obstructive sleep apnea alternative modes of treatment
TRANSCRIPT
Obstructive Sleep Apnea
Alternative Modes of Treatment
• CONFLICT OF INTEREST• No Financial disclosure
OBJECTIVES
• Learn about alternative treatments for OSA• Learn pro and cons of these devices• Learn role of these devices in patient
management
Obstructive Sleep Apnea
CONVENTIONAL TREATMENTS• Positive Airway Pressure – CPAP, BPAP• Oral Appliance Therapy – like TAP III• Upper airway surgery – nasal turbinate
reduction / septoplasty / UPPP / tongue base reduction
PAP Therapy
• Mask issues• Dryness of throat / nose• Aerophagia• Intolerance to mask / pressure
Oral Appliance Therapy
• ? Effectiveness• Tolerance issues• Jaw pain• Change in bite
Upper Airway Surgery / Nasal Surgery
• ? Effectiveness• Anesthesia risks• Post operative pain• Post Nasal regurgitation (with UPPP)• Recurrent OSA symptoms after few years
Alternative Therapies for OSA
• EPAP nasal resistive device • Oral Pressure Therapy• Hypoglossal Nerve Stimulation• Maxillo-Mandibular Advancement
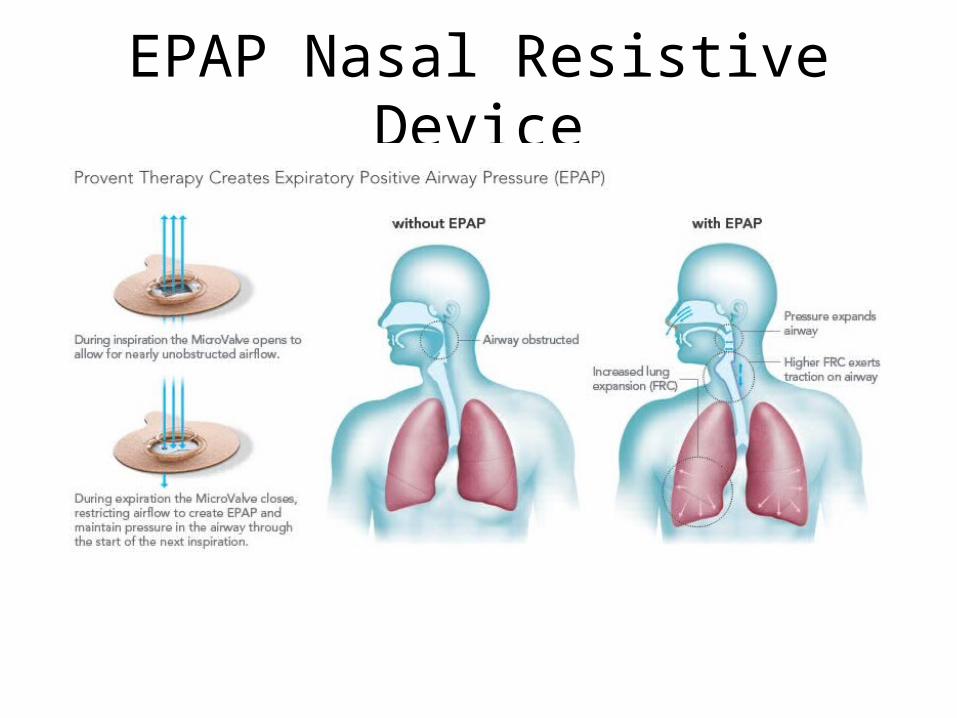
EPAP Nasal Resistive Device

Nasal Resistive Devicehttp://www.proventtherapy.com/how-to-use-provent.php
EPAP Nasal Resistive Device: Provent
• Uses a device to promote positive intranasal pressure at end expiration and this maintains airway patency (expiratory resistance of 80 cm H2O/s/L at flow rate of 100 mL/s)
• Prototype - 24 patients with OSA and 6 primary snorers, AHI reduced 24.8 + 22.1 to 14.2+22.1 and % of TST in snoring reduced (Colrain et al JCSM 2008)(similar results - Rosenthal et al JCSM 2009)
• Several studies with Provent – good results, long term adherence, • Predictors of success
– Mallampati score of <4– Lower baseline AHI– Lower baseline % of TST spent in O2 sat <90%
Provent Therapy
NEGATIVE FEATURES• Difficult to tailor as have fixed airway resistances• Can certainly use device with variable adjustable
