nybgh one voice initiative a regional strategy to integrate depression screening and management into...
TRANSCRIPT
1
NYBGH One Voice Initiative
A Regional Strategy to Integrate Depression Screening and
Management into Primary Care
1
2
• NYBGH & health care quality• The burden of depression• Challenges and barriers to improving
depression screening & management in primary care
• An evidence based model for depression care• The One Voice pilot
Overview
3
• NYBGH represents 175 employers, unions, health plans, providers, and other healthcare organizations operating in NY, NJ, and CT
• Focus is on education and quality improvement• Unique combination of stakeholders allows NYBGH
to launch major quality initiatives requiring collaboration between health plans and local partners
• One of 56 business coalitions around the country
NYBGH is an employer-driven, non-profit coalition dedicated to improving the quality and efficiency of healthcare
3
4
• eValue8: Nationwide health plan performance initiative. • Physician Performance Reports: Measures PCP performance
in the areas of diabetes, heart disease, prevention, COPD, depression by aggregating health plan data
• Patient Experience with PCPs: Working with Aetna, Cigna and United to measure patient experience with primary care physicians
• One Voice• Hospital Value Initiative: Working with plans, employers and
hospitals to create payment models that reward best outcomes and increase value for the purchaser
NYBGH Initiatives

5
PBMMedco
5
Mental Health Task Force comprised of key players in behavioral health care management in NY metro area
Purchasers/ConsultantsPitney Bowes
MercerCBS Corporation
CitiPricewaterhouseCoopers LLC
HewittNYC Labor Health Alliance
Professional SocietiesNew York County Medical SocietyNew York State Society for Clinical
Social Work
Local GovernmentNYC Dept. of Health and
Mental Hygiene
Consumer AdvocacyNational Alliance on Mental
Illness
Behavioral Health PlansValueOptions
LifesynchMHN
MyExpertSolutionTeenScreen
Harris Rothenberg
Health PlansEmblemHealth
AetnaEmpireCigna
United Healthcare
Mental Health Task Force
Chair: Mike Thompson, Principal,
PricewaterhouseCoopers

6
• Depression impedes functioning in nearly all aspects of a patient’s life1
– Co-occurs with other chronic mental and physical disorders 70% of the time2
– Physical comorbidities (heart disease, chronic pain, cancer, diabetes) become harder to manage– Co-occurring mental disorders are often misdiagnosed or incorrectly treated
• Depression costs employers ~$36.6 billion in excess productivity loss each year2
– Absenteeism: 1/3 of costs, ~8.7 days/year2
– Presenteeism (sub-obtimal performance at work): 2/3 of costs, ~18.2 days/year2
– Health care costs may be up to 50% greater for depressed employees1
Untreated depression creates heavy burden of disease for patients, and generates substantial costs for employers
6
380,000 working-age New Yorkers suffer from depression, but their illness is underdiagnosed and undertreated
Prevalence (last 12 months): 7.5% among adults 20+ (9.4% among 20-39 yr olds)3
Awareness (ever-diagnosed): 54.6% among adults 20+ (45% among 20-39 yr olds)3
Treatment: 36.7% among adults 20+3
1 Katon, Wayne. The Impact of Depression on Workplace Functioning and Disability Costs. American Journal of Managed Care, 2009. 15: S322-S327.2 Position Statement: Depression in the Working Population. American College of Occupational and Environmental Medicine, Jan. 2009.3 NYC Health and Nutrition Examination Survey (HANES), 2004.
7
– More than 7 major commercial health plans and nearly 10,000 primary care practice locations1
– Limited psychiatric participation in health plans– Prevalence of solo practices (34%)1 makes team approach
challenging
NYC health care landscape poses unique challenges for improving depression care
7
1 NYC Primary Care Physicians by Setting. Center for Health Workforce Studies.
8
Barriers to integrating mental health with primary care are common– Coverage challenges: Providers are not compensated for spending additional time with
patients, consulting with colleagues, or screening for and treating mental health problems1
– Provider resistance: Many PCPs feel they lack adequate decision support in managing mental illness, and have insufficient training in psychiatry1
– Limited access to specialists: Providers report major challenges accessing mental health care services for their patients2
– Patient resistance: Some patients may prefer to keep their mental health treatment separate from primary care, for privacy or care preference reasons2
– Cultural barriers: Historical isolation of mental health providers from other health care practitioners creates disconnects in communication, relationships and knowledge2
Barriers in current system severely limit screening and management of depression in primary care
8
1 Cunningham, Peter. Beyond Parity: Primary Care Physicians’ Perspectives on Access to Mental Health Care. Project HOPE DataWatch, Apr. 2009.2 Bazelon Center for Mental Health Law. Integration of Primary Care and Behavioral Health, 2005.
