nuove (e molte !) terapie per la sclerosi multipla. mario ... · nuove (e molte !) terapie per la...
TRANSCRIPT

Nuove (e molte !) terapie per la sclerosi multipla.
Mario Falcini
UO. Neurologia - Prato
«Gli uomini sono molto inventivi. Hanno
inventato tutte queste macchine e l’era
industriale, ma non hanno nessuna idea di
come migliorare il mondo».
Niki de Saint Phalle

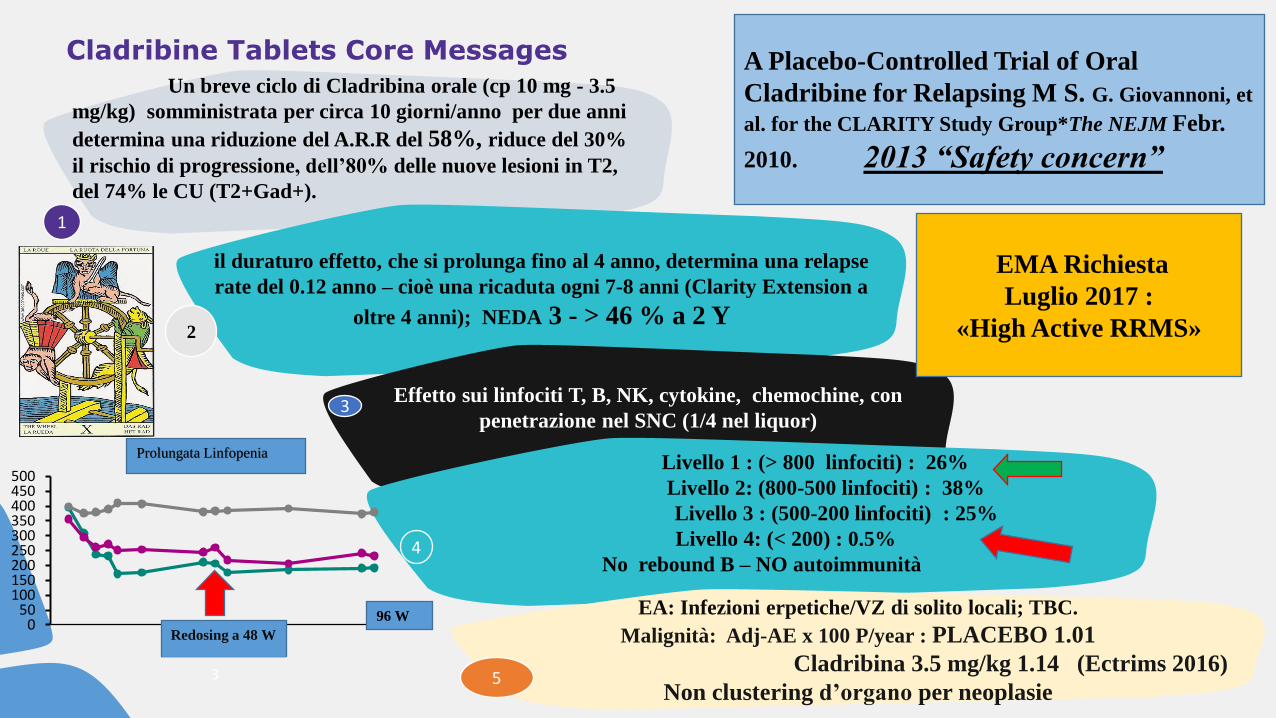
Cladribine Tablets Core Messages
3
Un breve ciclo di Cladribina orale (cp 10 mg - 3.5
mg/kg) somministrata per circa 10 giorni/anno per due anni
determina una riduzione del A.R.R del 58%, riduce del 30%
il rischio di progressione, dell’80% delle nuove lesioni in T2,
del 74% le CU (T2+Gad+).
il duraturo effetto, che si prolunga fino al 4 anno, determina una relapse
rate del 0.12 anno – cioè una ricaduta ogni 7-8 anni (Clarity Extension a
oltre 4 anni); NEDA 3 - > 46 % a 2 Y
Effetto sui linfociti T, B, NK, cytokine, chemochine, con
penetrazione nel SNC (1/4 nel liquor)
Livello 1 : (> 800 linfociti) : 26%
Livello 2: (800-500 linfociti) : 38%
Livello 3 : (500-200 linfociti) : 25%
Livello 4: (< 200) : 0.5%
No rebound B – NO autoimmunità
EA: Infezioni erpetiche/VZ di solito locali; TBC.
Malignità: Adj-AE x 100 P/year : PLACEBO 1.01
Cladribina 3.5 mg/kg 1.14 (Ectrims 2016)
Non clustering d’organo per neoplasie
1
2
3
5
4
A Placebo-Controlled Trial of Oral
Cladribine for Relapsing M S. G. Giovannoni, et
al. for the CLARITY Study Group*The NEJM Febr.
2010. 2013 “Safety concern”
050
100150200250300350400450500
96 W
Redosing a 48 W
Prolungata Linfopenia
EMA Richiesta
Luglio 2017 :
«High Active RRMS»

Siponimod SP 1-5 modulator : Phase III program (EXPAND): first positive results (ECTRIMS 2016) The study included 1,651
people with SPMS
• Treatment with BAF312 reduced the risk of three-month confirmed disability progression by 21% compared with placebo (p=0.013). The risk reduction for six-month confirmed disability progression was greater, further supporting robustness of the data.[1]
• A consistent reduction in the risk of confirmed disability progression across predefined subgroups, including patients without relapses.[1]
• A significant difference in favor of BAF312 compared to placebo in annualized relapse rate, the percent change in brain volume, and change from baseline in the volume of T2 lesions (brain lesions identified by a T2-weighted magnetic resonance imaging scan). Difference in change from baseline in the Timed 25-Foot Walk test (T25FW) was not significant.[1]
• BAF312 was generally safe and well tolerated, with a profile comparable to other drugs in the same class.[1]
Limphocitic count: rapid recover at 90% baseline
Titration over 9 or 10 days dose of 10 mg successfully
attenuates the initial bradycardia L. Kappos

