nwh medical staff orientation & annual education
TRANSCRIPT

NWH Medical Staff Orientation & Annual Education Marla Koroly, MD, FACP, MBA Senior VP, Medical Affairs and Chief Medical Officer
2017
1

Northern Westchester Hospital
MISSION • To provide the highest quality diagnostic & treatment services for
our community, while assuring access to a coordinated continuum of healthcare services. To improve and protect the health of individuals in the community through programs that promote healing and wellness.
VISION • We will provide the highest quality healthcare within a supportive
community setting and state of the art facilities
2

STRUCTURE: GOVERNANCE Three bodies have a role in governing NWH
3
Board of Trustees
Northwell Health - NWH
Senior Management MEC: Medical Board
CEO CMO CFO CNO Administrative Supervisor
3 ELECTED Officers – President; VP; Secretary/Treasurer 3 ELECTED Members at Large Appointed Chiefs
Committees: • Performance Improvement
Coordinating Group (PICG) • Professional Practice Evaluation (PPEC) • Credentials • Pharmacy & Therapeutics • Transfusion • Infection Prevention • Utilization Management • Ethics Review Committee
Governing Documents Bylaws (Hospital & Medical Staff) Rules & Regulations Policies & Procedures • On staff website • Electronic communication • On-Call and Coverage obligations

STRUCTURE: PEOPLE Our organization includes the organized Medical Staff, employed nurses, and other professional and support staff
Medical Staff (700+)
Hospital Based:
Employed: Internal Medicine & Pediatric Hospitalists; Critical Care Physicians; Hospital Neurologist; Neonatologists; Maternal-Fetal Medicine Specialist; Surgical Hospitalist & Advance Practitioners; Surgeons (breast, plastic, vascular, thoracic); Psychiatrists; Radiologists
Contracted: ED, Anesthesia, Pathology, Radiation Oncology, Clinical Trials
Large Groups: (PCMH, ACO, IT); Single Specialty Groups; Solo Practitioners
Nursing Staff (400+)
Other Professional & Support Staff
• Patient Care Team: RN, PCA, Pharmacy, Respiratory Therapy, Case Managers, Rehabilitation, Registered Dieticians, Social Workers
• Support: BA, Concierge, Service Associates, Transport, Facilities, Biomed, Finance
• Clinical Informatics
4
STRUCTURE: PROGRAM Our organization includes core services and centers of excellence, supported by a model of wellness
Hospital-based core services
• Advanced Imaging
• Core Laboratory
• Chappaqua Crossing: Rehabilitation, Balance Center, Wound Care HBOT
Centers of Excellence
• Cancer Treatment & Wellness Center
• Breast Institute
• Orthopedic & Spine Institute (OSI)
• Institute for Aesthetic Surgery & Medicine
• Institute for Robotic & Minimally Invasive Surgery (IRMIS)
• Surgical Weight Loss Program (Bariatric COE)
Wellness Model - Food; Physical Fitness; Mindful Wellness; Integrative Medicine
5

MANDATORY KEY TOPICS Northwell Health provides a comprehensive Education Program on line for all practitioners
6
• Patient’s & Parent’s Bill of Rights • Abuse/Neglect/Mistreatment of patients • Advance Directives • Ethical Issues • Abuse (Child, Elder) • TJC National Patient Safety Goals • Reporting Safety/Quality Concerns • Health Literacy; Limited English Proficiency • Infection Prevention
• Hand hygiene; Precautions; Exposures; Sharps; Waste • HIV; HBV; HCV; TB; Influenza; Pertussis; CDI • CA-UTI; CLABSI; SSI • PPE
• Sepsis • Fire Safety • Disaster Preparedness & HICS (Hospital Incident Command System) • Physician Health Assessment Requirements • Compliance – Fraud & Abuse; HIPAA
KEY TOPICS: Advance Directives We have a policy that governs medical decision making c/w NY State law
7
Family Health Care Decision Act NY State 6/1/2010
• Health Care Agent (HCA) – appointed in writing by the patient (Health Care Proxy)
• Surrogate - may make healthcare decisions – including end-of-life decisions – on behalf of incapacitated patients who do not have an HCA
- Court appointed guardian
- Spouse if not legally separated or Domestic Partner
- Son or daughter 18 years of age or older
- Parent
- Sibling 18 years of age or older
- Close friend
- No surrogate (unaffiliated patient) – Attending Physician + Hospital-designated concurring Physician
• Hospital presumes every patient has capacity, unless otherwise proven & indicated by the attending physician, and wishes to receive appropriate medical treatment, including cardiopulmonary resuscitation (CPR), unless otherwise indicated by an advance directive
• Patient, HCA, or Surrogate may request to have or to not have CPR or indicate other advance directives on the Medical Orders for Life Sustaining Treatment (MOLST) form
• The Attending Physician must enter a DNR order c/w the patient/HCA/surrogate wishes

