one-bone forearm reconstruction - ganga hospitali able to resume original work. range of motion...
TRANSCRIPT

One-Bone Forearm ReconstructionA Salvage Solution for the Forearm with Massive Bone Loss
Agraharam Devendra, DNB, Purnaganapathi Sundaram Velmurugesan, MS, Jayaramaraju Dheenadhayalan, MS,Hari Venkatramani, MS, MCh, Shanmuganathan Raja Sabapathy, MS, MCh, DNB, FRCS(Ed), FRCS(Glas), MAMS, and
Shanmuganathan Rajasekaran, MS, DNB, FRCS(Ed), MCh(Liv), FRCS(Eng), PhD
Investigation performed at Ganga Hospital, Coimbatore, India
Background: Salvaging the forearm is a major challenge in cases of massive bone loss from injuries in which theextremity is severely mangled or following bone resection secondary to pathological tissue excision. The purpose of thisstudy was to evaluate the role of one-bone forearm (OBF) reconstruction as a salvage option in these difficult situations.
Methods: A total of 38 patients with forearm segmental bone loss (acute and chronic) treated between 1995 and 2014were included (range of follow-up, 2 to 20 years). Sixteen of the patients, 8 with avulsion amputations and 8 with severelymangled extremities, were managed in the emergency department because they required immediate replantation andrevascularization, respectively. In the chronic setting, bone loss was due to infection with nonunion in 16 patients, tumorof the radius in 2 patients, and pseudarthrosis of the forearm in 4 patients. The surgical technique included conversion toOBF by achieving union between the distal part of the radius and the proximal part of the ulna in the majority of cases, withdistal radioulnar joint (DRUJ) fusion in 4 cases, and ulna to carpals in 5 cases. Direct bone contact was achieved in 16patients, a free vascularized fibular graft was used to bridge the bone gap in 10 patients, and 12 patients required iliaccrest bone-grafting.
Results: The mean patient age was 35.5 years (range, 6 to 87 years); there were 23 male and 15 female patients.Among those who underwent OBF for acute injuries, the mean time to union was 7.3 months; 14 patients had completeunion, and 2 patients had infection with nonunion requiring secondary procedures. As assessed using the criteria of Chen,10 patients had a grade-I functional outcome, 3 patients had a grade-II outcome, and 3 patients had a grade-III outcome. Inthe elective group of 22 patients, the average time to union was 7.1months. Nonunion was reported for 2 patients. On thebasis of the Peterson scoring system, the outcome was excellent for 12 patients, good for 6 patients, fair for 2 patients,and poor for 2 patients.
Conclusions: OBF reconstruction is a viable surgical treatment alternative. It is a demanding reconstruction but func-tions better and is cosmetically more appealing than a forearm amputation.
Level of Evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.
The forearm is unique in its anatomy, with the radiusand ulna and associated articulations including thehumeroulnar joint, the proximal and distal radioulnar
joints, the radiocarpal joint, and the interosseous membrane.The relative length of both the radius and ulna is important forproper functioning of the forearm1,2. A fracture of 1 or bothbones of the forearm may be an intra-articular fracture, withanatomical reduction required to restore normal function.Standard skeletal fixation methods may not be possible inreplantation and revascularization scenarios for a mangled
upper extremity or an avulsion amputation. In addition to theproblems of soft-tissue and bone loss, ischemic time related tovascular injury is also very important3-7. Despite the latestadvances in microsurgical techniques, salvage in cases of thesemajor injuries is a challenge, and, to our knowledge, there areno standard techniques described for reconstruction withmajor bone loss in the forearm8. We also are not aware of anyscoring system that has been described for mutilating injuriesof the upper limb with vascular injuries that can be used topredict salvage and functional outcome9,10.
Disclosure: The authors report support for manuscript preparation from the Ganga Orthopaedic Research Education Foundation (GOREF), Coimbatore,India during the conduct of this study. The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJS/F329).
e74(1)
COPYRIGHT � 2019 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2019;101:e74(1-12) d http://dx.doi.org/10.2106/JBJS.18.01235

Fig. 1
Figs. 1-A through 1-J Case example of a 50-year-old man who sustained a mid-forearm-level avulsion amputation following a machine injury
(Figs. 1-B and 1-C) andwas treatedwith one-bone forearm reconstruction. Radiographs (Figs. 1-A and 1-D) show a radial head dislocationwith a segmental
fracture of the ulna. Shortening of existing bones was required for direct end-to-end anastomosis of both vessels and nerves after debridement. Hence the
radius to ulna was fixed with adequate shortening, good osseous contact, and a stable forearm was achieved (Figs. 1-E and 1-F). The patient had a grade-I
outcome by the criteria of Chen, with the longest follow-up in our series (20 years) and no complications (Figs. 1-G through 1-J).
e74(2)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

Fig. 2
A 23-year-old man sustained a severe crushing injury to the left upper limb (Figs. 2-A and 2-B). Fixation between the proximal part of the ulna and the distal
part of the radius was chosen as there was segmental fracture of both the ulna and the radius, and the patient presented with polytrauma. He had an open-
book pelvic injury, severe hypovolemic shock, and vascular injury to the forearm as well. Here, immediate fixation was important for salvage, and thus, one-
bone forearm reconstruction was chosen (Figs. 2-C and 2-D). The patient improved and has resumed to his pre-injury profession of tailoring without any
complications (Figs. 2-E, 2-F, and 2-G).
e74(3)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

The management of chronic osteomyelitis and non-union of the forearm with infection following open fractureor surgical site infection is very difficult11. Initially, aggres-sive debridement and the removal of devitalized tissues andany previous implant may be performed to control infection,which may result in segmental bone loss. Composite soft-tissue and bone loss, scar adherence, and poor skin condi-tion due to prior multiple surgeries together pose a greatchallenge in reconstruction of the forearm. Functionaloutcomes following treatment of these injuries are highlyunpredictable12-14.
