northern exposure - home | tufts university school of...
TRANSCRIPT
MAGA ZINE OF THE TUF TS UN IVERSIT Y MED ICAL AND SACKLER ALUMNI ASSOCIAT IONS FALL 2009 VOL . 68 NO. 3
PLUS: AN UNEASY ALLIANCE ■ TEXAS GRIT ■ MY DAUGHTER IN THE ER
Northern Exposure
MEDICINE
The challenge and reward of beinga doctor in rural Maine

Seeds of ChangeAS A STUDENT IN CELL, MOLECULAR AND DEVELOPMENTAL
biology at the Sackler School of Graduate BiomedicalSciences, Kate Deyst, Ph.D. ’92, learned the skill ofadvocacy. Her training in critical thinking and grant-writing taught her how to develop arguments that“explained what you want to do and how to get othersto agree to fund your project,” she says.
Now Deyst is applying those skills to help low-incomefamilies in central Massachusetts grow their own foodthrough the Growing Places Garden Project, a nonprofitshe co-founded in 2001. Growing Places provides quali-fied families the materials and expertise required to raiseand harvest vegetables for at least two growing seasons.
In the first year, Deyst and the Growing Places staffand volunteers assemble three four-foot by eight-footraised-bed gardens at their clients’ homes, completewith composted soil, seeds and seedlings as well asguidance on how to tend and pick the vegetables.
In the second year, the garden beds are recondi-tioned, and seeds, seedlings and more technical supportare provided. The ultimate goal is for clients to becomeindependent gardeners. Growing Places is available tofamilies who demonstrate need (for example, a family offour making less than $42,000 a year) and an interestand commitment to tending their gardens.
Over the past eight years, Growing Places hasserved 166 households, feeding more than 550 people,and, more importantly, teaching gardening skills thatlast a lifetime. “When we empower our clients to growfresh food, it gives them a new level of independenceand control,” Deyst says. “Giving our clients more foodsecurity and helping them save money are especiallyimportant in these turbulent economic times.”
More information about Growing Places as well asvolunteer opportunities can be found at http://www.growingplaces.org. — dom i n ic brodeu r
PHOTO: STEVEN VOTE
V I TA L S I G N S
departments
2 LETTERS
3 FROM THE DEAN
4 PULSEA S C A N O F P E O P L E & E V E N T S
24 UNIVERSITY NEWS
26 BEYOND BOUNDARIESPROV I D I N G TH E M E A N S F O R E XC E L L E N C E
28 ON CAMPUSM E D I C A L S C H O O L N E W S
36 ALUMNI UPDATE
contents F A L L 2 0 0 9 V O L U M E 6 8 N O . 3
features8 Local Hero
University Chaplain David O’Leary
10 The Coding-and-Billing Spitfire
Dreama Sloan-Kelly, ’02, has found herprofessional niche at last.by Bruce Morgan
C OV E R S T O RY
12 Northern ExposureTufts teams up with an old friend to relievethe doctor shortage in rural Maine.by Bruce Morgan
22 My Unforgettable PatientHow can you stay calm when the patient’s yourown daughter?by Rachel Salguero Kowalsky, M.D./M.P.H., ’03
COVER PHOTO: Cynthia Robertson, ’80, in Bingham, Maine,by Patrick McNamara
34
10

MEDICINE
L E T T E R S
VO L U M E 6 8 N O . 3 FA L L 2 0 0 9
Medical EditorDr. John K. Erban, ’81
EditorBruce Morgan
Editorial DirectorKaren Bailey
Design DirectorMargot Grisar
DesignerBetsy Hayes
Contributing WritersDominic Brodeur, Rachel SalgueroKowalsky ’03, Jacqueline Mitchell,Mark Sullivan
Contributing EditorLeslie Macmillan
Alumni Association PresidentDr. David Wong, ’87
Vice PresidentDr. David S. Rosenthal, ’63
Medical School DeanDr. Michael Rosenblatt
Executive CouncilJoseph Abate, ’62, Carole E. Allen, ’71,Mark Aranson, ’78, Fred G. Arrigg, ’47, PaulG. Arrigg, ’82, Laurence S. Bailen, ’93,Henry H. Banks, ’45, Richard A. Binder,’64, Kenneth E. Blotner, ’64, Betsy Busch,’75, Alphonse F. Calvanese, ’78, Stephen J.Camer, ’65, Gena Ruth Carter, ’87, Do WingChan, ’01, Barbara A. Chase, ’73, Bartley C.Cilento, Jr., ’87, Eric R. Cohen, ’86, FrancisA. D’Ambrosio, ’45, Paul D. D’Ambrosio, ’88,Giacomo A. DeLaria, ’68, Gerard Desforges,’45, Jane M. Desforges, ’45, Ronald W.Dunlap, ’73, Scott K. Epstein, ’84, John K.Erban, ’81, David A. Fisher, ’63, CharlesGlassman, ’73, Brian M. Golden, ’65, Sher-wood L. Gorbach, ’62, Edward T. Gordon, ’47,Michael A. Gordon, ’76, Donna B. Harkness,’79, Thomas R. Hedges, ’75, Frederic F.Little, ’93, Kathleen M. Marc, ’80, Peter D.Martelly, ’83, Tejas S. Mehta, ’92, BrucePastor, ’68, Richard A. Reines, ’76, KarenReuter, ’74, Barbara A. Rockett, ’57, LauraK. Snydman, ’04, Paul J. Sorgi, ’81, Susan J.Stein, ’85, Elliott W. Strong, ’52, Gerard A.Sweeney, ’67, James A. York, ’92
Tufts Medicine is published three timesa year by the Tufts University Schoolof Medicine, Tufts Medical AlumniAssociation and Tufts University Offi ceof Publications. Send correspondence toBruce Morgan, Editor, Tufts Medicine,136 Harrison Avenue, Boston, MA 02111or e-mail [email protected] medical school’s website iswww.tufts.edu/med.
THE BIG DISCONNECTReading your Spring 2009 cover story(“Pressure Drop,” by Susan Cl intonMartin, M.D./M.P.H., ’04) about lifestyleissues during residency brought up a lot ofmemories. I was propelled back to my ownpediatrics residency at the same institu-tion in the early 1990s, when I would havediscussions with my advisor and residencydirector about whether I wanted to gopart-time.
As I was in my junior year of my resi-dency and expecting my first child, thiswas not an easy decision to make, and Ihad seen mixed results with other residentswho had attempted that path before me. Inthe end I opted to not go part-time, for thereasons mentioned in the article, includ-ing the longer length of overall residency,the decreased pay and benefits (not idealwith a baby at home!), the resentment ofcolleagues who feared extra work on theirplates, and the lack of support from theresidency program.
I opted to just forge ahead and deal withhaving a baby while being a full-time resi-dent. I don’t regret that decision. I had thesupport of some attending physicians andcolleagues, friends, my husband and thehelp of a wonderful nanny. It wasn’t easy,but is there ever a great time to have a babyin the medical profession? Let’s be honest—residency is one of the most challengingtimes for a physician, and adding any stressmakes it that much worse.
Balancing work and family is never easyin any career, but particularly challengingas a doctor and incredibly challenging asa resident physician, where you don’t con-trol your time. Residency programs haverather rigid schedules, and even the mostthought-through back-up systems can’taccommodate the last-minute issues thatoccur unexpectedly when you are a newparent and have a baby at home.
Reading that Dr. Martin was braveenough to go part-time was like seeing arose among weeds. The benefi t to her andher family was enormous. When workingher “on” months, she could focus and feelless guilty, knowing her time with her fam-ily was coming. During her “off” months,she could stay refreshed and emotionallyaccessible to her family.
There’s a big disconnect in medicaleducation between our desire for a betterlifestyle and what is available—no differentfrom what those of us who have completedour education and training have experi-enced in the health-care system for years.While it’s discouraging that our caring pro-fession doesn’t have a system that allows usto care for ourselves and our families, it’sencouraging that we are all fi nally speakingup to say that fi nding balance between workand home isn’t a frill, but a necessity—evenfor physicians.
gw en n schurgin o’k eefe , ’92ceo, pedi atr ics now
way l a nd, m assachusetts
2 t u f ts m e d i c i n e f a l l 2 0 0 9
Bruce Morgan
Editor, Tufts Medicine
Tufts University
Office of Publications
136 Harrison Ave.
Boston, MA 02111
TALK TO USTufts Medicine welcomes
letters, concerns and
suggestions from all its
readers. Address your
correspondence, which
may be edited for space, to
Bruce Morgan, Editor, Tufts
Medicine, Tufts University
Offi ce of Publications, 136
Harrison Ave., Boston, MA
02111. You can also fax us
at 617.636.4075 or e-mail
Tufts Prints GreenPrinted on 25% post-consumer wasterecycled paper. Please recycle.

F R O M T H E D E A N
Accordingly, rather than limiting basic sciences to the first two years and treating them as a separate curricular block, they will be woven throughout the entire four years of medical school. We want our students to stay current with developments in the lab for the betterment of their patients’ health—and develop the habit of staying current as well.
A second important divergence from the traditional curriculum addresses the changing role of doctors in the health-care process. Formerly, it was standard procedure for medical schools to educate their students with the idea that, once graduated, they would act as independent agents in their careers. That approach no longer makes sense. Medicine has grown too complex and science too complicated. Now it is more critical for physicians to be effective collabo-rators with their colleagues and co-workers. Doctors must be both team members and leaders to serve their patients well.
The third departure from curricular tra-dition involves an awareness of “best prac-tices.” In our context, best practices means simply that a stringent analysis of treatment and outcomes has been done to determine optimal approaches, whether the immedi-ate question concerns a patient’s chronic asthma, heart attack or broken hip. We intend to teach our students how to iden-tify best practices, deftly sort through trial implications and make good use of what they find through enhanced training in statistics.
It’s true that the future is an uncertain thing. But we believe we are primed and ready for the next stage of medicine.
if there is any one thing we are best known
for here at the medical school, it is the quality
of our education. From our humble beginnings
back in 1893, when seven visionary Boston
gentlemen pooled their resources to found the
school, the distinctive way we teach and train
students has been our f lagship product, first
embodied in the creation of skilled general prac-
titioners for New England and later by the graduates who ventured forth
to set up practices elsewhere in this country and around the world.
Education remains paramount in our thinking; nothing has changed in that regard. But beginning this fall, the curriculum at Tufts assumed a new shape and form to match our freshly renovated facilities. Developing our curriculum has been a passionate collaborative effort involving more than 150 faculty, staff and students in 17 working groups drawn from our seven affi liated hospitals over the past two years.
The challenge for any medical school is fi guring how best to provide its stu-dents with the essential elements they will need to practice medicine in the near future—say, fi ve to 10 years after they graduate—and beyond. Speaking in terms of American medicine, both the content and the delivery systems for health care are in fl ux and likely to remain so. This means that much of the body of knowledge acquired by medical students is destined to become obsolete before long.
What’s needed is a medical curriculum that holds lasting value throughout the permutations that the future will bring. In that light, we propose to teach our students some basic concepts fundamental to medicine. We’ll introduce them to good habits of medical thinking while modeling the social dynamics that we think are apt to prove most useful in their careers. To those of us who went through medical school 35 or 40 years ago, as I did, this may sound hopelessly open-ended and vague. Even so, in the early 21st century we can be sure that any curriculum that is over-designed will surely fail.
How will the new curriculum differ from what we’ve known? Let me high-light three main points of divergence.
First, medical students have traditionally concentrated on basic sciences during the fi rst two years and then shifted their attention to clinical practice in the third and fourth years. But the world of medicine has changed dramati-cally since that model was devised. Whether we are talking about fresh dis-coveries in genetics and genomics or human metabolism or some other aspect of “personalized medicine,” the basic sciences are more pressingly relevant to primary care than they were before.
Teaching the Future
f a l l 2 0 0 9 t u f ts m e d i c i n e 3
michael rosenblatt, m.d.
PHOTO: ALONSO NICHOLS
pulseA SCAN OF PEOPLE & EVENTS
4 t u f ts m e d i c i n e f a l l 2 0 0 9 ILLUSTRATIONS: HADLEY HOOPER
Off shore Surgeryn recent years, americans have been flocking to hospitals abroad
for cheaper surgery than can be found at home. That’s not necessarilya bad thing, argues Distinguished Professor Jerome P. Kassirer in anop-ed piece he co-authored for the New York Times in June.
Average fees at certain respectable hospitals in India are 60 to 90 percentless expensive than the average cost of the same procedures in the U.S., theessay notes. Most American medical travelers venture abroad for cosmetic pro-cedures such as facelifts and liposuction, but an increasing number are elect-ing high-risk operations like heart surgery and joint replacement in places likeIndia, Singapore and Thailand.
“Is this a good idea?” the authors ask, quite reasonably. “The only way toknow is to fi nd out how foreign hospitals and surgeons compare with theirAmerican counterparts.”
A few pioneering insurers—notably BlueCross BlueShield of South Carolina—have evaluated foreign hospitals, come away impressed, and now offer payment
for travel expenses and cash incentives ashigh as $10,000 for those choosing the off-shore option. The savings are so great that inmany cases, especially for the most complexoperations, “savings far exceed these pay-ments,” the authors point out.
More than 200 offshore hospitals havebeen accredited by the Joint CommissionInternational, an arm of the same organi-zation that accredits American hospitals.Many employ English-speaking surgeonswho have trained in the U.S. But right nowthere is no uniform standard for comparingdomestic and foreign surgical experiences,both short- and long-term.
“Should offshore surgery be welcomedas a modest way to make American healthcare more affordable?” the authors wonder.“We can’t know until we can directly com-pare the outcomes with those of Americansurgery.”
I
PHOTOS: ALONSO NICHOLS
Kuvin and Soffl er
HEART RISK INFORMATION AT YOUR FINGERTIPS
ESULTS OF A STUDY CONDUCTED BY RESEARCHERS AT TUFTS
Medical Center and the Mayo Clinic show that a simplefi nger sensor test is “highly predictive” of a major cardiacevent such as heart attack or stroke for people at low or
moderate cardiovascular risk.The fi nger device, called the EndoPAT, assesses the health of a
person’s endothelial cells by measuring blood fl ow. Endothelial cellsline the blood vessels and regulate normal blood fl ow. If these cellsdon’t function properly, the condition can lead to hardening of thearteries and major cardiovascular health problems. The technology forEndoPAT was fi rst described by Jeffrey Kuvin, associate professor ofmedicine, and his Tufts Medical Center colleagues in 2003 and hassince been widely adopted.
EndoPAT consists of digital recording equipment and two fi ngerprobes resembling large thimbles. For the 15-minute test, probesare placed on each index fi nger and hooked up to a small machine tomeasure blood fl ow. A blood pressure cuff is placed on one arm; theother, uncuffed arm acts as the control. A reading of the fi ngers’ bloodfl ow begins, and then the blood pressure cuff on one arm is infl atedand defl ated in sequence, allowing for timed readings.
Researchers tested the device in 270 patients between the agesof 42 and 66 and followed their progress from 1999 to 2007. Some49 percent of patients whose EndoPAT test indicated poor endothe-lial function had a cardiac event during the eight years of follow-up.Morgan Soffl er, ’11, assisted with the Tufts portion of the study.
“The results of the study may help clinicians identify patients whomay be at increased cardiovascular risk,” Kuvin points out.
RRalph Isberg, professor of molecularbiology and microbiology, has beenelected to the National Academy ofSciences in recognition of his distin-guished and continuing achievementin original research.
Isberg is a Howard HughesMedical Institute Investigator and a member of the pro-gram in molecular biology and microbiology at the SacklerSchool of Graduate Biomedical Sciences. His research isdirected toward investigating the molecular mechanismsof bacterial uptake and intravascular growth in host cells.
The National Academy of Sciences, founded in 1863,is a private organization of scientists and engineers whoserve as offi cial advisers to the federal government onscience and technology issues. The organization’s currentactive membership totals 2,150.
Surgery and airplane fl ights do not always mix well,
according to a new study conducted by a Tufts expert.
Air travel can increase the risk of deep vein throm-
bosis, or potentially lethal clots in the deep veins of
the legs, and the danger rises if you’ve recently had an
operation. Doctors sometimes fail to warn their patients
of this connection.
If you’ve had an orthopedic, chest, abdominal,
neurological, or ear, nose and throat procedure, it’s best
to wait 10 to 14 days before fl ying, says lead author Mark
Gendreau, assistant professor of emergency medicine.
A fi ve-day wait should suffi ce for a patient who’s under-
gone an uncomplicated appendectomy or laparoscopic
procedure, he said.
Once in fl ight, a good rule of thumb is to stay well
hydrated, avoid caffeine and alcohol, stretch your calves
by doing exercises in your seat or walking the aisles and
wear compression stockings.
Fly Safe
ISBERG NAMED TO NAS
f a l l 2 0 0 9 t u f ts m e d i c i n e 5
P U L S E
6 t u f ts m e d i c i n e f a l l 2 0 0 9
Old Men and Their Bones
Despite the prevailing culturalmessage that women are the onlyones at risk of developing thebone-thinning ailment known as
osteoporosis as they age, men can’t ignorethe threat, experts say. Though osteoporosisis less common in men than in women, ittakes a toll on both genders.
“It’s basically unrecognized,” says onephysician about the problem. “The wordon the street is that this is not a disease thatguys get, and that is clearly incorrect.”
While a 50-year-old woman faces a life-time risk of 50 percent for an osteopathicfracture, anywhere from one in eight to one infour 50-year-old men face that same risk. Thedisease may be even more serious in menthan in women, notes Felicia Cosman,medical director of the nonprofitNational Osteoporosis Foundation.In hip fractures, for example, “thecomplication rate is higher, thedeath rate is higher,” she says.
The death rate for women
is between 15 and 20 percent, and for menit stands between 20 and 25 percent. Thereason for the difference is not clear, butCosman suggests that men who fracturetheir hips are typically older than womenand may be in poorer initial health.
Since 2000, researchers funded bythe National Institute of Arthritis andMusculoskeletal and Skin Diseases havebeen studying 6,000 men age 65 and olderat six U.S. medical centers as well as sitesabroad to better comprehend the disease,from men’s bone geometry to bone loss andfracture rates. Dr. Clifford Rosen, professorof medicine at Tufts and the Maine MedicalResearch Institute, says the study can’t come
soon enough.“I don’t think we have a good
understanding of the epidemiologyof this disease,” Rosen observes.
“Men tend to come to physicianslater, and we don’t understand
what the natural history ofthis disease is in males.”
Mark S. Drapkin, associate chief of the InfectiousDisease Service at Newton-Wellesley Hospital anda professor of medicine, was among 20 Bay Statedoctors to be named 2009 Community Clinicians ofthe Year by their peers.
The award, established in 1998 by theMassachusetts Medical Society, recognizes a phy-sician from each of the Society’s district medical
societies who has made signifi cant contributionto his or her patients and the community. Drapkinhas been on staff at Newton-Wellesley and on theTufts faculty since 1975. A graduate of the StateUniversity of New York Downstate Medical Center,he has received 17 awards for teaching excellenceand was the 2007 recipient of the Milton O., M30,and Natalie V. Zucker Clinical Teaching Prize.
CLINICIAN OF THE YEAR
Responding to an article in the New
York Times about American medi-
cal care for elderly patients, Robert
Dickman, associate clinical profes-
sor of public
health and
family medicine,
pointed out in a
letter to the edi-
tor just how few
board-certifi ed geriatricians exist.
“I often see octogenarians along
with their daughters and aides, and
each person has questions that need
to be answered,” Dickman wrote.
“Granny has (at least) six problems
and 10 medicines. For all of this,
Medicare will pay a fee for service
that is not much more than might be
paid for treating a sore throat.”
He concluded: “Until our services
are adequately valued, there will be
way too few of us to care for Granny.”
Way Too Few
PHOTOS: COURTESY MASSACHUSETTS MEDICAL SOCIETY (DRAPKIN); RICHARD HOWARD (DICKMAN)

