nuevos escenarios para nab-paclitaxel: de la … · gem, gemcitabine; hr, hazard ratio; kps,...
TRANSCRIPT
Nuevos escenarios para nab-paclitaxel: de la
neoadyuvancia al paciente frágil
Dra. T. Macarulla
Hospital Vall d´Hebrón

• High mortality, PC constitutes the fourth leading cause of cancer-related deaths in US.
• 6.000 cases/year in Spain.
• Overall survival at 5 years: <10%
• -Less than 1cm with curative resection:100%
• -Stage I: 58%
• -Stage IIb:17%
• Curative resection: 10-15%.
Cáncer de páncreas
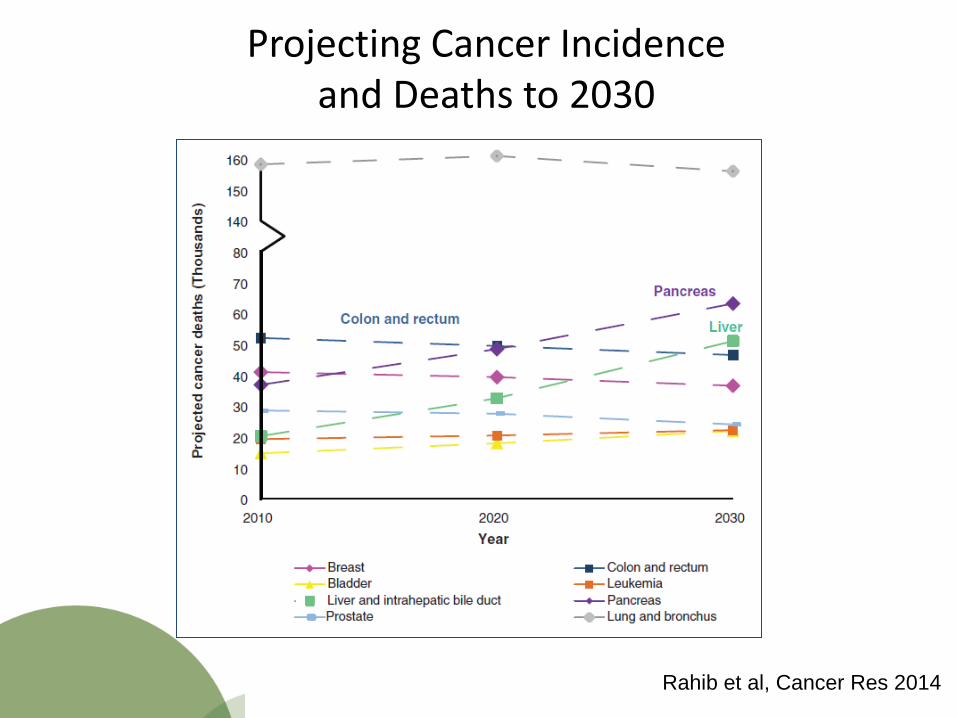
Projecting Cancer Incidence and Deaths to 2030
Rahib et al, Cancer Res 2014

Cáncer de páncreas: Estadiage
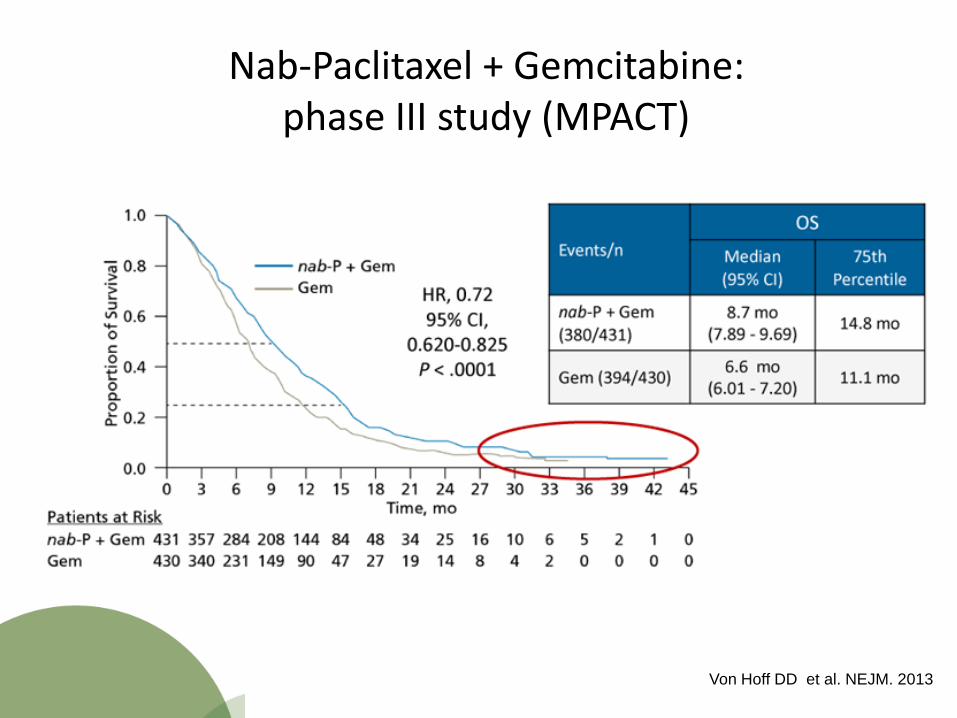
Nab-Paclitaxel + Gemcitabine: phase III study (MPACT)
Von Hoff DD et al. NEJM. 2013
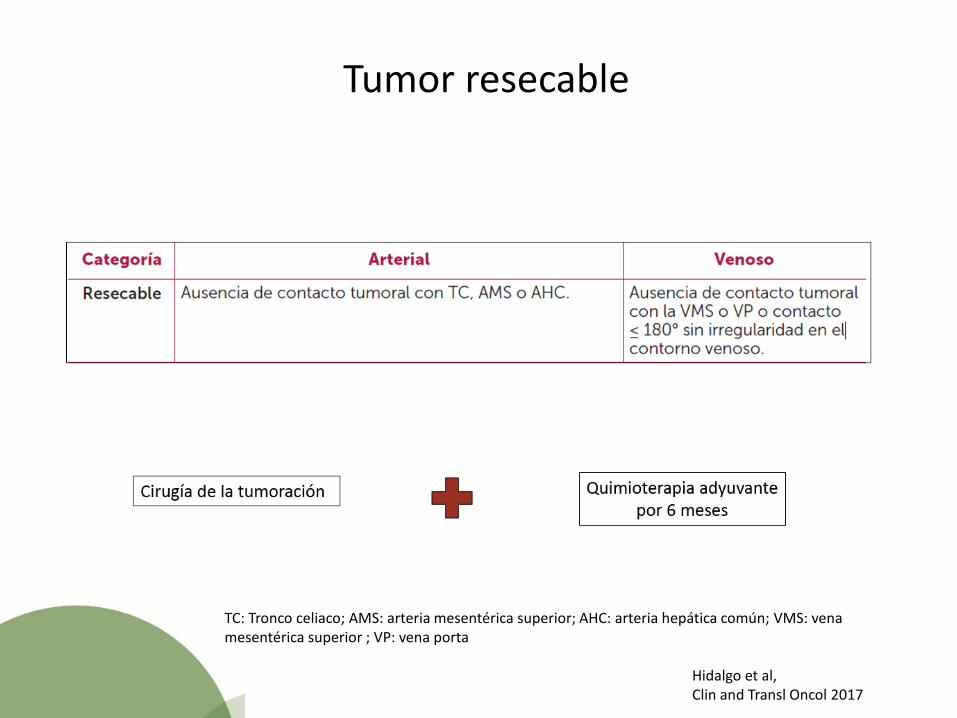
Tumor resecable
TC: Tronco celiaco; AMS: arteria mesentérica superior; AHC: arteria hepática común; VMS: vena mesentérica superior ; VP: vena porta
Hidalgo et al, Clin and Transl Oncol 2017
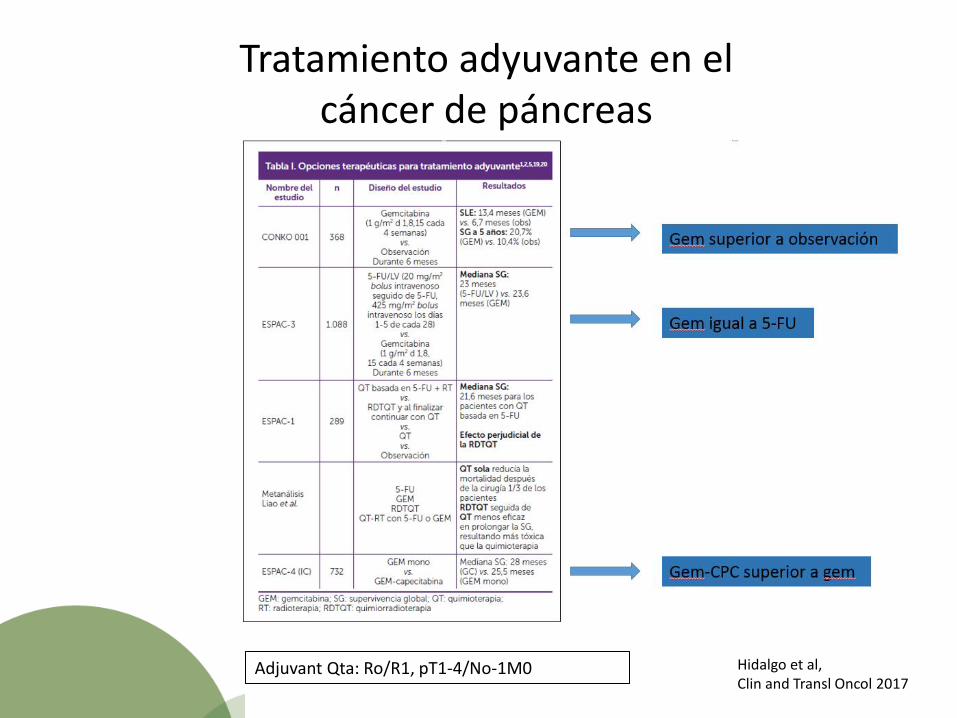
Tratamiento adyuvante en el cáncer de páncreas
Hidalgo et al, Clin and Transl Oncol 2017
Adjuvant Qta: Ro/R1, pT1-4/No-1M0

Tratamiento adyuvante en el cáncer de páncreas: Estudio APACT
Resultados esperados para 2018…
