occipital infarction with hemianopsia from carotid...
TRANSCRIPT

409
Occipital Infarction With HemianopsiaFrom Carotid Occlusive Disease
Michael S. Pessin, MD, Eddie S. Kwan, MD, R. Michael Scott, MD,
and Thomas R. Hedges III, MD
Extracranial internal carotid artery occlusive disease usually produces stroke in the middlecerebral artery territory or the border zone between the middle and anterior cerebral arteries.It is unusual for occipital infarction In the posterior cerebral artery territory to be caused byinternal carotid artery disease despite the fact that the posterior cerebral artery may arisedirectly from the internal carotid artery as an anatomic variation. We describe a patient witha fetal posterior cerebral artery originating from the internal carotid artery, and the initialmanifestation of his extracranial internal carotid artery occlusive disease was hemianopsia fromoccipital infarction. (Stroke 1989^0:409-411)
The usual clinical manifestations of extracra-nial internal carotid artery (ICA) athero-occlusive disease are well known.'-4 Tran-
sient ischemic attacks (TIAs) of the monocular orhemispheral type are common. When it occurs,stroke usually involves the middle cerebral artery(MCA) territory or the watershed region betweenthe MCA and the anterior cerebral artery andproduces contralateral sensorimotor abnormalitiesand dysphasia or behavioral abnormalities, depend-ing on the hemisphere affected. Rarely, ischemiadue to ICA occlusive disease includes infarction inthe posterior cerebral artery (PCA) territory whenthe PCA arises primarily from the ICA. This reportis prompted by our recent experience with a patientwhose initial sign of ICA occlusive disease washemianopsia from an occipital infarct related to afetal origin of the PCA from the ICA.
Case ReportA 70-year-old man was driving his automobile
when he suddenly lost vision throughout the left halfof space in both eyes. He described his visual loss tothe left as a "blank or nothing," and it persistedunchanged from the onset. An ophthalmologist doc-umented a complete left homonymous hemianopsiausing automated testing (Humphrey Instruments,San Leandro, California) and saw a cholesterol plaquein a right retinal arterial branch at the disk margin.
From the Departments of Neurology (M.S.P.), Radiology(E.S.K.), Neurosurgery (R.M.S.), and Ophthalmology (T.R.H.),Tufts-New England Medical Center, Boston, Massachusetts.
Address for reprints: Michael S. Pessin, MD, Department ofNeurology, Tufts-New England Medical Center, 750 Washing-ton Street, Boston, MA 02111.
Received August 2, 1988; accepted September 7, 1988.
On examination 13 days after the onset, a rightcarotid bifurcation bruit was present, the right retinalcholesterol plaque remained, and the patient's lefthomonymous hemianopsia was noted. Otherwise,the examination was normal.
The patient gave no history of transient monocularblindness, transient hemispheral attacks, or otherneurologic events. The patient had a history of poly-myalgia rheumatica and peripheral vascular disease.He had smoked two packs of cigarettes a day formany years.
The results of routine blood studies were normal.An echocardiogram showed normal left ventricularsize and no areas of dyskinesia or thrombus. He had2+ aortic and mitral regurgitation and slight leftatrial enlargement. Twenty-four-hour cardiac mon-itoring showed no significant arrhythmias.
A computed tomogram (CT scan) showed a rightoccipital infarct (Figure 1) in the PCA territory anda right frontal infarct. Cerebral angiography revealeda subtotal occlusion of the right ICA, with minimalantegrade blood flow and patent cervical and intra-cranial ICA on later films (Figure 2). A directcommunication was present between the right ICAand the vertebrobasilar circulation via a fetal rightposterior communicating artery (Figure 3). Theright PCA was patent, with no missing branches.
