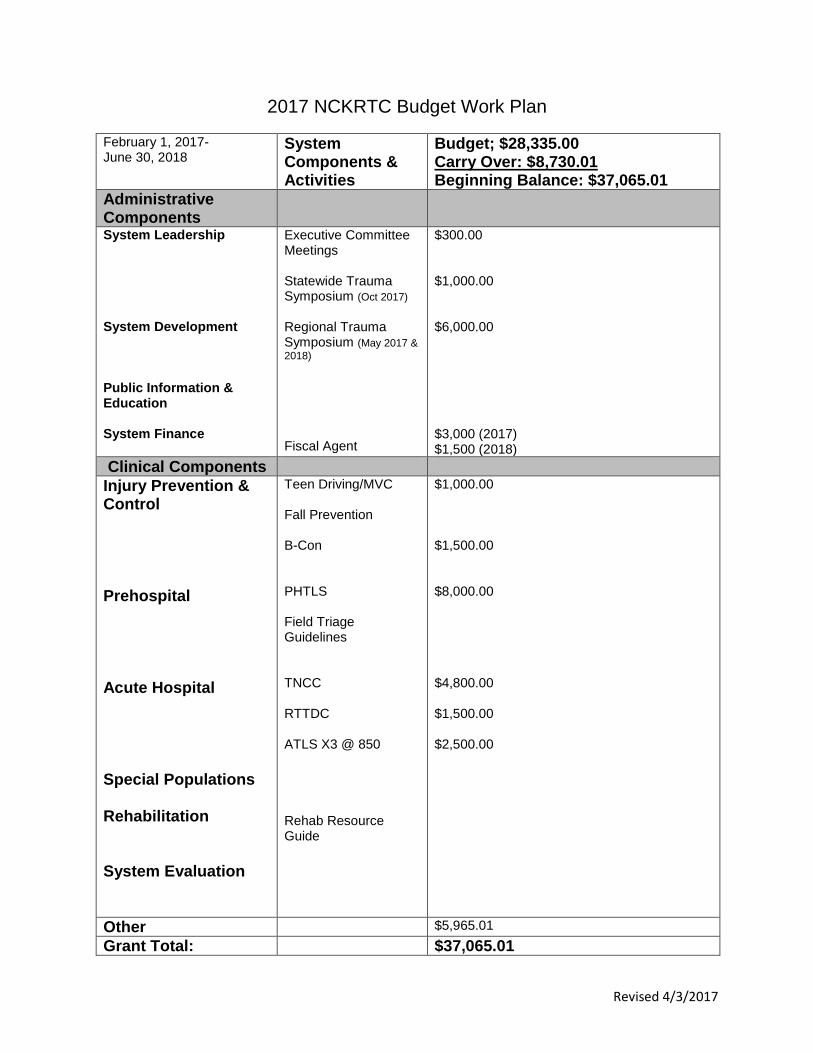
Revised 4/3/2017
2017 NCKRTC Budget Work Plan
February 1, 2017- June 30, 2018
System Components & Activities
Budget; $28,335.00 Carry Over: $8,730.01 Beginning Balance: $37,065.01
Administrative Components
System Leadership System Development Public Information & Education System Finance
Executive Committee Meetings Statewide Trauma Symposium (Oct 2017) Regional Trauma Symposium (May 2017 &
2018) Fiscal Agent
$300.00 $1,000.00 $6,000.00 $3,000 (2017) $1,500 (2018)
Clinical Components
Injury Prevention & Control Prehospital Acute Hospital Special Populations Rehabilitation System Evaluation
Teen Driving/MVC Fall Prevention B-Con PHTLS Field Triage Guidelines TNCC RTTDC ATLS X3 @ 850 Rehab Resource Guide
$1,000.00 $1,500.00 $8,000.00 $4,800.00 $1,500.00 $2,500.00
Other $5,965.01
Grant Total: $37,065.01

Date Recd
Level IV
Hospital
Submit
to RTC Course Region Organization Contact Name Contact email ATLS Provider Course Location
Course
Date
Requested
Amt Awarded Amt Award Date
Documents
Rec/verif
Date
Payment
Requested Notes
3/2/2017 Y 10-May ATLS NC Republic Co Lisa Meltonlmelton@Rphos
pital.org N Beavers Lincoln NE 2/10/2017 275 3/2/2017
3/2/2017 Y 10-May ATLS NC Republic Co Lisa Meltonlmelton@Rphos
pital.org A Walker Lincoln NE 2/10/2017 275 3/2/2017
3/16/2017 W 10-May ATLS NC Memorial Brenda Moffittbmoffitt@mhsks
.org D Sheern Wesley at Hays May 19-20 850 6/15/2017
3/16 I noticed you did not include
course date and location on the ATLS
funding request. Also a copy of ATLS
registration is required with funding
application indicating course cost. I
am not sure if your regional trauma
council will approve funding without
the information 3/17 Reply: We are
not sure when or where the physicians
and APPs will be able to go. Will advise
as soon as determined /// Recd
registration docs 6/12 // Recd
verification docs class completion 6/15
3/16/2017 W 10-May ATLS NC Memorial Brenda Moffittbmoffitt@mhsks
.org
S
Winegardner Springfield, MO April 13-14 850
3/16/2017 W 10-May ATLS NC Memorial Brenda Moffittbmoffitt@mhsks
.org B Holmes 20-May-17 Wesley 850 6/12/2017
3/16 I noticed you did not include
course date and location on the ATLS
funding request. Also a copy of ATLS
registration is required with funding
application indicating course cost. I
am not sure if your regional trauma
council will approve funding without
the information 3/17 Reply: We are
not sure when or where the physicians
and APPs will be able to go. Will advise
as soon as determined // Recd
registration & verification completion
docs 6/12
3/16/2017 W 10-May ATLS NC Memorial Brenda Moffittbmoffitt@mhsks
.org T Black Wesley TBD 850 6/12/2017
3/16 I noticed you did not include
course date and location on the ATLS
funding request. Also a copy of ATLS
registration is required with funding
application indicating course cost. I
am not sure if your regional trauma
council will approve funding without
the information 3/17 Reply: We are
not sure when or where the physicians
and APPs will be able to go. Will advise
as soon as determined // 6/12 recd
receipt for class and letter Black
completed and passed.
5/4/2017 W 10-May ATLS NC Cloud Co Ali Burchfieldaburchfiel@cchc
.com
Shawna
Huggans Via Christi
3/9-
10/2017 850 5/5/2017 Verification Recd
5/4/2017 W 10-May ATLS NC Cloud Co Ali Burchfieldaburchfiel@cchc
.com
Chantelle
Niles-Darrow Bryan Medical Ctr
7/13-
14/2017 695
5/4/2017 W 10-May ATLS Cloud Co Ali Burchfieldaburchfiel@cchc
.com
Layce
Simesen Bryan Medical Ctr
7/13-
14/2017 695

