objectives - · pdf filehx of rheumatic fever etiology of chf doe, ... % decrease in mean...
TRANSCRIPT

1
ObjectivesObjectives
•• Volume regulation entails the physiology of salt Volume regulation entails the physiology of salt content regulationcontent regulation
•• The edematous states reflect the The edematous states reflect the pathophysiologypathophysiologyof salt content regulationof salt content regulation
•• The mechanisms of normal volume regulation The mechanisms of normal volume regulation mediate the mediate the pathophysiologypathophysiology of the edematous of the edematous statesstates
ObjectivesObjectives
•• Serum sodium concentration reflects the physiology Serum sodium concentration reflects the physiology of water metabolismof water metabolism
•• Hypo and Hypo and hypernatremiahypernatremia reflect the reflect the pathophysiologypathophysiology of water metabolismof water metabolism
•• The mechanisms regulating normal water The mechanisms regulating normal water metabolism mediate the metabolism mediate the pathophysiologypathophysiology of hypo of hypo and and hypernatremiahypernatremia

2
Case SummaryCase Summary
HxHx of rheumatic feverof rheumatic fever etiology of CHFetiology of CHFDOE, SOB, DOE, SOB, ralesrales pulmonary edemapulmonary edemaPedal edema, Pedal edema, abdabd girthgirth peripheral edemaperipheral edema
weightweight
Question~ why edema?Question~ why edema?
Case SummaryCase Summary
HxHx of rheumatic feverof rheumatic fever etiology of CHFetiology of CHFDOE, SOB, DOE, SOB, ralesrales pulmonary edemapulmonary edemaPedal edema, Pedal edema, abdabd girthgirth peripheral edemaperipheral edema
weightweight
Serum [Na] = 128 Serum [Na] = 128 meqmeq/L/LQuestion~ why Question~ why hyponatremiahyponatremia??

3
70 kg subject:70 kg subject:Total body water 42LTotal body water 42L
2/3 Intracellular 2/3 Intracellular 28L28L1/3 1/3 ExtracellularExtracellular 14L14L
2/3 interstitial 2/3 interstitial 9L9L1/3 intravascular1/3 intravascular 5L5L
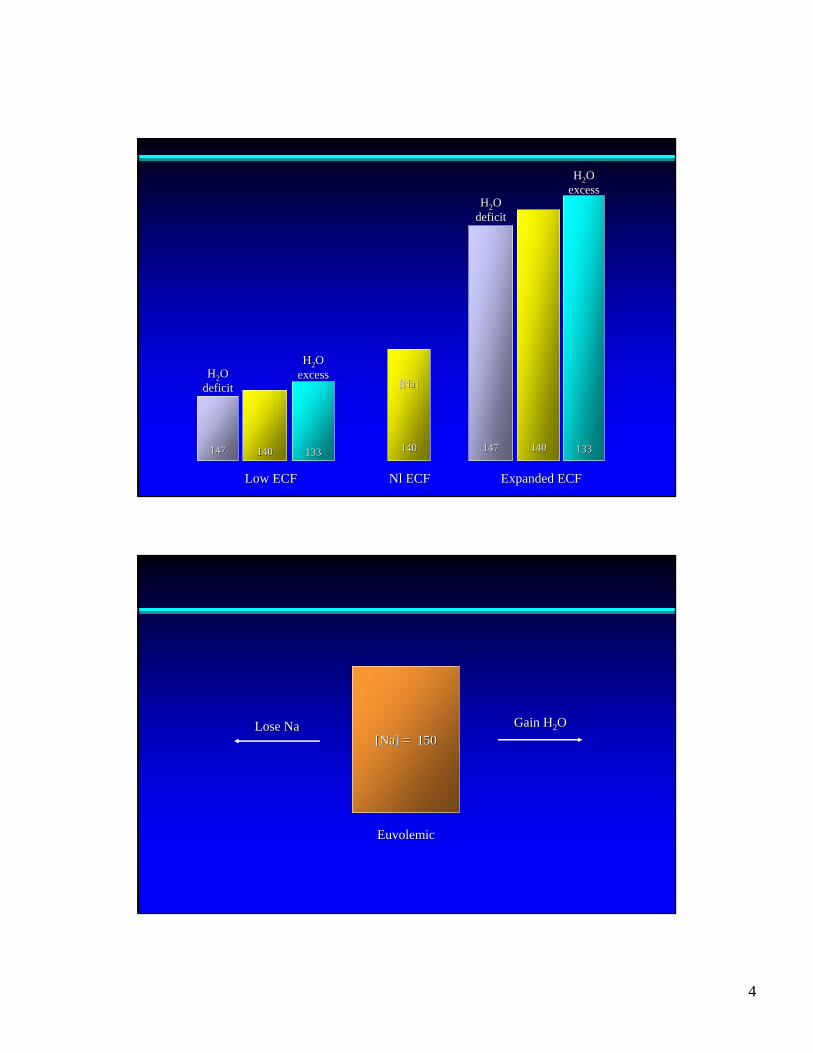
Low ECFLow ECF NlNl ECFECF Expanded ECFExpanded ECF
4
HH22OOdeficitdeficit
HH22OOexcessexcess
HH22OOdeficitdeficit
HH22OOexcessexcess
133133140140147147
[Na][Na]
140140133133140140147147
Low ECFLow ECF NlNl ECFECF Expanded ECFExpanded ECF
[Na] = 150[Na] = 150Lose NaLose Na Gain HGain H22OO
EuvolemicEuvolemic