The patient had a right carotid endarterectomy toremove a potential embolic source. The endarterec-tomy was performed uneventfully, and the patientwas discharged home after 3 days. On the afternoonof his discharge, however, he complained of occip-ital headache and nausea and developed left-sidedweakness and falling to his left. En route to thehospital by ambulance, he became unresponsive.Admission examination showed a comatose patient
by guest on July 18, 2018http://stroke.ahajournals.org/
Dow
nloaded from

410 Stroke Vol 20, No 3, March 1989
FIGURE 1. Axial noncontrast computed tomogram dem-onstrates large right occipital infarct (arrow).
with 3-mm nonreactive pupils and flexion of allextremities to pain stimulation. CT scan showed alarge parenchymatous hemorrhage in the right basalganglia, with extension into the ventricular system.The patient remained comatose and died 2 daysafter admission. Autopsy was not performed.
DiscussionUsually, PCA occlusion producing occipital in-
farction results from either cardiac source or localembolism from vertebrobasilar atheroma.5-7 A fewautopsy studies38 have described PCA territoryinfarction resulting from ICA occlusion, but noclinical features were discussed. In their text onextracranial cerebrovascular disease, Wylie andEhrenfeld9 mentioned the occurrence of hemianop-sia resulting from occipital infarction when the PCAanomalously arises from the ICA; however, theauthors provide no supporting data. Although it iswell known that one or both PCAs may ariseprimarily from the ICA rather than from the basilarartery, surprisingly, we were unable to find anydescriptions of the clinical consequences of thisanatomic variation.
Our patient illustrates the anatomic relationbetween the ICA and the PCA and highlights theinitial clinical presentation of hemianopsia from anoccipital infarct in the PCA territory likely causedby local embolism from a subtotal ICA occlusion.Our patient's right PCA also filled from the basilarartery, making embolism from the posterior circu-lation a possibility. However, the absence of verte-brobasilar atheromatous disease on angiography ora cardioembolic source plus the compelling clinical
?
. t
FIGURE 2. Left: Lateral view,early arterial phase of rightcommon carotid angiogramshows high-grade stenosis ofproximal right internal carotidartery (ICA) (arrow). Right:Lateral view, late arterialphase of right common carotidangiogram shows slow ante-grade filling of distal cervical(arrows), petrous, and cavern-ous ICA.
by guest on July 18, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Pessin et al Occipital Infarction 411
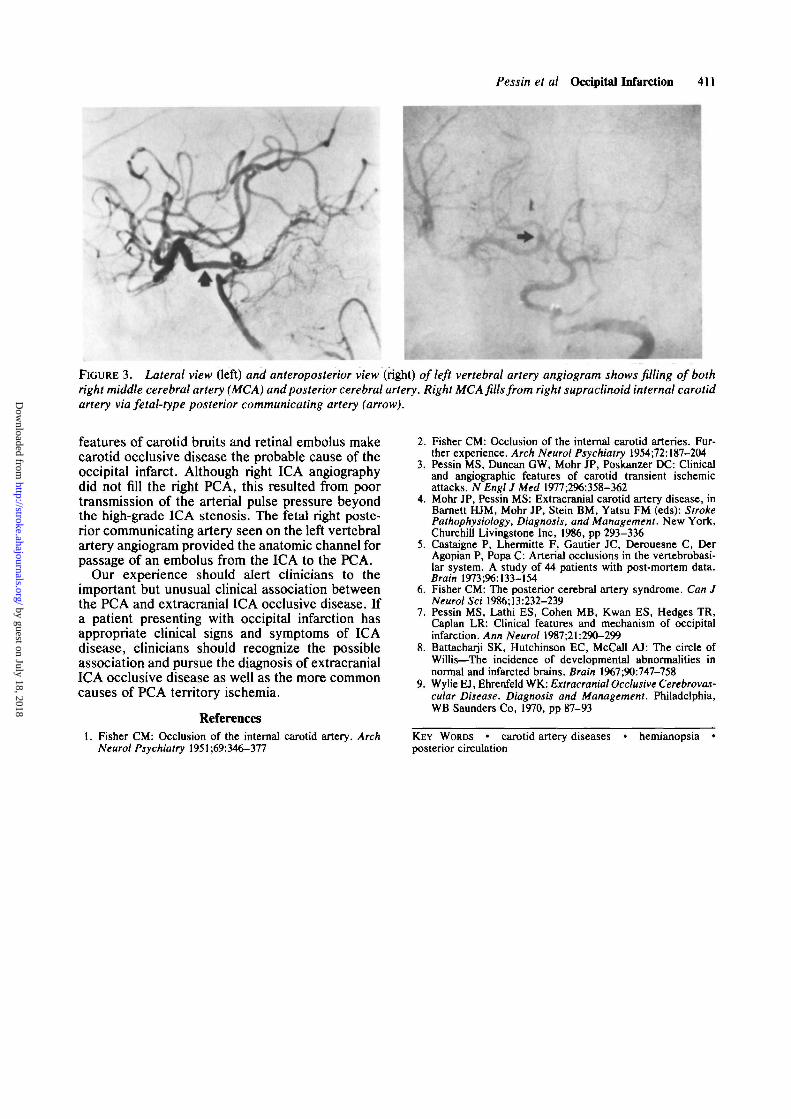
FIGURE 3. Lateral view Oeft) and anteroposterior view (right) of left vertebral artery angiogram shows filling of bothright middle cerebral artery (MCA) and posterior cerebral artery. Right MCA fills from right supraclinoid internal carotidartery via fetal-type posterior communicating artery (arrow).
