oh those swollen legs!! edema confusionis edema controlled? 6. is tissue growth optimized? 7. is the...
TRANSCRIPT
OH THOSE SWOLLEN LEGS!!EDEMA CONFUSION
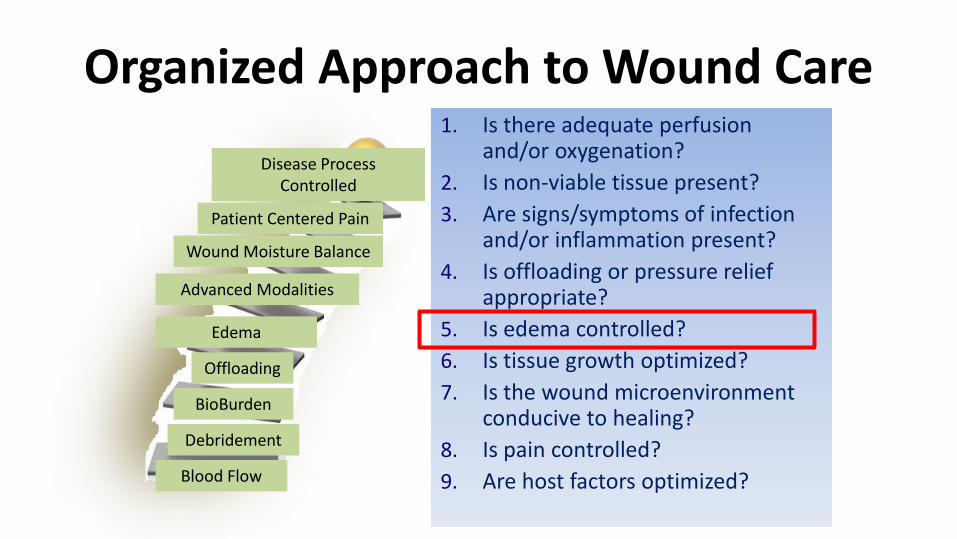
Organized Approach to Wound Care1. Is there adequate perfusion
and/or oxygenation?
2. Is non-viable tissue present?
3. Are signs/symptoms of infection and/or inflammation present?
4. Is offloading or pressure relief appropriate?
5. Is edema controlled?
6. Is tissue growth optimized?
7. Is the wound microenvironment conducive to healing?
8. Is pain controlled?
9. Are host factors optimized?
Offloading
Disease Process Controlled
BioBurden
Advanced Modalities
Wound Moisture Balance
Debridement
Blood Flow
Patient Centered Pain
Edema
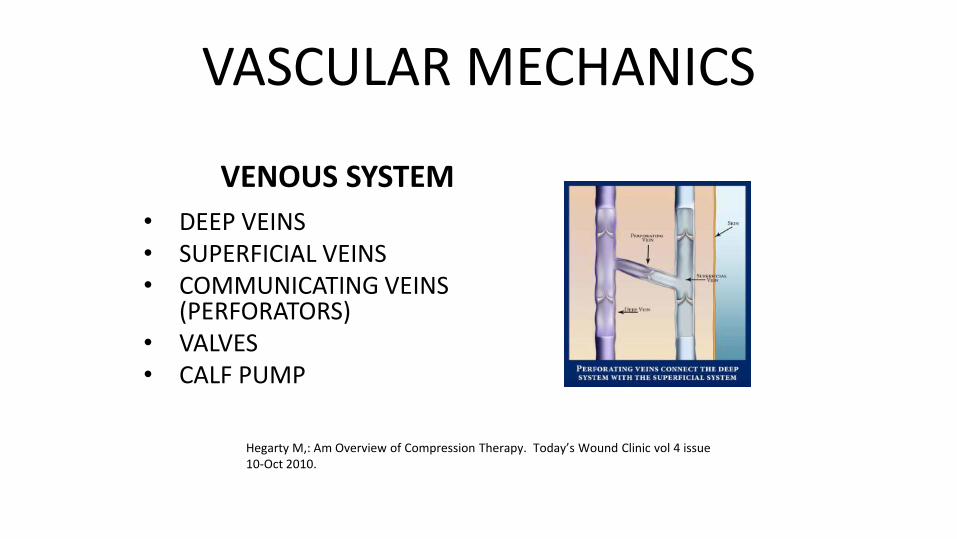
VASCULAR MECHANICS
VENOUS SYSTEM
• DEEP VEINS• SUPERFICIAL VEINS• COMMUNICATING VEINS
(PERFORATORS)• VALVES• CALF PUMP
Hegarty M,: Am Overview of Compression Therapy. Today’s Wound Clinic vol 4 issue 10-Oct 2010.


