nys doh emsc ppcc 1 children with special health care needs lesson 8
TRANSCRIPT

1
NYS DOH EMSC PPCC
Children with Special Health Care
NeedsLesson 8
2
NYS DOH EMSC PPCC
You respond for a child with difficulty breathing at home. On arrival, you find a 4 year old laying on a hospital bed amidst a gaggle of tubes and monitors. Your RFI reveals an alert child with rapid breathing rate and effort, pale skin and gurgling sounds. The child has a tracheostomy from which the gurgling originates.
Mother states that a new nurse was on duty when the trouble began. The new nurse had trouble operating the suction unit and called mother to return home and called 911 as well.

3
NYS DOH EMSC PPCC
Mother is visibly upset and frustrated, because the pulse oximeter has been fluctuating between 91 and 94%.
Mother asks to use your suction unit, and is successful in clearing the excess mucous in a matter of seconds. Immediately, the child looks more relaxed, has easier breathing and the pulse oximeter reads 98%.
At the request of mother, you transport the child to the hospital.
4
NYS DOH EMSC PPCC
CSHCNChildren with special health care needs (CSHCN) refers to children who have or are suspected of having a serious or chronic condition of:
physical, developmental, behavioral,or emotional health that requires
health- related services of a type or amount beyond that generally required by children (based on nat’l defn.).

5
NYS DOH EMSC PPCC
Technology-Assisted
• Technology-assisted children refers to those children who depend on medical devices to support bodily function.

6
NYS DOH EMSC PPCC
Why is this Population Increasing?
• Increased survival rates from children suffering from critical injuries or disease.
• Advances in medical technology allow more children into the mainstream.
• More plentiful support services has decreased the time spent in hospitals for these children.

7
NYS DOH EMSC PPCC
Assessment: General Points
• Use RFI and Initial Assessment Steps
• The baseline of these children may be different from others in their age group.
• Ask the family member or caregiver if there are deviations from this child’s normal state.

8
NYS DOH EMSC PPCC
Assessment - Airway
• Children with special needs are susceptible to airway obstruction.
• Technology-assisted children are at risk of device failure.

9
NYS DOH EMSC PPCC
Assessment - Breathing
Children with congenital heart disease or chronic illness may be unable to compensate for even mild respiratory distress.

10
NYS DOH EMSC PPCC
Assessment - Circulation
Signs of hypoperfusion may be masked because the baseline heart rate of the child may be accelerated.
Look for other signs including AMS.

11
NYS DOH EMSC PPCC
Always Urgent CSHCN
Child who has
respiratory distress or
signs of hypoperfusion
is treated as an urgent condition.
Transport ASAP with oxygen.
Additional assessment while en route.

12
NYS DOH EMSC PPCC
Delayed Mental DevelopmentAssessment Concerns
Use a sensitive approach:
• Ask for the child's name and use it.
•If necessary, use "special child" rather than terms like "retarded" or "slow."

13
NYS DOH EMSC PPCC
Ask the Parents/Caregivers
Determine the child's normal abilities and behavior in the following areas:
• mental status
• interaction with parents and strangers
• verbal abilities
• ability to sit, stand, and walk
• muscle tone and strength
14
NYS DOH EMSC PPCC
Ask the Parents/Caregivers
• Are there differences from normal abilities and behaviors now?
• Were these changes the primary reason for calling EMS?

15
NYS DOH EMSC PPCC
CUPS Assessment of Children with Special
Needs
Category
Assessment
Actions
16
NYS DOH EMSC PPCC
Critical
Assessment
Absent• Airway• Breathing• Circulation• AVPU = P or U
Action
Support and Transport
17
NYS DOH EMSC PPCC
UnstableAssessmentCompromised
• Airway• Breathing• Circulation• AVPU=V or P or• Normal airway
breathing and circulation, AVPU=A
with other risk factors.
Action
Support and Transport

18
NYS DOH EMSC PPCC
Potentially Unstable
AssessmentCompromised
• Airway• Breathing• Circulation• AVPU=V or P or• Normal ABC’s,
AVPU=A with other risk factors.
Action
Support and Transport