5
Tonicity and Serum [Na]Tonicity and Serum [Na]
•• Cell membranes are freely permeable to waterCell membranes are freely permeable to water•• No osmotic gradients exist between fluid compartmentsNo osmotic gradients exist between fluid compartments•• The tonicity of the intravascular compartment reflects the The tonicity of the intravascular compartment reflects the
tonicity of all fluid compartmentstonicity of all fluid compartments•• The calculated serum The calculated serum osmolalityosmolality is given by:is given by:
([Na]x2) + ([K]x2) + [([Na]x2) + ([K]x2) + [glucgluc] + [] + [BUNBUN]]1818 2.82.8
= (140x2) + (4x2) + = (140x2) + (4x2) + 9090 + + 12121818 2.82.8
= 280 + 8 + 5 + 4= 280 + 8 + 5 + 4
Free WaterFree Water
•• [Na] reflects balance of H[Na] reflects balance of H22O relative to saltO relative to salt•• HH22O input and output must be assessed but again O input and output must be assessed but again
relative to salt input and outputrelative to salt input and output•• Concept of Concept of ““Free HFree H22OO””::
one L 1/2 NS =one L 1/2 NS =1/2 L NS + 1/2 L salt free H1/2 L NS + 1/2 L salt free H22OO

6
Determinants of TonicityDeterminants of Tonicity
Free HFree H22O intake vs. free HO intake vs. free H22O excretion + free HO excretion + free H22O lossesO losses
OralOral UrineUrine RespiratoryRespiratoryIntravenousIntravenous CutaneousCutaneous
VolumeVolume ConcentrationConcentration
Proximal TubuleProximal Tubule
PeritubularPeritubular CapillariesCapillaries
Urinary SpaceUrinary Space
GlomerularGlomerularCapillariesCapillaries
JGAJGA
Afferent Afferent ArterioleArteriole
Efferent Efferent ArterioleArteriole

7
Free HFree H22O excretionO excretion Free HFree H22O retentionO retentionDeliveryDelivery MedullaryMedullary gradientgradient
GFR (GFR (ScrScr))Proximal Proximal reabsorptionreabsorption Collecting duct Collecting duct
HH22O permeabilityO permeabilityDiluting segment Diluting segment
Collecting DuctCollecting DuctHH22O permeabilityO permeability
VasopressinVasopressin
•• AntidiureticAntidiuretic hormone: hormone: neurohypophysealneurohypophyseal•• VV22--receptor: collecting ductreceptor: collecting duct

8
300300
600600
900900
12001200
14001400
35%35%
25%25%
15%15%
3%3%
< 1%< 1%
10%10%No ADHNo ADH
MaximalMaximalADHADH
Proximal Proximal tubuletubule
HenleHenle’’sslooploop
DistalDistaltubuletubule
Cortical Cortical collectingcollecting
ductduct
MedullaryMedullarycollectingcollecting
ductduct
Osm
olar
ityO
smol
arity
(( mO
smm
Osm
/L)
/L)
Urinary Concentration and DilutionUrinary Concentration and Dilution
% water remaining
ntsntsbrbr
opop
dsds
nhnhahah
ococ
sonsonoror
pvnpvn

