objectives renal physiology plasma osmolality vs effective osmolality hypoosmolar state hyponatremia...
TRANSCRIPT


Objectives Renal physiology
Plasma osmolality vs effective osmolalityHypoosmolar state
Hyponatremia (in most instances represents a hypoosmolar state BUT not always!)
More renal physiology!Regulation of antidiuretic hormone (ADH)
Hyperosmolar statesHypernatremiaIngestions

Total Body Water (TBW)~60% of lean body weight in men and ~50% in
womenDistribution
intracellular compartment (60% of TBW) extracellular compartment (40% of TBW)
Osmotic forces are the primary determinants of the distribution of water between compartments
Water flows from the compartment of low osmolality to that of high osmolality until the osmotic pressures are equalized

Osmotic ForcesEach compartment has one major solute that
is restricted within its compartment and thus acts to hold water within that spaceNa+ salts are the main extracellular osmolesK+ salts are the main intracellular osmoles
In contrast, urea rapidly crosses cell membranes and equilibrates throughout the TBW and thus does not affect the distribution of water between the intracellular and extracellular spaces.

Osmolality vs Effective OsmolalityOsmolality: total number of particles in an
aqueous solution (mosmol/kg H2O)Normal Posm = 275-290 mosmol/kg
Effective osmolality (tonicity): those particles that can exert osmotic force across membranes, via movement of water into or out of cellsExamples: Na+, glucose, mannitolNormal effective Posm = 270-285 mosmol/kg

Plasma OsmolalityNa+, glucose and BUN are major
determinants of plasma osmolalityPosm = 2 x plasma [Na+] + [Glucose]/18 +
[BUN]/2.8More important clinically to consider
effective osmolality than “total’’ osmolalityEffective osmoles (Na+ , glucose) exert water
shifts unlike urea (as well as ethanol)



Comprehensive Clinical Nephrology, 4th Edition

Take Home Messages Increase in effective ECF osmolality results in
cellular dehydrationDecrease in effective ECF osmolality results in
cellular overhydrationFlow of water in and out of brain cells is
primarily responsible for clinical CNS manifestations
Water shifts do not occur and symptoms of hyperosmolality are absent when the effective osmolality is not increased (ie in patients with uremia)

Take Home MessagesPlasma [Na+] is a function of the ratio of the
amounts of solute and water present and does not necessarily correlate with volume, which is a function of the total amount of Na+ and water present

Hypotonic HyponatremiaHypovolemic
↓ [Na+] = ↓↓TBNa/↓TBWEuvolemic
↓ [Na+] = ↔ TBNa/↑TBWHypervolemic
↓ [Na+] = ↑TBNa/↑↑TBW

Plasma Osmolality
Does hyponatremia represent low plasma osmolality in all cases?
NO

Plasma OsmolalityExample
Serum Na+ = 125 mEq/LBUN = 140 mg/dLBlood glucose = 90 mg/dLCalculated and measured osmolality = 305 mOsm/kg
Posm = 2 x 125 + 90/18 + 140/2.8In this case, hyponatremia is associated with an
elevated plasma osmolalityEffective osmolality = 255 mOsm/kg (calculation
excludes BUN) thus this patient may have symptoms of hypotonicity despite an elevated plasma osmolality

Plasma OsmolalityExample:
Serum Na+ = 133 mEq/LBUN = 11 mg/dLBlood glucose = 500 mg/dL
Effective osmolality = 294 mOsm/kg (2 x 133 + 500/18)
Hyponatremia is not always associated with hypoosmolality ; thus direct therapeutic intervention for hyponatremia may not be required (in this example, need to treat underlying hyperglycemia)
Does plasma hypoosmolality always represent hyponatremia?
YES•Most of the plasma osmoles are Na+ salts, with lesser contributions from other ions, glucose and urea•Osmotic effect of the plasma ions (Posm) can be estimated from 2 x plasma [Na+]
Do ineffective osmoles (urea, ethanol, ethylene glycol, methanol) cause hyponatremia?
NORemember these osmoles readily move between fluid compartments without causing water shifts