5/4/2017 W 10-May ATLS Cloud Co Ali Burchfieldaburchfiel@cchc
.com Justin Poore Bryan Medical Ctr
9/28-
29/2017 695
3/16/2017 W 10-May RTTDC NC Memorial Brenda Moffittbmoffitt@mhsks
.org TBD TBD 1500
3/16 I noticed you did not include
course date and location on the ATLS
funding request. Also a copy of ATLS
registration is required with funding
application indicating course cost. I
am not sure if your regional trauma
council will approve funding without
the information 3/17 Reply: We are
not sure when or where the physicians
and APPs will be able to go. Will advise
as soon as determined
5/5/2017 Y 10-May TNCC Mitchell Co Mary Gray [email protected]
om Mitchell Co
7/18-
19/2017 1500 App indicates class limited to 6
5/9/2017 W ATLS Cloud Co Ali Burchfieldaburchfiel@cchc
.com
Brandon
Fraley Wesley at Hays
10/6-
7/2017 850
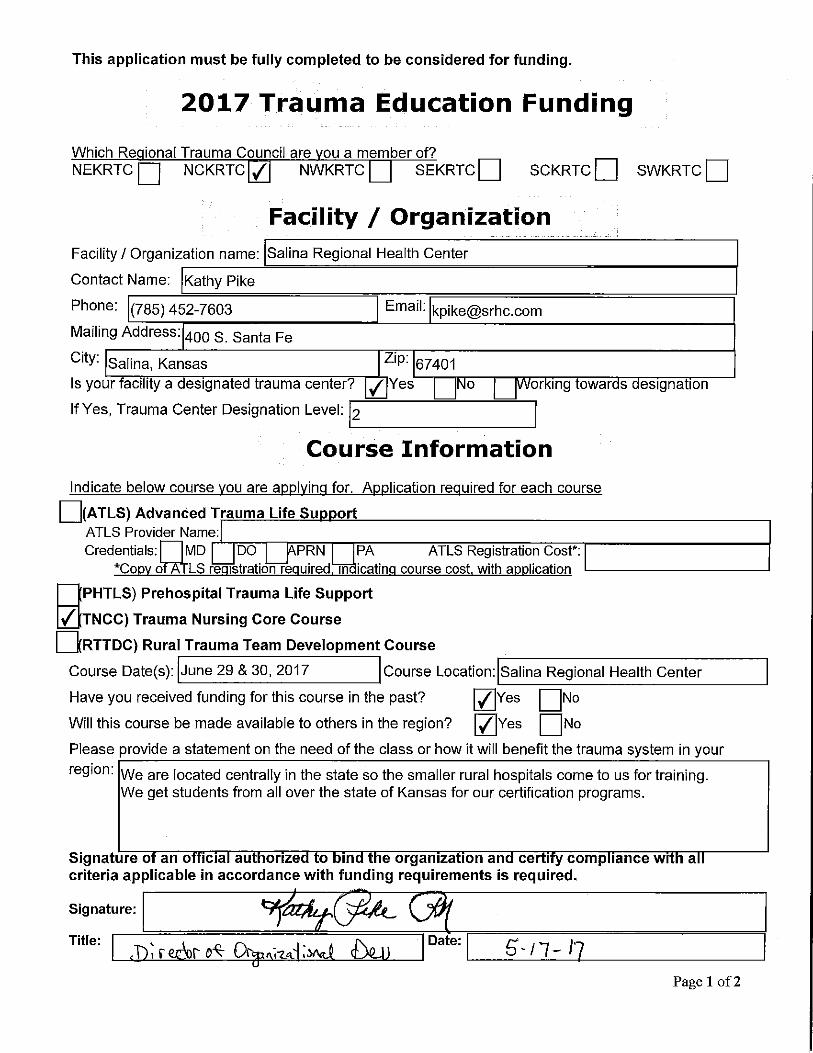
5/17/2017 Level II TNCC NC Salina Regional Kathy Pike [email protected] Salina
June 29-
30/2017 1500
6/12/2017 W TNCC NC Memorial Brenda Moffittbmoffitt@mhsks
.org Salina TBD $1,000.00
6/12 Application for 4 nurses to attend
varoius classes $250 for each nurse
total $1,000. note to Brenda to advise
who will be attend and dates attending.
6/13/2017
Pre-
Approve
d
PHTLS/T
ECC NC
Concordia
Fire/EMS Eric Vossfirechief@conco
rdiaks.org Concordia
May 16-
17/2017 $2,000 $2,000 6/13/2017 6/13/2017 6/13/2017
Needed additional info, attached email
from Eric
6/28/2017 TNCC NC
Ellsworth Co
Med Ctr Beth Vallierbvaliier@ewmed
.com Ellsworth
Oct 17-
18/2017 $1,000









96/28/2917 WED 3155 FAX 785 472 5769 ECMC Admin Qûû1/ûû3
' ellsw orth county. M edical center
Fu RO UTING SHEET
FROMR - VY vvkG
Eusworth Cokm ty Medical Center1604 Aylward P.O. Box 87Ellswouh, KS 67439Tel: 785-472-31 1 1 Y .YWVFax: 785-472-5396
TO ' '
M ESSAGE:
Department: G'O G
sent: Glz% I ODate'rime sent: * -,G G eax
PAX: 'n2...% - zqtp- efw'a.r.!x
TEL:
T: ShTOTAL NUMBER OF PAGES TRANSMIWED INCLUDING THIS FACE SHEE
IF THE TRANSM IW ED COPY IS UNREADABLE OR ALL W AS NOTRECEIVED , PLEASK CALL THE ABOVE NUM BER AND ADW SETHE SENDER YOU NEED IT TM NSM IW ED AGAIN.
TH ANK YOU
*****************************************************@***********
CONFIDENTIALITY NOTICE: The docum ents accom panying this telecopytransm ission contaita conlsdential inform ation belonging to the sender which
is legally privileged. The inform ation is itltended only for the use of theindividual or entity nqm ed above. If you are not the intended recipient, youaa-e hereby notiEed that any disclosure, copying, distribudon of the tnking ofany action in reliance on the contents of this telecopied information is stdctlyprohibited. If you have received this telecopy in en-or please imm ediately:
notify us by telephone to m'range for ret'una of the origm al docum ents to us.@*****************************W***************************+******

96/28/2917 WED 3155 FAX 785 472 5769 ECMC Admin 1992/993
Thls application m ust be fully com pllted to be considered for fundlng.
2017 Traum a Education Funding
W hioh Re ional Trauma Council aro a member of?
NEKRTC Uq NCKRTC Z NWKRTC SEKRTC UJ SCKRTC U1 SWKRTC UJ
Facility / OrganizationFacility / Organization name: Ellsworth County Medical Genter
Contact Name: Beth Vallier
Phone: (785) 472-31 1 1 Email: [email protected]
Mailing Address: 16c4 Aylward Ave.
City: Ellsworth Zip: 6743:
Is your ac1 I y a eslgnate trauma center. Yes / o or Ing owar s eslgna Ionlf Yes, Trauma Center Designation Level:
Course Inform ation
Indicate below course vou are aDnlvinc for. Anolication reatlired for each course
(ATLS) Advanced Tr a Life Su ortATLS Provider Name:Credentials: MD DO PRN PA ATLS Registration Cost*:
* o o LS re Istration re uire ' cost with a Iication
PHTLS) Prehospltal Trauma Life supportV TNCC) Trauma Nursing Gore GourseRTTDC) Rural Trauma Toam Development Course
Course Datels): October 17-18 Course Location: Ellsworth, KS
Have you received funding for this course in the past? I--IZ Yes I-SNOWill this course be made available to others in the region? Vlh'es I-7NOPlease provlde a statement on the need of the class or how it will benefit the trauma system in yourrooion: w e have had some turnover in our nursing depadment and need to keep our new staff ready for
trauma emergencies. W e have staff needing to recertify to remain profioient in these Iife-savingskills. Our proximity to two major roadways keeps our ER busy. Being able to work collaborativelywith our providers, and EMS staff, makes TNCC a crucial course for our nursing staff.
Sijnature O an O C a au OrIZ* O In e Organlza 10n an G0 COmP anco WI aorlteria applioable In accordance with funding requirements is required,
Slgnature: -
Title: , - .-. Date; n
Page 1 of 2

96/28/2917 WED 3156 FAX 785 472 5769 ECMC Admin 1993/993
This appllcation must be fully oompletod to be considered for fundlng,
Budget Inform ationThls sectlon does not aDDlv to AT'LS rafw ests
Will this course be open to others in the region? V Yes NoDo you plan to charge a registration fee for the course? F7/ Yes No Registration Fee $ 150.00
Estimated Course Ex endituresFacilit Char es/ Promotion & Publicit 0S eaker/lnstructor Fees so0Travel/ Lod in 2s0Books / Su lies 816Other: e1oOther: sû
Totals 272:.00Amount of Funding Requested $ 1 000.00Refer to your region's trauma eduoation reimbursement policy or maxfmnm amoant available.
Regional Traum a Council M em bers
Please confirm our m em ber re resentation to the Re ional Traum a Council:Hos itals Name Em ail Contact Num berAdministratorRe resentative
Ph sician Re resentativeNurse Re resentative Amanda Thfa:ll:r. D(3N athrasherlewmed.com 785-472-3111
EMS Name Email Contad Num berEMS Re resentative 1EMS Re resentative 2
Additional Comments:W G r <X rrwm bxoo ' k'dr Q LWJ
$4>.., %V r.n - û . Co ' ' ey'e..D .
Funding Requirem ents* Gompleted applications can be faxed to 785-296-2625 or emailed to Nancy,Akin@ Kszgov. Ghange in course date will require notification within 30 days of original course date to remain
eligible.. ATLS only: Copy of provider credentialing card must be submitted within 30 days of course
completion.* AII other courses: The following documents must be submitted wlthin 4.5 days of course
completion.o Copy of class roster which incltldes city, zip and indicates initial or renewal certificatiop
for each class participantFinal affidavit of expendituresFunded reimbursements will be made tc the facility or organization making request,
Page 2 of 2,

