nuclear medicine techniques for the imaging and treatment ... · nuclear medicine techniques for...
TRANSCRIPT

imaging and treatmen
SUPPLEMENT PAPEREndocrine-Related Cancer (2011) 18 S27–S51
Nuclear medicine techniques for thet of neuroendocrine
tumours
Jaap J M Teunissen1, Dik J Kwekkeboom1, R Valkema1 and Eric P Krenning1,2
Departments of 1Nuclear Medicine and 2Internal Medicine, Erasmus Medical Centre, Rotterdam, The Netherlands
(Correspondence should be addressed to J J M Teunissen; Email: [email protected])
Abstract
Nuclear medicine plays a pivotal role in the imaging and treatment of neuroendocrine tumours(NETs). Somatostatin receptor scintigraphy (SRS) with [111In-DTPA0]octreotide has proven itsrole in the diagnosis and staging of gastroenteropancreatic NETs (GEP-NETs). New techniques insomatostatin receptor imaging include the use of different radiolabelled somatostatin analogueswith higher affinity and different affinity profiles to the somatostatin receptor subtypes. Most ofthese analogues can also be labelled with positron-emitting radionuclides that are being used inpositron emission tomography imaging. The latter imaging modality, especially in the combinationwith computed tomography, is of interest because of encouraging results in terms of improvedimaging quality and detection capabilities. Considerable advances have beenmade in the imagingof NETs, but to find the ideal imaging method with increased sensitivity and better topographiclocalisation of the primary and metastatic disease remains the ultimate goal of research. Thisreview provides an overview of the currently used imaging modalities and ongoing developmentsin the imaging of NETs, with the emphasis on nuclear medicine and puts them in perspective ofclinical practice. The advantage of SRS over other imaging modalities in GEP-NETs is that it canbe used to select patients with sufficient uptake for treatment with radiolabelled somatostatinanalogues. Peptide receptor radionuclide therapy (PRRT) is a promising new tool in themanagement of patients with inoperable or metastasised NETs as it can induce symptomaticimprovement with all Indium-111, Yttrium-90 or Lutetium-177-labelled somatostatin analogues.The results that were obtained with [90Y-DOTA0,Tyr3]octreotide and [177Lu-DOTA0,Tyr3]octreotate are even more encouraging in terms of objective tumour responses with tumourregression and documented prolonged time to progression. In the largest group of patientsreceiving PRRT, treated with [177Lu-DOTA0,Tyr3]octreotate, a survival benefit of several yearscompared with historical controls has been reported.
Endocrine-Related Cancer (2011) 18 S27–S51
Introduction
The first description of the in vivo visualisation of
somatostatin receptor-positive tumours in patients was
based on the use of a radioiodine (123I) labelled
somatostatin analogue (Krenning et al. 1989). In the
years that followed an Indium-111 (111In) labelled
This paper forms part of a special issue of Endocrine-Related
Cancer on neuroendocrine tumours. Novartis Pharmaceuticals
Corporation has supported the publication of this special issue.
Logistical support during development and submission of this
article was provided by Springer Healthcare LLC. This support
was funded by Novartis.
Endocrine-Related Cancer (2011) 18 S27–S51
1351–0088/11/018–S27 q 2011 Society for Endocrinology Printed in Great
somatostatin analogue, chelated with diethylenetria-
minepentaaceticacid (DTPA), was successfully
developed. Subsequently, [111In-DTPA0]octreotide
(OctreoScan, Covidien, Petten, The Netherlands),
was introduced worldwide and became commercially
available. Despite the development of several radio-
labelled somatostatin analogues for scintigraphy,
[111In-DTPA0]octreotide is the only registered radio-
pharmaceutical for somatostatin receptor scintigraphy
(SRS) of gastroenteropancreatic neuroendocrine
tumours (GEP-NETs).
In the last decade, with the increasing use of positron
emission tomography (PET) imaging, somatostatin
Britain
DOI: 10.1530/ERC-10-0282
Online version via http://www.endocrinology-journals.org

J J M Teunissen et al.: Imaging and treatment of NET
analogues have been labelled with various positron-
emitting isotopes, such as Gallium-68 (68Ga) and
Copper-64 (64Cu) (Lewis et al. 1999, Schottelius et al.
2004, Gabriel et al. 2007). Scintigraphy with these
investigational compounds display encouraging good
imaging quality that might result in an improved
sensitivity in tumour site detection compared with
[111In-DTPA0]octreotide scintigraphy. Also, other
PET radiopharmaceuticals were developed, such as18F-dihydroxy-phenyl-alanine (18F-DOPA) and 11C-
labelled 5-hydroxytryptophan (11C-5-HTP) with
encouraging results in terms of visualisation of GEP-
NETs (Koopmans et al. 2008).
After the successful introduction of SRS in the
diagnosis and staging of NETs, the next logical step
was to increase the administered activity so that the
radiopharmaceutical can induce tumour shrinkage in
patients who had inoperable and/or metastasised NETs.
Therefore, the first peptide receptor radionuclide
therapy (PRRT) was performed with high administered
activity of [111In-DTPA0]octreotide (Krenning et al.
1994a). However, besides encouraging results with
regard to symptom relief, the reported number of
objective responses was rather disappointing with
relative low number of patients with tumour shrinkage.
To make significant advancements in the treatment
of somatostatin receptor-positive metastatic disease,
more efficient radiolabelled somatostatin analogues
were developed with higher affinity to the somatostatin
receptor. Also, more stable conjugation with high-
energy b-emitters, such as Yttrium-90 (90Y) and
Lutetium-177 (177Lu), was made possible with the
introduction of the chelator 1,4,7,10-tetraazcyclodode-
cane-1,4,7,10-tetraacetic acid (DOTA). These
developments, together with the introduction of
protective measures to limit the radiation dose to the
kidneys and maximisation of the total cumulative
administered activity respecting the currently inter-
national accepted dose limit to the bone marrow, were
important to make PRRT a valuable therapeutic
modality in the complete arsenal of treatment options
in patients with encouraging results in terms of tumour
shrinkage, quality of life (QoL) and survival.
This review covers the whole spectrum of the imaging
of GEP-NETs with the emphasis on somatostatin
receptor imaging and summarises the results of the
therapeutic options within the field of nuclear medicine.
Imaging
To detect the exact location and subsequent staging
of GEP-NETs, which is crucial for further patient
management, a sensitive imaging modality is important.
S28
Commonly used imaging modalities include conven-
tional radiology (computed tomography (CT), mag-
netic resonance imaging (MRI) and transabdominal
ultrasonography (US)), selective angiography, nuclear
imaging techniques (e.g. somatostatin receptor
imaging) and endoscopic US (EUS). In most patients,
however, more than one modality is needed to gather
enough information to establish the exact localisation
of the often small biochemically active tumours.
Beside the increasing number of interesting new
modalities, modalities are combined to increase the
overall sensitivity and specificity.
Conventional imaging
The exact localisation of the primary tumour in
patients diagnosed with a GEP-NET, especially
gastrinomas and carcinoids of the small intestine, is
often difficult to establish. The detection frequency
with the conventional imaging modalities CT and
MRI in pancreatic NETs is about 22–45%, which is
higher than the reported sensitivity of abdominal US
(13–27%; Modlin et al. 2008). For endoscopic US the
percentages are mostly dependent on suspected tumour
localisation with detection of 45–60% of the duodenal
lesions and 90–100% of the pancreatic lesions
(Anderson et al. 2000).
As most NETs are already metastasised at diagnosis,
imaging of (liver) metastases is important. To visualise
these metastases the use of specific acquisition
protocols for CT and MRI is of vital importance.
Owing to variability of appearance it is recommended
to use a triple-phase (early/late arterial and portal
venous) CT and a multiphasic (arterial, portal venous
and delayed) dynamic and T2 weighted MRI protocol
(Sheth & Fishman 2002). Even when these protocols
are followed, the reported detection rate varies widely.
For identification of metastasised disease, reported
sensitivities of the modalities ranges from 60 to 80%
visualisation with CT, 55–70% for MRI and 14–63%
for US (Sugimoto et al. 1995, Gibril et al. 1996, Gibril
& Jensen 2004, Tamm et al. 2007).
Somatostatin receptor-based radionuclide
imaging
All somatostatin receptor-based radionuclide imaging is
based on the principle of the binding of a radiolabelled
ligand to the somatostatin receptor. Somatostatin
receptors, which are structurally related membrane
glycoproteins, are expressed in various normal tissues,
including central nervous system (CNS), anterior
pituitary, thyroid, pancreas, gastrointestinal tract, spleen
and adrenals (Kwekkeboom et al. 2009).
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
The first report of overexpression of somatostatin
receptors on tumour tissue was published in 1984.
(Reubi & Landolt 1984) High density of somatostatin
receptors on pituitary tumours in acromegaly patients
was demonstrated. Five different subtypes of somato-
statin receptors (sst1–sst5) are currently known and
characterised (Rohrer et al. 1993, Patel & Srikant
1994). However, the expression of the various subtypes
and their density on the tumour cell surface differs
among the various tumours. Reubi et al. (2001), who
used autoradiography to study the sstr subtype profile
of numerous human tumours, reported a predominance
of sst2 and/or somatostatin sst1 in GEP-NETs. The first
report of the in vivo imaging of these NETs expressing
somatostatin receptors with 123I-labelled [Tyr3]octreo-
tide was published in 1989 (Krenning et al. 1989).
However, an important drawback considering routine
use of this compound for scintigraphy was the
relatively high non-receptor-based uptake in the liver
and intestinal uptake, which both can obscure occult
pathology. Therefore, a radiolabelled somatostatin
analogue with better characteristics, [111In-DTPA0]oc-
treotide, was developed. Since then, [111In-DTPA0]oc-
treotide is regarded as the gold standard in nuclear
imaging for patients with GEP-NETs (Krenning et al.
1993). The somatostatin analogue octreotide binds
with high affinity to receptor subtypes 2 and 5. Several
authors demonstrated that a positive [111In-DTPA0]oc-
treotide scintigraphy is mainly due to the sst2, whereas
sst1–sst5 are less important. Therefore, the presence of
sst2 is essential for imaging tumours with SRS (John
et al. 1996, Hofland et al. 2003).
The use of an optimal protocol for [111In-DTPA0]
octreotide scintigraphy in the diagnosis of GEP-NETs
is important to ensure good image quality and per-
formance (Kwekkeboom et al. 2009). The preferred
administered activity of [111In-DTPA0]octreotide (with
at least 10 mg of the peptide) is about 200 MBq.
Besides planar imaging, single photon emission
computed tomography (SPECT) has to be included
because of the increased sensitivity compared with
planar imaging and should, be performed of the upper
abdomen, including the liver, and of other regions with
suspicion of disease. Also, besides increased sensi-
tivity, SPECT imaging allows better anatomical
delineation than planar views. If available, it is
recommended to use hybrid SPECT/CT imaging for
even better anatomical delineation. Timing and
sufficient counts per view are also important acqui-
sition characteristics. Any change in the protocol might
influence the quality and therewith the sensitivity of the
SRS performed. In more detail, these recommen-
dations are available as procedure guidelines for
www.endocrinology-journals.org
somatostatin receptor imaging, published by the
Society of Nuclear Medicine (SNM; Balon et al.
2001). Furthermore, the most important acquisition
protocol recommendations have also been adapted
by the European Association of Nuclear Medicine
(EANM) and European Neuroendocrine Tumour Society
(ENETS; Bombardieri et al. 2010, Kwekkeboom
et al. 2009).
Normal scintigraphic findings with SRS with
[111In-DTPA0]octreotide include visualisation of
thyroid, spleen, liver, kidneys and in a proportion of
patients the adrenals and/or pituitary gland. Also, the
urinary bladder and the bowel are usually visualised to
a variable degree (Krenning et al. 1992, Jacobsson
et al. 2003). The visualisation of the pituitary, thyroid,
adrenals and spleen is due to receptor binding. The
uptake in the kidneys is mainly due to reabsorption of
the radiolabelled somatostatin analogue in the renal
tubular cells after glomerular filtration. Clearance of
the radiopharmaceutical is primarily via the kidneys
and some clearance is via the hepatobiliary pathway.
Because of the latter, the use of laxatives and 48 h
scanning is sometimes necessary to differentiate
between non-specific bowel uptake and somatostatin
receptor-positive abdominal pathology. Also, because
of possible competition between cold octreotide and
radiolabelled octreotide at the receptor site, temporary
discontinuation of the therapeutic use of somatostatin
analogues is recommended before imaging; at least
24 h in case of short-acting somatostatin analogues
and 6 weeks when long-acting forms of somatostatin
analogues are used. Unwanted competition may
negatively affect the sensitivity for the detection of
somatostatin receptor-positive pathological lesions,
and therewith can results in false negatives.
Imaging results of [111In-DTPA0]octreotide
scintigraphy
The sensitivity of somatostatin receptor imaging with
[111In-DTPA0]octreotide scintigraphy for detecting
NETs, including NETs of the pancreas (functioning
and non-functioning) and carcinoids, has been well-
documented. The overall reported sensitivity is high
with 80% to almost 100% sensitivity for carcinoids and
60–90% for pancreatic NETs, mostly depending on
tumour type and lesion size (Krenning et al. 1993,
Kwekkeboom et al. 1993, Westlin et al. 1993, de
Kerviler et al. 1994, Kalkner et al. 1995, Gibril et al.
1996, Zimmer et al. 1996, Lebtahi et al. 1997,
Virgolini et al. 2005).
The sensitivity of histologically or biochemically
proven neuroendocrine pancreatic tumours or
S29

J J M Teunissen et al.: Imaging and treatment of NET
carcinoids was evaluated in a European multi-centre
trial (Krenning et al. 1995). The highest success rates
were observed with glucagonomas (100%), VIPomas
(88%), gastrinomas (72%), non-functioning islet cell
tumours (82%) and carcinoids (87%). These excellent
imaging characteristics have made [111In-DTPA0]oc-
treotide scintigraphy essential in the clinical work-up
of GEP-NETs.
In contrast, the sensitivity to detect insulinomas with
[111In-DTPA0]octreotide scintigraphy is lower than for
most GEP-NETs with a sensitivity of 20–60%
(Krenning et al. 1993, Schillaci et al. 2000, Vezzosi
et al. 2005, de Herder et al. 2006). The variability in
sensitivity may be caused by the low number of patients
included in each study and an inferior scanning
protocol, such as low administered activity or short
acquisition time (Schillaci et al. 2000). Furthermore, in
malignant insulinomas, the expression and density of
somatostatin receptor subtypes is different from benign
insulinomas so that a higher rate of scan positivity with
[111In-DTPA0]octreotide scintigraphy can be expected
in malignant insulinomas (Bertherat et al. 2003). Most
of the reported patients with malignant insulinoma who
had an [111In-DTPA0]octreotide scintigram, demon-
strated uptake in the primary and metastatic lesions
(Bokenkamp et al. 2003, Hirshberg et al. 2005, Vezzosi
et al. 2005, Baldelli et al. 2007). However, the reported
numbers of patients within these studies are to low
to establish a reliable sensitivity of [111In-DTPA0]
octreotide scintigraphy in malignant insulinoma.
Of interest for the detection of insulinomas is the
recently introduced 111In-labelled (Lys40(Ahx-DOTA)
NH2)exendin-4 (111In-DOTA-exendin-4) which
displays a high sensitivity for insulinomas. It targets
specifically the glucagon-like peptide 1 receptor
(GLP1R), which is expressed in very high density in
almost all insulinomas (Christ et al. 2009). Although
the results with this compound are promising, most of
the insulinomas are benign and localised (90%).
Therefore, the need for staging with GLP1R imaging
in the preoperative setting for benign insulinoma
is questionable. Also, because of the already proven
high sensitivity of endoscopic ultrasound (de Geus-Oei
et al. 2002) in these tumours (Zimmer et al. 1996), the
need for this new imaging modality in clinical practice
warrants further studies.
[111In-DTPA0]octreotide scintigraphy versus
conventional imaging
Conventional imaging (including abdominal CT,
US and MRI) if compared with the combination of
planar and SPECT SRS has a lower sensitivity in the
S30
detection of GEP-NETs (Schillaci 2004) However,
with the recently introduced improved techniques in
conventional imaging, such as multi-detector CT
imaging, new MRI sequences and EUS, the accuracy
of these modalities is increasing (Kaltsas et al. 2004).
Unfortunately, studies in which direct comparison of
these improved imaging techniques with SRS are
performed, are limited and the studied population often
small. In one series of ten gastrinoma and ten
insulinoma patients reported sensitivities (per-lesion-
based analysis) for EUS were 79%, 86% for SRS and
29% for the combined conventional imaging of CT, US
and MRI. In the insulinoma patients, eight benign and
two malign, the reported sensitivities were 93% with
EUS, 14% with SRS, 21% with CT and 7% with US
and MRI (Zimmer et al. 1996). In another study by
Gibril et al. (1996), 80 consecutive patients with the
Zollinger–Ellison syndrome had conventional tumour
localisations studies and SRS. SRS localised a primary
gastrinoma in 56% of patients and had greater
sensitivity than any conventional study including
angiography, and was equal in sensitivity to all
conventional imaging studies combined.