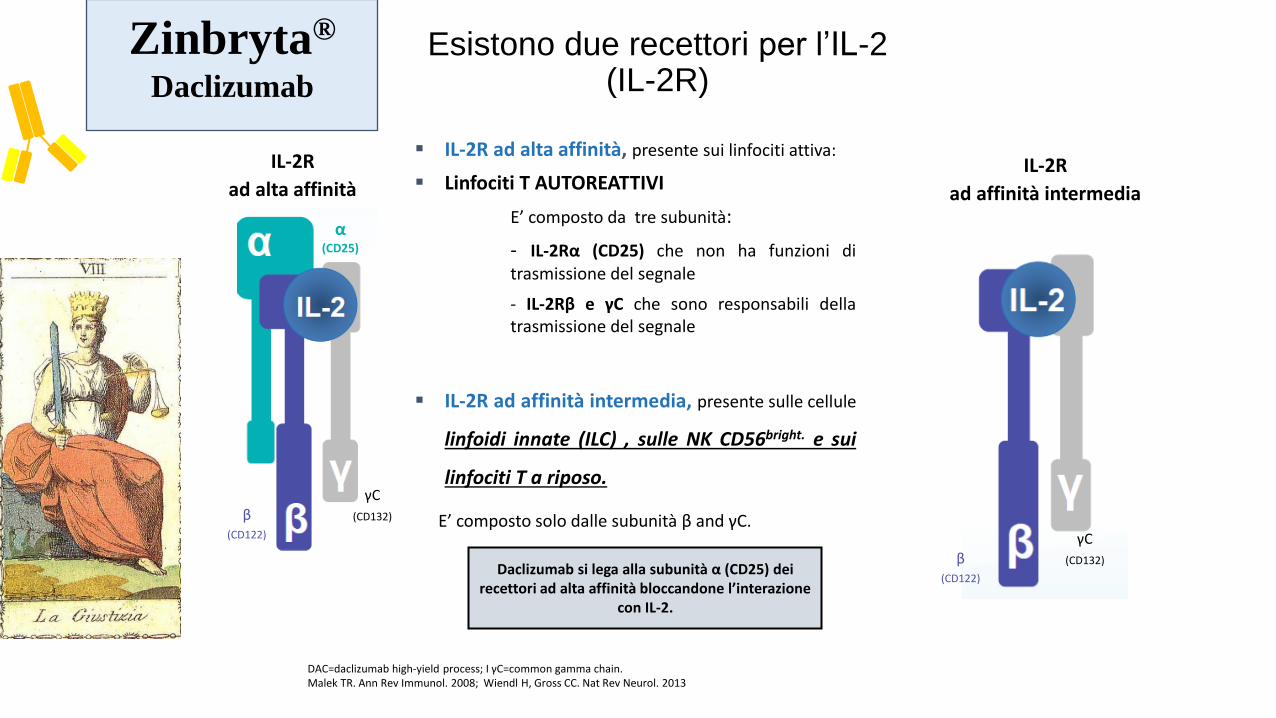
Esistono due recettori per l’IL-2 (IL-2R)
DAC=daclizumab high-yield process; I γC=common gamma chain. Malek TR. Ann Rev Immunol. 2008; Wiendl H, Gross CC. Nat Rev Neurol. 2013
α (CD25)
β (CD122)
γC
(CD132)
β
IL-2R
ad alta affinità
IL-2R ad alta affinità, presente sui linfociti attiva:
Linfociti T AUTOREATTIVI
E’ composto da tre subunità:
- IL-2Rα (CD25) che non ha funzioni di trasmissione del segnale
- IL-2Rβ e γC che sono responsabili della trasmissione del segnale
IL-2R ad affinità intermedia, presente sulle cellule
linfoidi innate (ILC) , sulle NK CD56bright. e sui
linfociti T a riposo.
E’ composto solo dalle subunità β and γC.
Daclizumab si lega alla subunità α (CD25) dei recettori ad alta affinità bloccandone l’interazione
con IL-2.
IL-2R
ad affinità intermedia
β (CD122)
γC
(CD132)
Zinbryta®
Daclizumab

SELECT trilogy e DECIDE/EXTEND: Disegni degli studi
1. Gold R, et al. Lancet. 2013; 2. Giovannoni G, et al. Lancet Neurol. 2014; 3. Gold R, et al. BMC Neurol. 2016; 4. Kappos L, et al. N Engl J Med. 2015; 5. Clinical Trials identifier: NCT01797965.
Daclizumab 300 mg SC q4w (n=84)
SELECT1 SELECTION2
1 year (Weeks 0–52)
Daclizumab 150 mg SC q4w (n=86)
Daclizumab 300 mg SC q4w (n=87)
Daclizumab 150 mg SC q4w (n=86)
1 year (Weeks 0–52)
Placebo SC q4w
(n=204)
Daclizumab 150 mg SC
q4w (n=208)
Daclizumab 300 mg SC
q4w (n=209)
Daclizumab 150 mg SC q4w
open label (N=410)
SELECTED3
Up to 6.5 years
IFN beta-1a 30 mg IM every week (n=922)
Daclizumab 150 mg SC q4w (n=919)
DECIDE4
2–3 years (Weeks 0 to 96–144)
Daclizumab 150 mg SC q4w
open label (N=1501)
EXTEND5
Up to 5 years
24-week washout (n=86)
24-week washout (n=88)
Daclizumab 150 mg SC q4w
Daclizumab 300 mg SC q4w
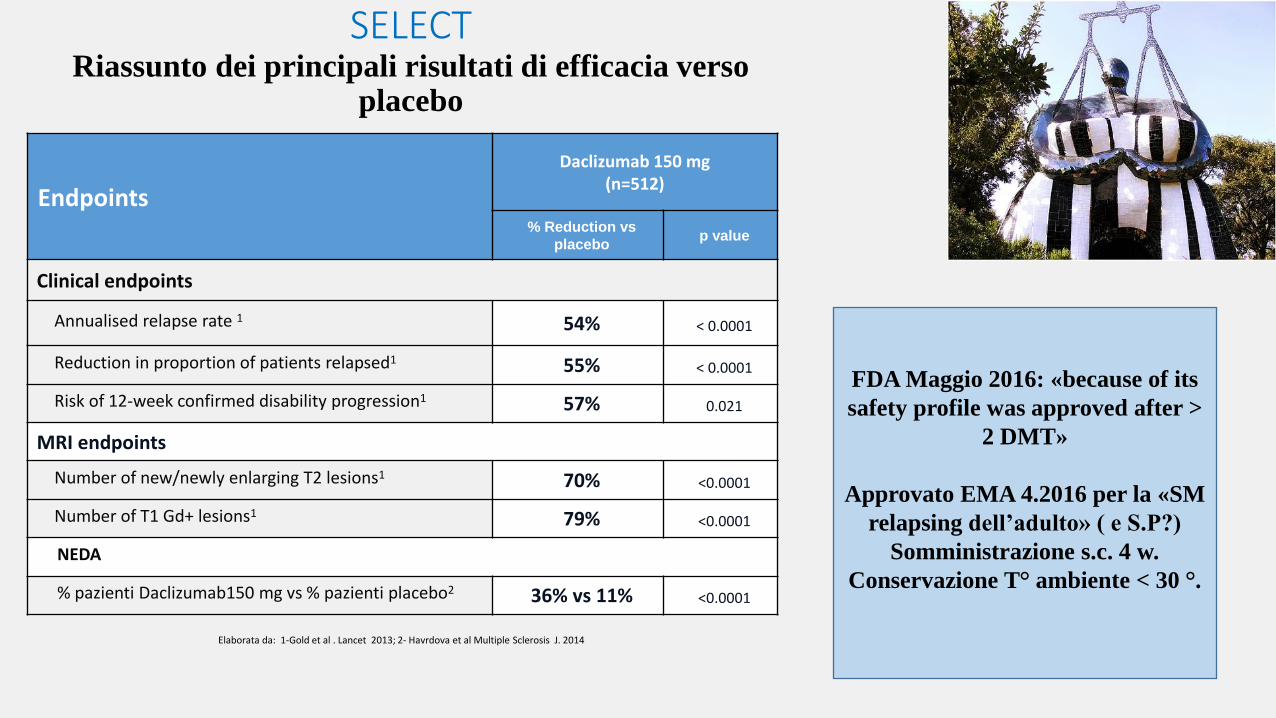
Endpoints
Daclizumab 150 mg (n=512)
% Reduction vs
placebo p value
Clinical endpoints
Annualised relapse rate 1 54% < 0.0001
Reduction in proportion of patients relapsed1 55% < 0.0001
Risk of 12-week confirmed disability progression1 57% 0.021
MRI endpoints
Number of new/newly enlarging T2 lesions1 70% <0.0001
Number of T1 Gd+ lesions1 79% <0.0001
NEDA
% pazienti Daclizumab150 mg vs % pazienti placebo2 36% vs 11% <0.0001
Elaborata da: 1-Gold et al . Lancet 2013; 2- Havrdova et al Multiple Sclerosis J. 2014
SELECT Riassunto dei principali risultati di efficacia verso
placebo
FDA Maggio 2016: «because of its
safety profile was approved after >
2 DMT»
Approvato EMA 4.2016 per la «SM
relapsing dell’adulto» ( e S.P?)
Somministrazione s.c. 4 w.
Conservazione T° ambiente < 30 °.

