odontogenic myxoma involving the maxilla: case report of a ... · show a locally aggressive...
TRANSCRIPT
IJSS Case Reports & Reviews | April 2015 | Vol 1 | Issue 11 1
Odontogenic Myxoma Involving the Maxilla: Case Report of a Rare Entity
Archana Shivamurthy1, Geetha Vasudevan2, Padmapriya Jaiprakash3, Dipak Ranjan Nayak4, Ajay M Bhandarkar5
1Assistant Professor, Department of Pathology, Melaka Manipal Medical College, Manipal University, Manipal, Karnataka, India, 2Additional Professor, Department of Pathology, Kasturba Medical College Manipal, Manipal University, Manipal, Karnataka, India, 3Associate Professor, Department of Pathology, Kasturba Medical College, Manipal University, Manipal, Karnataka, India, 4Professor and Head, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India, 5Assistant Professor, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India
Odontogenic myxomas (OMs) are rare, benign, slow-growing tumors that may arise in the maxilla. They are known to have a female predilection and present as a painless mass commonly in the second or third decade of life, comprising 3-6% of all odontogenic tumors. They show a locally aggressive behavior, are radioresistant tumor and hence the need for early recognition and surgical resection. A high rate of recurrence has also been noted owing to its infiltrative pattern of growth and lack of capsule. Clinical and radiological aspects of maxillary OMs are not conclusive hence it is necessary to have a histopathological exam for the final diagnosis. We present a case of OM involving the maxilla in a 51-year-old female patient. The various histopathological differentials are also discussed.
Keywords: Maxilla, Myxoma, Odontogenic, Painless
CASE REPORT
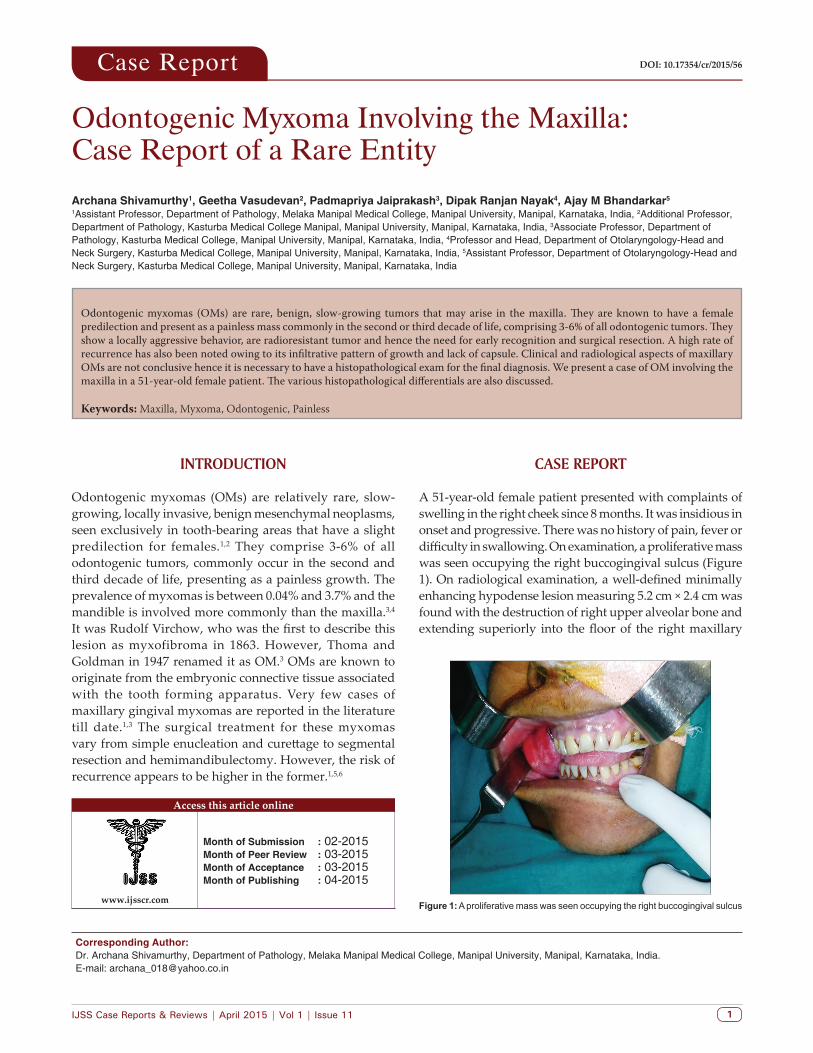
A 51-year-old female patient presented with complaints of swelling in the right cheek since 8 months. It was insidious in onset and progressive. There was no history of pain, fever or difficulty in swallowing. On examination, a proliferative mass was seen occupying the right buccogingival sulcus (Figure 1). On radiological examination, a well-defined minimally enhancing hypodense lesion measuring 5.2 cm × 2.4 cm was found with the destruction of right upper alveolar bone and extending superiorly into the floor of the right maxillary
INTRODUCTION
Odontogenic myxomas (OMs) are relatively rare, slow-growing, locally invasive, benign mesenchymal neoplasms, seen exclusively in tooth-bearing areas that have a slight predilection for females.1,2 They comprise 3-6% of all odontogenic tumors, commonly occur in the second and third decade of life, presenting as a painless growth. The prevalence of myxomas is between 0.04% and 3.7% and the mandible is involved more commonly than the maxilla.3,4 It was Rudolf Virchow, who was the first to describe this lesion as myxofibroma