nuove opportunitÀ terapeutiche in epatite da hcv · nuove opportunitÀ terapeutiche in epatite da...
TRANSCRIPT

NUOVE OPPORTUNITÀ
TERAPEUTICHE
IN EPATITE DA HCV
FRANCESCO ARCADU U.O. MEDICINA GENERALE E GASTROENTEROLOGIA
P.O. “SAN FRANCESCO” ASL 3 - NUORO

THE DISEASE – Common, chronic, and potentially progressive
– Complications are becoming more common
– Liver failure, HCC
THE TREATMENT
– Viral cure, or SVR, is achievable
– SVR associated with histologic improvement and gradual regression of fibrosis
– SVR reduces risk for liver failure and HCC, improves survival
Why Treat Chronic Hepatitis C
Kanwal F et al. Gastroenterology 2011; 140:1182-88. Maylin et al. Gastroenterology 2008, 3:821-9
Asselah et al. Liver Int. 2015;35 S1:56-64

Martinot-Peignoux et al.. Hepatology 2010;51:1122-1126 Swain MG, et al. . Gastroenterology 2010;139:1593-1601.
SVR 24 = SVR 12 = Cure
– The primary goal of HCV therapy is to cure the infection
– A sustained virological response - SVR - is defined as undetectable HCV RNA 12 weeks (SVR12) or 24 weeks (SVR 24) after treatment completion
– The infection is cured in more than 99% of patients who achieve an SVR

Hill AM, et al. AASLD 2014. Abstract 44
SVR Associated With Reduced 5-Yr Risk of
Death and HCC in All Populations
Analysis included survival data from 34.563 pts followed for average of 5 yrs
SVR on IFN-based therapy was associated with substantial benefit vs no SVR – 62% to 84% reduction in all-cause mortality – 90% reduction in liver transplantatio – 68% to 79% reduction in HCC
5-Yr Risk of All Cause Death by SVR
5-Yr Risk of HCC by SVR SVR No SVR

RISPOSTA VIROLOGICA SOSTENUTA (SVR)
Risposta alla terapia anti HCV (fino al 2013)
Terapia basata su IFN/RBV e nel GT1 anche sui DAA
di 1^ generazione (Telaprevir/Boceprovir)

Adapted from the US Food and Drug Administration, Antiviral Drugs Advisory Committee Meeting,
IFN
6 mos
PegIFN/ RBV
12 mos IFN
12 mos
IFN/RBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standard IFN
RBV
PegIFN
1991
DAAs
PegIFN/ RBV/ DAA
IFN/RBV
6 mos
6
0
16
34
42 39
55
70+
20
40
60
80
100
DAA ± DAA
± RBV
± PegIFN
2014
April 27-28, 2011, Silver Spring, MD.
The evolution of CHC therapy Virologic eradication is the goal
SVR
%
Adapted from the US Foof and Drug Administration , Antiviral Drugs Advisory Cmmitee Meeting,
27-28 2011, Silver Spring, MD
HCV therapeutic timeline 70+

BF, maschio, 58 anni HCV prevalence, diagnosis and treatment
rates in 2013
Dore G et al. J Viral Hepatitis 2014

BF, maschio, 58 anni Gaps in the achievement of effectiveness of
HCV treatment in national VA practice
Kramer et al, Journal of Hepatology 2012; 56: 320-325

PWID have a high willingness to receive HCV
treatment
PWID LIVING WITH HCV INFECTION