Govannoni et al ECTRIMS 2016
Pazienti NEDA 3 Daclizumab vs IFNβ1a (DECIDE)
NEDA SELECT : 36% DACLIZUMAB
vs Placebo 11%, a 52 W
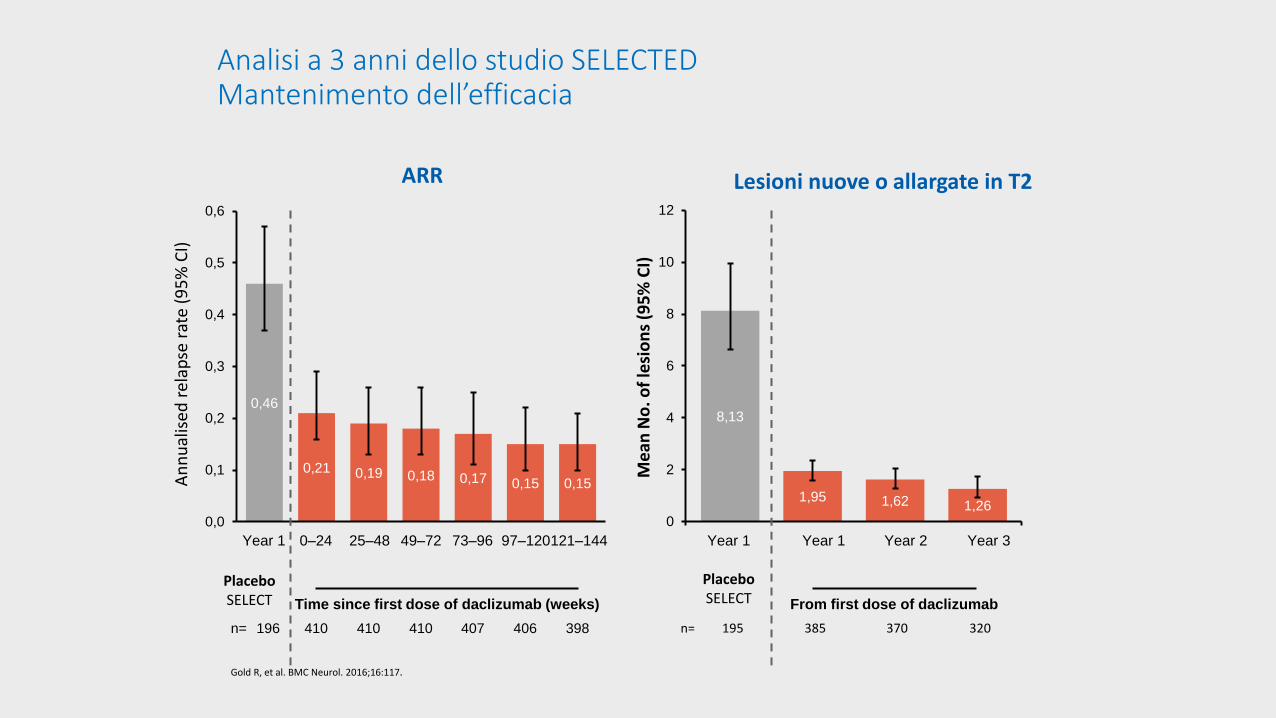
Analisi a 3 anni dello studio SELECTED Mantenimento dell’efficacia
Gold R, et al. BMC Neurol. 2016;16:117.
0,46
0,21 0,19 0,18 0,17 0,15 0,15
0,0
0,1
0,2
0,3
0,4
0,5
0,6
Year 1
n= 196 410 407 398
Time since first dose of daclizumab (weeks)
0–24 25–48 49–72
410 406 410
73–96 97–120 121–144
An
nu
alis
ed r
elap
se r
ate
(95
% C
I)
Placebo SELECT
ARR Lesioni nuove o allargate in T2
8,13
1,95 1,62 1,26 0
2
4
6
8
10
12
Year 1
n= 195 385 370 320
From first dose of daclizumab
Year 1 Year 2 Year 3
Placebo SELECT
Me
an N
o. o
f le
sio
ns
(95
% C
I)
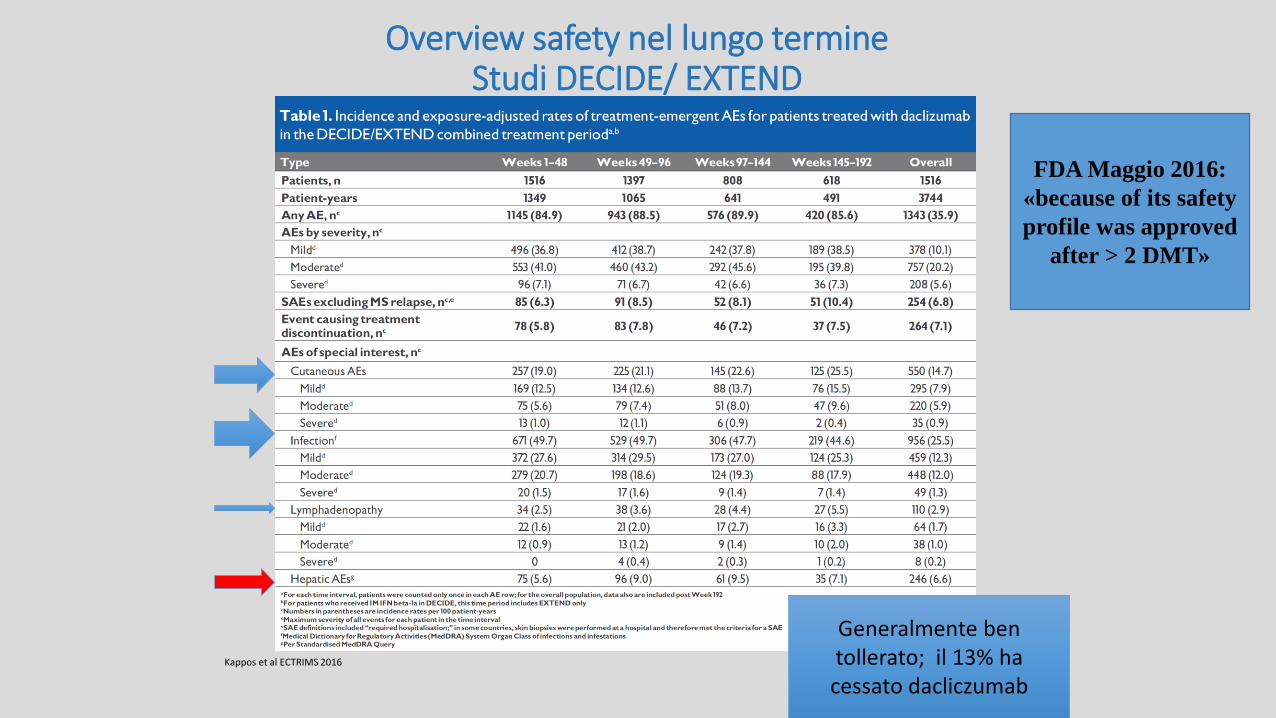
Overview safety nel lungo termine
Studi DECIDE/ EXTEND
Kappos et al ECTRIMS 2016
Generalmente ben tollerato; il 13% ha cessato dacliczumab
FDA Maggio 2016:
«because of its safety
profile was approved
after > 2 DMT»

Reazioni cutanee
1. Giovannoni G, et al. Mult Scler Rel Dis. 2016;9:36–46; 2. Zinbryta® (daclizumab) SmPC. July 2016; 3. Kappos L, et al. N Engl J Med. 2015;373:1418–28; 4. Krueger JG, et al. Adv Ther. 2016;33:1231–45.
INTEGRATED SAFETY
ANALYSIS1,2
DECIDE (2-3 y, vs IFN beta-1a)1–3
Daclizumab 150 mg
n=1943
IM IFN beta-1a n=922
Daclizumab 150 mg n=919
Skin reactions, % 32 19 37
Serious skin reactions, % 2 <1 2
Discontinuation due to skin reactions, % 4 1 5
• Nel DECIDE l’incidenza degli eventi valutati come correlati al trattamento è stata del 7% nel gruppo IFN beta-1a e del 15% nel gruppo daclizumab4
• Nei pazienti trattati con daclizumab gli eventi cutanei più comuni sono stati il rash, la dermatite e l’eczema,
dermatite allergica, psoriasi, acne e nei casi moderati o severi si sono usati corticosteroidi topici o
sistemici 4 . Nel DECIDE, la maggior parte degli eventi (94%) associati a daclizumab sono stati di gravità lieve o moderata 2,4Reazioni gravi sono state n=3) eruzione tossica e l’angioedema (n=2)4
1/3 dei casi