Do effective osmoles (glucose, mannitol) cause hyponatremia?
YesThese osmoles shift water out of the cells

Clinical Examples of HyponatremiaPlasma Na+ = 120 mEq/LBlood glucose = 90
mg/dLBUN = 14 mg/dLMeas Posm = 250
mosmol/kgHypotonic hyponatremia: identify some clinical conditions…
risk of cerebral edema

Clinical Examples of HyponatremiaPlasma Na+ = 120
mEq/LBlood glucose = 90
mg/dLBUN = 14 mg/dLMeas Posm = 290
mosmol/kgPseudohyponatremia ( lipids, protein)
No risk of cerebral edema

Clinical Examples of HyponatremiaPlasma Na+ = 120 mEq/LBlood glucose = 1350 mg/dLBUN = 14 mg/dLMeas Posm = 320 mosmol/kg
Hyponatremia caused by hyperglycemia
No risk of cerebral edema

Clinical Examples of HyponatremiaPlasma Na+ = 120 mEq/LBlood glucose = 90 mg/dLBUN = 14 mg/dLCalc Posm = 250 mosmol/kgMeas Posm = 325 mosmol/kgOsmolar gap = 75 mosmol/kgEffective osmolality =
320mosmol/kg
Dilutional hyponatremia caused by mannitol, which results in an elevated osmolar gap
No risk of cerebral edema

Clinical Examples of HyponatremiaPlasma Na+ = 120 mEq/LBlood glucose = 90 mg/dLBUN = 14 mg/dLCalc Posm = 250
mosmol/kgMeas Posm = 300
mosmol/kgOsmolar gap = 50
mosmol/kgEffective osmolality= 245
mosmol/kg
Beer Potomania
[EtOH] = 50 mmol/L
risk of cerebral edema

Clinical Examples of HyponatremiaPlasma Na+ = 120
mEq/LBlood glucose = 90
mg/dLBUN = 126 mg/dLMeas Posm = 290
mosmol/kgEffective osmolality =
245 mosmol/kg
Hyponatremia caused by renal failure risk of cerebral edema
Note: a normal measured plasma osmolality does not preclude an increased risk of cerebral edema

Laboratory Approach to HyponatremiaStart with plasma osmolality to exclude
pseudohyponatremia (normal Posm) and hypertonic hyponatremia (elevated Posm)
When hypotonicity is confirmed, then clinically evaluate the patients’ volume status

Current Medical Diagnosis & Treatment, 2009

Urine OsmolalityDetermine whether H2O excretion is normal or
impairedUosm > 100 mosmol/kg occurs in majority of
hyponatremic patients and indicates impaired H2O excretion
Uosm < 100 mosmol/kg indicates that ADH is appropriately suppressedPrimary polydipsiaLow solute intakeReset osmostat

Reset Osmostat• Normal osmotic responses to Posm but ADH
release is not suppressed until Posm falls well below normal (≠ SIADH in which there is nonsuppressible ADH release)• Plasma [Na] is subnormal but remains stable
(usually 125-130 mEq/L)• Associated with hypovolemia, psychosis,
malnutrition, quadriplegia and pregnancy• Therapy for hyponatremia is unnecessary

Urine Sodium ConcentrationUna < 20 mEq/L
Hypovolemia due to extra-renal lossesEdematous states in CHF, cirrhosis, nephrotic
syndromeDilutional effect in primary polydipsia due to
very high urine outputUna > 20 mEq/L
Hypovolemia due to renal lossesRenal failureSIADHReset osmostat

Other LabsPlasma uric acid concentration
Hypouricemia (< 4mg/dL) in SIADH Mild hypervolemia decreases proximal Na+
reabsorption, leading to increased urinary uric acid excretion
Blood urea nitrogenBUN may be < 5mg/dL in SIADH
Mild hypervolemia leads to urinary urea wasting

Hyponatremia: Case 62 year old woman noted an unpleasant, sweet
taste in her mouth. She otherwise felt well and was taking no medications. Because dysgeusia is a rare manifestation of hyponatremia, her serum sodium level was tested and was 122 mEq/L.
What labs would you order?