A lack of diligent hand-washing among doc-tors and nurses contributes to an estimated1.7 million hospital-acquired infections inthe U.S. each year. With that hazard in mind,several Boston hospitals have launchedaggressive hand-washing campaigns.
Tufts Medical Center used to havepoor hand-washing rates—as low as 33percent, according to a story broadcaston Boston’s WBUR radio. That was typi-cal of many U.S. hospitals, according tothe radio report. For example, fi ve yearsago Massachusetts General Hospital wasfound to be following its own hand-wash-ing rules just 30 percent of the time.
MGH has since installed hand sanitizersall over the hospital and launched a nurse-led rap video to boost compliance. Over the
past year, using campy humor, Tufts MedicalCenter launched its own hand-washing cam-paign to improve its numbers.
“If you ask anybody in the hospital,
everybody would answer, ‘Oh, yes, washingour hands—we do that, it’s important,’ ”says David Fairchild, chief medical offi cer atTufts Medical Center and associate professorof medicine. “It’s just that in the hectic day-to-day, it’s one of those things that occasion-ally get missed.”
For it s ca mpa ig n, Tuf t s Medica lCenter borrowed a page from the popularBudweiser commercials, distributing but-tons that say “washup” instead of “wassup.”The hospital has also placed giant signsnear sinks, reminding staffers to wash theirhands before and after direct contact withpatients or after touching any object near apatient such as pagers, keyboards and med-ical equipment. Hand-washing compliancenow approaches 100 percent.
f a l l 2 0 0 9 t u f ts m e d i c i n e 7
Wash Up, Dude?
‘GI JOE’ AT THE CENTURY MARKJoseph B. Kirsner, ’33, entered medical school the week the stockmarket crashed in 1929. He still goes to his offi ce at the University ofChicago Medical School three days a week.
In late May, friends and colleagues held a dinner in Kirsner’s honor. Therewas plenty to thank him for. Beginning with his gastroenterological researchin 1935, at a time when it was not yet a medical specialty and digestivedisorders were commonly thought to be more psychological than physical,Kirsner played a signal role in creating the fi eld of gastroenterology, publish-ing textbooks that are still considered the gold standard on infl ammatorybowel disease. In medical circles he earned the affectionate nickname “GI
Joe” for his specialty of choice.At the dinner, grateful former pa-
tients praised Kirsner’s sympathy andabiding warmth. “Because of you, Ihave had a very fulfi lling life,” ValerieHerschman, a grandmother fromFlorida who originally sought treat-ment for a complicated ailment morethan 50 years ago at the age of 19,told Kirsner with emotion in her voice.“I was never just a number to youwhen I was a patient in your care.”
Speaking of numbers, Kirsnerturned 100 years old on September 21.
MOTTA HEADS MMS
Mario Motta, ’78, a cardiolo-gist based in Salem, Mass., hasbeen elected president of theMassachusetts Medical Society. Aspresident, he will serve a one-yearterm as the top offi cer of the societywhose membership includes morethan 21,000 doctors, residents and
medical students across the state.Board-certifi ed in internal medicine, cardiology and
nuclear cardiology, Motta practices at North ShoreCardiovascular Associates, a private group practice inSalem. He has been a member of the Medical Societysince 1974 and has a long record of service to theorganization. He was president-elect and vice presidentfor the last two years and served as a member of theBoard of Trustees and House of Delegates, among otherresponsibilities.
A magna cum laude graduate of Boston College, Mottais director of the Nuclear Laboratory at Salem Hospitaland a member of the Committees on Cardiac Care,Pharmacy & Therapeutics, and Radiation Safety. He hasbeen a clinical professor of medicine at Tufts since 1993.
The Massachusetts Medical Society, founded in 1781,is the oldest continuously operating state medical societyin the country.
PHOTO: COURTESY MASSACHUSETTS MEDICAL SOCIETY (MOTTA)
BY BRUCE MORGAN PHOTOGRAPH BY ALONSO NICHOLS
the rev. david o’leary has been the university
chaplain at Tufts University and a senior lecturer inmedical ethics on the health sciences campus since2002. Although he holds a glittering raft of academiccredentials from St. John’s Seminary, Boston Collegeand Oxford University, he began humbly enough inthe working-class town of Lynn, Mass., where his dadpunched the clock at the United Shoe factory and hismom worked for the phone company. “We weren’tactive Catholics,” says O’Leary quietly, “but churchwas part of the life.”
His doctoral dissertation at Oxford was titledThe Roman Catholic Perspective on the Moralityof Withdrawing or Withholding Food and FluidAdministered to an Individual in the PersistentVegetative State. He survived his oral defense despitethe presence of a pesky Dominican priest on the facultypanel who quizzed him repeatedly about the metaphys-ics of the soul of a dying person. Each time the priestbore in, O’Leary responded that this topic lay beyondthe scope of his thesis. “I didn’t know anything about it,other than the defi nition of metaphysics as looking fora black cat in a dark room that isn’t there,” he laughs.
O’Leary wears many hats. In addition to his regularteaching responsibilities at several Tufts schools and hisday-to-day work in the trenches of campus ministry, healso serves as a member of the Institutional Review Board(IRB) at Tufts Medical Center. We spoke in O’Leary’ssunlit offi ce on the ground fl oor of Goddard Chapel onthe Medford/Somerville Campus.
Q: When you fi rst expressed an interest in entering thechurch, what was your parents’ reaction?Oh, they weren’t that pleased. They would have preferredgrandchildren and didn’t understand how a son couldbecome a priest. The idea grew on them after a while.
Q: Why did you pursue your doctorate in medicalethics, as opposed to some other focus?I was drawn towards moral theology, and then I got mylicentiate degree in Catholic social ethics. I fi gured I hada great foundation in moral Catholic social teaching,and then the fi eld was getting more and more involvedin medical issues, so I said, well, let’s jump on that.
Q: Tell me about the class you teach at the medicalschool.When I’m there I just try to raise the question: Who isthe doctor or the researcher working for? It’s not oneanswer—it’s profession, practice, patient. You haveto fi gure out where your lines are. And then I alwaystry to pass on what I learned from a great doctor atGeorgetown, Dr. Edmund Pellegrino. He always usedto say to his interns that the first question to ask is
“How may I help you?” and not “What is wrong?” Whyput the person in the negative to begin with? You arethere to help. Let the patient start the conversation. Inthat way you’re restoring dignity.
Q: What sorts of issues come up in your InstitutionalReview Board role?All research on human subjects has to be approved byan ethics committee, according to federal guidelines.Everyone on the committee has their one categorywhere they like to be a specialist, and for me it’s to makesure the subject has the freedom to say yes or no to par-ticipation. If someone’s coming at you with a clipboard,and it’s your doctor—well, where’s the line of freedom?Can the person say no?
Q: Freedom seems to run through a lot of what youcare about, whether it’s freedom at end of life orfreedom to determine one’s own course.Yes. Now I’m betraying my own training. I trainedunder a great priest, Josef Fuchs, a German theologian.His thing was freedom. He said the human person is soconstitutive of a being that’s created with freedom thateven after the point of physical death, God would giveus the freedom to choose.
I’ve used that many times in celebrating the sadoccasion of someone’s funeral due to suicide to say, OK,he or she might have made a wrong decision based ona clinical depression or a chemical imbalance in thebrain, but the next time they were given a choice I’msure they chose God. TM
Medical Ethicist
8 t u f ts m e d i c i n e f a l l 2 0 0 9

University ChaplainDavid O’Leary
L O C A L H E R O

10 t u f ts m e d i c i n e f a l l 2 0 0 9
Dreama Sloan-Kelly, ’02, in Shirley, Mass.

Spitfire
f a l l 2 0 0 9 t u f ts m e d i c i n e 11
what kind of med student has the spare time and
energy to pitch Mary Kay cosmetics to instructors during her third-year surgery rotation, and succeed at it? “You would see me in general surgery—all the sur-geons were buying baskets for their wives,” Dreama Sloan-Kelly, ’02, says. “They would tell me, ‘Dreama, you’ve got skills other than medicine.’ ”
Blame Texas, if you like. That’s where Sloan-Kelly spent her childhood, accompanying her ex-Air Force dad as he moved from managing one construction project to the next at sites across the Lone Star state. “I was always with him,” she recalls happily. “I was his partner in crime.” Her whole family had an entrepre-neurial spirit and a knack for reinvention. Sloan-Kelly was serving beer at rock concerts around her home-town of Dallas when she was 12 years old.
It wasn’t until she reached Wellesley College that her hyperkinetic intellectual style posed a problem. There, she had trouble settling down long enough to master a foreign language. A professor told her simply, “I think you have a problem.” Even now, Sloan-Kelly sounds vague about the nature of her disability. “I can analyze anything. I love puzzles,” she says, “but I couldn’t do a foreign language.”
Medical school tightened the screws. Sloan-Kelly describes it as “a time of utter confusion, misery and growth.” She got married. She got pregnant—twice—and left school each time, taking six years to earn her degree. Then there was her robust extracurricular life. She sold Mary Kay cosmetics her third year. By fourth year, she had begun teaching massage therapy in the evenings at a Cambridge school. And all through her medical training, she pursued a keen interest in medi-cal billing procedures. “The doctors used to tell me, ‘Dreama, this is not normal,’ ” she admits.
Her fi rst real job, as director of the medical assis-tant program at a technical school called the Career Education Institute in Somerville, Mass., tapped this
side of her. At CEI, she was teaching students, many of them from disadvantaged backgrounds, how to han-dle coding and billing procedures in doctors’ offi ces. With typical zeal, which included leading her charges in rapid-fi re chants of “I think I can, I think I can,” she made a success of it, and them. The program began with 10 students; by the time Sloan-Kelly left a few years later, 700 were enrolled.
Kelly, Sloan and Associates has been her life for the past four or fi ve years. Operating out of a small offi ce in a former mill building in Shirley, Mass., with her MIT-educated husband, Horace, as partner, the company sells coding-billing seminars—where she generally hits the stage wearing “a low-cut dress, high heels and all kinds of bling”—as well as coding-billing guidebooks she has written tailored to individual spe-cialties and software programs that provide computer “audits” for medical practices.
“No part of this is intuitive,” warns the boss. “Unless you know the reasons why you have been denied reimbursement, you will die on the vine.” Right now, the business is growing at a pace of 20 or 30 percent annually.
Boston lawyer Robert Blaisdell found Sloan-Kelly’s help decisive in a case where he was defending a phy-sician who had been caught in a random audit by Medicare. “She was fantastic. She made a huge dif-ference,” he says. The M.D. on Sloan-Kelly’s business card gave her instant credibility. “She knows the cod-ing inside out, all the nuances of it, and was able to explain things to Medicare by talking on their level. I was there, and I could see the impression this made” on the auditors, Blaisdell relates.
In a way, all the chickens have come home to roost, from her days as a beer-jerk teen to restless medical student with blush and lipstick for sale. As Sloan-Kelly told her mom recently, “Every ounce of my life makes sense now.” TM
The Coding-and-Billing
After years of hopping from one passion to the next,
Dreama Sloan-Kelly has found her niche BY BRUCE MORGAN
PHOTOGRAPHY BY STEVE MARSEL, A78
12 t u f ts m e d i c i n e f a l l 2 0 0 9
Northern
BY BRUCE MORGAN PHOTOGRAPHS BY PATRICK McNAMARA
12 t u f ts m e d i c i n e f a l l 2 0 0 9
f a l l 2 0 0 9 t u f ts m e d i c i n e 13
exposureA bold partnership between Tufts and Maine Medical
Center seeks to relieve the doctor shortage in rural
portions of New England’s largest state
the old guy wearing blue jeans and a ball cap leans inat the little arched window, his hips out to one side, to absorba story that his friend is telling about a mutual acquaintance.
“Well, I told him I don’t know if we can do it then. We’ve gotcompany coming for dinner that night,” the seated woman issaying. She is middle-aged, with glasses and a quiet, unhurriedmanner. “But you know how he is,” she adds.
Just then, another younger woman carrying a clipboardpasses by behind the fi rst. “Hello, neighbor,” says the man at thewindow, catching her eye. She looks up and fl ashes him a smile.“Haven’t seen you lately,” the young woman shoots back.
Remarkably, all of this geniality is occurring in the waitingroom of a doctor’s offi ce at a hospital in Houlton, Maine, two
thirds of the way up the state on the right-hand side. The easy-going woman expecting company for dinner is the receptionist;the man in loose-fi tting jeans is the patient, and the womangliding by in the background is a nurse. We are a far cry fromthe studied detachment and the-doctor-will-see-you-now cool-ness of an urban milieu.
The fun doesn’t end in the waiting room. Once the man injeans is called to his appointment, he can be heard laughing inthe near hallway, where someone new is telling him, “My grand-mother loves that place. The soups are good, too. So how youbeen?” “Oh, pretty good,” he says, moving gradually towardthe doctor’s exam as though this were a poker game with palsthat he’d been looking forward to all week.

CREDIT_SMALL_FL14 t u f ts m e d i c i n e f a l l 2 0 0 9
It’s a different pace up here, but the friend-liness and winsome good cheer on display in Houlton are misleading in a way. This after-noon’s sunny mood masks a crisis for rural Maine. Few young doctors are electing to practice medicine in small-town Maine, and the consequences of this long-term trend are dire for the people who live in far-fl ung loca-tions such as this.
There are really two Maines. The first, consisting roughly of the coastal band that arcs from the New Hampshire border up to Acadia National Park, is well-known and beloved by calendar makers, who can’t resist the look of snug harbors fi lled with sailing craft and lobster buoys heaped in the side yards of the cottages. Once you go 30 or 40 miles inland, or push much farther up the coast, however, all bets are off. You enter an area of small towns, immense fi elds and deep woods. The state turns poor and bedraggled-looking fast. “As you move away from the south-ern coast and get north of the I-95 corridor around Bangor, that’s where the challenge is,” confi rms Charles Dwyer, director of the state’s Offi ce of Rural Health and Primary Care.
Doctors tend to be more concen-trated in cities than in rural areas. While this is a national demographic truth, Maine is harder hit than most places. According to a comprehen-sive report released by Dwyer’s offi ce in 2008, only fi ve other states in the U.S. have a higher percentage of
people living in non-metropolitan areas—an index known as a state’s degree of “rural-ity.” The report found that Maine’s rural residents are older, poorer, sicker and less educated than its more-urban dwellers. They are more likely to be unemployed. They suf-fer disproportionately from chronic illness and substance abuse. In medical terms, rural residents are hanging by a thread. And just 39 percent of them have a personal doctor.
In Maine, as elsewhere, doctors are get-ting older and retiring. The trouble is that
their numbers are not being replenished. As director of the Maine Hospital Association, which tracks physician openings around the state, Jane Ham knows this better than any-one. (Few doctors in Maine are not affi liated with a hospital.) “It’s a worsening situation,” she states. “When we started our recruitment center a decade ago, we had 91 openings. A year or so ago, we had 206. Now we’ve got 272 physician openings, of which 121 are in primary care—the backbone of health-care delivery in Maine.”
To narrow the gap, Maine began importing foreign doctors to com-plete their residencies in rural areas under a federal J-1 visa program, which requires that the visa recipi-ents practice for three years in an underserved area. According to Dwyer, 116 foreign-trained doctors unpacked their bags at sites around the state between 1997 and 2004.
Charles Macomber, ’59, saw this f irsthand. Following retirement from a stressful obstetrics practice in Concord, N.H., Macomber spent a gratifying spell treating grateful patients at a hospital in Caribou, Maine, 50 miles north of Houlton.
Scenes from around the state reveal the plain life and simple beauty of the place. At left and above: streetscapes of Bingham and Houlton, respectively.Below: boats moored in a harbor near Sullivan, Maine.
“ We believe every physician we get coming to this state is a difference-maker.”
—Tim Chu rchil l , hospita l ceo