Eventi epatici: monitoraggio addizionale e gestione (un caso mortale di epatite autoimmune)
Zinbryta® (daclizumab) RCP 23 9 16 .
• Valutare livelli transaminasi (ALT e AST) e bilirubina sierica
• Si raccomanda di non iniziare il trattamento se: Al basale le transaminasi (ALT o AST) sono >2× ULN (possibile se < x 2) Pre-esistente insufficienza epatica severa (Child–Pugh class C) * “assicurarsi che il pz comprenda il rischio di danno epatico severo” e il concorso
eventuale di altri farmaci epatotossici . No problem con induttori citocromi CYP nè con sintomatici SM (es. 4-aminopiridina).
Durante il trattamento Alla
sospensione Prima di iniziare
Il trattamento
SCHEDA per il Paziente - contattare il medico se: nausea, vomito, dolore allo
stomaco, aumento stanchezza, anoressia, urine color thè, ittero. «Procedure per assistenza medica fuori orario»
Epatotossicità
16%

Durante il trattamento Alla
sospensione Prima di iniziare
il trattamento
• Valutare ALT e AST una volta al mese durante il trattamento e fino a 4 mesi dopo l’ultima dose
ALT o AST >3× ULN
Sospensione trattamento e stretto monitoraggio
Ripresa trattamento quando ALT o AST <2× ULN
Interruzione del trattamento*
ALT o AST >5× ULN oppure
ALT o AST > 3 x ULN & bilirubina >2 x ULN
*Si può considerare di ricominciare la terapia qualora si scoprano altre eziologie, i valori siano tornati normali e i benefici siano superiori ai
rischi RCP Zinbryta
Eventi epatici: monitoraggio e gestione

anticorpi ANTI CD 20
Murine
Chimeric
Humanized
Human
Mouse sequence
Human sequence
Ofatumumab
Ocrelizumab
Rituximab
aggregati ectopici simil follicolari
Presentazione antigene
Anticorpi

Targeting CD20+ B cells may preserve B cell reconstitution and long-term immune memory
Adapted from Krumbholz M, et al. Nat Rev Neurol 2012;8(11):613–23. 1. Hauser SL. Mult Scler 2015;21(1):8–21. 2. Pescovitz MD. Am J Transplant 2006;6(5 pt 1):859–66. 3. Leandro MJ, et al. Arthritis Rheum 2006;54(2):613–20. 4. DiLillo DJ, et al. J Immunol 2008;180(1):361–71.
B-cell Reconstitution1-3
v
Long-term Immune Memory1,2,4
Ocrelizumab is a humanised monoclonal antibody that selectively depletes CD20+ B cells

Ofatumumab Phase II Data in RRMS (MIRROR study results)
Dose dependent depletion of CD19 B cells was observed.
The q12w regimen was associated with partial repletion of B-cells during the dosing interval.
1st treatment cycle
Repeated, subcutaneous low doses of ofatumumab were associated with marked reduction of MRI activity
SC Dose Weeks 0-12 (new lesions)
Weeks 4-12 (new lesions)
3mg q12w
65%↓ (p<0.001)
71%↓ (p=0.002)
30mg q12w 90%↓ (p<0.001)
60mg q12w 91%↓ (p<0.001)
60mg q4w 92%↓ (p<0.001)
MRI Data:
Cumulative # of
GdE-T1 Lesions;
Effect vs Placebo
2nd treatment cycle
Amit Bar-Or et al. - Neurology April 8, 2014 vol. 82 no. 10 Supplement S23.006
ASCLEPIOS I – II (30 mg/4w vs TERIFLUNOMIDE) RMS (RR e SPMS) -> 2019
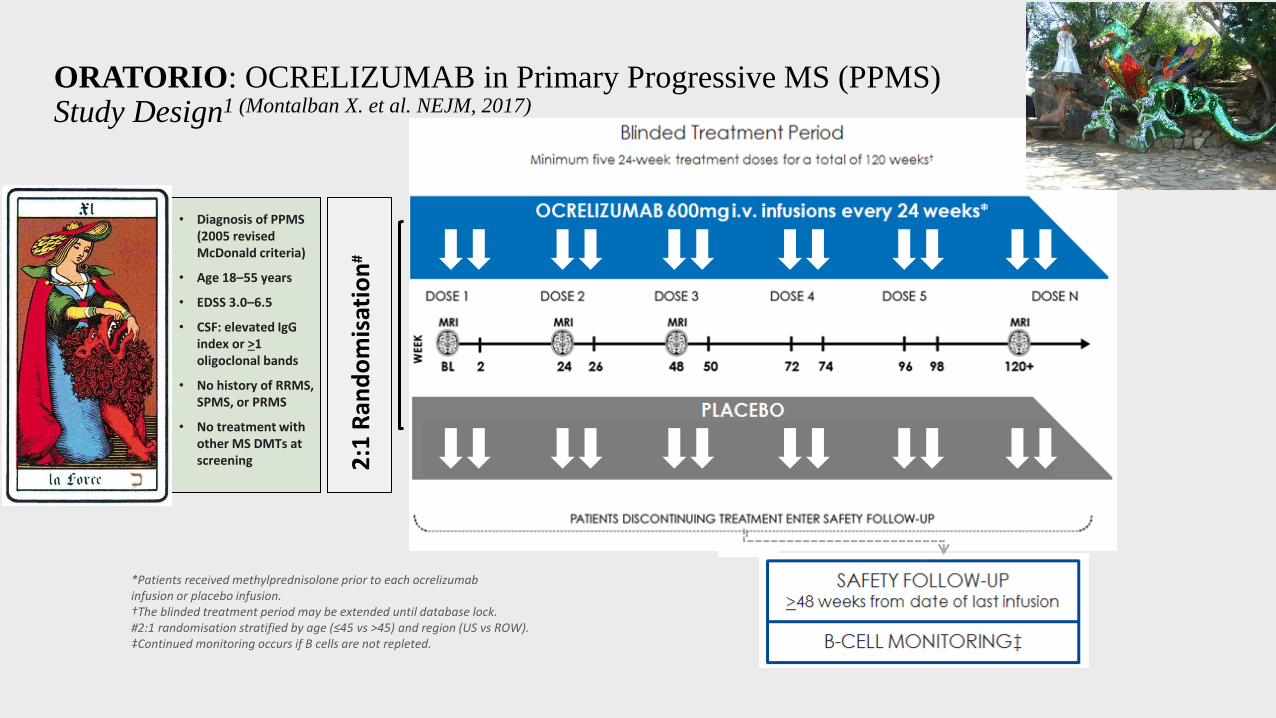
ORATORIO: OCRELIZUMAB in Primary Progressive MS (PPMS) Study Design1 (Montalban X. et al. NEJM, 2017)
• Diagnosis of PPMS (2005 revised McDonald criteria)
• Age 18–55 years
• EDSS 3.0–6.5
• CSF: elevated IgG index or >1 oligoclonal bands
• No history of RRMS, SPMS, or PRMS
• No treatment with other MS DMTs at screening 2
:1 R
and
om
isat
ion
#
*Patients received methylprednisolone prior to each ocrelizumab infusion or placebo infusion. †The blinded treatment period may be extended until database lock. #2:1 randomisation stratified by age (≤45 vs >45) and region (US vs ROW). ‡Continued monitoring occurs if B cells are not repleted.
ORATORIO: Study objectives and endpoints
Objectives
• To evaluate the efficacy and safety of ocrelizumab compared with placebo in patients with PPMS
Primary endpoint
• 12-week “confirmed disability progression (CDP)”
Key secondary endpoints
• 24-week CDP
• Timed 25-foot walk (baseline to Week 120)
• T2 lesion volume (baseline to Week 120)
• Whole brain volume (Week 24 to Week 120)
Adapted from Montalban X. et al. Presented at the American Academy of Neurology 2015 - 67th Annual Meeting | AAN. Poster P 7.017.