19
NYS DOH EMSC PPCC
StableAssessment
Normal • Airway• Breathing• Circulation• AVPU=V or A
Action
CSHCN or technologically dependent children often have the potential to abruptly deteriorate. For this reason, they are not considered stable.
20
NYS DOH EMSC PPCC
SPECIAL TECHNOLOGY
EMTs and Paramedics will
encounter various people who assist
these children.
• Tracheostomy Tubes
• Home Ventilators
• CPAP Devices
• Central Intravenous Catheters
• Pacemakers
• Feeding Catheters
• CSF Shunts
• Colostomies and Illeostomies

21
NYS DOH EMSC PPCC
Tracheostomy
A surgical opening into the trachea through which a tracheostomy tube can
be passed. The child then breathes through this opening.
22
NYS DOH EMSC PPCC
Reasons for a Tracheostomy
• To bypass an airway obstruction caused by birth defect, surgery, or trauma.
• To allow for long-term ventilator use.
• To access and remove excessive secretions.

23
NYS DOH EMSC PPCC
Single Cannula Tracheostomy Tube
• Used on all newborns and most pediatric patients.
• Has one single passage used for both air flow and suctioning.

24
NYS DOH EMSC PPCC
Double Cannula Tracheostomy Tube
• Features a removable inner cannula that fits inside an outer cannula.
• Inner cannula must be in place to ventilate the patient
• Outer cannula keeps the stoma open while the inner is removed for cleaning.

25
NYS DOH EMSC PPCC
Fenestrated Tracheostomy Tube
• Allows the child to breathe through either the tube or the mouth.
• Teaches the child to breathe through the mouth.
• Allows for speech.
26
NYS DOH EMSC PPCC
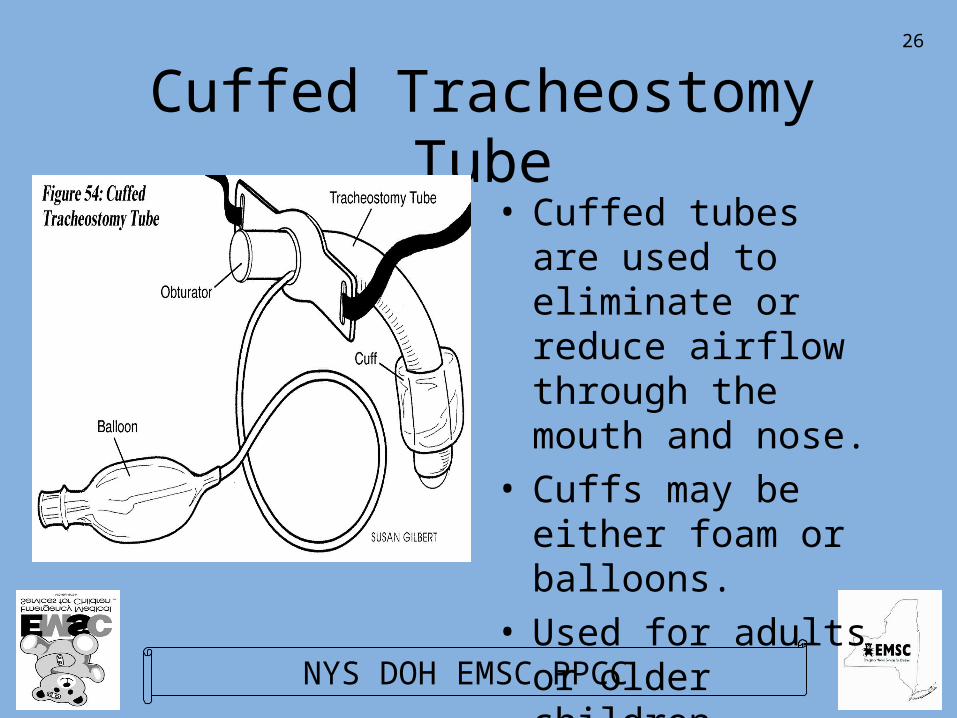
Cuffed Tracheostomy Tube• Cuffed tubes are
used to eliminate or reduce airflow through the mouth and nose.
• Cuffs may be either foam or balloons.
• Used for adults or older children.