9
ThirstThirst
1212
1010
88
66
44
22
00
270270 280280 290290 300300 310310
Plasma Plasma OsmolalityOsmolality ((mOsmmOsm/kg)/kg)
Plas
ma
Vas
opre
ssin
(pg/
ml)
Plas
ma
Vas
opre
ssin
(pg/
ml)
14001400
12001200
10001000
800800
600600
400400
200200
00
00 11 22 33 44 55 1010 1515
Plasma AVP (pg/ml)Plasma AVP (pg/ml)
Urin
e U
rine
Osm
olal
ityO
smol
ality
(( mO
smm
Osm
/kg)
/kg)

10
HyponatremiaHyponatremia((HypoosmolarHypoosmolar states)states)
•• Intake of free H2O > renal output + insensible lossesIntake of free H2O > renal output + insensible losses
•• Failure to make a large volume of dilute urineFailure to make a large volume of dilute urine–– Failure to deliverFailure to deliver–– Failure to diluteFailure to dilute–– Failure to suppress ADHFailure to suppress ADH
NormalNormal Congestive Heart FailureCongestive Heart FailureGCGC PTCPTC PTCPTCGCGC
ΔΔPP
ΔπΔπArb
itrar
y Pr
essu
reA
rbitr
ary
Pres
sure
Uni
tsU
nits
OO OO OO OOII II II II
A.A. B.B.
ΔΔPP
ΔπΔπ
ΔπΔπ
RPFRPF RPFRPF
GFRGFR GFRGFR
Eff Eff ArtArt
Eff Eff ArtArt
ΔΔPP
ΔπΔπ
ΔΔPP

11
ntsntsbrbr
opop
dsds
nhnhahah
ococ
sonsonarar
pvnpvn
10001000
600600400400
200200100100
60604040
2020
10106644
22
11
00 1515 3030 4545
% Decrease in Mean Arterial Pressure% Decrease in Mean Arterial Pressure
Plas
ma
Vas
opre
ssin
(pg/
ml)
Plas
ma
Vas
opre
ssin
(pg/
ml)

12
PressurePressure
VolumeVolumeBasalBasal
OsmolalityOsmolality
2525
2020
1515
1010
55
00
--3030 --2020 --1010 00 +10+10 +20+20
% Change% Change
Plas
ma
Vas
opre
ssin
Plas
ma
Vas
opre
ssin
(pg/
ml)
(pg/
ml)
--2020--1515
--1010NN
+10+10+15+15
+20+20
1010
88
66
44
22
00
Plas
ma
Vas
opre
ssin
Plas
ma
Vas
opre
ssin
pg/m
lpg
/ml
HypovolemiaHypovolemia ororHypotensionHypotension
HypervolemiaHypervolemia ororHypertensionHypertension
260260 270270 280280 290290 300300 310310 320320 330330 340340
Plasma Plasma OsmolalityOsmolalitymOsmmOsm/kg/kg

13
HyponatremiaHyponatremia in CHFin CHF
Free water intake has exceeded free water outputFree water intake has exceeded free water outputWhy has the kidney failed to make a large volume of dilute urineWhy has the kidney failed to make a large volume of dilute urine??
ThirstThirst AIIAII
Distal delivery Distal delivery AIIAII
Dilution at TALDilution at TAL DiureticsDiureticsHypokalemiaHypokalemia
ADHADH Volume Stimulus to ADHVolume Stimulus to ADH
1919181817171616151514141313121211111010998877665544332211Day of Experiment
TIVCTIVCConstrictionConstriction
IncreaseIncreaseConstrictionConstriction
ReleaseReleaseConstrictionConstriction
5050
150150
100100
HeartRate
100100
9090
8080
7070
Mean AorticMean AorticPressurePressure(mmHg)(mmHg)