CHRONIC VENOUS ULCERS (CVI)Venous Ulcer account for 60-90% of leg ulcers
More common in women: 3X
Difficult to heal: 50% > 9 months/20% > 2 years
High rate of reoccurrence: 60% WHY???
76% Diagnosed by presentation alone
Advances in Skin & Wound Care: August 2009 - Volume 22 - Issue 8 - p 384

What Effects the Pressure??Directly proportional to persons Height and Distance from head to feet
OBESITY: Linear relationship girth and venous pressure
Resting Pressure/supine: ~8 mmHG
Standing: + 100 mmHG
Ambulation: ~25-100 mmHg
Hegarty M,: Am Overview of Compression Therapy. Today’s Wound Clinic vol 4 issue 10-Oct 2010
Partsch H, Annuals Vascular Disease 2012

VENOUS PRESSURE :Anatomic FailureAmbulatory Venous Hypertension:The elevated pressure in the leg vein during walkingEven with intact vessels:25 mmHg calf pump - 8 mmhg rest = 17 mmHg
1. Venous Wall Physical Properties: Reduced Strength2. Venous Valves
Degenerative damage DVT3. Calf Pump (….exercise…..☺)
90% of venous return is through these 3
Partsch, H; compression therapy of venous ulcers;, Hemodynamic effects depend on interface pressure and stiffness; EWMA Journal 2006, vol 6 NO2.
Fletcher, Moffatt, Partsch, Vowden, Vowden: Principles of Compression in venous disease, a practitioner's guide to treatment and prevention of venous leg ulcers; Wounds International: 2013

LYMPHEDEMA
An abnormal collection of excessive tissue proteins, edema, chronic inflammation and fibrosis in the interstitial space. The International Society of Lymphology
CHRONIC PROBLEM
NO CURE
TREATMENT: CDT PROGRAM -Manual Lymphatic Drainage
-Compression Therapy-Skin Care-Exercise

ANATOMY• PRECOLLECTORS
• COLLECTORS
• LYMPHATIC CAPILLARIES
• NODES
• THORACIC DUCT


(Dr. Wade Farrow)“WITHOUT FUNCTIONAL LYMPHATICS, WE WOULD DIE IN ABOUT 24 HOURS.”
Guyton AC: Texbook of Medical Physiology. 8th ed. Philadelphia. PA: WB Saunders: 1991.
Carlson JA (2014) Lymphedema and subclinical lymphostasis (microlymphedema) facilitate cutaneous infection, inflammatory dermatoses, and neoplasia: A locus minoris resistentiae. Clin Dermatol32(5): 599–615Foldi M, Foldi E (2012) Textbook of Lymphology (3rd edn.). Elsevier GmbH, Munchen, Germany
Carlson and Foldi:
Failure= infection, inflammation and carcinogenesis