27
NYS DOH EMSC PPCC
Tracheostomy Emergencies
• EMTs may be called on to respond to children with tracheostomies for the following reasons:– obstruction of the tube– displacement of the tube– psychological care of the patient or care
giver

28
NYS DOH EMSC PPCC
Tracheostomy Emergencies
EMTs should follow assessment priorities with additional focus on the airway:
• Always consider obstructed airway.
• Check and recheck.
• May need suctioning repeatedly.
29
NYS DOH EMSC PPCC
Tracheostomy - Management
To correct respiratory distress for a patient with a tracheostomy:
– place a rolled towel under the child’s shoulders,
– make sure the tracheostomy tube is properly seated and the obturator/ decannulation plug has been removed.

30
NYS DOH EMSC PPCC
Tracheostomy - Management• Attempt assisted
ventilation through the tracheostomy tube.
• If the child is on a home ventilator, remove it and manually ventilate the child with a bag-valve device.
31
NYS DOH EMSC PPCC
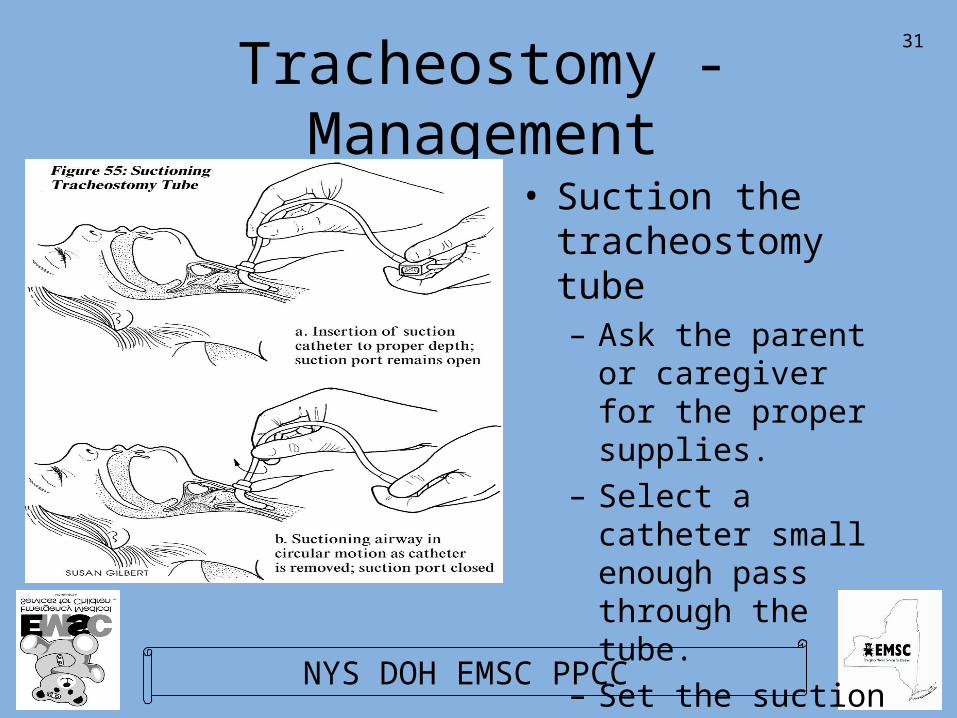
Tracheostomy - Management
• Suction the tracheostomy tube– Ask the parent or
caregiver for the proper supplies.
– Select a catheter small enough pass through the tube.
– Set the suction at 100 mm/Hg or less.
32
NYS DOH EMSC PPCC
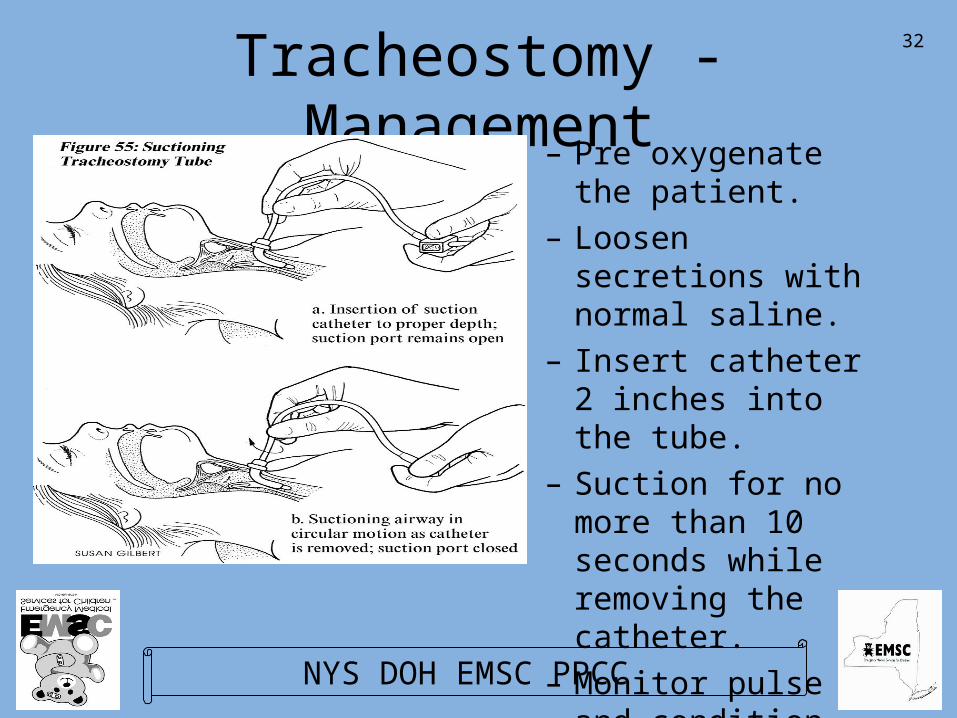
Tracheostomy - Management– Pre oxygenate the
patient.– Loosen secretions
with normal saline.– Insert catheter 2
inches into the tube.– Suction for no more
than 10 seconds while removing the catheter.
– Monitor pulse and condition.