f a l l 2 0 0 9 t u f ts m e d i c i n e 15
“Those were the two best years of my pro-fessional life,” he is quick to say. The bulk of doctors he worked with were not born in the United States, Macomber reports, citing Canadian, Sri Lankan, Indian, Filipino and Chinese physicians on staff.
Late this summer, in partnership with Maine Medical Center, the medical school launched an innovative program aimed at alleviating the physician shortage in rural and small-town Maine. Called the Maine Track, the program enrolled 36 students who have shown promise for establishing practices in the state. Of these, 20 slots were reserved for Maine natives or applicants with close ties to the state. Half-tuition scholar-ships were offered to these students as an added enticement (see sidebar, this page).
“Tufts has a strong track record of train-ing Maine physicians, and there are more than 300 Tufts-educated doctors now liv-ing in Maine, with perhaps half this num-ber engaged in active practice,” says Michael Rosenblatt, dean of the medical school. From the 1930s through the early 1980s, federal funding provided opportunities for Tufts stu-dents to work in Maine hospitals, including Maine Medical. “Although this is a new agree-ment,” Rosenblatt notes, “our affi liation with Maine Medical Center began in the 1930s. We are excited to re-establish and revitalize this important relationship.” Peter Bates, chief of medicine at Maine Medical, calls the joint enterprise “the perfect match of needs and philosophy” between the two institutions.
Maine Track students will spend their fi rst two years in Boston before shifting to the 600-bed Portland hospital for their third-year clerkships and part of their fourth-year rotations. Extended, multi-month clerkships will ultimately be offered at a half-dozen sites around the state so that students can immerse themselves in community-based medicine on an intimate scale.
Give the kids a whiff of pine and hope they like it and decide to stay—that’s the gist of the idea. “It’s all about quality of life,” Jane Ham points out. “We always tell doctors they can have a good clinical practice here, plus be able to spend time with their family.” And what if the prospective docs enrolled in the Maine Track sample the country life and decide they don’t like it? “Well, at least
The Home Team
AN ABIDING LOVE OF NEIGHBORHOOD, TOWN OR REGION IS A POWERFUL MOTIVATION TO HANG
near home in your professional life, as these Maine natives can attest. All three are mem-bers of the inaugural class of the Maine Track program, a partnership between Tufts Medical School and Maine Medical Center in Portland aimed at encouraging more physicians to practice in this doctor-starved state.
Growing up the daughter of a grocer in Steep Falls, near Sebago Lake in western Maine, Amanda Call, ’13, didn’t run into many doctors. Whenever she visited the nearby medical clinic in Cornish, she says, “It was always overcrowded, with a lot of impoverished people there.” That lack of access to medical care is something she hopes to rectify by establishing a practice in Steep Falls—perhaps in obstetrics and gynecology. “There aren’t many women physicians in my area. I would love to practice in the community that I grew up in, and maybe someday have my own clinic,” says the 22-year-old Call, who completed her pre-med studies at the Maine College of Pharmacy.
“My goal is not to make a bunch of money,” she remarks, “but to have a stable practice back home.”
Heather Bradford, ’13, concurs. A native of Eddington, Maine, a small town on the Penobscot River 20 miles east of Bangor, she has seen fi rsthand the twin barriers to quality health care for area residents—fi rst, the general scarcity of docs, and second, the inability of would-be patients to afford treatment. “A lot of times they don’t have insurance or the fi nances even to shell out for a co-pay,” Bradford says of her fellow Mainers. Coming from a single-parent household on a lean budget, Bradford is grateful for the half-price tuition deal she has gotten from her enrollment in the Maine Track.
With any luck, that generosity will help guide her return home. “I can’t imagine going anywhere else,” she says.
Chad Szylvian, ’13, the son of an electrician, refl ects a similar blend of gratitude and com-mitment. The salutatorian of his high school class, a member of the football team and a jazz pianist, he has spent time volunteering at Eastern Maine Medical Center near his home in Brewer. Four years at Boston College left him $146,000 in the hole. “Before the Maine Track program came along,” he says, “I was looking at $50,000-some a year for medical school on top of my other debt, so that half-tuition defi nitely helps.”
Because Maine has no allopathic medical school of its own, Szylvian notes that people in his shoes have no shot at an in-state tuition rate for their medical training. But he’s all set now. He intends to add a public health degree to his M.D. and return home to practice in a place where “it feels like you can breathe better,” he says.
Chad Szylvian, Heather Bradford,
and Amanda Call atMaine Medical Center
Continued on page 17

CREDIT_SMALL_FL16 t u f ts m e d i c i n e f a l l 2 0 0 9
Top: Cynthia Robertson on Bingham’s main drag. “I’m proud to do good medicine in a small place,” she
says. Above: The Kennebec River fl ows nearby. Right: the Bingham Area Health Center near the town center.

f a l l 2 0 0 9 t u f ts m e d i c i n e 17
they’ve had some exposure,” Ham responds, laughing. “Rural life is not for everybody. But right now they’re not getting any exposure at all.” Maine has no allopathic medical school of its own, exacerbating the doctor-supply problem.
Let’s do some math. The Maine Track will enroll 36 students per year. The program’s goal is to retain 75 percent of the class as physicians practicing in rural Maine. Even if the ambitious goal is reached—27 doctors annually—that’s not a huge number. A skep-tic might wonder how much difference this few can make when distributed across a state as large and needy as Maine.
Don’t let Tim Churchill hear it. He’s pres-ident and CEO of Western Maine Health, which operates Stephens Memorial Hospital in Norway, Maine, a blue-collar town of 5,000 residents a short hop north of Portland. The 50-bed hospital will provide four Maine Track students with clerkship rotations. “We believe every physician we get coming to this state is a difference-maker,” Churchill insists. And he should know—his hospital has been trying to fill a physician vacancy for more than a year now.
What is it like to practice medicine in rural Maine? In late June, Tufts Medicine set out to answer the question. We visited three Tufts graduates who have served three dis-tinctly different geographic regions of the state—woods, northern coast and potato fi eld—for a collective total of 85 years. We fi gured if these people didn’t know, no one would.
BINGHAM: Nothing Else for Milesthe town of bingham, maine, has seen better days. From its weather-beaten main street, with its handful of boarded-up store-fronts beside the surging Kennebec River, to its lone, mostly vacant motel, this town of fewer than a thousand people looks like it’s been whacked hard and is still reeling from the blow. Lumber trucks hurtle along the main drag, sometimes empty, sometimes full. Ten miles north of here, you are into some serious woods. Bingham residents have few employment options, either work-ing in the woods, or seasonally for one of
the river-rafting companies, or over at the nursing home.
“It’s a town in decline,” says resident Myron Morris, 82, bluntly. “The mill went away, and the logging industry has gone downhill.” Morris moved to town in 1950 and formerly owned a trucking company. Now he’s seated in the lobby of the Bingham Area Health Center, a modern one-story building in the middle of town, waiting for his regular check-up.
Cynthia Robertson, ’80, sweeps into the waiting room. Petite and dynamic, with frosted hair and a quick smile, she is per-
fectly cast for the role of the briskly effi cient, small-town doc. Robertson signed up with the National Health Service Corps, which gives fi nancial incentives for service in rural America, after graduation. In a way she was echoing her father, who had been a small-town physician in upstate New York. “The main thing I saw in him was a contentment in his life,” she says. Robertson did her resi-dency in Augusta and has been Bingham’s chief physician for the past 26 years.
The clinic serves as an all-purpose health
center for the town since there’s nothing else for miles around. A dentist stops by several days a week to examine Bingham’s teeth—and there are ambitious plans to expand the service. Two therapists are available part-time for mental health counseling. During the summer months, there’s even a high school guidance counselor who’s ready to advise kids one day a week in an office down the hall. The clinic has made itself a trusted neighbor. “When you’re a country doc, you’re sort of responsible for the health of that community,” says Robertson, who has served as medical director of the town
nursing home and worked in a nearby hos-pice. She still makes house calls two or three times a month.
Forging a close relationship with patients is a key concern in rural areas, and absolutely essential to cultivating good health, the doc-tors interviewed for this story agree. Your life is transparent. There’s no place to hide. You live or die by what people think of you. Robertson says the Bingham clinic’s central location and its staffi ng with town residents refl ects that focus. “All the people who work
Everything was personal. The handshake, the smile, the nod to a neighbor constituted another brand of cure.

18 t u f ts m e d i c i n e f a l l 2 0 0 9
here are familiar faces,” she points out. “People trust us, and therefore they bring their problems a little sooner, and they don’t get so sick. We keep them out of the ER, out of the hospital, and in that way we’re really cost-effective.”
A general wariness of the wider world underlies much of the need for treatment facilities near at hand, Robertson explains. Many country people aren’t comfortable venturing even short distances beyond their front porches and backyards. “This clinic is close to home for them. People who don’t like to come out of the woods—what do they call it, ‘woods queer’?—and those who would be afraid to drive around a big town like Waterville, an hour away, are willing to come in here and be looked at.”
The medical issues are about what you might expect in a county where the poverty rate runs about 50 percent higher than the state average. Depression and lots of addic-tion (“pills of all kinds”) are rife among Robertson’s patients. And although she has managed to develop a network of peer con-tacts around the state, medical support ser-vices near at hand are virtually nonexistent. So how would she describe the rewards of her demanding practice? At this, Robertson shakes her head side to side as though dazed, but grinning from ear to ear. “Beyond words,” she says.
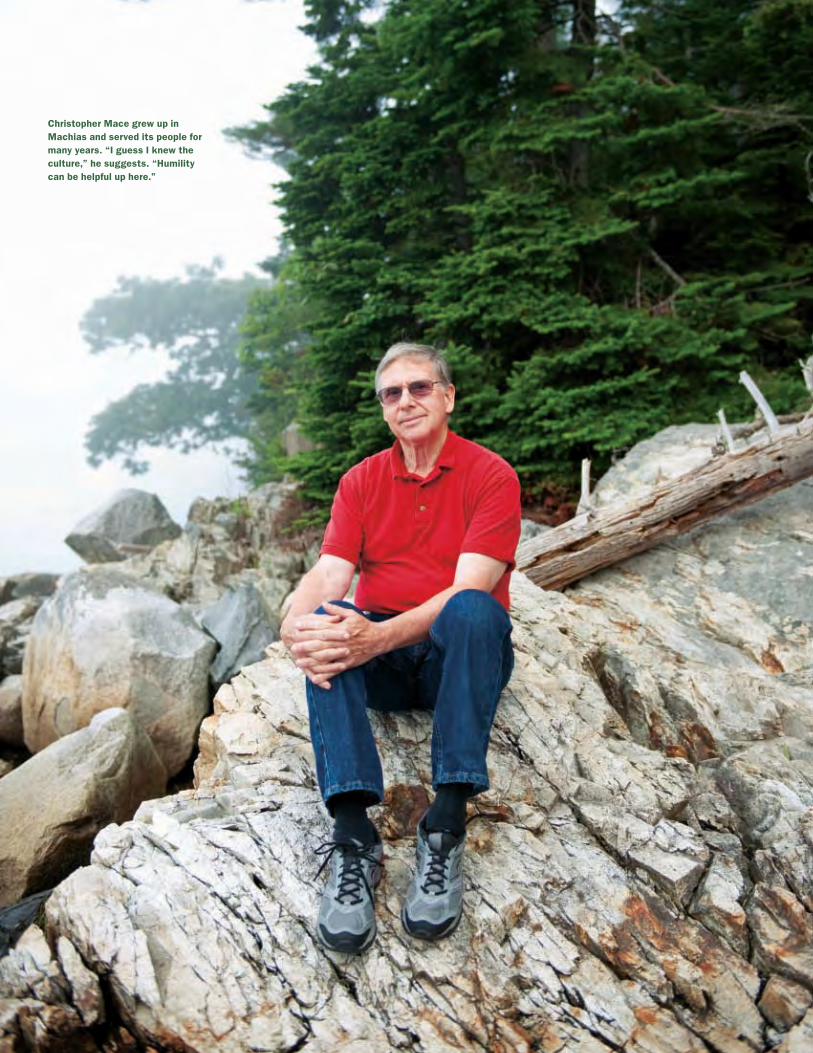
MACHIAS: Laughter in the Houseif you drive up the maine coast about 50 or 60 miles farther than tourists usually do, into Washington County, the people start to be outnumbered by lobster boats. The land is windswept and rocky, and the towns are scattered and few. Nobody makes much money; this is about as close to the bone as life in Maine gets. With slightly more than 1,000 residents, Machias is something like the capital of this north-ern stretch of coast. Christopher Mace, ’68, grew up in this community, where his dad ran a lumber mill.
After graduation from medical school, residency in Washington, D.C., and the beginning of military service in Vietnam, Mace was recruited back home by U.S. Sen.
Margaret Chase Smith to provide desper-ately needed medical care to the region. He ended up being one of the rare doctors in the vicinity, fi rst working for three years at a clinic in Gouldsboro and then carrying on his practice back in Machias for a longer stretch. Mace retired in 2005. When things were good in the practice, he says, they were very good, and when they were bad, “they could be exhausting.”
In Gouldsboro in the early days, “the demand was non-stop,” he recounts. “People would come to the house. Then I’d have to walk into my closet since I’d see them com-ing into the driveway and knew they would look in the windows.”
From a business perspective, being a doc-tor was simplicity itself. Seated on a couch in his comfortable retirement home an hour’s drive south of Machias, now white-haired, wearing a sweater and looking altogether relaxed, Mace laughs at the memory. “You didn’t have to document everything” for reimbursement, he comments in his light, soft voice that bears a salty trace of Maine. “It was much easier in that respect.” Mace took his own X-rays and read them, handled basic lab work, even provided veterinary care as needed. “I remember I treated a rab-bit with an abscess one time and also a dog with porcupine quills,” he muses.
Once back home in Machias, where he was one of a few doctors in solo practice, Mace found that everything was personal. The handshake, the smile, the nod to a neighbor was another brand of cure. The sense of responsibility also felt intensely personal. “As a doctor, you’re part of a com-munity where you have a certain standing,”
he says. “The major rewards of that involved dealing with patients who were grateful.” Every holiday season, townspeople would show up at the doctor’s door bearing home-made cakes and cookies in tribute to his devotion.
Often the doctor’s healing came down to an old-fashioned laying-on of hands or the deft application of a soothing voice. Mace had a home office in those days. His wife, Suzanne, recalls how she would often see a patient trudging into the house with some unknown complaint or other. “And then I’d hear this laughter,” she marvels. “The patient would come out saying, ‘I don’t know what he does, but I feel so much better.’ ”
It wasn’t all sunshine. In small communi-ties like Machias, turf battles often erupted between doctors fi ghting to preserve their practices. Asked if, even with these underly-ing tensions, he might have enjoyed a certain advantage from being a local boy, Mace read-ily concedes the point. “I would say so,” he says, chuckling. “I guess I knew the culture. In later years, some doctors would come in and be a little arrogant. Well, humility can be helpful up here. I knew I was in fact accepted when one man I had treated told me, ‘Next to God and Dr. Larson, your name is pretty good over in Jonesboro.’ ”
He wore his stethoscope for 30 years. Realizing that he would otherwise be swamped by the ever-increasing paperwork that went with medicine, Mace signed on with a hospital in town for the fi nal lap of his career. But he continued to make house calls right up until the end. “I was never able to let go of trying to take care of patients the best I could,” he says quietly.
CREDIT_SMALL_FL f a l l 2 0 0 9 t u f ts m e d i c i n e 19
Christopher Mace grew up in Machias and served its people for many years. “I guess I knew the culture,” he suggests. “Humility can be helpful up here.”

20 t u f ts m e d i c i n e f a l l 2 0 0 9
HOULTON: A Residue of Wind and Coldangling north of bangor on i-95, the land peels back and f lattens its line, grow-ing stupendous in sca le. Welcome to Aroostook County, the largest county east of the Mississippi River—it’s about the size of Connecticut and Rhode Island combined—and one of the emptiest, with only 11 folks per square mile. This is a part of Maine where a town of 5,000 people manages to be the biggest deal around.
Ted Sussman, ’77, has been a doctor in Houlton since 1980. He and his wife have raised three sons here, and although he doesn’t hunt or fish, he has a boat on a nearby lake and savors the life available to him. “Rural practice is the best medicine there is,” he says. “Unfortunately, we phy-sicians are a dying breed and can’t replace
ourselves.” Sussman loves his mostly elderly patients, many of whom he has known for many years, and if a morning’s sample is any indication, they love him right back.
Sussman’s office is at Houlton Regional Hospital, a modern 50-bed facility that resembles the anchor store in a suburban shopping mall and draws patients from a 45-mile radius. The doctor’s pace as he moves through the halls is not the easy country stroll you might expect. Instead, he strides between the rooms where the patients wait, swinging through each doorway in turn and, once inside, slowing the speed of his delivery to consult with them. Sussman grew up near New York City and you can see it in the hall.
Ed, the first patient, is 75 years old and drives a truck for work. He is wearing jeans and heavy boots. Ed has been coming to Sussman for 20 years now and reports, with typical Maine understatement, “He’s a pretty
good doctor, I think.” Ed has been taking medicine for a heart condition. Sussman tells him that his pulse rate is still too high and that he’d like to adjust his medication to slow it down a bit. “That’s what I’m scared of,” Ed replies, studying the doctor’s face. Sussman gives a careful explanation of the move. “Don’t give me too many big words—give me truck-driving words,” Ed jokes, but it’s clear he is reassured by what he’s hearing.
Minutes later, back in the doctor’s offi ce, the question arises of how an outsider goes about f itting into rural Maine culture. With his blue work shirt and khakis and his thin dark hair trailing back over the collar, Sussman has a semi-raffish, ex-hippie air. He admits that his politics are far to the left. How does a guy like this make it in a place like Houlton? Concerning his appearance, Sussman reports that his hair was a foot lon-ger a year ago. No big deal.