KEY TOPICS: Ethics Review Committee Our Ethics Review Committee is available for consultation & guidance
8
The physician must have two special objects in view with regard to disease, namely, to do good or to do no harm. Primum non nocere
As a profession, medicine is characterized by a specialized body of knowledge and by a code of ethics and duty of service that put patient care above self-interest.
Guiding Principles • Beneficence • Non-maleficence • Respect for autonomy & self-determination • Veracity • Distributive Justice
The NWH Ethics Review Committee: Hal Federman, MD, Chair • Last Friday of every month from 12:00–1:00 PM • Open to all members of our Medical & Hospital Staff • Available ad hoc at the request of any physician, staff member, or patient or family member for
consultation & guidance on ethical issues concerning patient care and treatment • Maria Hale 914.666.1951 [email protected]

KEY TOPICS: Infection Prevention We adhere to standard practices to prevent transmission of infection
NWH/Northwell Infection Prevention policies & procedures • Approved by the Infection Control Committee • Available on the Staff Website • NY State Practitioners must maintain current Infection Control Training Certificate
(every 4 years)
Key Points • Vaccination – Hepatitis B, Influenza, MMR, Varicella, Tdap • Standard Precautions – assume each patient has a blood-borne disease that can
be transmitted & do not directly contact blood or body fluids of ANY patient • HAND HYGIENE – consistent use of alcohol-based hand sanitizer or soap & water • Appropriate personal protective equipment (PPE) for anticipated exposures –
gloves, gowns, safety glasses, mask • Safe use of sharp instruments • Follow post-exposure protocols • Appropriate disposal of waste & cleaning of equipment/environment • Antibiotic Stewardship – RIGHT diagnosis (indication), debridement, drug, dose,
duration, de-escalation

KEY TOPICS: Infection Prevention There are 3 types of patient-specific transmission-based precautions in addition to standard precautions
CONTACT – C.diff, Salmonella, Shigella, MRSA, CRE, MDRO, Norovirus, Lice, Scabies • Spread by contact with skin, mucous membranes, feces, emesis, urine, wound
drainage, body fluids, environmental surfaces • Staff & visitors use gown & gloves when patient or environmental contact
anticipated • Use disposable single-use or dedicated equipment
DROPLET – Influenza, N. meningiditis, Pertussis, Rhinovirus, Rubella, Mumps • Transmitted through close respiratory or mucous membrane contact • Door need not be closed – large droplets DO NOT stay airborne • Staff & visitors use surgical mask when within 6 feet of the patient
AIRBORNE – TB, Varicella, Measles • Patient in negative pressure room with door closed • Staff & visitors use N95 respirator when entering room

KEY TOPICS: Infection Prevention NYS Law requires offering screening & immunization to specific populations
• Hepatitis C Virus (HCV) Screening - born 1945-1965
• HIV Screening - age 13-64
• Influenza Vaccine - age 6 months & older
• Pneumococcal Vaccination - age 65 & older
• Tdap – parents & anticipated caregivers of all newborns