in 1863. However, Thoma and Goldman in 1947 renamed it as OM.3 OMs are known to originate from the embryonic connective tissue associated with the tooth forming apparatus. Very few cases of maxillary gingival myxomas are reported in the literature till date.1,3 The surgical treatment for these myxomas vary from simple enucleation and curettage to segmental resection and hemimandibulectomy. However, the risk of recurrence appears to be higher in the former.1,5,6
Case Report DOI: 10.17354/cr/2015/56
Corresponding Author: Dr. Archana Shivamurthy, Department of Pathology, Melaka Manipal Medical College, Manipal University, Manipal, Karnataka, India. E-mail: [email protected]
Access this article online
www.ijsscr.com
Month of Submission : 02-2015 Month of Peer Review : 03-2015 Month of Acceptance : 03-2015 Month of Publishing : 04-2015
Figure 1: A proliferative mass was seen occupying the right buccogingival sulcus

Shivamurthy, et al.: Odontogenic Myxoma Involving the Maxilla
IJSS Case Reports & Reviews | April 2015 | Vol 1 | Issue 112
sinus. The patient thus underwent right partial maxillectomy and the specimen was sent for histopathological examination.
Gross examination revealed a 6 cm × 4 cm × 2.5 cm bosselated, polypoid growth involving the maxillary bone (Figure 2). On the cut section, the white lobulated myxoid appearance of the tumor was noted. On microscopic examination, the tumor was unencapsulated and composed of randomly dispersed stellate cells with eosinophilic cytoplasmic processes enmeshed in an abundant myxoid stroma (Figure 3a-c). The myxoid intercellular matrix stained positively with alcian blue (Figure 4), but periodic acid-Schiff (PAS) staining was negative. Ulceration of the overlying stratified squamous epithelium was noted along with granulation tissue. On immunohistochemistry, few stellate cells showed positivity for smooth muscle actin (Figure 5), but were negative for S-100. Based on the above observations, a diagnosis of OM was rendered.
DISCUSSION
OMs are rare benign, invasive tumors that exclusively occur in the jaw bone and have a tendency for bone destruction. The mandible is more commonly affected than the maxilla. Although OMs of the maxilla are less frequent, they behave more aggressively than that of the mandible, tend to fill and cause enlargement of the maxillary antrum before clinically presenting as a facial swelling.1,3,4,7,8 In the present case, the patient presented with a facial swelling since 8 months. Several case reports have reported a higher frequency of occurrence in females than males. It is most frequently diagnosed between the second and the fourth decade.1,6,7 However, the present case is being reported in a 51-year-old woman, who had the destruction of right upper alveolar bone and the lesion was extending to the floor of the right maxillary sinus.