9
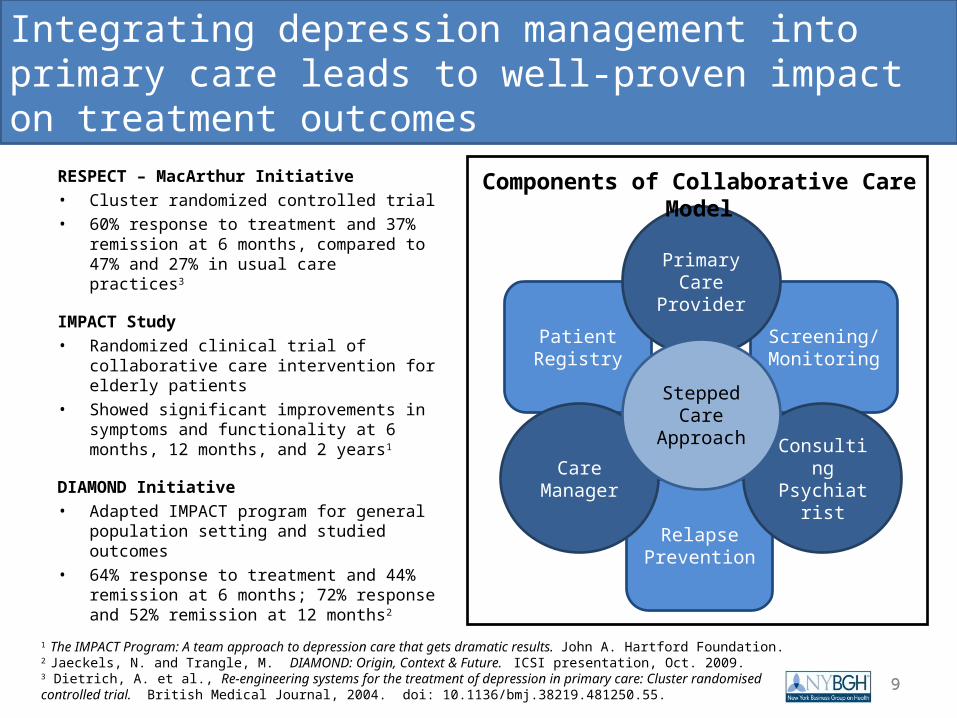
RESPECT – MacArthur Initiative• Cluster randomized controlled trial • 60% response to treatment and 37%
remission at 6 months, compared to 47% and 27% in usual care practices3
IMPACT Study• Randomized clinical trial of collaborative care
intervention for elderly patients• Showed significant improvements in
symptoms and functionality at 6 months, 12 months, and 2 years1
DIAMOND Initiative• Adapted IMPACT program for general
population setting and studied outcomes• 64% response to treatment and 44%
remission at 6 months; 72% response and 52% remission at 12 months2
Integrating depression management into primary care leads to well-proven impact on treatment outcomes
9
Relapse Prevention
Patient Registry
Screening/ Monitoring
Consulting Psychiatrist
Care Manager
Primary Care
Provider
Stepped Care
Approach
Components of Collaborative Care Model
1 The IMPACT Program: A team approach to depression care that gets dramatic results. John A. Hartford Foundation.2 Jaeckels, N. and Trangle, M. DIAMOND: Origin, Context & Future. ICSI presentation, Oct. 2009.3 Dietrich, A. et al., Re-engineering systems for the treatment of depression in primary care: Cluster randomised controlled trial. British Medical Journal, 2004. doi: 10.1136/bmj.38219.481250.55.