One-bone forearm (OBF) reconstruction is a viableoption in these challenging situations to salvage the limb and toachieve good stability and a functional forearm13-17. The termone-bone forearm was first described in 1921 by Hey-Groves18,who performed a procedure resulting in radioulnar synostosisfor failed bone-grafting in distal radial nonunion. Subsequently
many authors have described OBF reconstruction for variousclinical scenarios, such as posttraumatic bone loss, tumorresection, and congenital deformities; with OBF reconstruc-tion, the proximal part of the ulna typically is fixed to the distalpart of the radius13-17,19-25. As described by Vitale, “the ulna
Fig. 3
A case of infection with nonunion and segmental bone loss of the radius following open reduction and plating of a closed forearm fracture
(Fig. 3-A). Debridement and external fixation followed by distraction was initiated (Fig. 3-B). Once the length of the radius was achieved, one-bone forearm
reconstruction by distal radioulnar joint (DRUJ) fusion using cancellous screws was performed (Fig. 3-C). The final radiograph shows complete union
(Fig. 3-D). Photographs demonstrate a stable forearm (Figs. 3-E and 3-F).
TABLE I Types of One-Bone Forearm (OBF) Reconstruction inthe Elective Group
OBF Type No. of Patients
Plate osteosynthesis of the proximal part ofthe ulna and the distal part of the radius
9
Free vascularized fibular reconstruction 9
Distal radioulnar arthrodesis 2
Ulnocarpal fusion 2
e74(4)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

‘makes’ the elbow; the radius ‘makes’ the wrist,” meaning thatthe ulna as a distal extension of the arm is important for elbowfunction, and the radius as a proximal extension of the hand isimportant for radiocarpal function26.
In this study, we present the largest series, to ourknowledge, of patients treated with OBF reconstruction. Theobjective of this study was to analyze the role of OBF recon-struction as a salvage option in difficult clinical situations.
Materials and Methods
Atotal of 38 patients treated with OBF reconstructionbetween 1995 and 2014 were included in our retrospective
analysis. The mean patient age was 35.5 years (range, 6 to 87years; 23 males and 15 females). The right, dominant side wasinvolved in 19 patients and the left, nondominant side wasinvolved in an equal number of patients (19). The minimumfollow-up was 2 years, and the maximum follow-up was 20years.
The group treated for acute injuries in the emergencydepartment consisted of 16 patients: 8 presented with avulsionamputations requiring replantation and the other 8 hadseverely mangled extremities requiring revascularization. Themost common mechanism of injury, experienced by 11patients, was a work-related machine injury; 4 patients had aroad traffic accident, and 1 patient sustained a blast injury.
The group treated electively consisted of 22 patients: 16had nonunion of the forearm with infection, 2 had a tumor ofthe radius, and 4 had pseudarthrosis of the forearm. Of the 16patients with infection, 1 had chronic osteomyelitis of the ulnawith segmental bone loss, 13 presented with postoperativeinfection following internal fixation of fractures involving bothbones of the forearm, 1 presented with infection after replan-tation following traumatic amputation of the forearm, and1 presented with infection with nonunion and Volkmann
ischemic contracture of the forearm following local bonesettertreatment. In 3 patients, the radius only was involved; in1 patient, the ulna only; and in 18 patients, both the radius andthe ulna were involved.
Direct bone contact was achieved in 16 patients, a freevascularized fibular graft was used to bridge the bone gap in 10patients, and 12 patients required iliac crest bone-grafting.
Surgical TechniqueAcute Injury GroupOf the 16 patients in the acute injury group, 14 underwent OBFreconstruction by immediate plating between the ulna andradius, chiefly, the proximal part of the ulna and distal part ofthe radius (Figs. 1 and 2). This surgical strategy was chosenbecause of segmental bone loss and difficulty in fixation of eachbone due to comminution; the goal was primary osseous unionwith adequate osseous contact. Two patients with major boneloss involving the radius underwent late reconstruction withulnocarpal fusion with a free vascularized fibular graft anddistal radioulnar joint (DRUJ) fusion, respectively. Both patientshad polytrauma and underwent initial damage-control surgeriesfollowed by late reconstruction.
The position of the distal part of the reconstructedforearm and the hand was chosen to be in full supination forthe 8 patients with involvement of the dominant side and in 10�of pronation for the remaining 8 patients with involvement ofthe nondominant side.
Elective GroupOBF reconstruction was chosen as a salvage solution for thepatients in the elective group. When the distance between theproximal part of the ulna and distal part of the radius was ‡6cm, a free vascularized fibular graft was used to bridge the gap.In patients with bone loss of <6 cm, bone-grafting was per-formed. DRUJ fusion with cancellous screws was performed inpatients with only radial diaphyseal bone loss (Fig. 3, Table I).
The position of the distal part of the reconstructedforearm and the hand was chosen to be in full supination forthe 11 patients with involvement of the dominant side and in10� of pronation for the remaining 11 patients with involve-ment of the nondominant side. The mean number of surgicalprocedures that patients underwent prior to conversion to OBFreconstruction was 1.72 (range, 0 to 5 procedures).
ResultsAcute Injury Group
In the acute injury group, 14 patients achieved primaryosseous union. Shortening of osseous ends on either side
is required to facilitate primary repair of vessels and nerves.Among the 8 patients who underwent replantation, themean shortening of the forearm when compared with thecontralateral side was 7.1 cm (range, 6 to 8 cm), and amongthe 8 patients who required revascularization, it was 4.8 cm(range, 0 to 8 cm). Two patients had infection with non-union and required secondary procedures to achieve osseousunion. Among all 16 patients, the mean time to union was
TABLE II Chen Criteria of Functional Outcome in Patients withReplantation and Revascularization*
Grade Function
I Able to resume original work.Range of motion exceeds 60% of normal.Complete or nearly complete recovery of sensibility.Muscle power of Grades 4 and 5
II Able to resume some suitable work.Range of motion exceeds 40% of normal.Nearly complete sensibility.Muscle power of Grades 3 and 4
III Able to carry out activities of daily life.Range of motion exceeds 30% of normal.Partial recovery of sensibility.Muscle power of Grade 3
IV Almost no usable functions of surviving limb
*Modified by permission from: Springer Nature. World J Surg.Extremity replantation. Chung-Wei C, Yun-Qing Q, Zhong-Jia Y.COPYRIGHT 1978.
e74(5)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION
7.3 months (range, 4 to 18 months). All had improvement inpower and function with the progressive use of the upperextremity.
