nsaids
TRANSCRIPT

NSAIDs
Dr. Karun Kumar
JR-II
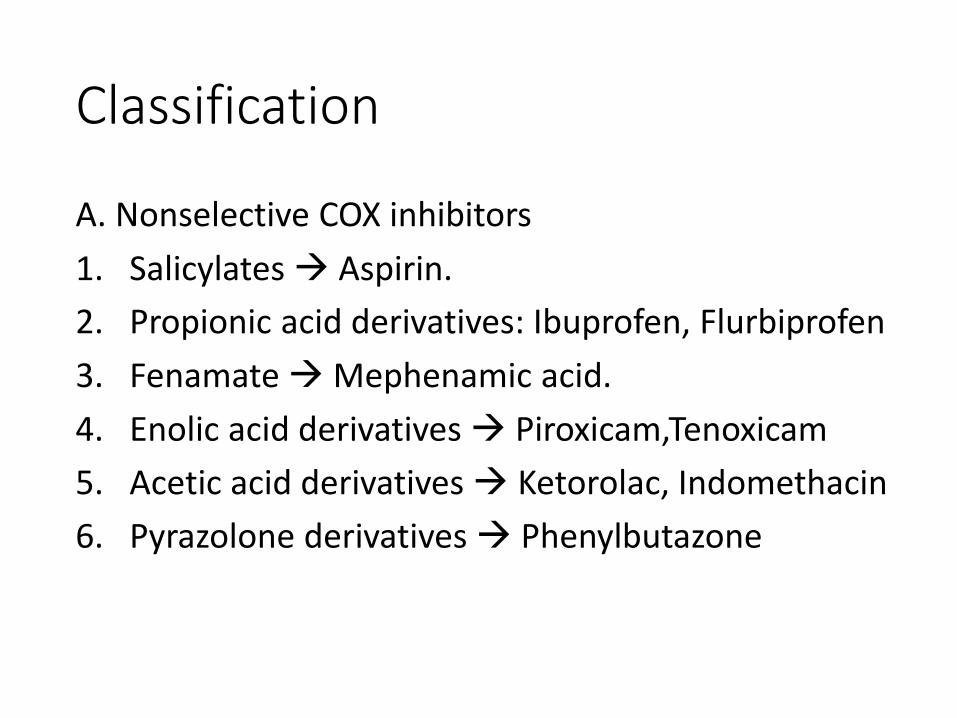
Classification
A. Nonselective COX inhibitors
1. Salicylates Aspirin.
2. Propionic acid derivatives: Ibuprofen, Flurbiprofen
3. FenamateMephenamic acid.
4. Enolic acid derivatives Piroxicam,Tenoxicam
5. Acetic acid derivatives Ketorolac, Indomethacin
6. Pyrazolone derivatives Phenylbutazone

B. Preferential COX-2 inhibitors Nimesulide, Diclofenac, Aceclofenac
C. Selective COX-2 inhibitors Celecoxib, Etoricoxib, Parecoxib
D. Analgesic-antipyretics with poor antiinflammatoryaction
1. Paraaminophenol derivative: Paracetamol(Acetaminophen).
2. Pyrazolone derivatives: Metamizol (Dipyrone), Propiphenazone.
3. Benzoxazocine derivative: Nefopam

What are prostanoids ?
• Subclass of eicosanoids consisting of
1. Prostaglandins Inflammatory and anaphylactic
reactions
2. Thromboxanes Stimulates platelet activation
3. Prostacyclins Inhibits platelet activation

COX - 1
• Expressed in all cells
• Constitutive form
• Serves “house keeping” functions • Vascular haemostasis
• Maintenance of renal & GI blood flow
• Renal function
• Intestinal mucosal proliferation
• Platelet function

COX – 2 • Inducible form
• Induced by cytokines at the site of inflammation
• “As needed” or specialized functions• Inflammation
• Fever
• Pain
• Mitogenesis (GIT)
• Renal adaptation to stress
• Deposition of bone
• Uterine contractions of labor


Aspirin
• Only irreversible acetylator of COX-1 & COX-2

Dose range
• Low (< 300 mg/day) ↓ platelet aggregation
(inhibits TXA2 synthesis)
• Intermediate dose (300-2400 mg/day)
Antipyretic and analgesic effects
• High dose (2400-4000 mg/day) Anti-
inflammatory effect (inhibits TXA2 + PGI2)
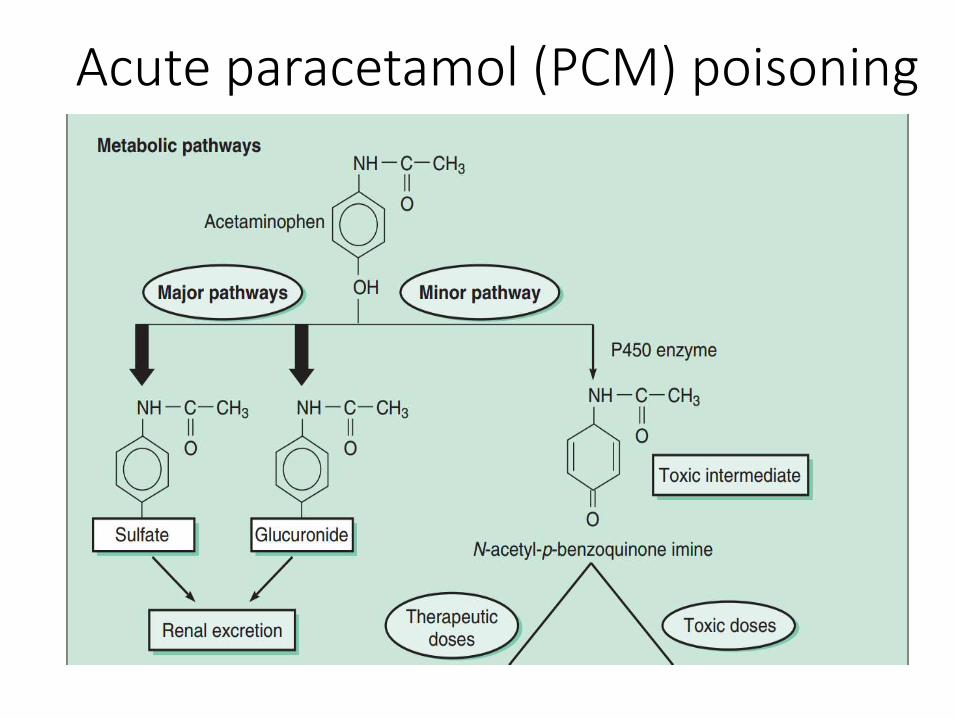
Acute paracetamol (PCM) poisoning