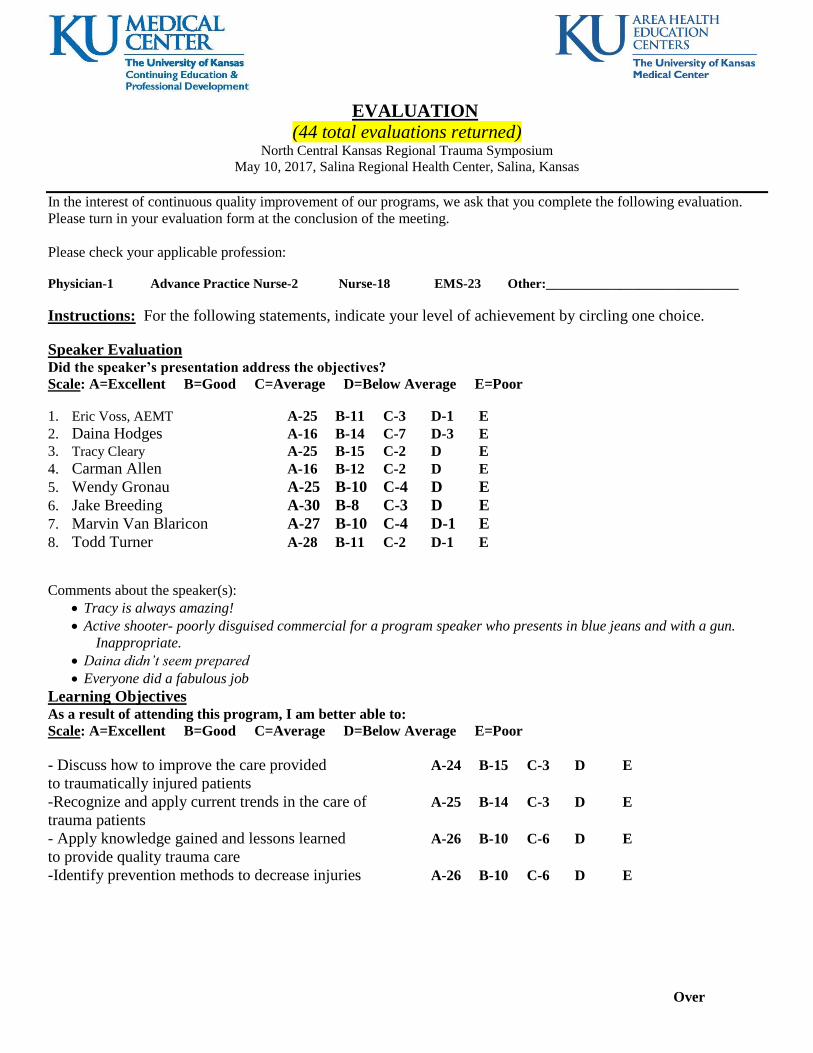
EVALUATION
(44 total evaluations returned) North Central Kansas Regional Trauma Symposium
May 10, 2017, Salina Regional Health Center, Salina, Kansas
In the interest of continuous quality improvement of our programs, we ask that you complete the following evaluation.
Please turn in your evaluation form at the conclusion of the meeting.
Please check your applicable profession:
Physician-1 Advance Practice Nurse-2 Nurse-18 EMS-23 Other:_____________________________
Instructions: For the following statements, indicate your level of achievement by circling one choice.
Speaker Evaluation Did the speaker’s presentation address the objectives?
Scale: A=Excellent B=Good C=Average D=Below Average E=Poor
1. Eric Voss, AEMT A-25 B-11 C-3 D-1 E
2. Daina Hodges A-16 B-14 C-7 D-3 E
3. Tracy Cleary A-25 B-15 C-2 D E 4. Carman Allen A-16 B-12 C-2 D E
5. Wendy Gronau A-25 B-10 C-4 D E
6. Jake Breeding A-30 B-8 C-3 D E
7. Marvin Van Blaricon A-27 B-10 C-4 D-1 E
8. Todd Turner A-28 B-11 C-2 D-1 E
Comments about the speaker(s):
Tracy is always amazing!
Active shooter- poorly disguised commercial for a program speaker who presents in blue jeans and with a gun.
Inappropriate.
Daina didn’t seem prepared
Everyone did a fabulous job
Learning Objectives As a result of attending this program, I am better able to:
Scale: A=Excellent B=Good C=Average D=Below Average E=Poor
- Discuss how to improve the care provided A-24 B-15 C-3 D E
to traumatically injured patients
-Recognize and apply current trends in the care of A-25 B-14 C-3 D E
trauma patients
- Apply knowledge gained and lessons learned A-26 B-10 C-6 D E
to provide quality trauma care
-Identify prevention methods to decrease injuries A-26 B-10 C-6 D E
Over

Please list any strategies recommended by today’s speakers that you plan to use that you haven’t used before?
Hemostatic gauze protocols, IECC Classes, PECC, Bleeding Control Classes, Trauma Activating
Stop the bleed training
Bypass protocol
Intentional accidental injuries- good knowledge to have.
Use of tourniquets was very informative
I will change the way we store our tourniquets
TCCC
Plan to look at ways to enhance existing policies and procedures
Tourniquets
Implement the use of hemostatic dressing for bleeding protocol
Clot
Work on PEDIATRICS
Possibly teach the Stop the Bleed
Look at Safe kids website info
Investigate starting a safe kids coalition in my community
Based on today’s program, what will you do differently?
More education
Consider more options when it comes to hemostatic gauze and tourniquets
Increase case reviews and define transfer protocols with EMS leaders
How to better provide care to my trauma patients
Will have to give this some thought….
I can now properly place a C.A.T.
Take the tourniquets out of drawer and package
Promote bypass protocol
Increase pediatric education and continually educate. There is never enough
Possibly starting field triage and bypass protocols
Most of what we talked about today is implemented now in how we do things
Early activation
Somehow get local EMS to work with us
Engage schools and law enforcement
Tourniquets! And continue to work on bypass protocol
Please check any factors which limit your ability to use today’s information/strategies.
Individual: current knowledge-2 skills-1 professional performance-2 working relationships-4
Institutional: operating systems-3 mission-1 staffing-11 equipment-7 finances-10
Other factors or specifics which limit your ability to use today’s information/strategies.
Lack of case review
Awareness of need for training at institutional level.

Content Integrity Evaluation
Evidence Based: All the recommendations involving clinical medicine and nursing in an accredited activity for healthcare
professionals must be based on evidence that is accepted within the profession of medicine or nursing as adequate
justification for their indications and contraindications in the care of patients. (Adapted from ACCME definition, 2007)
For clinical presentations, did the course provide evidence-based information? Yes-36 No, if no please explain:
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
Commercial Balance
The content or format of an accredited activity for healthcare professionals, e.g. CME and CNE, or its related materials
must promote improvements or quality in healthcare and not a specific proprietary business interest or a commercial
interest. Presentations must give a balanced view of therapeutic options. Use of generic names will contribute to this
impartiality. If the educational material or content includes trade names, where available trade names from several
companies should be used, not just trade names from a single company. (Adapted from ACCME July 2002)
Was the program free of commercial bias and balanced with respect to therapeutic options, and their risks and
benefits? Yes-35 No, if no please
explain:
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________

Needs Assessment:
For the next program, I would be interested in attending:
hands-on workshop on airway management, trauma skills, TECC, pediatric trauma, critical access level of
care, chest decompression
simulation of OB home delivery
small group discussions of case studies on more medical and trauma case studies, transfers, bypass,
anything!
other, please explain farm accident/response trauma, cardiology, new and upcoming changes with trauma
care
What has been your greatest clinical or professional practice challenge within the past year?
Fighting the mentality of just being good enough
Delay in transfers
Educating new staff
Varied traumas in ER
Difficult physicians
Always emotional with pediatric trauma
Implementing and following all the new protocols—trauma, heat, stroke, etc.…
Passing on the knowledge! This is always my biggest concern- I learn but I don’t know how to share. Recorded
webinar for trauma needs to be available to my staff can learn too.
EMS protocols
The following area(s) for future improvement were identified during this session:
Preparedness for trauma in ER-critical access level.
Tourniquet education and community education
We will work on Peds protocols. Keep complaining that we need a full-time EMS director
Additional Comments:
Thanks for the good education
The hands on was great training that can be taken back to facility
Enjoyed case studies. Very informative.
Good program overall!
Very good!
Thoughts of trauma activations for pe ds or elderly populations
Thank you for completing this evaluation.