Functional outcome was measured by the Disabilities ofthe Arm, Shoulder and Hand (DASH) score. The mean DASHscore was 12.8 (range, 1.7 to 33.3). On the basis of the Chencriteria27 (Table II), functional outcome was classified as grade Iin 10 patients, as grade II in 3 patients, and as grade III in 3patients. No patient had a grade-IV result or required sec-ondary amputation. The mean range of motion of the wristjoint achieved actively was 21.8� of palmar flexion, 15� ofextension, 9.3� of radial deviation, and 13.4� of ulnar deviation.The elbow range of motion was almost full in both flexion andextension for all patients (0� to 135�). However, no supination-pronation movements were possible. The pain level in theforearm at rest and during work was assessed with use of avisual analog scale (VAS). Eleven patients had no pain and 5patients had mild pain at rest. Seven patients had no pain and 9patients experienced mild pain during exertion involving thehand.
Dynamometric mean grip strength was 6.4 kg (range, 2to 11 kg) on the affected side and 32.4 kg (range, 20 to 42 kg) onthe unaffected side. Sensory examination on the affected side(both static and dynamic) showed that 2-point discriminationwas normal (2 to 6 mm) in 4 patients, fair (7 to 10 mm) in 3patients, and poor (11 to 15 mm) in 4 patients, with 5 patientsregaining protective (1-point perception) sensation. Cold-intolerance evaluation subjectively showed that only 4 patients
had little and 2 patients had intermediate cold intolerance. Theremaining 10 patients reported no intolerance to cold. Twelvepatients expressed that they were very satisfied with the cos-mesis of their forearm after reconstruction. While 3 patientssaid they were somewhat satisfied, only 1 patient was neithersatisfied nor dissatisfied with the forearm cosmesis.
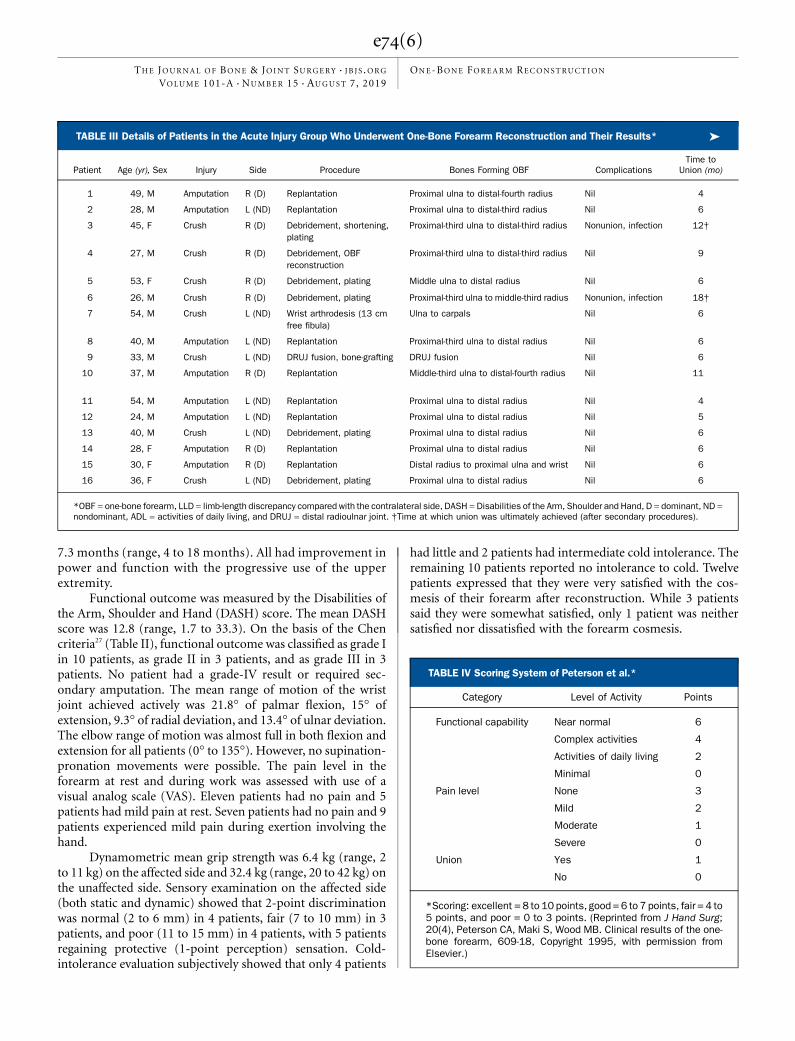
TABLE III Details of Patients in the Acute Injury Group Who Underwent One-Bone Forearm Reconstruction and Their Results* �
Patient Age (yr), Sex Injury Side Procedure Bones Forming OBF ComplicationsTime to
Union (mo)
1 49, M Amputation R (D) Replantation Proximal ulna to distal-fourth radius Nil 4
2 28, M Amputation L (ND) Replantation Proximal ulna to distal-third radius Nil 6
3 45, F Crush R (D) Debridement, shortening,plating
Proximal-third ulna to distal-third radius Nonunion, infection 12†
4 27, M Crush R (D) Debridement, OBFreconstruction
Proximal-third ulna to distal-third radius Nil 9
5 53, F Crush R (D) Debridement, plating Middle ulna to distal radius Nil 6
6 26, M Crush R (D) Debridement, plating Proximal-third ulna to middle-third radius Nonunion, infection 18†
7 54, M Crush L (ND) Wrist arthrodesis (13 cmfree fibula)
Ulna to carpals Nil 6
8 40, M Amputation L (ND) Replantation Proximal-third ulna to distal radius Nil 6
9 33, M Crush L (ND) DRUJ fusion, bone-grafting DRUJ fusion Nil 6
10 37, M Amputation R (D) Replantation Middle-third ulna to distal-fourth radius Nil 11
11 54, M Amputation L (ND) Replantation Proximal ulna to distal radius Nil 4
12 24, M Amputation L (ND) Replantation Proximal ulna to distal radius Nil 5
13 40, M Crush L (ND) Debridement, plating Proximal ulna to distal radius Nil 6
14 28, F Amputation R (D) Replantation Proximal ulna to distal radius Nil 6
15 30, F Amputation R (D) Replantation Distal radius to proximal ulna and wrist Nil 6
16 36, F Crush L (ND) Debridement, plating Proximal ulna to distal radius Nil 6
*OBF = one-bone forearm, LLD = limb-length discrepancy compared with the contralateral side, DASH =Disabilities of the Arm, Shoulder and Hand, D = dominant, ND =nondominant, ADL = activities of daily living, and DRUJ = distal radioulnar joint. †Time at which union was ultimately achieved (after secondary procedures).
