olv
TRANSCRIPT
ONE LUNG VENTILATION, COMPLIANCE CURVES,DLTs,GAS
EXCHANGE/MANAGEMENT OF OLV
MODERATOR: DR SANJAY SHRESTHA
11th september, 2014
kmcth
OLV separation of the two lungs
intentional collapse of a lung on the operative side of the patient
OLV provides: protection of healthy lung from infection/bleeding (lung isolation)
diversion of ventilation away from damaged airway or lung
improved exposure of surgical field
ONE LUNG VENTILATION (OLV)
Indications for One-Lung Ventilation
• ABSOLUTEIsolation of each lung to prevent contamination of a healthy lung
– Infection (abscess, infected cyst)
– Massive hemorrhage
• Control of distribution of ventilation to only one lung
– Bronchopleural fistula
– Bronchopleural cutaneous fistula
– Unilateral cyst or bullae
– Major bronchial disruption or trauma
• Unilateral lung lavage
• Video-assisted thoracoscopic surgery
• RELATIVESurgical access
– Thoracic aortic aneurysm
– Pneumonectomy
– Lobectomy
– Esophageal surgery
– Mediastinal surgery- mass resection, thymectomy
Thoracic spinal surgery
?Severe hypoxemia due to unilateral lung disease
Physiology
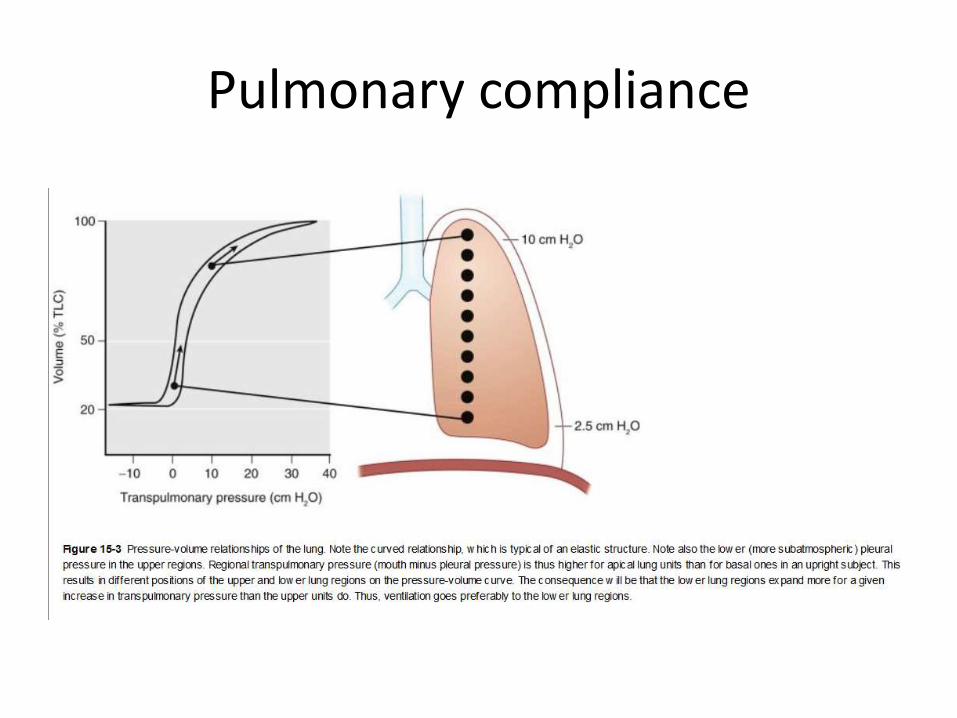
Pulmonary compliance
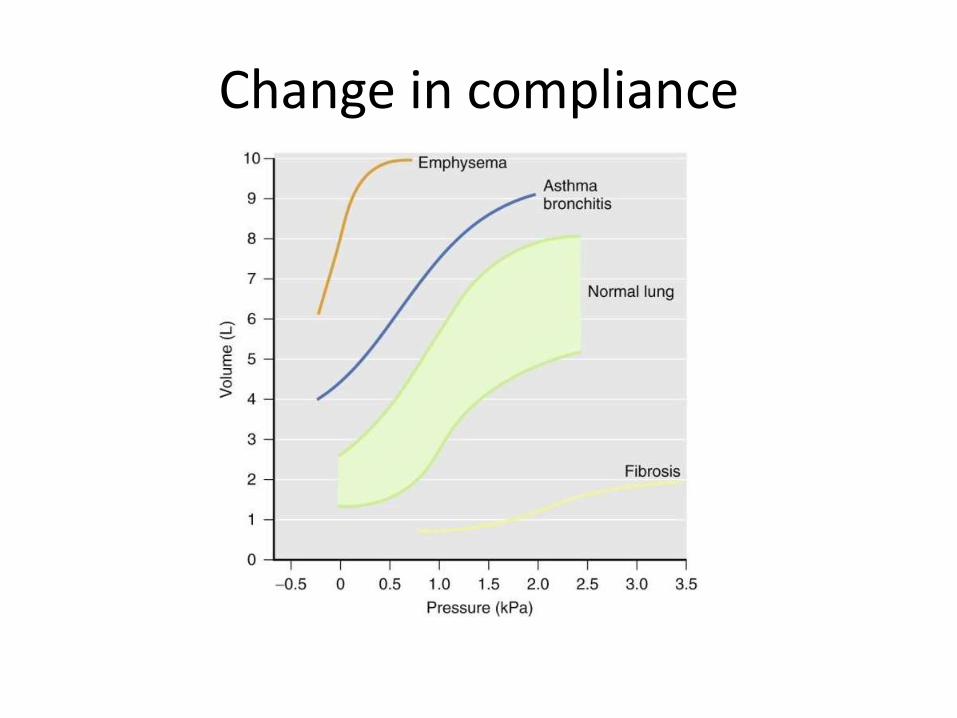
Change in complianceFigure 15curves of the lung in health and lung disease. Note the much flatter slope of the curve in fibrotic lung disease, which reflects a considerable increase in pressure variation and respiratory work. Also, note the parallel shift in the pressureasthmatic and shows that compliance need not change in these diseases, although lung volume may have increased. Finally, note the steep slope of the curve of an emphysematous patient. This indicates loss of elastic tissue and might even suggest reduced respiratory work. However, such patients, as well as asthmatic and airway resistance, which causes elevated respiratory work. the BMJ series: Respiratory Measurement.)
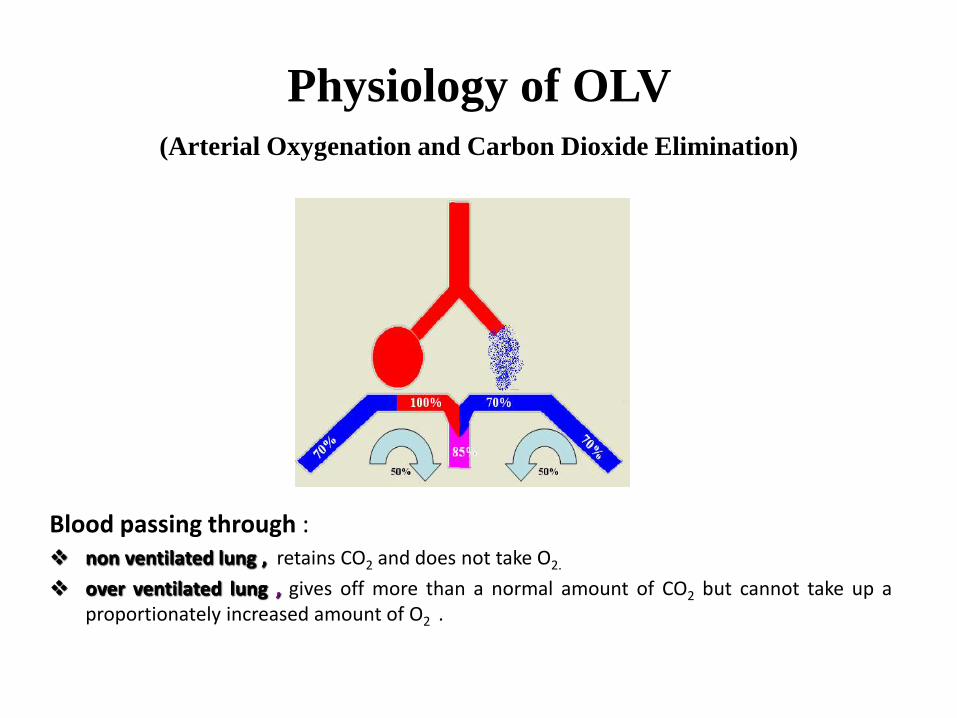
Physiology of OLV
(Arterial Oxygenation and Carbon Dioxide Elimination)
Blood passing through : non ventilated lung , retains CO2 and does not take O2.
over ventilated lung , gives off more than a normal amount of CO2 but cannot take up aproportionately increased amount of O2 .