PWID have a high willingness to receive HCV
treatment
PWID LIVING WITH HCV INFECTION
80% OF PWID ARE WILLING TO RECEIVE HCV TREATMENT
Doab A, Clinical Infectious Diseases 2005. Fischer B, et al. Presse Med 2005. Strathdee S, et al Clinical Infectious
Diseases 2005. Grebely J, et al. Drug and Alcohol Dependence 2008. Alavi M, et al. Clinical Infectious Diseases 2013.
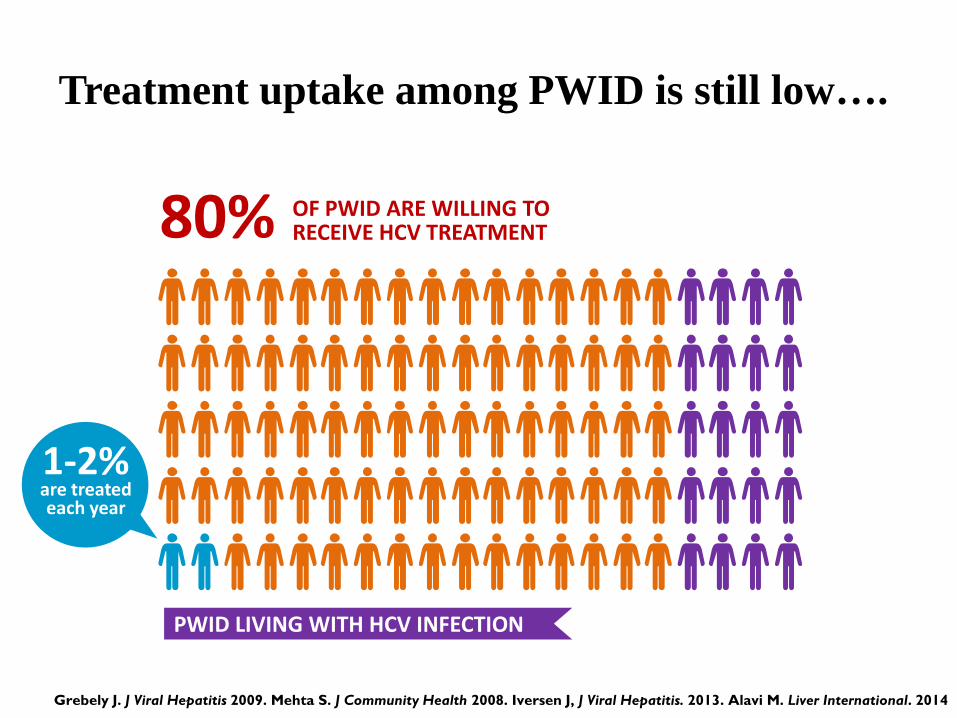
Treatment uptake among PWID is still low….
PWID LIVING WITH HCV INFECTION
80% OF PWID ARE WILLING TO RECEIVE HCV TREATMENT
Grebely J. J Viral Hepatitis 2009. Mehta S. J Community Health 2008. Iversen J, J Viral Hepatitis. 2013. Alavi M. Liver International. 2014
1-2% are treated each year

The HCV Care Cascade Less than 10% of people with HCV have been cured
Yehia BR, Schranz AJ, Umscheid CA, Lo Re V III (2014) The Treatment Cascade for Chronic Hepatitis C Virus Infection in
the United States: A Systematic Review and Meta-Analysis. PLoS ONE 9(7): e101554. doi:10.1371/journal.pone.0101554
Should improve with IFN-free therapy but long way to go……
Diagnosi
Accesso
Terapia SVR

Thomas, DL Lancet 2010 Oct 30;376(9751):1441-2
SVR in individuals SVR in the population
Efficacious treatments do not work if not
given…..
Need for reinforcing HCV screening and access to therapy to amplify the control of the disease

– 63 out of 353 Centers throughout Italy parteciped
– 33,433 patients were involved, 56% genotype 1
Combining these figure with NHS registries of HCV disease identification (016) the predicted number of known HCV patients are:
250,000 Monoinfected attending liver centers
30,000 HIV co-infected attending ID centres
25,000 Inmates
70,000 Under the care of GPs and legal migrants
Overall 350,000
Quanti HCV cronicamente infetti in Italia?
* Documento GdL Epatite C - AIFA-MinSal- ISS-SIMIT-AISF-EPAC-CNT Aprile 2014

Scenario 2014….quanti pazienti da trattare?
15.000 - 20.000* urgenti
60.000* entro 18 mesi
* Documento GdL Epatite C - AIFA-MinSal- ISS-SIMIT-AISF-EPAC-CNT Aprile 2014

15.000 - 20.000* urgenti
60.000* entro 18 mesi
* Documento GdL Epatite C - AIFA-MinSal- ISS-SIMIT-AISF-EPAC-CNT Aprile 2014
Con quali costi?