33
NYS DOH EMSC PPCC
Tracheostomy - Management
• Attempt to remove/ replace the tube– obtain a replacement
tube.– If the existing tube
has a balloon cuff, deflate it.
– Cut the ties that hold the tube in place and remove the tube.
34
NYS DOH EMSC PPCC
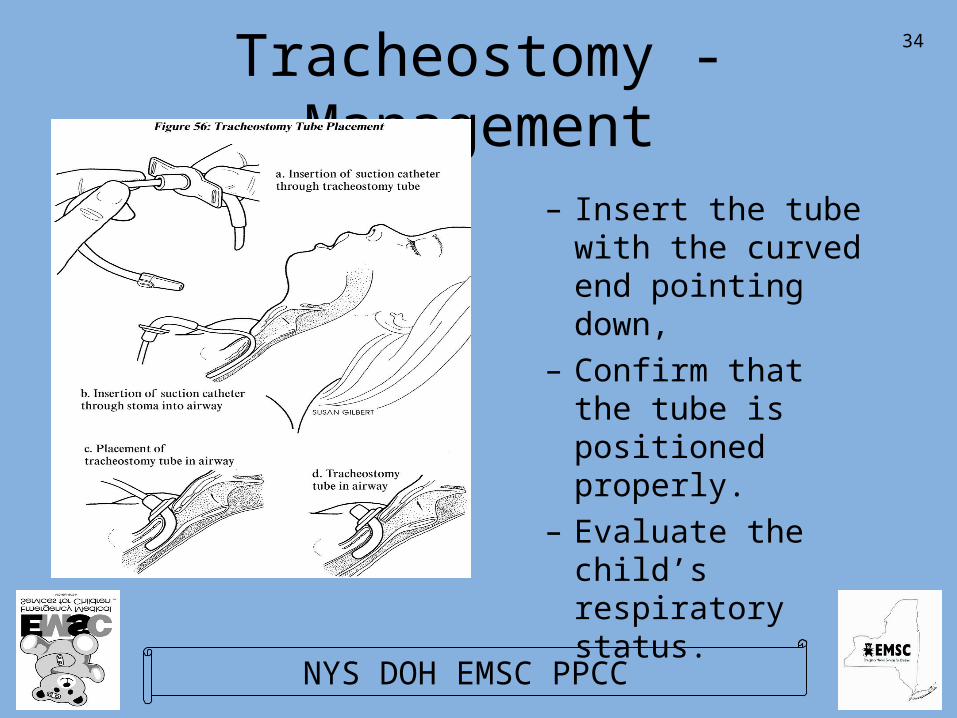
Tracheostomy - Management
– Insert the tube with the curved end pointing down,
– Confirm that the tube is positioned properly.
– Evaluate the child’s respiratory status.