resistance in sleep lab (similar to CPAP titration) to determine optimal resistance and then prescribing EPAP nasal device with matching resistance
• Pads come off spontaneously during the night• FDA approved but most insurance don’t cover the
cost
Hypoglossal Nerve Stimulation
• At onset of sleep apnea, there is reduction in drive to upper airway muscles (upper airway patency is strongly correlated with activation of genioglossus muscle)
• FDA Approved – released May 1, 2014
Hypoglossal Nerve Stimulation: Inspire STAR Trial
• Multicenter trial• 126 patients with OSA (with difficulty accepting or adhering to
PAP treatment)• Baseline PSG (AHI 20-50); endoscopy during drug induced sleep
(excluded if pronounced anatomic abnormalities or complete concentric collapse of retropalatal airway noted)
• Surgical procedure to implant system – stimulation electrode on hypoglossal nerve to recruit tongue protrusion function and sensing lead to detect ventilatory effort
• 2nd baseline PSG one month after implantation and then device was activated
• Follow up at 2,6 and 12 months – clinical and PSG
• At 12 months, AHI decreased by 68% (Median AHI 29.3 to 9.2)
• Oxygen Desaturation Index decreased by 70% (Median ODI score 25.4 to 7.4)
• Scores on FOSQ and ESS improved• At end of 12 months, half group stopped stimulator, and
within 1 week their AHI increased• ADVERSE EFFECTS– 2 patients required device repositioning and fixation of
stimulator– 18% reported temporary tongue weakness
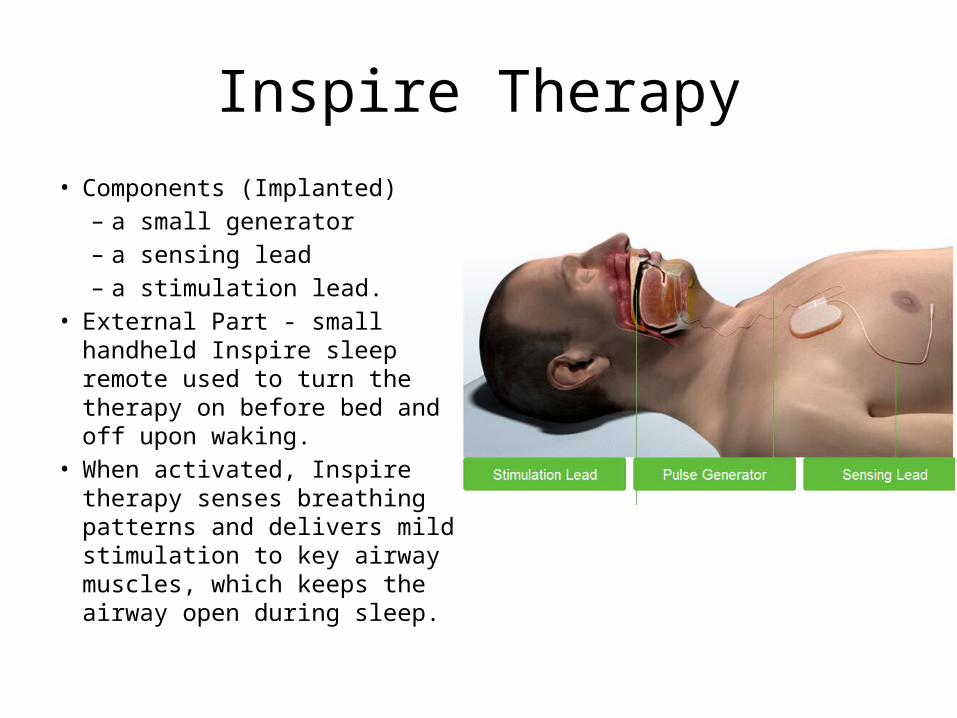
Inspire Therapy• Components (Implanted)
– a small generator– a sensing lead – a stimulation lead.
• External Part - small handheld Inspire sleep remote used to turn the therapy on before bed and off upon waking.
• When activated, Inspire therapy senses breathing patterns and delivers mild stimulation to key airway muscles, which keeps the airway open during sleep.