EASL & AASLD-IDSA Recommendations
Indications to treatment
All treatment-naïve and -experienced patients with compensated disease due to HCV should be considered for therapy (A1)
Treatment is recommended for patients with chronic HCV infection (IA)

All Clinical Practice Guidelines emphasizes the potential benefits of — and recommends treatment for — all pts with HCV infection
URGENT TREATMENT INITIATION RECOMMENDED FOR:
– Advanced fibrosis (Metavir F3)
– Compensated cirrhosis (Metavir F4)
– Liver transplantation
– Severe extrahepatic HCV
Treatment Benefits All Pts

Treatment Benefits All Pts
REDUCED HCV TRANSMISSION EXPECTED WITH
TREATMENT OF:
– Women wishing to become pregnant
– Long-term hemodyalisis pts
– MSM with high-risk sexual practices
– Injection drug users
– Incarcerated persons

– Extremely high efficacy (>95%)
– Tolerability - IFN free
– Minimal toxicity
– High barrier to resistance
– Once daily oral dosing
– Pangenotypic
– No drug – drug interactions
– Short duration (4-6 weeks)
– Affordable
Requirements for HCV regimen

Farmaci che interferiscono su processi
specifici nel ciclo di replicazione del virus
attraverso una diretta interazione con una
proteina virale o acido nucleico
Direct-Acting Antivirals (DAA)
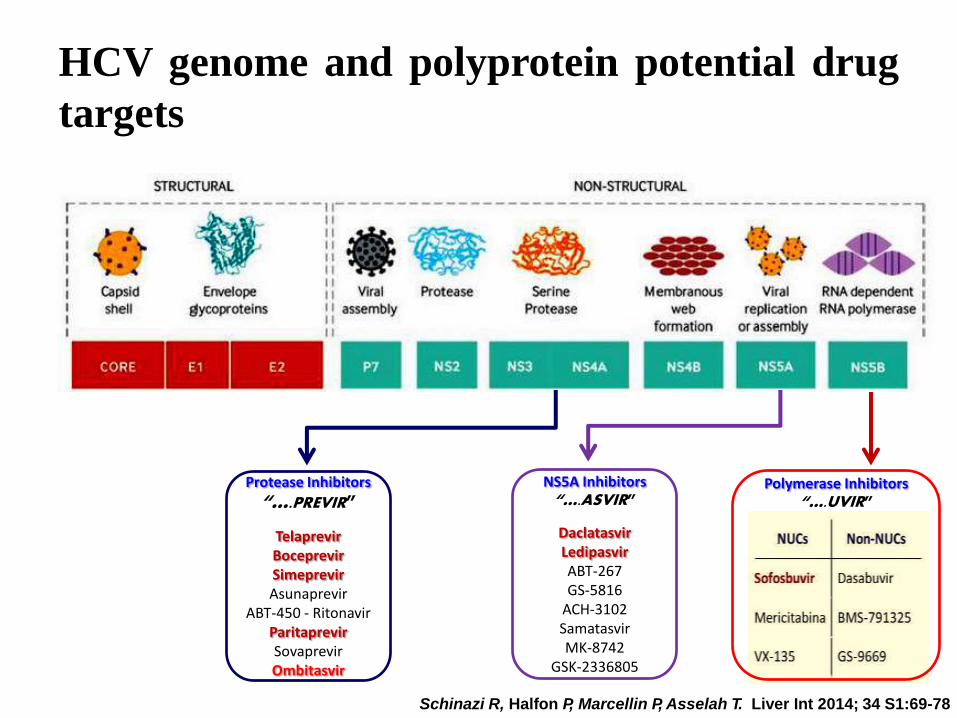
Protease Inhibitors
“….PREVIR”
Telaprevir Boceprevir Simeprevir Asunaprevir
ABT-450 - Ritonavir Paritaprevir Sovaprevir Ombitasvir
NS5A Inhibitors “….ASVIR”
Daclatasvir Ledipasvir ABT-267 GS-5816
ACH-3102 Samatasvir MK-8742
GSK-2336805
Polymerase Inhibitors “….UVIR”
Schinazi R, Halfon P, Marcellin P, Asselah T. Liver Int 2014; 34 S1:69-78
HCV genome and polyprotein potential drug
targets

Direct-Acting Antiviral Agents (DAAs) - Key
Characteristics
NS3 /4A Inhibitors (Protease inhibitor PI)
High potency
Limited genotypic coverage
Low barrier to resistance
NS5B Nucleos(t)ide Inhibitors (NI)
Intermediate potency
Pangenotypic coverage
High barrier to resistance
NS5A Inhibitors
High potency
Multi-genotypic coverage
Low barrier to resistance
NS5B Non Nucleoside Inhibitors (NNI)
Intermediate potency
Limited genotypic coverage
Low barrier to resistance
NS2 NS3 NS4A NS4B NS5A NS5B p7 E2 E1 C
Boc and Tel Simeprevir Paritaprevir
Sofosbuvir
Ledipasvir Ombitasvir Daclatasvir
Dasabuvir
NS= Nonstructural Proteins