10
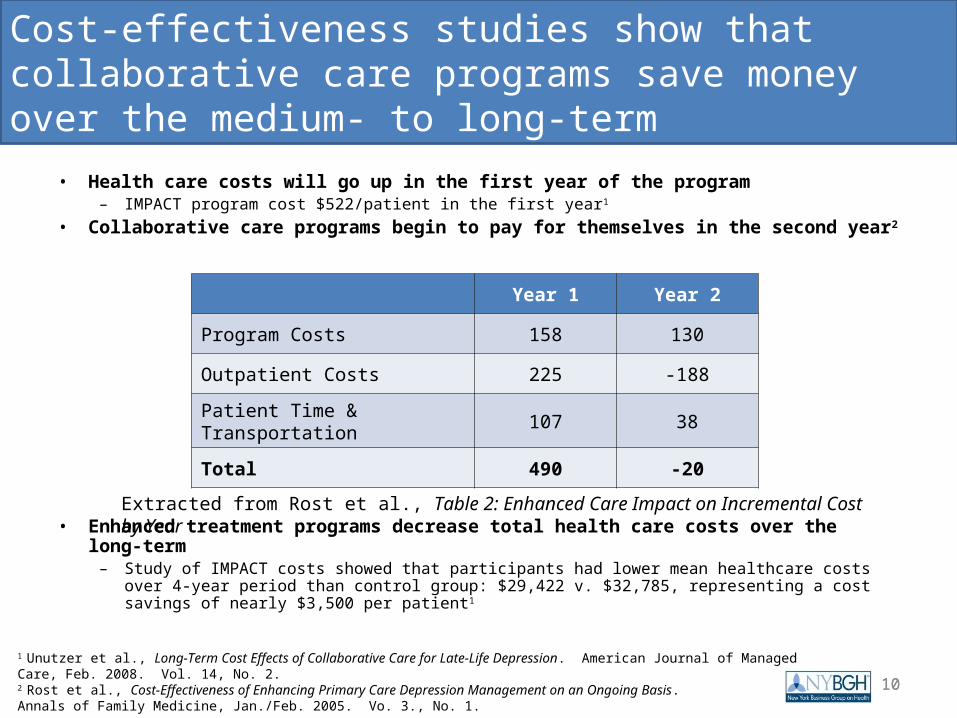
• Health care costs will go up in the first year of the program– IMPACT program cost $522/patient in the first year1
• Collaborative care programs begin to pay for themselves in the second year2
• Enhanced treatment programs decrease total health care costs over the long-term– Study of IMPACT costs showed that participants had lower mean healthcare costs over 4-year period
than control group: $29,422 v. $32,785, representing a cost savings of nearly $3,500 per patient1
Cost-effectiveness studies show that collaborative care programs save money over the medium- to long-term
10
1 Unutzer et al., Long-Term Cost Effects of Collaborative Care for Late-Life Depression. American Journal of Managed Care, Feb. 2008. Vol. 14, No. 2.2 Rost et al., Cost-Effectiveness of Enhancing Primary Care Depression Management on an Ongoing Basis. Annals of Family Medicine, Jan./Feb. 2005. Vo. 3., No. 1.
Year 1 Year 2
Program Costs 158 130
Outpatient Costs 225 -188
Patient Time & Transportation 107 38
Total 490 -20
Extracted from Rost et al., Table 2: Enhanced Care Impact on Incremental Cost by Year
11
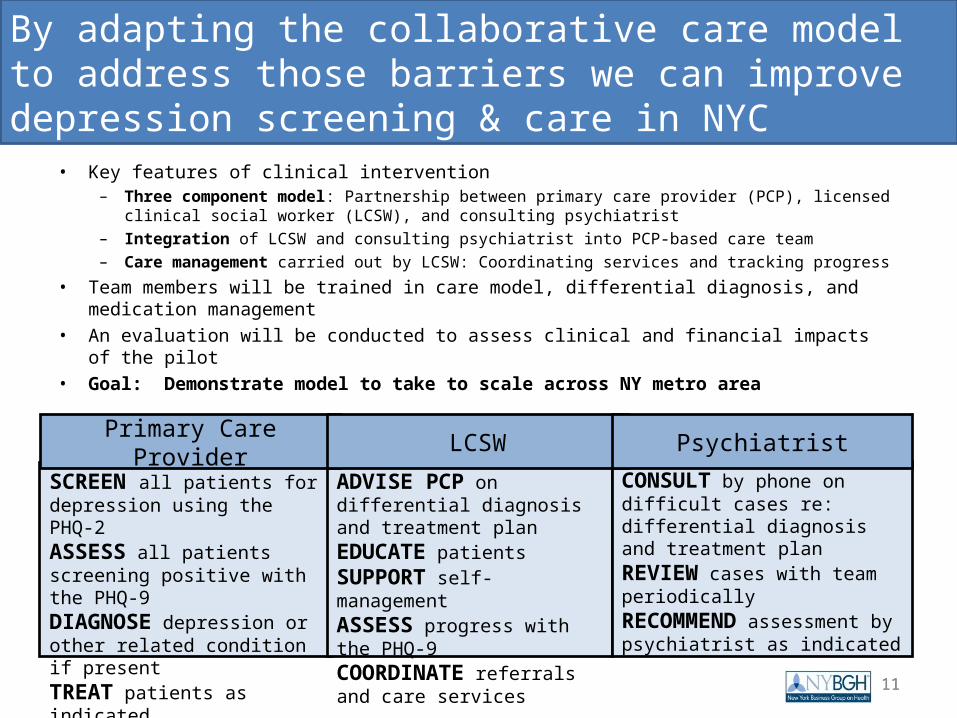
• Key features of clinical intervention– Three component model: Partnership between primary care provider (PCP), licensed clinical social
worker (LCSW), and consulting psychiatrist– Integration of LCSW and consulting psychiatrist into PCP-based care team– Care management carried out by LCSW: Coordinating services and tracking progress
• Team members will be trained in care model, differential diagnosis, and medication management