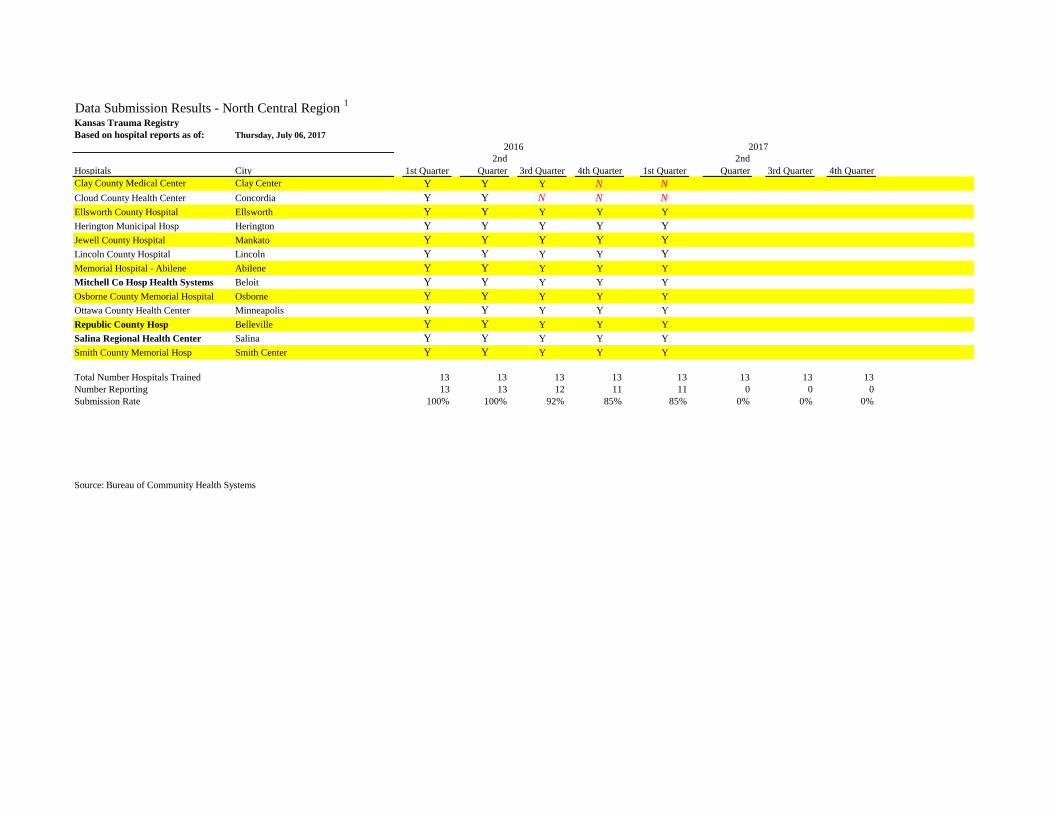
Kansas Trauma Registry
Based on hospital reports as of:
Hospitals City 1st Quarter
2nd
Quarter 3rd Quarter 4th Quarter 1st Quarter
2nd
Quarter 3rd Quarter 4th Quarter
Clay County Medical Center Clay Center Y Y Y N N
Cloud County Health Center Concordia Y Y N N N
Ellsworth County Hospital Ellsworth Y Y Y Y Y
Herington Municipal Hosp Herington Y Y Y Y Y
Jewell County Hospital Mankato Y Y Y Y Y
Lincoln County Hospital Lincoln Y Y Y Y Y
Memorial Hospital - Abilene Abilene Y Y Y Y Y
Mitchell Co Hosp Health Systems Beloit Y Y Y Y Y
Osborne County Memorial Hospital Osborne Y Y Y Y Y
Ottawa County Health Center Minneapolis Y Y Y Y Y
Republic County Hosp Belleville Y Y Y Y Y
Salina Regional Health Center Salina Y Y Y Y Y
Smith County Memorial Hosp Smith Center Y Y Y Y Y
Total Number Hospitals Trained 13 13 13 13
Number Reporting 13 13 12 11
Submission Rate 100% 100% 92% 85%
Source: Bureau of Community Health Systems
2017
Data Submission Results - North Central Region 1
2016
Friday, June 02, 2017
Kansas Trauma Registry
Based on hospital reports as of:
Hospitals City 1st Quarter
2nd
Quarter 3rd Quarter 4th Quarter 1st Quarter
2nd
Quarter 3rd Quarter 4th Quarter
Clay County Medical Center Clay Center Y Y Y N N
Cloud County Health Center Concordia Y Y N N N
Ellsworth County Hospital Ellsworth Y Y Y Y Y
Herington Municipal Hosp Herington Y Y Y Y Y
Jewell County Hospital Mankato Y Y Y Y Y
Lincoln County Hospital Lincoln Y Y Y Y Y
Memorial Hospital - Abilene Abilene Y Y Y Y Y
Mitchell Co Hosp Health Systems Beloit Y Y Y Y Y
Osborne County Memorial Hospital Osborne Y Y Y Y Y
Ottawa County Health Center Minneapolis Y Y Y Y Y
Republic County Hosp Belleville Y Y Y Y Y
Salina Regional Health Center Salina Y Y Y Y Y
Smith County Memorial Hosp Smith Center Y Y Y Y Y
Total Number Hospitals Trained 13 13 13 13 13 13 13 13
Number Reporting 13 13 12 11 11 0 0 0
Submission Rate 100% 100% 92% 85% 85% 0% 0% 0%
Source: Bureau of Community Health Systems
Thursday, July 06, 2017
2017
Data Submission Results - North Central Region 1
2016

Administrators: Austin Gillard Clay County Medical Center 617 Liberty Street Clay Center, KS 67432 785-632-2144 [email protected] Term - May 2017 – May 2020 Allen Van Driel Smith County Memorial Hospital 614 S. Main Street Smith Center, KS 66967 785-282-6845 [email protected] Term – May 2015 – May 2018
Health Departments: Tammy Ware, LPN Dickinson County Health Department 1001 N Brady Abilene, Kansas 67410 785-263-4179 [email protected] Term - May 2017 – May 2020 Dana Rickley, RN Clay County Health Department 820 Spellman Circle Clay Center, Kansas 67432 785-632-3193 [email protected] Term – May 2015 – May 2018
Physicians: Jake Breeding, MD, FACS Salina Regional Health Center 501 South Santa Fe Salina, KS 67401 785-452-7245 [email protected] Term - May 2017 – May 2020 Cayle Goertzen, MD (Chairperson) Republic County Hospital 2337 G Street Belleville, KS 66935 785-527-2217 [email protected] Term – May 2015 – May 2018
EMS: Rocky Cramer Clay County EMS 604 4th Street Clay Center, KS 67432 785-632-2166 [email protected] Term - May 2017 – May 2020 James Buller, Paramedic (Treasurer) Concordia Fire-EMS Division 701 Washington Concordia, KS 66901 785-243-4411 [email protected] Term – May 2015 – May 2018
Nurses: Rachelle Giroux (Secretary) Salina Regional Health Center 400 South Santa Fe Salina, KS 67401 785-452-6655 [email protected] Term - May 2017 – May 2020 Mary Gray, RN (Vice-Chairperson) Mitchell County Hospital 400 W. 8th Street, PO Box 399 Beloit, KS 67420 785-738-2266 [email protected] Term– May 2015 - May 2018
ACT Representative: Jake Breeding, MD, FACS Salina Regional Health Center 501 South Santa Fe Salina, KS 67401 785-452-7245 [email protected] Term expires 2019
2017-18 NORTH CENTRAL KANSAS REGIONAL TRAUMA COUNCIL
Executive Committee

NORTH CENTRAL KANSAS
REGIONAL TRAUMA SYSTEM
REGIONAL TRAUMA PLAN
Regional Trauma Plan
JULY 2015 – JUNE 2017
Developed by the NCRTC Executive Committee Cayle Goertzen, MD, Chairman
2015-2017 NCRTC Regional Trauma Plan Page 1