14
2020
1515
1010
55
00
PlasmaPlasmaReninRenin ActivityActivity
(mg/ml/h)(mg/ml/h)
Plas
ma
Plas
ma
Ren
inR
enin
Act
ivity
Act
ivity
(( ngng
/ml/h
r)/m
l/hr)
Pretreatment Serum Na Concentration (Pretreatment Serum Na Concentration (mEq/lmEq/l))
150150
6060
2525
1010
55
22
11
0.50.5
0.20.2
124124 128128 132132 136136 140140 144144 148148

15
Cardiac OutputCardiac Output
LVEDPLVEDP
Cardiac Cardiac OutputOutput
LVEDPLVEDP

16
00 66 1212 1818 2424 3030 3636
2020
00
4040
6060
8080
100100
MonthsMonths
% S
urvi
val
% S
urvi
val p<0.001p<0.001
Na >130 (n=163)Na >130 (n=163)
Na Na ≤≤ 130 (n=40)130 (n=40)
HyponatremiaHyponatremia with Increased ADHwith Increased ADH
•• Volume stimulusVolume stimulus
•• Syndrome of Inappropriate ADHSyndrome of Inappropriate ADH
•• Certain drugs, Certain drugs, endocrinopathiesendocrinopathies

17
DaysDays
5757
5454
22 44 66 88 1010 1212
Body Weight Body Weight kg kg
33
22
11
Urine VolumeUrine VolumeL/dayL/day
200200
100100Urinary Sodium Urinary Sodium
mEqmEq/day/day
10001000
500500
UrinaryUrinaryOsmololityOsmololity
mOsm/kgHmOsm/kgH22OO
PitressinPitressinRestrict HRestrict H22OO
140140
130130
120120
Serum [Na]Serum [Na]mEqmEq/L/L
–– BronchogenicBronchogenic carcinomacarcinoma–– AdenocarcinomaAdenocarcinoma of pancreasof pancreas–– AdencarinomaAdencarinoma of duodenumof duodenum–– Carcinoma of Carcinoma of ureterureter
–– TuberculosisTuberculosis–– PneumoniaPneumonia–– AspergillosisAspergillosis with with cavitationcavitation
–– Brain tumorBrain tumor–– EncephalitisEncephalitis–– MeningitisMeningitis–– Brain abscessBrain abscess–– Head injuryHead injury
–– LymphomaLymphoma–– HodgkinHodgkin’’s diseases disease–– ThymonaThymona
–– Lung abscessLung abscess–– Chronic chest infectionChronic chest infection
–– SubarachnoidSubarachnoid hemorrhagehemorrhage–– LandryLandry--GuillainGuillain--BarreBarre syndromesyndrome–– Systemic lupus Systemic lupus erythematsuserythematsus–– Acute intermittent Acute intermittent porphyriaporphyria
EctopicEctopic ADH Production from TumorsADH Production from Tumors
Etiology of SIADHEtiology of SIADH
Pulmonary Disease Associated with SIADHPulmonary Disease Associated with SIADH
SIADH in Central Nervous System DiseaseSIADH in Central Nervous System Disease

18
Approach to Approach to HyponatremiaHyponatremia
ADH despite ADH despite SSNaNa
ECF and intravascularECF and intravascular DrugsDrugscompartments depletedcompartments depleted(diarrhea)(diarrhea) EndocrinopathiesEndocrinopathies
SIADHSIADHECF expanded butECF expanded but tumorstumorsintravascular compartmentintravascular compartment pulmonarypulmonaryarterially arterially underfilledunderfilled (CHF)(CHF) CNSCNS
BUN/CrBUN/Cr
Renal Failure
Often Often UUNaNa ““nlnl UUNaNa”” CrCr
VasopressinVasopressin
•• AntidiureticAntidiuretic hormone Vhormone V22--receptor: receptor: collecting ductcollecting duct
•• VasopressorVasopressor hormone Vhormone V11--receptor: receptor: vascular smooth musclevascular smooth muscle