KEY TOPICS: Sepsis
12
Time-sensitive interventions: • AMI – “Door to Balloon” • Stroke – “Door to t-PA” • Trauma – “The Golden Hour”
• Sepsis
Systemic Inflammatory Response Syndrome
SIRS Infection Sepsis
SIRS – 2 or more: • Temperature > 101.0°F • Temperature <96.8 °F • Pulse > 90bpm • Respiratory Rate > 20/min • WBC count > 12,000 • WBC count < 4,000 • Band count > 5%
Pancreatitis
Trauma
Burns

The Sepsis Continuum
• Temperature > 101.0°F
• Temperature <96.8 °F
• Pulse > 90bpm
• Respiratory Rate > 20/min
• WBC count > 12,000
• WBC count < 4,000
• Band count > 5%
Known or suspected Infection + 2 or more SIRS
Sepsis SIRS
Severe
Sepsis
Septic
Shock
Sepsis with organ dysfunction • New AMS • Lactate > 2.0 • PaO2/FiO2 > 300 • New O2 required • SBP < 90 or ↓ by 40 • Cr > 2.0 mg/dl or ↑ 50% • UO < 0.5 ml/kg/h x 2h • Platelet count < 50,000 • Coagulopathy
Refractory Hypotension SBP < 90 or Lactate > 2.0 After fluids
KEY TOPICS: Sepsis
RRT Code GREEN

KEY TOPICS: Fire Safety All staff should be aware of fire safety measures
Two major causes of Hospital Fire • Smoking, Faulty Electrical Equipment
Particular risks • Patients confined to bed • Patients under sedation/anesthesia • Flammable gases such as oxygen • Large number of electrical devices & equipment
Order #1 is the Code for smoke, flames, or fire at NWH NWH Procedure for smoke or fire
• Rescue those in immediate danger • Alarm –PULL closest fire alarm box, CALL 1212 or PUSH “Fire/Code” button phone
• Contain the fire/smoke spread • Extinguish or evacuate

KEY TOPICS: Compliance Compliance simply means FOLLOWING THE RULES
2016 15
Northwell has a compliance program to ensure that all business practices and delivery of care to our patients are in compliance with applicable Hospital policies and procedures and applicable federal and state laws, rules, and regulations. Part of this program includes avoidance of any actual, potential, or perceived conflict of interest. People reporting compliance issues are protected.
Key Focus Areas for Hospitals • Submission of accurate claims and information • Referral statutes: Physician self-referral (“Stark”) law & Federal anti-kickback statute • Payments to reduce or limit services • Billing Medicare or Medicaid substantially in excess of usual charge • Emergency Medical Treatment and Labor Act (EMTALA) • Substandard care • Relationship with federal health care beneficiaries (Medicare patients) • HIPAA privacy and security rules
Report Compliance Concerns & Issues: • Division/Department chief, the Hospital Medical Director, or
the Office of Corporate Compliance at 516.465.8097
• Anonymous reporting: Compliance HelpLine 800.894.3226 or [email protected]
NWH Compliance Director:
Eric Sandhusen 516.465.3007 [email protected]

KEY TOPICS: HIPAA There are specific policies to protect patient rights
16
HIPAA
• Federal law to ensure the privacy & confidentiality of protected patient information (PHI)
• You may not use or disclose PHI- orally, electronically, or in writing
• Hospital Privacy Officer: Eric Sandhusen - 516.465.3007
Informed Consent • Except in emergency situations, written informed consent must be given by each patient (or
healthcare agent or surrogate for an incapacitated patient or minor) prior to any surgical operation, administration of anesthesia/sedation, blood transfusion, or all other MAJOR medical treatments (medical, surgical, or diagnostic intervention or procedure which involves significant risk or invasion of bodily integrity)
Disclosure • It is the practice at NWH to have honest discussions with patients about the outcomes of
treatments & procedures performed at the Hospital, including those outcomes that vary significantly from that which was anticipated