f a l l 2 0 0 9 t u f ts m e d i c i n e 21
People in rural Maine are surprisingly tolerant, the graduates interviewed for this story agree. All kinds of differences are fi ne by them. The one thing you cannot be is a deadbeat. If you stay, you must pitch in and contribute to the life of the community.
This Sussman has done. He carries a full patient load here at the hospital, seeing 20 or 25 patients a day, and is perpetually on call. Lynn York, proprietor of York’s Bookstore in the compact business district of Houlton, knows Sussman well as the man who tended his father through multiple surgeries during the fi nal stage of his life (“He kept my father alive for 20 years,” he says feelingly) and as someone available to his patients around the clock. “I’ve been with him at movies over there many times,” York relates, pointing directly across the street to the movie theater
marquee, “and his beeper would always go off. I doubt he ever saw a whole movie.”
Roy, today’s second patient, is neatly dressed in a cream-colored checked shirt and dark slacks. His combed hair is pure white. Roy tells the doctor, seated in front of him, that he has been feeling cramps in his right leg whenever he walks any distance. “Gettin’ so you can’t be 80 years old with-out going to hell just like that,” he exclaims, looking around the room with a giant smile.
Patients in Houlton are a good-hearted and cheerful bunch. No matter what hits them, it seems, they’ve seen worse.
Over the course of seven or eight patients, not one com-plains or plays the victim—a world apart from the under-current of self-pity that can pervade urban settings. Where does the serenity come from? It just might be one residue of the leveling wind and cold of north-ern Maine. “Nature’s taking its course,” an elderly woman in a wheelchair tells Sussman
matter-of-factly when he inquires how she is doing. It will be a while until you hear any-one say that in a doctor’s offi ce in Boston.
Before he leaves, Roy mentions the hunt-ing camp he owns 15 miles back in the woods. “My friend Billy and I made that road,” he says, his face brightening at the memory. Sussman listens appreciatively without saying a word. Then he concludes the visit by saying: “A little Tylenol, some heat, and you’ll be all right. Anything comes up, give a holler.”
Sussman worries about the prospects for patients like Roy in the days to come. There was a surge of young doctors into rural areas after the National Health Service Corps came along in 1970, a time coincident with the fi rst sizable crop of women to enter the medical profession. “Most docs came up here in the 1970s. There’s a generation about to retire,” he points out. “Our ability to replace them is, right now, zero.”
Don’t get Sussman started on what he believes are the soft, lifestyle-centered pri-orities of current medical school enrollees. It’s a fact that far fewer students are choos-ing primary-care specialties, compared to when he came through the system. “Folks now, they want to take no calls, have limited hours and make a lot of money,” he alleges. Does Sussman really believe that today’s stu-dents are completely spoiled? “Worse than spoiled,” he answers scornfully, his eyes fl ashing. “I think we have lost what it means to be a physician.”
That’s a sobering charge. If Sussman is correct, the challenge facing the graduates of the Maine Track is twofold—fi rst to buck stubborn historic trends by setting up shop in isolated places like Bingham, Machias and Houlton, and then to summon from some-where deep inside the essence of doctoring. With its rugged landscape, its poverty and its charm, rural Maine awaits the resolution. TM
Bruce Morgan is editor of this magazine.
“ Rural practice is the best medicine there is. Unfortunately, we physicians are a dying breed and can’t replace ourselves.”
—Ted Sussm a n
Facing page: Ted Sussman takes the long view from a potato fi eld near Houlton. Top: The doctor consults with a patient at Houlton Regional Hospital. Left, a glimpse of downtown.
22 t u f ts m e d i c i n e f a l l 2 0 0 9
M Y UNFORGETTABLE P AT I E N T
f a l l 2 0 0 9 t u f ts m e d i c i n e 23ILLUSTRATION: DAVID POHL
This Crazy LoveShe’s a doctor. She’s a fi rst-time mom. And when she enters the ER clutchingher injured child, all bets are off by Rachel Salguero Kowalsky, M.D./M.P.H. ’03
a few months ago, my eight-month-old daughter losther balance, teetered and fell face fi rst onto the livingroom carpet. She bit her lip. It bled.
Have you noticed already—the carpet, the fall fromher own height? These are cues that she was fi ne. If a med-ical student or resident had presented the same story tome in the children’s ER where I am a fellow, I would havesmiled and asked: “First-time mom?”
In pediatric emergency medicine, first-time momsachieve a certain level of notoriety for coming to the ERover benign issues: colic, constipation, spit-up. Whetherthis notoriety is deserved can be debated. But what is cer-tain is that being a fi rst-time mom myself, the fi rst thingI did was scoop the child into my arms and race to thenearest emergency room.
Was my reaction so crazy? The holy grail of pediatrics—and of motherhood—is a healthy baby. In fact, my vigilantprotection of our daughter began the day I learned I waspregnant. I took folate, renounced martinis and avoidedmercury-laden fish. If somebody on the sidewalk wassmoking a cigarette, I crossed the street. When my babywas born perfect and whole, I breathed a sigh of relief.
But now she was bleeding. Injured! I could hardly keepmyself from pushing past all the ER patients, through tri-age and into a sick bay.
A resident came out to the waiting room to take a lookat her. “Did you wash your hands?” I asked her. “It’s RSVseason.” [RSV is a common respiratory virus in smallchildren.]
She blinked at me. “Are you a doctor?”I was quickly brought back into the ER—not into a
sick bay, but into a non-acute bed. Since my daughterwas playful, eating the white paper off the stretcher andtrying to crawl around on the fl oor, I decided this wasprobably OK. Actually, I began to feel embarrassed thatwe had come to the ER at all. Was I one of those notori-ous fi rst-time moms?
A fellow exactly the same year as me examined mydaughter. Actually, we know each other well. Pediatricemergency medicine is a small world, especially inNew York City, where all fi ve fellowship programs are
crammed onto an island 13 miles long. “Wow,” she said.“You had your baby!” I felt my embarrassment turn torelief as she explored the tiny mouth, my daughter’s twolittle bottom teeth. She felt her clavicles, her belly. Mydaughter giggled.
Next the attending came to see us. “I have two kids,”she said. “I know exactly how you feel.”
Infi nitely relieved, I took my daughter home.A few hours later, on my overnight shift, the first
patient I saw had also fallen down. She had a big hema-toma on her forehead, but otherwise, she was completelyfi ne. In fact, most of the patients that night were fi ne.They had coughs and colds, minor bang-ups and stom-ach bugs. Their parents were all nervous, tired, upset. “Iknow exactly how you feel,” I said, more times than I’dever said it before. I had found those words to be power-ful, practically medicinal.
In an early photograph, I am standing next to my hus-band, holding our baby. She is jumping out of the pic-ture. She is reaching for something, her eyes enormous,her face full of hilarity and zeal. All the possibilities ofher life, all of her potential, are there on the page. Theyare dazzling. In the same photograph, my husband andI look happy but preoccupied. We are probably worriedthat she is hungry, wet or not dressed warmly enough.I can only imagine what shape these worries will takeas she starts to run around, ride bikes, cross streets andeven, eventually, leave home.
I’ll never second-guess a fi rst-time mom again, nomatter what brings her to me in the middle of the night.Parenthood is an awesome state of wonder and fear.Anyone who says otherwise has never watched theirtoddler lose her balance, and, following her tumblingtrajectory in slow motion, prayed that she’d land on hertwo tiny feet. TM
The author is a fellow in pediatric emergency medicineat Bellevue Hospital Center/NYU School of Medicine inNew York City. One of her essays, “The Care of Strangers,”was included in The Real Life of a Pediatrician (Kaplan),published this past spring.
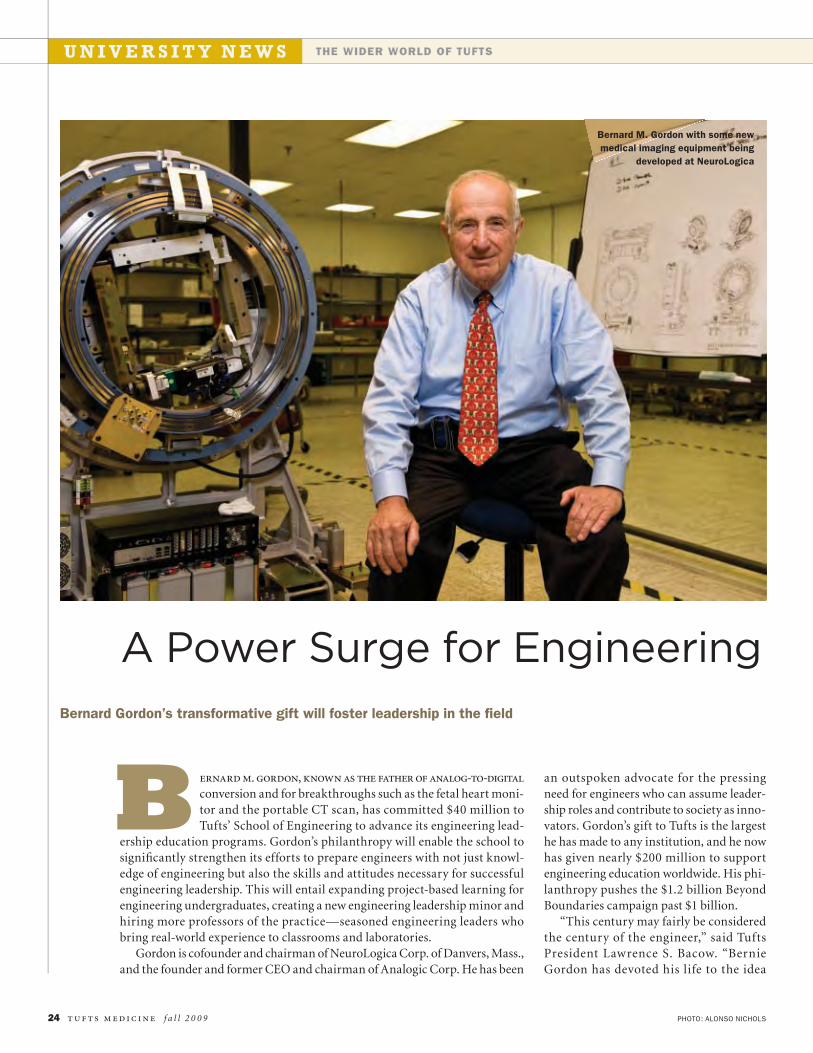
PHOTO: ALONSO NICHOLS
U N I V E R S I T Y N E W S THE WIDER WORLD OF TUFTS
24 t u f ts m e d i c i n e f a l l 2 0 0 9
ernard m. gordon, known as the father of analog-to-digital
conversion and for breakthroughs such as the fetal heart moni-tor and the portable CT scan, has committed $40 million toTufts’ School of Engineering to advance its engineering lead-
ership education programs. Gordon’s philanthropy will enable the school tosignifi cantly strengthen its efforts to prepare engineers with not just knowl-edge of engineering but also the skills and attitudes necessary for successfulengineering leadership. This will entail expanding project-based learning forengineering undergraduates, creating a new engineering leadership minor andhiring more professors of the practice—seasoned engineering leaders whobring real-world experience to classrooms and laboratories.
Gordon is cofounder and chairman of NeuroLogica Corp. of Danvers, Mass.,and the founder and former CEO and chairman of Analogic Corp. He has been
an outspoken advocate for the pressingneed for engineers who can assume leader-ship roles and contribute to society as inno-vators. Gordon’s gift to Tufts is the largesthe has made to any institution, and he nowhas given nearly $200 million to supportengineering education worldwide. His phi-lanthropy pushes the $1.2 billion BeyondBoundaries campaign past $1 billion.
“This century may fairly be consideredthe century of the engineer,” said TuftsPresident Lawrence S. Bacow. “BernieGordon has devoted his life to the idea
Bernard Gordon’s transformative gift will foster leadership in the fi eld
A Power Surge for Engineering
B
Bernard M. Gordon with some newmedical imaging equipment being
developed at NeuroLogica

f a l l 2 0 0 9 t u f ts m e d i c i n e 25
that engineers should make the world abetter place through their leadership. Heknows how to get things done, and weare delighted that he appreciated kindredspirits at Tufts.”
“Tufts is committed to educating lead-ers to serve the common good,” saidProvost and Senior Vice President JamshedBharucha. “Engineering leaders must beable to inspire teams of people to envisionand realize technological goals in complexand fast-paced environments. Theymust understand not just the sci-ence but also the people they leadand the people for whom theirtechnology is intended.”
Linda Abriola, dean of theSchool of Engineering since 2003,pointed out, “Many of the chal-lenges we face as a nation and a society aretechnical in nature, extraordinarily com-plex and intertwined with global fi nancialand political concerns. Engineers can-not cede leadership to those who may beill-equipped to understand the technicalaspects of our global, information- andenergy-driven society. Tufts’ School ofEngineering seeks to become the school ofchoice for aspiring technological leaders.”
Gordon has been a strong supporter ofengineering education that goes beyondtraditional technological preparation, amandate supported by a recent CarnegieFoundation report on the future of engi-neering education. “Engineers invent andbring to market new technologies thatenable advances in health care, manu-facturing, infrastructure, transportation,communications, energy production—the full range of human activity,” saidGordon. “Great engineers succeed becausethey are true leaders who combine tech-nical skill with the capacity to lead andmotivate others.”
The new engineering leadership ini-tiatives will benefi t from a close relation-ship with Tufts’ Gordon Institute, whichGordon founded in 1984 to further gradu-ate education for practicing engineers andmoved to Tufts in 1992. The institute’s M.S.in engineering management is a nationallyrecognized program designed to providepracticing engineers and applied scientistswith the knowledge and skills they need to
be leaders in technology-driven companies.The current class represents more than 30different firms from all industry sectors.In a 2008 survey, 45 percent of GordonInstitute alumni reported that they hadbeen promoted by their companies whilethey were still enrolled in the program, and95 percent had been promoted within twoyears of graduation.
Prior to his most recent gift, Gordonhad donated $35 million to Tufts for a
variety of purposes, including the GordonInstitute, the construction of SophiaGordon Hall and support for the School ofEngineering.
In addition, he established the BernardM. Gordon Pr ize for Innovat ion inEngineering and Technology Education atthe National Academy of Engineering—anaward that the academy bestowed on theGordon Institute in 2007. His philan-thropy has also made possible initiativesat numerous other institutions, includingMIT, the Museum of Science in Boston,Northeastern Universit y, WorcesterPolytechnic Institute and the Universityof California at San Diego.
CHANCE ENCOUNTERBernard Gordon has had an indelibleimpact on Tufts. But had it not been fora chance encounter between an aspiringnaval offi cer and the university president65 years ago, the close ties between Gordonand Tufts might not have developed.
Gordon grew up during the Depressionin western Massachusetts. As a boy, he likedto fi x radios and transmitters. He earnedhis fi rst dollar at age 13, building and sell-ing outhouses featuring a cord that, whenpulled, released lime and helped leach wasteinto the ground.
In his teens, Gordon entered the Navy’soffi cer training program. The Navy fi rstsent him to MIT, but Tufts was also oneof the schools selected to support the V-12
Navy College Training program, and in1944, the 17-year-old Gordon lived on theTufts campus. One evening, as he walkedacross campus in his uniform, a ta l lgentleman approached. It was PresidentLeonard Carmichael. Carmichael greetedhim: “And how are you, Bernard?”
“I didn’t know him, and to this day Iwonder how he knew me,” says Gordon.“But it seemed that Tufts was a friendlyplace with a personal atmosphere.”
Gordon spent more than half a year atTufts, studying engineering and psychol-ogy along with naval navigation and strat-egy. As a naval officer, Gordon was laterassigned to destroyer escorts. Remaining aReady Reserve offi cer, he returned to MITon the G.I. Bill, graduating with a bach-elor’s (1948) and a master’s in electricalengineering (1949).
Gordon’s core technology of high-speed analog-to-digital conversion isnow found in everything from comput-ers, compact disc players and televisionsto EKG machines, digital thermometers,atomic clocks and imaging equipment.His companies have developed manybreakthroughs, including the first fetalmonitor, the fi rst lightweight mobile CTscanner, the fi rst instant-imaging CT sys-tem and an advanced security imagingsystem to help detect explosives and othercontraband. At NeuroLogica, Gordon isdeveloping a portable imaging system tohelp stroke and trauma victims.
In 1986, Gordon was honored byPresident Ronald Reagan with the secondNational Medal of Technology. Electeda member of the National Academy ofEngineering in 1991, he has also beenawa rded severa l honora r y deg rees ,including one from Tufts in 1992. He isa Tufts trustee emeritus, a member of theEngineering Board of Overseers and hon-orary cochair of the Beyond Boundariescampaign.
“ Great engineers succeed because they. . . combine technical skill with the capacity to lead and motivate others.” — B e r n a r d G o r d o n
PROVIDING THE MEANS FOR EXCELLENCEB E Y O N D B O U N D A R I E S
PHOTO: JOHN SOARES26 t u f ts m e d i c i n e f a l l 2 0 0 9
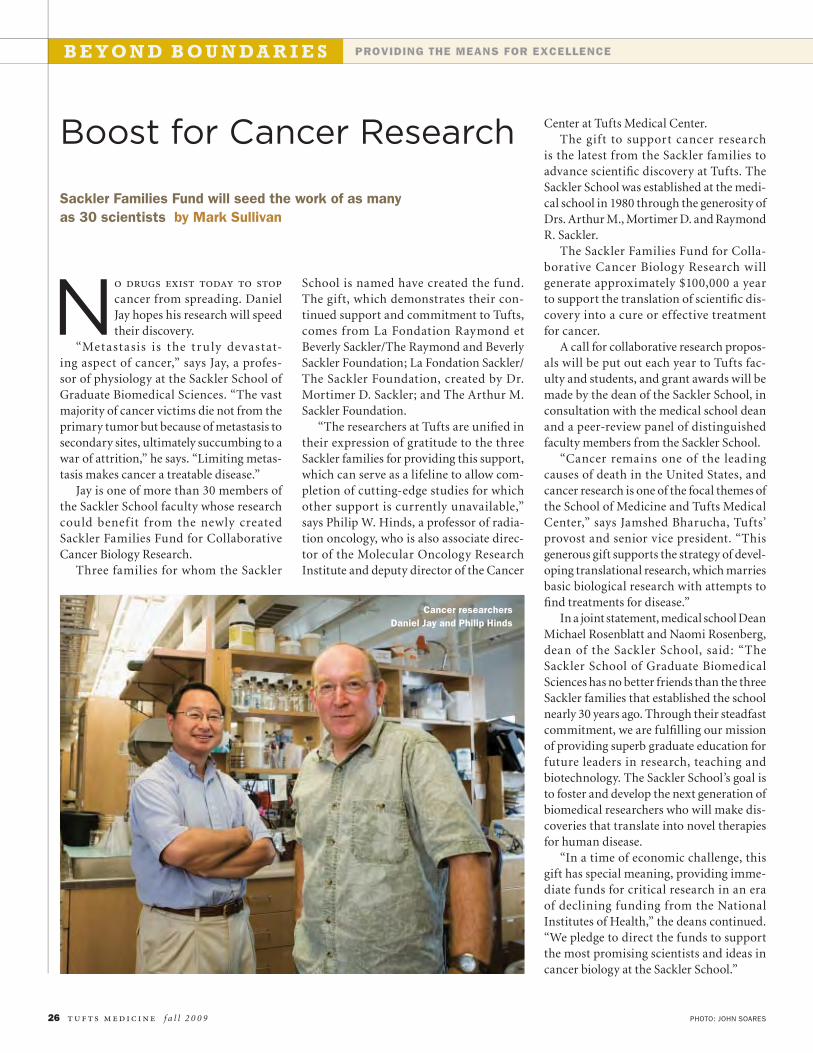
No drugs exist today to stop
cancer from spreading. DanielJay hopes his research will speedtheir discovery.
“Metastasis is the tru ly devastat-ing aspect of cancer,” says Jay, a profes-sor of physiology at the Sackler School ofGraduate Biomedical Sciences. “The vastmajority of cancer victims die not from theprimary tumor but because of metastasis tosecondary sites, ultimately succumbing to awar of attrition,” he says. “Limiting metas-tasis makes cancer a treatable disease.”
Jay is one of more than 30 members ofthe Sackler School faculty whose researchcould benef it from the newly createdSackler Families Fund for CollaborativeCancer Biology Research.
Three families for whom the Sackler
School is named have created the fund.The gift, which demonstrates their con-tinued support and commitment to Tufts,comes from La Fondation Raymond etBeverly Sackler/The Raymond and BeverlySackler Foundation; La Fondation Sackler/The Sackler Foundation, created by Dr.Mortimer D. Sackler; and The Arthur M.Sackler Foundation.
“The researchers at Tufts are unifi ed intheir expression of gratitude to the threeSackler families for providing this support,which can serve as a lifeline to allow com-pletion of cutting-edge studies for whichother support is currently unavailable,”says Philip W. Hinds, a professor of radia-tion oncology, who is also associate direc-tor of the Molecular Oncology ResearchInstitute and deputy director of the Cancer
Boost for Cancer Research
Cancer researchersDaniel Jay and Philip Hinds
Sackler Families Fund will seed the work of as manyas 30 scientists by Mark Sullivan
Center at Tufts Medical Center.The gift to support cancer research
is the latest from the Sackler families toadvance scientifi c discovery at Tufts. TheSackler School was established at the medi-cal school in 1980 through the generosity ofDrs. Arthur M., Mortimer D. and RaymondR. Sackler.
The Sackler Families Fund for Colla-borative Cancer Biology Research willgenerate approximately $100,000 a yearto support the translation of scientifi c dis-covery into a cure or effective treatmentfor cancer.
A call for collaborative research propos-als will be put out each year to Tufts fac-ulty and students, and grant awards will bemade by the dean of the Sackler School, inconsultation with the medical school deanand a peer-review panel of distinguishedfaculty members from the Sackler School.
“Cancer remains one of the leadingcauses of death in the United States, andcancer research is one of the focal themes ofthe School of Medicine and Tufts MedicalCenter,” says Jamshed Bharucha, Tufts’provost and senior vice president. “Thisgenerous gift supports the strategy of devel-oping translational research, which marriesbasic biological research with attempts tofi nd treatments for disease.”
In a joint statement, medical school DeanMichael Rosenblatt and Naomi Rosenberg,dean of the Sackler School, said: “TheSackler School of Graduate BiomedicalSciences has no better friends than the threeSackler families that established the schoolnearly 30 years ago. Through their steadfastcommitment, we are fulfi lling our missionof providing superb graduate education forfuture leaders in research, teaching andbiotechnology. The Sackler School’s goal isto foster and develop the next generation ofbiomedical researchers who will make dis-coveries that translate into novel therapiesfor human disease.
“In a time of economic challenge, thisgift has special meaning, providing imme-diate funds for critical research in an eraof declining funding from the NationalInstitutes of Health,” the deans continued.“We pledge to direct the funds to supportthe most promising scientists and ideas incancer biology at the Sackler School.”