“PHLEBOLYMPHEDEMA”
WHAT?????
Mixed-etiology swelling…….
CVI+ lymphatic insufficiency
=Phlebolymphedema
DEFINED….
Phlebolymphedema:
is due to insufficiency of the venous or/and lymphatic system, in combination with possible systemic contributors, leading to accumulation of protein-rich fluid in the interstitial space.
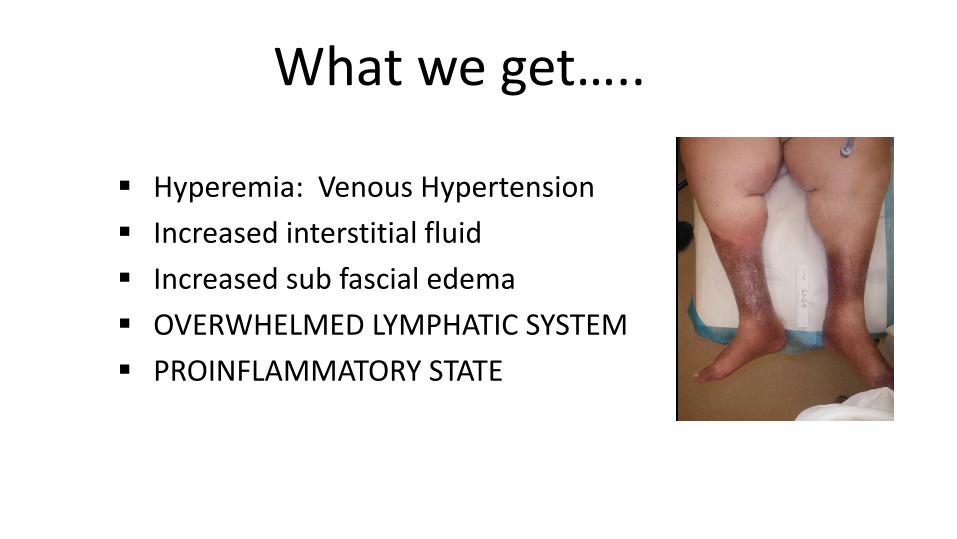
What we get…..
▪ Hyperemia: Venous Hypertension
▪ Increased interstitial fluid
▪ Increased sub fascial edema
▪ OVERWHELMED LYMPHATIC SYSTEM
▪ PROINFLAMMATORY STATE
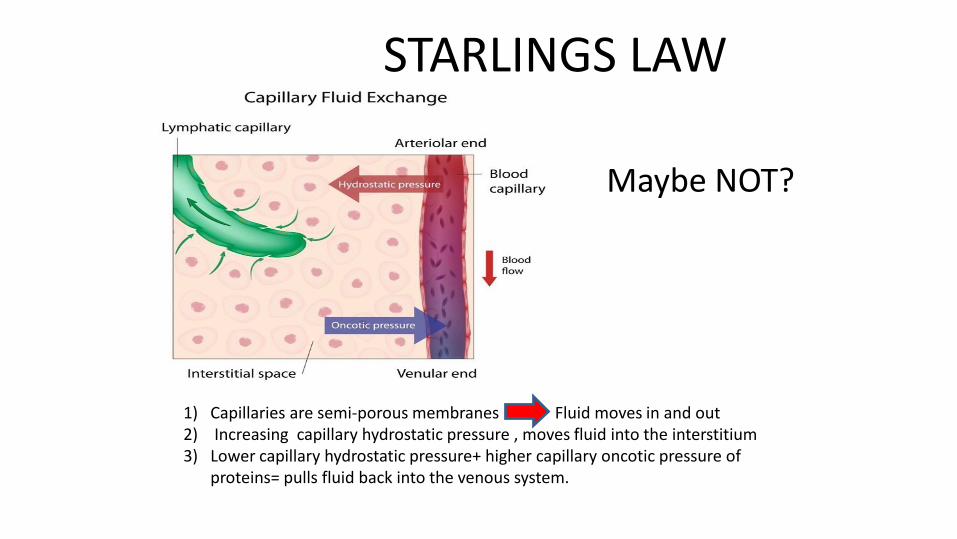
STARLINGS LAW
1) Capillaries are semi-porous membranes Fluid moves in and out2) Increasing capillary hydrostatic pressure , moves fluid into the interstitium3) Lower capillary hydrostatic pressure+ higher capillary oncotic pressure of
proteins= pulls fluid back into the venous system.
Maybe NOT?
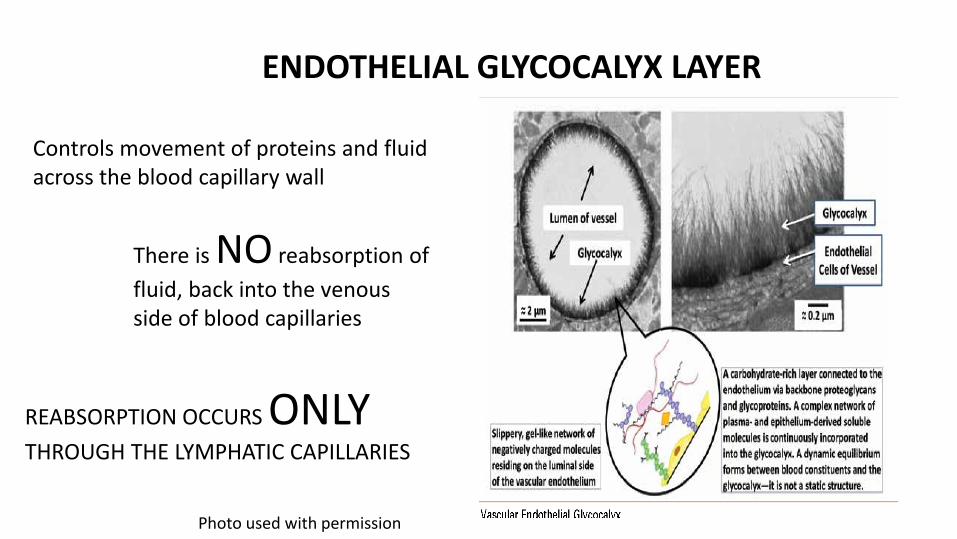
ENDOTHELIAL GLYCOCALYX LAYER
Controls movement of proteins and fluid across the blood capillary wall
There is NO reabsorption of
fluid, back into the venous side of blood capillaries
REABSORPTION OCCURS ONLYTHROUGH THE LYMPHATIC CAPILLARIES
Photo used with permission