Agents and Regimens

Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
EASL
guidelines
WHO
guidelines
EACS
guidelines
Sovaldi Olysio Daklinza Harvoni Viekirax
Exviera
EMA APPROVAL
FDA APPROVAL
AASLD recommendations 1
Sovaldi & Olysio
EASL recommendations
AASLD recommendations 2
Harvoni Viekira
Pack
HCV guidelines, recommendations & anti HCV drugs
approval by International agencies - 2014

Anti HCV drugs approval by International agencies
Sofosbuvir (Sovaldi®) 16/01/2014
Simeprevir (Olysio®) 14/05/2014
Daclatasvir (Daklinza®) 22/08/2014
Ledipasvir/Sofosbuvir (Harvoni®) 26/09/2014
Ombitasvir /Paritaprevir/Ritonavir (Viekirax®) 21/11/2014
Dasabuvir (Exviera®)
21/11/2014
European Medicines Agency (EMA) authorisations
Agenzia Italiana del Farmaco (AIFA) authorisations
– Sofosbuvir (Sovaldi®) 30/09/2014
– Simeprevir (Olysio®) 23/02/2015

Comunicato n. 423 27 febbraio 2015
Epatite C: accordo AIFA e Gilead Sciences per la rimborsabilità di Harvoni®
Ufficio Stampa Agenzia Italiana del Farmaco - Dott.ssa Arianna Gasparini Tel. 06 59784419 [email protected] – [email protected]

Pazienti con cirrosi in classe di Child A o B e/o con HCC con risposta completa a terapie resettive chirurgiche o locoregionali non candidabili a trapianto epatico nei quali la malattia epatica sia determinante per la prognosi
Criterio 1
Recidiva di epatite dopo trapianto di fegato con fibrosi METAVIR ≥2 (o corrispondente Ishack) o fibrosante colestatica
Criterio 2
Epatite cronica con gravi manifestazioni extra-epatiche HCV correlate (sindrome crioglobulinemica con danno d'organo, sindromi linfoproliferative a cellule B)
Criterio 3
Epatite cronica con fibrosi METAVIR F3 (o corrispondente Ishack) Criterio 4
In lista per trapianto di fegato con cirrosi MELD Criterio 5
Epatite cronica dopo trapianto di organo solido (non fegato) o di midollo con fibrosi METAVIR ≥2 (o corrispondente Ishack)
Criterio 6
Epatite cronica con fibrosi METAVIR F0-F2 (o corrispondente Ishack) (solo per Simeprevir)
Criterio 7
Priorità in base all'urgenza clinica 7 criteri di eleggibilità AIFA

Regimens with the best cost/benefit
* Si ritiene che il criterio 4 non comprenda pazienti con diagnosi clinica di cirrosi
Categorie Gt1 e 4 Gt2 Gt3
Cirrotici Child A/B – controind. a P/R
SIM + SOF ± RBV
SOF + RBV SOF + RBV (24 w) oppure
SOF + DACLA (compassionevole) – Non Responder
SIM + SOF ± RBV
SOF + RBV
Pazienti non cirrotici* appartenenti ai criteri
2,3,6
SOF + RBV + Peg-IFN
oppure SIM + SOF
± RBV
SOF + RBV SOF + RBV + Peg-IFN

FDA-Approved All-Oral Regimens for GT1
*Not recommended per AASLD/IDSA guidance. †8-wk course can be considered in pts without cirrhosis with pretreatment HCV RNA < 6 million IU/mL. ‡12-wk course may be considered for some patients based on previous treatment history.