Thus, during one-lung ventilation
more decreased oxygenation than during two-lung ventilation in LDP
due to an obligatory Rt-Lt transpulmonary shunt through the nonventilated
nondependent lung. Consequently, lower PaO2 & larger P(A-a)O2
usu CO2 elimination is not a problem; but retention of CO2 by blood
traversing the nonventilated lung slightly exceeds the increased
elimination of CO2 from blood traversing the ventilated lung, and the PaCO2
will usually slowly increase and P(A-a)CO2 decreases .
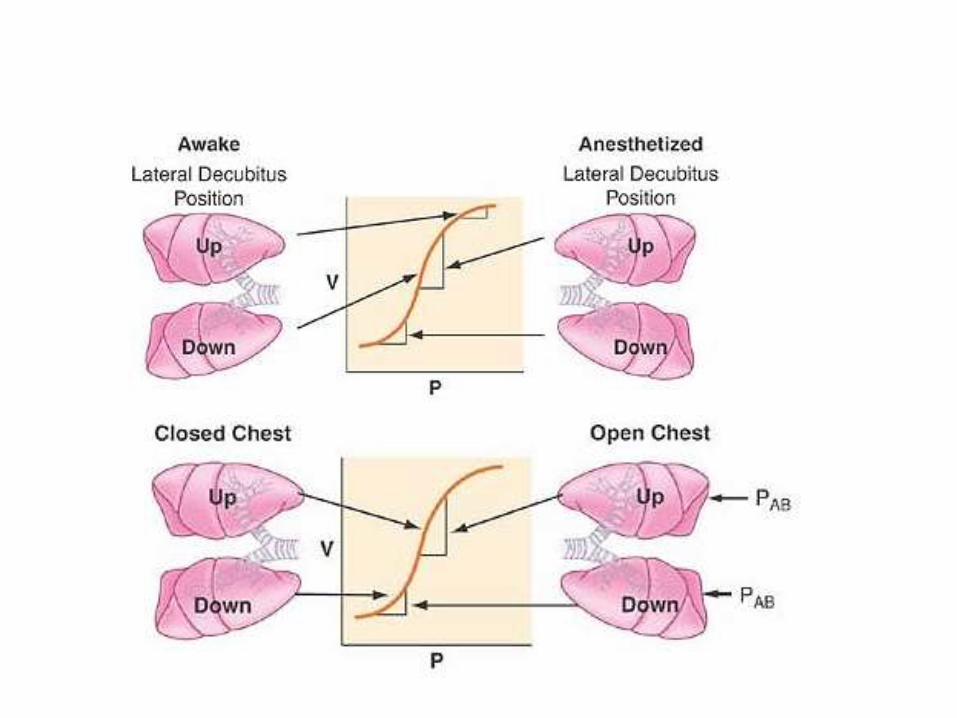
Physiology of the Lateral Decubitus Position
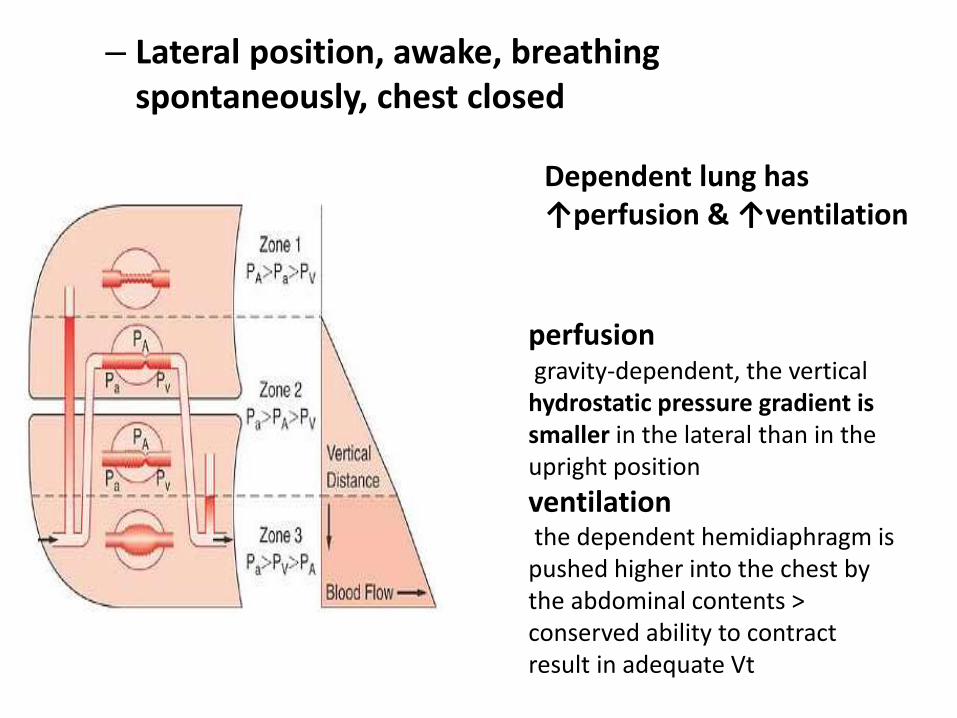
– Lateral position, awake, breathing spontaneously, chest closed
perfusiongravity-dependent, the vertical hydrostatic pressure gradient is smaller in the lateral than in the upright position
ventilationthe dependent hemidiaphragm is pushed higher into the chest by the abdominal contents > conserved ability to contract result in adequate Vt
Dependent lung has ↑perfusion & ↑ventilation
Lateral position, awake, breathing spontaneously, chest open
• e.g thoracoscopy under intercostal block
• Two complications can arise– Mediastinal Shift, usually occurring during inspiration >> can lead to
shock and respiratory distress
– Paradoxical Breathing
– Inspiration : negative pressure in intact hemithorax compared with atmospheric pressure in the open hemithorax can cause movement of air from the nondependent to dependent lung. opposite occurs during expiration (gas movement reversal)
– wasted ventilation and decreased amount of gas exchange
– increased by a large thoracotomy or by an increase in airway resistance in the dependent lung
– Positive-pressure ventilation or adequate sealing prevents it
Lateral position, anesthetized, breathing spontaneously, chest closed
• GA causes ↓vol. in both lungs
• More so in dependent lung due tocephalad displacement of diaphragmpressure due to mediastinal structures
• Thus, Most Vt enters the nondependent lung (underperfused)
• So significant V/Q mismatch
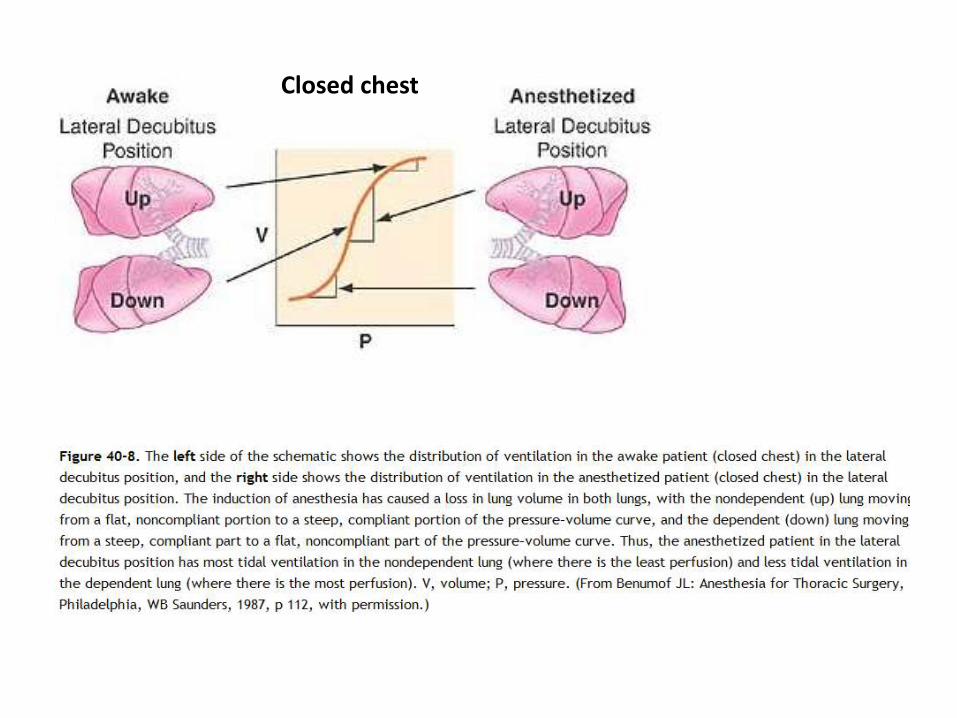
Closed chest
Lateral position, anesthetized, breathing spontaneously, chest open
• Little impact on perfusion
• Upper lung free to expand (without chest wall restriction)
• Increase in V/Q mismatch as the nondependent lung is preferentially ventilated
Lateral position, anesthetized, paralyzed, chest openTwo lung ventilation
• Due to positive-pressure ventilation, diaphragmatic displacement is maximal over the nondependent lung, where there is the least amount of resistance to diaphragmatic movement caused by the abdominal contents
• Depended (relatively perfused) less ventilated
• increases the V/Q mismatch.