State of Kansas Governor Sam Brownback
Kansas Department of Health and Environment Susan Mosier, MD, Secretary
Bureau of Community Health Systems
1000 SW Jackson, Suite 340 Topeka, Kansas 66612-1365
785-296-1200 http://www.kdheks.gov/olrh/
Acknowledgements:
Special thanks to the NCRTC Executive Committee: Cayle Goertzen, MD Jake Breeding, MD, FACS Mary Gray, RN Republic County Hospital Salina Regional Health Center Mitchell County Hospital Tammy Ware, LPN Dana Rickley Rachelle Giroux, RN Dickinson County Health Dept. Clay County Health Dept. Salina Regional Health Center Wendy Gronau James Buller Lincoln County EMS Concordia Fire-EMS Division
Additional Contributors Sue Cooper, RN, Salina Regional Health Center
2015-2017 NCRTC Regional Trauma Plan Page 2

Message from the NCRTC Page 4
Executive Summary Page 5
Regional System-Goals-Objectives-Strategies-July 2015-June 2017 Administrative Components System Leadership Page 9 System Development Page 10 System Public Information and Education Page 11 System Finance Page 12 Clinical Components Injury prevention and Control Page13 Emergency Preparedness Page 14 Prehospital Page 15 Acute Hospital Page 16 Special Populations Page 17 Rehab Availability Page 18 System Evaluation Page 19 Appendices Appendix A-SWRTC Hospital & EMS listing Page 20 Appendix B-2011 CDC Guidelines for Field Triage of Injured Patients Page 22
Table of Contents
2015-2017 NCRTC Regional Trauma Plan Page 3

Message from the NCRTC On behalf of the North Central Regional Trauma Council (NCRTC), we present to you the July 2015 – June 2017 NCRTC Regional Trauma Plan, as our roadmap for improvement of the NCRTC Trauma System. This plan is an adaptable and evolving document that will change as best practices and opportunities for performance improvement are identified and implemented. The North Central Region of Kansas is committed to the development and implementation of a cohesive and inclusive trauma system including injury prevention and control, public access to emergency medical dispatch; prehospital emergency response and care, definitive hospital care, rehabilitation access, regional system evaluation, disaster preparedness and trauma registry and research.
Each piece of the NCRTC trauma system continuum-of- care is essential to prevent injuries and save lives within our region. The NCRTC and its many trauma system partners have continued to expand partnerships and collaborative efforts to strengthen and ensure the successful implementation of the NC regional trauma system.
2015-2017 NCRTC Regional Trauma Plan Page 4

Executive Summary The Regional Trauma Councils (RTCs) are the cornerstone of the Kansas Trauma System. In accordance to regional bylaws, leadership for the RTCs are elected by the general membership and include physicians, nurses, hospital administrators, EMS and health department representatives. The RTC is comprised of members representing all areas of the trauma system: hospital, prehospital/EMS, and health departments.
The NCRTC serves as the coordinating and oversight body for the NC regional trauma system and is responsible for development and implementation of a comprehensive/inclusive regional trauma system. In collaboration with stakeholders and trauma system partners, the NCRTC writes the Plan which guides regional system development, implementation and evaluation. The development of this NC regional plan is an orchestrated “bringing together” of all trauma system stakeholder groups that contribute to the effective and efficient care of trauma patients in our community. The RTC meets at least quarterly to oversee implementation of the Plan, but may meet more frequently as determined by system demands.
The Kansas Department of Health & Environment (KDHE) was charged, under K.S.A. 75-5665, as the lead agency for development, implementation and evaluation of the statewide trauma system including support of the RTCs and administering a trauma registry.
In 1999, the Kansas legislature established the Advisory Committee on Trauma (ACT) Committee. Members are appointed by the Governor and are advisory to the Secretary of KDHE. The ACT members are recognized for their significant expertise and commitment to trauma care and system development in Kansas. They provide input and guidance to KDHE on developing a comprehensive, statewide trauma system. The ACT gives major stakeholders a voice in the policy process and functions to integrate the activities of the RTCs. A member from the NCRTC represents the region on the ACT. The ACT meets quarterly.
The Plan is composed of administrative and clinical components. The Plan goals are adapted from the state trauma plan, the Benchmark, Indicator, and Scoring (BIS) assessment, and NCRTC strategic planning priorities. This plan is used to guide the NCRTC strategic planning priorities.
Administrative Components System Leadership: The RTC is responsible for regional assessment, planning and assurance of the trauma system for their region. KDHE is the lead agency of the Kansas Trauma Program and provides coordination, planning, and support to the RTC. The ACT provides input and guidance to KDHE on developing a comprehensive, statewide trauma system and gives major stakeholders a voice in the policy process, and it functions to integrate the activities of the RTC. System Development: The development of a strong, efficient, well-coordinated regional trauma system is vital in providing optimal trauma care. The challenge to the trauma system is to ensure that
2015-2017 NCRTC Regional Trauma Plan Page 5

progress is made in a systematic and measured way. This plan addresses the need for a successful integration of a quality philosophy in all aspects of the trauma system and implementation of objectives and strategies and performance improvement that move the region toward the accomplishments of identified local and regional goals. Advancing the regional trauma system by being the best we can be through a continuum of care from injury prevention through return to the community with the highest quality of life possible needs to be embedded in all aspects of the regional council work.
System Public Information and Education: The NC region strives to provide education and inform local policy makers and members of the public as to the benefits of a trauma system and the importance of prevention.
System Finance: The goal of trauma system financing is to provide the public with an efficient system that provides optimal trauma care for injured patients. Trauma systems need sufficient funding to implement a statewide and regional system of care—one focused on each component of care from prevention through acute care and rehabilitation, including all-hazards preparedness. A major NCRTC goal and system need is to be a good steward of the contract funds provided through the State and support all system components. Clinical Components Injury Prevention and Control: Injury prevention and control is a key component of the regional trauma system because it offers the greatest potential for reducing the financial burden of trauma care, as well as reducing morbidity and mortality. The RTC focuses on injury prevention based on trauma registry data. Regional data shows that teen motor vehicle crashes and elderly falls are the primary cause of unintentional death and injury in the region and statewide. The RTC has identified the need to continue to provide funding support for evidence based injury prevention activities in the area of teen drivers and falls. Emergency Preparedness: Each disaster is unique and places tremendous strain on communities. Disaster planning requires a cooperative multidisciplinary effort by the local medical community; police and fire departments, local, regional, and national governments and industry to devise a comprehensive strategy to minimize mortality, injury, and destruction of property.
Prehospital Care: Prehospital care and access is a critical component of the regional trauma system. The prehospital trauma system is driven by the goal of getting the right patient to the right place at the right time. The goals of the prehospital component of the trauma system are to prevent further injury, initiate resuscitation, and provide safe and rapid transport of injured patients. Treatment protocols should be established to guide trauma patient care, and patients should be taken directly to the center most appropriately equipped and staffed to handle their injuries. Acute Hospital Care: Care of the injured takes place at various hospitals within the health care system ranging from critical access hospitals to designated trauma centers. While it is recognized
2015-2017 NCRTC Regional Trauma Plan Page 6

that hospitals have varying resources committed to the care of the injured patient, rural hospitals are often the port of entry for many patients and they, as well as other hospitals, should have consistent standards, adequately trained trauma care workforce and a performance improvement program.
Special Populations: For the purpose of the Plan, special populations include the elderly, pediatric and morbidly obese populations. The elderly population have different spectrum of injury patterns such as greater number of falls, higher mortality and morbidity from similar injuries when compared to younger adults. There are also significant physiologic changes and a greater number of co-morbidities. More children die of injury than of all other causes in Kansas. For injured children who survive, severe disability may become a lifelong problem requiring functional or custodial care. Injured children require special resources. Effective care of injured children requires a comprehensive approach by developing and implementing effective strategies for injury prevention, improving system of emergency medical care for children, and provide the best trauma care at every level available. The prevalence of obesity in the country continues to increase steadily. In trauma, obesity is associated with higher morbidity and mortality. Treatment and care of morbidly obese patients involves compassion, respect, and dignity. Without appropriate equipment, management of these patients can be a risk for both the healthcare provider and patient. Regional trauma councils are encouraged to identify the resources and equipment that are available within the region to assist in providing care for these patients. Hospitals and EMS providers should know the specifications of their equipment for weight, girth, and width limits. Rehabilitation Availability: Trauma rehabilitation plays a key role in returning the injured patient back to their community with the highest quality of life. Acute care should be consistent with preservation of optimal functional recovery. The ultimate goal of trauma care is to restore the patient to pre-injury status. Not only is this effort best for the patient, it also is less costly. When rehabilitation results in independent patient function, there is major cost savings compared with costs for custodial care and repeated hospitalizations. System Evaluation: Data collection, system evaluation, and performance improvement are essential for function of the trauma system. It involves a continuous multidisciplinary effort to measure, evaluate, and improve both the process of care and the outcome. All hospitals collect and submit data to the State trauma registry. Region Demographics The North Central region is comprised of 12 counties: Clay, Cloud, Dickinson, Ellsworth, Jewell, Lincoln, Mitchell, Osborne, Ottawa, Republic, Saline, and Smith. The region is primarily rural in nature: one county classified as semi-urban, one classified as densely settled rural, six classified as rural, and four classified as frontier. There are 16 EMS agencies (Appendix A) and 13 hospitals
2015-2017 NCRTC Regional Trauma Plan Page 7