Hyponatremia: Case (Cont)Measured Posm 250 mOsm/kgUrine osmolality 635 mOsm/kg Urine sodium 85 mEq/L. Her thyroid function and adrenal function
were normalA chest CT showed a mass in the lower lobe
of the left lung, which proved to be a small-cell carcinoma

N Engl J Med 2007;356:2064-2072

N Engl J Med 2007;356:2064-2072

Antidiuretic HormonePrimary determinant
of free water excretionIncreases water
permeability of the luminal membranes of the cortical and medullary collecting tubules, thus promoting water reabsorption (primarily in principal cells)
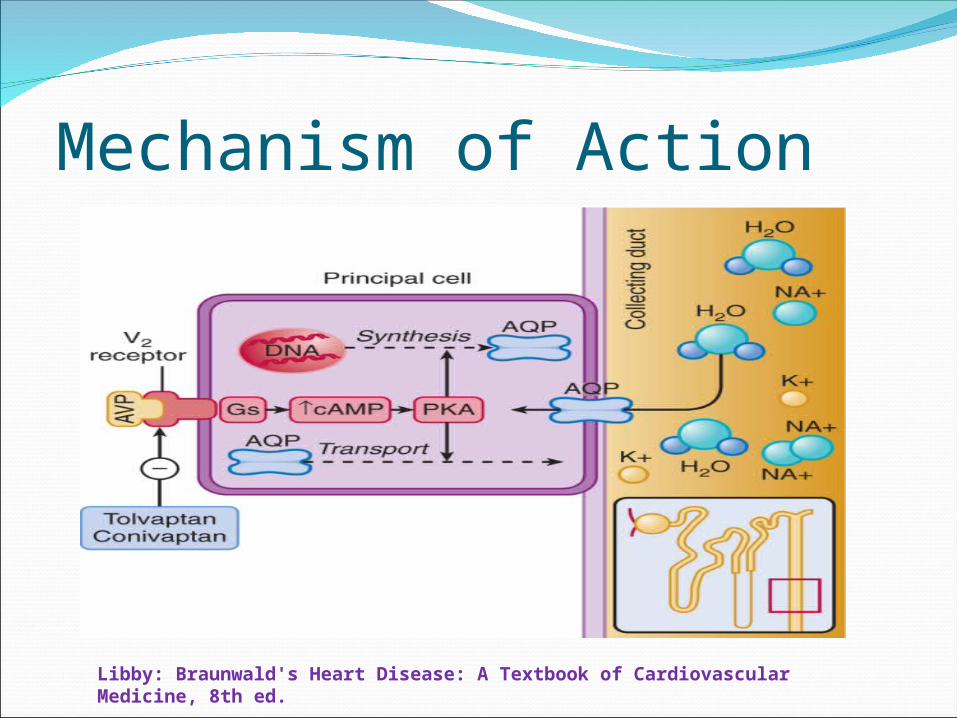
Mechanism of Action
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

Aquaporins
Brenner: Brenner and Rector's The Kidney, 8th ed.
Transmission electron micrograph illustrating immunogold labeling of aquaporin-1 in the descending thin limb (DTL) of a long-looped nephron from rat kidney. Labeling of aquaporin-1 is seen in both the apical and basolateral plasma membrane. BM, basement membrane. (Magnification, ×120,000.) (From Nielsen S, Kwon TH, Christensen BM, et al: Physiology and pathophysiology of renal aquaporins. J Am Soc Nephrol 10:647, 1999.)