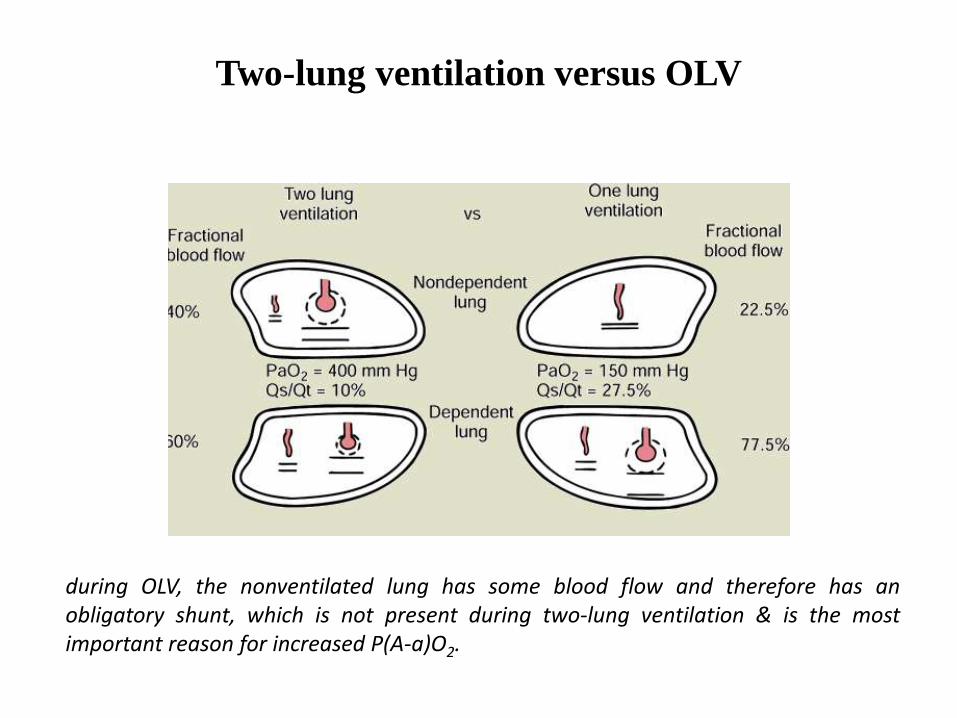
Two-lung ventilation versus OLV
during OLV, the nonventilated lung has some blood flow and therefore has anobligatory shunt, which is not present during two-lung ventilation & is the mostimportant reason for increased P(A-a)O2.
One-lung ventilation, anesthetized, paralyzed, chest open
• two-lung ventilation in the lateral position : nondependent lung 40% C.O. 60% dependent lung
• Shunt 5% in each lung
• C.O participating in gas exchange 35% nondependent 55% in the dependent
• right-to-left transpulmonary shunt
• active HPV, blood flow nondependent hypoxic lung will be decreased by 50% (35/2) = 17.5%+5%=22.5%+5%=27.5%(Pao2
= 150 mm Hg )
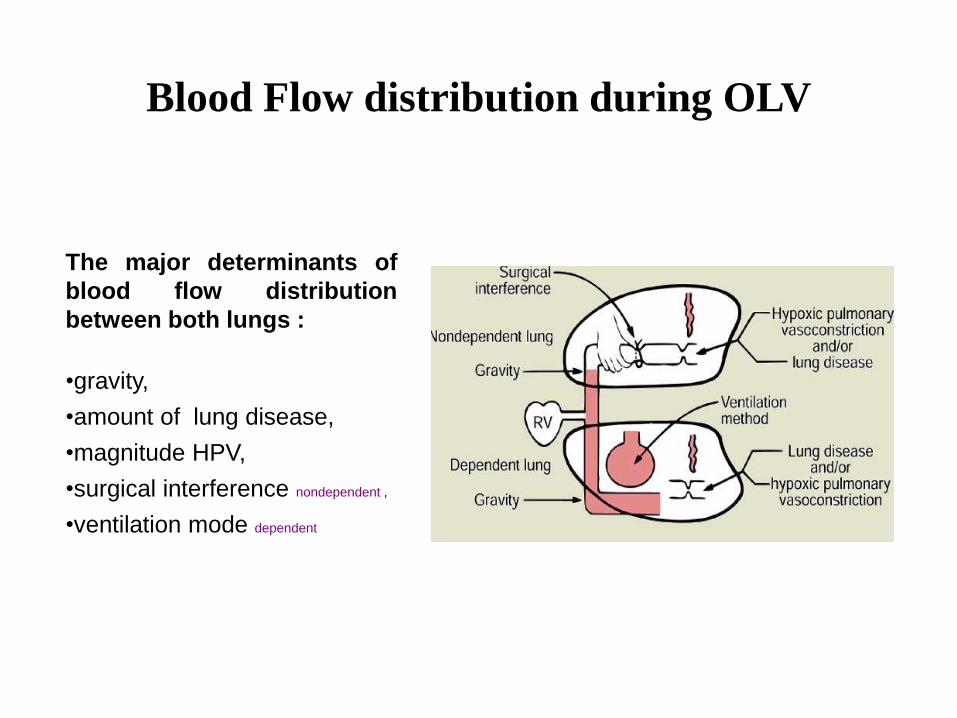
Blood Flow distribution during OLV
The major determinants of
blood flow distribution
between both lungs :
•gravity,
•amount of lung disease,
•magnitude HPV,
•surgical interference nondependent ,
•ventilation mode dependent
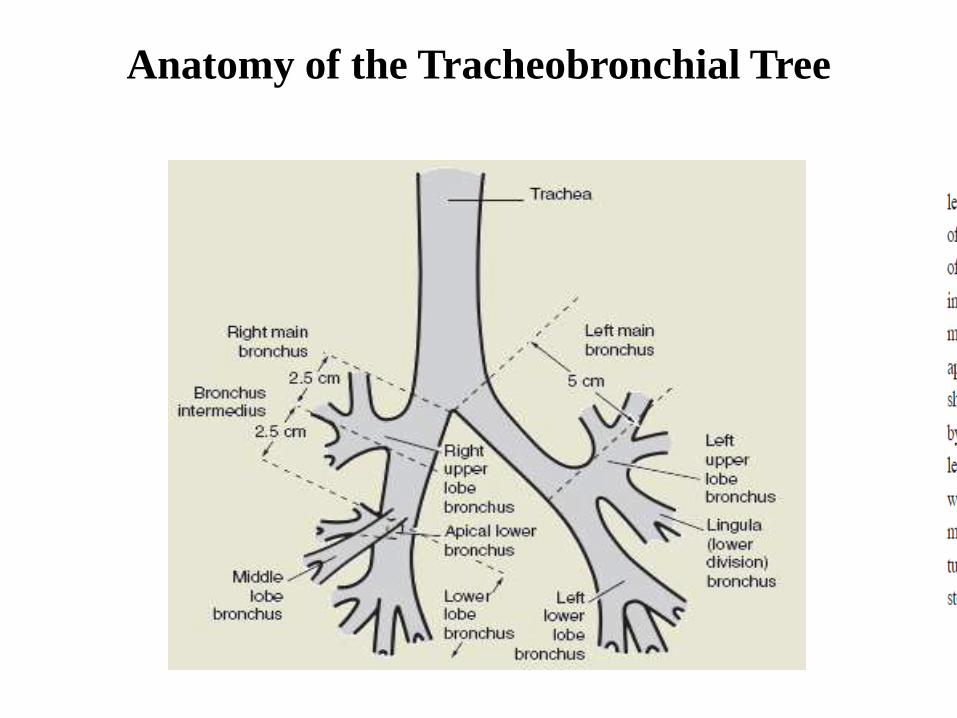
Anatomy of the Tracheobronchial Tree