(Appendix A) within the NC region that provide trauma care. The North Central region has one ACS verified and state designated level III trauma center and two state designated level IV trauma centers:
ACS Verified and State Designated Trauma Centers
Level III Salina Regional Health Center
400 S. Santa Fe Salina, Kansas 67402
State Designated Trauma Centers
Level IV
Mitchell County Hospital Health Systems Republic County Hospital 400 W. Eighth 2420 G Street Beloit, Kansas 6720 Belleville, Kansas 66935
2015-2017 NCRTC Regional Trauma Plan Page 8

ADMINISTRATIVE COMPONENTS System Leadership
Goal 1 There is a viable and active NCRTC comprised of multi-disciplinary representatives; hospital administrators, physicians, nurses, health departments, and EMS to plan, implement, and evaluate an inclusive regional trauma system. Objective 1: RTC will review council general membership, annually, for compliance with the NCRTC bylaws.
Strategy 1: Conduct a review of the general membership annually and revise/update membership as appropriate. Strategy 2: Review membership structure for possible other positions needed to advance the regional system.
Objective 2: NCRTC executive committee will encourage general membership members, stakeholders, and trauma partners to attend executive committee meetings and become engaged in implementing and evaluate regional trauma system initiatives and activities.
Strategy 1: Identify and maintain a membership recruitment committee. Strategy 2: Ensure that members, stakeholders, and trauma partners have access to regional council and subcommittee meeting dates, agendas, minutes and meeting materials through email alerts (sent in advance) and website postings. Strategy 3: Conduct an annual general membership meeting to promote participation in RTC activities, trauma system implementation, and evaluation. Strategy 4: Act as a forum for regional trauma issues to providers and consumers within the trauma care continuum. Strategy 5: Monitor component compliance with the Plan. Strategy 6: Encourage participation by stakeholders in the annual statewide leadership meeting of the executive committees.
Goals-Objectives-Strategies
July 2015-June 2017
2015-2017 NCRTC Regional Trauma Plan Page 9
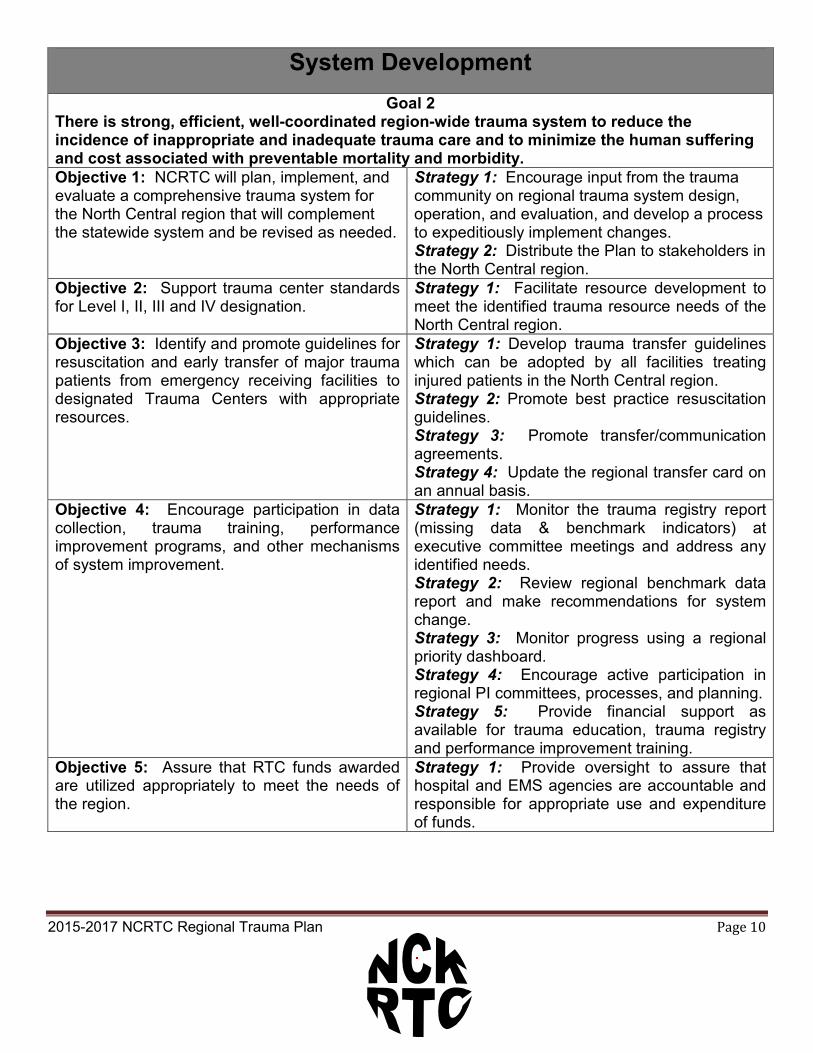
System Development
Goal 2 There is strong, efficient, well-coordinated region-wide trauma system to reduce the incidence of inappropriate and inadequate trauma care and to minimize the human suffering and cost associated with preventable mortality and morbidity. Objective 1: NCRTC will plan, implement, and evaluate a comprehensive trauma system for the North Central region that will complement the statewide system and be revised as needed.
Strategy 1: Encourage input from the trauma community on regional trauma system design, operation, and evaluation, and develop a process to expeditiously implement changes. Strategy 2: Distribute the Plan to stakeholders in the North Central region.
Objective 2: Support trauma center standards for Level I, II, III and IV designation.
Strategy 1: Facilitate resource development to meet the identified trauma resource needs of the North Central region.
Objective 3: Identify and promote guidelines for resuscitation and early transfer of major trauma patients from emergency receiving facilities to designated Trauma Centers with appropriate resources.
Strategy 1: Develop trauma transfer guidelines which can be adopted by all facilities treating injured patients in the North Central region. Strategy 2: Promote best practice resuscitation guidelines. Strategy 3: Promote transfer/communication agreements. Strategy 4: Update the regional transfer card on an annual basis.
Objective 4: Encourage participation in data collection, trauma training, performance improvement programs, and other mechanisms of system improvement.
Strategy 1: Monitor the trauma registry report (missing data & benchmark indicators) at executive committee meetings and address any identified needs. Strategy 2: Review regional benchmark data report and make recommendations for system change. Strategy 3: Monitor progress using a regional priority dashboard. Strategy 4: Encourage active participation in regional PI committees, processes, and planning. Strategy 5: Provide financial support as available for trauma education, trauma registry and performance improvement training.
Objective 5: Assure that RTC funds awarded are utilized appropriately to meet the needs of the region.
Strategy 1: Provide oversight to assure that hospital and EMS agencies are accountable and responsible for appropriate use and expenditure of funds.
2015-2017 NCRTC Regional Trauma Plan Page 10