[111In-DTPA0]octreotide scintigraphy versus
other radiolabelled somatostatin receptor
analogues
After the successful introduction of [111In-DTPA0]
octreotide scintigraphy developments focused on
new analogues that would have a better affinity profile
with higher sensitivity or a wider somatostatin
receptor subtype affinity profile compared with
[111In-DTPA0]octreotide. Some of the newly
developed 111In-labelled somatostatin analogues use
the macrocyclic chelator DOTA instead of DTPA. The
most important advantage of the use of DOTA is the
stable conjugation with the b-emitting radionuclides
such as 90Y and 177Lu, which are used in PRRT.
DTPA-labelled counterparts are not stable enough
in vivo to be used in a therapeutical setting (de Jong
et al. 2002a). Therefore, in view of selecting patients
for PRRT with diagnostic scintigraphy, the use of the
same (DOTA conjugated) somatostatin analogue is
preferable. Examples of such analogues that are used
in clinical studies include [111In-DOTA]lanreotide
(Virgolini et al. 2002) and [111In-DOTA0]octreotide
(Kwekkeboom et al. 1999, Gabriel et al. 2007).
Furthermore, the somatostatin analogues [111In-DOTA
[1-NaI3]octreotide (111In-DOTANOC; Wild et al.
2003), [111In-DOTA[NaI8Thr8]octreotide (111In-
DOTANOCATE) and [111In-DOTA0,BzThi3,Thr8]
octreotide (111In-DOTABOCATE) demonstrated
www.endocrinology-journals.org

Table 1 111In- and 99mTc-radiolabelled somatostatin analogues compared with [111In-DTPA0]octreotide for scintigraphy
Radioligand (references) Setting
Comparison with
[111In-DTPA0]octreotide Other reported results Comments
[111In-DOTA0,Tyr3]octreotide
(Kwekkeboom
et al. 1999)
Clinical Yes; equal to [111In-DTPA0]
octreotide
Higher background
radioactivity
Scan protocol adequate
[111In-DOTA0,Tyr3]octreotide
(Gabriel et al. 2007)
Clinical Not performed Inferior to
[68Ga-DOTA0,Tyr3]
octreotide
[111In-DOTA]lanreotide
(Virgolini et al. 2002)
Clinical Not performed Inferior to [111In-DOTA0]
octreotide
[111In-DOTA[1-NaI3]
octreotide (Wild et al. 2003)
Preclinical Not performed High affinity to hsst2, 3
and 5
No clinical studies
published
[111In-DOTA[NaI8Thr8]
octreotide (Ginj et al. 2005)
Preclinical Not performed High affinity to hsst2, 3
and 5
No clinical studies
published
Superior to [111In-DOTA0]
octreotide
[111In-DOTA0,BzThi3,Thr8]
octreotide (Ginj et al. 2005)
Preclinical Not performed High affinity to hsst2, 3
and 5
No clinical studies
published
Superior to [111In-DOTA0]
octreotide99mTc-depreotide (Lebtahi
et al. 2002)
Clinical Yes; inferior to [111In-DTPA0]
octreotide
High lung and bone
marrow uptake
Both registered radio-
pharmaceuticals
Scan protocol adequate
[99mTc-EDDA/HYNIC0,Tyr3]
octreotate (Hubalewska-
Dydejczyk et al. 2006)
Clinical Yes; superior to [111In-DTPA0]
octreotide
No 24/48 h p.i. imaging
possible
Scan protocol inadequate
[99mTc-EDDA/HYNIC0,Tyr3]
octreotide (Gabriel et al.
2003)
Clinical Yes; superior to [111In-DTPA0]
octreotide
No 24/48 h p.i.
imaging possible
Scan protocol inadequate
[99mTc-EDDA/HYNIC0,Tyr3]
octreotide (Bangard et al.
2000)
Clinical Yes; equal to [111In-DTPA0]
octreotide: liver lesions
superior to [111In-DTPA0]
octreotide: extrahepatic
No 24/48 h p.i.
imaging possible
Scan protocol inadequate
NA, not applicable; hsst2, human somatostatin receptor subtype 2; p.i., post-injection.
Endocrine-Related Cancer (2011) 18 S27–S51
promising affinity profile characteristics (Table 1; Ginj
et al. 2005). [111In-DOTA]lanreotide is a somatostatin
receptor imaging agent with a slightly different affinity
profile than [111In-DTPA0]octreotide (Reubi et al.
2000). In comparison with [111In-DTPA0]octreotide,
it has a lower sensitivity to demonstrate NETs.
However, the use of [111In-DOTA]lanreotide may
have advantages in other tumours, for instance in
differentiated thyroid carcinoma (Virgolini et al.
2002). In a direct comparison with [111In-DTPA0]oc-
treotide, [111In-DOTA0,Tyr3]octreotide demonstrated
a distribution and excretion pattern that resembled that
of [111In-DTPA0]ctreotide. However, the interstitial
background was higher, which could be disadvanta-
geous in therapy, thereby exposing a higher absorbed
dose to the dose-limiting organs (Kwekkeboom
et al. 1999). Although 111In-DOTANOC, 111In-DO-
TATATE, 111In-DOTANOCATE and 111In-DOTA-
BOCATE are promising analogues in terms of
www.endocrinology-journals.org
biodistribution and receptor affinity profile, in vivo
human studies are scarce.
Besides the various 111In-labelled somatostatin
analogues, metastable Technetium-99 (99mTc) has
been coupled to somatostatin analogues for imaging.
The most important advantages of the use of 99mTc
compared with 99mTc-labelled based somatostatin
analogues includes no expense of producing 111In in
a cyclotron and no need to wait 24–48 h after injection
for optimal detection of tumours. 99mTc-labelled
somatostatin analogues used in a clinical setting
include [99mTc-EDDA–HYNIC-D-Phe1,Tyr3]octreo-
tide (99mTc-HYNIC-TOC; Gabriel et al. 2005, 2007),
[99mTc-EDDA/HYNIC0,Tyr3]octreotate (99mTc-HYNIC-
TATE; Hubalewska-Dydejczyk et al. 2006) and99mTc-Depreotide (Lebtahi et al. 2002). As
[111In-DTPA0]octreotide scintigraphy is regarded as
the gold standard in SRS, several of these new
somatostatin analogues have been compared with
S31

J J M Teunissen et al.: Imaging and treatment of NET
[111In-DTPA0]octreotide in patients with GEP-NETs
(Table 1). Most important advantages in imaging
characteristics compared with [111In-DTPA0]octreo-
tide reported, included superior imaging capabilities of
the extrahepatic lesions, increased sensitivity with
more and new metastases and better individual
separation. However, these results have to be inter-
preted with caution since most of these reported
comparisons did not use the imaging protocols for
[111In-DTPA0]octreotide scintigraphy according to
the international guidelines, including those from the
EANM, ENETS and SNM (Balon et al. 2001,
Kwekkeboom et al. 2009, Bombardieri et al. 2010).
Especially the scanning time and the amount of
radiopharmaceutical injected formulated in these
guidelines are important to obtain an adequate image
with good sensitivity.
In general, the studies with the new 99mTc-labelled
somatostatin analogues show feasibility for imaging.
However, [111In-DTPA0]octreotide scintigraphy,
despite minor disadvantages, still remains the imaging
method of choice in SRS.
Furthermore, these studies illustrate that comparison
between compounds in a clinical setting is difficult
to interpret even in a single centre. To follow the
international guidelines is essential not only to guarantee
optimal acquisition protocols leading to optimal imaging
and diagnostic assessment of the patient, but also in
conducting a valid comparative study.
Imaging results of metaiodobenzylguanidine
scintigraphy
Metaiodobenzylguanidine (MIBG) is an arkyl-guani-
dine derivative, structurally similar to noradrenaline,
which utilises the vesicular monoamine transporters
and is incorporated into vesicles or neurosecretory
granules in the cytoplasm of neureoendocrine cells
(Wafelman et al. 1994). However, it is not significantly
metabolised. MIBG shows little binding to post-
synaptic receptors and causes little or no pharma-
cological response (Sisson & Wieland 1986).123I radiolabelled MIBG has been used for many
years to visualise carcinoid tumours as it is concen-
trated in endocrine cells (Hoefnagel et al. 1987). The
use of radiolabelled MIBG was initially concentrated
on detecting tumours arising from chromaffin cells
such as phaeochromocytomas, paraganglioma and
neuroblastoma with overall reported high sensitivity
of w90% and specificity as high as 99% (Hoefnagel
et al. 1987, Shapiro 1995). Although with lower
sensitivity, MIBG scintigraphy was thereafter utilised
to detect NETs. MIBG scintigraphy in carcinoid
S32
tumours, including the diagnostic scintigraphy with131I-labelled MIBG, has shown lower sensitivity than
the more frequently used [111In-DTPA0]octreotide
scintigraphy. In a review of 10 years experience with
MIBG, including MIBG scintigraphy, a median
detection rate and sensitivity of 50 and 76%,
respectively, was reported (Modlin et al. 2006). In
contrast, the largest review, that included pooled
imaging data from 35 centres with in total more than
1200 patients with carcinoid tumours, [111In-DTPA0]
octreotide scintigraphy demonstrated a higher sensi-
tivity of 84% (57–93%; Modlin et al. 2005).
Furthermore, imaging with 123I-MIBG has a poor
sensitivity in identifying islet cell tumours (Kaltsas
et al. 2001a). Interestingly, within the few studies that
compared 123I-MIBG and [111In-DTPA0]octreotide
scintigraphy in carcinoid tumours, despite the in
general lower uptake of 123I-MIBG, a complementary
role of 123I-MIBG scintigraphy has been noted as either
a different intensity or a different pattern of uptake in
non-octreotide avid regions (Taal et al. 1996a, Kaltsas
et al. 2001a). In one report in which a direct
comparison between these two imaging modalities
was performed, comparable results with sensitivities of
about 84% were demonstrated, whereas the com-
bination of these scans increased the sensitivity to 95%
(Taal et al. 1996a).
Considering these two imaging modalities, it was
concluded that [111In-DTPA0]octreotide scintigraphy
is more sensitive in detecting metastatic lesions from
GEP-NETs than with 123I-MIBG scintigraphy, with the
latter imaging modality useful in the occasional patient
who has MIBG-avid lesions, which do not show up
with the initially performed [111In-DTPA0]octreotide
scintigraphy (Kaltsas et al. 2001b). Also, differential
uptake of 123I-MIBG and [111In-DTPA0]octreotide in
different metastases within one subject has been
reported and may be important in view of further
clinical management (Quigley et al. 2005).
Imaging results of PET
PET using 18F-fluorodeoxyglucose (18F-FDG) is a
powerful functional modality for oncological imaging,
especially in tumours with high proliferative activity
and low differentiation grade. Unfortunately, since
most GEP-NETs are well-differentiated, 18F-FDG is
not accumulated in GEP-NETs except in the case of
less differentiated tumours with high proliferative
activity (Adams et al. 1998). Therefore, in general, it
is not used as the initial imaging modality in the early
diagnostic phase. However, a recently published study
reported a negative correlation of 18F-FDG uptake and
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
the prognosis of the disease (Binderup et al. 2010a).
Furthermore, in a recent study by the same group, the
combination of [111In-DTPA0]octreotide scintigraphy
and 18F-FDG PET yielded an overall sensitivity of 96%
compared with 89% with [111In-DTPA0]octreotide
scintigraphy alone, indicating that 18F-FDG PET
provides complementary diagnostic information
(Binderup et al. 2010b). 18F-FDG PET was especially
of value in GEP-NET patients with negative
[111In-DTPA0]octreotide scintigraphy or a high
proliferation index (Ki-67O15%). Also, in pathology
proven NETs that do not visualise on somatostatin
receptor imaging, it is recommended to perform
FDG-PET in staging, since these tumours show often
more aggressive behaviour and faster growth. (Belho-
cine et al. 2002).
Other PET radiopharmaceuticals are also used to
visualise these relatively slow growing tumours. In line
with the commonly used [111In-DTPA0]octreotide
scintigraphy, somatostatin analogues labelled with a
positron-emitting radionuclide are the most obvious
radiopharmaceuticals to use for imaging.
Currently, several 68Ga labelled somatostatin
analogues have been evaluated. 68Ga is a generator-
produced radionuclide that can be chelated with DOTA
to form a stable complex with somatostatin analogues.
[68Ga-DOTA0,Tyr3]octreotide (68Ga-DOTATOC) was
the first 68Ga-labelled somatostatin analogue that was
studied in patients. The results were promising
(Hofmann et al. 2001, Maecke et al. 2005, Gabriel
et al. 2007). Consequently, other clinically applicable68Ga-labelled somatostatin analogues were developed
to increase their sensitivity or widen their affinity
profile, including 68Ga-DOTANOC (Wild et al. 2005,
Ambrosini et al. 2008, Fanti et al. 2008, Krausz et al.
Table 2 Results of 68Ga labelled positron emission tomography liga
Radioligand (references) Compared with
[68Ga-DOTA0,Tyr3]octreotide
(Hofmann et al. 2001)
[111In-DTPA0]octreotide
[68Ga-DOTA0,Tyr3]octreotide
(Buchmann et al. 2007)
[111In-DTPA0]octreotide
[68Ga-DOTA,1-nal3]octreotide
(Fanti et al. 2008)
CT
[68Ga-DOTA,1-nal3]octreotide
(Ambrosini et al. 2008)
18F-DOPA
[68Ga-DOTA,1-nal3]octreotide
(Wild et al. 2005)
[111In-DOTA0]octreotide
[68Ga-DOTA0,Tyr3]octreotate
(Kayani et al. 2008)
18F-FDG
[68Ga-DOTA,1-nal3]octreotide
(Krausz et al. 2010)
[111In-DTPA0]octreotide
www.endocrinology-journals.org
2010) and [68Ga-DOTA0,Tyr3]octreotate (68Ga-
DOTATATE; Kayani et al. 2008).
All these positron-emitting radionuclide labelled
somatostatin analogues share the excellent image
quality with better spatial resolution compared with
the imaging with the g-emitting analogues. Compari-
son of 68Ga-labelled somatostatin analogues with
[111In-DTPA0]octreotide scintigraphy and other
imaging modalities has been performed in several
studies (Table 2; Hofmann et al. 2001, Buchmann et al.
2007, Ambrosini et al. 2008, Fanti et al. 2008, Krausz
et al. 2010). Unfortunately, however, inadequate
protocols for [111In-DTPA0]octreotide scintigraphy
were used in many studies and therefore the
comparison often inappropriate.
In clinical practice, PET imaging with the 68Ga-
labelled somatostatin analogues has some more
advantages compared with [111In-DTPA0]octreotide
scintigraphy besides the already mentioned higher
spatial resolution with excellent image quality. These
advantages include the easy accessibility and avail-
ability of the 68Ga generator, favourable acquisition
protocol, with relative short scanning time, and low
radiation exposure to the patient (Krausz et al. 2010). It
is likely that, if available, PET/CT with 68Ga-labelled
somatostatin analogues will become the image
modality to be used for SRS in the future.
Also in SRS with the use of 68Ga-labelled
somatostatin analogues in GEP-NET patients,18F-FDG PET might have its place in the diagnostic
work up with an increased overall sensitivity of 92%
with the combination of 68Ga-DOTATATE PET/CT
and 18F-FDG PET/CT especially in intermediate- and
high-grade NET (Kayani et al. 2008).
nds in clinical imaging compared with other imaging modalities
Reported results Comments
Superior Scan protocol [111In-DTPA0]
octreotide inadequate
Superior to SPECT Scan protocol [111In-DTPA0]
octreotide inadequate
Useful additional information No comparison with other
radioligands
Superior
Superior Case report
Superior: low-grade tumours
Inferior: high/intermediate-
grade tumours
Comparable, if not superior
S33
J J M Teunissen et al.: Imaging and treatment of NET
Besides, the 68Ga-labelled somatostatin analogues,
a glycosylated 18F-labelled somatostatin analogue,
Na-(1-deoxy-D-fructosyl)-N3-(2-[18F]fluoropropionyl)-
Lys0-Tyr3-octreotate (Gluc-Lys([18F]FP)-TOCA),
has been introduced for PET with a diagnostic
performance superior to [111In-DTPA0]octreotide
scintigraphy and probably comparable with 68Ga-
DOTATOC (Meisetschlager et al. 2006). However,
the preparation of Gluc-Lys([18F]FP)-TOCA requires a
time-consuming multistep synthesis that will probably
hamper its future clinical use.
Other interesting, not somatostatin analogue-based,
PET imaging agents in GEP-NETs include 18F-DOPA
and 11C-5-HTP.