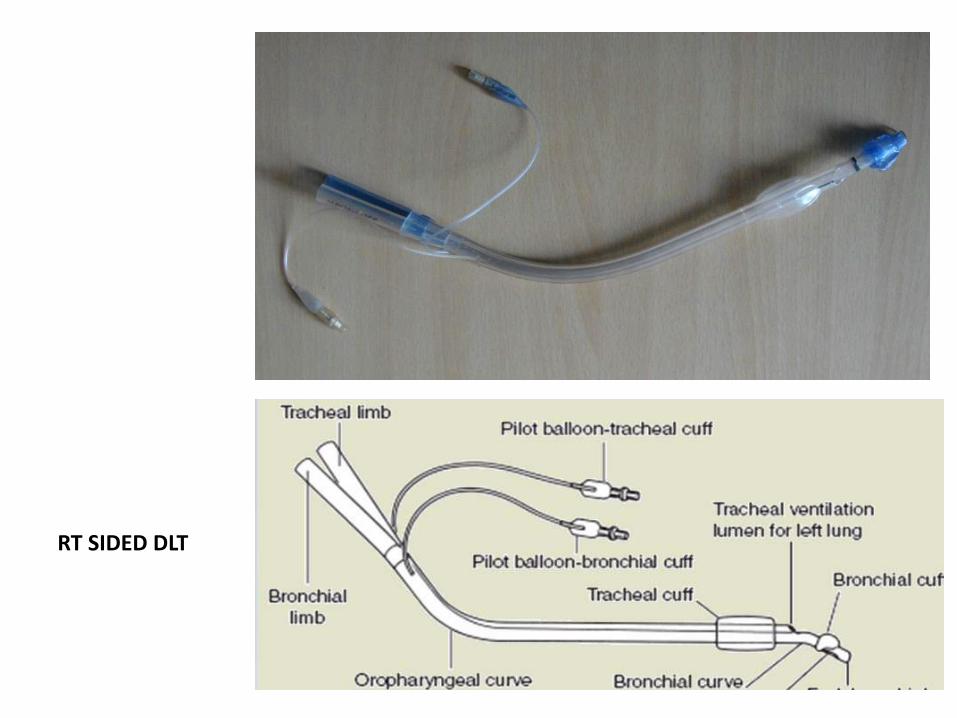
RT SIDED DLT
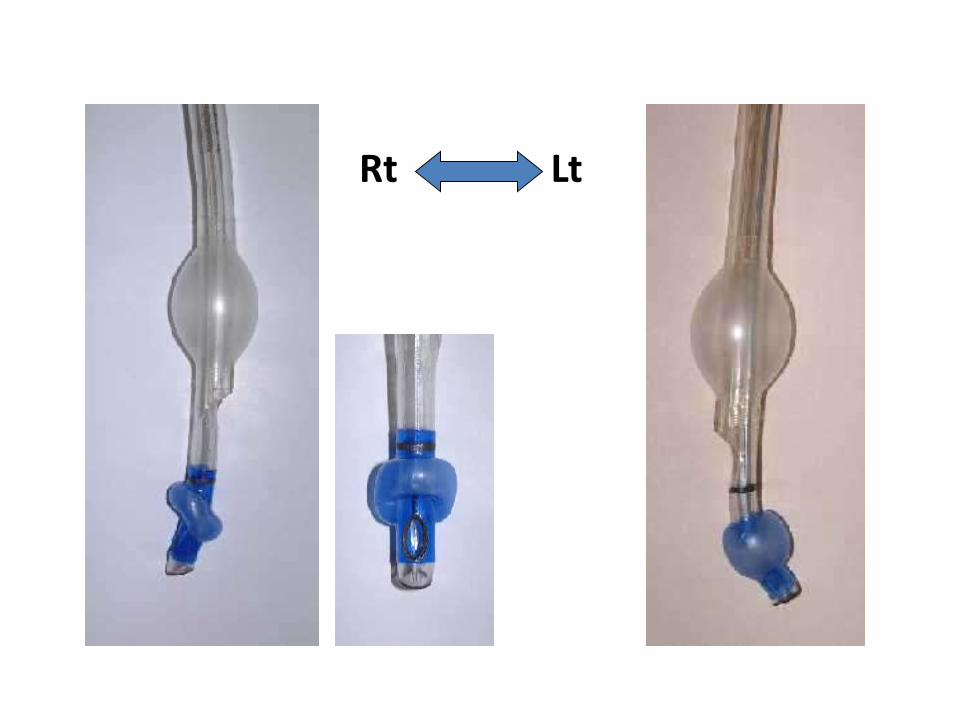
Rt Lt
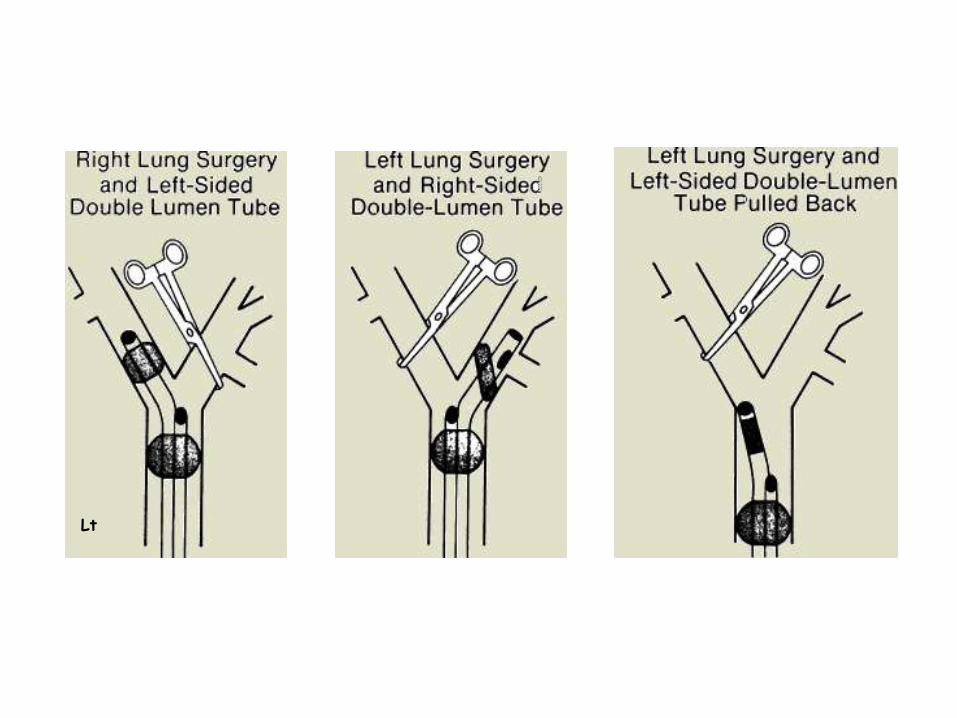
Lt
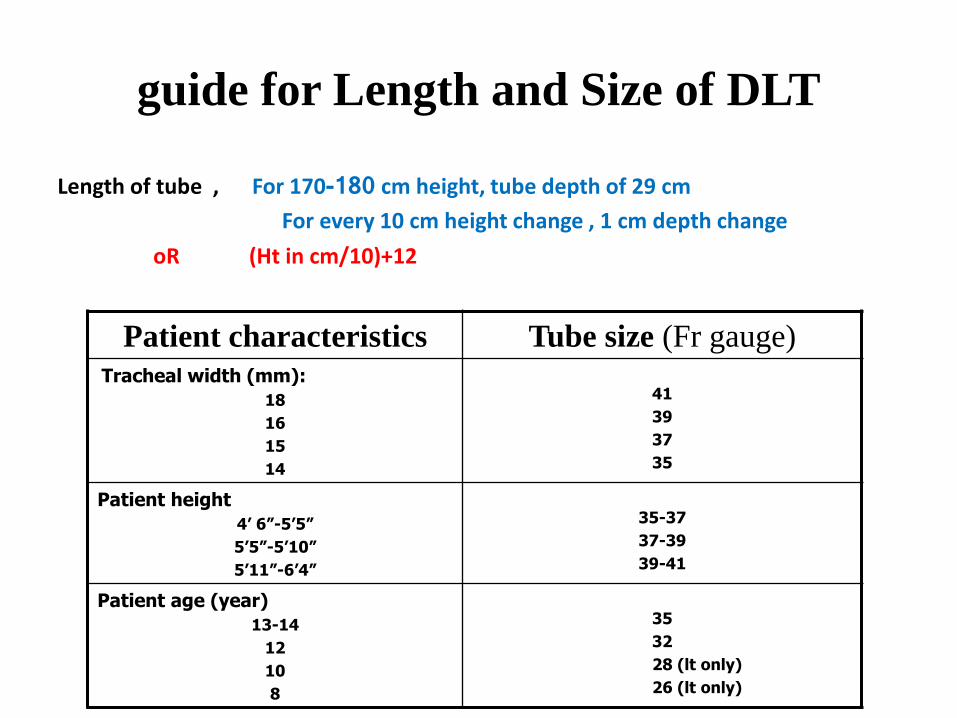
guide for Length and Size of DLT
Length of tube , For 170-180 cm height, tube depth of 29 cm
For every 10 cm height change , 1 cm depth change
oR (Ht in cm/10)+12
Patient characteristics Tube size (Fr gauge)Tracheal width (mm):
18
16
15
14
41
39
37
35
Patient height
4’ 6”-5’5”
5’5”-5’10”
5’11”-6’4”
35-37
37-39
39-41
Patient age (year)
13-14
12
10
8
35
32
28 (lt only)
26 (lt only)
DLT Placement
• Prepare and check tube– Ensure cuff inflates and deflates
• Lubricate tube • Insert tube with distal concave curvature facing
anteriorly• Remove stylet once through the vocal cords • Rotate tube 90 degrees (in direction of desired lung) • Advancement of tube ceases when resistance is
encountered. Average lip line is 29 ± 2 cm.
• *If a carinal hook is present, must watch hook go through cords to avoid trauma to them.