19
--1414 --1313 --1212 --1111 --1010 --99 --88 --77 --66 --55
Agonist (log M)Agonist (log M)
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
% r
educ
tion
in lu
men
dia
met
er%
red
uctio
n in
lum
en d
iam
eter
Efferent Arteriole of RatEfferent Arteriole of Rat
130
120120
110110
100100
9090
8080
7070
6060
5050
4040
3030
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424 2626 2828 3030
Systolic Blood PressureSystolic Blood Pressure
Diastolic Blood PressureDiastolic Blood Pressure
Pulse RatePulse Rate
Time (minutes)Time (minutes)
Average Changes in Blood Pressure and Pulse Rate in Nine Average Changes in Blood Pressure and Pulse Rate in Nine Normal Persons During Intravenous Administration of Normal Persons During Intravenous Administration of PitressinPitressin

20
Vasopressin in Vasopressin in VasodilatoryVasodilatory ShockShock
•• Exogenous vasopressin is a potent Exogenous vasopressin is a potent pressorpressor•• Endogenous vasopressin is deficientEndogenous vasopressin is deficient•• Vasopressin restores Vasopressin restores pressorpressor responsiveness by responsiveness by
inhibiting inhibiting vasodilatoryvasodilatory mechanismsmechanisms
Vasopressin In Vasopressin In VasodilatoryVasodilatory ShockShock88
00
00
0.000.00
55
0.040.04
140140
120120
100100
8080
150150
100100
5050
00
88
00
00
0.000.00
55
0.040.04
140140
120120
100100
8080
150150
100100
5050
00
NEPINEPIμμg/ming/min
EPIEPIμμg/ming/min
AVPAVPU/minU/min
SAPSAPmmHgmmHg
UUml/hml/h
NEPINEPIμμg/ming/min
EPIEPIμμg/ming/min
AVPAVPU/minU/min
SAPSAPmmHgmmHg
UUml/hml/h
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2424 2626 2828
Time (hours)Time (hours)

21
Effect of Vasopressin in Septic Shock in ManEffect of Vasopressin in Septic Shock in Man(n=10)(n=10)
ControlControl AVPAVP
160160
140140
120120
100100
8080
SBPSBP(mmHg)(mmHg)
88
77
66
55
COCO(L/min)(L/min)
15001500
10001000
500500
SVRSVR(dyne (dyne •• sec/cmsec/cm55))
NorepinephrineNorepinephrine(median)(median)
32 32 μμg/ming/min 0 0 μμg/ming/min
120120
100100
8080
0.020.02
0.000.00
11 22 33 44 55 66
Time (hour)Time (hour)
SAPSAPmmHgmmHg
AVPAVPU/minU/min
Discontinuation of Vasopressin in FirstDiscontinuation of Vasopressin in FirstProspective Patient in Prospective Patient in VasodilatoryVasodilatory Septic ShockSeptic Shock

22
140140
120120
100100
8080AVPAVP No AVPNo AVP AVPAVP
SAPSAP(mmHg)(mmHg)
Discontinuation of Vasopressin in 6 of 10 PatientsDiscontinuation of Vasopressin in 6 of 10 Patientsin in VasodilatoryVasodilatory Septic ShockSeptic Shock
Vasopressin in Vasopressin in VasodilatoryVasodilatory ShockShock
• Exogenous vasopressin is a potent pressor• Endogenous vasopressin is deficient• Vasopressin restores pressor responsiveness by
inhibiting vasodilatory mechanisms