The EGL: regulates fluid/protein movement1. through the capillary wall to tissue2. Prevents movement back into venous side of
capillaries: even in presence of higher pressures.
“All fluid/protein exiting the blood capillaries into the interstitium MUST be removed by the lymphatics.”
THEREFORE:
“ Arguably, it may be better to consider the presence of chronic oedema as synonymous with the presence of lympheoedema, in as much all oedema represents relative lymph drainage failure.” Mortimer
and Rockson (2014)

CLINCAL CONSIDERATIONS
Consider lymphatic function
Recognize lymphedema comes in various forms
Consider CDT/MLD program: Referral -compression -exercise-manual lymphatic mobilization-skin care

WHAT DOES ALL THIS LOOK LIKE??





COMPRESS

PURPOSE OF COMPRESSION
1. Counteract the force of gravity and promote the normal flow of venous blood up the leg
2. Acts on the venous and lymphatic systems to improve venous and lymph return and reduce edema
2. Causes narrowing of the superficial veins
Meissner,M, Lower Extremity Venous Anatomy, Interventional Radiology, Sept. 2005, ; 22(3): 147-158

WHAT IS ADAQUATE COMPRESSION Overcomes intravenous pressure
Exerts a sub-bandage resting pressure that is well tolerated in a resting position
Provides a pressure increase when the patient rises to a standing position: (50-70mmHG)
Provides external compression improving venous reflux during walking: calf pump
Fletcher, Moffatt, Partsch, Vowden, Vowden: Principles of Compression in venous disease, a practitioner's guide to treatment and prevention of venous leg ulcers; Wounds International: 2013
Partsch, H; compression therapy of venous ulcers;, Hemodynamic effects depend on interface pressure and stiffness; EWMA Journal 2006, vol 6 NO2.