35
NYS DOH EMSC PPCC
Tracheostomy - Management
• Perform ventilations with a bag valve mask over the stoma or the mouth.

36
NYS DOH EMSC PPCC
Tracheostomy - Management
• Children with tracheostomies often have asthma.
• Treat according to local protocol.

37
NYS DOH EMSC PPCC
Home Ventilators
• Children who depend on home ventilators have a problem with their respiratory drive or respiratory effort.

38
NYS DOH EMSC PPCC
Home Ventilators - Settings
• Home ventilators are set to control:– breathing rate– tidal volume
– FIO2
– Peak Inspiratory Pressure (PIP)– Positive End Expiratory Pressure (PEEP)

39
NYS DOH EMSC PPCC
Home Ventilators - Types
• There are two types of home ventilators:– Pressure cycled ventilators– Volume ventilators
40
NYS DOH EMSC PPCC
Home Ventilators - Modes
• Home ventilators operate in two modes:– Intermittent Mechanical Ventilation (IMV)– Continuos Mechanical Ventilation (CMV)

41
NYS DOH EMSC PPCC
Home Ventilators - Management
• Possible causes of emergencies involving home ventilators include:– equipment failure– problems with the oxygen supply– an obstruction in the ventilator tubing– an obstruction in the tracheostomy tube– a medical condition
42
NYS DOH EMSC PPCC
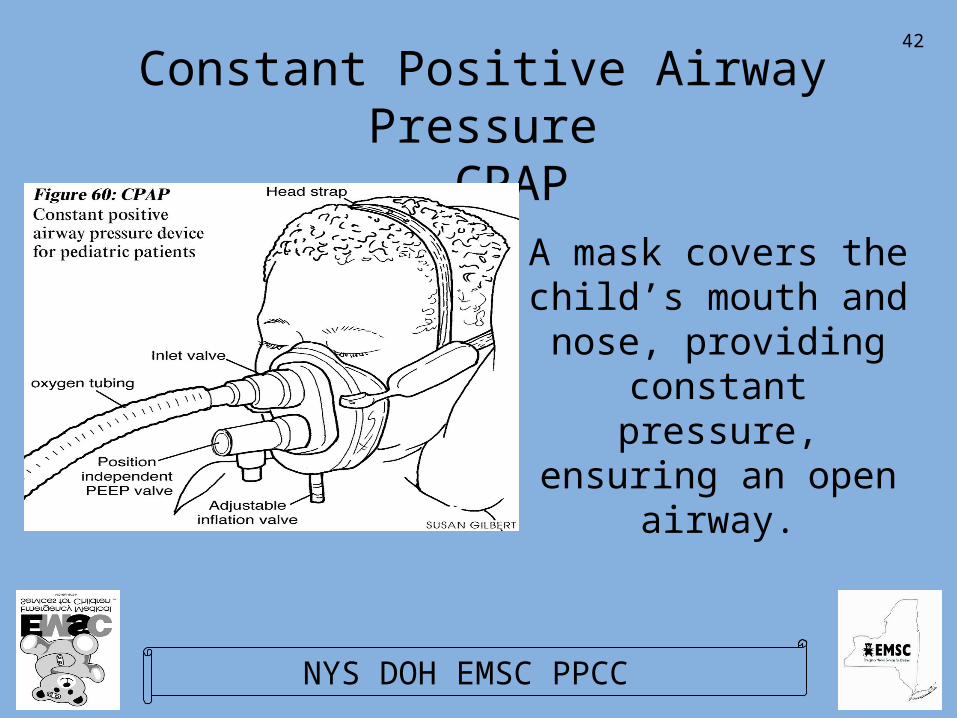
Constant Positive Airway Pressure- CPAP
A mask covers the child’s mouth and nose, providing
constant pressure, ensuring an open
airway.
43
NYS DOH EMSC PPCC
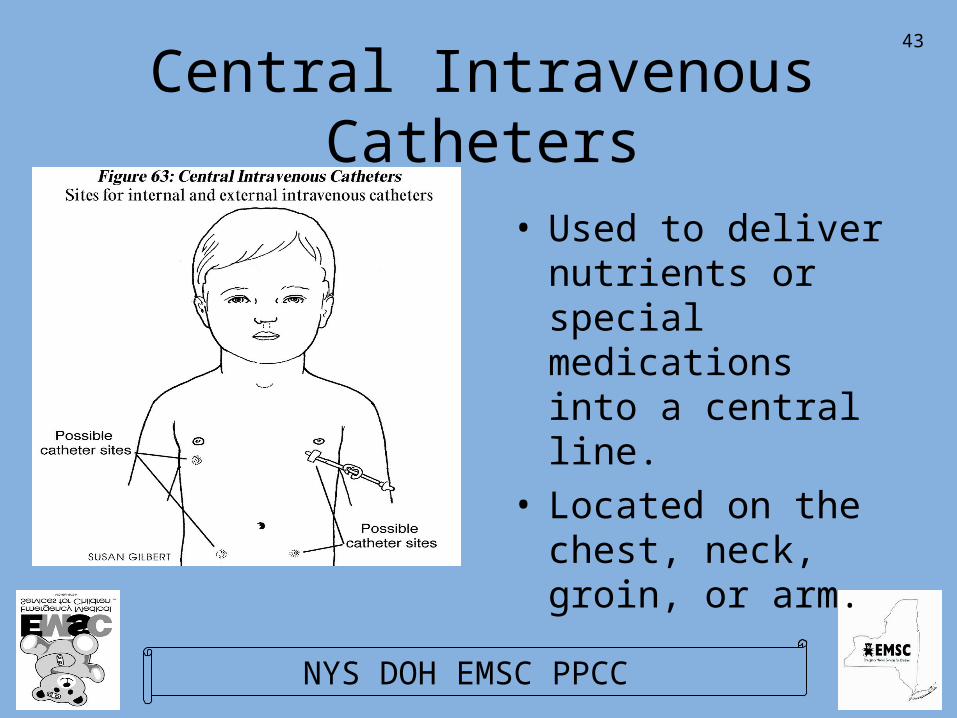
Central Intravenous Catheters
• Used to deliver nutrients or special medications into a central line.
• Located on the chest, neck, groin, or arm.

44
NYS DOH EMSC PPCC
Central Intravenous Catheters
There are two common types of catheters used for this purpose:
•Broviac Catheters
•Hickman or Mediport Catheters
45
NYS DOH EMSC PPCC
Central Intravenous Catheters
Problem• Bleeding or broken
catheter
• Obstructed• Fever
Solution• Control bleeding with
direct pressure and transport, clamp catheter end.
• Transport, request ALS to clear obstruction.
• Transport immediately.