Public Information and Education
Goal 3 Educate the public about the NC trauma care system and the purpose of this plan is to inform the general public, decision-makers and the healthcare community about the role and function of the NC Regional Trauma System. Objective 1: Develop a public education plan. Strategy 1: Implement a regional public
information campaign to educate the public about the regional trauma system. Strategy 2: Identify topics and talking points to increase public awareness of the system and value. Strategy 3: Develop pre-packaged public information messages to send to media. Strategy 4: May is trauma awareness month. Develop media release to recognize trauma awareness month with signing of proclamation with Governor, county and city elected officials and distribute trauma awareness materials. Strategy 5: Develop a comprehensive list of media contacts. Strategy 6: Develop a speaker’s bureau.
Objective 2: Provide information to policy makers on key trauma system initiatives and system needs.
Strategy 1: Identify a regional legislative liaison on an annual basis. Strategy 2: Identify key policy makers and/or advocates for the trauma system. Strategy 3: Develop a priority platform plan for distributing information about the trauma system including the trauma DVD and annual report. Strategy 4: Use the RTC specific trauma registry data to describe the trauma system.
Objective 3: Share information with stakeholder organizations on key initiatives (i.e. EMS regional council, regional homeland security council, regional health department council).
Strategy 1: Provide NCRTC information to other stakeholder organizations.
2015-2017 NCRTC Regional Trauma Plan Page 11

System Finance
Goal 4 There is adequate, long-term and sustainable funding to ensure a financially viable trauma system. The trauma system will be recognized as a public good and therefore valued and adequately funded not only for the clinical care actually delivered, but also for the level of readiness required to meet the needs of all injured patients in Kansas. Objective 1: On an annual basis, the NCRTC will develop and implement an operation budget that aligns with the identified goals, objectives and strategies of the Plan.
Strategy 1: Develop and implement an itemized budget annually based on priority needs. Strategy 2: Review financial reports (budget, expenditure spreadsheet) at each executive committee meeting. Strategy 3: Research alternate funding for initiatives and projects. Strategy 4: Provide a quarterly report of expenditures to the ACT.
2015-2017 NCRTC Regional Trauma Plan Page 12

CLINICAL COMPONENTS
Injury Prevention and Control Goal 5
Reduce injury-related morbidity and mortality in the region through primary injury prevention efforts, with trauma system partners, using trauma registry data to identify injury causes and evaluate program outcomes. Objective 1: NCRTC will promote evidenced-based primary injury prevention activities and projects regionally.
Strategy 1: Annually, will identify the top injury causes using trauma registry data and other data sources as appropriate. Strategy 2: Work with EMS and public health systems to identify at least one evidence-based strategy in which will decrease the leading cause of injury for the region. Strategy 3: Work with local health departments and identified health care delivery systems, such as rural health clinics and physician offices, to disseminate injury prevention materials. Strategy 4: Identify available funding sources to support evidence-based and/or best practices activities. Strategy 5: Allocate funds (if available) based on identified injury prevention needs through a grant process that includes an evaluation component. Strategy 6: Coordinate with injury prevention partners to compile a regional (statewide) list of trauma center-based primary injury prevention activities, projects, and programs by county and injury mechanism to post on the Trauma program website www.kstrauma.org.
2015-2017 NCRTC Regional Trauma Plan Page 13

Emergency Preparedness
Goal 6 Have a trauma system prepared to respond to emergency and disaster situations in coordination with regional and state disaster plans. Objective 1: The trauma system, EMS, and all-hazard response plans will be integrated and operational.
Strategy 1: Identify ways to integrate trauma system response into all-hazard state and regional disaster plans. Strategy 2: Invite emergency preparedness key stakeholders to participate at regional council meetings (i.e. provide verbal or written reports of activities in the North Central Region). Strategy 3: Encourage NCRTC leadership involvement in local and regional disaster preparedness planning and training.
Objective 2: Perform a gap analysis on the resources assessment for trauma emergency preparedness.
Strategy 1: Collaborate with regional emergency preparedness coordinators to assess resource gaps.
2015-2017 NCRTC Regional Trauma Plan Page 14
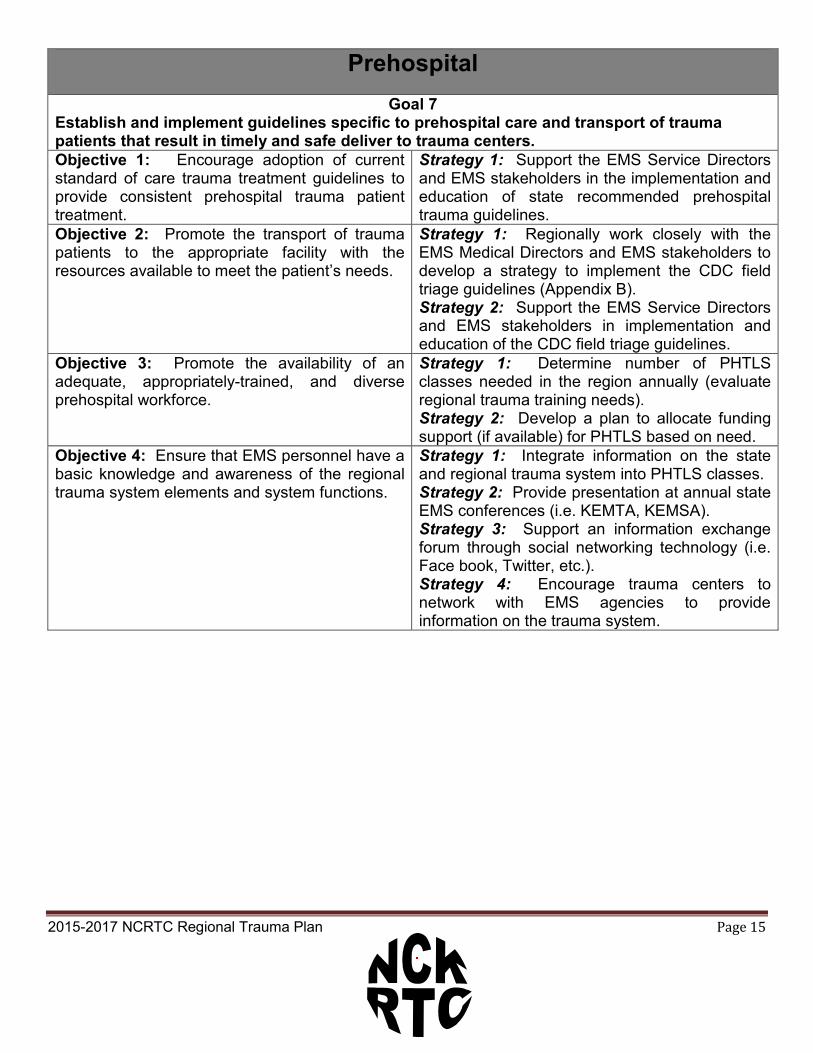
Prehospital Goal 7
Establish and implement guidelines specific to prehospital care and transport of trauma patients that result in timely and safe deliver to trauma centers. Objective 1: Encourage adoption of current standard of care trauma treatment guidelines to provide consistent prehospital trauma patient treatment.
Strategy 1: Support the EMS Service Directors and EMS stakeholders in the implementation and education of state recommended prehospital trauma guidelines.
Objective 2: Promote the transport of trauma patients to the appropriate facility with the resources available to meet the patient’s needs.
Strategy 1: Regionally work closely with the EMS Medical Directors and EMS stakeholders to develop a strategy to implement the CDC field triage guidelines (Appendix B). Strategy 2: Support the EMS Service Directors and EMS stakeholders in implementation and education of the CDC field triage guidelines.
Objective 3: Promote the availability of an adequate, appropriately-trained, and diverse prehospital workforce.
Strategy 1: Determine number of PHTLS classes needed in the region annually (evaluate regional trauma training needs). Strategy 2: Develop a plan to allocate funding support (if available) for PHTLS based on need.
Objective 4: Ensure that EMS personnel have a basic knowledge and awareness of the regional trauma system elements and system functions.
Strategy 1: Integrate information on the state and regional trauma system into PHTLS classes. Strategy 2: Provide presentation at annual state EMS conferences (i.e. KEMTA, KEMSA). Strategy 3: Support an information exchange forum through social networking technology (i.e. Face book, Twitter, etc.). Strategy 4: Encourage trauma centers to network with EMS agencies to provide information on the trauma system.
2015-2017 NCRTC Regional Trauma Plan Page 15