PET with 18F-DOPA is based on the fact that DOPA
is a catecholamine precursor, which is taken up by
neuroendocrine cells (Becherer et al. 2004), whereas
5-HTP is a direct precursor for the serotonin pathway
and therefore a potentially sensitive universal method
for NET detection (Orlefors et al. 2005).
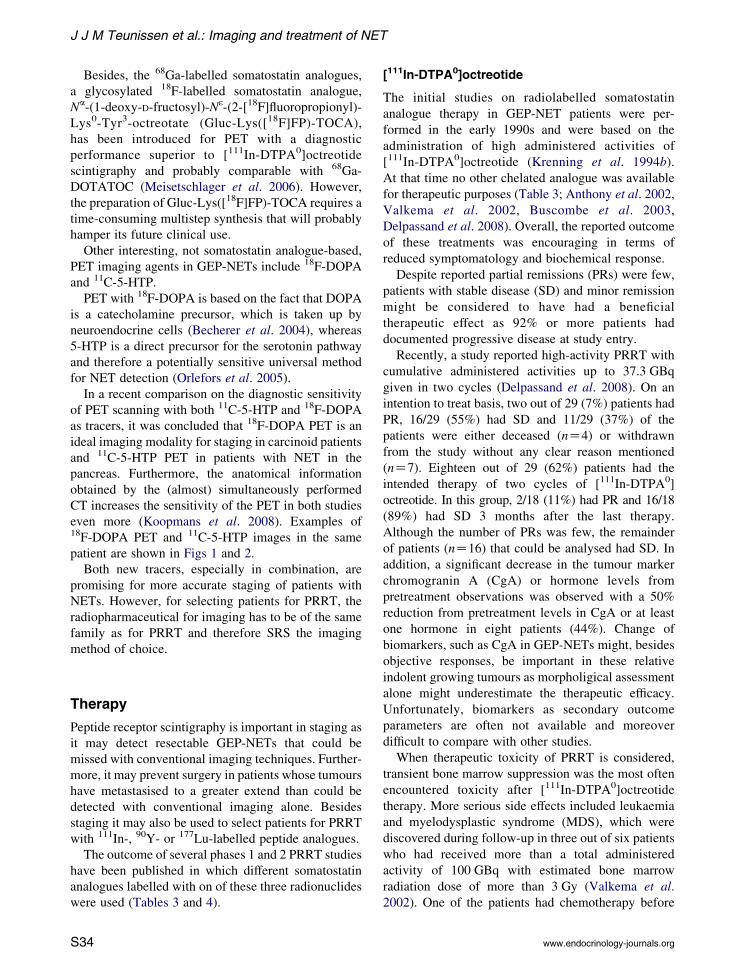
In a recent comparison on the diagnostic sensitivity
of PET scanning with both 11C-5-HTP and 18F-DOPA
as tracers, it was concluded that 18F-DOPA PET is an
ideal imaging modality for staging in carcinoid patients
and 11C-5-HTP PET in patients with NET in the
pancreas. Furthermore, the anatomical information
obtained by the (almost) simultaneously performed
CT increases the sensitivity of the PET in both studies
even more (Koopmans et al. 2008). Examples of18F-DOPA PET and 11C-5-HTP images in the same
patient are shown in Figs 1 and 2.
Both new tracers, especially in combination, are
promising for more accurate staging of patients with
NETs. However, for selecting patients for PRRT, the
radiopharmaceutical for imaging has to be of the same
family as for PRRT and therefore SRS the imaging
method of choice.
Therapy
Peptide receptor scintigraphy is important in staging as
it may detect resectable GEP-NETs that could be
missed with conventional imaging techniques. Further-
more, it may prevent surgery in patients whose tumours
have metastasised to a greater extend than could be
detected with conventional imaging alone. Besides
staging it may also be used to select patients for PRRT
with 111In-, 90Y- or 177Lu-labelled peptide analogues.
The outcome of several phases 1 and 2 PRRT studies
have been published in which different somatostatin
analogues labelled with on of these three radionuclides
were used (Tables 3 and 4).
S34
[111In-DTPA0]octreotide
The initial studies on radiolabelled somatostatin
analogue therapy in GEP-NET patients were per-
formed in the early 1990s and were based on the
administration of high administered activities of
[111In-DTPA0]octreotide (Krenning et al. 1994b).
At that time no other chelated analogue was available
for therapeutic purposes (Table 3; Anthony et al. 2002,
Valkema et al. 2002, Buscombe et al. 2003,
Delpassand et al. 2008). Overall, the reported outcome
of these treatments was encouraging in terms of
reduced symptomatology and biochemical response.
Despite reported partial remissions (PRs) were few,
patients with stable disease (SD) and minor remission
might be considered to have had a beneficial
therapeutic effect as 92% or more patients had
documented progressive disease at study entry.
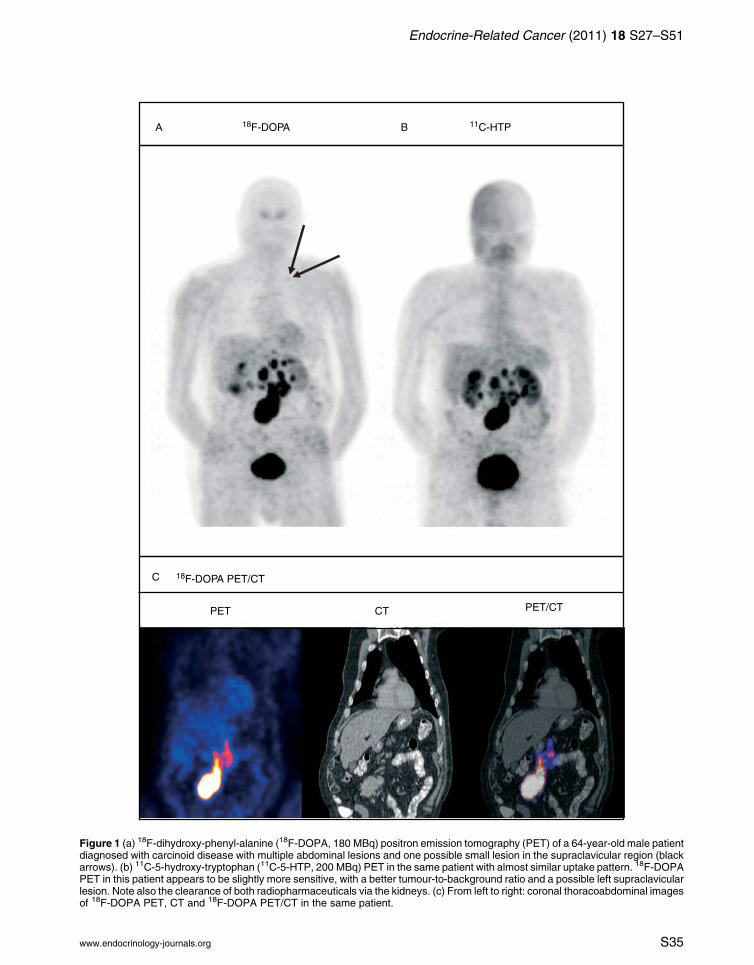
Recently, a study reported high-activity PRRT with
cumulative administered activities up to 37.3 GBq
given in two cycles (Delpassand et al. 2008). On an
intention to treat basis, two out of 29 (7%) patients had
PR, 16/29 (55%) had SD and 11/29 (37%) of the
patients were either deceased (nZ4) or withdrawn
from the study without any clear reason mentioned
(nZ7). Eighteen out of 29 (62%) patients had the
intended therapy of two cycles of [111In-DTPA0]
octreotide. In this group, 2/18 (11%) had PR and 16/18
(89%) had SD 3 months after the last therapy.
Although the number of PRs was few, the remainder
of patients (nZ16) that could be analysed had SD. In
addition, a significant decrease in the tumour marker
chromogranin A (CgA) or hormone levels from
pretreatment observations was observed with a 50%
reduction from pretreatment levels in CgA or at least
one hormone in eight patients (44%). Change of
biomarkers, such as CgA in GEP-NETs might, besides
objective responses, be important in these relative
indolent growing tumours as morpholigical assessment
alone might underestimate the therapeutic efficacy.
Unfortunately, biomarkers as secondary outcome
parameters are often not available and moreover
difficult to compare with other studies.
When therapeutic toxicity of PRRT is considered,
transient bone marrow suppression was the most often
encountered toxicity after [111In-DTPA0]octreotide
therapy. More serious side effects included leukaemia
and myelodysplastic syndrome (MDS), which were
discovered during follow-up in three out of six patients
who had received more than a total administered
activity of 100 GBq with estimated bone marrow
radiation dose of more than 3 Gy (Valkema et al.
2002). One of the patients had chemotherapy before
www.endocrinology-journals.org
A B18F-DOPA 11C-HTP
C 18F-DOPA PET/CT
PET CT PET/CT
Figure 1 (a) 18F-dihydroxy-phenyl-alanine (18F-DOPA, 180 MBq) positron emission tomography (PET) of a 64-year-old male patientdiagnosed with carcinoid disease with multiple abdominal lesions and one possible small lesion in the supraclavicular region (blackarrows). (b) 11C-5-hydroxy-tryptophan (11C-5-HTP, 200 MBq) PET in the same patient with almost similar uptake pattern. 18F-DOPAPET in this patient appears to be slightly more sensitive, with a better tumour-to-background ratio and a possible left supraclavicularlesion. Note also the clearance of both radiopharmaceuticals via the kidneys. (c) From left to right: coronal thoracoabdominal imagesof 18F-DOPA PET, CT and 18F-DOPA PET/CT in the same patient.
Endocrine-Related Cancer (2011) 18 S27–S51
www.endocrinology-journals.org S35

A B18F-DOPA 11C-HTP
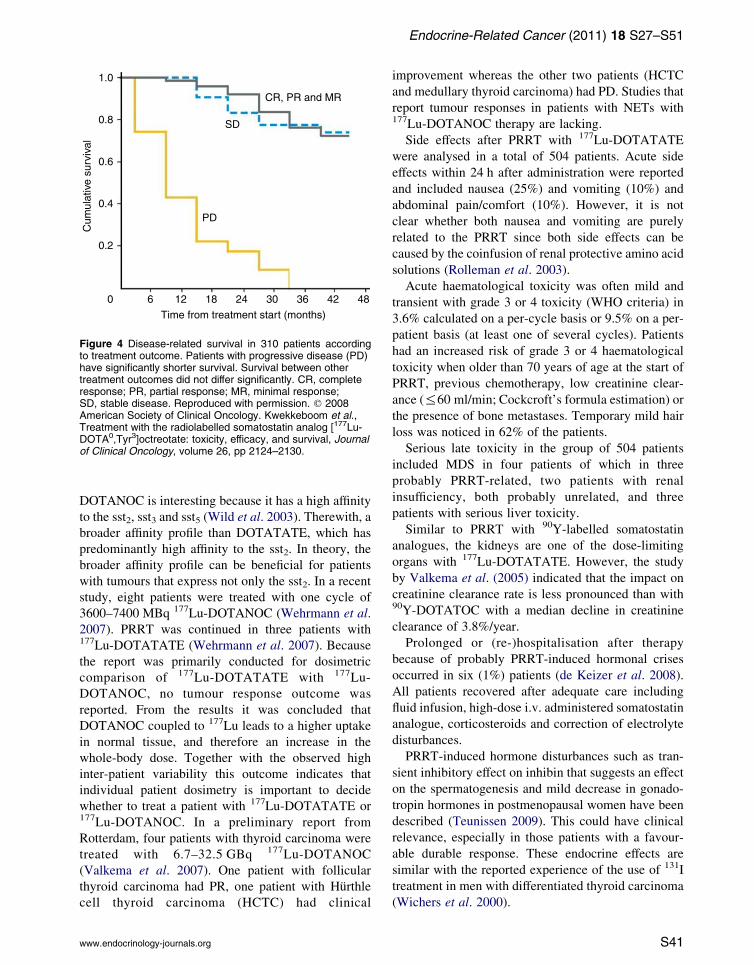
Figure 2 (a) 18F-dihydroxy-phenyl-alanine (18F-DOPA) positron emission tomography (PET) of a 56-year-old female patientdiagnosed with an endocrine tumour of the pancreas extending towards the spleen with liver metastases. Note the knownphysiological uptake in the gallbladder (Balan 2005). (b) 11C-5-hydroxy-tryptophan (11C-5-HTP) PET in the same patient indicatingmore tumour mass and a higher number of liver metastasis in comparison with the 18F-DOPA PET. Note also the clearance of bothradiopharmaceuticals via the kidneys.
J J M Teunissen et al.: Imaging and treatment of NET
[111In-DTPA0]octreotide therapy, which could have
contributed or caused this severe complication.
Renal insufficiency was reported by Anthony et al.
(2002) in one patient and was probably related to
retroperitoneal fibrosis already present before therapy.
Three patients with tumour replacement of more than
75% of their hepatic parenchyma and with treatment-
associated necrosis on CT experienced transient grade
4 hepatic toxicity.
From the clinical studies with [111In-DTPA0]
octreotide, it can be concluded that [111In-DTPA0]
octreotide therapy is not the ideal radiolabelled peptide
for PRRT, at least not for metastatic GEP-NETs.
Experimental data in rats have shown that high
absorbed doses of [111In-DTPA0]octreotide can inhibit
the growth of liver metastases after injection of
somatostatin receptor sst2 tumour cells into the portal
vein. Therefore, 111In-based PRRT might be effica-
cious in the treatment of micro-metastases or in the
prevention of metastatic spread during initial surgery
(Slooter et al. 1999). However, clinical studies that
confirm these preclinical observations are lacking.
S36
90Y-labelled somatostatin analogues
The next generation of radiolabelled somatostatin
analogues was coupled to the b-emitting radionuclide 90Y.
DOTA-chelated somatosatin analogues were used for
more stable conjugation of analogue and radionuclide.
The different somatostatin analogues have different
affinities for the somatostatin receptor subtypes, which
can have accounted for the difference in reported
outcome as is shown in Table 4. However, since no
randomised trial has been performed, other differences,
such as used protocol, selected patient population and
the total administered activity, could have been
reponsible for the observed differences. In a small
group of patients, Otte et al. (1998). Reported two PRs
out of ten patients with somatostatin receptor-positive
tumours treated with [90Y-DOTA0,Tyr3]octreotide
(90Y-DOTATOC), whereas six patients had SD. In
the studies that followed, response rates (complete
response (CR) and PR) in patients with GEP-NETs,
who were either treated with upto 6.0 GBq/m2 (dose-
escalating study of four cycles) or 7.4 GBq/m2, were
10/37 (27%) and 8/37 (22%) respectively (Waldherr
www.endocrinology-journals.org
Table
3PRRTwith[111In-D
TPA0]octreotidein
patients
withgastroenteropancreaticneuroendocrinetumours
References
No.of
evaluable
patients
Progressivedisease
before
PRRT
Cumulativeactivity
(GBq)
Response
PR
MRa
SD
PD
Criteriab
Valkemaetal.(2002)
26
24/26(92%)(clinicaland/or
imagingbased)
4.7–160.0
02(8%)
15(58%)
9(35%)
SWOG
Anthonyetal.(2002)
26
100%
(clinicaland/or
imagingbased)
6.7–46.6
2(8%)
N/I
21(81%)
3(11%)
WHO
Buscombeetal.(2003)
12
100%
(biochemicalor
imagingbased)
3.1–36.6
2(17%)
N/I
7(58%)
3(25%)
RECIST
Delpassandetal.(2008)
29
100%
(imagingbased)
35.3–37.3
2(7%)
N/I
16/29(55%)
11/29(38%)c
RECIST
PRRT,peptidereceptorradionuclidetherapy;cumulativeactivity,totaladministeredactivityof[111In-D
TPA0]octreotide;N/I,notindicated.
aModificationofSouthwestOncologyGroup(SWOG)criteriaincludingMR
(minorremission),between25and50%
reductionoftumoursize.
bCriteriaoftumourresponse:S
WOG:P
R(partialremission),R
30%
reductionoftumoursize;M
R(m
inorremission),30%
reductionorincrease
ofS
D(stabledisease
),!30%
reductio
norincreaseof!
20%
oftumoursize;PD(progressivedisease),R
20%
increaseoftumoursizeornewlesion(s).WHO:PR,R50%
reductionoftumoursize;SD,!50%
reductionor
increaseof!25%
oftumoursize;PD,R
25%
increase
oftumoursizeornewlesion(s).Responseevaluationcriteriain
solid
tumours
(RECIST):PR,R
50%
reductio
noftumoursize;
SD,!25%
reductionorincreaseoftumoursize;PD,O
50%
increaseoftumoursize.
cFourpatients
deceasedbefore
theseco
ndcycle
given,seve
npatients
were
withdrawnfrom
thestudywithoutanyreasonmentioned.