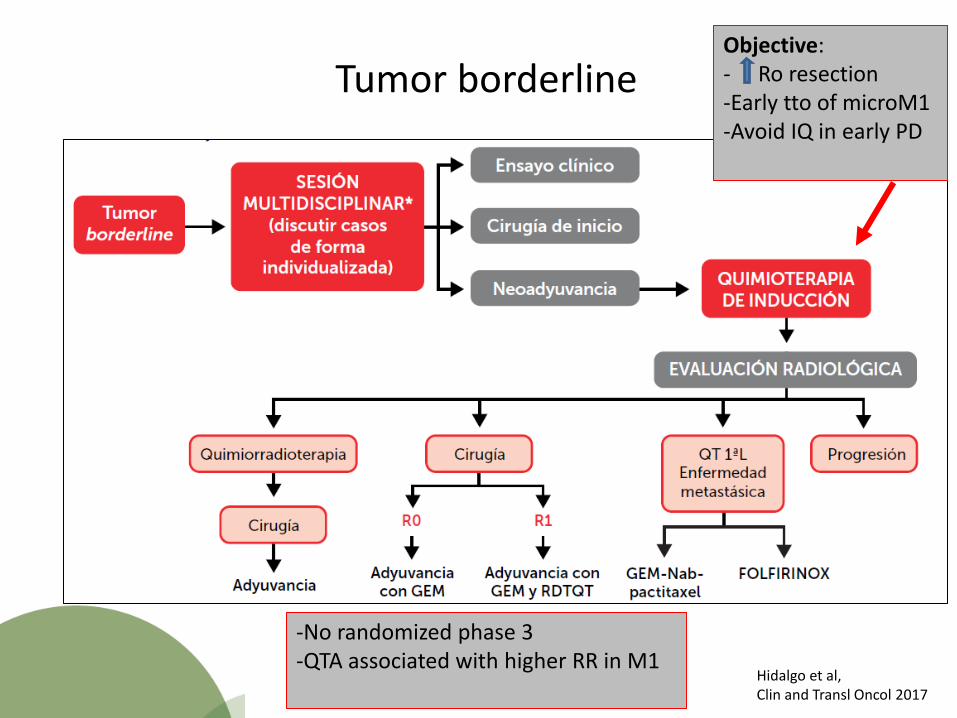
Tumor borderline
Hidalgo et al, Clin and Transl Oncol 2017
Objective: - Ro resection -Early tto of microM1 -Avoid IQ in early PD
-No randomized phase 3 -QTA associated with higher RR in M1

Tumor borderline
Lelpo et al, European Journal of Surgical Oncology
N 25 potentially resectable PA (R 14, BR 11) Resection rate N 17/25 (68%) (DPC 10, DP 4, TP 3) R0 17 (100%), 13/17(76.5%) major pathological regressions Vascular resection 6/17(35%) (PV 2, SMV 4)
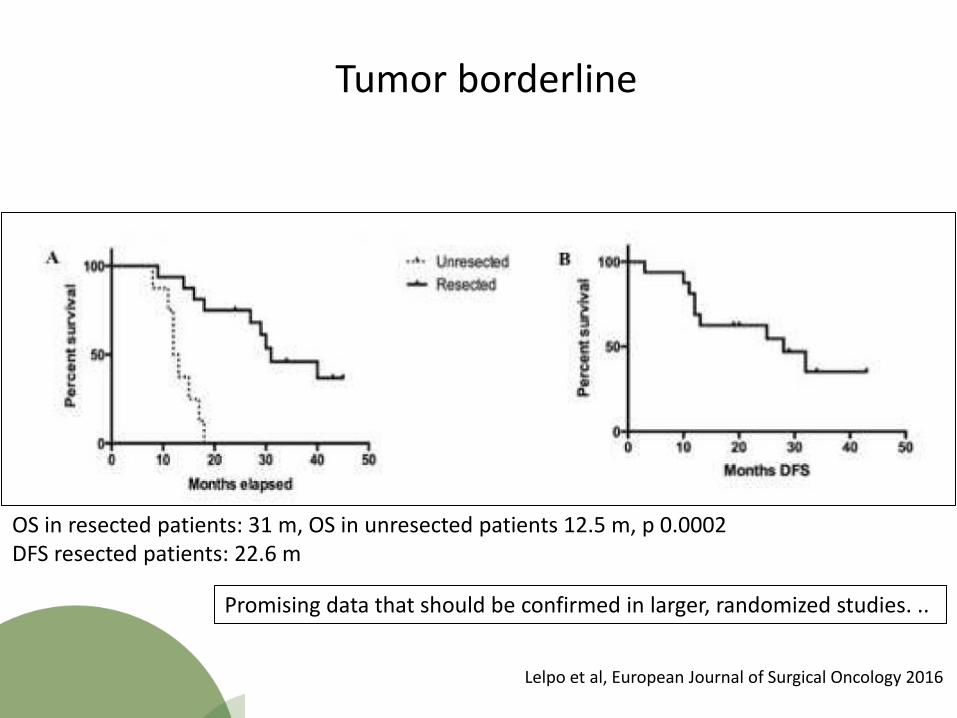
Tumor borderline
OS in resected patients: 31 m, OS in unresected patients 12.5 m, p 0.0002 DFS resected patients: 22.6 m
Lelpo et al, European Journal of Surgical Oncology 2016
Promising data that should be confirmed in larger, randomized studies. ..

Tumor irresecable
-No randomized clinical trials -Goal: Improve Survival

LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
Previously untreated,
unresectable LAPC
Planned N = 110
Induction Phase
nab-Paclitaxel 125 mg/m2 qw 3/4
+ gemcitabine
1000 mg/m2 qw 3/4
Maximum of 6 cyclesa
Investigator’s Choice
For patients without disease progression or unacceptable
toxicity • nab-Paclitaxel +
gemcitabine • Chemoradiationb
• Surgical resection
Periodic follow-up