DLT Placement
• Check for placement by auscultation• Inflate tracheal cuff- expect equal lung ventilation• Clamp the white side (marked "tracheal" for left-sided tube) and
remove cap from the connector– Expect some left sided ventilation through bronchial lumen, and some
air leak past bronchial cuff, which is not yet inflated
• Slowly inflate bronchial cuff until minimal or no leak is heard at uncapped right connector– Go slow- it only requires 1-3 cc of gas and bronchial rupture is a risk
• Remove the clamp and replace the cap on the tracheal side• Check that both lungs are ventilated• Selectively clamp each side, and expect visible chest movement and
audible breath sounds only on the right when left is clamped, and vice versa
DLT Placement
• Checking tube placement with the fiberoptic bronchoscope• When auscultation maneuvers unreliable preexisting lung disease so
that breath sounds are not very audible, or if the tube is only slightly malpositioned
• In patients with double-lumen tubes whose position seemed appropriate to auscultations, 48% had some degree of malposition. So always check position with fiberoptic if available.
• After advancing the fiberoptic scope thru the “tracheal” tube should see the “bronchial blue balloon” in a semi lunar shape, just peeking out of the bronchus
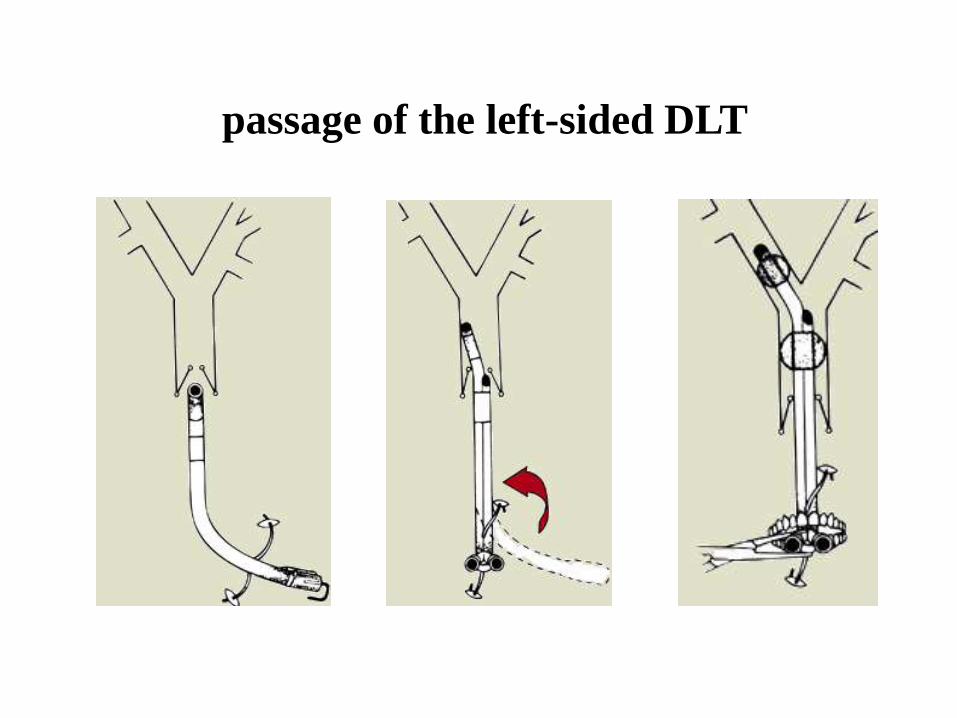
passage of the left-sided DLT
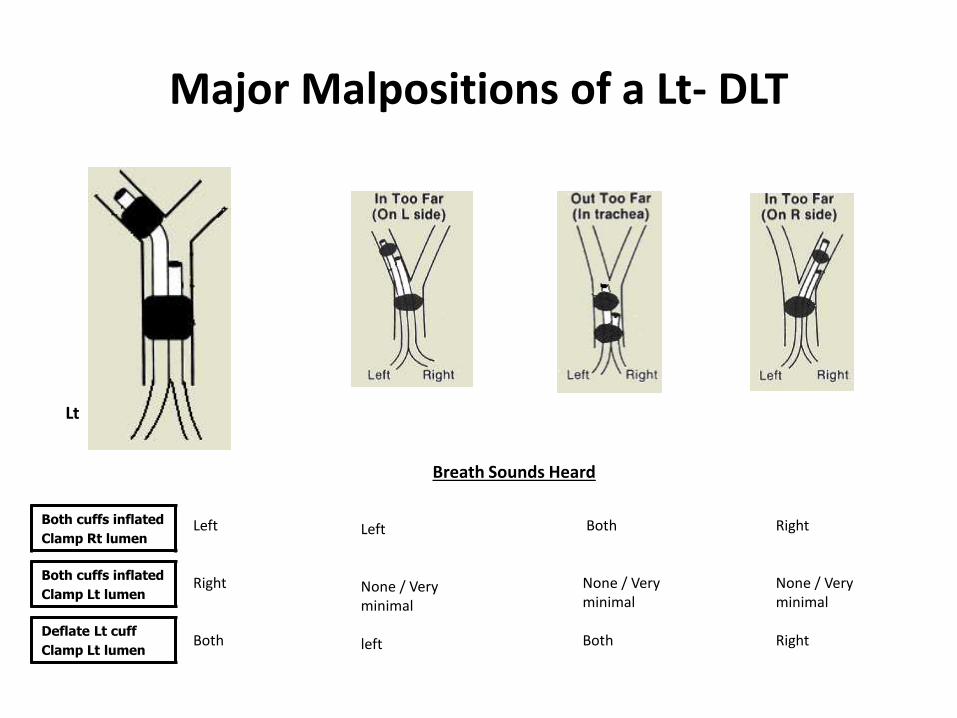
Major Malpositions of a Lt- DLT
Both cuffs inflated
Clamp Rt lumen
Both cuffs inflated
Clamp Lt lumen
Deflate Lt cuff
Clamp Lt lumen
Left
None / Very minimal
left
Left
Right
Both
Both
None / Very minimal
Both
Right
None / Very minimal
Right
Breath Sounds Heard
Lt
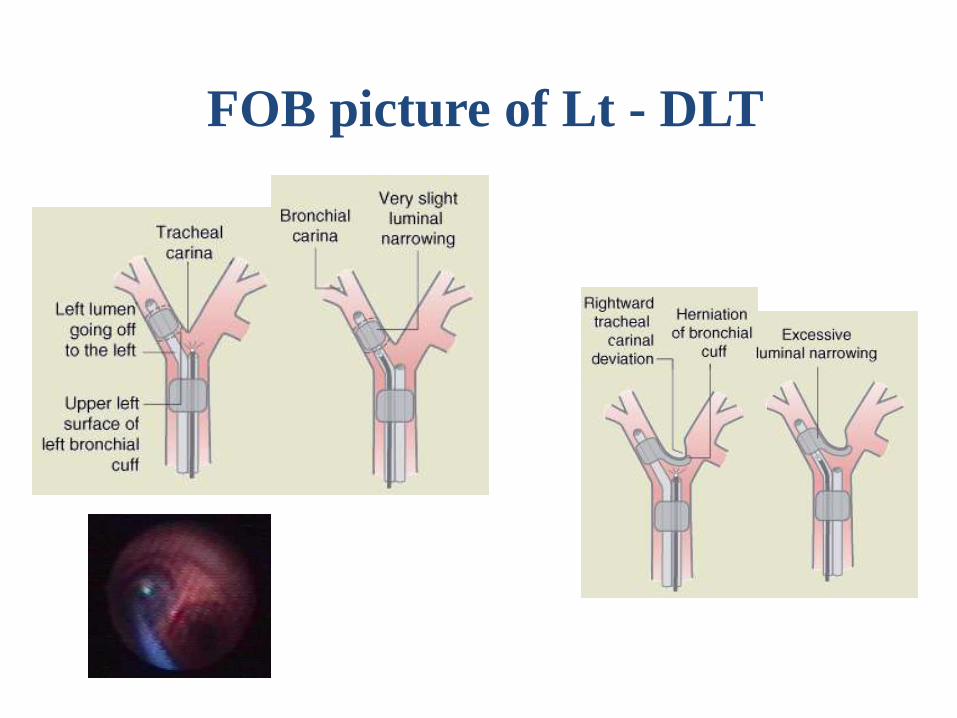
FOB picture of Lt - DLT
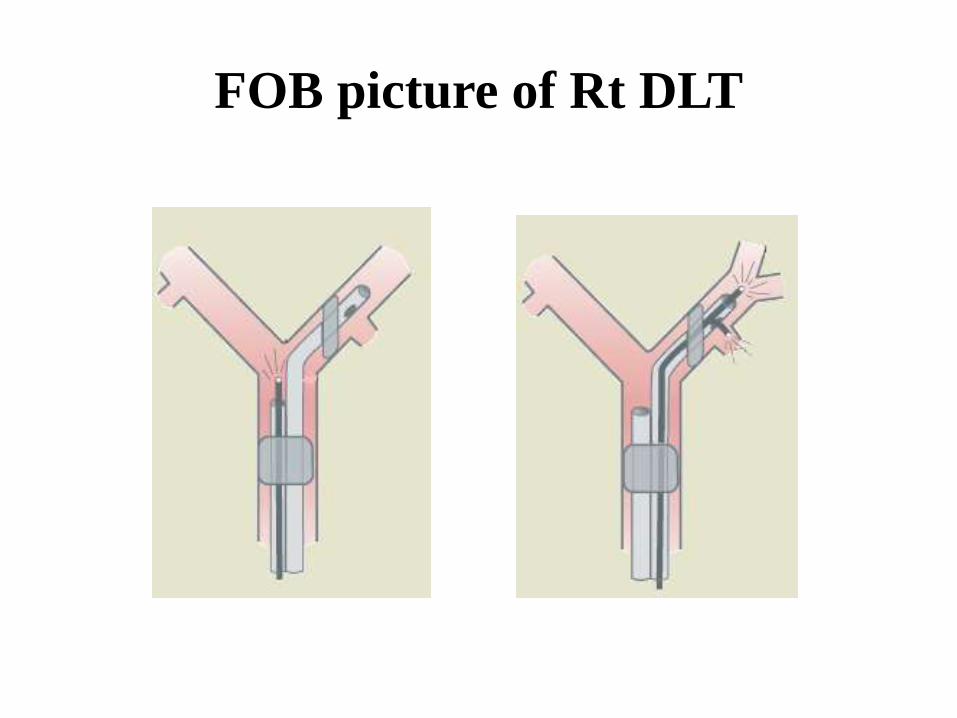
FOB picture of Rt DLT
Other Methods to Check DLT Position
Chest radiograph ;may be more useful than conventional auscultation and clamping in somepatients, but it is always less precise than FOB. The DLT must haveradiopaque markers at the end of Rt and Lt lumina.