KEY POLICIES & PROCEDURES We have a code of conduct that calls for professionalism at all times
Code of Conduct – Professionalism
• High quality patient care & a culture of safety depend on teamwork, communication, and a collaborative work environment.
• Disruptive and intimidating behavior can foster medical errors and contribute to staff and patient dissatisfaction.
Treat all individuals with respect & dignity
No tolerance for discrimination and/or harassment
• Intimidating or threatening behavior
• Offensive jokes, slurs, negative stereotyping
• Unwanted sexual advances, innuendos, commentaries, displays
No tolerance for false accusations OR retaliatory behavior for reporting
2016 17

KEY POLICIES & PROCEDURES We have the dueling obligations of reducing the incidence of opioid abuse, while adequately managing pain
2016 18
Assessment and Management of Pain • All patients at NWH are entitled to a timely response to reports of pain (1996:5th vital) • The RN caring for each patient will assess pain on initial presentation and at least every shift
thereafter • Numerical Scale: None (0) Mild (1-3) Moderate (4-6) Severe (7-10) • Behavioral Pain Scale: FLACC • Neonatal Infant Pain Scale (NIPS)
I-STOP Internet System for Tracking Over-Prescribing Act – NY State • 8/27/13 - Physicians/NPs/PAs have a DUTY TO CONSULT the Prescription Monitoring Program
(PMP) registry prior to prescribing or dispensing any controlled substance • Practitioners may delegate consulting to office staff • Exceptions: ED < 5 days; facility administration; hospice care; vet; technical failure • 3/27/16 – Physicians/NPs/PAs must e-prescribe ALL prescriptions including controlled substances
(EPCS)
QUALITY
19
VALUE = [Clinical Quality & Safety] [Patient Experience] [Cost/Efficiency]
NWH Guiding Principles:
• TEAM WORK & COMMUNICATION
• PROCESS reduce variability, increase efficiency
• ELECTRONIC MEDICAL INFORMATION SYSTEM as an enabler
• Evidence-Based Order Sets (CPOE)
• Medication Safety (CPOE, BMV, Alerts)
• Communication & Transition (PDOC POC; DC)

CLINICAL QUALITY
20
IQR: Inpatient Quality Reporting OQR: Outpatient Quality Reporting
• Evidence-based, best practice PROCESS measures • Regulatory/Accreditation Requirement • Reputational Impact www.hospitalcompare.hhs.gov
• Financial Impact (P4P, VBP)
NYS Primary Stroke Center Sepsis Protocol

CLINICAL QUALITY: IQR, OQR
21
VENOUS THROMBOEMBOLISM (VTE) 2013 2014 2015 2016 2017Q1 Medicine/Surgery admissions with VTE prophylaxis or documented reason for no prophylaxis (%)
92.6 99.1 99.6 e-CQM e-CQM
Critical Care admissions with VTE prophylaxis or documented reason for no prophylaxis (%)
87.8 100 100 e-CQM e-CQM
POTENTIALLY PREVENTABLE HA-VTE Patients with confirmed hospital-acquired VTE who did not have VTE prophylaxis the day before diagnosis and no documented reason for no prophylaxis (%)
0 0
0
0 0