Osmoreceptor ControlOsmoreceptors are specialized neurons in the
anterolateral hypothalamusThe plasma [Na+] is the primary osmotic
determinant of ADH releaseOsmoreceptors are extremely sensitive and
respond to changes in plasma osmolality of as low as 1%
Stimulation of ADH occurs when osmoreceptor cells shrink in response to increased plasma osmolality from effective osmoles (Na+, hyperglycemia, mannitol)

Osmotic threshol
d
(2-5 mOsmol/kg)

Baroreceptor ControlAfferent stimuli from carotid sinus
baroreceptors affect the activity of the vasomotor center in the medulla and subsequently ADH secretion by the cells in the paraventricular nuclei
Small changes in pressure or volume have little effect on ADH release

Reduction of > 10% blood
volume leads to exponential
increase in ADH release
Make sense teleologically!

Major stimuli to ADH secretion are hyperosmolality (via osmoreceptors) and effective circulating volume depletion (via baroreceptors)
V1 V2
+ decreased Posm
HypernatremiaDefined as serum [Na+] > 145 mEq/LRepresents hyperosmolalityResults from water loss (skin, respiratory and
GI tracts, dilute urine) or Na+ retentionDefense against hypernatremia:
ADH releaseThirst
Provides ultimate protection against hypernatremia Should never see an alert adult patient with serum
[Na+] > 150 mEq/L who has normal thirst and access to water

Comprehensive Clinical Nephrology, 4th Edition

Comprehensive Clinical Nephrology, 4th Edition

Comprehensive Clinical Nephrology, 4th Edition

Hypernatremia: Case83 y/o female s/p emergent cholecystectomy
for acute cholecystitis with sepsis, 5 days ago. You are called to see her for hypernatremia. She is very weak and ill, and complains of thirst. Her water pitcher is on the bedside table, which is pushed against the wall in her room.
PMH: HTN, HLD, OAPE: Ill appearing elderly female. T 101.2, BP
110/68, P 95, Wt 54 kg. Mucous membranes dry. + drainage bag in upper abdomen draining bile. + NG tube. Dressed surgical wound. No edema.

Hypernatremia: CaseMeds:
D5 1/2 NS at 100 ml/hourTPNAztreonam, Flagyl, Vancomycin (all in 0.9%
NS)Labs: Na 155; K 4.6; HCO3 32; Cl 110;
glucose 95; BUN 45; creatinine 0.8Drainage bag output 100 ml/day; Urine
output is 2.5 liters/day; Urine osmolality 516 mOsm/kg

Etiologies of this patient’s hypernatremia?Unable to access waterHypotonic fluid losses:
NG and biliary drainage Increased insensible losses due to fever
Averages 800-1000 ml/day in adults Estimation: 15 ml/kg/day; 15% increase for each 1 VC Fever, respiratory infections, burns increase
insensible losses? Mild renal insufficiency results in suboptimal
urinary concentration (Uosm 516 mOsm/kg)Hypertonic gains: total parenteral nutrition
(hyperosmotic), 0.9% NS used for antibiotics

What’s her free water deficit?[Na+] [TBW] desired = [Na+] [TBW] actual
[140 mEq/L] [TBW] = [155 mEq/L] [0.5 (54kg)][TBW] desired = 29.9kgFree water deficit= 29.95kg – 27kg= 2.9kgReplace ½ of deficit with free water over 24 hours
Lower serum [Na+] no more than 10 mEq/L over 24 hours
Also need to take into account daily insensible losses and free water loss via urinary and GI tracts.

Does she have an osmotic diuresis?Osmotic diuresis: increased urinary water loss
induced by the presence of large amounts of nonreabsorbed solute in the tubular lumen (resulting in hypotonic urine)
How many osmoles a day is she excreting in her urine?516 mOsm/Kg x 2.5 liter/day = 1290 mOsm/day
An average person excretes about 600-900 mOsm/day
The high urinary osmolar excretion likely accounts for the elevated urine osmolality, due to a high urea concentration from the high protein TPN
The high urine [urea] results in an osmotic diuresis

Comprehensive Clinical Nephrology, 4th Edition

Toxic Alcohol Ingestions: CaseA 38-year-old man presented to the
emergency department after reportedly ingesting antifreeze.
He appeared to be intoxicated and was agitated and combative; chemical sedation was induced.
Initial laboratory studies revealed a pH of 7.0, an anion gap of 22 mmol per liter, and an osmolar gap of 79 mOsm.
N Engl J Med 2007;356:6

N Engl J Med 2007;356:6


Comprehensive Clinical Nephrology, 4th Edition

Comprehensive Clinical Nephrology, 4th Edition

Kidney International 2008; 73: 1201–1202
(a) The urine sediment with multiple refractile, needle-shaped crystals, which in (b), using a polarizer, shows birefringence (original magnification 40).

