obstetric haemorrhage obstetric emergencies empangeni hospital 28th july 2000
TRANSCRIPT
Obstetric HaemorrhageObstetric Haemorrhage
Obstetric Emergencies
Empangeni Hospital
28th July 2000
Obstetric HaemorrhageObstetric Haemorrhage
Causes of ANTEPARTUM haemorrhage
• Abruptio Placentae
• Placenta praevia
• Local causes
• Unknown origin
ABRUPTIO PLACENTAEABRUPTIO PLACENTAE
Underlying pathology• Hypertensive Disease• Multiple pregnancy• Trauma• Anaemia• Polyhydramnios
PLACENTA PRAEVIAPLACENTA PRAEVIA
Predisposing factors• Previous Caesarean
Section• Most have no known
cause – presumed late implantation
Local & Unknown CausesLocal & Unknown Causes of of APHAPH
• Rupture of uterus• Carcinoma of cervix• Trauma• Cervical polyp• Bilharzia of cervix
• ? Edge bleed• ? Haemorrhoids
Obstetric HaemorrhageObstetric Haemorrhage
• Induction of labour with oxytocin is associated with an increased rate of uterine rupture in gravid women with 1 prior uterine scar, in comparison with the rate in spontaneously labouring women.
Abruptio PlacentaeAbruptio Placentae
Features• Pain and tenderness• Often I.U.F.D• “Hypotension on
hypertension”• Clotting defects• Renal impairment
Antepartum HaemorrhageAntepartum Haemorrhage
• Exclude abruption, uterine rupture, placenta praevia with labour
• Is she stable? - ?BP, pulse
• Check Abdomen - previous C/S scar, fundal height and uterine tenderness
• Check FH
• Vaginal examination and ARM
Abruptio placentaeAbruptio placentae
Abruptio PlacentaeAbruptio Placentae
• Resuscitate - FDP, whole blood
• Monitor BP and urine output
• Give oxytocin infusion or prostaglandin if necessary to induce contractions
• Avoid Caesarean Section unless salvageable baby, or no progress
• Watch out for PPH
Placenta PraeviaPlacenta Praevia
• Diagnose by Ultrasound
• Resuscitate, monitor BP and amount of bleeding
• Persistent bleeding requires delivery whatever the gestation
34 weeks - buy time for steroids
• prevent contractions with indocid
Placenta PraeviaPlacenta Praevia
• Transfer anterior placenta praevia
• Elective caesarean if 37 weeks
• Never cut through the placenta
• Lower segment may need to be packed
Post Partum HaemorrhagePost Partum Haemorrhage
Predisposing factors• Antepartum haemorrhage• Multiple pregnancy• Prolonged labour• Caesarean Section
Post Partum HaemorrhagePost Partum Haemorrhage
Causes* Uterine atony* Obstetric trauma
Post Partum HaemorrhagePost Partum Haemorrhage
Atonic uterus (soft uterus)* Compression - bimanual
is best* Oxytocin - 10 units IV* Syntometrine 1 amp IM* PgF2α 5mg in 500 ml IV* Misoprostol (PgE1) 1mg
(5 tabs) rectally
Trauma (hard uterus)* Vaginal tears are most
common* Cervical tears rare
unless instrumental* Remember the ruptured
uterus* Uterine inversion
Post Partum HaemorrhagePost Partum Haemorrhage
Other causes• Instrumental Delivery• After Caesarean Section• Infection - 2° PPH• Retained placental
fragments
Post Post PPartum Haemorrhageartum Haemorrhage
• Rub up a contraction• Get help• Insert two large bore IV lines - Haes-Steril• Give an oxytocic• Explore digitally for fragments and tears• Explore with speculum for tears - especially
cervix• Evacuate under GA
Rupture of UterusRupture of Uterus
Two types• True rupture• Dehiscence of scar
Rupture of UterusRupture of Uterus
True Rupture• Contractions stop• Continuous pain• Tender abdomen• Fundus ill-defined• PV Bleeding• Fetal heart dips or absent
fetal heart
Scar Dehiscence• Dehiscence may be
silent – no bleeding• Fetal distress• Haematuria• Vague uterine outline• Failed induction
Rupture of UterusRupture of Uterus
• High Index of suspicion in grande multips and in scarred uteri
• All cases of Ante and Intra partum haemorrhage must exclude rupture
• Laparotomy if suspected
• Repair or Hysterectomy?
Surgical ManagementSurgical Management
• Direct suture• Stepwise devascularisation• Internal iliac artery ligation • Hysterectomy• B-Lynch, “foley
tourniquet”, packing
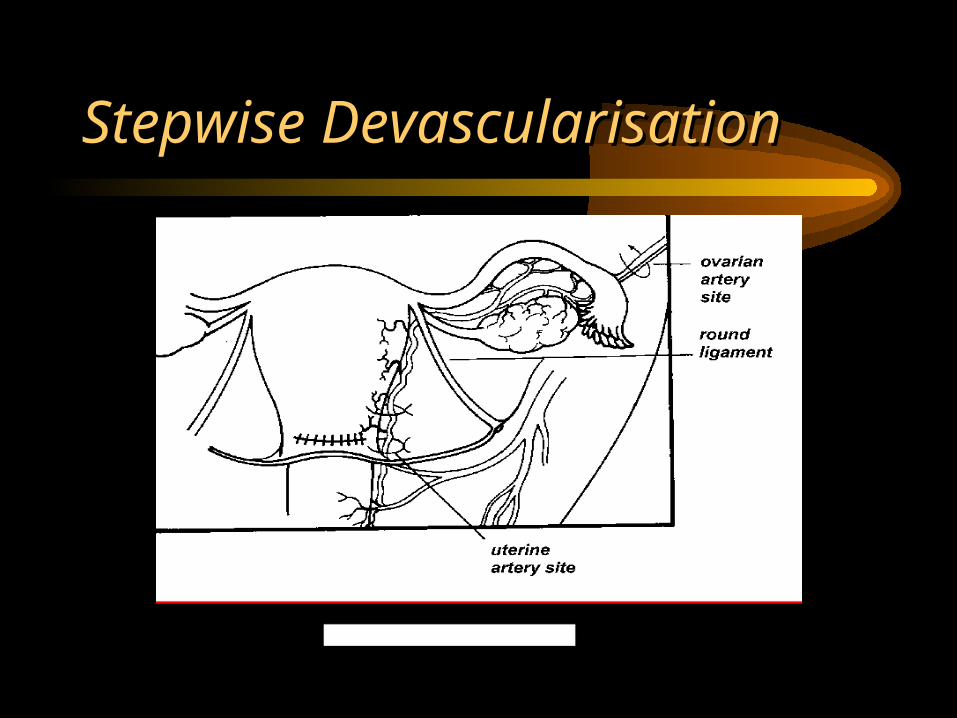
Stepwise DevascularisationStepwise Devascularisation