TABLE IV Scoring System of Peterson et al.*
Category Level of Activity Points
Functional capability Near normal 6
Complex activities 4
Activities of daily living 2
Minimal 0
Pain level None 3
Mild 2
Moderate 1
Severe 0
Union Yes 1
No 0
*Scoring: excellent = 8 to 10 points, good = 6 to 7 points, fair = 4 to5 points, and poor = 0 to 3 points. (Reprinted from J Hand Surg;20(4), Peterson CA, Maki S, Wood MB. Clinical results of the one-bone forearm, 609-18, Copyright 1995, with permission fromElsevier.)
e74(6)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

Eleven patients had returned to their pre-injury occu-pation of manual work. While 2 patients changed their workto suitable light work, 3 patients could not return to theiroriginal manual work and could do only household ac-tivities of daily living (ADL). Among the 8 patients withdominant-side involvement, 4 had returned to their originalwork, 1 had changed to suitable light work, and 3 could doonly ADL. Of those with nondominant-side involvement,7 returned to their pre-injury work, and 1 patient had tochange to suitable light work. The poor result for 2 patientsin this acute injury group was mostly due to infection andnonunion of the OBF fixation site in addition to only partialrecovery of motor and sensory function. No patient usedany kind of external support at the time of final follow-up(Table III).
Elective GroupOf the 16 patients in the elective group who had infectionwith nonunion prior to the OBF procedure, complete unionfollowing reconstruction was achieved in 15 patients withoutany need for secondary procedures. In 1 patient, union wasnot achieved; the patient experienced infection of the freefibular graft and anastomosis failure. She underwentdebridement, graft removal, and control of infection fol-lowed by shortening and plating of the proximal part of theulna to the distal part of the ulna with DRUJ fusion. Themean time to union among all 16 patients was 6 months(range, 4 to 8 months).
Among the 6 patients in the elective group withoutinfection, 5 achieved union following the OBF procedure. One
patient did not initially heal: a young male patient with oste-ogenesis imperfecta with deformity of the forearm; he required2 revision procedures to achieve osseous union. In the patientswithout infection, the mean time to union was 10.2 months(range, 3 to 24 months).
Among the patients without infection in the electivegroup, the mean shortening of the limb when compared withthe contralateral side was 2.3 cm (range, 1 to 6 cm), and amongthose with infection, it was 1.8 cm (range, 1 to 8 cm). Amongall patients in the elective group, the elbow and shoulder jointshad unrestricted range of motion. The mean wrist palmarflexion was 30.5� and extension was 22�, and 10� of radial andulnar deviation were present. The mean DASH score was 10.9(range, 0.8 to 50.8), with a lower score indicating a betteroutcome.
Of the 22 patients in the elective group, 12 had anexcellent outcome, 6 had a good outcome, 2 had a fair outcome,
TABLE III (continued)
LLD (cm)Distal OBF
Position of HandChen
OutcomeDASHScore
Grip Strength:Affected Limb (kg)
Grip Strength:Unaffected Limb (kg)
Cosmesis ofForearm
Return to OriginalOccupation
6.5 Full supination Grade I 12.5 7.5 30 Very satisfied Yes (manual)
8 10� pronation Grade I 5 5.25 38 Very satisfied Yes (manual)
8 Full supination Grade III 32.3 9.5 40 Somewhat satisfied No, only ADL
5 Full supination Grade I 2.8 7 34 Very satisfied Yes (manual)
4.5 Full supination Grade I 9.2 2 20 Very satisfied Yes (manual)
6 Full supination Grade III 32.6 7 28 Somewhat satisfied No, only ADL
2 10� pronation Grade II 12.3 2.5 36 Somewhat satisfied Suitable light work
7.5 10� pronation Grade I 4.3 3.5 30.7 Very satisfied Yes (manual)
Nil 10� pronation Grade I 1.7 11 40 Very satisfied Yes (manual)
6 Supination Grade III 33.3 7.25 35 Neither satisfied nordissatisfied
No, only ADL
7 10� pronation Grade I 12 4 30 Very satisfied Yes (manual)
6.5 10� pronation Grade I 8.6 7.2 22 Very satisfied Yes (manual)
6 10� pronation Grade II 13.3 6 28 Very satisfied Yes (manual)
8 Supination Grade I 8.1 10.5 35 Very satisfied Yes (manual)
7.5 Supination Grade II 11 8 42 Very satisfied Suitable light work
7 10� pronation Grade I 5.6 4 30 Very satisfied Yes (manual)
TABLE V Mean Functional Outcome Score in the ElectiveGroup*
Grading No. of Patients Mean Score
Excellent 12 8.5
Good 6 6.4
Fair 2 5
Poor 2 2.5
*Based on the scoring system of Peterson et al.14.
e74(7)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

and 2 had a poor functional outcome on the basis of the scoringsystem of Peterson et al.14 (Tables IV and V).
A segmental bone defect of the forearm of >6 cm wastreated by free vascularized fibular graft in 9 patients. Themean length of the bone defect was 11 cm (range, 8 to 15 cm).As noted above, 1 patient had infection of the fibula thatrequired removal of the graft and secondary procedures. Oneadditional patient had nonunion of the graft-host junctiondistally at the wrist arthrodesis. However, at the time ofwriting, no further procedure had been performed as thepatient was asymptomatic. The skin island flap of the fibulargraft, which is helpful for monitoring the viability of thefibular graft, showed necrosis requiring debridement; how-
ever, graft union was achieved without any further interven-tion (Tables VI and VII).