Time to onset of 12 and 24 week confirmed disability progression
Wolinsky J. et al.; Presented at Americas Committee for Treatment and Research in Multiple Sclerosis - 2016 Forum | ACTRIMS. Platform presentation number LB1.3

Secondary endpoint: Significant reduction in T2 lesion volume from baseline to Week 120
Montalban X, et al. Presented at the 31st Congress of the European Committee for Treatment and Research in Multiple Sclerosis 2015. Platform Presentation number 228.
n
Placebo 234 233 220 183
Ocrelizumab 464 459 454 400
p<0.0001*
On placebo, T2 lesion volume increases by 7.4% Ocrelizumab 600 mg decreases T2 lesion volume by 3.4%
Change of whole brain volume from Week 24 to Week 120
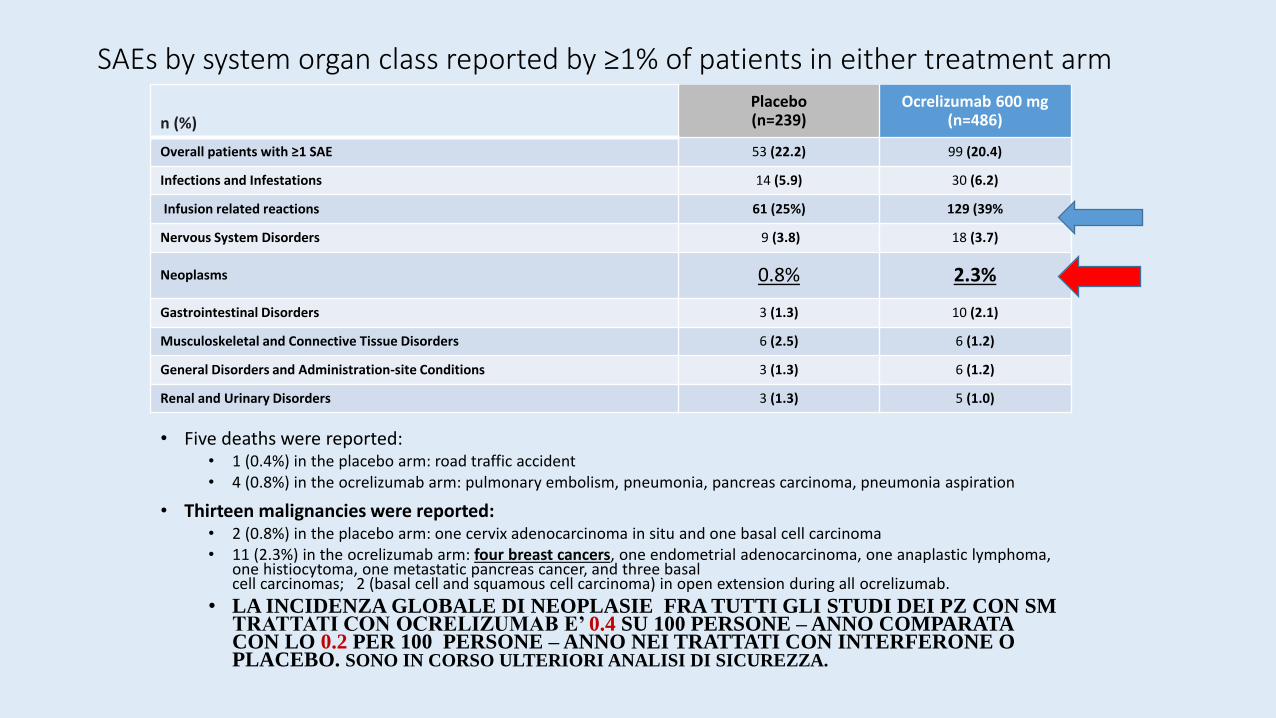
SAEs by system organ class reported by ≥1% of patients in either treatment arm
• Five deaths were reported: • 1 (0.4%) in the placebo arm: road traffic accident • 4 (0.8%) in the ocrelizumab arm: pulmonary embolism, pneumonia, pancreas carcinoma, pneumonia aspiration
• Thirteen malignancies were reported: • 2 (0.8%) in the placebo arm: one cervix adenocarcinoma in situ and one basal cell carcinoma • 11 (2.3%) in the ocrelizumab arm: four breast cancers, one endometrial adenocarcinoma, one anaplastic lymphoma,
one histiocytoma, one metastatic pancreas cancer, and three basal cell carcinomas; 2 (basal cell and squamous cell carcinoma) in open extension during all ocrelizumab.
• LA INCIDENZA GLOBALE DI NEOPLASIE FRA TUTTI GLI STUDI DEI PZ CON SM TRATTATI CON OCRELIZUMAB E’ 0.4 SU 100 PERSONE – ANNO COMPARATA CON LO 0.2 PER 100 PERSONE – ANNO NEI TRATTATI CON INTERFERONE O PLACEBO. SONO IN CORSO ULTERIORI ANALISI DI SICUREZZA.
n (%)
Placebo (n=239)
Ocrelizumab 600 mg (n=486)
Overall patients with ≥1 SAE 53 (22.2) 99 (20.4)
Infections and Infestations 14 (5.9) 30 (6.2)
Infusion related reactions 61 (25%) 129 (39%
Nervous System Disorders 9 (3.8) 18 (3.7)
Neoplasms 0.8% 2.3%
Gastrointestinal Disorders 3 (1.3) 10 (2.1)
Musculoskeletal and Connective Tissue Disorders 6 (2.5) 6 (1.2)
General Disorders and Administration-site Conditions 3 (1.3) 6 (1.2)
Renal and Urinary Disorders 3 (1.3) 5 (1.0)

FINGOLIMOD
INFORMS study
OCRELIZUMAB
ORATORIO study
Eta’ media Età mediana
48.5 (42% > 50y) 49
44.7* 46
Durata di malattia ys. (dai sintomi)
5.8 6.7
Pz. Gadolinio + 14% 27% *
N. Lesioni Gadolinio + media
0.3 1.2 *
T2 volume load (cm3) 13 9.4
EDSS medio baseline 4.7 4.7
END point 1° CDP at composite (EDSS+25TWT+9HPT)
CDP - EDSS
Olympus P.P. trial group. Wawker K. et al 2009, Neurology
Differences in time to CDP between rituximab and placebo did not reach significance (96-week rates: 38.5% placebo, 30.2% rituximab). From baseline to week 96, rituximab patients had less (p < 0.001) increase in T2 lesion volume; brain volume change was similar (p = 0.62) to
placebo. Subgroup analysis showed time to CDP was delayed in rituximab-treated patients aged <51 years - those with gadolinium +
enhancing lesions and those aged <51 years AND gadolinium-enhancing lesions compared with placebo.
«A glimmer of hope» . Hartung H.
2009.