Choice of NSAID
1. Mild-to-moderate pain with little inflammation
PCM
2. Postoperative or similar acute but shortlasting
pain Ibuprofen, diclofenac
3. Acute musculoskeletal, osteoarthritic, injury
associated pain PCM or diclofenac

4. Exacerbation of rheumatoid arthritis, ankylosing
spondylitis, acute gout, acute rheumatic fever
Indomethacin, high dose aspirin
5.Gastric intolerance to traditional NSAIDs
Selective COX-2 inhibitor or paracetamol
6.Arthritis patients on NSAIDs & have PU PPI
7. Paediatric patients PCM
8. Elderly patients Lower dose of chosen NSAID
9. Pregnancy PCM is safest

Review Questions
Q.1. Aspirin is often used in low doses to prevent platelet aggregation by inhibiting the synthesis of which substance?
(A) leukotriene
(B) prostacyclin (prostaglandin I2 [PGI2])
(C) thromboxane A2
(D) arachidonic acid
(E) phospholipase A+

Q.2. Acetaminophen is a potent analgesic and antipyretic NSAID but differs from other agents in that it has no Anti inflammatory action. Which of the following reasons explains this unique aspect of acetaminophen?
(A) the distribution of acetaminophen does not reach peripheral sites of inflammation
(B) acetaminophen it is not an inhibitor of the COX enzyme
(C) antiinflammatory doses of acetaminophen are too high and toxic
(D) it is selective for a newly discovered isozyme of COX
(E) acetaminophen undergoes significant fist-pass
metabolism

Q.3. A 65-year-old lady presented with pain in both knees, more on the left side. The pain is worsened by walking or standing for some time. X-ray of knee shows narrowing of joint space, mild effusion and osteophytic projections. A diagnosis of osteoarthritis of knee is made. She gave history of suffering a heart attack one year back which was treated by angioplasty and a stent was placed. She regularly takes aspirin 75 mg daily for prophylaxis of further myocardial infarction.
(a) Which analgesic/NSAID will be suitable for relieving her knee pain?
(b) Which analgesic/NSAIDs should not be prescribed for her?
(c) Whether any locally applied medication can be helpful in relieving her knee pain?

Q.4. A 64-year-old male presents with mild to moderate
musculoskeletal back pain after playing golf. He states
he has tried acetaminophen and that it did not help. His
past medical history includes diabetes, hypertension,
hyperlipidemia, gastric ulcer (resolved), and coronary
artery disease. Which of the following is the most
appropriate NSAID regimen to treat this patient’s pain?
A. Celecoxib
B. Indomethacin and omeprazole
C. Naproxen and omeprazole
D. Naproxen

Q.5. Among NSAIDs, aspirin is unique because it
(A) Irreversibly inhibits its target enzyme
(B) Prevents episodes of gouty arthritis with long-term use
(C) Reduces fever
(D) Reduces the risk of colon cancer
(E) Selectively inhibits the COX-2 enzyme

Q. 6. Which of the following is an analgesic and antipyretic drug that lacks an anti-inflammatory action?
(A) Acetaminophen
(B) Celecoxib
(C) Colchicine
(D) Indomethacin
(E) Probenecid

Q.7. An 18-month-old boy dies from an accidental overdose of acetaminophen. Which of the following is the most likely cause of this patient’s death?
(A) Arrhythmia
(B) Hemorrhagic stroke
(C) Liver failure
(D) Noncardiogenic pulmonary edema
(E) Ventilatory failure

Q.8. A 54-year-old woman presented with signs and symptoms consistent with an early stage of rheumatoid arthritis. The decision was made to initiate NSAID therapy. Which of the following patient characteristics is the most compelling reason for avoiding Celecoxib in the treatment of her arthritis?
(A) History of alcohol abuse
(B) History of gout
(C) History of myocardial infarction
(D) History of osteoporosis
(E) History of peptic ulcer disease
Q.9. A patient comes in to the emergency department with nausea, vomiting, and tinnitus (high pitched ringing in the ears) and admits to having taken a bottle of aspirin in a suicide attempt (aspirin is a weak acid). Would making the urine more alkaline or more acidic cause the patient to excrete the aspirin more quickly?

Q.10. Aspirin (acetylsalicylic acid) attaches an acetyl group to the cyclooxygenase enzyme of platelets, preventing expression of thromboxane and preventing platelet aggregation—this effect lasts the lifetime of the platelet even when the aspirin is metabolized away. What is the explanation for this?