Fourteen patients had returned to their original occu-pation comfortably, and all manual work included weightlifting. Three patients could not return to pre-injury work andwere able to perform only ADL, and 5 patients needed tomodify their original work and could do only suitable lightwork. When considering only the patients with injury to thedominant limb, 9 patients returned to their original occupation(1 with modification), whereas 1 patient changed to suitablelight work and another patient could perform only ADL.
Infection and nonunion were the main reasons for thepoor result in 2 patients requiring multiple procedures. A fair
TABLE VI Details of Patients in the Elective Group with Infection Who Underwent One-Bone Forearm (OBF) Reconstruction andTheir Results*
�
PatientAge (yr),Sex Side Diagnosis Procedure Bones Forming OBF
No. of ProceduresBefore OBF
1 6, F L (ND) Post-infection bone loss Debridement, OBF Proximal-third ulna to distalradius
2
2 16, F L (ND) VIC, infection with nonunion Debridement, OBF withfree fibula
Proximal- third ulna withwrist arthrodesis
1
3 20, M R (D) Infection with nonunion Excision of sequestratedradius, OBF with freefibula
Proximal- third ulna to distalradius
0
4 11, F R (D) Infection with nonunion Debridement, OBF withfree fibula
Proximal- third ulna to distal-third radius
1
5 37, F L (ND) Infection with nonunion OBF with free fibula Proximal-third ulna to distal-fourth radius
2
6 38, F R (D) Infection with nonunion OBF with free fibula Proximal-third ulna to distalradius
1
7 44, M R (D) Infection with nonunion OBF with free fibula Proximal-third ulna to distal-third radius
1
8 28, F L (ND) Infection with nonunion OBF with free fibula,DRUJ fusion
Ulnar plating with DRUJfusion
3
9 32, F L (ND) Infection followingreplantation
OBF with bone-grafting,plating
Proximal ulna to distal radius 1
10 55, M L (ND) Infection with nonunion OBF with free fibula Proximal ulna to distal radius 3
11 30, M R (D) Infection with nonunion OBF Distal radius to proximalulna and wrist fusion
5
12 70, F L (ND) Infection with nonunion OBF Distal radius to proximalulna
3
13 22, M R (D) Infection with nonunion OBF Distal radius to proximalulna
2
14 54, M R (D) Infection with nonunion Initial resection followedby OBF
Distal radius to proximalulna and wrist arthrodesis
5
15 18, M L (ND) Malunited distal radius withulnar osteomyelitis
OBF, ulnocarpalarthrodesis
Ulna to carpals 1
16 62, M L (ND) Malunited distal radialfracture with DRUJsubluxation with infection
OBF, wrist arthrodesiswith bone-grafting
Ulna to carpals 1
*DASH = Disabilities of the Arm, Shoulder and Hand, LLD = limb-length discrepancy compared with the contralateral side, ND = nondominant, D =dominant, VIC= Volkmann ischemic contracture, DRUJ= distal radioulnar joint, and ADL= activities of daily living. †Time at which union was ultimatelyachieved (following revision).
e74(8)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION
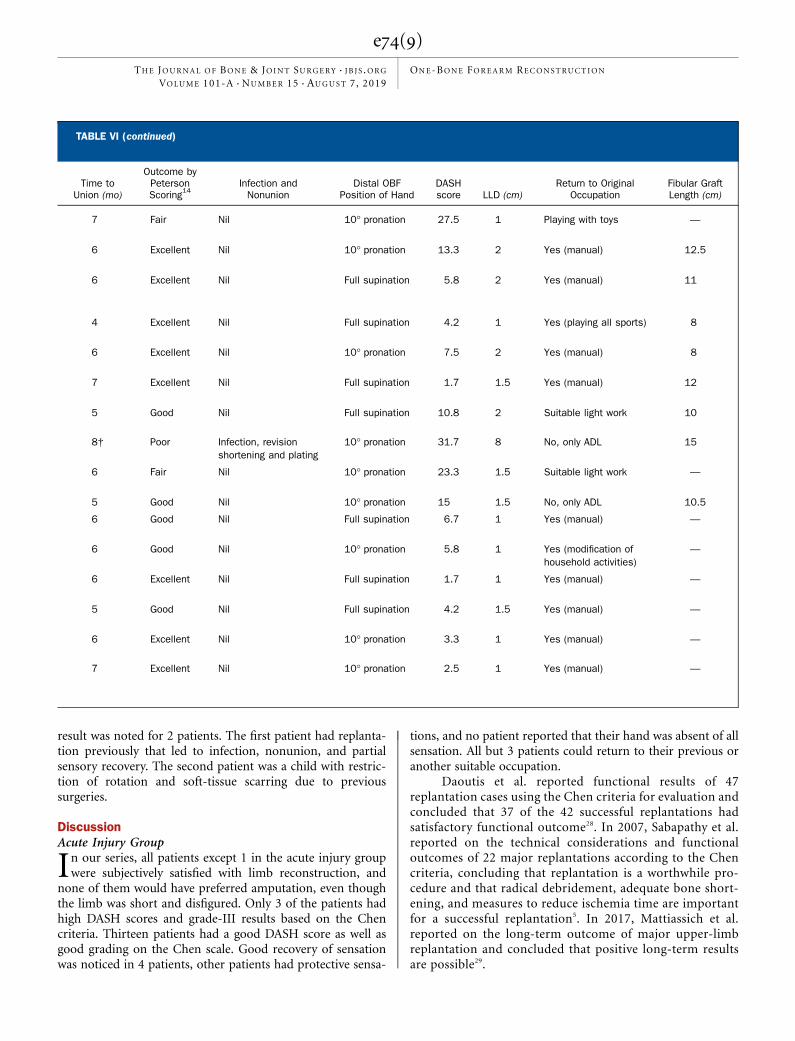
result was noted for 2 patients. The first patient had replanta-tion previously that led to infection, nonunion, and partialsensory recovery. The second patient was a child with restric-tion of rotation and soft-tissue scarring due to previoussurgeries.