f a l l 2 0 0 9 t u f ts m e d i c i n e 27
FUNDAMENTAL CONCEPTSJay’s research seeks to identify new pro-teins on cancer cells that play a role incancer invasion and mestastasis. “We areemploying a unique technology, usinglight to destroy specifi c proteins expressedon cancer cells, to see if this affects thecells’ ability to invade,” he says. “Usingthis approach, we’ve identifi ed three newproteins and are beginning to test them fortheir role in breast cancer metastasis andthe spread of brain tumors.”
Hinds’ work may also benefi t from thefunding. He is investigating “the funda-mental mechanisms that allow cancer cellsto escape the signals that normally act tostop cells from dividing and tissues fromgrowing.” The explicit goal of his ongoingresearch is to identify proteins involved inthe proliferation of cancer stem cells sothat methods can be developed to inter-rupt their function.
“We are particularly excited at the pros-pect of fi nally understanding the identityand source of the cells that produce tumorsand that persist after conventional chemo-therapy,” Hinds says. The potential appli-cations of his work are vast.
“The fundamental concepts we arestudying and the hypotheses generatedalso apply to a variety of other diseasesof excess or impaired tissue formation,and so they have implications for diseasesbeyond cancer,” he continues. “We nowhave increased confi dence that our workwill have practical as well as fundamentalimpact in the near future.”
Hinds notes that “Tuf ts has beenan outstanding place to perform thisresearch, in part due to the physicalresources that are readily available, butmore so because of the highly collabora-tive atmosphere. Tufts people at all lev-els are uniformly and genuinely excitedabout working together to solve prob-lems ranging from an understandingof the molecular basis of disease to theproduction of preclinical and clinicalmodels useful for identifying and testingtherapeutics.”
Mark Sullivan, an editor in AdvancementCommunications, can be reached at [email protected].
DANIEL KAPLAN, ’56, SAYS HE OWES HIS SUCCESSFUL CAREER AS A RADIOLOGIST TO
his late parents, who escaped czarist oppression as young teenagers andimmigrated to America on their own. His father worked as a house painter inChelsea, Mass., to support their family through the Depression.
After Dan Kaplan worked his way through Harvard College, he presentedhis diploma to his mother. When he fi nished Tufts University School ofMedicine, he gave his diploma to his father. “They earned them,” says Kaplan.“I owe them an enormous debt of gratitude.”
Now Kaplan again will pay tribute to his parents—Joseph and SylviaKaplan—this time with a gift to name a classroom in the newly renovatedSackler Center at the medical school in their memory. If his parents were hereto see it, Kaplan says, they would be “honored beyond belief.”
“This is a marvelous place to direct a gift because it will benefi t genera-tions of students on a daily basis, enhancing their educational experience,”he says. With his $100,000 gift, Kaplan says he also wanted to express hisappreciation. The medical school, he explains, enabled him to experience aradiology career in both academic and public spheres that has been “gratify-ing and satisfying on so many levels.”
Kaplan’s gift has been doubled under a challenge by the Jaharis FamilyFoundation.
ALUM DEDICATES SACKLER CLASSROOM TO HIS PARENTS
Alumni, faculty, students and staff are invited to celebrate the offi cialopening of the refurbished Sackler Center on Thursday, October 22, from5 to 8 p.m. For more information, contact Kara Brassil at [email protected] or register online at http://medical.alumni.tufts.edu.
PHOTO: ALONSO NICHOLS
Students confer in a Sackler studyarea between classes.
28 t u f ts m e d i c i n e f a l l 2 0 0 9
on campusMEDICAL SCHOOL NEWS
How do we ensure that academic medicine isn’t tainted by ties to thepharmaceutical industry? by Jacqueline Mitchell
Uneasy Alliance
o most bostonians, the idea would be patently absurd. what if the
umpires calling a Red Sox-Yankees game were on the Steinbrenners’payroll?
“It’s a pretty basic principle—we all recognize that people in aposition of judgment shouldn’t have ties to the parties they judge,” said AdamC. Urato, assistant professor of obstetrics and gynecology at the School ofMedicine. He was the keynote speaker at a Tufts symposium in May on con-fl ict of interest in academic medicine; he urged his colleagues to guard againstthe damage confl icts of interest—and even perceived confl icts of interest—canwreak on the medical profession.
Urato first became concerned with conf licts of interest in medicine in
T
2005. Attending grand rounds at TuftsMedical Center, he heard a speaker fromGlaxoSmithKline advocate universal pre-natal herpes screening. Urato knew thatscreening the four million U.S. womenwho are pregnant every year for the herpesvirus would result in about a million pre-scriptions for the drug company’s antivi-ral medication Valtrex. He also knew thatwhile there is no proven benefi t of univer-sal prenatal screening, there is evidence thepractice causes some harm by increasingthe likelihood of Caesarian deliveries.
“No expert panel recommends herpestesting during pregnancy, but we have thisoddball scenario where physicians in theUnited States are more likely to learn thewrong protocol because these continu-ing education activities are sponsored by[pharmaceutical companies],” Urato said.
Now Urato is worried about drug

f a l l 2 0 0 9 t u f ts m e d i c i n e 29ILLUSTRATION: EMILIANO PONZI
companies’ inf luence on the debate sur-rounding antidepressant use during preg-nancy. “This is a huge unknown; we’re basi-cally doing an experiment on the humanpopulation by exposing embryos andfetuses to [antidepressants],” Urato said.
In 2006, the Journal of the AmericanMedical Association published research thatfound that women who discontinue antide-pressant medications during pregnancy havea high risk of relapsing into depression.
But, noted Urato, the article failed toaddress the well-known problem of with-drawal from antidepressants. Nor did itmention pregnancy outcomes of womenwho took medications during gestation.The authors also didn’t disclose their closeties to the pharmaceutical companies thatmake antidepressant drugs, claiming theirstudy did not advocate any particular classor brand of antidepressant, and thereforewas confl ict-free.
“Who buys that argument? Not theeditor of the New York Times, who calledit ‘preposterous,’ ” Urato said, citing evi-dence that the public is wary of physicians’“cozy” ties with industry. While 94 percentof physicians have relationships with drugand device makers, 85 percent of the publicfi nds these arrangements unacceptable.
Doctors ignore the public’s skepticismat their peril, Urato said. “Medicine is los-ing the public’s trust for the same reason wedon’t trust Ronald McDonald when he tellsus where to buy a hamburger,” he said. “Wesimply can’t be both paid spokesmen andunbiased authorities.”
FULL DISCLOSURE“Medical research enjoys a huge percentageof the federal budget for research,” addedTufts Vice Provost Peggy Newell, a panelist atthe ethics symposium, which was sponsoredby the University-wide Committee on Ethics.“Once the public loses faith in research donein hospitals and universities, they will notbe so eager to support it, so it’s critical thatall of us worry about conflicts of interest,”said Newell, whose office manages Tufts
researchers’ collaborations with industry, aswell as patenting and research compliance.Newell tells researchers that before they signany agreements, imagine the disclosure oftheir fi nancial ties splashed across the frontpage of the New York Times.
Such disclosure of fi nancial ties is “nec-essary but not sufficient to solve the prob-lem of confl ict of interest,” argued panelist
Jerome P. Kassirer, Distinguished Professorof Medicine at Tufts. Kassirer, who wrote thebook On the Take: How Medicine’s Complicitywith Big Business Can Endanger Your Health(Oxford University Press, 2004) is a well-known critic of confl icts of interest in medi-cal research. “The individual listening to anexpert or reading a study does not know howto interpret [disclosures]. The answer to con-fl ict of interest is to get rid of it.”
But Michael Rosenblatt, dean of themedical school and a professor of physi-ology and medicine, cautioned against“applying a blunt instrument to somethingthat should be done more thoughtfully andsurgically.”
Rosenblatt’s own collaborations withindustry resulted in the development ofFosamax, the first medication shown toreduce fractures in patients with osteoporosis.“I’m very proud of what I did with Fosamax.I feel like I’ve saved lives,” Rosenblatt said,citing research that 20 percent of elders whosuffer hip fractures die within two years.Rosenblatt added that many antibiotics,vaccines, gene therapies and drugs that curecancers and manage AIDS “would not havebeen developed without the very real inter-face between academia and industry.”
“I think there’s a risk that rigid stan-dards can damage important elementsof the research mission,” concurred Paul
Summergrad, professor and chair of thedepartment of psychiatry at the medicalschool. Summergrad argued that people actnot just in their own interests, but also outof certain professional and personal obliga-tions. Noting that such confl icts are “ubiq-uitous in human life,” Summergrad won-dered if limiting physicians’ earning powermight discourage the best and brightest
students from entering the fi eld.However, panel moderator Sheldon
Krimsky, a professor of urban and environ-mental policy and planning in the Schoolof Arts and Sciences, considers conf lictsof interest a threat to the academy itself.“Universities are the rare place in our culturewhere people don’t have to get permission towrite or publish, and this privilege should beprotected at any cost. It’s important to pro-tect the knowledge process,” he said.
Calling himself “not anti-industry, butpro-patient,” Urato cast no blame on thepharmaceutical companies. It’s their obli-gation to their shareholders to market andadvertise their products, he said. Uratowants the medical profession not to writemore rules and regulations, but to “changethe culture” by gaining consensus on theissues and providing financial incentivesand rewards for conf lict-free expertisethroughout the health-care system.
“Umpires do get paid, paid to be impar-tial,” Rosenblatt agreed, proposing a Foodand Drug Administration kitty to pay forunbiased, confl ict-free consultants. “Thereare lots of solutions that would allow indus-try and academia to continue interacting.”
Jacqueline Mitchell, a senior health scienceswriter in Tufts’ Offi ce of Publications, canbe reached at [email protected].
“ Medicine is losing the public’s trust for thesame reason we don’t trust Ronald McDonaldwhen he tells us where to buy a hamburger.”
—A da m C . Ur ato
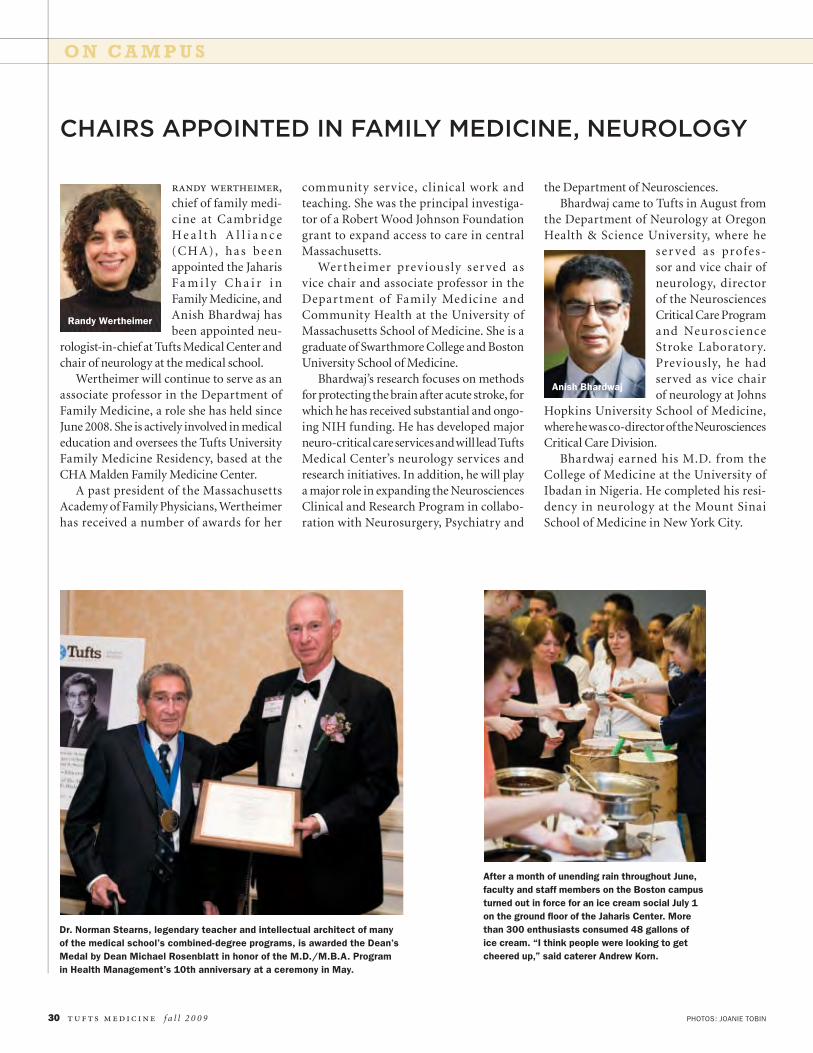
O N C A M P U S
PHOTOS: JOANIE TOBIN30 t u f ts m e d i c i n e f a l l 2 0 0 9
randy wertheimer,
chief of family medi-cine at CambridgeH e a l t h A l l i a n c e(CH A), ha s beenappointed the JaharisFa m i l y C h a i r i nFamily Medicine, andAnish Bhardwaj hasbeen appointed neu-
rologist-in-chief at Tufts Medical Center andchair of neurology at the medical school.
Wertheimer will continue to serve as anassociate professor in the Department ofFamily Medicine, a role she has held sinceJune 2008. She is actively involved in medicaleducation and oversees the Tufts UniversityFamily Medicine Residency, based at theCHA Malden Family Medicine Center.
A past president of the MassachusettsAcademy of Family Physicians, Wertheimerhas received a number of awards for her
community service, clinical work andteaching. She was the principal investiga-tor of a Robert Wood Johnson Foundationgrant to expand access to care in centralMassachusetts.
Wertheimer prev iously ser ved asvice chair and associate professor in theDepartment of Family Medicine andCommunity Health at the University ofMassachusetts School of Medicine. She is agraduate of Swarthmore College and BostonUniversity School of Medicine.
Bhardwaj’s research focuses on methodsfor protecting the brain after acute stroke, forwhich he has received substantial and ongo-ing NIH funding. He has developed majorneuro-critical care services and will lead TuftsMedical Center’s neurology services andresearch initiatives. In addition, he will playa major role in expanding the NeurosciencesClinical and Research Program in collabo-ration with Neurosurgery, Psychiatry and
the Department of Neurosciences.Bhardwaj came to Tufts in August from
the Department of Neurology at OregonHealth & Science University, where he
ser ved a s profes-sor and vice chair ofneurology, directorof the NeurosciencesCritical Care Programand NeuroscienceStroke Laboratory.Previously, he hadserved as vice chairof neurology at Johns
Hopkins University School of Medicine,where he was co-director of the NeurosciencesCritical Care Division.
Bhardwaj earned his M.D. from theCollege of Medicine at the University ofIbadan in Nigeria. He completed his resi-dency in neurology at the Mount SinaiSchool of Medicine in New York City.
CHAIRS APPOINTED IN FAMILY MEDICINE, NEUROLOGY
Randy Wertheimer
Dr. Norman Stearns, legendary teacher and intellectual architect of manyof the medical school’s combined-degree programs, is awarded the Dean’sMedal by Dean Michael Rosenblatt in honor of the M.D./M.B.A. Programin Health Management’s 10th anniversary at a ceremony in May.
After a month of unending rain throughout June,faculty and staff members on the Boston campusturned out in force for an ice cream social July 1on the ground fl oor of the Jaharis Center. Morethan 300 enthusiasts consumed 48 gallons ofice cream. “I think people were looking to getcheered up,” said caterer Andrew Korn.
Anish Bhardwaj
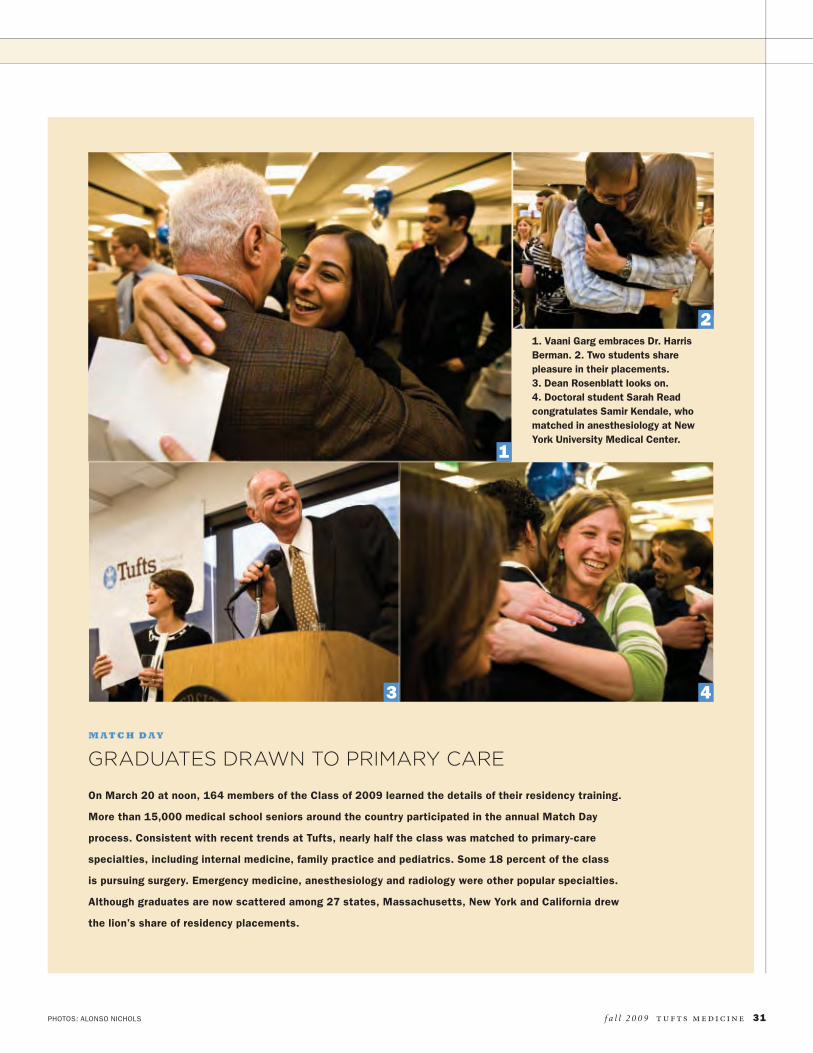
PHOTOS: ALONSO NICHOLS
GRADUATES DRAWN TO PRIMARY CARE
f a l l 2 0 0 9 t u f ts m e d i c i n e 31
On March 20 at noon, 164 members of the Class of 2009 learned the details of their residency training.
More than 15,000 medical school seniors around the country participated in the annual Match Day
process. Consistent with recent trends at Tufts, nearly half the class was matched to primary-care
specialties, including internal medicine, family practice and pediatrics. Some 18 percent of the class
is pursuing surgery. Emergency medicine, anesthesiology and radiology were other popular specialties.
Although graduates are now scattered among 27 states, Massachusetts, New York and California drew
the lion’s share of residency placements.
1. Vaani Garg embraces Dr. HarrisBerman. 2. Two students sharepleasure in their placements.3. Dean Rosenblatt looks on.4. Doctoral student Sarah Readcongratulates Samir Kendale, whomatched in anesthesiology at NewYork University Medical Center.
M AT C H D A Y
1
3 4
2