Comparison of capnography;
waveform and ETCO2 from each lumen may reveal a marked discrepancy(different degree of ventilation).
Surgeon ;
may be able to palpate, redirect or assist in changing DLT position fromwithin the chest (by deflecting the DLT away from the wrong lung, etc..).
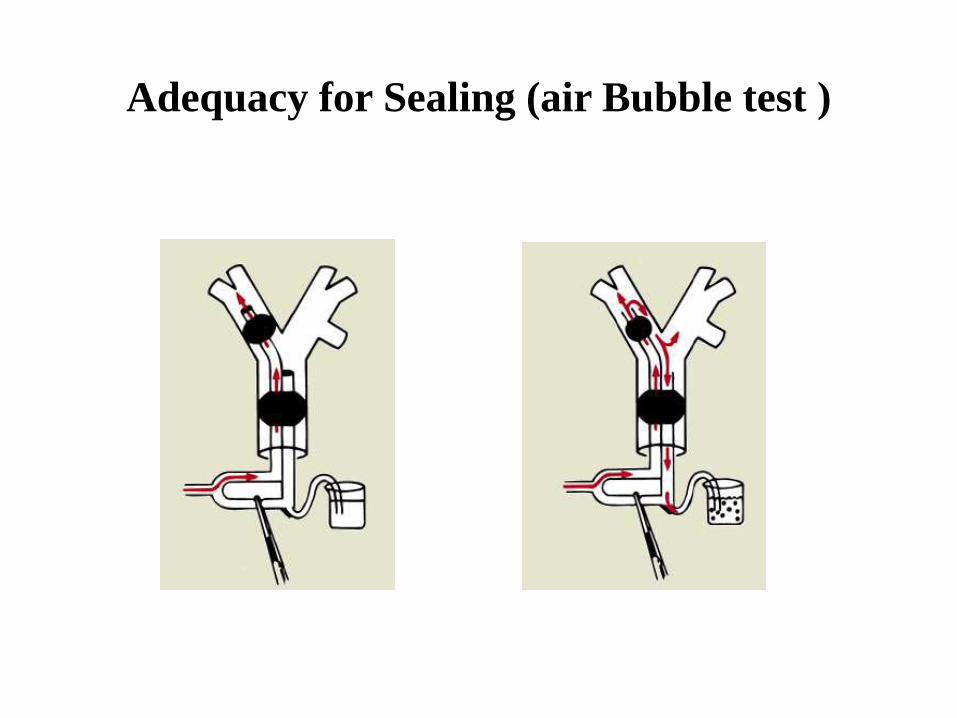
Adequacy for Sealing (air Bubble test )
Indications for a Right-Sided Double-Lumen Tube
Distorted Anatomy of the Entrance of Left Mainstem Bronchus
External or intraluminal tumor compression
Descending thoracic aortic aneurysm
Site of Surgery Involving the Left Mainstem Bronchus
Left lung transplantation
Left-sided tracheobronchial disruption
Left-sided pneumonectomy †
Left-sided sleeve resection
Advantages of DLT
Relatively easy to place
Allows conversion back and forth from OLV to two-lung ventilation
Allows suctioning of both lungs individually
Allows CPAP to be applied to the non-dependent lung
Allow sPEEP to be applied to the dependent lung
Ability to ventilate around scope in the tube
Relative Contraindications to Use of DLT
full stomach (risk of aspiration);
lesion (stricture, tumor) along pathway of DLT (may be traumatized);
small patients;
anticipated difficult intubation;
extremely critically ill patients who have a single-lumen tube already in placeand who will not tolerate being taken off mechanical ventilation and PEEPeven for a short time;
Under these circumstances, it is still possible to separate the lungs by : -using a single-lumen tube + FOB placement of a bronchial blocker ; or FOB placement of a single-lumen tube in a main stem bronchus.
Disadvantages
Size selection more difficult
Difficult to place in patients with difficult airways or abnormal tracheas
Not optimal for postoperative ventilation
Potential laryngeal trauma
Potential bronchial trauma
Clinical Approach to OLV management
Maintain two-lung ventilation until pleura is opened
Check tube after change in position Dependent lung
• FIO2 = 1.0
• VT = 6-8 ml / Kg
• RR , so that PaCO2 ~ 35-40 mmHg
• PEEP = 5 - 10 cmH2O
Frequent recruitment maneuvers
Avoiding fluid overload
?TIVA over inhalational anesthetics
Factors That Correlate with an ↑Risk of Desaturation during One-Lung
Ventilation
• High % of V or Q to operative lung pre-operatively
• Poor PaO2 during 2LV, esp in lat. Position
• Rt sided thoracotomy (lt lung 10% smaller)
• Normal pre-op spirometry or restrictive lung disease
• Supine position during OLV
1. If hypoxaemia occurs
• Check DLT position by FOB/clinically
• Check haemodynamic status
• Non dependent lung CPAP (5 - 10 cmH2O)
• Dependent lung PEEP
• Intermittent two lung ventilation
• Clamp pulmonary artery (pneumonectomy)
Bronchial Blockers(With Single-Lumen Endotracheal Tubes)
Lung separation can be effectively achieved with the use of asingle-lumen endotracheal tube and a FOB placed bronchialblocker.
Often necessary in children as DLTs are too large to be used inthem. The smallest DLT available is a left-sided 26 Fr tube,which may be used in patients 8 -12 years old and weighing25 -35 kg.
Balloon-tipped luminal catheters have the advantage ofallowing suctioning and injection of oxygen down the centrallumen.
Indications for Use of Bronchial Blockers
1st , limitations to DLT (severely distorted airway, small patients ,
anticipated difficult intubation)
2nd , to avoid a risky change of DLT to single-lumen tube• whenever postoperative ventilation is anticipated
• in cases of thoracic spine surgery in which a thoracotomy in the supineor LDP is followed by surgery in the prone position.