for PFS and OS
Primary endpoint
TTF: time from first dose of study therapy to treatment failure (treatment failure defined as discontinuation of study therapy due to disease
progression, death by any cause, or the start of a nonprotocol-defined therapy)
a Surgical intervention was allowed prior to completing 6 cycles of nab-paclitaxel plus gemcitabine if deemed operable by the treating medical team. b Concurrent capecitabine or gemcitabine plus radiation according to institutional practice.
c Combined incidence of CR, PR, and SD measured at the end of the treatment visit.
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].
Secondary endpoints
• DCRc (after 6 cycles of therapy) • ORR • PFS • OS • Safety • QoL (EORTC QLQ-C30 and QLQ-PAN26)
N 47
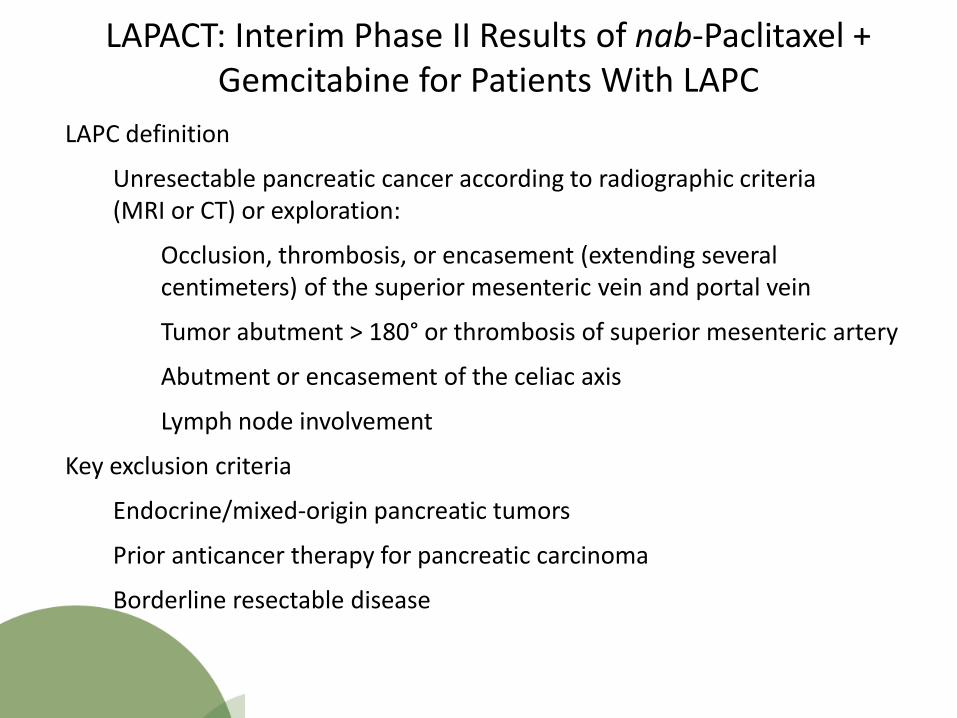
LAPC definition
Unresectable pancreatic cancer according to radiographic criteria (MRI or CT) or exploration:
Occlusion, thrombosis, or encasement (extending several centimeters) of the superior mesenteric vein and portal vein
Tumor abutment > 180° or thrombosis of superior mesenteric artery
Abutment or encasement of the celiac axis
Lymph node involvement
Key exclusion criteria
Endocrine/mixed-origin pancreatic tumors
Prior anticancer therapy for pancreatic carcinoma