O N C A M P U S
32 t u f ts m e d i c i n e f a l l 2 0 0 9
CALIFORNIAHakeem Adeniyi, Family MedicineUniversity of California–San FranciscoEmily Amunwa, Ob/GynUniversity of California–San DiegoJoel Braman, TransitionalNaval Medical Center, San DiegoHugh Davis, Internal MedicineCedars-Sinai Medical Center,Los AngelesNathan Dettori, OtolaryngologyNaval Medical Center, San DiegoKyle Drullinger, Emergency MedicineStanford University Program,StanfordSarah Fitch, Internal MedicineUniversity of California–Davis,SacramentoBrandon Grimes, Internal MedicineCedars-Sinai Medical Center, LosAngelesHanh Hoang, Ob/GynSanta Clara Valley Medical Center,San JoseMichael Homer, Ob/GynUniversity of California–San DiegoJennifer Jones, Medicine Prelim.Harbor-UCLA Medical Center, LosAngelesDaniel Kahn, Internal MedicineUCLA Medical Center, Los AngelesYvonne Lee, PediatricsUniversity of California–Davis,SacramentoAndrew Ma, Internal MedicineCedars-Sinai Medical Center, LosAngelesElizabeth Morey, PediatricsStanford University Program,StanfordTuan Nguyen, PsychiatryUCLA/VA Greater LA, Los AngelesRebecca O’Neill, Internal MedicineUniversity of California–SanFrancisco, San FranciscoStephanie Phan, Internal MedicineUniversity of Southern CaliforniaProgram, Los AngelesMichelle Ploutz, PediatricsStanford University Program,StanfordDerek Richardson, Family MedicineDavid Grant Medical Center, Travis AirForce Base, Fairfi eldRajiv Saigal, Neurological SurgeryUniversity of California–San FranciscoEmmanuil Smorodinsky,Internal MedicineUniversity of California–San DiegoThomas Stafford, Medicine/PediatricsUniversity of Southern CaliforniaProgram, Los AngelesJeffrey Thomas, Internal MedicineUniversity of California–Irvine MedicalCenterDavid Tsai, Internal MedicineUniversity of Southern CaliforniaProgram, Los Angeles
Elizabeth Waters, PediatricsUniversity of California–San Diego
COLORADOHeather Robbins, Family MedicineUniversity of Colorado UniversityHospital Program, Denver
CONNECTICUTAaron Dickstein, Internal MedicineYale-New Haven Medical Center, NewHavenNicholas Dutton-Swain,Emergency MedicineUniversity of Connecticut HealthCenter, FarmingtonCarol Ilzarbe, PediatricsUniversity of ConnecticutHealth Center, FarmingtonLaurel Parker, Emergency MedicineUniversity of Connecticut HealthCenter, FarmingtonTushar Patel, Emergency MedicineUniversity of Connecticut HealthCenter, FarmingtonKristen Scarpato, UrologyUniversity of Connecticut HealthCenter, FarmingtonBenjamin Schmidt, General SurgeryUniversity of Connecticut HealthCenter, FarmingtonSmita Sukhatme,Diagnostic RadiologyHospital of St. Raphael, New HavenMedicine Prelim., Geisinger HealthSystem, Danville, Pa.
DISTRICT OF COLUMBIABehzad Bidadi, PediatricsGeorgetown University MedicalCenterMichael Lucke, Internal MedicineGeorge Washington UniversityPhuc Nguyen, Emergency MedicineGeorge Washington UniversityPhilip Sarges, Internal MedicineGeorgetown University MedicalCenter
FLORIDAAllan Bassan, General SurgeryUniversity of Miami-Jackson MemorialMedical Center, MiamiAlejandro Diaz, Orthopedic SurgeryUniversity of Miami-Jackson MemorialMedical Center, MiamiManuel Moreno, Internal MedicineUniversity of Miami-Jackson MemorialMedical Center, MiamiMichelle Pacheco, UrologyUniversity of South Florida College ofMedicine, Tampa
GEORGIAAaron Harris, Internal MedicineEmory University School of Medicine,Atlanta
ILLINOISHeather Begley, PediatricsMcGaw Medical Center, NorthwesternUniversity, Chicago
Nima Desai, PediatricsMcGaw Medical Center, NorthwesternUniversity, Chicago
IOWAAdam Asarch, DermatologyUniversity of Iowa Hospitals andClinics, Iowa CityTransitional, Caritas Carney Hospital,Boston
MAINEKaren Dmytrasz, Family MedicineMaine Medical Center, Portland
MARYLANDCarissa Meyer, Orthopedic SurgeryUniversity of Maryland MedicalCenter, BaltimoreMichael Silverman,Internal MedicineJohns Hopkins Hospital, BaltimoreWinnie Szeto, Medicine/PediatricsUniversity of Maryland MedicalCenter, BaltimorePolina Teslyar, PsychiatryUniversity of Maryland, SheppardPratt Program, Baltimore
MASSACHUSETTSNaomi Anker, Internal MedicineBeth Israel Deaconess MedicalCenter, BostonLisa Arvold, Emergency MedicineBrigham & Women’s Hospital, BostonJanelle Baptiste, Internal MedicineBoston University Medical Center,BostonChristine Bielick, Medicine/PediatricsUniversity of MassachusettsProgram, WorcesterKerry Biggs, Medicine/PediatricsBaystate Medical Center, Springfi eldJoseph Bornstein, General SurgeryMassachusetts General Hospital,BostonSusan Bruckert, PediatricsBaystate Medical Center, Springfi eldMichael Chin, Plastic SurgeryUniversity of MassachusettsProgram, WorcesterLisa Choi, AnesthesiologyCaritas St. Elizabeth’s MedicalCenter, BostonMedicine Prelim., University ofNevada Affi liated Hospitals, LasVegasSeema Chowdhury, AnesthesiologyBeth Israel Deaconess MedicalCenter, BostonTransitional, Lemuel ShattuckHospital, BostonVictor Chung, OtolaryngologyTufts Medical Center, BostonDanielle DeParalta, General SurgeryMassachusetts GeneralHospital, BostonMaria Dibner, NeurologyTufts Medical Center, BostonMedicine Prelim., Lahey Clinic,Burlington
Adam Drobnis, NeurologyTufts Medical Center, BostonMedicine Prelim., Caritas St.Elizabeth’s Medical Center, BostonJohn Duell, Internal MedicineTufts Medical Center, BostonErika Freebern, Internal MedicineTufts Medical Center, BostonDavid Glazier, Diagnostic RadiologyBeth Israel Deaconess Hospital,BostonMedicine Prelim., Caritas St.Elizabeth’s Medical Center, BostonRyan Gosselin, Medicine Prelim.North Shore Medical Center-SalemHospital, SalemAndrew Grandine, Surgery Prelim.Tufts Medical Center, BostonStephanie-Marie Guay, Ob/GynBeth Israel Deaconess MedicalCenter, BostonSeth Homer, Internal MedicineTufts Medical Center, BostonMichael Huang, Internal MedicineBoston University Medical Center,BostonTaj Kattapuram, DiagnosticRadiologyMassachusetts General Hospital,BostonMedicine Prelim., Exempla St. JosephHospital Program, Denver, Col.Maryanne Kazanis, DermatologyUniversity of MassachusettsProgram, WorcesterMedicine Prelim., Beth IsraelDeaconess Medical Center, BostonKevin Kotkowski,Emergency MedicineUniversity of MassachusettsProgram, WorcesterMichelle Long, Internal MedicineMassachusetts General Hospital,BostonDavid Lyczkowski,Medicine/PediatricsMassachusetts General Hospital,BostonGunjan Malik, Diagnostic RadiologyBeth Israel Deaconess MedicalCenter, BostonTransitional, McGaw Medical Center,Northwestern University, ChicagoGrace Mitchell,Diagnostic RadiologyBaystate Medical Center, Springfi eldMedicine Prelim., Caritas CarneyHospital, BostonTaylor Monica, PediatricsMassachusetts General Hospital,BostonJonathan Moran, PsychiatryMassachusetts General Hospital,BostonChristine Mulligan, Family PracticeCambridge Health Alliance/TuftsUniversity Program, CambridgeDavid Munson, Medicine/Primary CareMassachusetts General Hospital,Boston
RESIDENCIES
f a l l 2 0 0 9 t u f ts m e d i c i n e 33
Matthew Niemi, Internal MedicineBeth Israel Deaconess MedicalCenter, BostonJonathan Pack, DiagnosticRadiologyTufts Medical Center, BostonMedicine Prelim., Caritas CarneyHospital, BostonRupal Patel, General SurgeryUniversity of MassachusettsProgram, WorcesterSameer Puri, Orthopedic SurgeryTufts Medical Center, BostonTobi Quinto, PathologyTufts Medical Center, BostonAnthony Rios, Surgery Prelim.Beth Israel Deaconess MedicalCenter, BostonAnthony Rodriguez,Pediatrics/Child NeurologyTufts Medical Center, BostonJonathan Rogg, Emergency MedicineBrigham & Women’s Hospital, BostonEthan Rowin, Internal MedicineTufts Medical Center, BostonKara Smith, NeurologyBeth Israel Deaconess MedicalCenter, BostonMedicine Prelim., Beth IsraelDeaconess Medical Center, BostonHanni Stoklosa, EmergencyMedicineBrigham & Women’s Hospital, BostonBrett Sylvia, Emergency MedicineBeth Israel Deaconess MedicalCenter, BostonTrevor Szymanski, AnesthesiologyBrigham & Women’s Hospital, BostonMedicine Prelim., Caritas CarneyHospital, BostonNazbeh Taghizadeh,Internal MedicineTufts Medical Center, BostonNathaniel Temin,Diagnostic RadiologyLahey Clinic, BurlingtonTransitional, Caritas Carney Hospital,BostonEleonora Teplinsky,Internal MedicineTufts Medical Center, BostonThomas Tomszyk, Surgery Prelim.University of MassachusettsProgram, WorcesterLaurel Vuong, OphthalmologyTufts/New England Eye Center,BostonTransitional, Newton-WellesleyHospital, Newton Lower FallsIan Warrington, Emergency MedicineBeth Israel Deaconess MedicalCenter, BostonHelen Yeung, PediatricsMassachusetts General Hospital,BostonKatherine Zaleski, Surgery Prelim.Brigham & Women’s Hospital, Boston
MICHIGANZachary Fisk, AnesthesiologyUniversity of Michigan Program, AnnArbor
MINNESOTADaniel Kenney, Pediatrics/ChildNeurologyMayo Clinic Program, Rochester
MISSISSIPPIAdam Ackerman, Internal MedicineKeesler Medical Center, Keesler AirForce Base, Biloxi
MISSOURIJessica Groden, Ob/GynWashington University/Barnes-JewishHospital, St. LouisAron Rosenstock, Internal MedicineWashington University/Barnes-JewishHospital, St. LouisAnita Sarathi, Internal MedicineWashington University/Barnes-JewishHospital, St. Louis
NEW JERSEYJessica Mitchell,Emergency MedicineUMDNJ, Robert Wood JohnsonProgram, CamdenHannah Nien, Diagnostic RadiologyMonmouth Medical Center Program,Long BranchMedicine Prelim., University ofMassachusetts Program, Worcester
NEW YORKMohamad Abouzeid, General SurgeryNew York University Medical Center,New YorkAlok Anand, Surgery Prelim.North Shore Long Island JewishHealth System, ManhassetMelissa Chang, General SurgeryMount Sinai Hospital, New YorkBryan Conti, Orthopedic SurgerySUNY Health Science Center,BrooklynGiselle Cruz, Emergency MedicineNew York University Medical Center,New YorkJoshua Davenport, EmergencyMedicineSt. Luke’s/Roosevelt Hospital, NewYorkCamila Deza, Medicine/Primary CareNew York University Medical Center,New YorkLaura Doyon, General SurgeryMount Sinai Hospital, New YorkVaani Garg, Internal MedicineMount Sinai Hospital, New YorkSamir Kendale, AnesthesiologyNew York University Medical Center,New YorkMedicine Prelim., Caritas St.Elizabeth’s Medical Center, BostonShefali Kothary,Diagnostic RadiologyBeth Israel Medical Center, New YorkMedicine Prelim., NYU School ofMedicine, North Shore UniversityHospital, ManhassetBenjamin Krantz, Internal MedicineNew York Presbyterian Hospital–Columbia, New York
Evgeniya Krapivinsky, InternalMedicine/Social MedicineEinstein College of Medicine–Montefi ore, BronxTeodora Kurteva, UrologyEinstein College of Medicine–Montefi ore, BronxTheodore Macnow, PediatricsNew York Presbyterian Hospital–Columbia, New YorkAhmed Nasser, General SurgerySUNY Stony BrookAlexis Pappas, Internal MedicineMount Sinai Hospital, New YorkRavin Ratan, Internal MedicineNew York Presbyterian Hospital–WeillCornell, New YorkDilip Sidhu, AnesthesiologySt. Vincent’s Hospital, New YorkEric Silverman, AnesthesiologyMount Sinai Hospital, New YorkMedicine Prelim., St. Luke’s/Roosevelt Hospital, New YorkBrian Sullivan, AnesthesiologyNew York Presbyterian Hospital–WeillCornell, New YorkAnne Wyman, Internal MedicineSt. Luke’s/Roosevelt Hospital, NewYork
NORTH CAROLINALaura Martelly, Emergency MedicineCarolinas Medical Center Program,CharlotteMark Toyer, Emergency MedicineDuke University Medical Center,DurhamMichael Ward, Emergency MedicineDuke University Medical Center,Durham
OHIOCyrus King, Neurological SurgeryUniversity of Cincinnati College ofMedicine Program, Cincinnati
OREGONPatricia Ritze, Internal MedicineOregon Health & Science University,Portland
PENNSYLVANIADaisy Bang, Internal MedicineUniversity of Pittsburgh MedicalCenter, PittsburghAudrey Daggan, Internal MedicineHospital of the University ofPennsylvania, PhiladelphiaRichard Dalyai, Neurological SurgeryThomas Jefferson Hospital,PhiladelphiaStephanie Daniel, PediatricsChildren’s Hospital, PhiladelphiaAdam Griska, Orthopedic SurgeryHospital of the University ofPennsylvania, PhiladelphiaJoseph Kupferman, Internal MedicineHospital of the University ofPennsylvania, PhiladelphiaMichael Nathenson,Internal MedicineUniversity of Pittsburgh MedicalCenter, Pittsburgh
Thomas Rock, PediatricsChildren’s Hospital, Philadelphia
RHODE ISLANDMarilyn Barry, Diagnostic RadiologyBrown University Program, RhodeIsland Hospital, ProvidenceTransitional, Broadlawns MedicalCenter, Des Moines, IowaManisha Kumar, Family MedicineBrown University Program, MemorialHospital, PawtucketRobert Scaffi di, Internal MedicineBrown University Program, ProvidenceSameer Shah, Internal MedicineBrown University Program, Providence
SOUTH CAROLINANicole Dray, Diagnostic RadiologyMedical University of South Carolina,CharlestonTransitional, Trident Medical Center,Charleston
TEXASEva Christensen, Radiation OncologyUniversity of Texas M.D. AndersonCancer Center, HoustonTransitional, Tufts Medical Center,BostonAlice Leung, General SurgeryUniversity of Texas SouthwesternMedical School Program, DallasOlubunmi Ogundadegbe,Medicine/PediatricsUniversity of Texas Medical School,HoustonElaine Trieu, Ob/GynBaylor College of Medicine Program,Houston
UTAHDaniel Adams, TransitionalIntermountain Medical Center, MurrayBenjamin Romney,Diagnostic RadiologyUniversity of Utah Affi liated Hospitals,Salt Lake CityTransitional, Caritas Carney Hospital,Boston
VERMONTJessica Heath, AnesthesiologyUniversity of Vermont Program,BurlingtonTransitional, MetroWest MedicalCenter, Framingham, Mass.
WASHINGTONMaya Narayanan, Internal MedicineUniversity of Washington Program,SeattleLewis Rieley, AnesthesiologyUniversity of Washington Program,SeattleMedicine Prelim., Lahey Clinic,Burlington, Mass.K. Eiko Tubridy, Family MedicineValley Medical Center, Renton
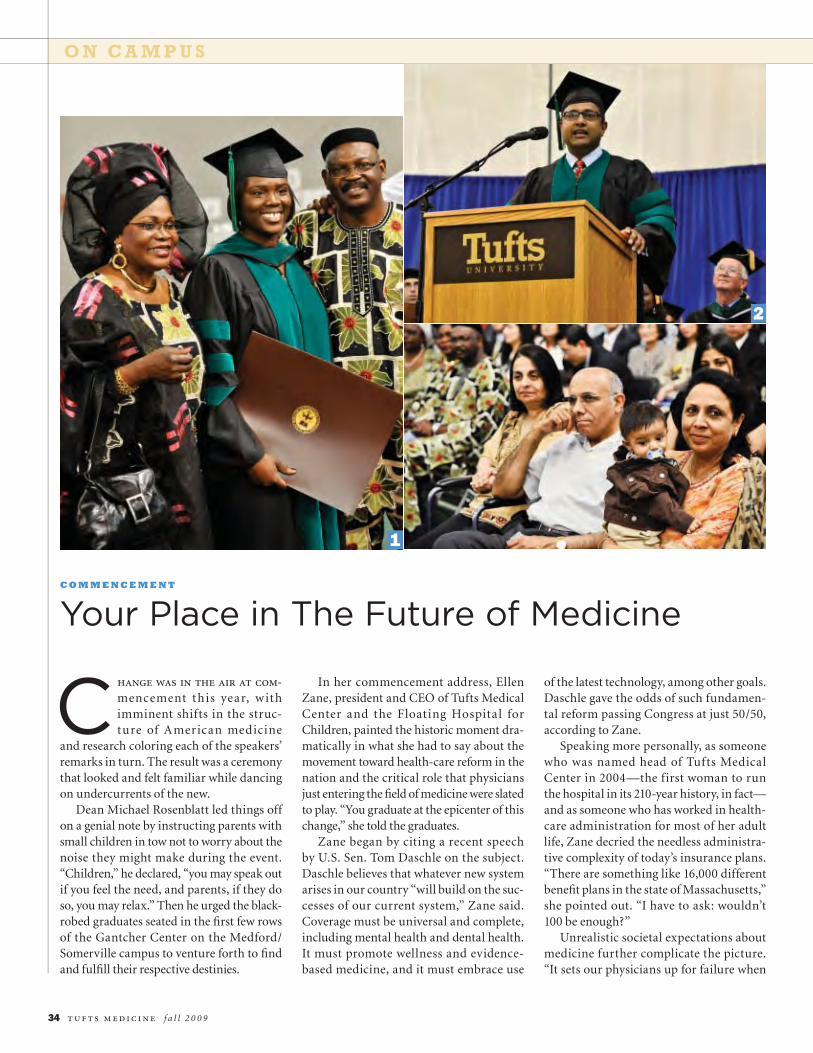
O N C A M P U S
34 t u f ts m e d i c i n e f a l l 2 0 0 9
C hange was in the air at com-
mencement this year, withimminent shifts in the struc-ture of American medicine
and research coloring each of the speakers’remarks in turn. The result was a ceremonythat looked and felt familiar while dancingon undercurrents of the new.
Dean Michael Rosenblatt led things offon a genial note by instructing parents withsmall children in tow not to worry about thenoise they might make during the event.“Children,” he declared, “you may speak outif you feel the need, and parents, if they doso, you may relax.” Then he urged the black-robed graduates seated in the fi rst few rowsof the Gantcher Center on the Medford/Somerville campus to venture forth to fi ndand fulfi ll their respective destinies.
In her commencement address, EllenZane, president and CEO of Tufts MedicalCenter and the Floating Hospital forChildren, painted the historic moment dra-matically in what she had to say about themovement toward health-care reform in thenation and the critical role that physiciansjust entering the fi eld of medicine were slatedto play. “You graduate at the epicenter of thischange,” she told the graduates.
Zane began by citing a recent speechby U.S. Sen. Tom Daschle on the subject.Daschle believes that whatever new systemarises in our country “will build on the suc-cesses of our current system,” Zane said.Coverage must be universal and complete,including mental health and dental health.It must promote wellness and evidence-based medicine, and it must embrace use
of the latest technology, among other goals.Daschle gave the odds of such fundamen-tal reform passing Congress at just 50/50,according to Zane.
Speaking more personally, as someonewho was named head of Tufts MedicalCenter in 2004—the first woman to runthe hospital in its 210-year history, in fact—and as someone who has worked in health-care administration for most of her adultlife, Zane decried the needless administra-tive complexity of today’s insurance plans.“There are something like 16,000 differentbenefi t plans in the state of Massachusetts,”she pointed out. “I have to ask: wouldn’t100 be enough?”
Unrealistic societal expectations aboutmedicine further complicate the picture.“It sets our physicians up for failure when
Your Place in The Future of MedicineC O M M E N C E M E N T
1
2
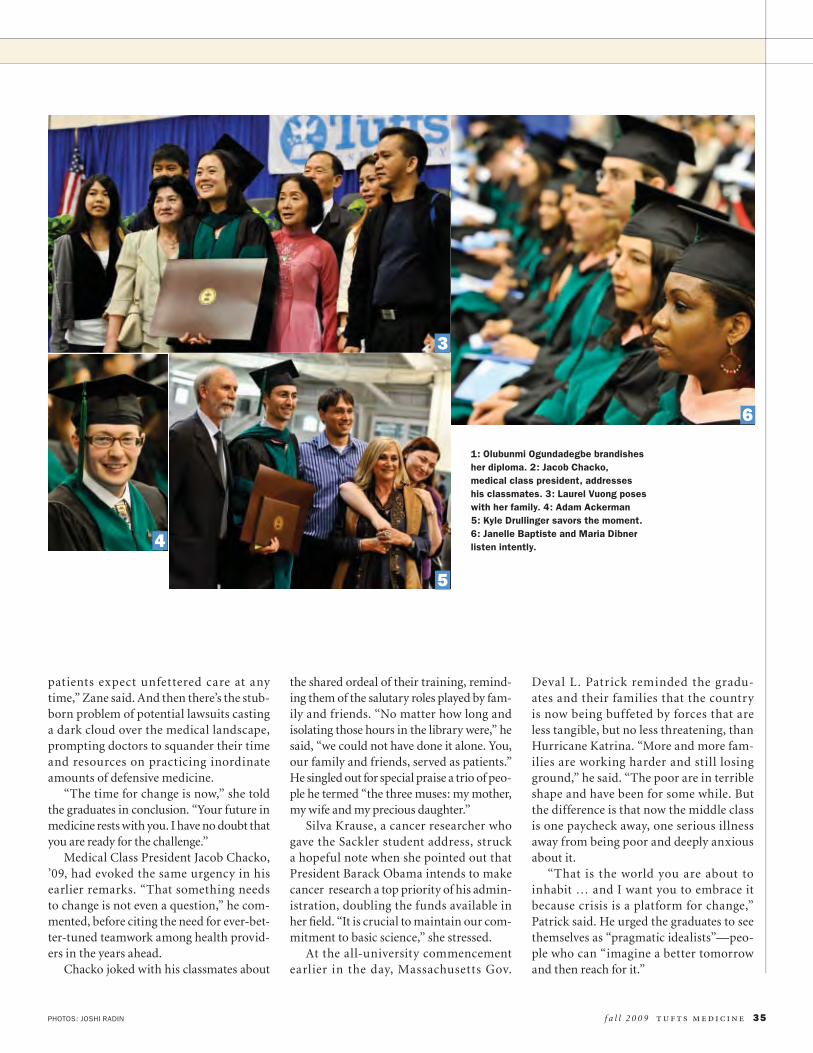
PHOTOS: JOSHI RADIN f a l l 2 0 0 9 t u f ts m e d i c i n e 35
patients expect unfettered care at anytime,” Zane said. And then there’s the stub-born problem of potential lawsuits castinga dark cloud over the medical landscape,prompting doctors to squander their timeand resources on practicing inordinateamounts of defensive medicine.
“The time for change is now,” she toldthe graduates in conclusion. “Your future inmedicine rests with you. I have no doubt thatyou are ready for the challenge.”
Medical Class President Jacob Chacko,’09, had evoked the same urgency in hisearlier remarks. “That something needsto change is not even a question,” he com-mented, before citing the need for ever-bet-ter-tuned teamwork among health provid-ers in the years ahead.
Chacko joked with his classmates about
the shared ordeal of their training, remind-ing them of the salutary roles played by fam-ily and friends. “No matter how long andisolating those hours in the library were,” hesaid, “we could not have done it alone. You,our family and friends, served as patients.”He singled out for special praise a trio of peo-ple he termed “the three muses: my mother,my wife and my precious daughter.”
Silva Krause, a cancer researcher whogave the Sackler student address, strucka hopeful note when she pointed out thatPresident Barack Obama intends to makecancer research a top priority of his admin-istration, doubling the funds available inher fi eld. “It is crucial to maintain our com-mitment to basic science,” she stressed.
At the all-university commencementearlier in the day, Massachusetts Gov.
Deval L. Patrick reminded the gradu-ates and their families that the countryis now being buffeted by forces that areless tangible, but no less threatening, thanHurricane Katrina. “More and more fam-ilies are working harder and still losingground,” he said. “The poor are in terribleshape and have been for some while. Butthe difference is that now the middle classis one paycheck away, one serious illnessaway from being poor and deeply anxiousabout it.
“That is the world you are about toinhabit … and I want you to embrace itbecause crisis is a platform for change,”Patrick said. He urged the graduates to seethemselves as “pragmatic idealists”—peo-ple who can “imagine a better tomorrowand then reach for it.”
1: Olubunmi Ogundadegbe brandishesher diploma. 2: Jacob Chacko,medical class president, addresseshis classmates. 3: Laurel Vuong poseswith her family. 4: Adam Ackerman5: Kyle Drullinger savors the moment.6: Janelle Baptiste and Maria Dibnerlisten intently.
3
4
5
6
STAYING CONNECTEDA L U M N I N E W S
36 t u f ts m e d i c i n e f a l l 2 0 0 9
We’re Counting on You
We will be going green with a futurealumni association dues solicitation byproviding an electronic means of makingyour dues payment. The advantages will beto save on postage, avoid repetitive solicita-tions of those who have already contributedand keep you updated about your medi-cal school via email. For those who prefercontact by conventional mail, we will stillmaintain that capability.
In these tough fi nancial times, your con-tinued support is more important than ever.Your generosity allows us to act on issuesand to continue to make our voices heard.
the fund for tufts medicine and the annual dues
collected for the Tufts Medical Alumni Associationare two ways of investing in the school that has givenso much to us over the years. They are both essen-tial instruments in providing support for the placewhere we began our professional lives.
As the medical school website says, “Gifts tothe Fund for Tufts Medicine support vital stu-dent fi nancial aid, faculty development, innova-tive curriculum enhancements, laboratory andtechnological upgrades, and library and research
resources, all the tools essential to making Tufts Medicine a distinguishedleader in medical education and research.”
Your alumni association dues allow us to support a variety of causes that haveproven themselves to be worthy, important and memorable: our annual SeniorClass Dinner, the White Coat Ceremony each fall, the festivity of reunions thatround out the school year, the fi nancial aid that is so critical to our ongoingefforts to recruit the best and brightest students and our award-winning TuftsMedicine magazine. I encourage you to support both your alumni associationand the Fund for Tufts Medicine.
David Wong, ’[email protected]
v i s i t : www. t u f t s . e du / a l umn i / e d - t r ave l - l e a r n . h tm l
Visit ourwebsite to seethe exciting newline-up of 2010destinations!
Visit ourwebsite to seethe exciting newline-up of 2010destinations!
TRAVEL-LEARN TRAVEL-LEARN
T R A V E L T O E X T R A O R D I N A R Y P L A C E S W I T H E X C E P T I O N A L P E O P L ET R A V E L T O E X T R A O R D I N A R Y P L A C E S W I T H E X C E P T I O N A L P E O P L E
From Germany to Greece,
from Tuscany to Tanzania, our
journeys feature intellectual
inquiry with lectures and
exploration. There’s a perfect
trip for every taste! Call
Usha Sellers, Ed.D., Program
Director, at 800-843-2586
for our brochure or visit our
website for itineraries.
From Germany to Greece,
from Tuscany to Tanzania, our
journeys feature intellectual
inquiry with lectures and
exploration. There’s a perfect
trip for every taste! Call
Usha Sellers, Ed.D., Program
Director, at 800-843-2586
for our brochure or visit our
website for itineraries.