Beidler et al, Multiplexed analysis of matrix metalloproteinases in leg ulcer tissue of patients with chronic venous insufficiency before and after
compression therapy. Wound Rep Regen 16:642-648, 2008.
Elevated MMP-1 in Venous Ulcers

TYPESCOMPRESSION WRAPS
COMPRESSION HOSIERY
INTERMITTENT PNEUMATIC COMPRESSION (IPC)
MIXED TYPES
Types of Compression• ELASTIC• INELASTIC• STATIC• DYNAMIC • WRAPS• HOSE• LONG STRETCH, SHORT STRETCH • NON-STRETCH
HELP!!!!!
PARTNER WITH A LYMPHATIC THERAPIST
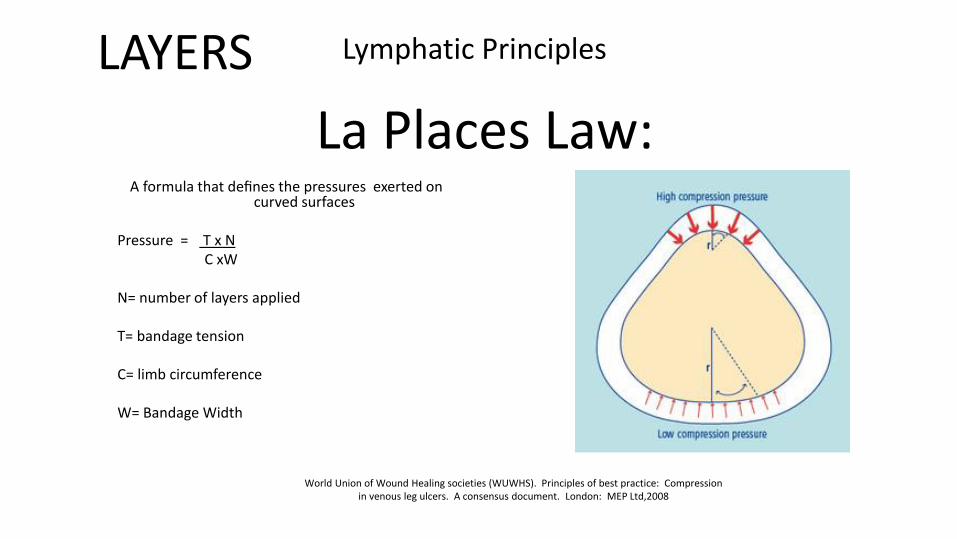
La Places Law:A formula that defines the pressures exerted on
curved surfaces
Pressure = T x N C xW
N= number of layers applied
T= bandage tension
C= limb circumference
W= Bandage Width
World Union of Wound Healing societies (WUWHS). Principles of best practice: Compression in venous leg ulcers. A consensus document. London: MEP Ltd,2008
Lymphatic PrinciplesLAYERS

Non-Stretch
ZINC PASTE BANDAGES

Short Stretch
Bandages that stretch to less than 100% of their original length: minimal extensibility
High Working Pressure/Low Resting Pressure

Long Stretch
Expands over 100% of its original length
Low Working Pressure/High Resting Pressure
Contains Elastomeric Fibers: fibers that are able to stretch and return to almost their original size.
World Union of Wound Healing societies (WUWHS). Principles of best practice: Compression in venous leg ulcers. A consensus document. London: MEP Ltd,2008