CLINICAL QUALITY: IQR, OQR Medicine Admission and Plan of Care/Progress Notes
22
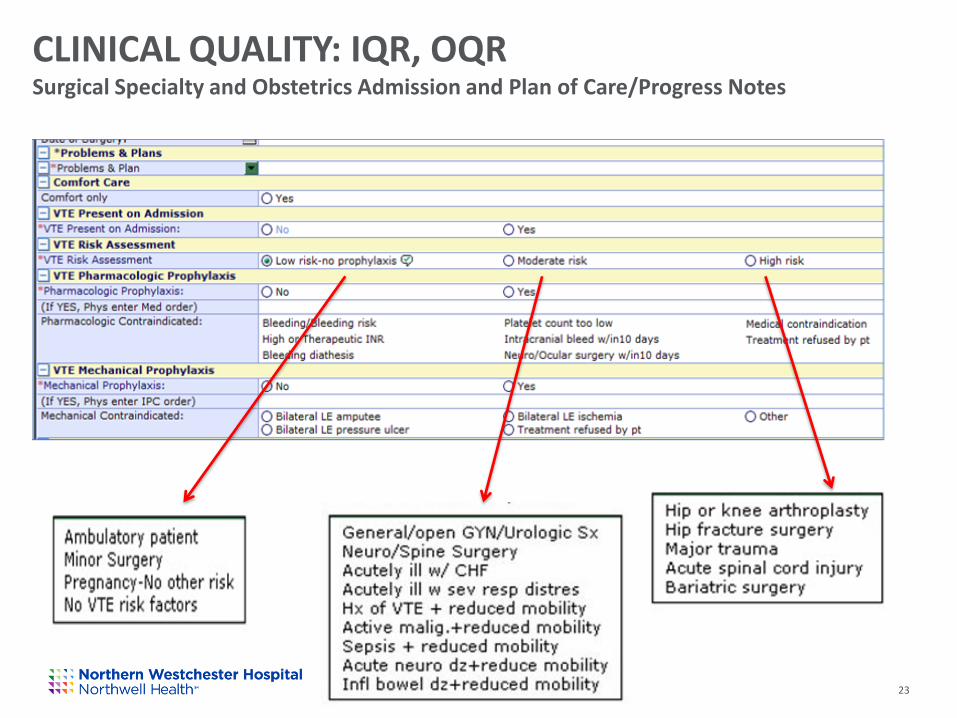
CLINICAL QUALITY: IQR, OQR Surgical Specialty and Obstetrics Admission and Plan of Care/Progress Notes
2016 23

CLINICAL QUALITY: IQR, OQR
24
PERINATAL CARE 2013 2014 2015 2016 2017Q1
Of pregnant women admitted for induction or Cesarean section from 37-39 weeks gestation, percentage who have no documented medical indication (percent “elective” deliveries) (Target = 0%)
4.2 1.0 0 0 0
Antenatal Steroid Use in women 24-32 weeks gestation who are at risk for preterm delivery (Target = 100%)
66.7 83.3 100 100 100
C-section rate in full term, single, vertex presentation, first time mothers (goal is to decrease) (Target = 23.9%)
31.9 41.5 43.2 42.5 44.4
Newborn Hospital-Acquired Blood Stream Infections (Target = 0%)
0 0 0 0 0
Single term newborns fed exclusively breast milk (Target = 70%)
N/A 66.7 62.3 61.0 67.7

CLINICAL QUALITY: IQR, OQR
25
HOSPITAL-BASED INPATIENT PSYCHIATRY (HBIPS)
2013 2014 2015 2016 2017Q1
Admission Screening (risk of violence, substance use, psych trauma history, patient strengths) (%)
87.6 98.9 100 99.3 93.3
Multiple medications at discharge with appropriate reason (%)
76.5 85.0 100 100 100
Alcohol Use Screening (%) N/A 53.6 98.5 99.6 96.6
Alcohol Use Brief Intervention Offered (%) N/A N/A N/A 51.1 77.8
Alcohol Use Brief Intervention Provided (%) N/A N/A N/A 51.1 77.8
Tobacco Use Screening (%) N/A N/A 99.6 100 100
Tobacco Use Treatment Offered (%) N/A N/A 78.0 84.1 100
Tobacco Use Treatment Provided (%) 45.0 36.6 14.3

CLINICAL QUALITY: IQR, OQR
26
EMERGENCY DEPARTMENT FLOW MEASURES 2013 2014 2015 2016 2017Q1
ED Admitted Patients – Median Arrival to Departure (minutes) – TARGET = 240
272 309 278 275 266
ED Admitted Patients – Median Decision to Admit to Departure (minutes) – TARGET = 43
39 68 52 49 77.5
ED All Patients – Median Arrival to Practitioner (minutes) – TARGET = 13
15 14 16 13.0 12.0
ED Treated & Released Patients – Median Arrival to Departure (minutes) – TARGET = 120
141 160 150 158 178.0
ED Median Time to Pain Management for long bone fracture (minutes) – TARGET = 38
37 36 45 43 34.5
ED CT Result for Acute Stroke within 45 minutes (%) – TARGET = 100%
53% 88.9% 71.4% 81.8% 100%
ED Chest Pain – Median Time to ECG (minutes) – TARGET = 10
3.5 3.0 3.0 3.5 8.0
ED Chest Pain – Aspirin at Arrival (%) – TARGET = 100%
100% 100% 100% 100% 100%
ED Chest Pain – Median Time to Transfer (minutes) – TARGET = 30
85.0 42.5 54.0 53.0 52.5