23
00
55
1010
1515
2020
2525
3030
3535
Septic ShockSeptic Shock(n=19)(n=19)
CardiogenicCardiogenic ShockShock(n=12)(n=12)
3.1 3.1 ±± 0.40.4
22.7 22.7 ±± 2.22.2
AVPAVPpg/mlpg/ml
VasodilatoryVasodilatory Shock States with Vasopressin Shock States with Vasopressin Deficiency and HypersensitivityDeficiency and Hypersensitivity
•• Septic shockSeptic shock•• CPBCPB--induced induced vasodilatoryvasodilatory shockshock•• MilrinoneMilrinone--induced induced vasodilatoryvasodilatory shockshock•• Brain deathBrain death•• Irreversible shockIrreversible shock
24
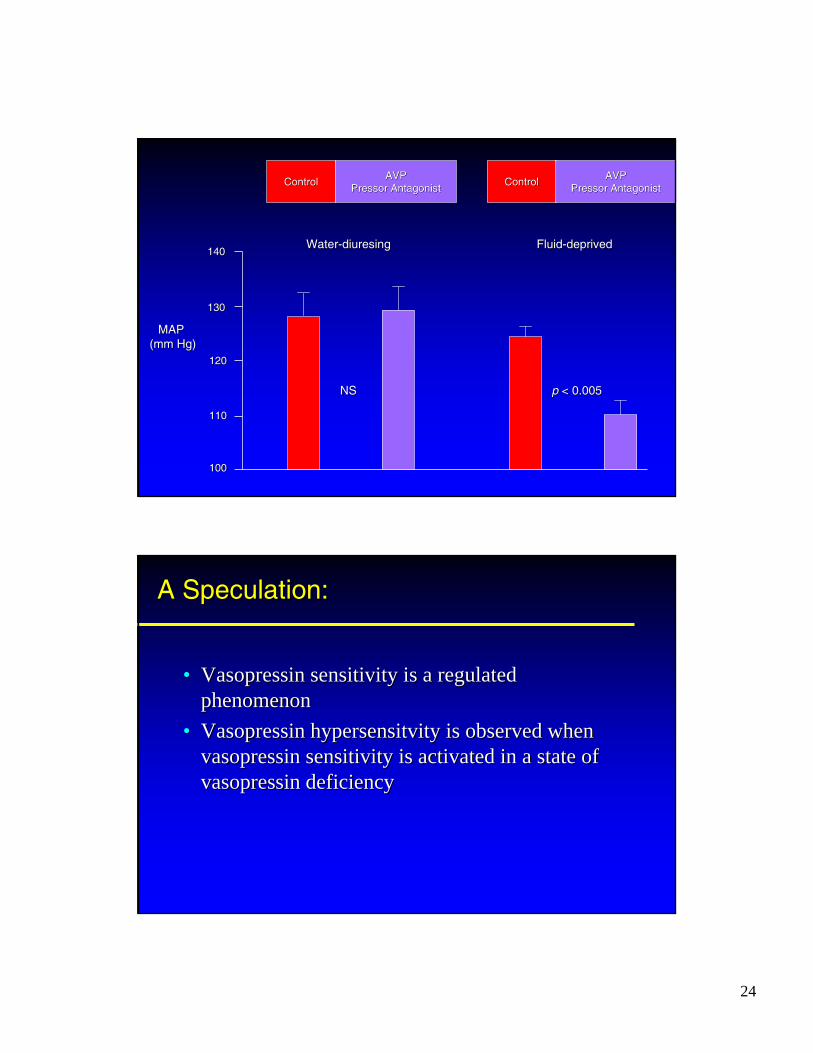
ControlControl AVPAVPPressorPressor AntagonistAntagonist ControlControl AVPAVP
PressorPressor AntagonistAntagonist
140140
130130
120120
110110
100100
NSNS pp < 0.005< 0.005
WaterWater--diuresingdiuresing FluidFluid--depriveddeprived
MAPMAP(mm Hg)(mm Hg)
•• Vasopressin sensitivity is a regulated Vasopressin sensitivity is a regulated phenomenonphenomenon
•• Vasopressin Vasopressin hypersensitvityhypersensitvity is observed when is observed when vasopressin sensitivity is activated in a state of vasopressin sensitivity is activated in a state of vasopressin deficiencyvasopressin deficiency
A Speculation:A Speculation:

25
100100
9090
8080
7070
6060
5050
4040
3030
2020
1010
00--1414 --1313 --1212 --1111 --1010 --99 --88 --77 --66 --55
Agonist (Log M)Agonist (Log M)
AVPAVP
NENE
100100
9090
8080
7070
6060
5050
4040
3030
2020
1010
00--1414 --1313 --1212 --1111 --1010 --99 --88 --77 --66 --55
Agonist (Log M)Agonist (Log M)
AVPAVP
NENE
% R
educ
tion
in L
umen
Dia
met
er%
Red
uctio
n in
Lum
en D
iam
eter
% R
educ
tion
in L
umen
Dia
met
er%
Red
uctio
n in
Lum
en D
iam
eter
Efferent and Afferent Arterioles of RatEfferent and Afferent Arterioles of Rat