Borderline resectable disease
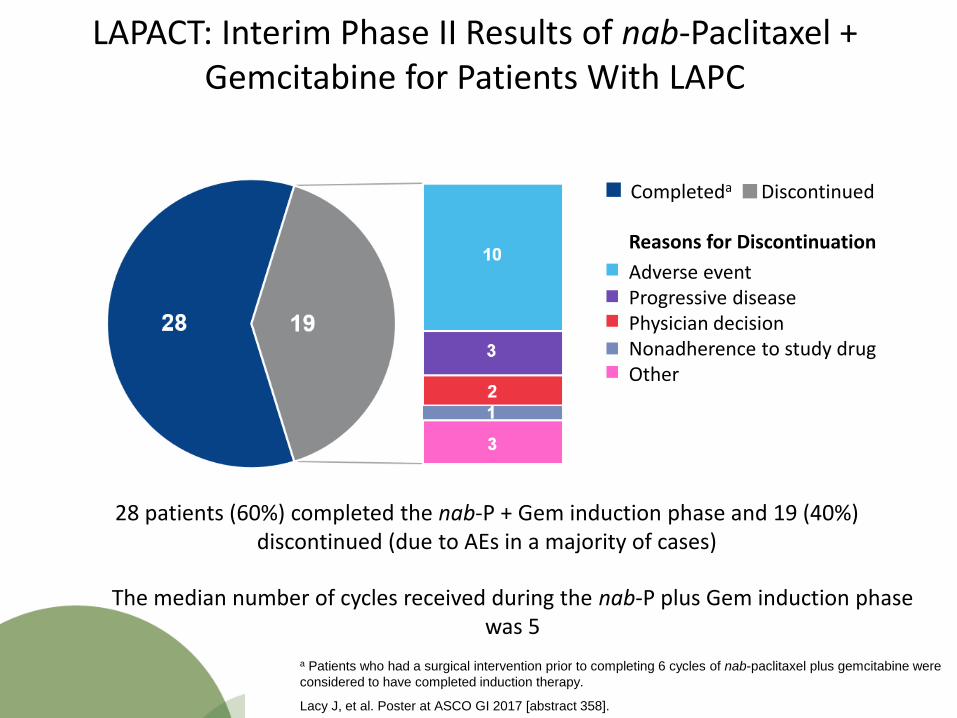
LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
Completeda Discontinued
Reasons for Discontinuation
Adverse event Progressive disease Physician decision Nonadherence to study drug Other
28 patients (60%) completed the nab-P + Gem induction phase and 19 (40%) discontinued (due to AEs in a majority of cases)
a Patients who had a surgical intervention prior to completing 6 cycles of nab-paclitaxel plus gemcitabine were
considered to have completed induction therapy.
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].
The median number of cycles received during the nab-P plus Gem induction phase was 5
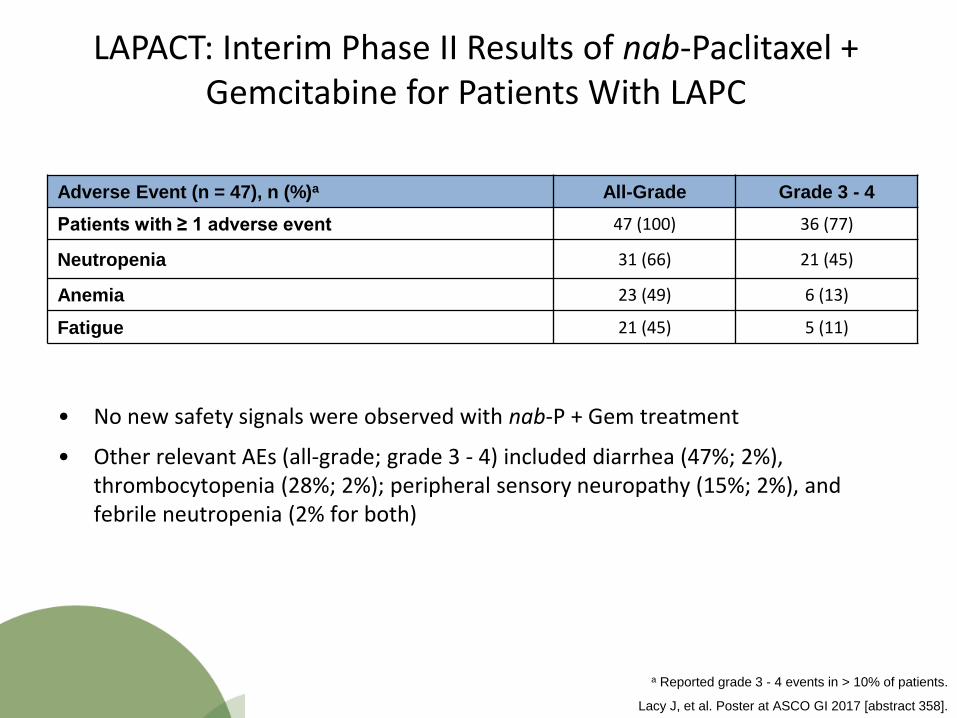
LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
Adverse Event (n = 47), n (%)a All-Grade Grade 3 - 4
Patients with ≥ 1 adverse event 47 (100) 36 (77)
Neutropenia 31 (66) 21 (45)
Anemia 23 (49) 6 (13)
Fatigue 21 (45) 5 (11)
• No new safety signals were observed with nab-P + Gem treatment
• Other relevant AEs (all-grade; grade 3 - 4) included diarrhea (47%; 2%), thrombocytopenia (28%; 2%); peripheral sensory neuropathy (15%; 2%), and febrile neutropenia (2% for both)
a Reported grade 3 - 4 events in > 10% of patients.