Hypoglossal Nerve Stimulation
• http://www.inspiresleep.com/inspire-system.php
Oral Pressure Therapy
• http://apnicure.com/about/
• Rationale– Negative pressure applied on soft palate pulls soft palate anteriorly,
and stabilizes tongue to reduce obstruction during sleep
• Study published – 6 centers, 63 subjects- baseline PSG and repeat PSG on 1 night and 28 nights of OPT
Median AHI improved from 27.5 to 14.8ESS improved from 13 to 7Median usage per night 6 hours
Oral Pressure Therapy
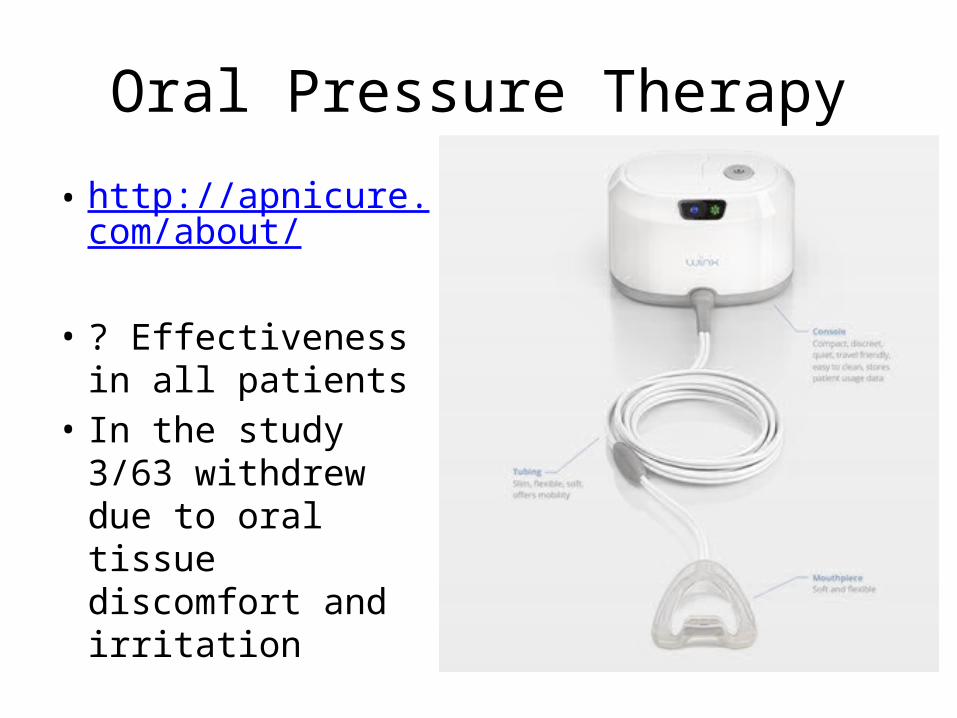
• http://apnicure.com/about/
• ? Effectiveness in all patients
• In the study 3/63 withdrew due to oral tissue discomfort and irritation