Endocrine-Related Cancer (2011) 18 S27–S51
www.endocrinology-journals.org
et al. 2001, 2002a). In a preliminary subsequent
study the same total administered activity of
7.4 GBq/m2 was given in two cycles to determine
whether a decrease in the number of treatments could
increase PRRT efficacy in terms of objective responses
(Waldherr et al. 2002b). Twelve out of 35 patients
(34%) had CR or PR, which indicated a higher
percentage of tumour regression. No increase in side
effects was reported. Unfortunately, published random-
ised clinical studies to indicate a therapeutic benefit of
less cycles in PRRT are lacking.
Reported clinical studies of PRRT from Milan,
also used the radiolabelled somatostatin analogue90Y-DOTATOC to treat patients with various somato-
statin receptor-positive tumours (Paganelli et al.
2001, 2002, Chinol et al. 2002, Bodei et al. 2003,
2004). Objective tumour responses, including CR and
PR varied from 26 to 29%. Unfortunately, a clear
description of the tumour response in relation to a
specific tumour type on a per-patient basis was not
always given. Instead, it was reported that most of
the patients who had a favourable outcome, had
GEP-NETs.
In a multi-centre (Rotterdam, The Netherlands;
Brussels, Belgium; Tampa, USA) dose escalation
phase I study, also with 90Y-DOTATOC, escalating
administered activities up to 14.8 GBq/m2 in four
cycles or up to 9.3 GBq/m2 in a single cycle were given
to a total of 58 GEP-NET patients (Valkema et al.
2006). The maximum tolerated single dose was not
reached. The total administered activity was limited
according to a maximum estimated dose of 27 Gy to
the kidneys. Furthermore, concomitantly with the
therapy, an amino acid (lysine 2.5%/arginine 2.5%)
solution was administered for kidney protection. Five
out of 55 (9%) evaluable patients had PR, seven (13%)
had minimal response (MR) and 29 (53%) had SD.
Although a detailed QoL assessment was not
performed, 21 of the 36 patients (58%) had improve-
ment in Karnofsky performance score (KPS) or
symptoms.
In a recently published study, 90 GEP-NET patients
were treated with a fixed dose regimen of three cycles
of 4.4 GBq 90Y-DOTATOC (90Y-edotreotide, Onalta,
Molecular Insight Pharmaceuticals, Cambridge, MA,
USA; Bushnell et al. 2010). The maximum cumulative
administered activity of 13.3 GBq was chosen as it is
regarded as both safe and effective (Smith et al. 2000,
Valkema et al. 2006). Four out of 90 (4%) evaluable
patients had PR and 63 (70%) had SD. Median
progression-free survival was 16.3 months. The
number of patients who had PR and SD is comparable
with the results of the second largest (multi-centre)
S37

Table 4 Peptide receptor radionuclide therapy clinical trials with 90Y- or 177Lu-labelled somatostatin analogues in patients with
gastroenteropancreatic neuroendocrine tumours
References
No. of
evaluable
patients
Progression at
inclusion (%)
Reported response
CR PR MRa SD PD CRCPR Criteriab
[90Y-DOTA0,Tyr3]octreotide
Otte et al. (1999) 16 N/I 0 1 (6%) N/I 14 (88%) 1 (6%) 1/16 (6%) N/I
Waldherr et al. (2001) 37 84 1 (3%) 9 (24%) N/I 23 (62%) 4 (11%) 10/37 (27%) WHO
Waldherr et al. (2002a) 37 100 1 (3%) 7 (19%) N/I 6 (70%) 3 (8%) 8/37 (22%) WHO
Waldherr et al. (2002b) 36 100 2 (6%) 10 (28%) N/I 19 (54%) 4 (12%) 12/35 (34%) WHO
Bodei et al. (2003) 21 N/I 0 6 (29%) N/I 11 (52%) 4 (19%) 6/21 (29%) WHO
Valkema et al. (2006) 58 81 0 5 (9%) 7 (13%) 29 (53%) 14 (25%) 5/58 (9%) SWOG
Bushnell et al. (2010) 90 100 0 4 (4%) N/I 63 (70%) 23 (26%) 4/90 (4%) SWOG
[90Y-DOTA]lanreotide
Virgolini et al. (2002) 39 100 0 0 8 (20%) 17 (44%) 14 (36%) 0/39 (0%) WHO
[90Y-DOTA0,Tyr3]octreotate
Baum et al. (2004) 75 89 0 28 (37%) N/I 39 (52%) 8 (11%) 28/75 (37%) N/I
[177Lu-DOTA0,Tyr3]octreotate
Kwekkeboomet al. (2008) 310 38 5 (2%) 86 (28%) 51 (16%) 107 (35%) 61 (20%) 91/310 (29%) SWOG
Garkavij et al. (2010) 12 N/I 0 2 (17%) 3 (25%) 5 (50%) 2 (17%) 2/12 (17%) RECIST
N/I, not indicated or not specified to the number of evaluable patients.aModification of the Southwest Oncology Group (SWOG) criteria including MR (minor remission), between 25 and 50% reduction oftumour size.bCriteria of tumour response: SWOG: PR (partial remission),R30% reduction of tumour size; MR (minor remission), 30% reductionor increase of SD (stable disease),!30% reduction or increase of!20% of tumour size; PD (progressive disease),R20% increaseof tumour size or new lesion(s), measurements: bidimensional. WHO: PR,R50% reduction of tumour size; SD,!50% reduction orincrease of !25% of tumour size; PD, R25% increase of tumour size or new lesion(s), measurements: bidimensional. Responseevaluation criteria in solid tumours (RECIST): PR,R50% reduction of tumour size; SD,!25% reduction or increase of tumour size;PD, O50% increase of tumour size, measurements: unidimensional.
J J M Teunissen et al.: Imaging and treatment of NET
PRRT phase I study with 90Y-DOTATOC (Valkema
et al. 2006). Furthermore, in this study, a subgroup
analysis of 19 patients who received a cumulative
activity between 9.9 and 13.3 GBq 90Y-DOTATOC
was performed to mimic the cumulative activity
administered in the phase II studies. Median overall
survival (OS) in these 19 patients was 21.3 months,
which is in line with the reported OS of 26.9 months in
the larger group of 90 patients (Bushnell et al. 2010).
Also clinically used, is the 90Y-labelled somatostatin
analogue [DOTA0,Tyr3]octreotate (DOTATATE).
DOTATATE is formed by replacing the C-terminal
threoninol in DOTATOC with threonine. This small
change of molecular structure improved the binding
to somatostatin receptor-positive tissues in animals
(de Jong et al. 1998). Furthermore, a ninefold increase
in affinity for the sst2 for DOTATATE if compared
with DOTATOC was reported (Reubi et al. 2000).
After coupling of Yttrium to both analogues, an almost
sevenfold increase was preserved.
Preliminary results of the therapeutic efficacy of90Y-DOTATATE in patients with somatostatin
receptor-positive tumours was reported by Baum
et al. (2004) Twenty-eight out of 75 (37%) patients
had PR and 39/75 (52%) had SD after therapy.
Therefore, 90Y-DOTATATE might also be a promis-
ing 90Y-labelled somatostatin analogue. In analogy
S38
with [111In-DTPA0]octreotide therapy, transient, but
mild bone marrow suppression was the most often
observed side effect in patients treated 90Y-labelled
somatostatin analogues. Acute grades 3 and 4
haematologic toxicity was observed for platelets in
3–12% of the patients, 1–7% for haemoglobulin and
2–7% for white blood cells (Otte et al. 1999, Waldherr
et al. 2002a, Bodei et al. 2003, Valkema et al. 2006)
The latter toxicity has recently been addressed in
a study by Sierra et al. (2009) in which it was
concluded that the toxicity regarding the lymphocytic
subpopulation is mainly directed to the B-cell
subpopulation.
Despite the current use of kidney protection which
consists of coinfusion of an amino acid solution during
PRRT, the kidneys are often found to be dose-limiting.
Especially in patients treated with 90Y based somato-
statin analogues with and without kidney protection
renal toxicity has been reported in a limited number
of patients.
In an intra-patient dose-escalating study renal
toxicity was seen in four out of 29 (14%) treated
patients after administration of cumulative activities of
7.6–8.9 GBq/m2 90Y-DOTATOC (Otte et al. 1999).
None of these four patients received coinfusion of an
amino acid solution during and after PRRT. Two
of them needed haemodialysis treatment. No renal
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
toxicity was observed in the other patients who
received a maximum of administered cumulative
activity of 7.4 GBq/m2. A cumulative administered
activity of 7.5 GBq/m2 was, therefore, suggested to
be dose-limiting for the kidneys in PRRT with90Y-DOTATOC. However, a case report of a patient
treated with 5.6 GBq/m2 90Y-DOTATOC, who
developed end-stage renal disease, suggests that this
limit is not completely reliable to exclude renal toxicity
(Cybulla et al. 2001).
In a more detailed study focusing on renal function,
28 patients who had a cumulative radiation dose to the
kidneys up to 38.7 Gy and a median follow-up 2.9
years, had a median decline of creatinine clearance of
7.3%/year (Valkema et al. 2005). Furthermore, a
decline of O15% was reported in a subgroup of nine
patients of which five had hypertension and/or
diabetes. In this and another study by Bodei et al.
(2008), it was concluded that cumulative renal
radiation dose, per-cycle renal radiation dose, age,
hypertension and diabetes are probable contributing
factors responsible for the high rate of decline in
creatinine clearance after PRRT demonstrated in a
subgroup of patients.
All the clinical trials with 90Y-labelled somatostatin
analogues, despite the differences in analogues and
protocols used, report favourable outcome in terms of
percentages of patients with complete or PR ranging up
to 37% (Table 4) and, therefore, compare favourably
with [111In-DTPA0]octreotide based PRRT. Further-
more, survival data are encouraging in terms of a
longer documented OS. In the multi-centre study
comprising a group of 58 patients treated with90Y-DOTATOC, the OS compared favourably
with a historical group of patients treated with
[111In-DTPA0]octreotide with a median time of
survival of 3 years (versus 12 months; Valkema et al.
2002, 2006). Limitation of this comparison is the fact
that both were separate phase I studies and thus without
randomisation. However, the observed difference in
median survival can probably not be solely explained
by this.
177Lu-labelled somatostatin analogues
In preclinical studies by de Jong et al. (2002b),
different radiolabelled somatostatin analogues were
evaluated for future clinical therapeutic use. Besides
[111In-DTPA0]octreotide and 90Y-DOTATOC, the
b-emitting radionuclide 177Lu coupled to DOTATATE
(177Lu-DOTATATE) was used. 177Lu-DOTATATE
demonstrated the highest tumour uptake together
with excellent tumour-to-kidney ratios compared
www.endocrinology-journals.org
with [111In-DTPA0]octreotide and 90Y-DOTATOC.
Furthermore, in a clinical study by Esser et al. (2006)
was compared with 177Lu-DOTATOC in a thera-
peutical setting. A mean residence time ratio of 2.1 in
favour of 177Lu-DOTATATE for PRRT was reported.
Therefore, in our view for GEP-NETs 177Lu-
DOTATATE is the radiolabelled somatostatin
analogue of choice for PRRT.
The first reports on the results of the clinical use of177Lu-DOTATATE were promising with CR and PR
in 30%, MR in 12% and SD in 40% of the treated
GEP-NET patients (Kwekkeboom et al. 2003a). In a
more recent analysis these results were confirmed in a
large group of a total of 310 GEP-NET patients
(Kwekkeboom et al. 2008). Patients were treated up to
a total administered activity of 27.8–29.6 GBq, usually
in four treatment cycles, with treatment intervals of
6–10 weeks. Complete and partial tumour remissions
occurred in 2 and 28% of patients respectively. Factors
predictive of a favourable response with tumour
shrinkage (CR, MR and PR) were high uptake on
pre-PRRT [111In-DTPA0]octreotide scintigraphy and a
KPS higher than 70. Interestingly, a reduced tumour
uptake after the third or fourth treatment in comparison
with the scan after the first treatment was frequently
seen in patients who eventually had a tumour
regression during follow-up (Kwekkeboom et al.
2005). This phenomenon is illustrated in Fig. 3. In
line with these observations on post-PRRT scintigra-
phy, similar results of reduced somatostatin receptor
mediated uptake after PRRT was recently published by
Haug et al. (2010). In their study, decreased68Ga-DOTATATE uptake in tumours after the first
cycle of PRRT predicted the time to progression (TTP)
after completion of PRRT (one, two or three cycles)
and was correlated with improvement in clinical
symptoms. Most obvious cause of the observed
decrease in uptake is a decreased amount of viable
somatostatin receptor-expressing tumour cells and
thereby reflecting the cytotoxic therapeutic effect of
PRRT. Other suggested causes included the induction
of dedifferentiating of NET cells within the tumour as
somatostatin expression depends on the grade of
differentiation of NET (Miederer et al. 2009).
However, dedifferentiation is less likely because the
observed favourable effect on tumour response, TTP
and clinical symptoms in tumours with reduced uptake
in the tumours after PRRT. Also, the effect of PRRT on
receptor expression and density on a single tumour cell
is not know and has to be elucidated in further studies.
Four patients who were judged inoperable by the
surgeon, became operable after adequate reduction of
tumour mass, 6–12 months after PRRT. Three of these
S39

A Anterior Posterior
Cycle 3
Cycle 2
Cycle 1
Cycle 4
B Pre-PRRT Post-PRRT
Figure 3 (a) Posttherapy scans (anterior/posterior, abdominal spot view images) after each cycle of PRRT with 7400 MBq[177Lu-DOTA0,Tyr3]octreotate (top to bottom row indicates the first to last cycle) in a patient with rectal carcinoid with metastases whoeventually had partial remission as tumour outcome. Note the decrease of uptake in the liver lesions compared to physiological liveruptake with every post-therapy scan. (b) CT of the abdomen of the same patient before (left panel) and 3 months after (right panel)the last cycle.
J J M Teunissen et al.: Imaging and treatment of NET
patients were succesfully operated upon, whereas one
died of unfortunate postoperative complications.
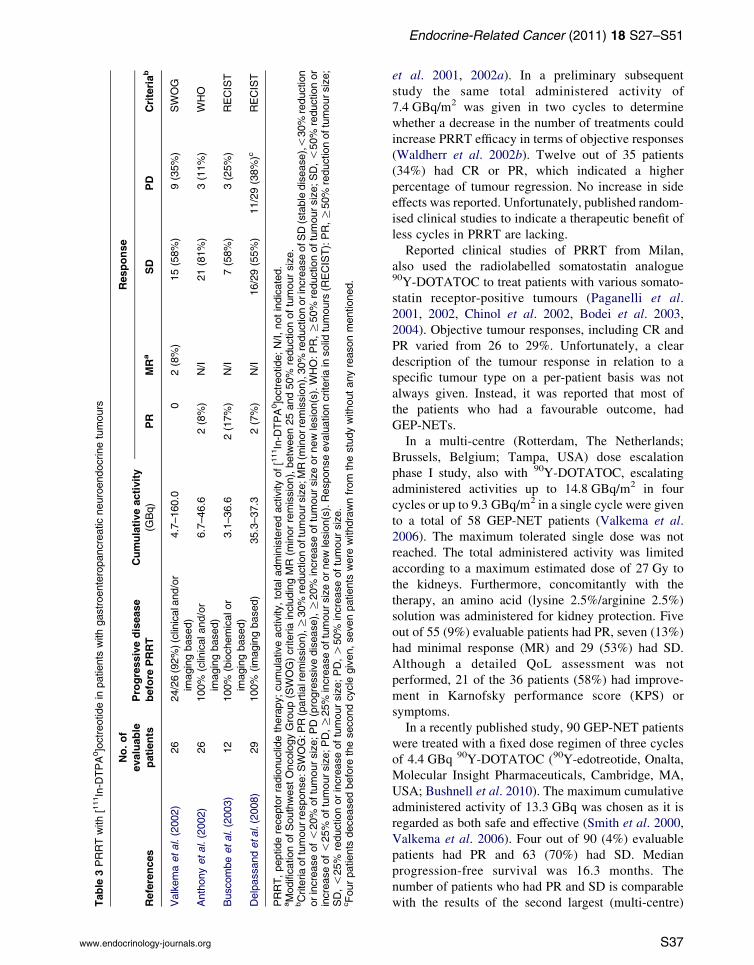
Median TTP in the GEP-NET patients who did not
have PD (nZ249) was 40 months from start of the first
cycle. Median OS was 46 months and median disease-
related survival was O48 months. Median pro-
gression-free survival was 33 months (Kwekkeboom
et al. 2008). Not surprisingly, the most important factor
predicting increased survival was treatment outcome.
Patients with PD had significantly shorter survival
compared with patients with SD or tumour shrinkage.
Survival between other treatment outcomes did not
differ significantly (Fig. 4).
Furthermore, patients with a low KPS or extensive
tumour load within the liver had a less favourable
survival.