f a l l 2 0 0 9 t u f ts m e d i c i n e 37
47 Ted Gordon of Milton,Mass., has retired after
60 years of practicing medicine,most recently at the V.A. MedicalCenter in Boston. He received acongratulatory note from DeanMichael Rosenblatt and TuftsPresident Lawrence S. Bacowin recognition of the milestone.Gordon and his wife, Claire, havebeen faithful and generous sup-porters of the medical school formany years.
Hyman J. Roberts of WestPalm Beach, Fla., an internalmedicine specialist, is celebrat-ing publication of his 24thbook, A Manifesto for AmericanMedicine: Goal: ImprovedDoctoring and Health Care(Sunshine Sentinel Press). Henotes that the latest volume isbeing released exactly 50 yearsafter the publication of his fi rstbook, Diffi cult Diagnosis (W.B.Saunders Co.).
50 Joseph Dowling ofProvidence, R.I.,
writes that he is still practicingophthalmology on a reducedschedule, three days a week.His health is good, and hisinterests include his four chil-dren and 11 grandchildren, aswell as tennis, golf and travel.In June, Dowling presented aDistinguished Alumnus Lectureat the Massachusetts Eye andEar Infi rmary in Boston.
54 Daniel Tassel ofLexington, Mass.,
retains fond memories of hissecond year of medical schooland of William B. Schwartz,whom he cites as an infl uentialfaculty member. He writes thathe is grateful for Tufts having in-stilled in him “the importance ofpatients’ concerns and patientcare.” Tassel enjoys birding, trav-el, reading and family time. Fora hobby, he has been collecting
19th-century photographs ofIsrael and the Middle East.
57 Ira Pastan, A53, ofPotomac, Md., chief
of the Laboratory of MolecularBiology at the National CancerInstitute, has been awardedthe 2009 International AntonioFeltrinelli Prize for Medicinein recognition of his work inreceptor biology and for thedevelopment of immunotoxinsto treat cancer. He received theaward in Rome in June from theAccademia Nazionale dei Lincei,Italy’s most prestigious societyfor the sciences and humani-ties. The award is given everyfi ve years for achievement inthe arts, music, literature, his-tory, philosophy, medicine andthe physical and mathematicalsciences, and includes a size-able monetary prize and a goldmedal. Pastan established theLaboratory of Molecular Biologyin 1970. He was among the fi rstto clone and sequence the EGFreceptor and to demonstratethat it is amplifi ed in manycancers.
59 Gerald Bernstein ofLarchmont, N.Y., is a
specialist in endocrinology anddiabetes, with affi liations at theFriedman Diabetes Institute,Beth Israel Medical Center (N.Y.)and the Albert Einstein Collegeof Medicine. He was presidentof the American DiabetesAssociation from 1998–99.He and his wife, Sophia, havetwo grown children, Cary andClifford, and two grandchildren,Samantha, 7, and Chester, 4.
John Donovan of Shrewsbury,Mass., has retired from hispediatrics practice. He wasformerly chief of pediatrics atWorcester Hahnemann Hospitalin Worcester, Mass. Donovancredits Tufts with having made
him into a skilled diagnostic phy-sician, citing the time he made adiagnosis of Addington diseasein a 13-year-old boy he met ona house call. These days hespends his free time babysitting,gardening and fi shing.
Joseph Kennedy Jr. of Boston,an associate professor of pedi-atrics at Tufts for more than 40years, is happily retired. He andhis wife, Patricia, have sevenchildren and 16 grandchildren.
Ronald Loescher of Amherst,a family medicine specialistbased in Holyoke, Mass., is afounder of Amherst MedicalAssociates and of the HolyokeHealth Center. He likes to garden,hike, listen to music, stay activein his church and run marathons,having completed eight BostonMarathons. Loescher recallsattending worship services atPark Street Church back in hisstudent days. “You need a strongand vibrant religious faith if youwant to be a good doctor and agood person,” he advises today’sstudents.
James Shira of GreenwoodVillage, Colo., refl ects that dur-ing his 20 years in U.S. Armypediatrics he was able to mentor
and train more than 750 pediatricresidents, as well as many otherfaculty members. He is currentlyaffi liated with Children’s Hospitalin Aurora, Colo., and happily mar-ried to Paula, his wife of 51 years.They have three children andfour grandchildren, one of whomstarted college at Tufts this fall.
60 Herbert Rakatanskyof Providence, R.I.,
retired from his gastroenter-ology practice last year. Hecontinues to chair the PhysicianHealth Program in Rhode Islandand to teach at the WarrenAlpert Medical School at BrownUniversity. In 2008 the RhodeIsland Medical Society estab-lished the Herbert RakatanskyAward for Professionalism; hewas the fi rst recipient.
62 Donald E. Wilson,H08, senior vice
president for health services atHoward University and a medi-cal school overseer, receivedthe Abraham Flexner Award fordistinguished service to medicaleducation from the Associationof American Medical Colleges.The fi rst African-American dean
DON’T FORGET TO CHECK OUTTHE NEW TUFTS UNIVERSITY HOMEPAGE
www. .eduThe expandedformat showcasesmore storiesabout the people,programs, researchand scholarshipthat define youruniversity.
CLASS NOTES
A L U M N I N E W S
of an accredited non-minoritymedical school, the Universityof Maryland School of Medicine,Wilson was instrumental in theschool’s emergence as a leadingresearch institution.
64 John Carroll ofWinchester, Mass.,
continues to practice full-time inMalden, and was recently volun-tarily recertifi ed by the AmericanBoard of Internal Medicine. Heand his wife have four childrenand eight grandchildren.
Robert Nadeau of Rochester,N.Y., divides his time betweenhis part-time psychiatry practicein the Rochester area and asummer home in Little Compton,R.I., where he plans to retire.Nadeau and his wife, Betsy, havebeen together nearly 50 years.He reports that they travel oftento keep in touch with their scat-tered family and friends.
69 Charles Hemenway Jr.,of Fairfi eld, Conn., has
been named the 2009 Physicianof the Year by the GreaterBridgeport Medical Association.Each year the associationhonors a physician for outstand-ing dedication to the practiceof medicine in the GreaterBridgeport area. Hemenway hasa pediatrics practice in Fairfi eld.
71 Jeffry Brand ofMarblehead, Mass.,
has been elected presidentof the Society for AmbulatoryAnesthesia, a national organiza-tion that promotes education,research and safety for thoseundergoing outpatient surgery.Brand reports that his anesthe-siology practice continues to bebusy and rewarding. He and hisfamily enjoy travel, skiing and es-pecially cycling. This spring, Brandpaid a visit to classmate RussellBrynes out in Los Angeles and
found that Brynes “like myself, isstill working too hard.”
72 M. Katherine Shearof New York City is a
member of the National AdvisoryCouncil for Complementary andAlternative Medicine, a compo-nent of the National Institutesof Health that is the lead federalagency for complementary andalternative medicine research.Members contribute their ex-pertise over four-year terms andmeet three times a year to offeradvice and recommendationsfor research in the fi eld. Shearis the Marion E. KenworthyProfessor of Psychiatry anddirector of the Bereavementand Grief Research and TrainingProgram at Columbia University,where she mentors studentsand new faculty. She alsoserves as an adjunct facultymember at the University ofPittsburgh.
73 Martha Linet of ChevyChase, Md., chief of
the Radiation EpidemiologyBranch in the Division of CancerEpidemiology and Genetics atthe National Cancer Institute,has been elected to the JohnsHopkins University Society ofScholars. Linet and 14 otheresteemed scientists and clini-cians were honored during thesociety’s 40th induction cer-emony in May and again at theuniversity-wide commencementceremonies. She is considereda leading expert in the epidemi-ology of leukemia.
74 Karen ReuterKrolikowski of
Wellesley, Mass., professorof radiology at Tufts and anultrasound specialist at theLahey Clinic, cites one facultymember in particular as havingmade a difference in her medical
training. “Dr. Barbara Carterinfl uenced me strongly to spe-cialize in diagnostic radiology,”she says. “I learned effectiveteaching from her.” In her sparetime, Krolikowski enjoys homedecorating, reading novels, work-ing out, playing tennis and takingdance lessons.
76 Timothy Murphy ofEast Amherst, N.Y.,
an internationally recognizedexpert in bacterial infections inthe respiratory tract, has beenappointed to the new position ofsenior associate dean for clini-cal and translational research atthe University of Buffalo Schoolof Medicine and BiomedicalSciences, where he has servedas a Distinguished Professor inthe department of medicine.
78 Mario E. Motta ofGloucester, Mass.,
an assistant clinical professorof medicine, has been electedpresident of the MassachusettsMedical Society, the statewideprofessional organization ofphysicians. He will serve aone-year term as the top offi cerof the society whose member-ship includes more than 21,000
physicians, residents and medi-cal students throughout theCommonwealth. Motta hasbeen on the faculty of TuftsMedical School since 1993and is a fellow of the AmericanCollege of Cardiology and theAmerican Society of NuclearCardiology.
79 Beatrice Desper ofMandeville, La., is
president of the AmericanMedical Women’s Association,a national organization of morethan 13,000 women physiciansand medical students thatwas founded in 1915. Desperand her husband moved fromConnecticut to Louisiana fi veyears ago. Last year she openedher own ob/gyn practice,beginning with a roster of 300patients and serving twice thatnumber now.
81 Patricia Abbitt ofGainesville, Fla., a
professor of radiology at theUniversity of Florida College ofMedicine, received the 2009Hippocratic Award from thecollege’s graduating class. Theaward honors teachers whoserve as role models for the
38 t u f ts m e d i c i n e f a l l 2 0 0 9
A L U M N I N E W S
WE WANT TO HEAR FROM YOU!Fill us in on your news. Have you been getting togetherwith classmates? Have a new job? A special project orappointment? Is your family growing? Keep your fellowalumni/ae posted by dropping us a line.
CHECK HERE IF ADDRESS IS NEW.Send to:Tufts Medical Alumni Relations,136 Harrison Avenue, Boston, MA 02111or e-mail [email protected]
CLASS NOTES DEADLINE FOR NEXT ISSUE IS NOVEMBER 1, 2009