• An evaluation will be conducted to assess clinical and financial impacts of the pilot• Goal: Demonstrate model to take to scale across NY metro area
By adapting the collaborative care model to address those barriers we can improve depression screening & care in NYC
11
SCREEN all patients for depression using the PHQ-2ASSESS all patients screening positive with the PHQ-9DIAGNOSE depression or other related condition if presentTREAT patients as indicated
ADVISE PCP on differential diagnosis and treatment plan EDUCATE patients SUPPORT self-managementASSESS progress with the PHQ-9 COORDINATE referrals and care services
CONSULT by phone on difficult cases re: differential diagnosis and treatment planREVIEW cases with team periodicallyRECOMMEND assessment by psychiatrist as indicated
Primary Care Provider LCSW Psychiatrist
12
• Pilot will aim to enroll ~1,000 patients – adult working population• Anticipate working with 2-3 large/group practices and 5-6 small providers• Practices and providers will be selected based on interest and willingness to adapt
their clinic systems, participate in training, and share data• NYBGH has secured commitments from key partners
– 6 major NYC health plans have expressed interest and support– Providers have demonstrated willingness to participate– NYS Society of Clinical Social Workers supports the project
• Participatory planning process should minimize unexpected logistical or financial challenges during implementation
• Goal of One Voice Initiative is to drive dissemination throughout region– Demonstrate results in NYC context– Refine model to optimize clinical and logistical methodologies– Produce materials for training, education, and clinical practices that can be reused