On radiography, OM may appear as radiolucent, unilocular or multilocular masses with either honeycomb or soap-
Figure 2: Gross examination revealed a 6 cm × 4 cm × 2.5 cm bosselated, polypoid growth involving the maxillary bone. On cut section, white lobulated myxoid appearance of the tumor was noted
Figure 4: The myxoid intercellular matrix stained positively with alcian blue, but periodic acid-Schiff staining was negative
Figure 5: On immunohistochemistry, few stellate cells showed positivity for smooth muscle actin
Figure 3: (a-c) The tumor was unencapsulated and composed of randomly dispersed stellate cells with eosinophilic cytoplasmic processes enmeshed in an abundant myxoid stroma
c
ba

Shivamurthy, et al.: Odontogenic Myxoma Involving the Maxilla
IJSS Case Reports & Reviews | April 2015 | Vol 1 | Issue 11 3
bubble pattern. Cortical expansion and tooth displacement can also be noted.1,2,9 In the present case, a well-defined minimally enhancing hypodense lesion measuring 5.2 cm × 2.4 cm was detected. The various clinical and radiographic differential diagnosis of OMs include: Odontogenic keratocysts, simple cysts, traumatic bone cysts, intraosseous hemangioma, cherubism, aneurysmatic bony cyst, fibrous dysplasia, ameloblastoma, central giant cell granuloma, and metastatic tumor.1,9,10
OMs are aggressive unencapsulated lesions and said to have been derived from embryonic mesenchymal tissue associated with the development of the teeth/odontogenesis. They are primarily composed of widely scattered undifferentiated spindled to stellate mesenchymal cells in a myxomatous ground substance. The spindle cells have long eosinophilic fibrillary processes that intermesh with each other and do not
show evidence of significant pleomorphism or mitotic figures. Interspersed capillaries and occasionally strands of collagen may be seen. Calcification may or may not be present.3,10,11 Odontogenic epithelium arranged in islands and cords may be present. However, it is not a histological criteria for the diagnosis of OMs. Tumor cells also may show slight alkaline phosphatase activity.1,3,11 Hyaluronic acid (80%) is the major component of the ground substance with a relatively small amount of chondroitin sulfate, fibronectin, and proteoglycans. The myxoid intercellular matrix stains positively with alcian blue, but PAS staining may be negative.3-5 In the present case, a bosselated, polypoid growth was seen, involving the maxillary bone with white lobulated myxoid appearing cut surface. On microscopy, the tumor was unencapsulated and composed of randomly dispersed stellate cells with eosinophilic cytoplasmic processes enmeshed in an abundant myxoid stroma, which was alcian blue positive.
Table 1: Differential diagnosis of OMsEntity Clinicoradiographic features Histopathological featuresMyxoid nerve sheath tumorsCentral neurofibroma
Localized facial or intraoral swellingWide age range (2‑65 years)Rarely involve mandible and maxillaCan be seen in association with neurofibromatosisRadiolucent
Circumscribed but unencapsulated lesionInterlacing bundles of elongated cells with tapering, wavy nucleiWire‑like strands of collagenIHC: S‑100 positive
Chondromyxoid fibroma Very rarely involves maxilla/mandibleMales between the age of 10 and 35 yearsLytic ovoid lesion with sharp sclerotic margins and pseudo loculated on radiography
Usually encapsulated masses composed of nodules cartilage found in between fibromyxoid areasThe chondrocytes are disposed in sparsely cellular lobules of myxoid or chondroid matrixSpindle cell stromal areas and areas of calcification
Rhabdomyosarcoma Most common malignant tumor of soft tissue in children under 15 years of ageAre known to occur in the maxillary sinusPain of the cheek is the major facial symptom
Embryonal form is the most frequentSheets of small, spindled or moderate to poorly differentiated round cells with scant or deeply eosinophilic cytoplasm and eccentric, small oval nucleiMyogenin/desmin positive
Myxoid liposarcoma Extremely rare in the head and neckCan very rarely present as a periodontal mass
Lobules of bland, relatively uniform, spindled to ovoid to round cells in an abundant light pink to blue‑gray myxoid/mucoid matrixNeoplastic nuclei have a uniform chromatin pattern and generally inconspicuous nucleoliProminent delicate plexiform capillary networkUnivacuolated signet‑ring lipoblasts and multivacuolated lipoblasts
Myxoid fibrosarcoma Major symptoms are pain, swelling, and sometimes loosening of the teethUsually affects subcutis of distal extremities in elderly patients, rarely found around the maxillary region