DiscussionAcute Injury Group
In our series, all patients except 1 in the acute injury groupwere subjectively satisfied with limb reconstruction, and
none of them would have preferred amputation, even thoughthe limb was short and disfigured. Only 3 of the patients hadhigh DASH scores and grade-III results based on the Chencriteria. Thirteen patients had a good DASH score as well asgood grading on the Chen scale. Good recovery of sensationwas noticed in 4 patients, other patients had protective sensa-
tions, and no patient reported that their hand was absent of allsensation. All but 3 patients could return to their previous oranother suitable occupation.
Daoutis et al. reported functional results of 47replantation cases using the Chen criteria for evaluation andconcluded that 37 of the 42 successful replantations hadsatisfactory functional outcome28. In 2007, Sabapathy et al.reported on the technical considerations and functionaloutcomes of 22 major replantations according to the Chencriteria, concluding that replantation is a worthwhile pro-cedure and that radical debridement, adequate bone short-ening, and measures to reduce ischemia time are importantfor a successful replantation5. In 2017, Mattiassich et al.reported on the long-term outcome of major upper-limbreplantation and concluded that positive long-term resultsare possible29.
TABLE VI (continued)
Time toUnion (mo)
Outcome byPetersonScoring14
Infection andNonunion
Distal OBFPosition of Hand
DASHscore LLD (cm)
Return to OriginalOccupation
Fibular GraftLength (cm)
7 Fair Nil 10� pronation 27.5 1 Playing with toys —
6 Excellent Nil 10� pronation 13.3 2 Yes (manual) 12.5
6 Excellent Nil Full supination 5.8 2 Yes (manual) 11
4 Excellent Nil Full supination 4.2 1 Yes (playing all sports) 8
6 Excellent Nil 10� pronation 7.5 2 Yes (manual) 8
7 Excellent Nil Full supination 1.7 1.5 Yes (manual) 12
5 Good Nil Full supination 10.8 2 Suitable light work 10
8† Poor Infection, revisionshortening and plating
10� pronation 31.7 8 No, only ADL 15
6 Fair Nil 10� pronation 23.3 1.5 Suitable light work —
5 Good Nil 10� pronation 15 1.5 No, only ADL 10.5
6 Good Nil Full supination 6.7 1 Yes (manual) —
6 Good Nil 10� pronation 5.8 1 Yes (modification ofhousehold activities)
—
6 Excellent Nil Full supination 1.7 1 Yes (manual) —
5 Good Nil Full supination 4.2 1.5 Yes (manual) —
6 Excellent Nil 10� pronation 3.3 1 Yes (manual) —
7 Excellent Nil 10� pronation 2.5 1 Yes (manual) —
e74(9)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION
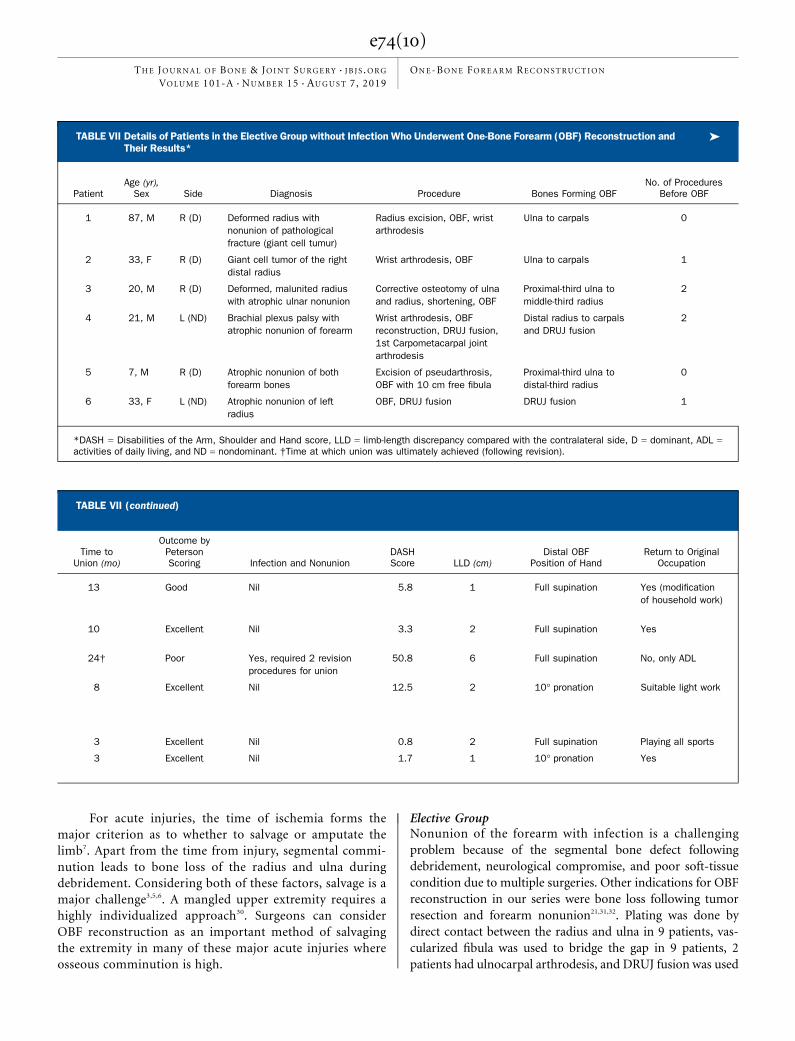
For acute injuries, the time of ischemia forms themajor criterion as to whether to salvage or amputate thelimb7. Apart from the time from injury, segmental commi-nution leads to bone loss of the radius and ulna duringdebridement. Considering both of these factors, salvage is amajor challenge3,5,6. A mangled upper extremity requires ahighly individualized approach30. Surgeons can considerOBF reconstruction as an important method of salvagingthe extremity in many of these major acute injuries whereosseous comminution is high.