Initiative will work with small set of providers to showcase and refine integrated care model for regional uptake
12
13
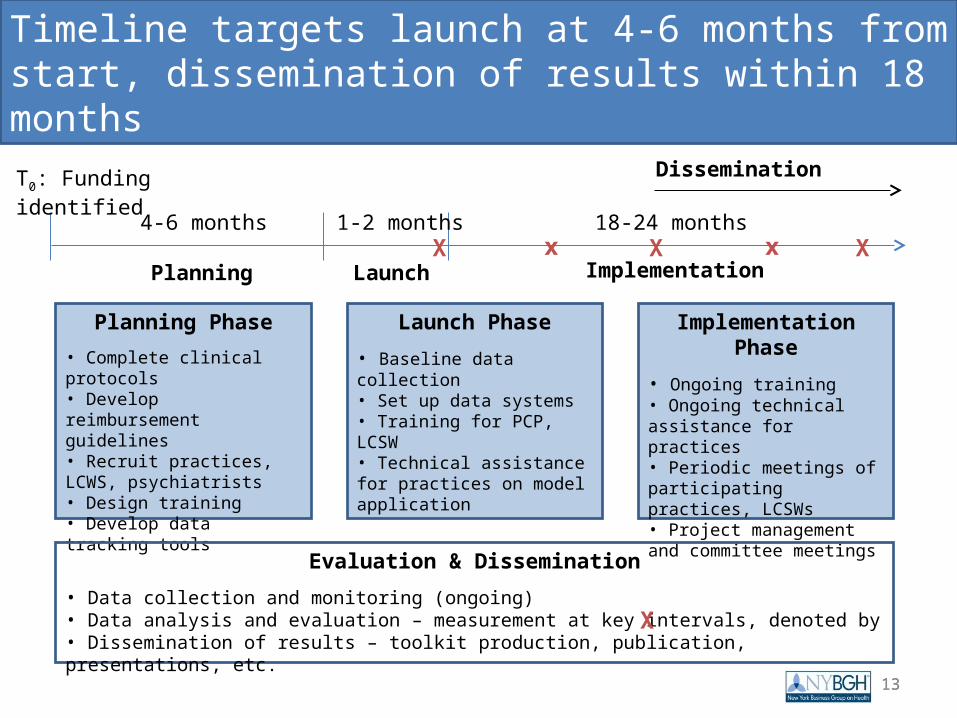
Timeline targets launch at 4-6 months from start, dissemination of results within 18 months
13
4-6 months
T0: Funding identified
1-2 months 18-24 months
Planning Phase
• Complete clinical protocols• Develop reimbursement guidelines• Recruit practices, LCWS, psychiatrists• Design training• Develop data tracking tools
Launch Phase
• Baseline data collection• Set up data systems• Training for PCP, LCSW• Technical assistance for practices on model application
Implementation Phase
• Ongoing training• Ongoing technical assistance for practices• Periodic meetings of participating practices, LCSWs• Project management and committee meetings
Planning Launch ImplementationX X Xxx
Evaluation & Dissemination
• Data collection and monitoring (ongoing)• Data analysis and evaluation – measurement at key intervals, denoted by • Dissemination of results – toolkit production, publication, presentations, etc.
X
Dissemination
14
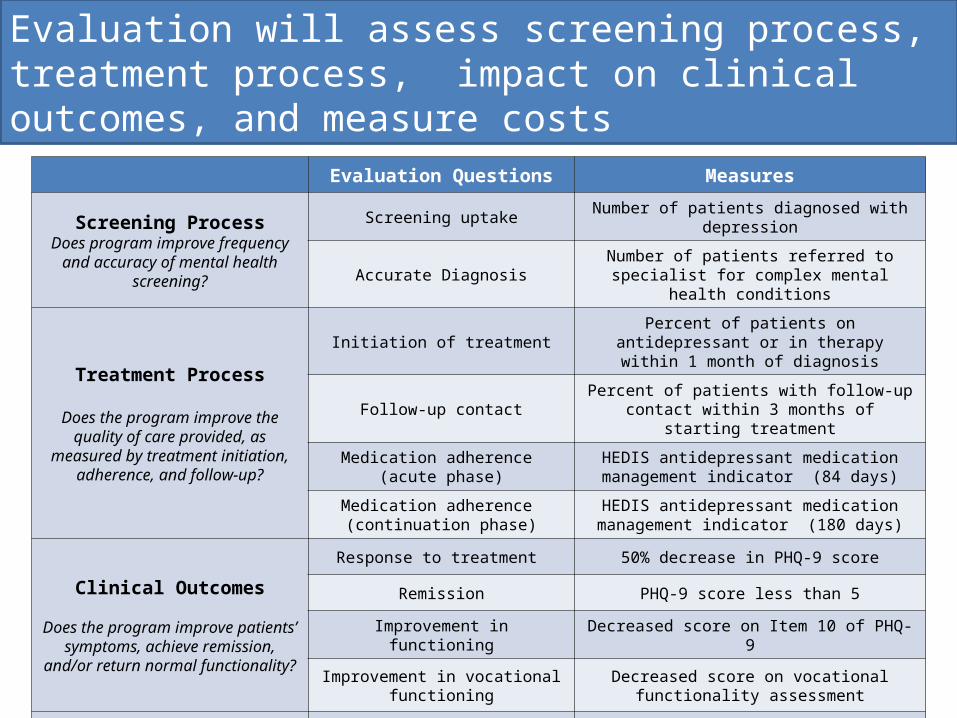
Evaluation will assess screening process, treatment process, impact on clinical outcomes, and measure costs
14
Evaluation Questions Measures
Screening ProcessDoes program improve frequency and accuracy of mental health screening?
Screening uptake Number of patients diagnosed with depression
Accurate Diagnosis Number of patients referred to specialist for complex mental health conditions
Treatment Process
Does the program improve the quality of care provided, as measured by
treatment initiation, adherence, and follow-up?