*Up to 48 wks or until transplantation, whichever occurs first. †Not FDA approved but recommended in AASLD/IDSA guidance.
‡24 wks of SOF/LDV if anemia or RBV intolerance; 24 wks of SOF/LDV + RBV (600 mg/day with increasing dose if tolerated) if prior SOF failure.
www.hcvguidelines.org
All-Oral Regimens for Other Populations

SVR rates >90% in genotype 1

AASLD/IDSA HCV Guidelines

Sofosbuvir and Ribavirin in HCV Genotype 4 Egyptian Ancestry Trial: results
SVR 12 by Regimen Duration and Treatment Experience
Source: Ruane P, et al. 49th EASL. April 2014: Abstract P1243
Treatment Naive Treatment Experienced
11/14 10/17 14/14 13/15

SVR 12 by Regimen Duration and Treatment Experience
11/14 10/17 14/14 13/15
Liver Int. 2015 Jan;35 Suppl 1:27-34 Optimal therapy in genotype 4 chronic hepatitis C: finally cured? Abdel-Razek W, Waked I.
Optimal therapy for patients with hepatitis C virus (HCV) genotype 4 (HCV-4) infection is changing rapidly, and the possibility of a total cure is near.
IFN-free combinations with paritaprevir-ombitasvir, SOF-ledipasvir, or DCV-asunaprevir (ASV)-beclabuvir (BMS-791325) for 12 weeks or less with close to 100% cure rates will soon become the optimal therapy

I pazienti con cirrosi avevano significativamente meno probabilità di
raggiungere SVR rispetto ai pazienti non cirrotici per tutti i genotipi
studiati, e in particolare per il genotipo 3
GT3 GT2 GT1, 4-6
Mangia A. et al AASLD 2013 Abstract 1115
Treatment naïve Treatment naïve Treatment
experienced
Treatment
experienced
Genotype 3 HCV: still difficult to treat?

Sofosbuvir-Ledipasvir +/- Ribavirin in GT 1 & 3 ELECTRON 2: Results
SVR 12, by GT and Treatment Regimen
Gane EJ, et al. 49th EASL. 2014: Abstract O6
SOF-Experienced Treatment Naive CTP Class B

