onset of labour – recognition and failures caroline diamond supervisor of midwives lead midwife...
TRANSCRIPT

Onset of Labour –Recognition and Failures
Caroline Diamond
Supervisor of Midwives
Lead Midwife Obstetrics and Gynaecology Causeway Hospital
NHSCT
Onset of Labour –Recognition and Failures
Caroline Diamond
Supervisor of Midwives
Lead Midwife Obstetrics and Gynaecology Causeway Hospital
NHSCT

Failures Failures Failure to recognise the onset of labour has been
a predominant failing highlighted in Coroners inquest and in a number of SAIs
The ability to recognise the onset of labour is an essential core skill to the midwives role;
“3. Determine the onset of labour.”(Essential Skills Clusters (ESCs) for pre-registration
midwifery education3. NMC Standards for pre-registration midwifery education 2010).

Recognition of labour- what is the problem?
Recognition of labour- what is the problem?
Diagnosis of labour can be problematicA workforce planning tool identified that up to 30% of
women admitted to labour wards were not in labour
Women are more likely to have
some form of medical intervention
O’Driscoll et al (1973) asserts that recognition of labour is among the most important clinical decisions in labour care.
The WHO (1996) states that the most important aspect of assessing and managing a labour is the diagnosis of labour onset and that women may come to harm if misdiagnosed.
Despite the impact of misdiagnosis, there is a dearth of research on the process of decision-making by midwives in relation to diagnosis of labour
What’s the problem?What’s the problem? Midwives continue to struggle to
articulate the nature of their expertise Midwives have both tacit and practical
knowledge derived from experiential
learning and intuition. Midwives use a variety of emotional, psychological and
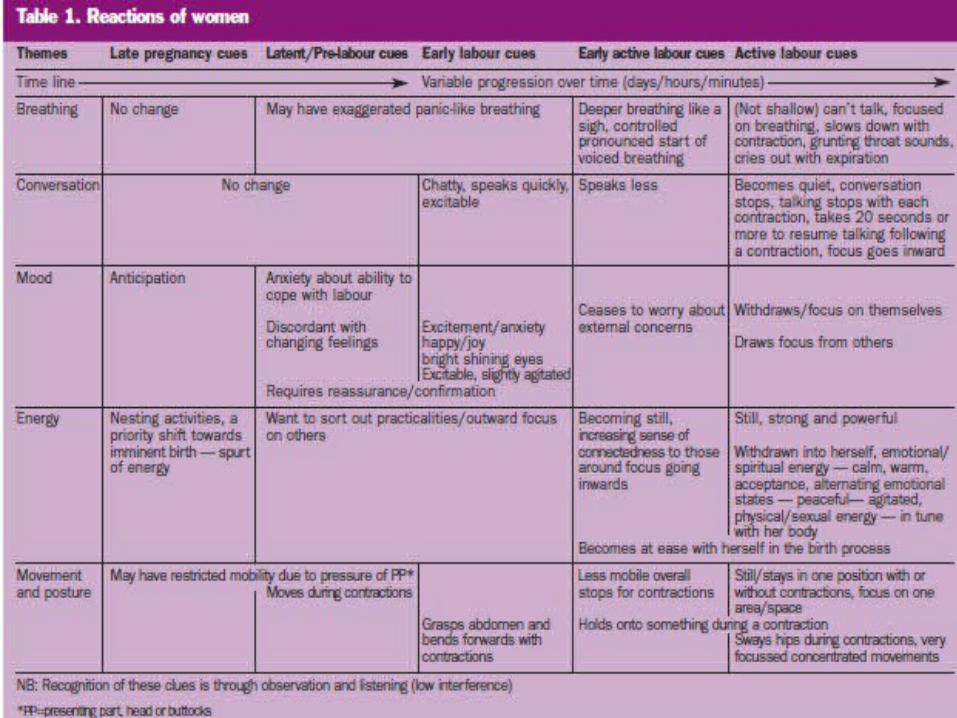
physical cues to diagnose labour onset such as a woman’s movements, breathing, conversation and emotional states.
HOWEVER, recognition and use of these cues is influenced by the political and social context in which a midwife works.
Why are we getting it wrong?Why are we getting it wrong? Physiological criteria
Use of vague but frequently used medical definitions of labour onset such as cervical dilatation
– Use of medical cues of labour onset- regular, rhythmical painful contractions and a cervical dilatation of 3cm, do not represent the experience and reality of all women
– Descriptors of ‘false’ ‘spurious’ and ‘true’ labours’ are antiquated and imprecise
Why are we getting it wrong?Why are we getting it wrong?
Physiological criteria Diagnosis of labour can only be made in retrospect
– Impossible to determine the precise moment when labour begins
– Inappropriate use of labels in the latent stage such as ‘nigglers’ and ‘gel pains’ if IOL
– Blurring of the Normality Boundary by induction agents deters the midwife’s intuitive ability to diagnose onset of labour, revert to medical model

What influences the decision-making
What influences the decision-making
Psychological processesMidwives respond to the cues presented to them by the use of heuristic processes (experience-based techniques for problem solving), or shortcuts to decision-making
The more complex the clinical case, the greater the use of heuristics in early labour
The use of heuristics is useful in identifying that unexplainable, intuitive knowledge and expertise.

What influences the decision-making
What influences the decision-making
Socio-political and philosophical perspective
Midwifery knowledge has become distorted by over reliance on the medical model and hospital routine practices
The competing nature of explicit or technical knowledge versus indeterminate or intuitive knowledge is a challenge to midwives seeking autonomy in a system influenced by the scientific paradigm
Midwives need to explore and understand midwifery ideology in order to preserve ‘normal’ midwifery

How do we get it right?How do we get it right?
Spontaneous labour External signs of labour i.e.
vaginal discharge, red line, contractions with and without abdominal palpation
Internal signs of labour- VE to include effacement, dilatation, application, consistency and position
Observe subtle maternal behaviours and reactions i.e. nesting, bright shining eyes, excitement, mood, conversation
Induction of labour Clear, unambiguous terminology
to describe contractions i.e. mild, moderate, strong, regular, irregular and timings
Avoid vague use of terms such as ‘gel pains’ ‘irritable uterus’
Perform VE as per policy or when analgesia requested


In summaryIn summary Midwives need to be vigilant that the future
midwifery ideology is not rooted purely in the biomedical model
Midwives need to clearly differentiate the normal pathway, spontaneous onset of labour and the high risk induced onset of labour
Midwives need to be able to articulate the indeterminate midwifery expertise and knowledge with regards to diagnosis of onset of labour
More research in the processes of diagnosing labour and is required

References References Ball & Washbrook (1996). Birthrate Plus: A Framework for Workforce Planning and Decision Making for Midwifery Services. Books for Midwives Press, London
Burvill (2002) Midwifery diagnosis of labour onset. British Journal of Midwifery, Vol 10, No 10, pp 600-605.
Cheyne, H., Dowding, D.W., Hundely, V. (2006) Making the diagnosis of labour; midwives’ diagnostic judgment and management decisions. Issues and Innovations in Nursing Practice. The Authors Journal compliation. Blackwell PUBLISJ=HING ltD
O’Driscoll, K., Stronge, J.M., Minogue, M. (1973) Active Management of Labour: British Medical Journal 3: 135-137.
WHO (1996) Care in Normal Birth: A Practical Guide Report of a Technical Working Group. Maternal and Newborn Health/ Safe Motherhood Unit, WHO, Geneva.