Elective GroupNonunion of the forearm with infection is a challengingproblem because of the segmental bone defect followingdebridement, neurological compromise, and poor soft-tissuecondition due to multiple surgeries. Other indications for OBFreconstruction in our series were bone loss following tumorresection and forearm nonunion21,31,32. Plating was done bydirect contact between the radius and ulna in 9 patients, vas-cularized fibula was used to bridge the gap in 9 patients, 2patients had ulnocarpal arthrodesis, and DRUJ fusion was used
TABLE VII Details of Patients in the Elective Group without Infection Who Underwent One-Bone Forearm (OBF) Reconstruction andTheir Results*
�
PatientAge (yr),Sex Side Diagnosis Procedure Bones Forming OBF
No. of ProceduresBefore OBF
1 87, M R (D) Deformed radius withnonunion of pathologicalfracture (giant cell tumur)
Radius excision, OBF, wristarthrodesis
Ulna to carpals 0
2 33, F R (D) Giant cell tumor of the rightdistal radius
Wrist arthrodesis, OBF Ulna to carpals 1
3 20, M R (D) Deformed, malunited radiuswith atrophic ulnar nonunion
Corrective osteotomy of ulnaand radius, shortening, OBF
Proximal-third ulna tomiddle-third radius
2
4 21, M L (ND) Brachial plexus palsy withatrophic nonunion of forearm
Wrist arthrodesis, OBFreconstruction, DRUJ fusion,1st Carpometacarpal jointarthrodesis
Distal radius to carpalsand DRUJ fusion
2
5 7, M R (D) Atrophic nonunion of bothforearm bones
Excision of pseudarthrosis,OBF with 10 cm free fibula
Proximal-third ulna todistal-third radius
0
6 33, F L (ND) Atrophic nonunion of leftradius
OBF, DRUJ fusion DRUJ fusion 1
*DASH = Disabilities of the Arm, Shoulder and Hand score, LLD = limb-length discrepancy compared with the contralateral side, D = dominant, ADL =activities of daily living, and ND = nondominant. †Time at which union was ultimately achieved (following revision).
TABLE VII (continued)
Time toUnion (mo)
Outcome byPetersonScoring Infection and Nonunion
DASHScore LLD (cm)
Distal OBFPosition of Hand
Return to OriginalOccupation
13 Good Nil 5.8 1 Full supination Yes (modificationof household work)
10 Excellent Nil 3.3 2 Full supination Yes
24† Poor Yes, required 2 revisionprocedures for union
50.8 6 Full supination No, only ADL
8 Excellent Nil 12.5 2 10� pronation Suitable light work
3 Excellent Nil 0.8 2 Full supination Playing all sports
3 Excellent Nil 1.7 1 10� pronation Yes
e74(10)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

in 2 patients. Among 22 patients, all but 4 had a good toexcellent outcome according to the Peterson scoring system aswell as a good DASH score and were able to return to theirprevious or another suitable occupation.
The ideal position of forearm rotation has been debated.Jones, in 1934, recommended a rotational position of 10� ofpronation for fusion33, and more recent studies have reportedvarying degrees of rotation, from 0� to 45� of supination16,17,19.In our series, the right-side, dominant forearm was positionedin full supination, which is useful to receive objects and foreating, and shoulder rotatory movements are helpful to com-pensate for absent forearm rotations. The left-side, nondominantforearm was fixed in 10� of pronation, mainly for maintenanceof personal hygiene.
The largest previous series that we are aware of is that ofPeterson et al.14, with 19 patients. The authors reported goodresults following OBF reconstruction, with notable complica-tions in 10 patients (Table VIII). Allende and Allende reportedan average clinical score of 7.7 (Peterson et al. grading system14)with no cases of infection, nonunion, hardware failure, or
fracture16. In our study, the average clinical score was 6.6. Pe-terson et al. reported 59% with an excellent or good outcome;26%, fair; and 5%, poor14. In our elective group, 2 patients hada poor outcome because they had infection and nonunionrequiring additional procedures. Among the 4 patients with afair or poor outcome, 1 had limited hand function due toprevious infection and repeated debridement procedures, asecond patient hadwound dehiscence, a third patient had infectionfollowing replantation, and the fourth patient had median nervepalsy with forearm rotational deformity requiring multiplesecondary surgeries.
ConclusionsOBF reconstruction is a viable surgical treatment alternative indifficult clinical situations involving acute or chronic forearmbone loss. n
Agraharam Devendra, DNB1
Purnaganapathi Sundaram Velmurugesan, MS1
Jayaramaraju Dheenadhayalan, MS1
Hari Venkatramani, MS, MCh1
Shanmuganathan Raja Sabapathy, MS, MCh, DNB, FRCS(Ed),FRCS(Glas), MAMS1
Shanmuganathan Rajasekaran, MS, DNB, FRCS(Ed), MCh(Liv),FRCS(Eng), PhD1
1Departments of Orthopaedics (A.D., P.S.V., J.D., and S.R.) and Plastic &Micro Reconstructive Surgery (H.V. and S.R.S.), Ganga Hospital,Coimbatore, India
ORCID iD for A. Devendra: 0000-0001-5007-3644ORCID iD for P.S. Velmurugesan: 0000-0002-5713-2616ORCID iD for J. Dheenadhayalan: 0000-0002-1295-136XORCID iD for H. Venkatramani: 0000-0003-1792-267XORCID iD for S.R. Sabapathy: 0000-0002-0456-8555ORCID iD for S. Rajasekaran: 0000-0001-6043-006X
References
1. Sarmiento A, Ebramzadeh E, Brys D, Tarr R. Angular deformities and forearmfunction. J Orthop Res. 1992 Jan;10(1):121-33.2. Richard MJ, Ruch DS, Aldridge JM 3rd. Malunions and nonunions of the forearm[vii.]. Hand Clin. 2007 May;23(2):235-43.3. Sabapathy SR. Replantation. Semin Plast Surg. 2013 Nov;27(4):163-4.4. Sabapathy SR, Bhardwaj P. Secondary procedures in replantation. Semin PlastSurg. 2013 Nov;27(4):198-204.5. Sabapathy SR, Venkatramani H, Bharathi RR, Dheenadhayalan J, Bhat VR,Rajasekaran S. Technical considerations and functional outcome of 22 majorreplantations (the BSSH Douglas Lamb Lecture, 2005). J Hand Surg Eur Vol. 2007Oct;32(5):488-501.6. Chuang DC, Lai JB, Cheng SL, Jain V, Lin CH, Chen HC. Traction avulsionamputation of the major upper limb: a proposed new classification, guidelines foracute management, and strategies for secondary reconstruction. Plast ReconstrSurg. 2001 Nov;108(6):1624-38.7. Bueno RA Jr, Neumeister MW. Outcomes after mutilating hand injuries: review of theliterature and recommendations for assessment. Hand Clin. 2003 Feb;19(1):193-204.8. Bumbasirevic M, Stevanovic M, Lesic A, Atkinson HDE. Current management of themangled upper extremity. Int Orthop. 2012 Nov;36(11):2189-95. Epub 2012 Aug 25.9. Durham RM, Mistry BM, Mazuski JE, Shapiro M, Jacobs D. Outcome and utility ofscoring systems in the management of the mangled extremity. Am J Surg. 1996 Nov;172(5):569-73; discussion 573-4.
