obstructive sleep apnea
TRANSCRIPT
INTRODUCTIONDESTINE TAWIAH
TAISHAN MEDICAL UNIVERSITYSECTION A
4TH YEAR
TOPIC: OBSTRUCTIVE SLEEP APNEA PRESENTATION DATE: 2014TIME:
• CONTENT: Sleep apnea and Obstructive sleep apnea
• Causes , syptoms,diagnosis and treatment of obstructive sleep apnea
• CPAP Device,principle and usage,• Obstrutive sleep apnea in children(syptoms)• Snoring and obstructive sleep apnea
Sleep apnea
• What Is Sleep Apnea?Apnea literally means "cessation of breath." If
you have sleep apnea, your breath can become very shallow or you may even stop breathing while you are asleep. This state of not breathing can occur up to hundreds of times a night in some oxygen to vital organs and cause irregular heart rhythms.
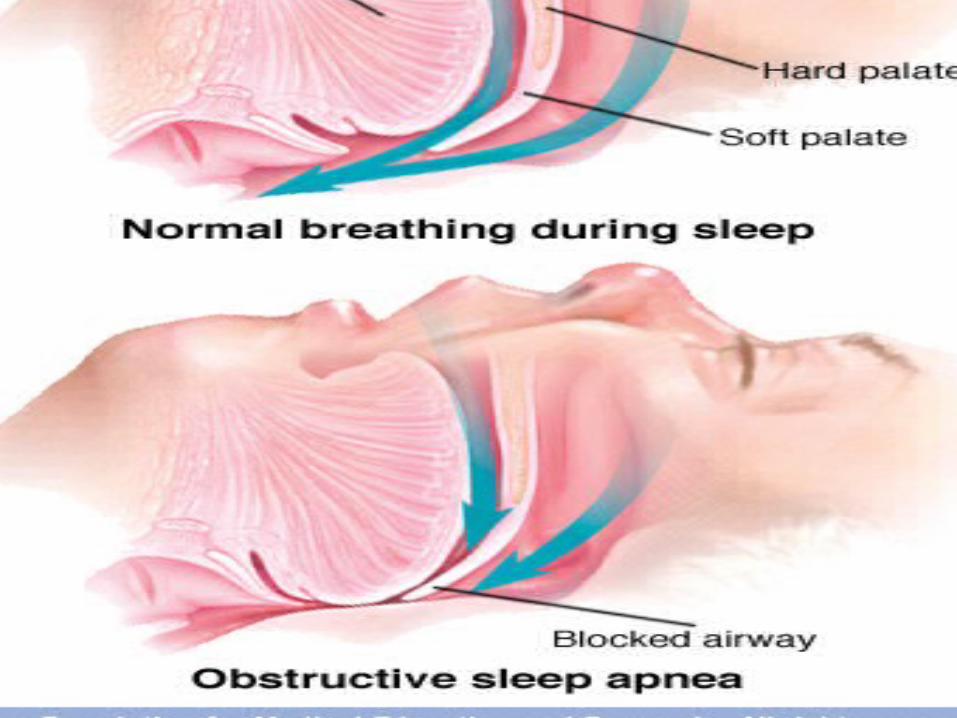
• What Is Obstructive Sleep Apnea?
• Obstructive sleep apnea (OSA) -- also called obstructive sleep apnea syndrome -- occurs when there are repeated episodes of complete or partial blockage of the upper airway during sleep. During an obstructive sleep apnea episode, the diaphragm and chest muscles work harder to open the obstructed airway and pull air into the lungs. Breathing usually resumes with a loud gasp, snort, or body jerk. These episodes can interfere with sound sleep.