FUNCTIONAL COMPRESSIONS: shape
T: texture
R: refill
I: issues
D: dosage
E: etiology CVIDFUARTERIAL
20-3030-40….
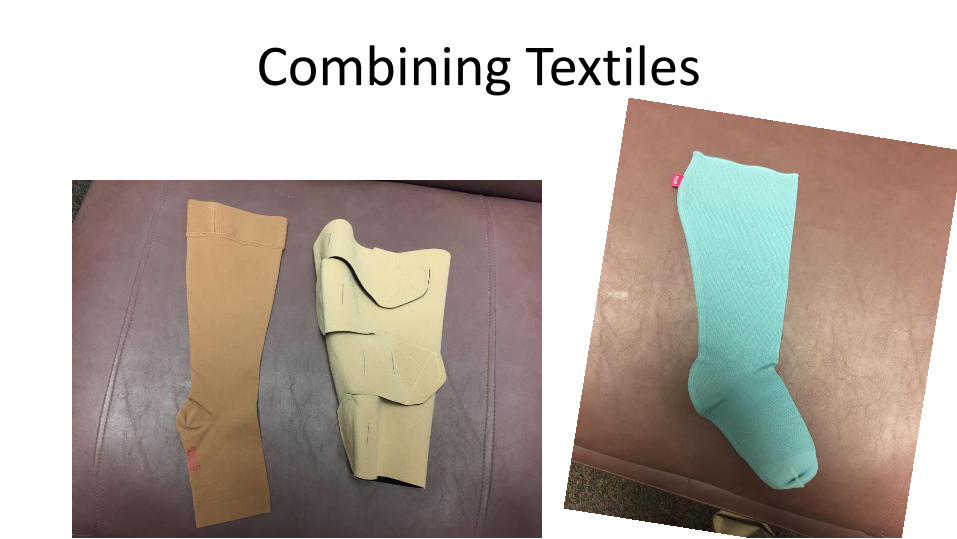
Combining Textiles




7 Year recaltrate ulcer: CVI
Active treatment x 3 years: 3 days/week
Referral to Physical Therapy
-elevation
-exercise/gait
-multilayer compression wrap: short stretch



TAKE HOME PEARLS
• THINK ABOUT THE WHOLE PATIENT…..
• REMEMBER OTHER SPECIALITIES THAT MAY BE ABLE TO HELP
• EDEMA IS NOT DIAGNOSIS SPECIFIC: ALWAYS, NEVER…ETC
• EXERCISE/MOBILITY
• LYMPHATIC CARE/EDUCATION
• COMPRESSION TOOLS/TRICKS
SOME COMPRESSION IS ALWAYS BETTER
THAN NO COMPRESSION

BIBLIOGRAPHY• Brenner E, Putz D.MorigglB: Stemmer (Kaposi-Stemmer-sign-30 years later. Phlebologie.2007: 36(6):320-324.
• Farrow W, Phlebolymphedema-A common Underdiagnosed and Undertreated problem in the wound Care clinic. Journal fo the Am. College of certified Wound specialists (2010) 2: 14-23
• Valencia IC, Falabella A, Kirsner RS, Eaglstein WH: chronic venous insufficiency and venous leg ulceration . J am Acad, Dermatol. 2001 44(3):401-421.
• Guyton AC: texbook of Medial Physiology. 8th Ed. Philadelphia PA: WB Saunders: 1991.
• FoldiE, Foldi M, Chronic venous insufficiency and venous-lymphostatic insufficiency. In: Foldi’s texbook of lymphlogy . 2nd ed. Munich, Germany; Elsevier, 2006 p. 434-447.
• Fugman SL, Clar, RA, Stasis dermatitis. Available at Http://emedicine . Medscape,com/article/1084813-overview. Accessed april 26, 2010
• Goldman MP: Lipodermatosclerosis: review of ases evaluated at the Mayo clinic H Am Acad Dermatol. 2002:46: 187-192.
• Blankfield RP, Finkelhor RS, AlexanderJJ, et al: Etiology and diagnosis of bilateral leg edema in primary care. Am J Med. 1998: 105: 192-197.
• Beidler, S. K., Douillet, C. D., Berndt, D. F., Keagy, B. A., Rich, P. B., & Marston, W. A. (2009). Inflammatory cytokine levels in chronic venous insufficiency ulcer tissue before and after compression therapy. Journal of Vascular Surgery, 49(4), 1013–1020. http://doi.org/10.1016/j.jvs.2008.11.049
• Bjork R, Hettrick H; Endothelial glycocalyx layer and interdependence of lymphatic and integumentary systems, Wounds International 2018, Vol 9 Issue 2 .
• Best Practice for the Management of Lymphoedema - 2nd edition, www.lympho.org
• Bjork, Ehman, S.T.R.I.D.E. Professional Guide to Compression Garment Selection for the Lower Extremity, Journal of Wound Care Vol. 28, No Sup6a free access,Published Online:7 Jun 2019