Osmolar GapOsmolar gap = measured Posm – calculated
PosmPosm (mOsm/L) = 2 x plasma [Na+] + Glucose
(mg/dL)/18 + BUN (mg/dL)/2.8Measured Posm is usually within 10 mOsm/L of
the calculated PosmElevated osmolar gap:
Alcohol ingestions: methanol, ethanol, isopropanol, ethylene glycol, propylene glycol, diethylene glycol (OG > 20 mOsm/L)
Diabetic or alcoholic ketoacidosis, lactic acidosis, renal failure (OG < 15-20 mOsm/L)

Osmolar Gap: PitfallsThe plasma osmolal gap cannot distinguish
among various alcohol ingestionsAbsence of an osmolar gap does NOT exclude
an alcohol-related intoxicationThe plasma osmolal gap increases only in the
presence of the parent alcohols. The toxic acid metabolites of methanol and ethylene glycol do not contribute to the calculated osmolal gap. As a result, the plasma osmolar gap is insensitive in late presentations, since most of the parent alcohol has already been metabolized.
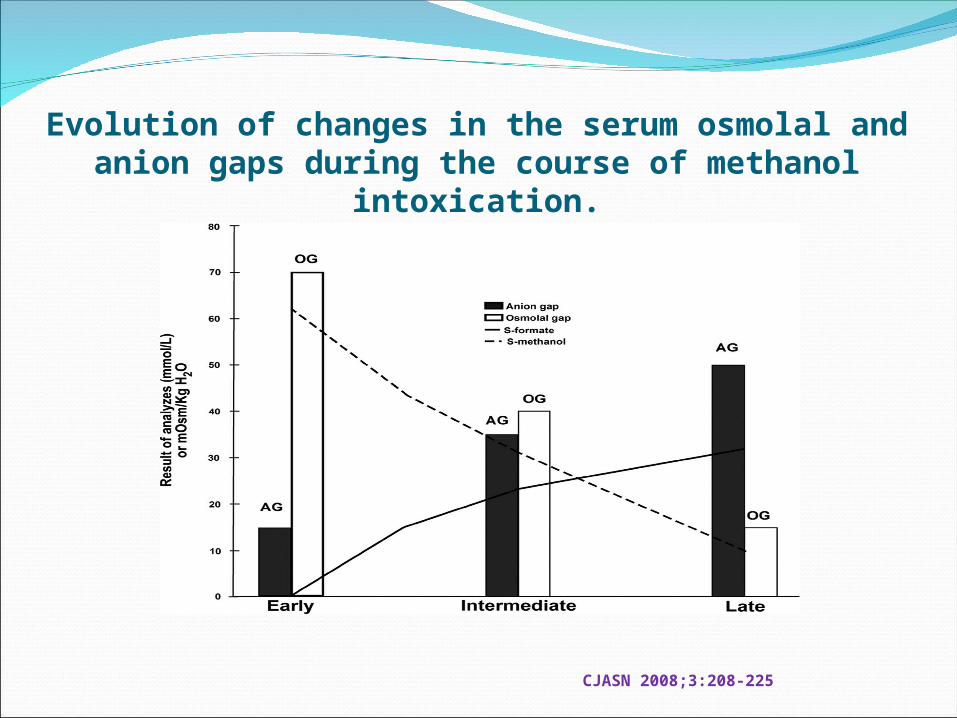
Evolution of changes in the serum osmolal and anion gaps during the course of methanol intoxication.
CJASN 2008;3:208-225