Initiation of treatment Percent of patients on antidepressant or in therapy within 1 month of diagnosis
Follow-up contact Percent of patients with follow-up contact within 3 months of starting treatment
Medication adherence (acute phase)
HEDIS antidepressant medication management indicator (84 days)
Medication adherence (continuation phase)
HEDIS antidepressant medication management indicator (180 days)
Clinical Outcomes
Does the program improve patients’ symptoms, achieve remission, and/or
return normal functionality?
Response to treatment 50% decrease in PHQ-9 score
Remission PHQ-9 score less than 5
Improvement in functioning Decreased score on Item 10 of PHQ-9
Improvement in vocational functioning
Decreased score on vocational functionality assessment
Financial Measures Cost of healthcare services 12-month average total paid claims data
15
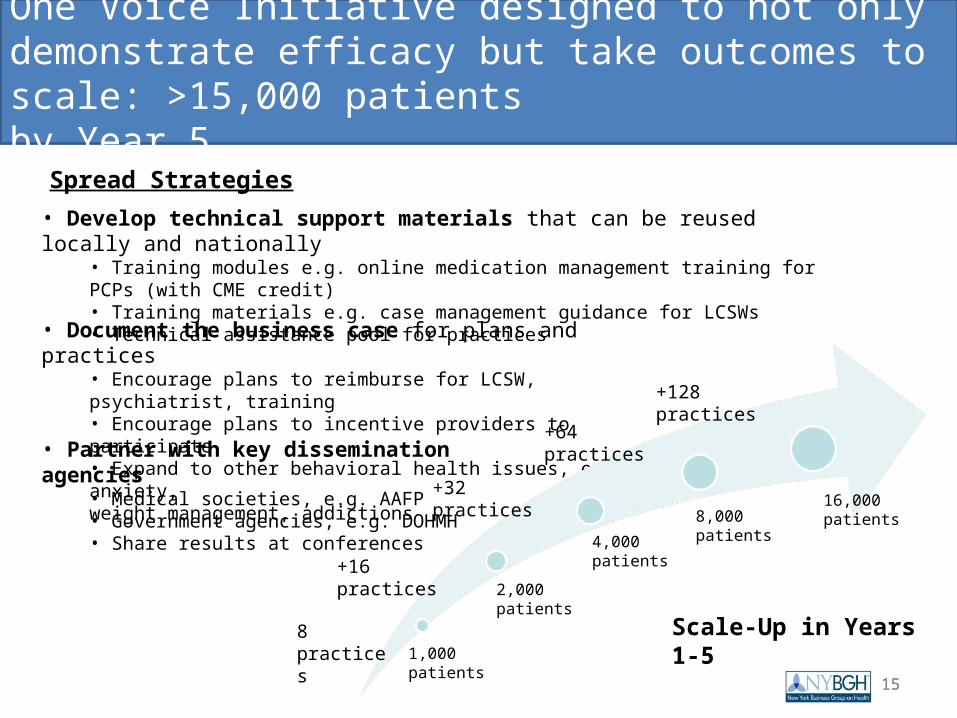
One Voice Initiative designed to not only demonstrate efficacy but take outcomes to scale: >15,000 patients by Year 5
15
Scale-Up in Years 1-5
• Develop technical support materials that can be reused locally and nationally• Training modules e.g. online medication management training for PCPs (with CME credit)• Training materials e.g. case management guidance for LCSWs• Technical assistance pool for practices
• Document the business case for plans and practices• Encourage plans to reimburse for LCSW, psychiatrist, training• Encourage plans to incentive providers to participate• Expand to other behavioral health issues, e.g. anxiety,weight management, addictions
• Partner with key dissemination agencies• Medical societies, e.g. AAFP• Government agencies, e.g. DOHMH• Share results at conferences
Spread Strategies
+16 practices
+128 practices
+64 practices
+32 practices
1,000 patients
2,000 patients
4,000 patients
8,000 patients16,000 patients
8 practices
16
Thank You
For further information:
Joslyn LevyPresidentJoslyn Levy & Associates501 Fifth Avenue, Suite 1702New York, NY [email protected]
16
Laurel PickeringExecutive DirectorNY Business Group on Health61 Broadway, Suite 2705New York, NY 10006212-252-7440 [email protected]