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].

LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
Best Response by RECIST v1.1, n (%) Efficacy Population (n = 45)a
CR 0
PR 14 (31)
All SDb
SD ≥ 16 weeks
28 (62)
22 (49)
DCR [SD ≥ weeks + CR + PR] 36 (80)
PD 3 (7)
a Includes patients who had a baseline and ≥ 1 postbaseline assessment. b Six patients had a best response of SD at 8 weeks, but response at 16 weeks could not be confirmed.
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].

LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
Chemotherapy
Chemoradiation
Surgical resection
R0
R1
R2
Deemed unresectable
during surgery
Patients (n = 21) who received investigator’s choice intervention
Six of the 47 patients (13%) had surgical tumor resection after nab-P + Gem induction
1 of 6 (17%) had an R0 resection margin
4 (67%) had an R1 resection margin
1 (17%) had an R2 resection margin
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].
LAPACT: Interim Phase II Results of nab-Paclitaxel + Gemcitabine for Patients With LAPC
• Results from this interim analysis suggest a tolerable safety profile for nab-paclitaxel plus gemcitabine; no new safety signals were identified thus far, and most patients (60%) completed the induction phase
• The 80% disease control rate for the first 47 patients to complete the nab-paclitaxel plus gemcitabine induction phase is promising and indicative of antitumor activity in patients with locally advanced pancreatic cancer
• Notably, all patients were identified as unresectable at baseline, yet 13% were resectable after the nab-paclitaxel plus gemcitabine induction phase
• Most patient-reported symptoms stabilized or improved during the induction phase
Lacy J, et al. Poster at ASCO GI 2017 [abstract 358].
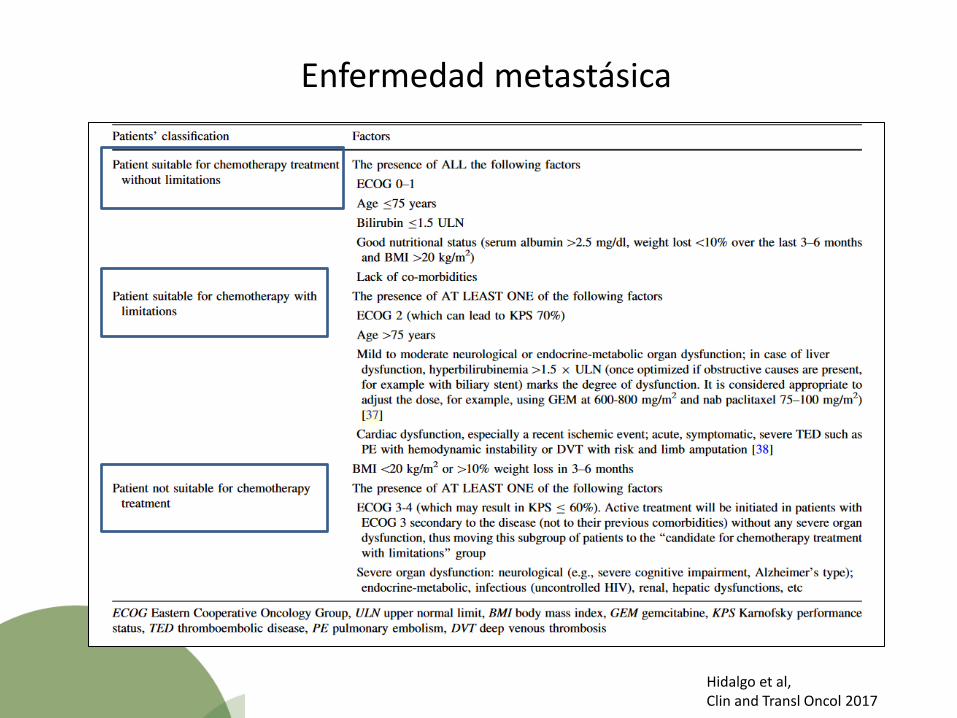
Enfermedad metastásica
Hidalgo et al, Clin and Transl Oncol 2017
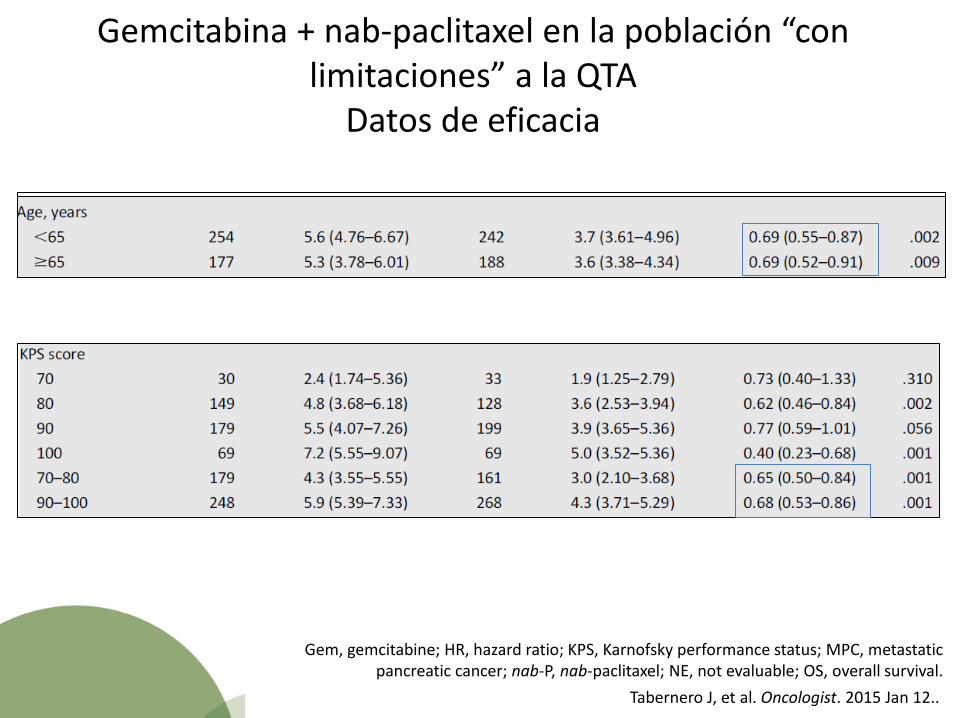
Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA
Datos de eficacia
Gem, gemcitabine; HR, hazard ratio; KPS, Karnofsky performance status; MPC, metastatic pancreatic cancer; nab-P, nab-paclitaxel; NE, not evaluable; OS, overall survival.