In 42 patients with metastasised bronchial or
GEP-NETs who had an objective tumour response of
tumour remission or SD with clearly clinical benefit
after the regular 177Lu-DOTATATE therapy, salvage
therapy, with two additional cycles of 7.4 GBq, was
evaluated (van Essen et al. 2010). On radiological
evaluation, eight (24%) out of 33 eligible patients had
tumour remission (MR or PR), ten (31%) had SD and
15 (45%) had PD 3 months after the last therapy.
The additional treatments were well tolerated with
acceptable haematological toxicity and without any
S40
serious delayed toxicity. A similar study was
performed by Forrer et al. (2005) in patients with
NETs previously successfully treated with 90Y-
DOTATOC. Twenty-seven patients received an
additional treatment of 7.4 GBq 177Lu-DOTATATE.
On radiological evaluation, seven (26%) had tumour
remission (MR or PR) and 12 (44%) had SD 8–12
weeks after therapy.
Published reports of PRRT with 177Lu-DOTATATE
in other clinical centres are in a small group of
patients or anecdotal. In the study by Muros et al.
(2009), PRRT with 177Lu-DOTATATE was performed
in two patients with advanced NETs in addition to
previously given treatments of 90Y-DOTATOC. In
both patients disease stabilisation was the maximum
achieved objective tumour response. In a recently
published study, which was mainly focused on
dosimetric issues instead of the therapeutic efficacy
of PRRT, two out of 12 (17%) patients, who were
evaluable and had completed the treatments (three and
four cycles of 7.4 GBq) with 177Lu-DOTATATE, had
PR, 3/12 (25%) had MR and 5/12 (42%) had SD
(Garkavij et al. 2010). Although a limited number of
patients studied, the results are in line with the large
series by Kwekkeboom et al. (2008).
Clinical PRRT studies with other 177Lu-labelled
somatostatin analogues are limited. The use of
www.endocrinology-journals.org
1.0
0.8
0.6
PD
SD
CR, PR and MR
0.4
Cum
ulat
ive
surv
ival
0.2
0 6 12 18 24 30 36
Time from treatment start (months)
42 48
Figure 4 Disease-related survival in 310 patients accordingto treatment outcome. Patients with progressive disease (PD)have significantly shorter survival. Survival between othertreatment outcomes did not differ significantly. CR, completeresponse; PR, partial response; MR, minimal response;SD, stable disease. Reproduced with permission. q 2008American Society of Clinical Oncology. Kwekkeboom et al.,Treatment with the radiolabelled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate: toxicity, efficacy, and survival, Journalof Clinical Oncology, volume 26, pp 2124–2130.
Endocrine-Related Cancer (2011) 18 S27–S51
DOTANOC is interesting because it has a high affinity
to the sst2, sst3 and sst5 (Wild et al. 2003). Therewith, a
broader affinity profile than DOTATATE, which has
predominantly high affinity to the sst2. In theory, the
broader affinity profile can be beneficial for patients
with tumours that express not only the sst2. In a recent
study, eight patients were treated with one cycle of
3600–7400 MBq 177Lu-DOTANOC (Wehrmann et al.
2007). PRRT was continued in three patients with177Lu-DOTATATE (Wehrmann et al. 2007). Because
the report was primarily conducted for dosimetric
comparison of 177Lu-DOTATATE with 177Lu-
DOTANOC, no tumour response outcome was
reported. From the results it was concluded that
DOTANOC coupled to 177Lu leads to a higher uptake
in normal tissue, and therefore an increase in the
whole-body dose. Together with the observed high
inter-patient variability this outcome indicates that
individual patient dosimetry is important to decide
whether to treat a patient with 177Lu-DOTATATE or177Lu-DOTANOC. In a preliminary report from
Rotterdam, four patients with thyroid carcinoma were
treated with 6.7–32.5 GBq 177Lu-DOTANOC
(Valkema et al. 2007). One patient with follicular
thyroid carcinoma had PR, one patient with Hurthle
cell thyroid carcinoma (HCTC) had clinical
www.endocrinology-journals.org
improvement whereas the other two patients (HCTC
and medullary thyroid carcinoma) had PD. Studies that
report tumour responses in patients with NETs with177Lu-DOTANOC therapy are lacking.
Side effects after PRRT with 177Lu-DOTATATE
were analysed in a total of 504 patients. Acute side
effects within 24 h after administration were reported
and included nausea (25%) and vomiting (10%) and
abdominal pain/comfort (10%). However, it is not
clear whether both nausea and vomiting are purely
related to the PRRT since both side effects can be
caused by the coinfusion of renal protective amino acid
solutions (Rolleman et al. 2003).
Acute haematological toxicity was often mild and
transient with grade 3 or 4 toxicity (WHO criteria) in
3.6% calculated on a per-cycle basis or 9.5% on a per-
patient basis (at least one of several cycles). Patients
had an increased risk of grade 3 or 4 haematological
toxicity when older than 70 years of age at the start of
PRRT, previous chemotherapy, low creatinine clear-
ance (%60 ml/min; Cockcroft’s formula estimation) or
the presence of bone metastases. Temporary mild hair
loss was noticed in 62% of the patients.
Serious late toxicity in the group of 504 patients
included MDS in four patients of which in three
probably PRRT-related, two patients with renal
insufficiency, both probably unrelated, and three
patients with serious liver toxicity.
Similar to PRRT with 90Y-labelled somatostatin
analogues, the kidneys are one of the dose-limiting
organs with 177Lu-DOTATATE. However, the study
by Valkema et al. (2005) indicated that the impact on
creatinine clearance rate is less pronounced than with90Y-DOTATOC with a median decline in creatinine
clearance of 3.8%/year.
Prolonged or (re-)hospitalisation after therapy
because of probably PRRT-induced hormonal crises
occurred in six (1%) patients (de Keizer et al. 2008).
All patients recovered after adequate care including
fluid infusion, high-dose i.v. administered somatostatin
analogue, corticosteroids and correction of electrolyte
disturbances.
PRRT-induced hormone disturbances such as tran-
sient inhibitory effect on inhibin that suggests an effect
on the spermatogenesis and mild decrease in gonado-
tropin hormones in postmenopausal women have been
described (Teunissen 2009). This could have clinical
relevance, especially in those patients with a favour-
able durable response. These endocrine effects are
similar with the reported experience of the use of 131I
treatment in men with differentiated thyroid carcinoma
(Wichers et al. 2000).
S41

J J M Teunissen et al.: Imaging and treatment of NET
Quality of life
Another study evaluated the QoL in patients with
metastatic somatostatin receptor-positive GEP-NETs
treated with 177Lu-DOTATATE (Teunissen et al.
2004). Fifty Dutch patients completed the European
Organization for the Research and Treatment of Cancer
Quality of Life Questionnaire C30 (Aaronson et al.
1993) before therapy and at follow-up visit 6 weeks
after the last cycle. A significant improvement in the
global health status/QoL scale was observed after
therapy with 177Lu-DOTATATE. Furthermore, signi-
ficant improvement was observed in the role, emotional
and social function scales. The symptom scores for
fatigue, insomnia and pain decreased significantly.
Patients with proven tumour regression most frequently
had an improvement of QoL domains. However,
because of the lack of a control group in this study,
some placebo effect cannot be ruled out completely.
Comparison of the various radiolabelled
somatostatin analogues used for PRRT
Treatment with 90Y- and 177Lu-labelled somatostatin
analogues is very encouraging in terms of tumour
shrinkage. However, studies that compare the different
radiopharmaceuticals in a direct randomised manner,
are lacking. Even comparison of studies using the same
compound (e.g. 90Y-DOTATOC, Table 4) is difficult
because of differences in the used PRRT such as the
amount of administered activity, number of cycles,
selection of patients and the tumour response criteria
used. These among other causes can be responsible for
the observed differences in treatment outcome. There-
fore, randomised controlled trials are necessary to
define the optimal PRRT and treatment scheme fur
future use. It may be kept in mind, however, that 50
years of experience of 131I treatment for thyroid
disease, has not lead to a general accepted consenses
on treatment protocols.
Comparison of PRRT with conventional therapy
At this moment the opportunity for a prospective
randomised comparison of PRRT with no further
treatment has passed. It seems unethical to perform
such a trial with the impressive reported results of
PRRT to date. Of interest is the use of ‘cold’
somastostatin analogues and interferon-a. In a group
of 80 progressive therapy-naive GEP-NET patients,
somatostatin analogues and/or interferon-a was started
(Faiss et al. 2003). Four (5%) patients had a tumour
remission and 19 (24%) had SD. In another recently
published prospective randomised trial, patients with
S42
metastatic mid-gut NET (carcinoids) were assigned to
either placebo or octreotide LAR 30 mg/month (Rinke
et al. 2009). Octreotide LAR significantly lenghtened
the TTP compared with placebo with 8–9 months, with
the most favourable effect in patients with low hepatic
tumour load and resected primary tumour. The next
logical step would be a similar randomised trial with
octreotide LAR versus PRRT.
Studies in which a direct comparison of PRRT with
chemotherapy was performed are lacking. However, in
a recent article (Kwekkeboom et al. 2005) the outcome
of historical studies with single or combination
chemotherapy regimens was used as a surrogate for
the comparison with the outcome of PRRT with177Lu-DOTATATE (Kwekkeboom et al. 2005).
Compared with these historical control groups, a
survival benefit of 40–72 months was observed.
Although comparison with historical controls always
has to be interpreted with caution, the consistent
differences with these studies is at least suggestive for a
better survival after 177Lu-DOTATATE therapy.
Options to improve PRRT
Various methods to improve the efficacy of PRRT have
been proposed. The combination of 90Y- and 177Lu-
labelled somatostatin analogues, which demonstrated
more favourable tumour responses in animal experi-
ments than either analogue tested as a single agent,
might be more effective (de Jong et al. 2002b).
However, an adequate prospective randomised trial
has not yet been performed.
Currently, locoregional administration of radio-
labelled somatostatin analogues administered via the
hepatic artery to increase the uptake in liver lesions is
studied. This therapeutic approach could be especially
effective when the major tumour bulk is within the
liver. Selective hepatic intra-arterial administrated
[90Y-DOTA]lanreotide proved to be both safe and
effective, resulting in PR in 3/19 (16%) and SD in
12/19 (63%) of patients. Comparison with the same
therapy i.v. administered, however, was impossible,
because of the absence of randomisation, limited
number of patients included and because locoregional
administration was performed with and without
embolisation (McStay et al. 2005).
Another study reported the results in 17 patients
after multiple cycles (maximum of 15 per patient) of
intra-arterially administered [111In-DTPA0]octreotide
(Limouris et al. 2008). An average of 6.3G2.3 GBq
per cycle was administered. The use of [111In-DTPA0]
octreotide in this therapeutic setting resulted in CR in
1/17 (6%), PR in 8/17 (47%) and SD in 3/12 (25%)
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
according to the response evaluation criteria in solid
tumours.
PRRT in combination with the chemosensitisation
agents 5-fluorouracil (5-FU) or its prodrug capecita-
bine, which was performed in analogy with radio-
immunotherapy (Wong et al. 2003) and (fractionated)
external beam radiotherapy (Rich et al. 2004), could
also be more effective than PRRT with a single agent.
A phase 1 feasibility study with the combination of177Lu-octreotate and relatively low doses (1650 mg/m2
per day for 2 weeks) of capecitabine, indicated that
treatment with this combination was feasible and safe
considering acute and subacute side effects (van Essen
et al. 2008). Subsequently, a randomised, controlled
clinical trial to compare this combination with177Lu-octreotate as a single agent was started.
As mentioned, the kidneys and bone marrow are the
dose-limiting organs in PRRT. To widen its therapeutic
window, both the reduction of the absorbed radiation
dose to these organs and a tumour-specific increase in
somatostatin receptor density are subjects of research.
Lastly, individualised tailored dosimetry for each
patient is the ideal method of treating patients with
PRRT, combining the highest possible radiation dose
to the tumour and a maximally well-tolerated dose to
the dose-limiting organs. Both kidneys and bone
marrow absorbed radiation dose vary widely between
patients (Kwekkeboom et al. 2001, Forrer et al. 2009).
Therefore, the administration of fixed activities to our
patients with relatively few side effects implicate that
some patients had suboptimal administered activities
and thus suboptimal doses to the tumours. This means
that with fixed dose regimens that show relatively few
side effects, a proportion of patients is undertreated.
The currently used method of tailored dosimetry
includes urine collection, repeated imaging and blood
sampling and is time-consuming. However, although
practically difficult, tailored dosimetry could indicate
the maximum cumulative activity that can be safely
administered to the patient and thereby increase the
effectiveness of PRRT. Studies into more accurate and,
if possible, simplified individualised dosimetry are
necessary to address this method of tailored PRRT.
MIBG therapy
Except for the diagnosis and staging of GEP-NETs,123I-MIBG scintigraphy can also be used to select
patients for 131I-MIBG therapy. In a similar approach as
with PRRT, 131I-MIBG therapy has the advantage that
the treatment targets all sites of disease, including
distant metastases, that were visible on 123I-MIBG
scintigraphy. Visualisation of disease on 123I-MIBG
www.endocrinology-journals.org
scintigraphy is therefore a prerequisite for the initiation
of treatment. Treatment protocols vary between
different centres. The usual prescribed activities range
between 7.4 and 11.2 GBq, administered at 3–6 months
intervals. Reported tumour responses after 131I-MIBG
therapy in patients with metastatic carcinoid disease
range from 13 to 35% (Hoefnagel 1994, Bomanji et al.
2003, Safford et al. 2004), with objective tumour
shrinkage (WHO criteria), evaluated with CT or MRI,
in 13 and 15% of patients in the two largest studies
comprising 75 and 52 evaluable patients respectively.
In general, biochemical response, which was defined
as O50% reduction in the tumour marker levels such
as CgA or 5-hydroxyindoleacetic acid (5-HIAA), was
demonstrated in 37–46% (Bomanji et al. 2003, Safford
et al. 2004). However, biochemical responses do not
correlate well with objective tumour responses.
Symptomatic control was reported in a higher
proportion of patients, being present in 49–87%131I-MIBG treated patients (Taal et al. 1996b,
Pathirana et al. 2001, Bomanji et al. 2003, Safford
et al. 2004). Reports on survival in patients with NETs
(including carcinoids) treated with 131I-MIBG are few.
Recently, two studies reported survival benefit when
patients with carcinoid tumour were treated with at
least 15 GBq 131I-MIBG given in a period of 6 months
(Safford et al. 2004, Sywak et al. 2004).
In general, 131I-MIBG treatment is well tolerated
with side effects limited to nausea or vomiting 24–72 h
after administration, mild hepatic dysfunction with
spontaneous recovery and temporary myelosuppression
4–6 weeks posttherapy. Only incidentally patients may
develop significant side effects such as severe myelo-
suppression, especially when extensive metastatic
spread within the bone marrow is present, or hepatic
failure in patients with widespread liver metastases
(Bongers et al. 1997). Furthermore, the frequency and
severity of most haematological side effects is clearly
dependent on the (cumulative) administered activity
(Bomanji et al. 2003, Safford et al. 2004).
In conclusion, in patients with GEP-NETs who have
low tumoural uptake on SRS and do not qualify
for PRRT, but have uptake on MIBG scintigraphy,131I-MIBG therapy can be an alternative treatment
option to offer possible tumour size reduction and/or
effective palliation. Furthermore, survival analyses
after 131I-MIBG suggest that there may be a survival
benefit.
Summary
Conventional imaging techniques such as CT, MRI and
US to image NETs have been improved over the years.
S43

J J M Teunissen et al.: Imaging and treatment of NET
Nonetheless, to image the small primary tumours and
metastases that can be encountered during the initial
diagnostic work up, nuclear medicine imaging with
SRS continues to play a pivotal role with
[111In-DTPA0]octreotide scintigraphy, including the
acquisition methodology of planar imaging, SPECT
and SPECT–CT as the gold standard. Different
alternative somatostatin analogues labelled with
g-emitting radionuclides have been proposed, and
although some of them are encouraging in terms of
imaging quality and sensitivity to detect GEP-NETs,
none of them is approved by the European Medicines
Agency (Daly et al. 2006) and/or FDA.
The same holds true for the very promising
somatostatin analogue-based PET radiopharmaceuti-
cals, such as 68Ga-DOTATOC, 68Ga-DOTATATE and68Ga-DOTANOC. Other interesting and promising
PET imaging modalities includes metabolic imaging
of GEP-NETs with 18F-DOPA and 11C-HTP.
Treatment with radiolabelled peptides or PRRT is a
promising new therapeutic option in the management
of inoperable or metastasised NETs. Symptomatic
control can be achieved with all 111In-, 90Y- and177Lu-labelled somatostatin analogue-based PRRT.