46
NYS DOH EMSC PPCC
Pacemakers
Pacemakers regulate heart rate. A pacemaker is needed if the natural heart
rate is not fast enough to ensure adequate perfusion.

47
NYS DOH EMSC PPCC
Pacemakers - Types
There are three types of pacemakers:
•Demand
•Constant
•Antiarrhythmia

48
NYS DOH EMSC PPCC
Pacemaker - Management
Problem
• Pacemaker failure
• Failure to
compensate
Solution• Transport
immediately, request ALS back-up, treat for shock as indicated.
• Transport immediately, request ALS back-up, treat for shock as indicated.
49
NYS DOH EMSC PPCC
Pacemaker - Management
Problem
• Dislodged Leads
• Broken Leads
Solution• Treat symptoms as
necessary, rapid transport.
• Treat symptoms, treat for shock, rapid transport.
50
NYS DOH EMSC PPCC
Feeding Catheters
A feeding catheter provides a route for nutritional support when the child is
unable to take food by mouth

51
NYS DOH EMSC PPCC
Surgical Feeding Catheters
• Used for long term support of the child.– Gastrostomy
Tube(GT)– Jejunostomy
Tube(JT)– Gastrostomy Button

52
NYS DOH EMSC PPCC
Nonsurgical Feeding TubesUsed for temporary support of the child– Nasogastric Tube
(NGT)– Nasojejunal Tube
(NJT)– Orogastric Tube
(OGT)– Orojejunal Tube
(OJT)
53
NYS DOH EMSC PPCC
Feeding Tubes - Management
Problem
• Bleeding
• Leaking
• Broken
• Dislodged
Solution
• Control bleeding at site.
• Treat skin irritation
• Monitor, transport
• Monitor, transport

54
NYS DOH EMSC PPCC
CSF Shunts
• A special Catheter to drain cerebrospinal fluid (CSF) from the brain.
• Runs under the skin from the skull to the chest or abdomen.
55
NYS DOH EMSC PPCC
CSF Shunt Concerns
• Altered mental status
• Listlessness• Increased sleep• Nausea or vomiting• Fever• Headaches• Difficulty walking
• Initiate transport• Continually assess
and reassess ABCs• Request ALS when
the child has - Periods without breathing - Seizures - Rapid AMS

56
NYS DOH EMSC PPCC
Colostomies and Ileostomies
• A portion of the small or large intestine is attached to a surgical opening in the abdominal wall and a bag is placed to collect digestive waste.
57
NYS DOH EMSC PPCC
Congenital Heart Disease
• Children may be born with structural defects of the heart:– Heart valve problems– Arteries don’t function correctly– Cyanotic heart disease– Heart doesn’t fire properly
58
NYS DOH EMSC PPCC
Congenital Heart Disease - Mgmt
EMTs should consider:– These children will have low blood oxygen
levels.– Hypoperfusion (shock) is severely life
threatening.– Children with irregular pulses should be
rapidly transported and constantly monitored.
59
NYS DOH EMSC PPCC
Children with Mobility Problems
• Mobility problems may be caused by spasticity or paralysis.– Spasticity is a condition where muscles
and tendons become tight, restricting movement of joints and extremities.
– Paralysis is the inability to move a portion of the body.

60
NYS DOH EMSC PPCC
Children with Chronic Illnesses
• Children with chronic illness may have medical emergencies for other reasons:– They may experience an unrelated illness
or a traumatic injury.– They may suffer a sudden worsening of the
underlying chronic condition.
61
NYS DOH EMSC PPCC
Children with Chronic Illnesses - Special Considerations
• The child’s baseline vitals may be different from others his/her own age.
• The child may have a decreased tolerance.• The child may have received significant
medical care prior to EMS’ arrival.• The parent/caregiver can provide valuable
information.

62
NYS DOH EMSC PPCC
Summary• CSHCN - Technology Assisted children
present unique challenges for EMTs.
• Modify RFI and Initial Assessment steps
• Focus on any condition of the airway, respiratory or circulatory system.
• Take nothing for granted.
• Parent/caregiver is key in assessment.