Tabernero J, et al. Oncologist. 2015 Jan 12..
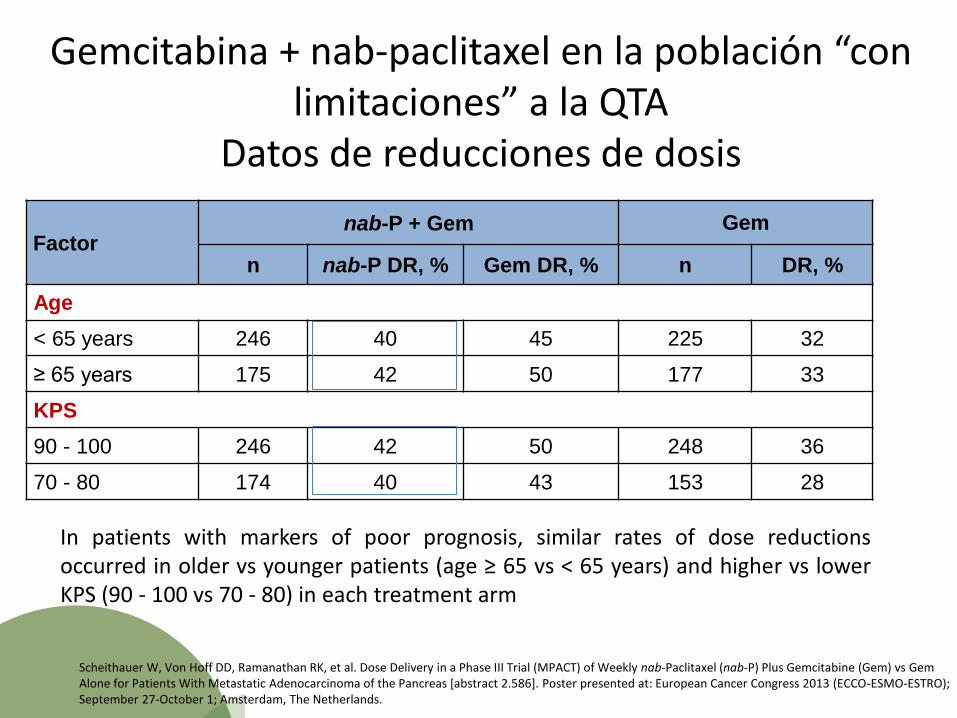
Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA
Datos de reducciones de dosis
Factor nab-P + Gem Gem
n nab-P DR, % Gem DR, % n DR, %
Age
< 65 years 246 40 45 225 32
≥ 65 years 175 42 50 177 33
KPS
90 - 100 246 42 50 248 36
70 - 80 174 40 43 153 28
• In patients with markers of poor prognosis, similar rates of dose reductions occurred in older vs younger patients (age ≥ 65 vs < 65 years) and higher vs lower KPS (90 - 100 vs 70 - 80) in each treatment arm
Scheithauer W, Von Hoff DD, Ramanathan RK, et al. Dose Delivery in a Phase III Trial (MPACT) of Weekly nab-Paclitaxel (nab-P) Plus Gemcitabine (Gem) vs Gem Alone for Patients With Metastatic Adenocarcinoma of the Pancreas [abstract 2.586]. Poster presented at: European Cancer Congress 2013 (ECCO-ESMO-ESTRO); September 27-October 1; Amsterdam, The Netherlands.
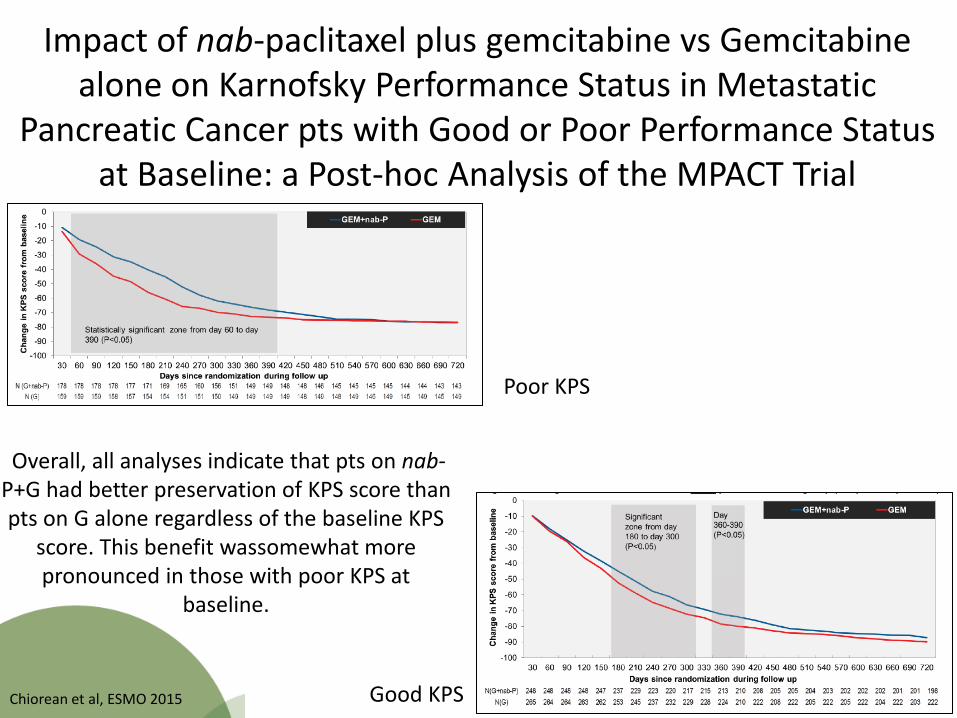
Impact of nab-paclitaxel plus gemcitabine vs Gemcitabine alone on Karnofsky Performance Status in Metastatic
Pancreatic Cancer pts with Good or Poor Performance Status at Baseline: a Post-hoc Analysis of the MPACT Trial
Poor KPS
Good KPS
Overall, all analyses indicate that pts on nab-P+G had better preservation of KPS score than pts on G alone regardless of the baseline KPS
score. This benefit wassomewhat more pronounced in those with poor KPS at
baseline.