Metabolic pathways for ethanol, methanol, and ethylene glycol
CJASN 2008;3:208-225

Metabolic pathways for isopropanol, diethylene glycol, and propylene glycol
CJASN 2008;3:208-225©

DisorderSubstance(s) Causing
ToxicityClinical and Laboratory
Abnormalities CommentsAlcoholic (ethanol) ketoacidosis
β-hydroxybutyric acid, Acetoacetic acid
Metabolic acidosis May be most frequent alcohol-related disorder; mortality low relative to other alcohols; rapidly reversible with fluid administration; increase in SOsm inconsistent
Methanol intoxication(windshield wiper fluid, model airplane fuel, antifreeze)
Formic acid, Lactic acid, Ketones
Metabolic acidosis, hyperosmolality, retinal damage with blindness, putaminal damage with neurologic dysfunction
Less frequent than ethylene glycol; hyperosmolality and high anion gap acidosis can be present alone or together; mortality can be high if not treated quickly
Ethylene glycol intoxication(antifreeze, runway deicers)
Glycolic acid, Calcium oxalate
Myocardial and cerebral damage and renal failure; metabolic acidosis, hyperosmolality, hypocalcemia
More frequent than methanol intoxication; important cause of intoxications in children; hyperosmolality and high anion gap acidosis can be present alone or together
Diethylene glycol intoxication(brake fluid)
2-Hydroxyethoxyacetic acid Neurological damage, renal failure, metabolic acidosis, hyperosmolality
Very high mortality possibly related to late recognition and treatment; most commonly results from ingestion in contaminated medications or commercial products; hyperosmolality may be less frequent than with other alcohols
Propylene glycol intoxication(solvent for hydralazine, nitroglycerin, lorazepam, diazepam, phenytoin, phenobarbital, digoxin)
Lactic acid Metabolic acidosis, hyperosmolality
May be most frequent alcohol intoxication in ICU; minimal clinical abnormalities; stopping its administration is sufficient treatment in many cases
Isopropanol intoxication(rubbing alcohol)
Isopropanol Coma, hypotension, hyperosmolality
Hyperosmolality without acidosis; positive nitroprusside reaction
CJASN 2008;3:208-225

Disorder Epidemiology Diagnostic Cluesb Poor Prognostic FactorsMethanol intoxication Accidental or intentional
ingestion of adulterated alcohol or products with methanol; rare cases of inhalation of methanol
Osmolal gap with HAGAc Blood pH <7.1; LA; severe coma; severe hypotension; serum methanol >50 to 100 mg/dl
Visual difficulties with optic papillitis
Ethylene glycol intoxication
Accidental or intentional ingestion of antifreeze, alcohol adulterated with ethylene glycol, or products with ethylene glycol
Osmolal gap with HAGAc Blood pH <7.1; glycolate level >8 to 10 mmol/L; ARF requiring HD; diagnosis >10 h after ingestion; serum ethylene glycol >50 to 100 mg/dl
ARF with osmolal gapCalcium oxalate crystals in urine, monohydrate or dihydrate
Diethylene glycol intoxication
Ingestion of contaminated medication or products with diethylene glycol
Osmolal gap with HAGAc Blood pH <7.1; ARF requiring HD; severe coma; ingestion of >1.34 mg/kg body wt
Osmolal gap with ARFOsmolal gap with coma
Propylene glycol intoxication
Intravenous administration of medication with propylene glycol; rare ingestion of products with propylene glycol
Osmolal gap with or without LA
Severe LA; serum propylene glycol level >400 to 500 mg/dl
Isopropanol intoxication Accidental or intentional ingestion of rubbing alcohol
Osmolal gap without HAGA Severe LA; hypotension; serum isopropanol level ≥200 to 400 mg/dl
Alcoholic ketoacidosis Binge drinking often in alcoholic patients associated with starvation and often vomiting
HAGA, trace positive or negative nitroprusside reaction with increase with H2O2; hypoglycemia; osmolal gap
Blood pH <7.0; severe comorbid conditions
CJASN 2008;3:208-225