OPERA I and II: Two identical studies evaluating the efficacy and safety of
ocrelizumab versus Interferon Beta 1-a s.c. in RMS (Hauser S.L. et al. NEJM, 2017)
• RMS diagnosis • 18–55 yrs • ≥2 clinical
relapses within last 2 yrs or 1 relapse in last yr
• EDSS of 0.0–5.5
1:1
Ran
do
mis
atio
n
OLE
OLE
scr
ee
nin
g p
eri
od
Safety follow-up ≈48 weeks from date of last infusion
B-cell monitoring‡

Primary endpoint: significant reduction in ARR compared with IFN β-1a
0,292
0,156
0,0
0,1
0,2
0,3
0,4
0,5
IFN β-1a 44 μg
(n=411)
Ocrelizumab 600 mg (n=410)
Ad
just
ed
AR
R a
t 9
6 W
ee
ks*
0,290
0,155
0,0
0,1
0,2
0,3
0,4
0,5
IFN β-1a 44 μg
(n=418)
Ocrelizumab 600 mg (n=417)
Ad
just
ed
AR
R a
t 9
6 W
ee
ks*
ITT *Adjusted ARR calculated by negative binomial regression and adjusted for baseline EDSS score (<4.0 vs ≥4.0), and geographic region (US vs ROW). ARR, annualised relapse rate; EDSS, Expanded Disability Status Scale; IFN, interferon; ROW, rest of the world. Hauser SL, et al. Presented at the 31st Congress of the European Committee for Treatment and Research in Multiple Sclerosis 2015. Platform Presentation number 190.
46% ARR reduction vs
IFN β-1a p<0.0001
OPERA I OPERA II
47% ARR reduction
vs IFN β-1a p<0.0001
Over 85% of
patients in the
ocrelizumab arms
completed the
OPERA I and
OPERA II studies

Secondary RMI end points : Reduction in total new and/or enlarging T2 hyperintense lesions compared with IFN β-1a
0,0
0,5
1,0
1,5
2,0
2,5
Week 24 Week 48 Week 96
Mea
n N
um
ber
Per
Pat
ien
t P
er M
RI S
can
*
IFN β-1a 44 μg
Ocrelizumab 600 mg
n
IFN β-1a 373 357 336
Ocrelizumab 385 378 360
0,0
0,5
1,0
1,5
2,0
2,5
Week 24 Week 48 Week 96
Mea
n N
um
ber
Per
Pat
ien
t P
er M
RI S
can
*
IFN β-1a 44 μg
Ocrelizumab 600 mg
OPERA I OPERA II
n
IFN β-1a 374 337 314
Ocrelizumab 387 376 360
98% p<0.0001
94% p<0.0001
41% p=0.0002
61% p<0.0001
96% p<0.0001
97% p<0.0001 - 77% - 83%
- 96% lesioni T1 GAD +


Any adverse event 80% 80% 86% 85%
Treatment discont. 3% 6% 3.8% 6%
Infusion reaction (>1) 30% 7% 37% 12%
Infections 56% 54% 60% 52%
Herpes zoster 2.2% 1% 1.9% 1%
Oral Herpes 2.2% 2% 3.6% 2.2%
Neoplasm (3) 0.7% (1) 0.2% (1) 0.2% (1) 0.2%
Serious infections 1.2% 2.9% 1.4% 2.9%
Ocrel. 1 Int.b1a Ocrel. 2 Int.b1a
NEJM: Ocrelizumab versus interferon Beta 1 a in RELAPSING MULTIPLE SCLEROSIS (Hauser S.L.et al. 2017)
A) le reazioni da infusione erano più frequenti nel gruppo trattato con Ocrelizumab, compreso
un broncospasmo di 4 grado. Reazioni di ipersensibilità del 2 tipo, da rilascio di citochine, che si
riducono successivamente ma sono sempre possibili. Bassa incidenza (0.3%) di anticorpi anti
Ocrelizumab. B) nasofaringiti e infezioni del tratto respiratorio superiore sono le più comuni
con Ocrelizumab; le urinarie con IntFB1a. Le infezioni serie erano più frequenti con Int.B1a
(2.9%) vs Ocrelizumab (1.3%). Nessuna infezione opportunistica. Eccesso di infezioni erpetiche
con Ocrelizumab. C 4 neoplasie con Ocrelizumab (2 seno, 1 renale, 1 melanoma), 2 con
Intf.B1a (1 linfoma 1 carcinoma squamocellulare). Durante la fase di estensione in cui
ricevevano tutti Ocrelizumab vi sono stati altri 5 casi.

Disease modifying therapy RMS
More active disease
Breakthrough disease
HSCT
Mild to moderate disease
Dimethyl fumarate (oral)
Glatiramer acetate (SC)
IFN beta (IM/SC)
Peginterferon beta-1a (SC)
Teriflunomide (oral)
Rapidly evolving severe disease
Refractory disease
Refractory disease
Safety issues
Safety issues
JC +
JC - Cladribina os (?) Fingolimod os Daclizumab sc
Ofatumumab sc Ocrelizumab ev Natalizumab ev Alentuzumab ev
Fingolimod os Daclizumab sc
Ofatumumab sc Ocrelizumab ev Natalizumab ev Alentuzumab ev
Post HSCT


Targeting “bad” B cells in multiple
Sclerosis: Could laquinimod be
part of the armamentarium? Forsthuber & Stuve, Neurol. Neuroimmun. Neuroinflamm.
2016
..Decrease in meningeal B-cell aggregates noticed in
EAE mice treated with laquinimod. Meningeal B-cell
follicles may very well contribute to disease etiology
in patients with progressive MS…
LAQUINIMOD
ALLEGRO E BRAVO a 2 anni in RRMS
ARR non significativo (-21% vs INTb1a)
Riduzione della progressione a 3 e 6 mesi:
- 34 e 46% Riduzione della atrofia: - 30%
Sia S.B. che talamo – corticale
ETP (10/ 3 mammella vs 6/1mammella)
CONCERTO 2200 pz con RRMS (0.6 e
1.2 mg)
CDP – atrofia- RR (2019)
ARPEGGIO fase II nella P. MS (HD)

Brain-wide pathway for waste clearance
captured by contrast-enhanced MRI Jeffrey J. . M. Nedergaard, H. Benveniste, J.Cl.inv. 3.2013
Grandi pulizie per i neuroni. Il sistema Glymphatico.

Siponimod Phase III program (EXPAND): first positive results (ECTRIMS 2016)
The Phase III EXPAND study of BAF312 (siponimod) in secondary progressive multiple sclerosis (SPMS) met its primary endpoint of reducing the risk of three-month confirmed disability progression versus placebo
EXPAND is the largest study ever conducted in SPMS, and is part of Novartis' ongoing leadership and commitment to people with MS1
The study included 1,651 people with SPMS from 31 countries. Patients were randomized to receive either 2mg BAF312 or placebo in a 2:1 ratio respectively2
The Secondary endpoints included2:
• delay in the time to six-month confirmed disability progression versus placebo
• time to confirmed worsening of at least 20% from baseline in the timed 25-foot walk test (T25FW)
• T2 lesion volume
• annualized relapse rate (ARR)
• the safety and tolerability of BAF312 in people with SPMS.
[1] Kappos L et al. Baseline Subgroup Characteristics of EXPAND: A Phase 3 Study of Siponimod (BAF312) for the Treatment of Secondary Progressive Multiple Sclerosis (P3.084). Neurology. 2016; 86(16):suppl. P3.084 [2] ClinicalTrials.gov. Exploring the Efficacy and Safety of Siponimod in Patients With Secondary Progressive Multiple Sclerosis (EXPAND). https://clinicaltrials.gov/ct2/show/NCT01665144?term=BAF312+expand&rank=1

Endpoints
Daclizumab 150 mg (n=512)
% Reduction vs IFNβ1a IM p value
Clinical endpoints
Annualised relapse rate 45% < 0.0001
Reduction in proportion of patients relapsed 41% < 0.0001
Risk of 24-week confirmed disability progression 27% 0.021
MRI endpoints
Number of new/newly enlarging T2 lesions 54% <0.0001
Number of T1 Gd+ lesions 65% <0.0001
Number of new hypointense T1 lesions 52% <0.0001
NEDA OR=2.059 <0.0001
Brain Volume Change Less reduction in
Daclizumabgroup <0.001
Elaborata da: Kappos L, et al. N Engl J Med. 2015
DECIDE Riassunto dei risultati di efficacia verso IFNβ1a