Chiorean et al, ESMO 2015
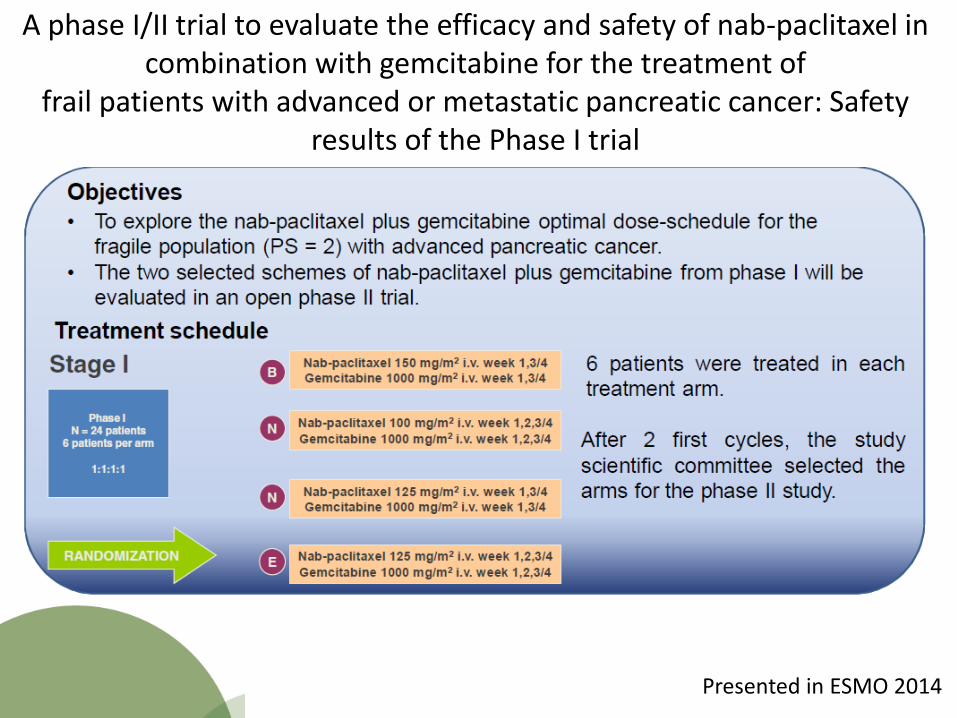
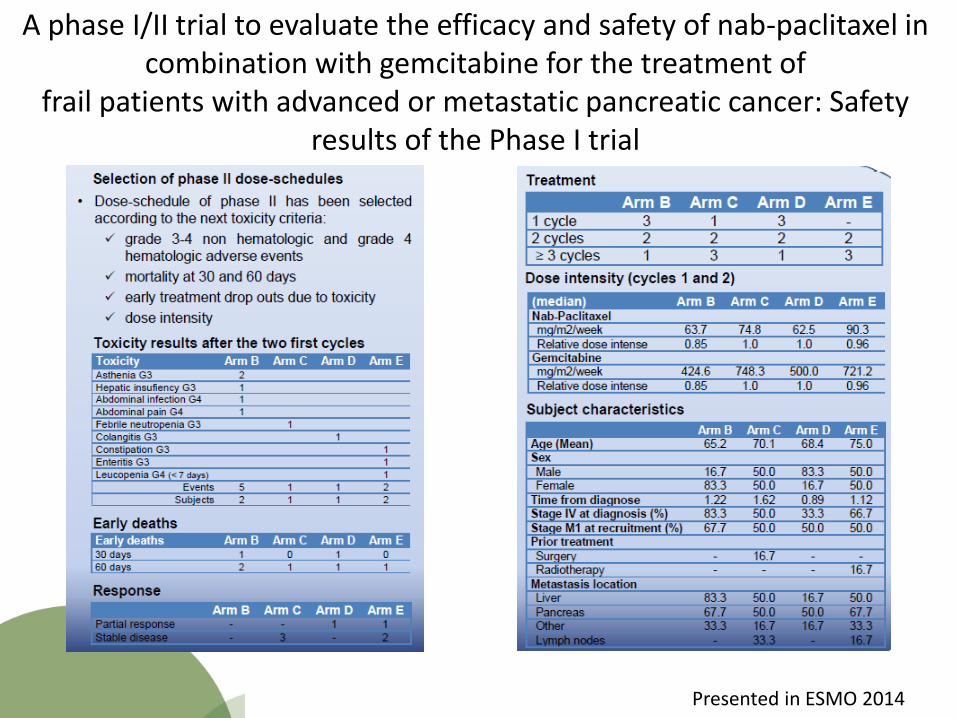
A phase I/II trial to evaluate the efficacy and safety of nab-paclitaxel in combination with gemcitabine for the treatment of
frail patients with advanced or metastatic pancreatic cancer: Safety results of the Phase I trial
Presented in ESMO 2014
A phase I/II trial to evaluate the efficacy and safety of nab-paclitaxel in combination with gemcitabine for the treatment of
frail patients with advanced or metastatic pancreatic cancer: Safety results of the Phase I trial
Presented in ESMO 2014

A phase I/II trial to evaluate the efficacy and safety of nab-paclitaxel in combination with gemcitabine for the treatment of
frail patients with advanced or metastatic pancreatic cancer: Safety results of the Phase I trial
Presented in ESMO 2014
A phase I and randomized phase II trial to evaluate the efficacy and safety of nab-paclitaxel (nab-P) in combination with gemcitabine (G) for the treatment of patients with ECOG 2
advanced pancreatic cancer (PDAC).