features of carotid bruits and retinal embolus makecarotid occlusive disease the probable cause of theoccipital infarct. Although right ICA angiographydid not fill the right PCA, this resulted from poortransmission of the arterial pulse pressure beyondthe high-grade ICA stenosis. The fetal right poste-rior communicating artery seen on the left vertebralartery angiogram provided the anatomic channel forpassage of an embolus from the ICA to the PCA.
Our experience should alert clinicians to theimportant but unusual clinical association betweenthe PCA and extracranial ICA occlusive disease. Ifa patient presenting with occipital infarction hasappropriate clinical signs and symptoms of ICAdisease, clinicians should recognize the possibleassociation and pursue the diagnosis of extracranialICA occlusive disease as well as the more commoncauses of PCA territory ischemia.
References1. Fisher CM: Occlusion of the internal carotid artery. Arch
Neurol Psychiatry 1951 ;69:346-377
2. Fisher CM: Occlusion of the internal carotid arteries. Fur-ther experience. Arch Neurol Psychiatry 1954;72:187-204
3. Pessin MS, Duncan GW, Mohr JP, Poskanzer DC: Clinicaland angiographic features of carotid transient ischemicattacks. N Engl J Med 1977^96:358-362
4. Mohr JP, Pessin MS: Extracranial carotid artery disease, inBarnett HJM, Mohr JP, Stein BM, Yatsu FM (eds): StrokePathophysiology, Diagnosis, and Management. New York,Churchill Livingstone Inc, 1986, pp 293-336
5. Castaigne P, Lhermitte F, Gautier JC, Derouesne C, DerAgopian P, Popa C: Arterial occlusions in the vertebrobasi-lar system. A study of 44 patients with post-mortem data.Brain 1973;96:133-154
6. Fisher CM: The posterior cerebral artery syndrome. Can JNeurol Sci 1986;13:232-239
7. Pessin MS, Lathi ES, Cohen MB, Kwan ES, Hedges TR,Caplan LR: Clinical features and mechanism of occipitalinfarction. Ann Neurol 1987;21:290-299
8. Battacharji SK, Hutchinson EC, McCall AJ: The circle ofWillis—The incidence of developmental abnormalities innormal and infarcted brains. Brain 1967;90:747-758
9. Wylie EJ, Ehrenfeld WK: Extracranial Occlusive Cerebrovas-cular Disease. Diagnosis and Management. Philadelphia,WB Saunders Co, 1970, pp 87-93
KEY WORDS • carotid artery diseases • hemianopsia •posterior circulation
by guest on July 18, 2018http://stroke.ahajournals.org/
Dow
nloaded from

M S Pessin, E S Kwan, R M Scott and T R Hedges, 3rdOccipital infarction with hemianopsia from carotid occlusive disease.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.20.3.409
1989;20:409-411Stroke.
http://stroke.ahajournals.org/content/20/3/409World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 18, 2018http://stroke.ahajournals.org/
Dow
nloaded from