For objective response and long-lasting duration of
response, 90Y-DOTATOC and 177Lu- DOTATATE are
the most promising radiopharmaceuticals. Side effects
of PRRT are few and mild, if adequate kidney
protective measures are taken and dose-limits are
respected. In a minority of patients, when SRS fails to
identify neuroendocrine disease, MIBG scintigraphy
and subsequent 131I-MBG therapy might be an
alternative treatment option.
Declaration of interest
E P Krenning is a member of the advisory board of
BioSynthema, and a consultant of Biosynthema and
Covidien. He receives research or material support from
Covidien, Novartis and BioSynthema, and is a shareholder
in BioSynthema. D J Kwekkeboom is a shareholder in
BioSynthema.
Funding
This research did not receive any specific grant from any
funding agency in the public, commercial or not-for-profit
sector.
Acknowledgements
The images of Figs. 1 and 2 have been kindly provided by K P
Koopmans MD PhD, University Medical Centre Groningen,
The Netherlands.
S44
References
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A,
Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes
JC et al. 1993 The European Organization for Research
and Treatment of Cancer QLQ-C30: a quality-of-life
instrument for use in international clinical trials in
oncology. Journal of National Cancer Institute 85
365–376. (doi:10.1093/jnci/85.5.365)
Adams S, Baum R, Rink T, Schumm-Drager PM, Usadel KH
& Hor G 1998 Limited value of fluorine-18 fluorode-
oxyglucose positron emission tomography for the
imaging of neuroendocrine tumours. European Journal of
Nuclear Medicine 25 79–83. (doi:10.1007/s0025900
50197)
Ambrosini V, Rubello D, Nanni C, Al-Nahhas A & Fanti S
2008 68Ga-DOTA-peptides versus 18F-DOPA PET for
the assessment of NET patients. Nuclear Medicine
Communications 29 415–417. (doi:10.1097/MNM.
0b013e3282ffd70d)
Anderson MA, Carpenter S, Thompson NW, Nostrant TT,
Elta GH & Scheiman JM 2000 Endoscopic ultrasound is
highly accurate and directs management in patients with
neuroendocrine tumors of the pancreas. American
Journal of Gastroenterology 95 2271–2277. (doi:10.
1111/j.1572-0241.2000.02480.x)
Anthony LB, Woltering EA, Espenan GD, Cronin MD,
Maloney TJ & McCarthy KE 2002 Indium-111-pente-
treotide prolongs survival in gastroenteropancreatic
malignancies. Seminars in Nuclear Medicine 32 123–132.
(doi:10.1053/snuc.2002.31769)
Balan KK 2005 Visualization of the gall bladder on F-18
FDOPA PET imaging: a potential pitfall. Clinical Nuclear
Medicine 30 23–24. (doi:10.1097/00003072-200501000-
00006)
Baldelli R, Ettorre G, Vennarecci G, Pasimeni G, Carboni F,
Lorusso R, Barnabei A & Appetecchia M 2007
Malignant insulinoma presenting as metastatic liver
tumor. Case report and review of the literature.
Journal of Experimental & Clinical Cancer Research 26
603–607.
Balon HR, Goldsmith SJ, Siegel BA, Silberstein EB,
Krenning EP, Lang O & Donohoe KJ 2001 Procedure
Guideline for Somatostatin Receptor Scintigraphy with111In-Pentetreotide. Journal of Nuclear Medicine 42
1134–1138.
Bangard M, Behe M, Guhlke S, Otte R, Bender H, Maecke
HR & Biersack HJ 2000 Detection of somatostatin
receptor-positive tumours using the new 99mTc-tricine-
HYNIC-D-Phe1-Tyr3-octreotide: first results in patients
and comparison with 111In-DTPA-D-Phe1-octreotide.
European Journal of Nuclear Medicine 27 628–637.
Baum RP, Soldner J, Schmucking M & Niesen A 2004
Intravenous and intra-arterial peptide receptor radio-
nuclide therapy (PRRT) using Y-90-DOTA-Tyr3-octreo-
tate (Y-90-DOTA-TATE) in patients with metastatic
neuroendocrine tumors. European Journal of Nuclear
Medicine 31 (Suppl 2). S238 (abstract).
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
Becherer A, Szabo M, Karanikas G, Wunderbaldinger P,
Angelberger P, Raderer M, Kurtaran A, Dudczak R &
Kletter K 2004 Imaging of advanced neuroendocrine
tumors with 18F-FDOPA PET. Journal of Nuclear
Medicine 45 1161–1167.
Belhocine T, Foidart J, Rigo P, Najjar F, Thiry A, Quatresooz
P & Hustinx R 2002 Fluorodeoxyglucose positron
emission tomography and somatostatin receptor scinti-
graphy for diagnosing and staging carcinoid tumours:
correlations with the pathological indexes p53 and Ki-67.
Nuclear Medicine Communications 23 727–734. (doi:10.
1097/00006231-200208000-00005)
Bertherat J, Tenenbaum F, Perlemoine K, Videau C, Alberini
JL, Richard B, Dousset B, Bertagna X & Epelbaum J 2003
Somatostatin receptors 2 and 5 are the major somatostatin
receptors in insulinomas: an in vivo and in vitro study.
Journal of Clinical Endocrinology and Metabolism 88
5353–5360. (doi:10.1210/jc.2002-021895)
Binderup T, Knigge U, Loft A, Federspiel B & Kjaer A
2010a 18F-fluorodeoxyglucose positron emission
tomography predicts survival of patients with neuro-
endocrine tumors. Clinical Cancer Research 16 978–985.
(doi:10.1158/1078-0432.CCR-09-1759)
Binderup T, Knigge U, Loft A, Mortensen J, Pfeifer A,
Federspiel B, Hansen CP, Hojgaard L & Kjaer A 2010b
Functional imaging of neuroendocrine tumors: a head-
to-head comparison of somatostatin receptor scintigraphy,123I-MIBG scintigraphy, and 18F-FDG PET. Journal of
Nuclear Medicine 51 704–712. (doi:10.2967/jnumed.109.
069765)
Bodei L, Cremonesi M, Zoboli S, Grana C, Bartolomei M,
Rocca P, Caracciolo M, Macke HR, Chinol M & Paganelli
G 2003 Receptor-mediated radionuclide therapy with90Y-DOTATOC in association with amino acid infusion:
a phase I study. European Journal of Nuclear Medicine
and Molecular Imaging 30 207–216. (doi:10.1007/
s00259-002-1023-y)
Bodei L, Cremonesi M, Grana C, Rocca P, Bartolomei M,
Chinol M & Paganelli G 2004 Receptor radionuclide
therapy with 90Y-[DOTA]0-Tyr3-octreotide (90Y-
DOTATOC) in neuroendocrine tumours. European
Journal of Nuclear Medicine and Molecular Imaging 31
1038–1046. (doi:10.1007/s00259-004-1571-4)
Bodei L, Cremonesi M, Ferrari M, Pacifici M, Grana CM,
Bartolomei M, Baio SM, Sansovini M & Paganelli G 2008
Long-term evaluation of renal toxicity after peptide
receptor radionuclide therapy with 90Y-DOTATOC and177Lu-DOTATATE: the role of associated risk factors.
European Journal of Nuclear Medicine and Molecular
Imaging 35 1847–1856. (doi:10.1007/s00259-008-0778-1)
Bokenkamp R, Duchateau CS & Stokkel MP 2003 An
endocrine active insulinoma with extended lymphogenic
dissemination. Clinical Nuclear Medicine 28 316–317.
(doi:10.1097/01.RLU.0000057560.65838.AB)
Bomanji JB, Wong W, Gaze MN, Cassoni A, Waddington W,
Solano J & Ell PJ 2003 Treatment of neuroendocrine
www.endocrinology-journals.org
tumours in adults with 131I-MIBG therapy. Clinical
Oncology 15 193–198. (doi:10.1016/S0936-6555(02)
00273-X)
Bombardieri E, Ambrosini V, Aktolun C, Baum RP, Bishof-
Delaloye A, Del Vecchio S, Maffioli L, Mortelmans L,
Oyen W, Pepe G et al. 2010 111In-pentetreotide scinti-
graphy: procedure guidelines for tumour imaging.
European Journal of Nuclear Medicine and Molecular
Imaging 37 1441–1448. (doi:10.1007/s00259-010-1473-6)
Bongers V, de Klerk JMH, Zonnenberg BA, de Kort G, Lips
CJM & van Rijk PP 1997 Acute liver necrosis induced by
iodine-131-MIBG in the treatment of metastatic carcinoid
tumors. Journal of Nuclear Medicine 38 1024–1026.
Buchmann I, Henze M, Engelbrecht S, Eisenhut M, Runz A,
Schafer M, Schilling T, Haufe S, Herrmann T &
Haberkorn U 2007 Comparison of 68Ga-DOTATOC PET
and 111In-DTPAOC (OctreoScan) SPECT in patients with
neuroendocrine tumours. European Journal of Nuclear
Medicine and Molecular Imaging 34 1617–1626. (doi:10.
1007/s00259-007-0450-1)
Buscombe JR, Caplin ME & Hilson AJ 2003 Long-term
efficacy of high-activity 111in-pentetreotide therapy in
patients with disseminated neuroendocrine tumors.
Journal of Nuclear Medicine 44 1–6.
Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, Menda Y,
Hicks RJ, Van Cutsem E, Baulieu JL, Borson-Chazot F,
Anthony L & Benson AB 2010 90Y-edotreotide for
metastatic carcinoid refractory to octreotide. Journal of
Clinical Oncology 28 1652–1659. (doi:10.1200/JCO.
2009.22.8585)
Chinol M, Bodei L, Cremonesi M & Paganelli G 2002
Receptor-mediated radiotherapy with Y-DOTA-D-Phe-
Tyr-octreotide: the experience of the European Institute
of Oncology Group. Seminars in Nuclear Medicine 32
141–147. (doi:10.1053/snuc.2002.31563)
Christ E, Wild D, Forrer F, Brandle M, Sahli R, Clerici T,
Gloor B, Martius F, Maecke H & Reubi JC 2009
Glucagon-like peptide-1 receptor imaging for localization
of insulinomas. Journal of Clinical Endocrinology and
Metabolism 94 4398–4405. (doi:10.1210/jc.2009-1082)
Cybulla M, Weiner SM & Otte A 2001 End-stage renal
disease after treatment with 90Y-DOTATOC. European
Journal of Nuclear Medicine 28 1552–1554. (doi:10.
1007/s002590100599)
Daly AF, Jaffrain-Rea ML, Ciccarelli A, Valdes-Socin H,
Rohmer V, Tamburrano G, Borson-Chazot C, Estour B,
Ciccarelli E, Brue T et al. 2006 Clinical characterization
of familial isolated pituitary adenomas. Journal of
Clinical Endocrinology and Metabolism 91 3316–3323.
(doi:10.1210/jc.2005-2671)
Delpassand ES, Sims-Mourtada J, Saso H, Azhdarinia A,
Ashoori F, Torabi F, Espenan G, Moore WH, Woltering E
& Anthony L 2008 Safety and efficacy of radionuclide
therapy with high-activity In-111 pentetreotide in patients
with progressive neuroendocrine tumors. Cancer
Biotherapy & Radiopharmaceuticals 23 292–300.
(doi:10.1089/cbr.2007.0448)
S45

J J M Teunissen et al.: Imaging and treatment of NET
van Essen M, Krenning EP, Kam BL, de Herder WW,
van Aken MO & Kwekkeboom DJ 2008 Report on
short-term side effects of treatments with 177Lu-octreotate
in combination with capecitabine in seven patients with
gastroenteropancreatic neuroendocrine tumours.
European Journal of Nuclear Medicine and Molecular
Imaging 35 743–748. (doi:10.1007/s00259-007-0688-7)
van Essen M, Krenning EP, Kam BL, de Herder WW,
Feelders RA & Kwekkeboom DJ 2010 Salvage therapy
with 177Lu-octreotate in patients with bronchial and
gastroenteropancreatic neuroendocrine tumors. Journal of
Nuclear Medicine 51 383–390. (doi:10.2967/jnumed.109.
068957)
Esser JP, Krenning EP, Teunissen JJ, Kooij PP, van Gameren
AL, Bakker WH & Kwekkeboom DJ 2006 Comparison
of [(177)Lu-DOTA(0),Tyr(3)]octreotate and [(177)Lu-
DOTA(0),Tyr(3)]octreotide: which peptide is preferable
for PRRT? European Journal of Nuclear Medicine and
Molecular Imaging 33 1346–1351. (doi:10.1007/s00259-
006-0172-9)
Faiss S, Pape UF, Bohmig M, Dorffel Y, Mansmann U,
Golder W, Riecken EO & Wiedenmann B 2003
Prospective, randomized, multicenter trial on the anti-
proliferative effect of lanreotide, interferon alfa, and their
combination for therapy of metastatic neuroendocrine
gastroenteropancreatic tumors – the International
Lanreotide and Interferon Alfa Study Group. Journal of
Clinical Oncology 21 2689–2696. (doi:10.1200/JCO.
2003.12.142)
Fanti S, Ambrosini V, Tomassetti P, Castellucci P, Montini G,
Allegri V, Grassetto G, Rubello D, Nanni C & Franchi R
2008 Evaluation of unusual neuroendocrine tumours by
means of 68Ga-DOTA-NOC PET. Biomedicine &
Pharmacotherapy 62 667–671. (doi:10.1016/j.biopha.
2008.01.010)
Forrer F, Uusijarvi H, Storch D, Maecke HR & Mueller-
Brand J 2005 Treatment with 177Lu-DOTATOC of
patients with relapse of neuroendocrine tumors after
treatment with 90Y-DOTATOC. Journal of Nuclear
Medicine 46 1310–1316.
Forrer F, Krenning EP, Kooij PP, Bernard BF, Konijnenberg
M, Bakker WH, Teunissen JJ, de Jong M, van Lom K,
de Herder WW et al. 2009 Bone marrow dosimetry in
peptide receptor radionuclide therapy with [(177)
Lu-DOTA (0),Tyr (3)]octreotate. European Journal of
Nuclear Medicine and Molecular Imaging 36 1138–1146.
(doi:10.1007/s00259-009-1072-6)
Gabriel M, Decristoforo C, Donnemiller E, Ulmer H, Watfah
Rychlinski C, Mather SJ & Moncayo R 2003 An
intrapatient comparison of 99mTc-EDDA/HYNIC-TOC
with 111In-DTPA-octreotide for diagnosis of somatostatin
receptor-expressing tumors. Journal of Nuclear Medicine
44 708–716.
Gabriel M, Hausler F, Bale R, Moncayo R, Decristoforo C,
Kovacs P & Virgolini I 2005 Image fusion analysis of
(99m)Tc-HYNIC-Tyr(3)-octreotide SPECT and diagnos-
tic CT using an immobilisation device with external
S46
markers in patients with endocrine tumours. European
Journal of Nuclear Medicine and Molecular Imaging 32
1440–1451. (doi:10.1007/s00259-005-1875-z)
Gabriel M, Decristoforo C, Kendler D, Dobrozemsky G,
Heute D, Uprimny C, Kovacs P, Von Guggenberg E, Bale
R & Virgolini IJ 2007 68Ga-DOTA-Tyr3-octreotide PET
in neuroendocrine tumors: comparison with somatostatin
receptor scintigraphy and CT. Journal of Nuclear
Medicine 48 508–518. (doi:10.2967/jnumed.106.035667)
Garkavij M, Nickel M, Sjogreen-Gleisner K, Ljungberg M,
Ohlsson T, Wingardh K, Strand S & Tennvall J 2010177Lu-[DOTA0,Tyr3]octreotate therapy in patients with
disseminated neuroendocrine tumors: analysis of dosim-
etry with impact on future therapeutic strategy. Cancer
116 (Suppl 4) 1084–2092. (doi:10.1002/cncr.24796)
de Geus-Oei LF, Oei HY, Hennemann G & Krenning EP
2002 Sensitivity of 123I whole-body scan and thyro-
globulin in the detection of metastases or recurrent
differentiated thyroid cancer. European Journal of
Nuclear Medicine and Molecular Imaging 29 768–774.
(doi:10.1007/s00259-002-0781-x)
Gibril F & Jensen RT 2004 Diagnostic uses of radiolabelled
somatostatin receptor analogues in gastroenteropancreatic
endocrine tumours. Digestive and Liver Disease
36 (Suppl 1) S106–S120. (doi:10.1016/j.dld.2003.11.024)
Gibril F, Reynolds JC, Doppman JL, Chen CC, Venzon DJ,
Termanini B, Weber HC, Stewart CA & Jensen RT 1996
Somatostatin receptor scintigraphy: its sensitivity
compared with that of other imaging methods in detecting
primary and metastatic gastrinomas. A prospective study.
Annals of Internal Medicine 125 26–34.
Ginj M, Chen J, Walter MA, Eltschinger V, Reubi JC &
Maecke HR 2005 Preclinical evaluation of new and
highly potent analogues of octreotide for predictive
imaging and targeted radiotherapy. Clinical Cancer
Research 11 1136–1145.