Risk Factors • Nonstructural risk factors for OSA include the following:• Obesity• Central fat distribution• Male sex• Age• Postmenopausal state• Alcohol use• Sedative use• Smoking• Habitual snoring with daytime somnolence• Supine sleep position• Rapid eye movement (REM) sleep
• Other conditions associated with the development of OSA are as follows:• Hypothyroidism• Neurologic syndromes• Stroke
• Structural factors• Structural factors related to craniofacial bony anatomy that predispose patients
with OSA to pharyngeal collapse during sleep include the following: • Innate anatomic variations (facial elongation, posterior facial compression)• Retrognathia and micrognathia• Mandibular hypoplasia• Brachycephalic head form - ]
• Inferior displacement of the hyoid• Adenotonsillar hypertrophy,( particularly in children and young adults)• Pierre Robin syndrome• Down syndrome• Marfan syndrome• Prader-Willi syndrome• High, arched palate (particularly in women)
• signs and symptoms• Daytime symptoms may include the following:• Nonrestorative sleep (ie, “waking up as tired as when they went to bed”)• Morning headache, dry or sore throat• Excessive daytime sleepiness that usually begins during quiet activities (eg,
reading, watching television); as the severity worsens, patients begin to feel sleepy during activities that generally require alertness (eg, school, work, driving)
• Daytime fatigue/tiredness• Cognitive deficits; memory and intellectual impairment (short-term memory,
concentration)• Decreased vigilance• Morning confusion• Personality and mood changes, including depression and anxiety• Sexual dysfunction, including impotence • Gastroesophageal reflux
• Nocturnal symptoms may include the following:• Snoring, usually loud, habitual, and bothersome to others• Witnessed apneas, which often interrupt the snoring and end
with a snort• Gasping and choking sensations that arouse the patient from
sleep, though in a very low proportion relative to the number of apneas they experience
• Nocturia• Insomnia; restless sleep, with patients often experiencing
frequent arousals and tossing or turning during the night
I
Diagnosis• IT INCLUDES THE FOLLWOWING:• Sleep stages are recorded via an electroencephalogram,
electro-oculogram, and chin electromyogram.
• Heart rhythm is monitored with a single-lead electrocardiogram
• Leg movements are recorded via an anterior tibialis electromyogram
• Breathing is monitored, including airflow at the nose and mouth (using both a thermal sensor and a nasal pressure transducer), effort (using inductance plethysmography), and oxygen
• saturation
• The breathing pattern is analyzed for the presence of apneas and hypopneas .
obtain a thyrotropin test on any patient with possible OSA who has other signs or symptoms of hypothyroidism, particularly in elderly individuals.
• Routine laboratory tests, however, are usually not helpful in OSA unless a specific indication is present. Pulmonary function tests are not indicated to make a diagnosis of, or treatment plan for, OSA alone. The standard indications for such testing apply to all patients, with or without OSA.
• Management• Treatment of OSA partly depends on the patients’ severity of sleep-
disordered breathing. Those with mild apnea have more options, whereas people with moderate to severe apnea should be treated with nasal continuous positive airway pressure (CPAP).