81%
71%
83%
69%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Daclizumab (DECIDE) INFβ1 a IM (DECIDE) Fingolimod(TRANSFORMS)
IFNβ1a IM (TRANSFORMS)
% Pazienti relapse free a 1 anno
Grafici elaborati da: Kappos L, et al. N Engl J Med. 2015 (DECIDE) ; Cohen et al N. Engl J Med 2010 (TRANSFORMS)
Risultati tratti dagli studi registrativi verso placebo. I risultati di studi clinici indipendenti non possono essere paragonati direttamente.
Risultati studi di fase III vs IFNβ1a im

Daclizumab : ZINBRYTA
• ha un meccanismo di azione unico (immunomodulante), con incremento
fin dalla 4 settimana dei NK regolatori CD56bright, che arriva al 600%,
mantenuto nel tempo, reversibile; non linfopenia (max – 10%).
• Superiorità all’interferone beta-1 a IM su piu’ end points
• Gli eventi avversi sono, di solito, maneggevoli.
• Somministrazione sc mensile 150 mg. con monitoraggio mensile indici
epatici, e emocromo trimestrale. Screening per TBC al basale se
precedenti e paesi ad alta prevalenza.
• Conservazione a temperatura ambiente ( < 30°) per un mese.
FDA Maggio 2016:
«because of its safety
profile was approved
after > 2 DMT»
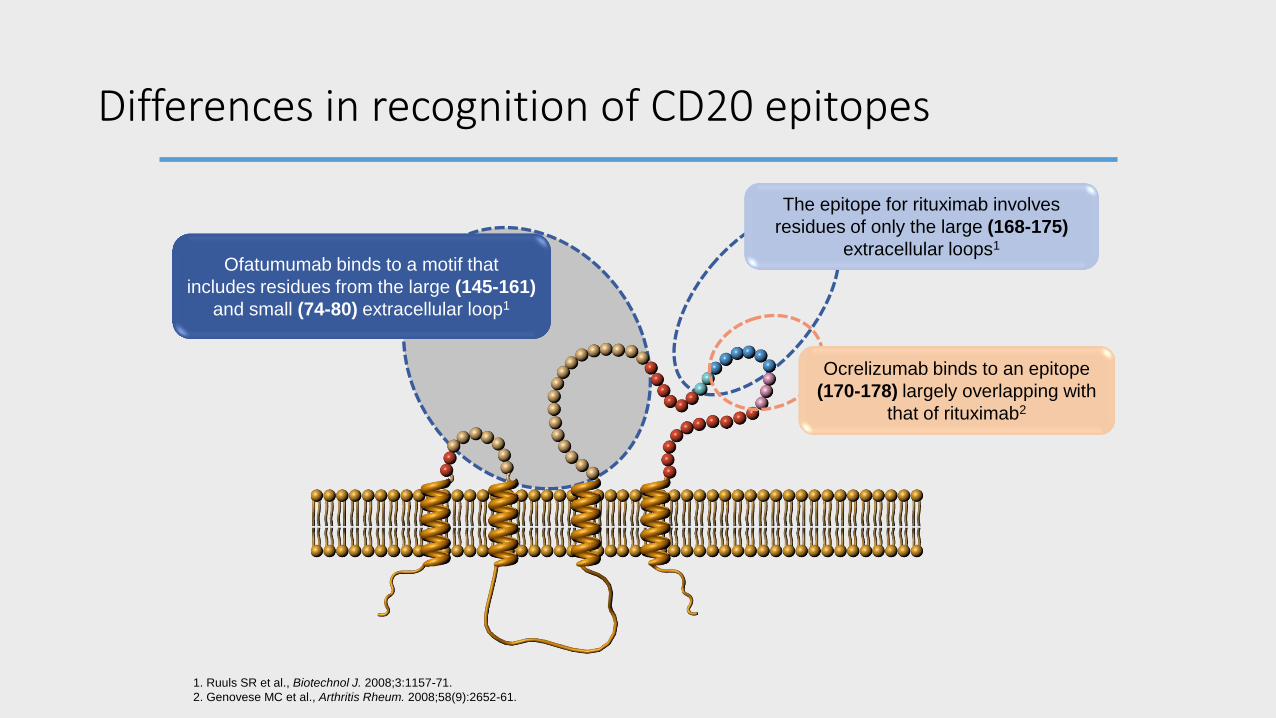
Differences in recognition of CD20 epitopes
Ofatumumab binds to a motif that
includes residues from the large (145-161)
and small (74-80) extracellular loop1
The epitope for rituximab involves
residues of only the large (168-175)
extracellular loops1
1. Ruuls SR et al., Biotechnol J. 2008;3:1157-71.
2. Genovese MC et al., Arthritis Rheum. 2008;58(9):2652-61.
Ocrelizumab binds to an epitope
(170-178) largely overlapping with
that of rituximab2

MS disease history and baseline characteristics
Placebo n=244
Ocrelizumab 600 mg n=488
Age, yr, mean (SD) 44.4 (8.3) 44.7 (7.9)
Female, n (%) 124 (50.8) 237 (48.6)
Time since symptom onset, yr, mean (SD) 6.1 (3.6) 6.7 (4.0)
Time since diagnosis, yr, mean (SD) 2.8 (3.3) 2.9 (3.2)
MS disease-modifying treatment naive, n (%) 214 (87.7) 433 (88.7)
EDSS, mean (SD) 4.7 (1.2) 4.7 (1.2)
MRI Patients with Gd+ lesions, n (%) Number of Gd+ T1 lesions, mean (SD) T2 lesion volume, cm3, mean (SD)
Normalised brain volume, cm3, mean (SD)
60 (24.7) 0.6 (1.6)
10.9 (13.0) 1469.9 (88.7)
133 (27.5) 1.2 (5.1)
12.7 (15.1) 1462.9 (83.9)
ITT EDSS, Expanded Disability Status Scale; Gd, gadolnium; MRI, magnetic resonance imaging; MS, multiple sclerosis; SD, standard deviation; yr, year. Montalban X, et al. Presented at the 31st Congress of the European Committee for Treatment and Research in Multiple Sclerosis 2015. Platform Presentation number 228.

Epatotossicità
*Only patients treated with daclizumab 150 mg in development programme studies are shown; patients exposed to daclizumab 300 mg dose in SELECT and/or SELECTION not represented. Duration was defined as length of time in days from the last ALT or AST measurement ≤1× ULN until return of both ALT and AST to ≤1.5× ULN. ALT, alanine aminotransferase; AST, aspartate aminotransferase; ULN, upper limit of normal. 1. Giovannoni G, et al. Mult Scler Rel Dis. 2016;9:36–46; 2. Kappos L, et al. N Engl J Med. 2015;373:1418–28. 3. Zinbryta® (daclizumab) SmPC. July 2016; 4. Fam S, et al. Poster presentation at EAN 2016;P31134.
Nella maggior parte dei casi l’innalzamento degli enzimi epatici è rimasto asintomatico e si è risolto spontaneamente. L’88% di coloro che avevano valori x 5 ha recuperato durante lo
studio e nel 86% dei casi è stato ri-trattato con Daclizumab senza ricorrenza. Un caso mortale per epatite autoimmune anticorpo negativa alla ripresa di Daclizumab 300 mg, dopo stop per 24 w (Selection)
INTEGRATED SAFETY ANALYSIS1*
DECIDE (2–3 y; vs IFN beta-1a)1–3
Daclizumab 150 mg
(n=1943) IM IFN beta-1a
(n=922) Daclizumab 150
mg (n=919)
Hepatic events, % 15 14 16
Serious hepatic events, % <1 <1 1
ALT or AST, %
≥3× ULN 9 9 10
>5× ULN 6 3 6
Discontinuation due to hepatic events, %
5 4 5
16%