A 12-week regimen of DCV plus SOF achieved SVR12 in 96% of patients with genotype 3 infection without cirrhosis and was well tolerated. Additional evaluation to optimize efficacy in genotype 3 infected patients with cirrhosis is underway
HEPATOLOGY 2015;00:000-000
Afdhal N et al, EASL OC #68
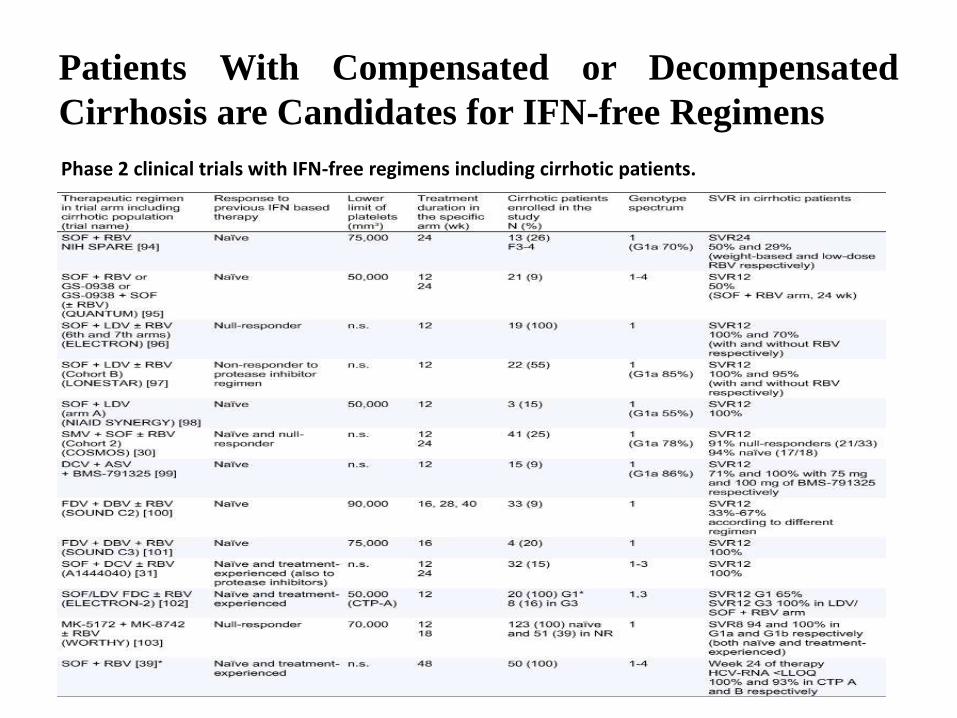
Phase 2 clinical trials with IFN-free regimens including cirrhotic patients.
Patients With Compensated or Decompensated
Cirrhosis are Candidates for IFN-free Regimens
Afdhal N et al, EASL OC #68
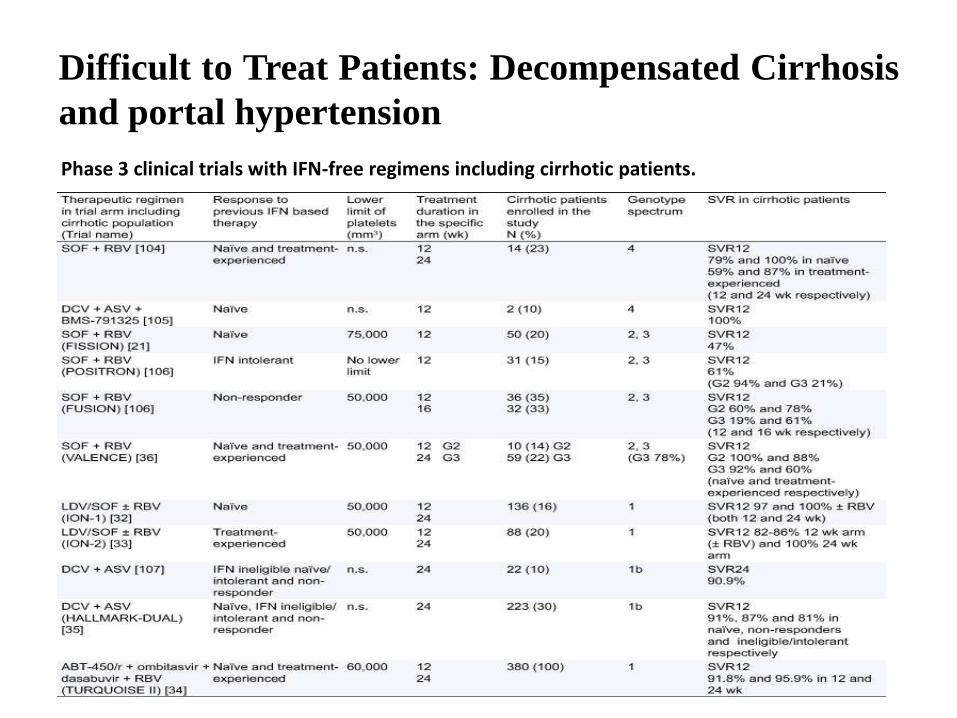
Difficult to Treat Patients: Decompensated Cirrhosis
and portal hypertension
Phase 3 clinical trials with IFN-free regimens including cirrhotic patients.

Flamm SL, al. 65th AASLD. 2014: Abstract 239
Ledipasvir-Sofosbuvir + Ribavirin in HCV GT 1,4 SOLAR-1 (Decompensated Cirrhosis): Preliminary Study Results
42/47 45/52 24/27 26/30 18/20 19/22
Treatment Naïve and Treatment Experienced

Therapeutic approaches of HCV infection in
cirrhosis decompensated, in waiting list & after LT
Flamm SL, al. 65th AASLD. 2014: Abstract 239. Afdhal N, et al. ILC 2014, Abstract #O68

Feedback from the real-world: do HCV cure rates in real-life
patient cohorts hold what clinical trials promised?
HCV-TARGET & TRIO
Data from two large observational databases demonstrate that:
– IFN-free regimens dominate the treatment landscape
– SOF-based regimens are effective in “real-world” settings
– Safety demonstrated in non-cirrhotic and cirrhotic patients
Jensen D, et al. AASLD 2014. Abstract 45. Dieterich D, et al. AASLD 2014. Abstract 46

Source: Liver Int © 2014 Blackwell
….in summary, after 2015

Where do we go from here??

Mild Severe
Decomp
Currently treated
HCV chronic disease spectrum

Mild Severe
Decomp
The future treatment
HCV chronic disease spectrum
By enrolling new patients at the extreme of the spectrum
By enforcing need for mass screening for HCV
IFN-free DAA will expand the pool of
treatable patients
WHO. Guidelines on the screening, care and treatment of persons with hepatitis C infection. April 2014
We must strive to obtain appropriate and effective treatment for all patients