• Conservative therapy and prevention• The following conservative measures may help manage or prevent OSA:• Restriction of body positions during sleep (avoid supine position)• Sleeping in an upright position for markedly obese patients• Avoiding smoking; smoking cessation• Avoiding alcohol and other sedatives (particularly 4-6 hours before
bedtime)
• Avoiding sleep deprivation• Mechanical measures• Mechanical measures used in the treatment of
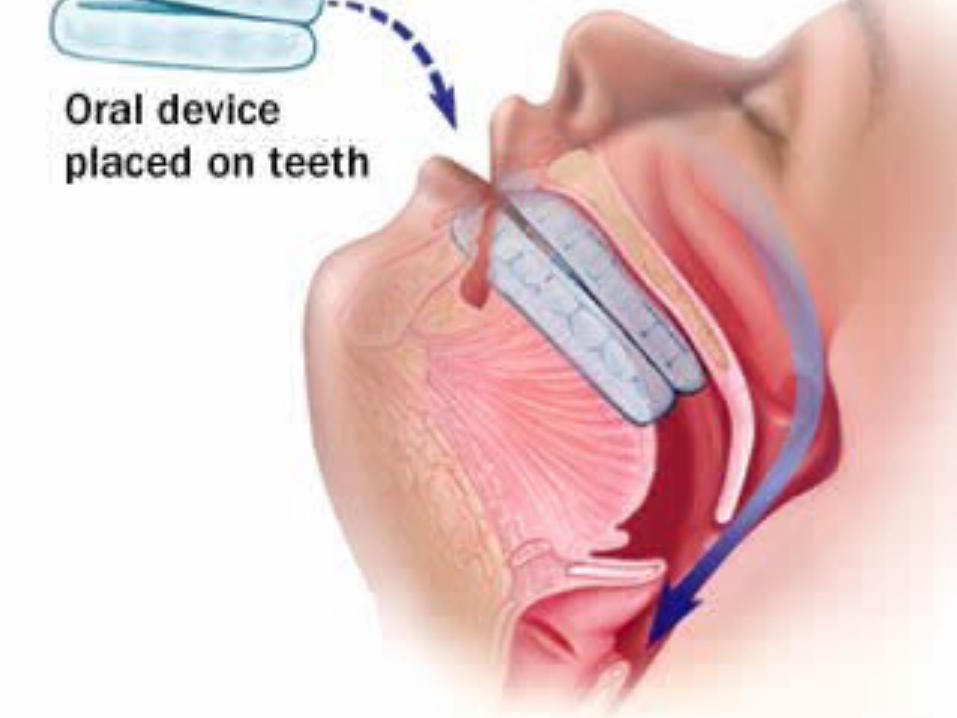
OSA include the following:• Nasal CPAP: Standard treatment option• Bilevel positive airway pressure• Oral appliance therapy
• Pharmacotherapy• Medications are generally not a part of the
primary treatment recommendations for OSA. However, central nervous system stimulants such as modafinil and armodafinil have been used adjunctively in the management of this condition.
• Surgery• Surgical intervention for OSA includes, but is
not limited to, the following:• Uvulopalatopharyngoplasty• Craniofacial reconstruction • tracheoscopy
• Continuous Positive airway pressure(CPAP)
To eliminate snoring and prevent sleep apnea, a device called a continuous positive airway pressure (CPAP) machine. A CPAP machine delivers just enough air pressure to a mask to keep your upper airway passages open, preventing snoring and apnea.


• . Although snoring can be a sign of sleep apnea, there's a big difference between the two. People with sleep apnea actually stop breathing up to 400 times throughout the night. These interruptions last 10 to 30 seconds and are often followed by a snort when breathing resumes. This breaks your sleep cycle and can leave you tired during


• Polysomnography has developed from our understanding of sleep and its associated physiologic processes. .The two critical components of polysomnography are the determination of sleep-wake stage and identification of related bodily processes.
POLYSOMNOGRAPHY requires three reliable types of measurement to determine sleep stages:
• necessary types of • measurement to reliably • determine sleep stages
• EMG• – Three electrodes are placed beneath • the chin overlying the mentalis and submentalis• muscles. This is done for the sake of • convenience and since these muscles are • particularly sensitive to changes in muscle tone
• EEG• the low(Electroencephalogram) measures continuous • variance in voltage (from the 5 – 200 microvolts range) • and is in er portion of the EEG spectrum (0.5 to 14 • Hz). • •• EOG• (Electro-oculogram) to detect the slow-rolling eye • movements (SEM) associated with sleep onset and the • cardinal rapid eye movements in REM sleep
• •EEG• -• reliable recording of the EEG begins with • accurate measurement of the skull according to the • international “10-20 system”. For sleep recordings, • electrodes are usually attached on the scalp over the • central region of the cortex between the motor and • sensory cortex (at locations C3 or C4) and the occipital
• EOG• - Electrodes placed at left and right outer • canthus with one below and one beneath the • horizontal plane. EOG recording are based on • the electro-potential difference between the • cornea (positively charged) and the retina • (negatively charged). This strategy allow for eye • movements in any direction to be seen as out-of-