Next steps…Abstract has been sent to ESMO 2017
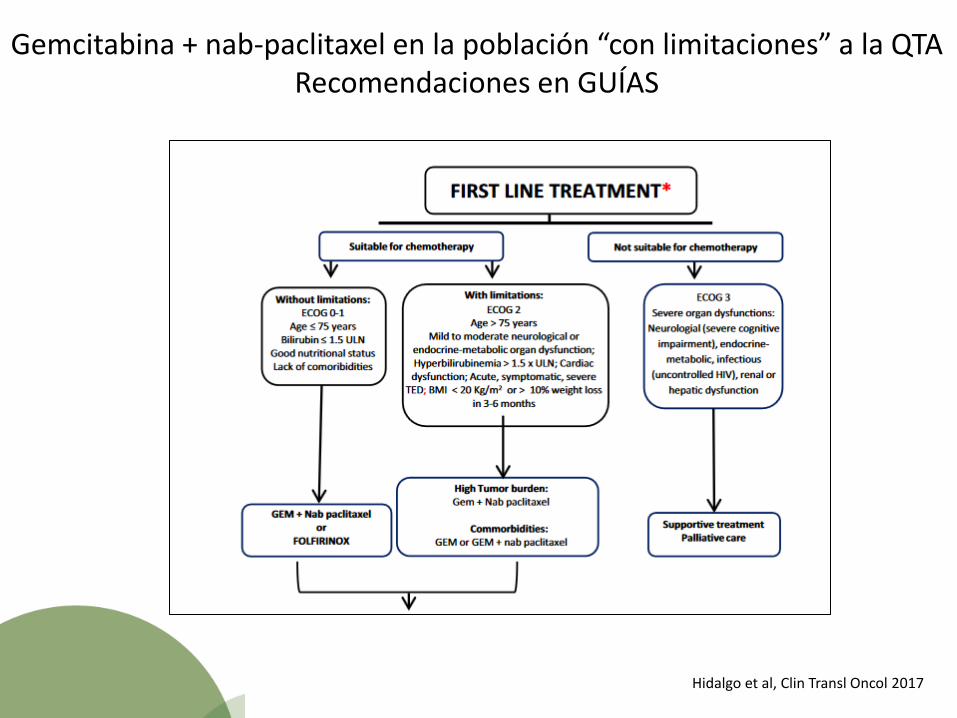
Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA Recomendaciones en GUÍAS
Hidalgo et al, Clin Transl Oncol 2017
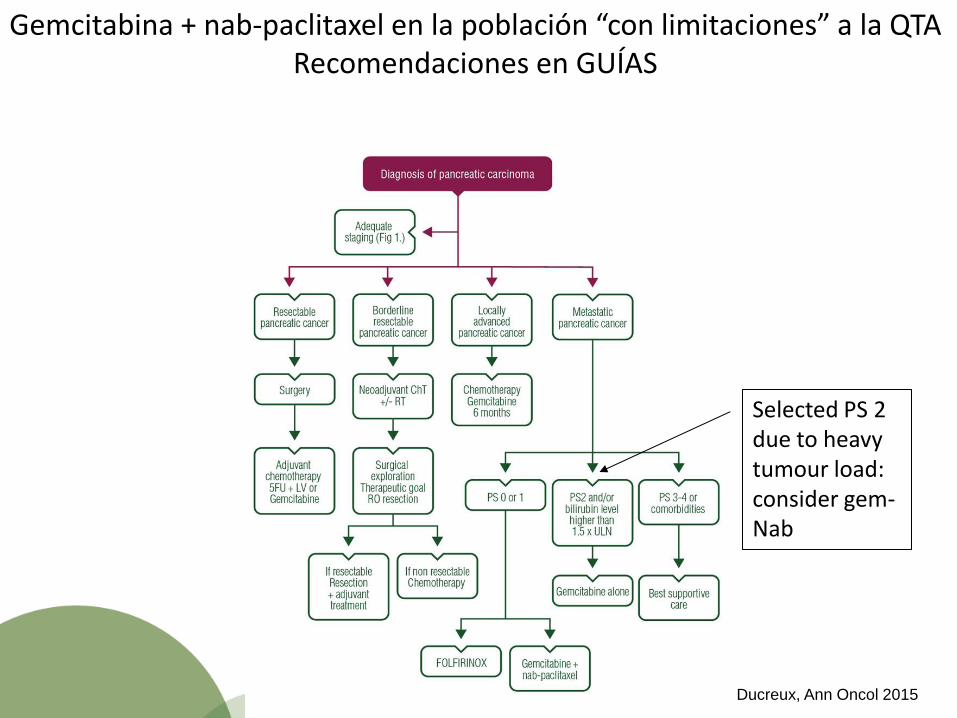
Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA Recomendaciones en GUÍAS
Selected PS 2 due to heavy tumour load: consider gem-Nab
Ducreux, Ann Oncol 2015

Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA: Recomendaciones en GUÍAS
Gemcitabine + albumin-bound paclitaxel is reasonable for patients with KPS ≥ 70

Gemcitabina + nab-paclitaxel en la población “con limitaciones” a la QTA Recomendaciones en GUÍAS
Fig. 1 *Comorbidities, cognition, mental health status and support, fatigue, assessment of
polypharmacy, and the
presence of geriatric syndromes.
**The efficacy of GEM/nabpaclitaxel over gemcitabine in this specific subgroup of patients is
currently insufficient
Vera et al, Clin Trans Oncol 2016

Conclusiones
• El cáncer de páncreas presenta alta mortalidad, constituyendo la cuarta causa de muerte por cáncer.
• En los últimos años dos nuevos esquemas de tratamiento han demostrado un aumento de la supervivencia respecto a la gemcitabina: FOLFIRINOX y nab-paclitaxel+gemcitabina.
• El papel de nab-paclitaxel en adjuvancia está pendiente de los resultados del estudio APACT.
• Experiencias unicéntricas han demostrado eficacia de gemcitabina y nab-paclitaxel en el contexto de la neoadjuvancia: necesidad de estudios clínicos multicéntricos y randomizados en este contexto.

Conclusiones
• Datos preliminares del estudio LAPACT demuestran eficacia de la combinación de gemcitabina y nab-paclitaxel en el CP LA. Resultados completos en ESMO 2017.
• Sub-análisis del estudio MPACT indican igual eficacia y tolerabilidad de gemcitabina y nab-paclitaxel en los pacientes “con limitaciones” que la población general del estudio.
• Datos del estudio fragance (ESMO 2017) nos permitirán tener datos de la combinación en la población ECOG 2 (dosis, eficacia y tolerabilidad).
• Todas las guías de manejo de cáncer de páncreas incluyen la población “ con limitaciones a la quimioterapia” y consideran la acción de que esta población se trate con gemcitabina y nab-paclitaxel.