Haug AR, Auernhammer CJ, Wangler B, Schmidt GP,
Uebleis C, Goke B, Cumming P, Bartenstein P, Tiling R
& Hacker M 2010 68Ga-DOTATATE PET/CT for the
early prediction of response to somatostatin receptor-
mediated radionuclide therapy in patients with well-
differentiated neuroendocrine tumors. Journal of Nuclear
Medicine 51 1349–1356. (doi:10.2967/jnumed.110.
075002)
de Herder WW, Niederle B, Scoazec JY, Pauwels S, Kloppel
G, Falconi M, Kwekkeboom DJ, Oberg K, Eriksson B,
Wiedenmann B et al. 2006 Well-differentiated pancreatic
tumor/carcinoma: insulinoma. Neuroendocrinology 84
183–188. (doi:10.1159/000098010)
Hirshberg B, Cochran C, Skarulis MC, Libutti SK, Alexander
HR, Wood BJ, Chang R, Kleiner DE & Gorden P 2005
Malignant insulinoma: spectrum of unusual clinical
features. Cancer 104 264–272. (doi:10.1002/cncr.21179)
Hoefnagel CA 1994 Metaiodobenzylguanidine and somato-
statin in oncology: role in the management of neural crest
tumours. European Journal of Nuclear Medicine 21
561–581.
www.endocrinology-journals.org
Endocrine-Related Cancer (2011) 18 S27–S51
Hoefnagel CA, den Hartog Jager FC, Taal BG, Abeling NG
& Engelsman EE 1987 The role of I-131-MIBG in the
diagnosis and therapy of carcinoids. European Journal
of Nuclear Medicine 13 187–191. (doi:10.1007/
BF00256489)
Hofland LJ, Lamberts SWJ, van Hagen PM, Reubi J-C,
Schaeffer J, Waaijers M, van Koetsveld PM, Srinivasan A,
Krenning EP & Breeman WAP 2003 Crucial role for
somatostatin receptor subtype 2 in determining the uptake
of [111In-DTPA-D-Phe1]octreotide in somatostatin
receptor-positive organs. Journal of Nuclear Medicine 44
1315–1321.
Hofmann M, Maecke H, Borner R, Weckesser E, Schoffski P,
Oei L, Schumacher J, Henze M, Heppeler A, Meyer J
et al. 2001 Biokinetics and imaging with the somatostatin
receptor PET radioligand (68)Ga-DOTATOC: pre-
liminary data. European Journal of Nuclear Medicine 28
1751–1757. (doi:10.1007/s002590100639)
Hubalewska-Dydejczyk A, Fross-Baron K, Mikolajczak R,
Maecke HR, Huszno B, Pach D, Sowa-Staszczak A,
Janota B, Szybinski P & Kulig J 2006 99mTc-EDDA/
HYNIC-octreotate scintigraphy, an efficient method for
the detection and staging of carcinoid tumours: results of
3 years’ experience. European Journal of Nuclear
Medicine and Molecular Imaging 33 1123–1133. (doi:10.
1007/s00259-006-0113-7)
Jacobsson H, Bremmer S & Larsson SA 2003 Visualisation
of the normal adrenals at SPET examination with111In-pentetreotide. European Journal of Nuclear
Medicine and Molecular Imaging 30 1169–1172. (doi:10.
1007/s00259-003-1210-5)
John M, Meyerhof W, Richter D, Waser B, Schaer JC,
Scherubl H, Boese-Landgraf J, Neuhaus P, Ziske C,
Molling K et al. 1996 Positive somatostatin
receptor scintigraphy correlates with the presence of
somatostatin receptor subtype 2. Gut 38 33–39. (doi:10.
1136/gut.38.1.33)
de Jong M, Bakker WH, Breeman WA, Bernard BF, Hofland
LJ, Visser TJ, Srinivasan A, Schmidt M, Behe M, Macke
HR et al. 1998 Pre-clinical comparison of [DTPA0]
octreotide, [DTPA0,Tyr3] octreotide and [DOTA0,Tyr3]
octreotide as carriers for somatostatin receptor-targeted
scintigraphy and radionuclide therapy. International
Journal of Cancer 75 406–411. (doi:10.1002/(SICI)1097-
0215(19980130)75:3!406::AID-IJC14O3.0.CO;2-6)
de Jong M, Bernard BF, Breeman WAP, van Gameren A
& Krenning EP 2002a Combination of 90Y- and177Lu-labeled somatostatin analogs is superior for
radionuclide therapy compared to 90Y- or 177Lu-labeled
analogs only. European Journal of Nuclear Medicine 43.
123P (abstract).
de Jong M, Valkema R, Jamar F, Kvols LK, Kwekkeboom DJ,
Breeman WA, Bakker WH, Smith C, Pauwels S &
Krenning EP 2002b Somatostatin receptor-targeted
radionuclide therapy of tumors: preclinical and clinical
findings. Seminars in Nuclear Medicine 32 133–140.
(doi:10.1053/snuc.2002.31027)
www.endocrinology-journals.org
Kalkner KM, Janson ET, Nilsson S, Carlsson S, Oberg K &
Westlin JE 1995 Somatostatin receptor scintigraphy in
patients with carcinoid tumors: comparison between
radioligand uptake and tumor markers. Cancer Research
55 5801s–5804s.
Kaltsas G, Korbonits M, Heintz E, Mukherjee JJ, Jenkins PJ,
Chew SL, Reznek R, Monson JP, Besser GM, Foley R
et al. 2001a Comparison of somatostatin analog and
meta-iodobenzylguanidine radionuclides in the diagnosis
and localization of advanced neuroendocrine tumors.
Journal of Clinical Endocrinology and Metabolism 86
895–902. (doi:10.1210/jc.86.2.895)
Kaltsas GA, Mukherjee JJ & Grossman AB 2001b The
value of radiolabelled MIBG and octreotide in the
diagnosis and management of neuroendocrine tumours.
Annals of Oncology 12 (Supplement 2) S47–S50. (doi:10.
1023/A:1012436710878)
Kaltsas G, Rockall A, Papadogias D, Reznek R & Grossman
AB 2004 Recent advances in radiological and radio-
nuclide imaging and therapy of neuroendocrine tumours.
European Journal of Endocrinology 151 15–27. (doi:10.
1530/eje.0.1510015)
Kayani I, Bomanji JB, Groves A, Conway G, Gacinovic S,
Win T, Dickson J, Caplin M & Ell PJ 2008 Functional
imaging of neuroendocrine tumors with combined
PET/CT using 68Ga-DOTATATE (DOTA-D-Phe1,Tyr3-
octreotate) and 18F-FDG. Cancer 112 2447–2455.
(doi:10.1002/cncr.23469)
de Keizer B, van Aken MO, Feelders RA, de Herder WW,
Kam BL, van Essen M, Krenning EP & Kwekkeboom DJ
2008 Hormonal crises following receptor radionuclide
therapy with the radiolabeled somatostatin analogue
[177Lu-DOTA0,Tyr3]octreotate. European Journal of
Nuclear Medicine and Molecular Imaging 35 749–755.
(doi:10.1007/s00259-007-0691-z)
de Kerviler E, Cadiot G, Lebtahi R, Faraggi M, Le Guludec D
& Mignon M 1994 Somatostatin receptor scintigraphy in
forty-eight patients with the Zollinger-Ellison syndrome.
GRESZE: Groupe d’Etude du Syndrome de Zollinger-
Ellison. European Journal of Nuclear Medicine 21
1191–1197.
Koopmans KP, Neels OC, Kema IP, Elsinga PH, Sluiter WJ,
Vanghillewe K, Brouwers AH, Jager PL & de Vries EG
2008 Improved staging of patients with carcinoid and
islet cell tumors with 18F-dihydroxy-phenyl-alanine and11C-5-hydroxy-tryptophan positron emission
tomography. Journal of Clinical Oncology 26 1489–1495.
(doi:10.1200/JCO.2007.15.1126)
Krausz Y, Freedman N, Rubinstein R, Lavie E, Orevi M,
Tshori S, Salmon A, Glaser B, Chisin R, Mishani E
et al. 2010 (68)Ga-DOTA-NOC PET/CT imaging
of neuroendocrine tumors: comparison with
(111)In-DTPA-octreotide (OctreoScan (R)). Molecular
Imaging and Biology 13 583–593. (doi:10.1007/s11307-
010-0374-1)
Krenning EP, Bakker WH, Breeman WA, Koper JW, Kooij
PP, Ausema L, Lameris JS, Reubi JC & Lamberts SW
S47

J J M Teunissen et al.: Imaging and treatment of NET
1989 Localisation of endocrine-related tumours with
radioiodinated analogue of somatostatin. Lancet 1
242–244. (doi:10.1016/S0140-6736(89)91258-0)
Krenning EP, Bakker WH, Kooij PP, Breeman WA, Oei HY,
de Jong M, Reubi JC, Visser TJ, Bruns C, Kwekkeboom
DJ et al. 1992 Somatostatin receptor scintigraphy with
indium-111-DTPA-D-Phe-1-octreotide in man: metab-
olism, dosimetry and comparison with iodine-123-Tyr-3-
octreotide. Journal of Nuclear Medicine 33 652–658.
Krenning EP, Kwekkeboom DJ, Bakker WH, Breeman WA,
Kooij PP, Oei HY, van Hagen M, Postema PT, de Jong M,
Reubi JC et al. 1993 Somatostatin receptor scintigraphy
with [111In-DTPA-D-Phe1]- and [123I-Tyr3]-octreotide:
the Rotterdam experience with more than 1000 patients.
European Journal of Nuclear Medicine 20 716–731.
(doi:10.1007/BF00181765)
Krenning EP, Kooij PP, Bakker WH, Breeman WA, Postema
PT, Kwekkeboom DJ, Oei HY, de Jong M, Visser TJ,
Reijs AE et al. 1994a Radiotherapy with a radiolabeled
somatostatin analogue, [111In-DTPA-D-Phe1]-octreotide.
A case history. Annals of the New York Academy of
Sciences 733 496–506. (doi:10.1111/j.1749-6632.1994.
tb17300.x)
Krenning EP, Kwekkeboom DJ, Oei HY, de Jong RJ, Dop FJ,
Reubi JC & Lamberts SW 1994b Somatostatin-receptor
scintigraphy in gastroenteropancreatic tumors. An over-
view of European results. Annals of the New York
Academy of Sciences 733 416–424. (doi:10.1111/j.1749-
6632.1994.tb17291.x)
Krenning EP, Kwekkeboom DJ, Pauwels S, Kvols LK &
Reubi JC 1995 Somatostatin receptor scintigraphy. In
Nuclear Medicine Annual, pp 1–50. Ed. LM Freeman.
New york: Lippincott Williams & Wilkins.
Kwekkeboom DJ, Krenning EP, Bakker WH, Oei HY, Kooij
PP & Lamberts SW 1993 Somatostatin analogue
scintigraphy in carcinoid tumours. European Journal of
Nuclear Medicine 20 283–292.
Kwekkeboom DJ, Kooij PP, Bakker WH, Macke HR &
Krenning EP 1999 Comparison of 111In-DOTA-Tyr3-
octreotide and 111In-DTPA-octreotide in the same
patients: biodistribution, kinetics, organ and tumor
uptake. Journal of Nuclear Medicine 40 762–767.
Kwekkeboom DJ, Bakker WH, Kooij PP, Konijnenberg MW,
Srinivasan A, Erion JL, Schmidt MA, Bugaj JL, de Jong
M & Krenning EP 2001 [177Lu-DOTAOTyr3]octreotate:
comparison with [111In-DTPAo]octreotide in patients.
European Journal of Nuclear Medicine 28 1319–1325.
(doi:10.1007/s002590100574)
Kwekkeboom DJ, Bakker WH, Kam BL, Teunissen JJ, Kooij
PP, De Herder WW, Feelders RA, Van Eijck CH, De Jong
M, Srinivasan A et al. 2003a Treatment of patients
with gastro-entero-pancreatic (GEP) tumours with the
novel radiolabelled somatostatin analogue [(177)Lu-
DOTA(0),Tyr(3)]octreotate. European Journal of
Nuclear Medicine and Molecular Imaging 30 417–422.
(doi:10.1007/s00259-002-1050-8)
S48
Kwekkeboom DJ, Teunissen JJ, Bakker WH, Kooij PP,
de Herder WW, Feelders RA, van Eijck CH, Esser JP,
Kam BL & Krenning EP 2005 Radiolabeled somatostatin
analog [177Lu-DOTA0,Tyr3]octreotate in patients with
endocrine gastroenteropancreatic tumors. Journal of
Clinical Oncology 23 2754–2762. (doi:10.1200/JCO.
2005.08.066)
Kwekkeboom DJ, de Herder WW, Kam BL, van Eijck CH,
van Essen M, Kooij PP, Feelders RA, van Aken MO &
Krenning EP 2008 Treatment with the radiolabeled
somatostatin analog [177Lu-DOTA0,Tyr3]octreotate:
toxicity, efficacy, and survival. Journal of Clinical
Oncology 26 2124–2130. (doi:10.1200/JCO.2007.15.
2553)
Kwekkeboom DJ, Krenning EP, Scheidhauer K, Lewington
V, Lebtahi R, Grossman A, Vitek P, Sundin A, Plockinger
U, participants MCC et al. 2009 ENETS Consensus
Guidelines for the Standards of Care in Neuroendocrine
Tumors: somatostatin receptor imaging with (111)In-
pentetreotide. Neuroendocrinology 90 184–189. (doi:10.
1159/000225946)
Lebtahi R, Cadiot G, Sarda L, Daou D, Faraggi M, Petegnief
Y, Mignon M & le Guludec D 1997 Clinical impact of
somatostatin receptor scintigraphy in the management of
patients with neuroendocrine gastroenteropancreatic
tumors. J Nuclear Medicine 38 853–858.
Lebtahi R, Le Cloirec J, Houzard C, Daou D, Sobhani I,
Sassolas G, Mignon M, Bourguet P & Le Guludec D 2002
Detection of neuroendocrine tumors: 99mTc-P829 scinti-
graphy compared with 111In-pentetreotide scintigraphy.
Journal of Nuclear Medicine 43 889–895.
Lewis JS, Srinivasan A, Schmidt MA & Anderson CJ
1999 In vitro and in vivo evaluation of 64Cu-TETA-
Tyr3-octreotate. A new somatostatin analog with
improved target tissue uptake. Nuclear Medicine and
Biology 26 267–273. (doi:10.1016/S0969-8051(98)
00105-X)
Limouris GS, Chatziioannou A, Kontogeorgakos D, Mour-
ikis D, Lyra M, Dimitriou P, Stavraka A, Gouliamos A &
Vlahos L 2008 Selective hepatic arterial infusion of
In-111-DTPA-Phe1-octreotide in neuroendocrine liver
metastases. European Journal of Nuclear Medicine and
Molecular Imaging 35 1827–1837. (doi:10.1007/s00259-
008-0779-0)
Maecke HR, Hofmann M & Haberkorn U 2005 (68)Ga-
labeled peptides in tumor imaging. Journal of Nuclear
Medicine 46 (Supplement 1) 172S–178S.
McStay MK, Maudgil D, Williams M, Tibballs JM,
Watkinson AF, Caplin ME & Buscombe JR 2005 Large-
volume liver metastases from neuroendocrine tumors:
hepatic intraarterial 90Y-DOTA-lanreotide as effective
palliative therapy. Radiology 237 718–726. (doi:10.1148/
radiol.2372041203)
Meisetschlager G, Poethko T, Stahl A, Wolf I, Scheidhauer K,
Schottelius M, Herz M, Wester HJ & Schwaiger M 2006
Gluc-Lys([18F]FP)-TOCA PET in patients with
www.endocrinology-journals.org

Endocrine-Related Cancer (2011) 18 S27–S51
SSTR-positive tumors: biodistribution and diagnostic
evaluation compared with [111In]DTPA-octreotide.
Journal of Nuclear Medicine 47 566–573.
Miederer M, Seidl S, Buck A, Scheidhauer K, Wester HJ,
Schwaiger M & Perren A 2009 Correlation of immuno-
histopathological expression of somatostatin receptor 2
with standardised uptake values in 68Ga-DOTATOC
PET/CT. European Journal of Nuclear Medicine and
Molecular Imaging 36 48–52. (doi:10.1007/s00259-
008-0944-5)
Modlin IM, Kidd M, Latich I, Zikusoka MN & Shapiro MD
2005 Current status of gastrointestinal carcinoids.
Gastroenterology 128 1717–1751. (doi:10.1053/j.gastro.