SAFETY We support a culture of safety in which we openly discuss events as an opportunity for improvement and monitor several hospital-acquired conditions
• Culture of Safety
• Safety Event Reporting System
• Hospital Acquired Infections
• Catheter associated urinary tract infection (CA-UTI)
• Central Line Associated Blood Stream Infection
• Ventilator Associated Pneumonia
• Multidrug Resistant Organisms (MRSA/CRE)
• Clostridium difficile Intestinal Infection
• Surgical Site Infections (Colon, Hip, Hysterectomy)
• Medication Errors
• Nursing (Falls, Pressure Ulcers)

SAFETY Our hospital-wide alert codes help create a safe environment for patients, staff, and visitors
Summary of NWH Codes:
Code 444 – cardiopulmonary arrest age 18 and older
Code 444 Junior – cardiopulmonary arrest age < 18 years
Code Pink – possible infant/child abduction
Code H – maternal hemorrhage
Code Purple – behavioral emergency/risk
RRT – Rapid Response Team - serious change in patient’s medical condition
RRT/Code Grey – possible stroke in hospital/ED
RRT/Code Green – possible severe sepsis or septic shock in hospital/ED
Code HICS – Hospital Incident Command System – an event possibly disruptive to normal
hospital operations (emergency hotline ext 7911)
• Active Shooter – active shooter in building • Order #1 – fire or smoke alert • Watch Plan – fire system disruption • Plan Water Crisis - loss of water pressure
• Plan 02 – emergency oxygen shut down • Plan Generator – loss of Con-Ed electrical
power • Plan PBX – phone system failure

SAFETY: Restraint & Seclusion Restraint or seclusion may only be used when absolutely necessary to ensure the safety of a patient, staff member, or other individual
Mechanical Restraint (non-violent: two point) – restraint to both wrists to prevent a patient from interfering with life sustaining equipment Mechanical Restraint (violent: four point) – restraint to both wrists AND ankles to protect the patient from injuring him/herself or others Medication Restraint – any medication used for the purpose of restricting or managing behavior or freedom of movement that is NOT a standard treatment or dosage for a patient’s condition Seclusion – involuntary confinement alone in a room from which a patient is physically prevented from leaving (only on our behavioral health unit)
Key Points
• Must be ordered by attending or covering physician or NP/PA ONLY after face to face physician evaluation
• May NOT be ordered PRN and should be discontinued at the EARLIEST possible time
• Must be renewed at specific time intervals (daily for 2 point, every 4 hours for 4 point)
• Physician must do a daily evaluation of the patient

SAFETY: MRI Safety Mandatory questions when ordering an MRI help ensure MRI Safety
• The Magnet is ALWAYS on and is 40,000 x stronger than gravity • All equipment brought into room must be non-ferrous • Patients who can NEVER have an MRI:
• Other implanted devices must have proper documentation and verification of
safety o stents, valves, IUD, wire mesh, shunts, ports, orbital or penile prostheses, cochlear implants

PATIENT EXPERIENCE NWH is a designated Planetree Hospital with distinction
IOM: Providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions Planetree (1970s) - a framework for patient-centered care
• Caring interactions with providers • Access to meaningful information • Involvement of family • Healing physical environment • Role of spirituality • Arts in healing • Food in healing

PATIENT EXPERIENCE NWH exceeds national & state performance in patient experience survey scores

EFFICIENCY To achieve HIGH VALUE CARE, we need to optimize resource utilization & efficiency, in addition to focusing on quality, safety, & patient experience
• Cost of Care: Utilization Management
• Appropriate Level of Care – Observation/Admission
“2 midnight rule”
• Optimum utilization of resources
• Time Efficiency/Discharge Planning: Length of Stay
• Clinical Documentation Excellence