10. Shanmuganathan R. The utility of scores in the decision to salvage or ampu-tation in severely injured limbs. Indian J Orthop. 2008 Oct;42(4):368-76.11. Spiegel DA, Penny JN. Chronic osteomyelitis in children. Tech Orthop. 2005;20(2):142-52.12. PrasarnML, Ouellette EA, Miller DR. Infected nonunions of diaphyseal fractures ofthe forearm. Arch Orthop Trauma Surg. 2010 Jul;130(7):867-73. Epub 2009 Dec 10.13. Castle ME. One-bone forearm. J Bone Joint Surg Am. 1974 Sep;56(6):1223-7.14. Peterson CA 2nd, Maki S, Wood MB. Clinical results of the one-bone forearm. JHand Surg Am. 1995 Jul;20(4):609-18.15. Lee SJ, Jazrawi LM, Ong BC, Raskin KB. Long-term follow-up of the one-boneforearm procedure. Am J Orthop. 2000 Dec;29(12):969-72.16. Allende C, Allende BT. Posttraumatic one-bone forearm reconstruction. A reportof seven cases. J Bone Joint Surg Am. 2004 Feb;86(2):364-9.17. Kim SY, Chim H, Bishop AT, Shin AY. Complications and outcomes of one-boneforearm reconstruction. Hand (N Y). 2017 Mar;12(2):140-4. Epub 2016 Jul 7.18. Hey-Groves EW. Modern methods of treating fractures. 2nd ed. Bristol: JohnWright; 1921. Fractures of the upper limb; p 203-5.19. Jacoby SM, Bachoura A, Diprinzio EV, Culp RW, Osterman AL. Complicationsfollowing one-bone forearm surgery for posttraumatic forearm and distal radioulnarjoint instability. J Hand Surg Am. 2013 May;38(5):976-982.e1. Epub 2013 Apr 6.20. Bachoura A, Jacoby SM, Osterman AL. One-bone forearm procedure for Hajdu-Cheney syndrome: a case report. Hand (N Y). 2013 Dec;8(4):479-82.
TABLE VIII Reports on One-Bone Forearm Reconstruction inthe Literature
Study YearNo of
Patients Results
Castle13 1974 6 Good
Peterson et al.14 1995 19 Poor results in10 patients
Chen et al.22 1998 7 Good
Allende and Allende16 2004 7 Good
Jacoby et al.19 2013 10 Average results
Kim et al.17 2017 8 Good
Current series 2019 38 Good to excellentresults
e74(11)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION

21. Maffulli N, Fixsen JA. Pseudoarthrosis of the ulna in neurofibromatosis. A reportof four cases. Arch Orthop Trauma Surg. 1991;110(4):204-7.22. Chen F, Culp RW, Schneider LH, Osterman AL. Revision of the ununited one-bone forearm. J Hand Surg Am. 1998 Nov;23(6):1091-6.23. Murray RA. The one-bone forearm: a reconstructive procedure. J Bone Joint SurgAm. 1955 Apr;37(2):366-70.24. Haque IU. The production of a one-bone forearm as a salvage procedure afterhaematogenous osteomyelitis. A case report. J Bone Joint Surg Br. 1982;64(4):454-5.25. Reid RL, Baker GI. The single-bone forearm—a reconstructive technique. Hand.1973 Oct;5(3):214-9.26. Vitale CC. Reconstructive surgery for defects in the shaft of the ulna in children.J Bone Joint Surg Am. 1952 Oct;34(4):804-10.27. Chung-Wei C, Yun-Qing Q, Zhong-Jia Y. Extremity replantation. World J Surg.1978 Jul;2(4):513-24.28. Daoutis NK, Gerostathopoulos N, Efstathopoulos D, Misitzis D, Bouchlis G,Anagnostou S. Major amputation of the upper extremity. Functional results after
replantation/revascularization in 47 cases. Acta Orthop Scand Suppl. 1995 Jun;264:7-8.29. Mattiassich G, Rittenschober F, Dorninger L, Rois J, Mittermayr R, Ortmaier R,Ponschab M, Katzensteiner K, Larcher L. Long-term outcome following upperextremity replantation after major traumatic amputation. BMC Musculoskelet Dis-ord. 2017 Feb 10;18(1):77.30. Miller EA, Iannuzzi NP, Kennedy SA. Management of the mangled upperextremity: a critical analysis review. JBJS Rev. 2018 Apr;6(4):e11.31. Szabo RM, Thorson EP, Raskind JR. Allograft replacement with distal radioulnarjoint fusion and ulnar osteotomy for treatment of giant cell tumors of the distalradius. J Hand Surg Am. 1990 Nov;15(6):929-33.32. Ververidis AN, Drosos GI, Tilkeridis KE, Kazakos KI. Carpus translocation intothe ipsilateral ulna for distal radius recurrence giant cell tumour: a case report andliterature review. J Orthop. 2015 Feb 21;12(Suppl 1):S125-9.33. Jones RW. Reconstruction of the forearm after loss of the radius. Br J Surg.1934;22(85):23-6.
e74(12)
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 101-A d NUMBER 15 d AUGUST 7, 2019ONE-BONE FOREARM RECONSTRUCTION