3rd , situations in which both lungs may need to be blocked (e.g.,
bilateral operations)
Types of bronchial blockers
Univent bronchial blocker system
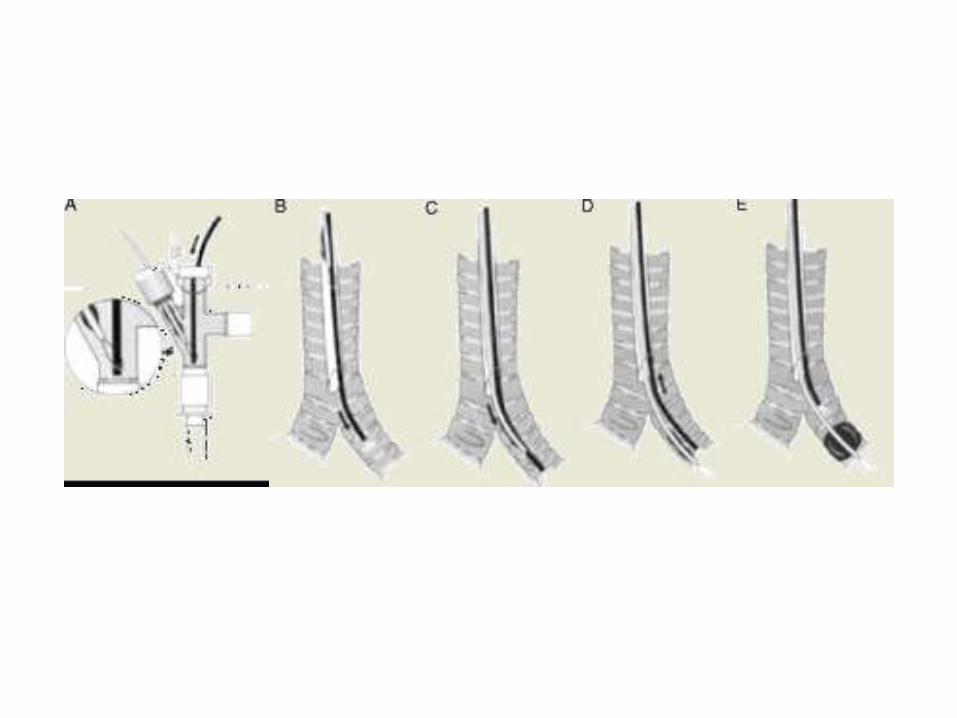
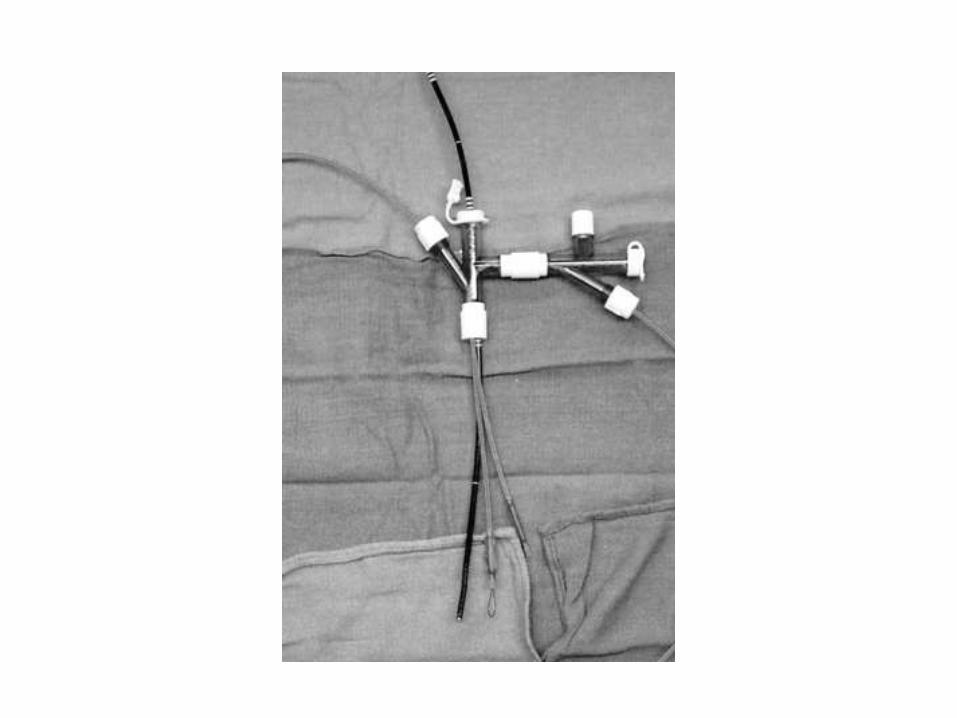
Arndt endobronchial blocker
Cohen Flexitip Endobronchial Blocker
BB independent of a single-lumen tube
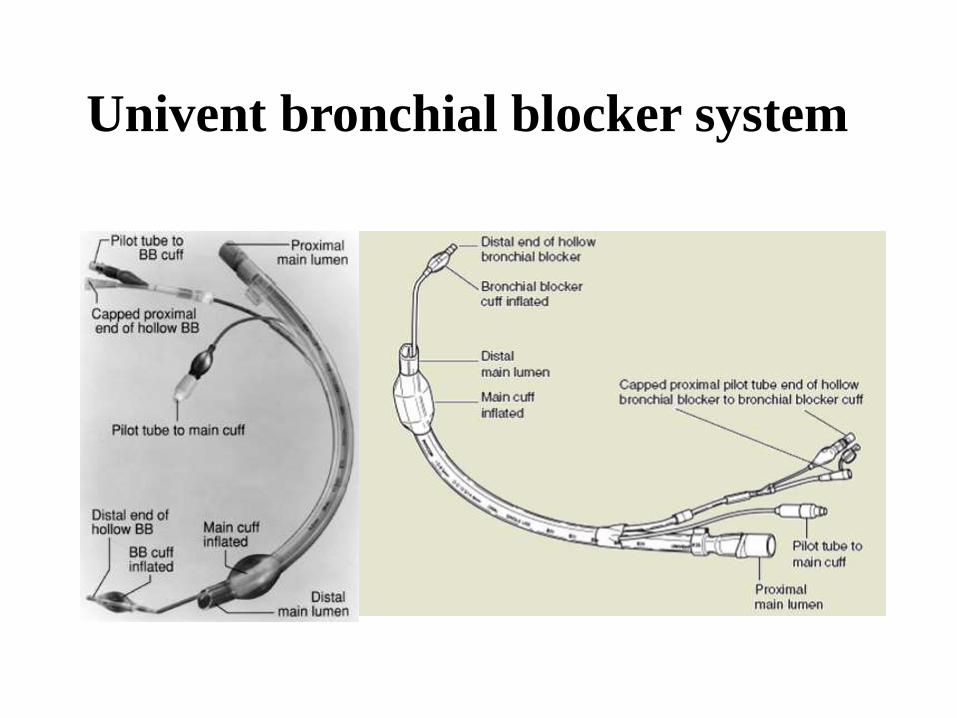
Univent bronchial blocker system
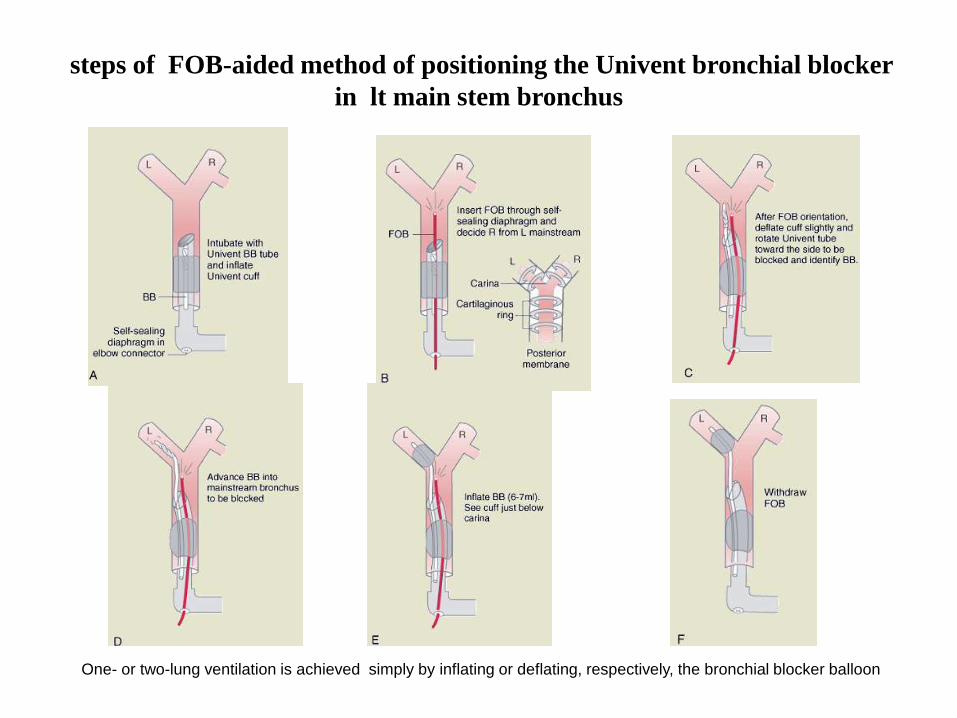
steps of FOB-aided method of positioning the Univent bronchial blocker
in lt main stem bronchus
One- or two-lung ventilation is achieved simply by inflating or deflating, respectively, the bronchial blocker balloon
Advantages of the Univent Bronchial Blocker Tube
( Relative to DLT )
1. Easier to insert and properly position.
2. Can be properly positioned during continuous ventilation and
in the lateral decubitus position.
3. No need to change the tube when turning from the supine to
prone position or for postoperative mechanical ventilation.
4. Selective blockade of some lobes of each lung.
5. Possible to apply CPAP to nonventilated operative lung.
Limitations to the Use of Univent Bronchial Blocker
LIMITATION SOLUTION1. Slow inflation time (a) Deflate BB cuff and administer +ve pressure breath
through the main single lumen;
(b) carefully administer one short high pressure (20–30psi) jet ventilation
2. Slow deflation time (a) Deflate BB cuff and compress and evacuate the lungthrough the main single lumen;
(b) apply suction to BB lumen
3. Blockage of BB lumen
( blood, pus,..)