PROFESSIONAL PRACTICE EVALUATION - OPPE The organized Medical Staff must continuously monitor the competency & performance of ALL practitioners granted privileges
Profile for JOHN BONE, MD
SERVICE: ORTHOPEDIC SURGERY AND SPORTS MEDICINE SPECIALTY: ORTHOPEDIC SURGERY
Profile last viewed by Provider: 01/18/2016
Status Indicator My
Score Peers Score
Target SPC Alert
Current Period
24 Month Values
My Score
Start Month
A - Volume and Acuity
Volume Procedures Total NW PPE 86 670 N/A Jul-Dec 15
410 Jan
2014
A1 - Inpatient
Volume Admissions Inpatient PPE 29 330 N/A Jul-Dec 15
120 Jan
2014
Volume Procedures Inpatient NW PPE 32 359 N/A Jul-Dec 15
119 Jan
2014
A2 - Observation
Volume Consultations Observation PPE Reports
0 3 N/A Jul-Dec 15
0 Jan
2014
A3 - Emergency Department
Volume Consultations ED PPE Reports
1 5 N/A Jul-Dec 15
2 Aug
2014
A6 - OSI
Volume OSI Orthopedics Surgical TOTAL PPE
86 663 N/A Jul-Dec 15
407 Jan
2014
Volume OSI Joint Replacement PPE 32 304 N/A Jul-Dec 15
114 Jan
2014
Volume OSI Knee Uni-Compartment Navio PPE
0 13 N/A Jul-Dec 15
0 Jan
2014
Volume OSI Sports Medicine Surgery PPE
38 272 N/A
Jul-Dec 15
233 Jan
2014
B - Medical Knowledge Skill Judgment
Core VTE1 - VTE Prophylaxis Med Surg NW PPE
100.0% 100.0% 100.0% Jul-Dec 15
100.0% Feb
2015
Core VTE6 - Preventable HA-VTE NW PPE
No Data
0.0% 0.0% Jul-Dec 14
No Data No
Data
B3 - Patient Safety Indicators - PSI 90
PSI-15 Accidental Puncture or Laceration PPE
0 0 0 Jul-Dec 15
0 Jan
2014
PSI-12 Postoperative Pulmonary Embolism PPE
0 0 0 Jul-Dec 15
0 Jan
2014
PSI-12 Postoperative Deep Vein Thrombosis PPE
0 0 0 Jul-Dec 15
0 Jan
2014
PSI-13 Postoperative Sepsis PPE 0 2 0 Jul-Dec 15
0 Jan
2014
PSI-14 Postoperative Wound Dehiscence PPE
0 0 0 Jul-Dec 15
0 Jan
2014
Goal: an unbiased, reliable, and efficient structure and process for the Medical Staff to measure their own performance with a goal of continuous improvement in patient care
Patient safety & quality Fairness & collegiality
• Focused Professional Practice Evaluation • Ongoing Professional Practice Evaluation • PPEC
• Case Review – rated 1-3 • Aggregated data review every 6 months

Other Documents for Review (in orientation packet and on Northwell site)
Policies • Disruptive, Intimidating, and Inappropriate Behavior • Impaired Physicians • Perioperative Evaluation of Adults • Sepsis Protocol • Assessment and Management of the Patient with Pain
General Information • Committee for Physician Health • Dictation Procedures (for medical record documentation) • Hospital Department Contact Sheet • The Hal Federman, MD Health Sciences Library • Welcome Letter from the Medical Staff Liaison • Welcome Letter from Officers of the Medical Staff • Meditech Training & Parking Key ID Badge Information • Meditech Remote Access Instructions • Northern Westchester Hospital 24/7 Language Interpretation Services • American Sign Language Interpretation Services • Policy Tech Policies & Procedures Overview • Quick Guide to the NWH Physician Section of the NWH Staff Web Site