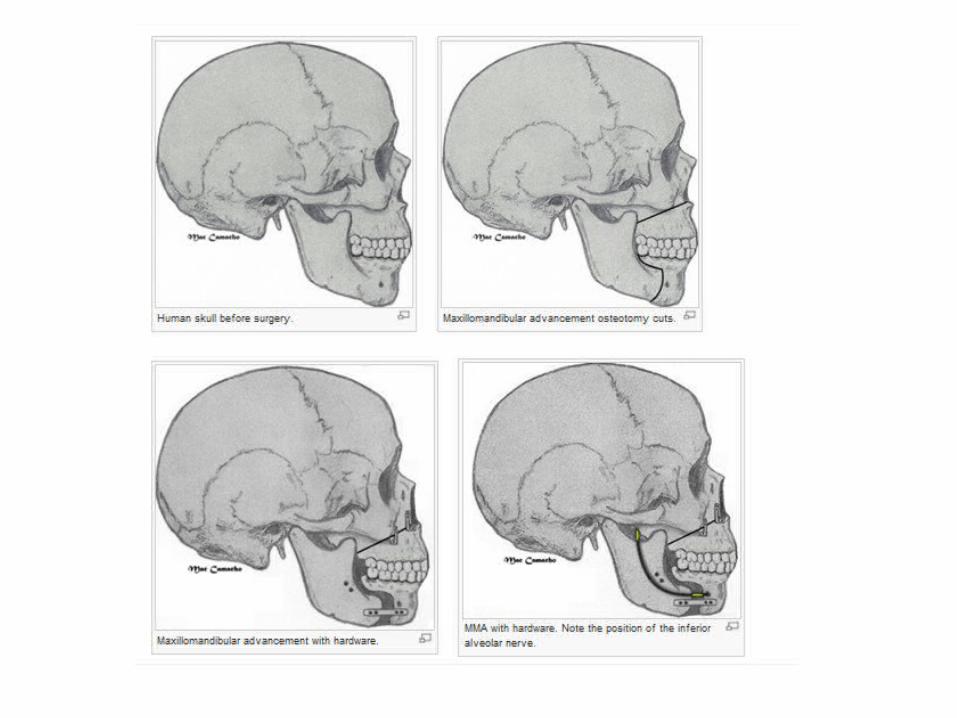
Maxillo-Mandibular Advancement
• Creating osteotomy in maxilla and mandible to advance both of them together (+ genioglossus advancement)
• No change in shape of face• LONG process
A Patient’s story
Currently 46 years old MaleKnown OSA since 1989 (age 22)Had UPPP, tonsillectomy, nasal septoplasty prior to 2000,In 2000, PSG - AHI 116/hourOn PAP – not tolerating, not benefitingUnderwent radiofrequency genioplastyUsing BPAP 21/17 – not tolerating well; tracheostomy recommended by ENT
• 1st visit – 3/2012 – BMI – 37• S/N sleep study 3/2012 – – AHI 115– Recommended BPAP 25/19; full face mask,– Poor tolerance, not sleeping well, tired, sleepy