class. She received the awardfrom the Class of 2004. Abbittalso received the SustainedExcellence in Medical EducationAward.
William Ladd of San Diego,Calif., has been inducted as afellow in the American Collegeof Radiology. He is a partnerand shareholder of LJR MedicalGroup in San Diego and a staffradiologist at Scripps MemorialHospital, with locations in LaJolla, Chula Vista, Encinitas andSan Diego.
83 Kevin Killeen, a board-certifi ed urologist, has
joined the North Adams, Mass.,offi ce of Berkshire HealthSystems’ Urology Services ofthe Berkshires. He completedhis residency training in urologyat the Lahey Clinic in Burlington,Mass.
84 Jane Fay of Concord,Mass., and her hus-
band, Ed, a lawyer, have fi vechildren ranging in age from 17to 25; she says they keep herbusy. Two of her children are nowenrolled at the medical school:Daniel Fay, ’11, and Caitlin Fay,’13. Fay works as a diagnosticradiologist at Emerson Hospitalin Concord.
85 Therese Mulvey ofMilton, Mass., has been
chosen to direct oncology servic-es at the new Centers for CancerCare at the Southcoast HospitalsGroup in Fairhaven, Mass., witha satellite location in Fall River,Mass. The centers provide afull range of oncology services,including radiation therapy, che-motherapy, lab and radiology, aswell as patient support, nutritioncounseling and complementarytherapies. Mulvey is presidentof Commonwealth HematologyOncology in Quincy, Mass.
88 Scott Cohen, apediatrician in Bangor,
Maine, drew on the miseryhe’d seen during his three-month-long Albert SchweitzerFellowship in West Africa follow-ing graduation to launch an over-seas medical outreach agencyin 2002 called the GlobalPediatric Alliance (GPA). Theorganization works to improvethe quality of life among childrenin developing countries. Thealliance teaches lay health work-ers in places like Guatemala,Mexico and Ecuador how to treatcommon injuries and assist withchildbirth. “In these regions,most women, at least 85percent, deliver babies in theirhuts,” Cohen told the BangorDaily News in June. “If we spend$100 training a midwife, she’llreturn to her village and trainanother generation. That’s myhope.” While infant mortalityin many developing countriesruns as much as 10 timeshigher than what it does in theU.S., “it’s all due to preventablediseases and preventableproblems,” Cohen notes.That’s why his organizationprovides rain catch basins tosupply clean drinking water,and has installed dry ecologi-cal toilets for basic sanitationin remote villages. In recogni-tion of his work with GPA, theAmerican Academy of Pediatricshas named Cohen a “PediatricHero.” The heroes campaignwas created last fall “to fi ndstories of the everyday pediatricheroes among us,” according tothe group’s website. Cohen wasone of just four pediatricianshonored nationally. He and hiswife, Andrea, have a one-year-old son, Lucas. The entirefamily will attend the hero awardpresentation ceremony at theAAP’s 2009 national conventionin Washington, D.C., in October.
Nancy Rappaport ofCambridge, Mass., has a bookcalled In Her Mother’s Wake(Basic Books) coming out this fallthat addresses the trauma of hermother’s suicide when the authorwas a child. Rappaport is a childpsychiatrist who works with youthin the Cambridge Public Schoolsystem on issues including vio-lence prevention.
89 Richard Antaya ofOrange, Conn., is an
associate professor of dermatol-ogy and pediatrics and directorof pediatric dermatology at YaleMedical School. Last year he wasnamed the state’s top doctorin dermatology by ConnecticutMagazine. Antaya singles out sur-geon Ernie Grable as an infl uen-tial fi gure in his training because“he was intense and cared deeplyabout the students and aboutmaking us perform beyond our ex-pectations.” Antaya and his wife,Mary, have two children, Nicole,14, and Joseph, 10.
Elisa Alter Zenni, J85, ofPonte Vedra Beach, Fla., anassociate professor of pediatricsand assistant dean for educa-tional affairs at the Universityof Florida College of Medicine inJacksonville, is a member of theCollege of Medicine’s Society ofTeaching Scholars, establishedfor faculty who have demonstrat-ed teaching excellence and acommitment to mentoring futurephysicians and scientists. Zenniwas the fi rst female faculty mem-ber inducted into the society.
93 Lynette Scherer ofSacramento, Calif.,
has been named chief of theUniversity of California–DavisTrauma Program for the UC DavisMedical Center. She is an associ-ate professor in the departmentof surgery, where she directs thesurgical residency program.
95 John Wigneswaranof Dayton, Ohio, is
CEO of Nephroceuticals, acompany that produces nutri-tional supplements aimed atpromoting health in patientswith chronic kidney disease.The company recently struck upan educational partnership withthe National Kidney Foundation,focusing on the importance ofnutrition and early detectionof kidney disease. Developingand distributing print and onlineeducational materials for bothpatients and professionals willbe a central part of the deal.“Nutrition is one aspect of thecare of kidney patients that isfar too often overlooked,” saysWigneswaran. “As a practicingnephrologist, I know how impor-tant it is to counsel our patientson appropriate nutritionalsupplementation based on theclinical evidence.”
01 Len Leonidas ofCastleton, N.Y., and his
wife, Jen Albanese, welcomedtheir second son, Jonah Blaise,on March 31. Their fi rst son,Kaedan, is two years old. Len fi n-ished his residency in pediatricsat Albany Medical Center andis in practice with CommunityCare Physicians in Schodack,N.Y., about 12 miles south ofAlbany. His father, LeonardoLeonidas, assistant clinical pro-fessor of pediatrics, received aDistinguished Career in Teachingaward from the Class of 2009this past May.
06 Becky Rich, J01, andDave Konieczny of
North Andover, Mass., welcomedtheir son, Aidan James, on April11. She is fi nishing her pediatricresidency at MassachusettsGeneral Hospital and will be join-ing Dowd Medical Associates inReading, Mass.
f a l l 2 0 0 9 t u f ts m e d i c i n e 39
A L U M N I N E W S
MORTON A. MADOFF, M82P, WHO SERVED AS DEAN OF TUFTS UNIVERSITY
School of Medicine from 1992 to 1995 and founded the TuftsAssociated Health Plan, died of pneumonia on June 6 at the age of 81.
“Mort was a physician, a public-health leader, an innovator, butfi rst and foremost, Mort was an educator,” Harris Berman, vicedean and former chief executive of the Tufts Health Plan, said of hiscolleague.
“He truly loved Tufts Medical School and his students,”Berman continued. “He taught students the importanceof community medicine, public health and populationmedicine. His vision of the skills needed by the modernphysician was both expansive and prescient. He spawnedinnovative new educational programs: combined degreesfor medical students in public health, in managementand business, and even in international law and diploma-cy. Mort had a profound effect on medical education,”Berman said.
The Boston Globe described how Madoff, with a$3,000 grant from the medical school, created what-would become one of the largest health maintenance organizationsin the state. Long a student of infectious disease, Madoff hopedto keep patients at the center of any health-care model, and at itslaunch in 1981, Tufts Associated Health Plan was designed so peoplecould stay with their private physicians. By 1998 it was the second-
largest HMO in Massachusetts, with more than one million membersthroughout New England and more than $1 billion in annual revenues.He retired as chairman of the board of Tufts Health Plan in 1997.
Born in Clinton, Mass., where his father was a tailor, Madoff was achild of the Great Depression. “He was very proud of the fact that hewas born and raised poor, and he looked out for people who didn’t have
a lot,” his son, Lawrence, ’82, told the Globe.After graduating from Clinton High School in 1944,
Madoff joined the Navy, serving stateside until 1946.He then attended Tulane University, earning a bach-elor’s degree in English in 1951 and a medical degreein 1955. He married fellow student Marjorie JaneKahn in 1953. He completed his residency at TuftsMedical Center and the Boston Veterans AdministrationHospital and worked for Lemuel Shattuck Hospital inBoston, specializing in infectious diseases.
Marjorie, his wife of 48 years, died in 2001. Hemarried Betty Solomon in 2003. He is also survivedby two daughters, a brother and six grandchildren.
Memorial gifts in support of the Morton A. Madoff, M.D., M.P.H.,Professorship in Public Health and Family Medicine at Tufts Schoolof Medicine may be sent to Tufts University School of Medicine,Offi ce of Development & Alumni Relations, 136 Harrison Avenue,Boston, MA 02111.
MORTON A. MADOFF, FORMER MEDICAL SCHOOL DEAN
Morton A. Madoff
John Sarafi an, ’34, died onFebruary 10. He was a mem-ber of the medical staff at St.Joseph’s Hospital in Providence,R.I., from 1936 until his retire-ment in 1982. In addition to hisprivate practice, he providedmedical services to the GorhamSilver Co. for many years andwas an avid golfer.
Casimir Bielecki, A35, ’39,of Crestone, Colo., died onJuly 17, 2008. He practicedin Norwich, Conn., from 1941until he retired in 1982. He wasa life member of St. JosephParish, the Norwich Elks and theKnights of Columbus. An avidgolfer, he was a founding mem-ber of the Pautipaug CountryClub in Baltic, Conn.
Edward Israel, ’55, of New Yorkdied on January 26. He fi rst stud-ied and became board-certifi edin radiology and then enrolledat Stony Brook University tostudy psychiatry. He was board-certifi ed in psychiatry and chiefof psychiatry for the RiverheadClinic in New York. He served inthe U.S. Army and was stationedin Chateauroux, France. Hisinterests included playing theoboe and photography.
FACULTYRobert Rustigian of NorthEaston, Mass., who taughtbacteriology, immunology, mi-crobiology and virology, died onJune 9 at age 93. He grew up inMedford, Mass., and attendedthe University of Massachusettsbefore obtaining his Ph.D.
in microbiology from BrownUniversity. He had served aschief of the Virology ResearchLaboratory at the V.A. Hospitalin Brockton, Mass., until retiringin 1986.
Richard Stiles, ’45, of Atlantis,Fla., an assistant clinical profes-sor of urology, died on May 14at age 88. He had been headurologist at Winchester Hospitalin Winchester, Mass., for manyyears. A native of Boston, heattended Boston Latin Schooland Boston College. While inmedical school, he was part ofthe naval reserve, and his medi-cal degree was expedited so thathe could serve in the U.S. Navyduring the fi nal months of WorldWar II. Stiles began his career atWinchester Hospital in 1951. He
became chief of urology andwas elected president of themedical staff in 1979. He issurvived by his wife of 63 years,Joan, two sons, two daughtersand two grandchildren.
Lorande Woodruff of Needham,Mass., an instructor in urology,died on April 9. Born in NewHaven, Conn., he was a graduateof Yale Medical School. He wasinducted into the U.S. Navy in1941 and served with the NavyMedical Corps in the Pacifi c.Woodruff taught at both Tuftsand Harvard medical schools andwas on staff at MassachusettsGeneral and Deaconess hospi-tals, where he remained in activepractice for more than 50 yearsand was known for his attentivecare of patients.
PHOTO: BRAFORD F. HERZOG40 t u f ts m e d i c i n e f a l l 2 0 0 9
OBITUARIES
For more information please contact Tufts’ Gift Planning Office888.748.8387 giftplanning@ tufts.edu www.tufts.edu/giftplanning
G. MARSHAL GOLDBERG, MD, A54, M57, A82P, and his wife, Sandra, A82P,
an active Simmons College alumna, have “proudly watched Tufts grow locally
and internationally in academic stature and influence on medical care.” Dr.
and Mrs. Goldberg will establish the G. Marshal and Sandra E. Goldberg Schol-
arship Fund by designating the School of Medicine as a beneficiary in their
wills. It is their hope that this gift “will serve as a token of how grateful our
family is to Tufts and how proud we are to be connected to it.”
“ Having considered Tufts
College as well as Tufts
School of Medicine
my first choices, I have
always been grateful
that I was one of Tufts’
choices twice. I always
felt at home at the Med
School and enjoyed
training there and at its
hospital affiliates. To this
day, I judge medical ethics
and education with Tufts
as my highest standard.”
“ Having considered Tufts
College as well as Tufts
School of Medicine
my first choices, I have
always been grateful
that I was one of Tufts’
choices twice. I always
felt at home at the Med
School and enjoyed
training there and at its
hospital affiliates. To this
day, I judge medical ethics
and education with Tufts
as my highest standard.”
NONPROFIT ORG.U.S. POSTAGE
PAIDBOSTON, MA
PERMIT NO. 1161
School of Medicine
136 Harrison AvenueBoston, ma 02111www.tufts.edu/med
THE INNER LIFEUniversity Chaplain David O’Leary has always had a keen interest in moral theology. For the past seven years, he has brought his training to bear in a class he teaches at the medical school, helping students to think about the humane and spiritual dimensions of medicine. Our interview appears on page 8.
TUFTS
UN
IVERS
ITY OFFIC
E OF PU
BLIC
ATION
S 7
95
9 0
9/0
9
PH
OTO
: ALO
NS
O N
ICH
OLS