Spindle‑shaped cells, deposited in a variably fibrous and myxoid stroma with significant mitotic activity and nuclear pleomorphismPositive for vimentin and MIB‑1, andfocally positive for CD68Negative for: 1‑SMA, desmin, S100, EMA
Myxoid chondrosarcoma Usually occurs in the soft tissue of extremities of adultsOnly rarely originate in the head and neck in childrenShow a permeative pattern of osseous destruction on radiography associated soft tissue mass
Abundant chondroid matrix and malignant chondroblastic cells arranged in cords resembling chordoma
Nodular fasciitis Up to 20% of cases may occur in the head and neck regionMost common in the third decadeMales and females are equally affected
May be circumscribed but not encapsulatedSpindle‑cell lesion composed of loose, plump, bipolar fibroblastic cells arranged in a storiform pattern with loose myxoid backgroundMitotic activity may be presentExtravasated red blood cells and a mixed inflammatory infiltrate is presentIHC: Vimentin‑positive,Actin, keratin, SMA, S‑100, and desmin are negative
SMA: Smooth muscle actin, OMs: Odontogenic myxoma, IHC: Immunohistochemistry, EMA: Epithelial membrane antigen

Shivamurthy, et al.: Odontogenic Myxoma Involving the Maxilla
IJSS Case Reports & Reviews | April 2015 | Vol 1 | Issue 114
Some of the microscopic differential diagnoses include myxoid nerve sheath tumors, chondromyxoid fibroma, rhabdomyosarcoma, and nodular fasciitis. Rapidly growing neoplasms showing myxoid degeneration such as fibrosarcomas, chondrosarcomas, and liposarcomas also fall into the differential diagnosis (Table 1).3,10,11
OM tumor cells are mesenchymal in origin and express vimentin and muscle-specific actin. They are negative for, neuron-specific enolase, S-100 alpha and beta subunits, factor VIII-related antigen, and cytokeratin.1,2,11
Effective nucleation and curettage difficult as OMs tend to permeate and destroy marrow spaces. Larger tumors require complete excision with free margins. Recurrence rates from various studies average about 25%. Despite the fact that OM shows aggressive local growth, it is believed that it never undergoes malignant transformation or gives rise to metastasis.4,6,11
CONCLUSION
Clinical and radiological aspects of maxillary OMs are not conclusive, it is necessary to have a histopathological exam for the final diagnosis. Because of its high rate of recurrence, especially due to its gelatinous and mucous aspect, surgical treatment through bone resection is the most indicated treatment modality, and the patient must be followed-up closely for years.
REFERENCES
1. Jain VK, Reddy SN. Peripheral odontogenic myxoma of maxillary gingiva: A rare clinical entity. J Indian Soc Periodontol
2013;17:653-6.2. Manjunath S, Gupta A, Swetha P, Moon NJ, Singh S, Singh
A. Report of a rare case of an odontogenic myxoma of the maxilla and review of literature. Ann Med Health Sci Res 2014;4:S45-8.
3. Shah A, Lone P, Latoo S, Ahmed I, Malik A, Hassan S, et al. Odontogenic myxoma of the maxilla: A report of a rare case and review on histogenetic and diagnostic concepts. Natl J Maxillofac Surg 2011;2:189-95.
4. Halfpenny W, Verey A, Bardsley V. Myxoma of the mandibular condyle. A case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:348-53.
5. Landa LE, Hedrick MH, Nepomuceno-Perez MC, Sotereanos GC. Recurrent myxoma of the zygoma: A case report. J Oral Maxillofac Surg 2002;60:704-8.
6. Saylam G, Dursun E, Albayrak L, Akmansu H, Korkmaz H, Eryilmaz A. Odontogenic myxoma of the maxilla: A case report. Kulak Burun Bogaz Ihtis Derg 2007;17:294-7.
7. Noffke CE, Raubenheimer EJ, Chabikuli NJ, Bouckaert MM. Odontogenic myxoma: Review of the literature and report of 30 cases from South Africa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101-9.
8. Kumar N, Jain S, Gupta S. Maxillary odontogenic myxoma: A diagnostic pitfall on aspiration cytology. Diagn Cytopathol 2002;27:111-4.
9. Ramaraj PN, Shah SP. Peripheral myxoma of maxilla. A case report. Indian J Dent Res 2003;14:67-9.
10. Arul AS, Verma S, Arul AS, Verma R. Infiltrative odontogenic myxoma of the posterior maxilla: Report of a case. J Nat Sci Biol Med. 2013;4:484-7.
11. Adebiyi KE, Ndukwe KC, Aregbesola SB. Odontogenic and oral soft tissue myxomas: Clinicopathologic analysis of 16 cases from Ile-Ife, Nigeria. Afr J Med Med Sci 2012;41:445-9.
How to cite this article: Shivamurthy A, Vasudevan G, Jaiprakash P, Nayak DR, Bhandarkar AM. Odontogenic Myxoma Involving the Maxilla: Case Report of a Rare Entity. IJSS Case Reports & Reviews 2015;1(11):1-4.
Source of Support: Nil, Conflict of Interest: None declared.