Exploratory endpoints compared with IFN β-1a:
29,2
47,9
0
10
20
30
40
50
60
70
80
IFN β-1a 44 μg
(n=384)
Ocrelizumab 600 mg (n=382)
Pro
po
rtio
n o
f P
atie
nts
With
NED
A (
%)*
NEDA
64% improvement
vs IFN β-1a p<0.0001
NEDA is defined as: no protocol-defined relapses, no CDP events, no new or enlarging T2 lesions, and no Gd+ T1 lesions
OPERA I
25,1
47,5
0
10
20
30
40
50
60
70
80
IFN β-1a 44 μg
(n=375)
Ocrelizumab 600 mg (n=379)
Pro
po
rtio
n o
f P
atie
nts
Wit
h N
EDA
(%
)*
89% improvement
vs IFN β-1a p<0.0001
NEDA is defined as: no protocol-defined relapses, no CDP events, no new or enlarging T2 lesions, and no Gd+ T1 lesions
NEDA OPERA II
Percentage Change in Brain Volume from Baseline to Week 96
-1,6
-1,2
-0,8
-0,4
0
0 24 48 96
%C
ha
ng
e F
rom
Ba
selin
e t
o
We
ek
96
(M
ea
n, 9
5%
CI)
IFN β-1a 44 μg
Ocrelizumab 600 mg
Week
OPERA I Percentage Change in Brain Volume
from Baseline to Week 96
-1,6
-1,2
-0,8
-0,4
0
0 24 48 96
%C
ha
ng
e F
rom
Ba
selin
e t
o
We
ek
96
(M
ea
n, 9
5%
CI)
IFN β-1a 44 μg
Ocrelizumab 600 mg
Week
OPERA II
Change in brain volume
23.5% reduction in rate of brain volume loss vs IFN β-1a
p<0.0001
23.8% reduction in rate of brain volume loss vs IFN β-1a
p=0.0001
No evidence of disease activity (NEDA)

MRI – related secondary end points: Reduction in mean T1 Gd+ lesions compared with IFN β-1a
0,0
0,1
0,2
0,3
0,4
0,5
0,6
Week 24 Week 48 Week 96
Mea
n N
um
ber
Per
Pat
ien
t P
er M
RI S
can
*
IFN β-1a 44 μg
Ocrelizumab 600 mg
0,0
0,1
0,2
0,3
0,4
0,5
0,6
Week 24 Week 48 Week 96
Mea
n N
um
ber
Per
Pat
ien
t P
er M
RI S
can
*
IFN β-1a 44 μg Ocrelizumab 600 mg
n
IFN β-1a 372 357 335
Ocrelizumab 382 377 359
OPERA I OPERA II
n
IFN β-1a 372 334 311
Ocrelizumab 385 373 359
95% p<0.0001
98% p<0.0001
91% p<0.0001
92% p<0.0001
96% p<0.0001
97% p<0.0001 - 96% - 96%

n
Placebo 239 233 228 230 218 211 207 196 190 180 174
Ocrelizumab 473 460 454 454 450 435 432 425 419 412 397
29% reduction vs placebo
p=0.0404*
Secondary endpoint: Significant reduction in the progression rate of walking time
*Analysis based on ITT population; p-value based on ranked ANCOVA at 120-week visit adjusted for baseline timed 25-foot walk, geographic region and age with missing values imputed by LOCF. Point estimates and 95% CIs based on MMRM analysis on log-transformed data adjusted for baseline timed 25-foot walk, geographic region and age. CI, confidence interval; HR, hazard ratio; ITT, intent to treat; LOCF, last observation carried forward. Montalban X, et al. Presented at the 31st Congress of the European Committee for Treatment and Research in Multiple Sclerosis 2015. Platform Presentation number 228.
Percent Change in Timed 25-Foot Walk From Baseline to Week 120
% C
han
ge f
rom
Bas
elin
e W
alki
ng
Tim
e
(Mea
n, 9
5%
CI)

Ofatumumab Clinical Development Plan Phase 3:
ASCLEPIOS I & ASCLEPIOS II studies
• Annualized relapse rate 2.5 years Primary
end-point
• Time to 3-month confirmed disability worsening
• Time to 6-month confirmed disability worsening
• Time to 6-month confirmed disability improvement
• Number of new/enlarging T2 lesions per year
• Number of T1 Gd orT2 lesions per MRI scan
• Rate of brain volume loss
• Safety and tolerability
Key Secondary endpoints
MS, multiple sclerosis; GdE, gadolinium-enhancing; MRI, magnetic resonance
imaging
Randomized, double-blind, double-dummy, parallel-group study comparing the efficacy and safety of ofatumumab 30 mg s.c. every 4 W versus teriflunomide in
patients with relapsing forms of multiple sclerosis (RR or SP MS) Estimated Enrollment: 900 +900
https://clinicaltrials.gov/ct2/show/NCT02792218 https://clinicaltrials.gov/ct2/show/study/NCT02792231
DATI al 2019

Risk reduction: 40% HR (95% CI): 0.60 (0.45, 0.81); p=0.0006
Risk reduction: 40% HR (95% CI): 0.60 (0.43, 0.84); p=0.0025
Time to 12-week CDP Time to 24-week CDP
n
IFN β-1a 828 784 741 696 665 632 608 583 449
OCR 827 795 765 737 716 702 688 672 526
15.2
9.8 12.0
7.6
n
IFN β-1a 828 785 747 705 677 644 622 600 466
OCR 827 797 772 748 731 717 704 688 540
Secondary endpoints: Significant reduction in CDP in the pre-specified pooled analysis of OPERA I and OPERA II

L’IL-2 è una citochina essenziale per l’equilibrio tra tolleranza immunitaria e autoimmunità1-2
IL-2
NK=natural killer cells;Tact=activated T cells; Treg=regulatory T cells.
Nella SM, invece, l’IL-2 causa la
sopravvivenza e la proliferazione dei
linfociti T autoreattivi attivati, con
conseguente danno alla mielina.
1. Cheng G, Immunol Rev. 2011;241(1):63-76; 2. Malek TR, Immunity. 2010;33(2):153-165; 3. Wuest SC, Nat Med. 2011;17(5):604-609
L’interleuchina 2 (IL-2) è una citochina modulante prodotta dai linfociti T attivati e da altre cellule del
sistema immunitario1-3
In un soggetto sano l’IL-2 mantiene l’equilibrio tra tolleranza immunitaria e autoimmunità1-2
SM
Tact Tact
Tact Tact
Tact NK Tact Tact
Tact
NK
Breg
Treg
Treg Treg
NK
NK
Tact Tact Tact
Tact
Tact
Tact
Tact
Tact
Breg
Treg
Treg
Treg
Tact
Soggetto sano

Siponimod is a S1P (1-5) receptor modulator
• Siponimod is a selective S1P receptor modulator that targets MS via effects on the immune system and may also have effects within the CNS1,2
• Novel chemotype, not a prodrug
• Lipophilic, therefore, readily crosses the BBB3,4
• Fast immune reconstitution: half-life ~30 hours; washout period of 6 days2
BBB, blood-brain barrier; CNS, central nervous system; EC50, half maximal effective concentration; Emax, maximum effect; MS, multiple sclerosis; S1P, sphingosine 1-phosphate; SD, standard deviation. 1. Jackson SJ, et al. J Neuroinflammation. 2011;8:76. 2. Gergely P, et al. Br J Pharmacol. 2012;167:1035-1047. 3. Seabrook TJ, et al. Mult Scler. 2010;16:S301. Abstract P858. 4. Brinkmann V. Br J Pharmacol. 2009;158:1173.
Siponimod selectively targets S1P receptor subtypes 1 and 52
Siponimod reduces S1P1 expression in astrocytes and endothelial cells within chronic lesions in MS3
Siponimod reduces S1P5 reactivity in demyelinated lesions, correlating with a reduction in loss of myelin3
ALC will recover to lower limit of normal
(≥1.0×109 cells/L) in 4 days on average,
and to 90% of baseline level in 7 days on
average, after interrupting siponimod 2
mg treatment in MS patients
Titration over 9 or 10 days to a BAF312
dose of 10 mg successfully attenuates the
initial bradycardia observed on Day 1 of
treatment with BAF312 10 mg full dose