Suction, stylet, and then suction
4. High-pressure cuff Use just-seal volume of air
5. Leak in BB cuff Make sure BB cuff is subcarinal, increase inflation volume,rearrange surgical field
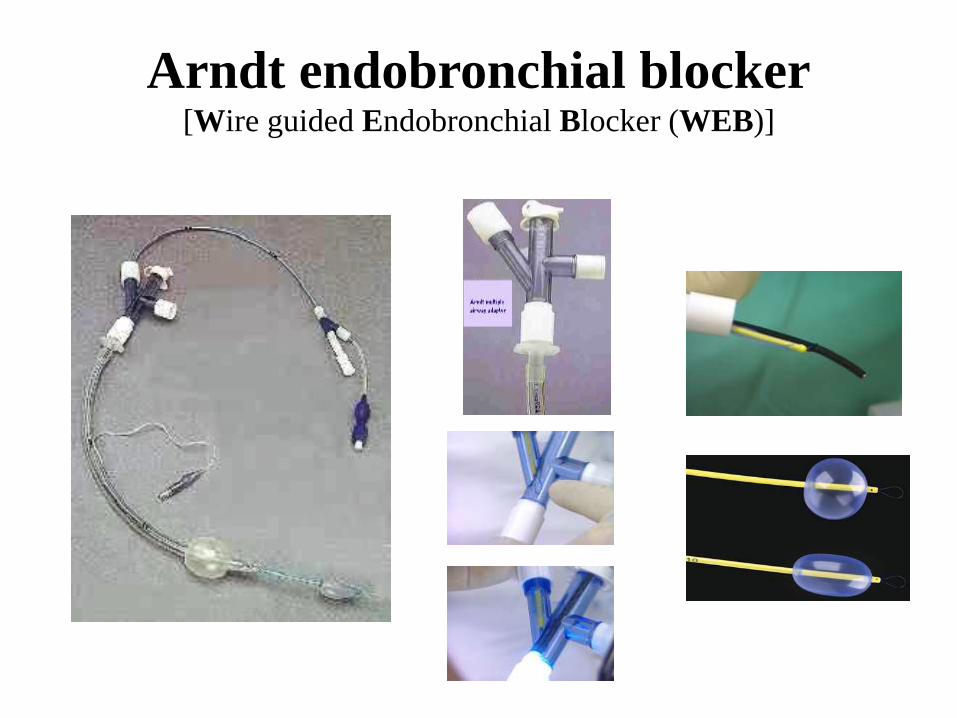
Arndt endobronchial blocker[Wire guided Endobronchial Blocker (WEB)]
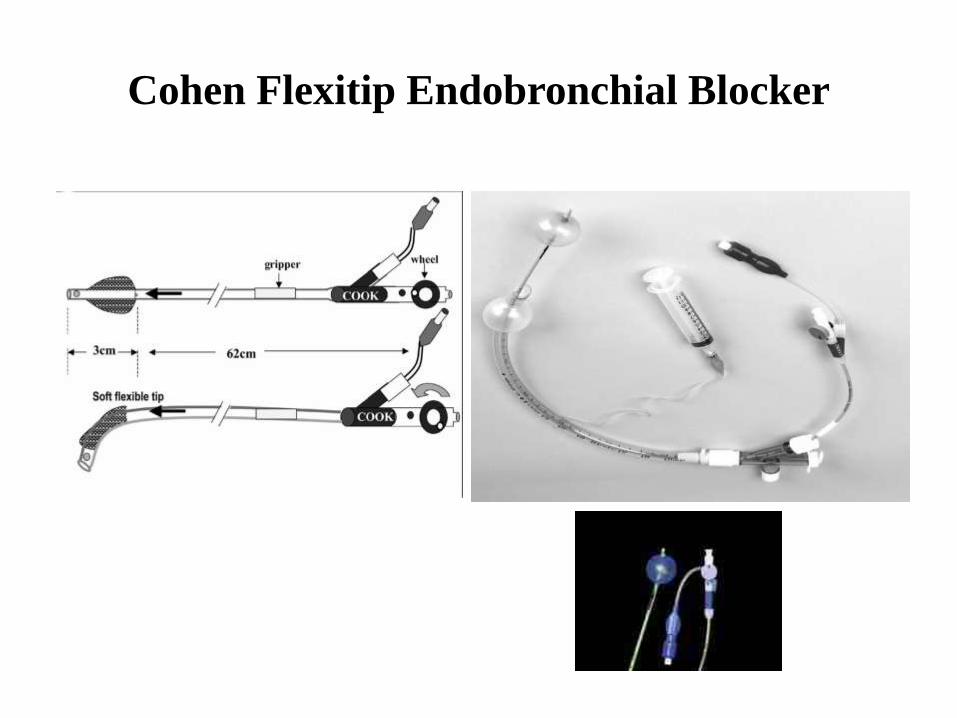
Cohen Flexitip Endobronchial Blocker
Bronchial Blockers that are Independent of a
Single-Lumen Tube
Adults-Fogarty (embolectomy) catheter with a 3 ml balloon.
It includes a stylet so that it is possible to place a curvature at the distal tip to facilitate entry into thelarynx and either mainstem bronchus .
-balloon-tipped luminal catheters (such as Foley type) may be used as bronchial blockers.
Very small children (10 kg or less)- Fogarty catheter with a 0.5 ml balloon
- Swan-Ganz catheter (1 ml balloon)
* these catheters have to be positioned under direct vision; a FOB method is perfectly acceptable; the FOBoutside diameter must be approximately 2 mm to fit inside the endotracheal tube (3 mm internaldiameter or greater).Otherwise, the bronchial blocker must be situated with a rigid bronchoscope.
* Paediatric patients of intermediate size require intermediate size occlusion catheters and judgment onthe mode of placement (i.e., via rigid versus FOB).
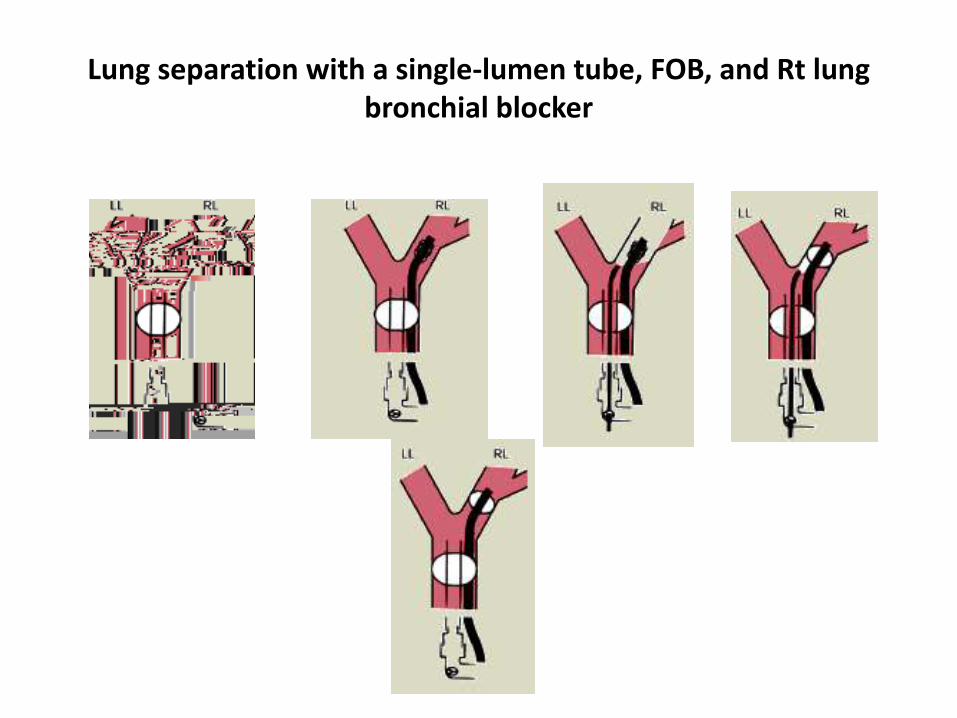
Lung separation with a single-lumen tube, FOB, and Rt lung bronchial blocker
Endobronchial Intubation with Single-Lumen Tubes
In adults, is often the easiest, quickest way for lung separation in patientspresenting with haemoptysis , either
-blind, or
-FOB , or-guidance by surgeon from within chest
In children it may be the simplest way to achieve OLV
Disadvantages-inability to do suctioning or ventilation of operative side.-difficult positioning bronchial cuff with inadequate ventilation of
Rt upper lobe after Rt endobronchial intubation.
Disadvantages of a blocker that is independent of the
single-lumen tube as compared with DLT
inability to suction and/or to ventilate the lung distal to theblocker.
increased placement time.
the definite need for a fiberoptic or rigid bronchoscope.
if bronchial blocker backs out into the trachea, the sealbetween the two lungs will be lost and the trachea will be atleast partially obstructed by the blocker, and ventilation willbe greatly impaired.
Post-operatively
• Non-ventilated lung suctioned and preferentially inflated
• CXR to rule out pneumo/hemothorax, collapse
• High care unit
• Adequate pain relief (thoracic epidural), oxygen/inhaler therapy,