2005.03.038)
Modlin IM, Latich I, Zikusoka M, Kidd M, Eick G & Chan AK
2006 Gastrointestinal carcinoids: the evolution of diag-
nostic strategies. Journal of Clinical Gastroenterology 40
572–582. (doi:10.1097/00004836-200608000-00003)
Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW,
Thakker RV, Caplin M, Delle Fave G, Kaltsas GA,
Krenning EP et al. 2008 Gastroenteropancreatic neuro-
endocrine tumours. Lancet Oncology 9 61–72. (doi:10.
1016/S1470-2045(07)70410-2)
Muros MA, Varsavsky M, Iglesias Rozas P, Valdivia J,
Delgado JR, Forrer F, Bodei L & Paganelli G 2009
Outcome of treating advanced neuroendocrine tumours
with radiolabelled somatostatin analogues. Clinical &
Translational Oncology 11 48–53. (doi:10.1007/s12094-
009-0310-5)
Orlefors H, Sundin A, Garske U, Juhlin C, Oberg K, Skogseid
B, Langstrom B, Bergstrom M & Eriksson B 2005 Whole-
body 11C-5-hydroxytryptophan positron emission
tomography as a universal imaging technique for
neuroendocrine tumors: comparison with somatostatin
receptor scintigraphy and computed tomography.
Journal of Clinical Endocrinology and Metabolism 90
3392–3400. (doi:10.1210/jc.2004-1938)
Otte A, Mueller-Brand J, Dellas S, Nitzsche E, Herrmann R
& Maecke H 1998 Yttrium-90-labelled somatostatine-
analogue for cancer treatment. Lancet 351 417–418.
(doi:10.1016/S0140-6736(05)78355-0)
Otte A, Herrmann R, Heppeler A, Behe M, Jermann E,
Powell P, Maecke HR & Muller J 1999 Yttrium-90
DOTATOC: first clinical results. European Journal
of Nuclear Medicine 26 1439–1447. (doi:10.1007/
s002590050476)
Paganelli G, Zoboli S, Cremonesi M, Bodei L, Ferrari M,
Grana C, Bartolomei M, Orsi F, De Cicco C, Macke HR
et al. 2001 Receptor-mediated radiotherapy with 90Y-
DOTA-D-Phe1-Tyr3-octreotide. European Journal
of Nuclear Medicine 28 426–434. (doi:10.1007/
s002590100490)
Paganelli G, Bodei L, Handkiewicz Junak D, Rocca P, Papi S,
Lopera Sierra M, Gatti M, Chinol M, Bartolomei M,
Fiorenza M et al. 2002 90Y-DOTA-D-Phe1-Try3-octreotide
in therapy of neuroendocrine malignancies. Biopolymers
66 393–398. (doi:10.1002/bip.10349)
www.endocrinology-journals.org
Patel YC & Srikant CB 1994 Subtype selectivity of peptide
analogs for all five cloned human somatostatin receptors
(hsstr 1–5). Endocrinology 135 2814–2817. (doi:10.1210/
en.135.6.2814)
Pathirana AA, Vinjamuri S, Byrne C, Ghaneh P, Vora J &
Poston GJ 2001 (131)I-MIBG radionuclide therapy is safe
and cost-effective in the control of symptoms of the
carcinoid syndrome. European Journal of Surgical
Oncology 27 404–408. (doi:10.1053/ejso.2001.1132)
Quigley AM, Buscombe JR, Shah T, Gnanasegaran G,
Roberts D, Caplin ME & Hilson AJ 2005 Intertumoural
variability in functional imaging within patients suffering
from neuroendocrine tumours. An observational, cross-
sectional study. Neuroendocrinology 82 215–220.
(doi:10.1159/000092522)
Reubi JC & Landolt AM 1984 High density of somatostatin
receptors in pituitary tumors from acromegalic patients.
Journal of Clinical Endocrinology and Metabolism 59
1148–1151. (doi:10.1210/jcem-59-6-1148)
Reubi JC, Schar J-C, Waser B, Wenger S, Heppeler A,
Schmitt JS & Macke HR 2000 Affinity profiles for human
somatostatin receptor subtypes SST1–SST5 of somato-
statin radiotracers selected for scintigraphic and radio-
therapeutic use. European Journal of Nuclear Medicine
and Molecular Imaging 27 273–282. (doi:10.1007/
s002590050034)
Reubi JC, Waser B, Schaer JC & Laissue JA 2001
Somatostatin receptor sst1–sst5 expression in normal and
neoplastic human tissues using receptor autoradiography
with subtype-selective ligands. European Journal of
Nuclear Medicine 28 836–846. (doi:10.1007/
s002590100541)
Rich TA, Shepard RC & Mosley ST 2004 Four decades of
continuing innovation with fluorouracil: current and
future approaches to fluorouracil chemoradiation therapy.
Journal of Clinical Oncology 22 2214–2232. (doi:10.
1200/JCO.2004.08.009)
Rinke A, Muller HH, Schade-Brittinger C, Klose KJ, Barth
P, Wied M, Mayer C, Aminossadati B, Pape UF, Blaker
M et al. 2009 Placebo-controlled, double-blind, pro-
spective, randomized study on the effect of octreotide
LAR in the control of tumor growth in patients with
metastatic neuroendocrine midgut tumors: a report from
the PROMID Study Group. Journal of Clinical
Oncology 27 4656–4663. (doi:10.1200/JCO.2009.22.
8510)
Rohrer L, Raulf F, Bruns C, Buettner R, Hofstaedter F &
Schule R 1993 Cloning and characterization of a fourth
human somatostatin receptor. PNAS 90 4196–4200.
(doi:10.1073/pnas.90.9.4196)
Rolleman E, Valkema R, de Jong M, Kooij P & Krenning E
2003 Safe and effective inhibition of renal uptake of
radiolabelled octreotide by a combination of lysine and
arginine. European Journal of Nuclear Medicine and
Molecular Imaging 30 9–15. (doi:10.1007/s00259-002-
0982-3)
S49

J J M Teunissen et al.: Imaging and treatment of NET
Safford SD, Coleman RE, Gockerman JP, Moore J, Feldman
J, Onaitis MW, Tyler DS & Olson JA Jr 2004 Iodine-131
metaiodobenzylguanidine treatment for metastatic carci-
noid. Results in 98 patients. Cancer 101 1987–1993.
(doi:10.1002/cncr.20592)
Schillaci O 2004 Functional–anatomical image fusion
in neuroendocrine tumors. Cancer Biotherapy and
Radiopharmaceuticals 19 129–134. (doi:10.1089/
108497804773391775)
Schillaci O, Massa R & Scopinaro F 2000 111In-pentetreotide
scintigraphy in the detection of insulinomas: importance
of SPECT imaging. Journal of Nuclear Medicine 41
459–462.
Schottelius M, Poethko T, Herz M, Reubi JC, Kessler H,
Schwaiger M & Wester HJ 2004 First (18)F-labeled tracer
suitable for routine clinical imaging of sst receptor-
expressing tumors using positron emission tomography.
Clinical Cancer Research 10 3593–3606. (doi:10.1158/
1078-0432.CCR-03-0359)
Shapiro B 1995 Ten years of experience with MIBG
applications and the potential of new radiolabeled
peptides: a personal overview and concluding remarks.
Quarterly Journal of Nuclear Medicine 39 150–155.
Sheth S & Fishman EK 2002 Imaging of uncommon
tumors of the pancreas. Radiologic Clinics of North
America 40 1273–1287. (doi:10.1016/S0033-8389(02)
00040-4)
Sierra ML, Agazzi A, Bodei L, Pacifici M, Arico D, De Cicco
C, Quarna J, Sansovini M, De Simone M & Paganelli G
2009 Lymphocytic toxicity in patients after peptide-
receptor radionuclide therapy (PRRT) with 177Lu-DO-
TATATE and 90Y-DOTATOC. Cancer Biotherapy &
Radiopharmaceuticals 24 659–665. (doi:10.1089/cbr.
2009.0641)
Sisson JC & Wieland DM 1986 Radiolabeled meta-
iodobenzylguanidine: pharmacology and clinical studies.
American Journal of Physiologic Imaging 1 96–103.
Slooter GD, Breeman WA, Marquet RL, Krenning EP & van
Eijck CH 1999 Anti-proliferative effect of radiolabelled
octreotide in a metastases model in rat liver. International
Journal of Cancer 81 767–771. (doi:10.1002/(SICI)1097-
0215(19990531)81:5!767::AID-IJC17O3.0.CO;2-T)
Smith MC, Liu J, Chen T, Schran H, Yeh CM, Jamar F,
Valkema R, Bakker W, Kvols L, Krenning E et al. 2000
OctreoTher: ongoing early clinical development of a
somatostatin-receptor-targeted radionuclide antineoplas-
tic therapy. Digestion 62 (Suppl 1) 69–72. (doi:10.1159/
000051858)
Sugimoto E, Lorelius LE, Eriksson B & Oberg K 1995
Midgut carcinoid tumours. CT appearance. Acta Radi-
ologica 36 367–371.
Sywak MS, Pasieka JL, McEwan A, Kline G & Rorstad O
2004 131I-meta-iodobenzylguanidine in the management
of metastatic midgut carcinoid tumors. World
Journal of Surgery 28 1157–1162. (doi:10.1007/s00268-
004-7603-1)
S50
Taal BG, Hoefnagel CA, Valdes Olmos RA & Boot H 1996a
Combined diagnostic imaging with 131I-metaiodobenzyl-
guanidine and 111In-pentetreotide in carcinoid tumours.
European Journal of Cancer 32A 1924–1932. (doi:10.
1016/0959-8049(96)00241-9)
Taal BG, Hoefnagel CA, Valdes Olmos RA, Boot H &
Beijnen JH 1996b Palliative effect of metaiodobenzyl-
guanidine in metastatic carcinoid tumors. Journal of
Clinical Oncology 14 1829–1838.
Tamm EP, Kim EE & Ng CS 2007 Imaging of neuroendo-
crine tumors. Hematology/Oncology Clinics of North
America 21 409–432. (doi:10.1016/j.hoc.2007.04.006)
Teunissen JJM 2009 Effects of therapy with [177Lu-DO-
TA0,Tyr3]octreotate on endocrine function. European
Journal of Nuclear Medicine and Molecular Imaging 36
1758–1766. (doi:10.1007/s00259-009-1151-8)
Teunissen JJ, Kwekkeboom DJ & Krenning EP 2004 Quality
of life in patients with gastroenteropancreatic tumors
treated with [177Lu-DOTA0,Tyr3]octreotate. Journal of
Clinical Oncology 22 2724–2729. (doi:10.1200/JCO.
2004.10.016)
Valkema R, De Jong M, Bakker WH, Breeman WA, Kooij
PP, Lugtenburg PJ, De Jong FH, Christiansen A, Kam BL,
De Herder WW et al. 2002 Phase I study of peptide
receptor radionuclide therapy with [In-DTPA]octreotide:
the Rotterdam experience. Seminars in Nuclear Medicine
32 110–122. (doi:10.1053/snuc/2002.31025)
Valkema R, Pauwels SA, Kvols LK, Kwekkeboom DJ, Jamar
F, de Jong M, Barone R, Walrand S, Kooij PP, Bakker
WH et al. 2005 Long-term follow-up of renal function
after peptide receptor radiation therapy with (90)Y-
DOTA(0),Tyr(3)-octreotide and (177)Lu-DOTA(0),
Tyr(3)-octreotate. Journal of Nuclear Medicine 46 (Suppl
1) 83S–91S.
Valkema R, Pauwels S, Kvols LK, Barone R, Jamar F,
Bakker WH, Kwekkeboom DJ, Bouterfa H & Krenning
EP 2006 Survival and response after peptide receptor
radionuclide therapy with [90Y-DOTA0,Tyr3]octreotide
in patients with advanced gastroenteropancreatic neuro-
endocrine tumors. Seminars in Nuclear Medicine 36
147–156. (doi:10.1053/j.semnuclmed.2006.01.001)
Valkema R, Froberg AC, Bakker W, Maecke HR,
Breeman WA, de Jong M & Krenning EP 2007
Peptide receptor scintigraphy (PRS) with in-111-
DOTANOC and peptide receptor radionuclide therapy
(PRRT) with Lu-177-DOTANOC. Journal of Nuclear
Medicine 48 394.
Vezzosi D, Bennet A, Rochaix P, Courbon F, Selves J,
Pradere B, Buscail L, Susini C & Caron P 2005 Octreotide
in insulinoma patients: efficacy on hypoglycemia,
relationships with OctreoScan scintigraphy and immu-
nostaining with anti-sst2A and anti-sst5 antibodies.
European Journal of Endocrinology 152 757–767.
(doi:10.1530/eje.1.01901)
Virgolini I, Britton K, Buscombe J, Moncayo R, Paganelli G
& Riva P 2002 In- and Y-DOTA-lanreotide: results and
www.endocrinology-journals.org
Endocrine-Related Cancer (2011) 18 S27–S51
implications of the MAURITIUS trial. Seminars in
Nuclear Medicine 32 148–155. (doi:10.1053/snuc.2002.
31565)
Virgolini I, Traub-Weidinger T & Decristoforo C 2005
Nuclear medicine in the detection and management of
pancreatic islet-cell tumours. Best Practice & Research:
Clinical Endocrinology & Metabolism 19 213–227.
Wafelman AR, Hoefnagel CA, Maes RA & Beijnen JH
1994 Radioiodinated metaiodobenzylguanidine: a
review of its biodistribution and pharmacokinetics, drug
interactions, cytotoxicity and dosimetry. European
Journal of Nuclear Medicine 21 545–559. (doi:10.1007/
BF00173043)
Waldherr C, Pless M, Maecke HR, Haldemann A & Mueller-
Brand J 2001 The clinical value of [90Y-DOTA]-D-Phe1-
Tyr3-octreotide (90Y-DOTATOC) in the treatment of
neuroendocrine tumours: a clinical phase II study. Annals
of Oncology 12 941–945. (doi:10.1023/A:1011160913619)
Waldherr C, Pless M, Maecke HR, Schumacher T,
Crazzolara A, Nitzsche EU, Haldemann A & Mueller-
Brand J 2002a Tumor response and clinical benefit in
neuroendocrine tumors after 7.4 GBq (90)Y-DOTATOC.
Journal of Nuclear Medicine 43 610–616.
Waldherr C, Schumacher T, Macke HR, Schirp U, Forrer F,
Nitzsche EU & Mueller-Brand J 2002b Does tumor
response depend on the number of treatment sessions at
constant injected dose using 90Yttrium-DOTATOC in
neuroendocrine tumors? European Journal of Nuclear
Medicine 29. S100 (abstract).
Wehrmann C, Senftleben S, Zachert C, Muller D & Baum RP
2007 Results of individual patient dosimetry in peptide
receptor radionuclide therapy with 177Lu DOTA-TATE
and 177Lu DOTA-NOC. Cancer Biotherapy &
Radiopharmaceuticals 22 406–416. (doi:10.1089/cbr.
2006.325)
www.endocrinology-journals.org
Westlin JE, Janson ET, Arnberg H, Ahlstrom H, Oberg K &
Nilsson S 1993 Somatostatin receptor scintigraphy of
carcinoid tumours using the [111In-DTPA-D-Phe1]-
octreotide. Acta Oncology 32 783–786.
Wichers M, Benz E, Palmedo H, Biersack HJ, Grunwald F &
Klingmuller D 2000 Testicular function after radioiodine
therapy for thyroid carcinoma. European Journal of
Nuclear Medicine 27 503–507. (doi:10.1007/
s002590050535)
Wild D, Schmitt JS, Ginj M, Macke HR, Bernard BF,
Krenning E, De Jong M, Wenger S & Reubi JC 2003
DOTA-NOC, a high-affinity ligand of somatostatin
receptor subtypes 2, 3 and 5 for labelling with various
radiometals. European Journal of Nuclear Medicine and
Molecular Imaging 30 1338–1347. (doi:10.1007/s00259-
003-1255-5)
Wild D, Macke HR, Waser B, Reubi JC, Ginj M, Rasch H,
Muller-Brand J & Hofmann M 2005 68Ga-DOTANOC: a
first compound for PET imaging with high affinity for
somatostatin receptor subtypes 2 and 5. European
Journal of Nuclear Medicine and Molecular Imaging 32
724. (doi:10.1007/s00259-004-1697-4)
Wong JY, Shibata S, Williams LE, Kwok CS, Liu A, Chu DZ,
Yamauchi DM, Wilczynski S, Ikle DN, Wu AM et al. 2003
A Phase I trial of 90Y-anti-carcinoembryonic antigen
chimeric T84.66 radioimmunotherapy with 5-fluorouracil
in patients with metastatic colorectal cancer. Clinical
Cancer Research 9 5842–5852.
Zimmer T, Stolzel U, Bader M, Koppenhagen K, Hamm B,
Buhr H, Riecken EO & Wiedenmann B 1996
Endoscopic ultrasonography and somatostatin receptor
scintigraphy in the preoperative localisation of insulino-
mas and gastrinomas. Gut 39 562–568. (doi:10.1136/gut.
39.4.562)
S51