N Engl J Med 2009;360:2216-23





Gastric lavage, induced emesis, or use of activated charcoal to remove alcohol from gastrointestinal tract needs to be initiated within 30 to 60 min after ingestion of alcohol
Administration of ethanol or fomepizole to delay or prevent generation of toxic metabolites needs to be initiated while sufficient alcohol remains unmetabolized measurement of blood alcohol concentrations and/or serum osmolality can be helpful
Dialysisb (hemodialysis > continuous renal replacement therapy > peritoneal dialysis) helpful in removing unmetabolized alcohol and possibly toxic metabolites and delivering base to patient to ameliorate metabolic acidosis
General Principles in the Treatment of Alcohol Intoxications

Disorder Treatmentb
Methanol intoxication Initiate fomepizole (alcohol if fomepizole not available) and HD with methanol >20 mg/dl, in presence of HAGA with osmolal gap and high suspicion of ingestion. Initiate HD alone if HAGA present and methanol levels <10 mg/dl or no osmolal gap but strong suspicion of ingestion. Give folinic or folic acid. Give base with severe acidosis if patient not undergoing HD. Discontinue treatment when pH normalized and methanol levels <10 to 15 mg/dl or undetectable. If measurement of methanol not available use return of blood pH and serum osmolality to normal as goals of therapy.
Ethylene glycol intoxication Initiate fomepizole (alcohol if fomepizole not available) and HD with ethylene glycol levels >20 mg/dl or in presence of HAGA with osmolal gap and high suspicion of ingestion. Initiate HD alone if HAGA present and ethylene glycol level <10 mg/dl or no osmolal gap but strong suspicion of ingestion. Give base with severe acidosis if patient not undergoing HD. Give thiamine and pyridoxine. Discontinue treatment when pH normalized and ethylene glycol levels <10 to 15 mg/dl or undetectable. If measurement of ethylene glycol not available use return of blood pH and serum osmolality to normal as goals of therapy.
Diethylene glycol intoxication Initiate HD with osmolal gap, HAGA, and ARF or with high suspicion of ingestion because of cohort of cases ingesting contaminated medication. Administration of fomepizole not approved but recommended in addition to dialysis. Discontinuation of treatment with recovery of renal function, normalization of acid-base parameters and osmolal gap.
Propylene glycol intoxication Discontinue medication containing propylene glycol which will be effective alone in most cases. Initiate dialysis and/or fomepizole with severe LA or very high serum concentrations >400 mg/dl and evidence of severe clinical abnormalities.
Isopropanol intoxication Supportive therapy usually sufficient. Initiate HD with serum level 200 to 400 mg/dl or in presence of marked hypotension or coma.c
Alcoholic ketoacidosis Administer intravenous fluids including dextrose and NaCl; base rarely needed, might be considered with blood pH <6.9 to 7.0; consider administering insulin with marked hyperglycemia


Solids 7%
Solids 14%
HYPERLIPIDEMIA
HYPERPROTEINEMIA
Serum [Na+] = 140 mEq/L
Serum [Na+] = 130 mEq/L
Na+ 140 mEq in 930 ml
Na+ 130 mEq in 860 ml
Water 93% Water
86%
1 liter plasma
1 liter plasma
OSMOLALITY
Measures solute per unit plasma water
140 mEq/930 ml = 151 mEq/liter = 130 mEq/860 ml


Other factors affecting ADH secretionNausea
Extremely potent stimulus (as much as 500-fold rise in ADH level)
Hypoglycemia 3-fold rise in ADH level when plasma glucose decreases
by 50%Pregnancy (reset osmostat)
Lowers the osmoregulatory threshold for ADH release and thirst
Fall in plasma [Na+] by about 5mEq/LMay be mediated by ↑release of chorionic gonadotropin
which causes systemic vasodilation and fall in BPMultiple drugs (i.e. morphine, nicotine,
cyclophosphamide)