• 5/2012 – tried auto titrating BPAP (average use – 3h, AHI 19, 95th percentile pressure 24/20)
• Discussions regarding possible tracheostomy (he doesn’t like the idea) of maxillomandibular advancement
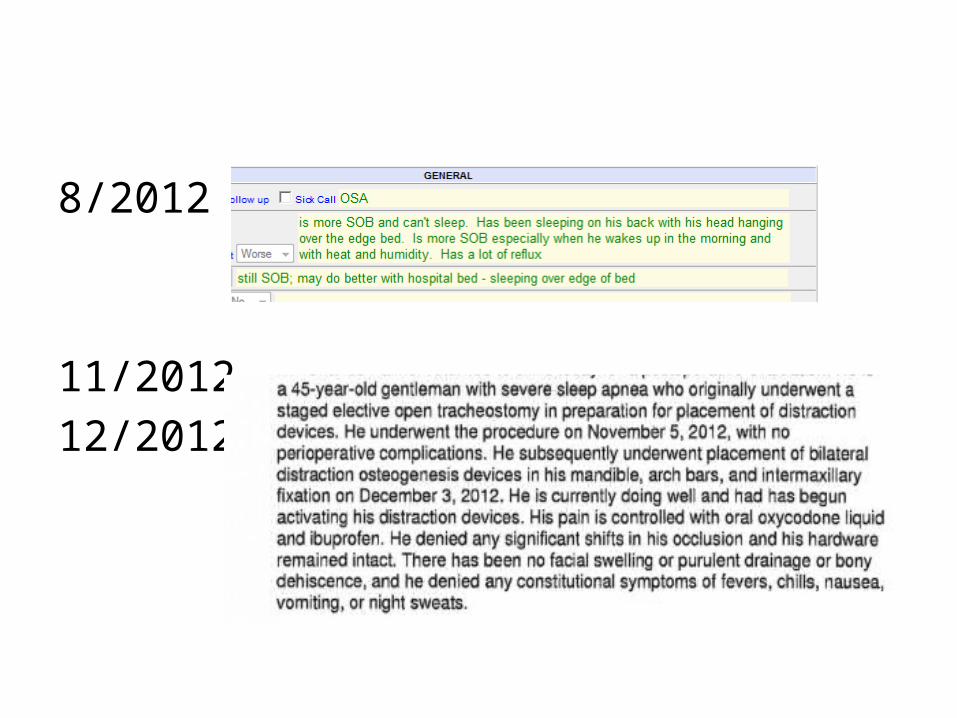
8/2012 –
11/2012 – 12/2012
• 2/2013 – BMI – 33; sleeping better; keeping trach capped
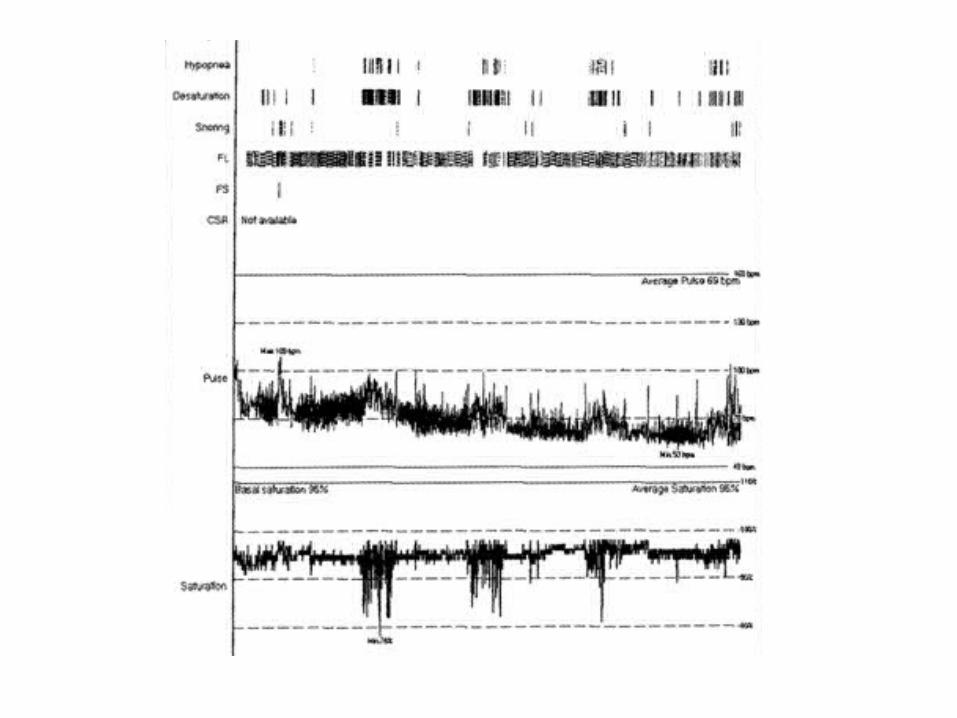
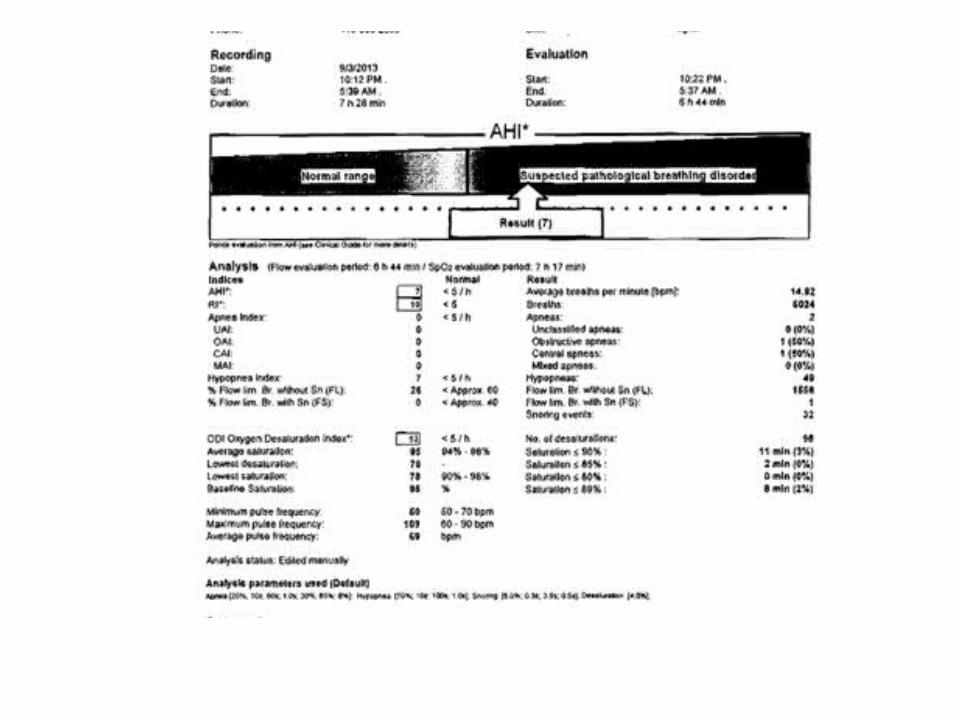
• 5/2013 – jaw wires removed• 9/2013 – BMI 30.6• 9/2013 – Apnea Link Plus (not using PAP
device)
In Conclusion
• Newer options for patients with OSA• Don’t give up and keep trying