Acute Hospital Goal 8
Establish and maintain a regional (statewide) network of trauma centers, meeting or exceeding standards, for operation and provision of quality trauma care in coordination with all other trauma system participants. Objective 1: Identify additional Trauma Center and Trauma System capacity needs within the region.
Strategy 1: The region will complete a system inventory that identifies the availability and distribution of current capabilities and resources. Strategy 2: Support a statewide “how to” level IV trauma center designation workshop. Strategy 3: Support non-designated participating hospitals to be brought up to Trauma Center designation status. Strategy 4: Encourage that all hospitals work with local EMS agency (ies) to develop trauma treatment protocols. Strategy 5: Ensure that all trauma centers work with local EMS agency (ies) to develop trauma treatment protocols including level IV trauma centers.
Objective 2: All designated and non-designated trauma centers will actively participate in regional performance improvement programs.
Strategy 1: Designated trauma centers will have representation at annual meetings and specific regional PI meetings as identified by the regional PI committee leadership. Strategy 2: Encourage non-designated trauma center participation in specific regional PI meetings as identified by the regional PI committee leadership. Strategy 3: Encourage active participation in regional PI committees, processes, and planning. Strategy 4: Funding priority for education will be given to those hospitals that submit data to the statewide trauma registry.
Objective 3: Assure the availability of an adequate, appropriately-trained, and diverse emergency and trauma care workforce.
Strategy 1: Develop a sustainable regional trauma education plan to meet the needs of TNCC®, ATLS®, and RTTDC® in the region. Strategy 2: Advocate and educate on the need for nursing personnel to be verified in TNCC®. Strategy 3: Advocate and educate on the need for emergency department midlevel practitioner and physician personnel to be certified in ATLS®. Strategy 4: Advocate and educate on the need for hospitals to host a RTTDC®. Strategy 5: Establish a trauma telemedicine network to link trauma centers to rural/community hospitals to provide trauma education.
2015-2017 NCRTC Regional Trauma Plan Page 16

Special Populations Goal 9
The appropriate match of resources will be identified for injured patients with special needs, such as elderly, pediatric, and morbidly obese patients. Objective 1: Evaluate and identify the region’s ability to meet the pediatric care needs and make recommendations for further system development.
Strategy 1: Review trauma registry data for the age group 0-14 to identify trends in injury patterns. Strategy 2: Utilize regional data to develop recommendations for meeting pediatric care needs for further trauma system planning. Strategy 3: Develop and distribute a pediatric resource guide.
Objective 2: Evaluate and identify the region’s ability to meet the geriatric care needs and make recommendations for further system development.
Strategy 1: Identify an age standard for a geriatric patient. Strategy 2: Collaborate with regional EMS Medical Directors in developing prehospital geriatric treatment protocols (example: treatment protocol of patient on anticoagulants). Strategy 3: Utilize regional data to develop recommendations for meeting geriatric care needs for further trauma system planning. Strategy 4: Develop and distribute a geriatric resource guide.
Objective 3: Evaluate and identify the region’s ability to meet the morbidly obese trauma care needs and make recommendations for further system development.
Strategy 1: Identify available resources (such as CT scanners) that can accommodate the needs of the morbidly obese. Strategy 2: Identify prehospital transport systems that can accommodate the needs of the morbidly obese patient. Strategy 3: Promote utilization of EMResource for most current facility resources.
2015-2017 NCRTC Regional Trauma Plan Page 17

Rehabilitation Availability
Goal 10 The region will have well-integrated rehab programs. Post-acute care will focus on helping patients achieve greater independence, a higher degree of functionality, and a faster return to productivity. Objective 1: Identify rehab programs that provide rehab services for injured patients.
Strategy 1: Develop a rehab program resource guide and distribute to hospitals in the region.
2015-2017 NCRTC Regional Trauma Plan Page 18

System Evaluations
Goal 11 Establish a regional trauma system evaluation and performance improvement process. Objective 1: Develop mechanisms that support prehospital agency participation in data submission.
Strategy 1: Review regional trauma data for submission of EMS records as required by state statute. Strategy 2: Encourage completion and submission of a minimal data set to KEMSIS.
Objective 2: Review aggregate data on system performance to identify opportunities for improvement.
Strategy 1: Assure trauma center/hospitals participate in the state trauma registry. Strategy 2: Review and analyze missing and under reported data. Strategy 3: Recommend and review regional benchmark indicators to evaluate system performance, improve care, and further system planning in the region.
Objective 3: There is an organized and regularly monitored system to ensure the patients are expeditiously transferred to the appropriate, system-defined trauma facility.
Strategy 1: Identify indicators for inclusion in regional PI committee trending reports. Strategy 2: Analyze data variances related to utilization of CDC field triage guidelines for EMS transport. Strategy 3: Analyze data variances related to transfer of severely injured patients.
Objective 4: Develop a trauma system data linkage system from all entities in the region to include EMS, trauma centers, other medical facilities, and other data sources that may be available.
Strategy 1: Evaluate different methodologies linking trauma registry data and other data sets such as traffic records and death records.
2015-2017 NCRTC Regional Trauma Plan Page 19

Appendix A NCRTC Hospital Listing
Clay County Medical Center Could County Health Center 617 Liberty 1100 Highland Drive Clay Center, Kansas 67432 Concordia, Kansas 66901 Ellsworth County Hospital Herington Municipal Hospital 1604 Alyward Street 100 E. Helen Ellsworth, Kansas 67439 Herington, Kansas 67449 Jewell County Hospital Lincoln County Hospital 100 Crestvue 624 N. Second Mankato, Kansas 66956 Lincoln, Kansas 67455 Memorial Hospital Mitchell County Hospital Health Systems 511 NE 10th 400 W. Eighth Abilene, Kansas 67410 Beloit, Kansas 67420 Osborne County Memorial Hospital Ottawa County Health Center 424 W. New Hampshire 215 E. Eighth Osborne, Kansas 67473 Minneapolis, Kansas 67467 Republic County Hospital Salina Regional Health Center 2420 G Street 400 S. Santa Fe Belleville, Kansas 66935 Salina, Kansas 67402 Smith County Memorial Hospital 614 S. Main Street Smith Center, Kansas 66967 2015-2017 NCRTC Regional Trauma Plan Page 20

NCRTC Emergency Medical Services (EMS)
Type Legend Type 1: Paramedic or Nurse staffed 24 hours Type 2A: BLS Service with the capability/availability to upgrade to Type 1 Type 2: BLS Service only BENNINGTON AMBULANCE SERVICE 584 N 180TH RD BENNINGTON KS 67422 2A OTTAWA CLAY COUNTY EMS 603 FOURTH STREET CLAY CENTER KS 67432 2A CLAY
CLIFTON CITY AMBULANCE 104 EAST PARALLEL PO BOX 86 CLIFTON KS 66937 2A CLAY
CLYDE COMMUNITY AMBULANCE SERVICE
412 WASHINGTON STREET CLYDE KS 66938 2 CLOUD
CONCORDIA FIRE DEPT EMS DIVISION 701 WASHINGTON CONCORDIA KS 66901 2A CLOUD DICKINSON COUNTY EMS 1001 N BRADY ABILENE KS 67410 1 DICKINSON ELLSWORTH COUNTY EMS 1107 EVANS ELLSWORTH KS 67439 2A ELLSWORTH JEWELL COUNTY EMS 510 E NORTH ST MANKATO KS 66956 2A JEWELL
LIFE TOUCH EMS INC 901 E CRAWFORD SUITE 300 SALINA KS 67401 2A SALINE
LINCOLN COUNTY AMBULANCE SERVICE 216 E LINCOLN AVE LINCOLN KS 67455 2A LINCOLN MILTONVALE AMBULANCE SERVICE 107 STARR AVENUE MILTONVALE KS 67466 2 CLOUD MINNEAPOLIS AMBULANCE SERVICE
218 NORTH ROCK STREET MINNEAPOLIS KS 67467 2A OTTAWA
MITCHELL COUNTY EMS 1906 KS 14 HWY BELOIT KS 67420 2A MITCHELL OSBORNE COUNTY EMS 117 NORTH 1ST ST OSBORNE KS 67473 2A OSBORNE REPUBLIC COUNTY EMS 2405 F STREET BELLEVILLE KS 66935 2A REPUBLIC SALINA FIRE DEPARTMENT 222 WEST ELM SALINA KS 67401 1 SALINE SMITH COUNTY EMS 914 E HWY 36 SMITH CENTER KS 66967 2A SMITH
2015-2017 NCRTC Regional Trauma Plan Page 21

Appendix B 2011 CDC Guidelines for Field Triage of Injured Patients
2015-2017 NCRTC Regional Trauma Plan Page 22