openbite mia ajodo
TRANSCRIPT
CASE REPORT
Treatment of open bite with microscrewimplant anchorageHyo-Sang Park, DDS, MSD, PhD,a Tae-Geon Kwon, DDS, MSD, PhD,b and Oh-Won Kwon, DDS, MSD, PhDc
Taegu, South Korea
Open bite treatment with microscrew implant anchorage is discussed in relation to vertical control of theposterior dentoalvelar dimension. Maxillary microscrew implants provided anchorage for intruding theposterior teeth and retracting the anterior teeth; mandibular microscrew implants were used to applyintrusion force distal to the mandibular first molars to prevent mesial tipping of the posterior teeth duringspace closure. Closing the mandibular plane after intruding the maxillary posterior teeth and bodily mesialmovement of the mandibular posterior teeth contributed to facial profile improvement. The efficacy andpotency of microscrew implants in open bite treatment are discussed. (Am J Orthod Dentofacial Orthop
2004;126:627-36)Open bite malocclusion has long been consid-ered a difficult problem to treat orthodonti-cally because its etiology is complicated and
multifactorial.1,2
Many treatment modalities to control open bitehave been proposed. However, they are not alwayssatisfactory because of the strong relapse tendency,which calls for orthognathic surgery,3 especially inadults. Dental compensation, such as uprighting theposterior teeth, and uprighting and extruding the ante-rior teeth, obtainable from multiloop edgewise arch-wires,2 can be optional for borderline patients and thosewho are reluctant to undergo surgery.
Intermaxillary elastics, used in conventional andmultiloop edgewise archwire mechanics, usuallycause extrusion of the posterior teeth4,5; this opensthe mandibular plane and has detrimental effects onthe facial profile. Therefore, vertical control of theposterior teeth is crucial in the orthodontic treatmentof open bite.
Skeletal anchorage, with dental implants,6
miniplates,7 miniscrews,8,9 and microscrews,10-13
has been used to provide absolute anchorage. Micro-screw implants are small enough to place in any areaof the alveolar bone, easy to place and remove, and
From the College of Dentistry, Kyungpook National University, Taegu, SouthKorea.aAssociate professor, Department of Orthodontics.bAssistant professor, Department of Oral and Maxillofacial Surgery.cProfessor, Department of Orthodontics.Reprint requests to: Hyo-Sang Park, DDS, MSD, PhD, Department of Orth-odontics, College of Dentistry, Kyungpook National University, 101, Dongin-2-Ga, Jung-Gu, Taegu, Korea 700-422; e-mail, [email protected], June 2003; revised and accepted, July 2003.0889-5406/$30.00Copyright © 2004 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2003.07.019inexpensive. In addition, orthodontic force applica-tion can begin almost immediately after place-ment.9,11 Therefore, the many advantages have ex-panded its use to various orthodontic problems.
In managing open bite, skeletal anchorage fromminiplates has been reported.7 The use of microscrewimplants, however, has not been discussed. This casereport shows the efficiency and simplicity of micro-screw implants to control anterior open bite; theyprovide anchorage to retract the maxillary incisors andcontrol the posterior teeth vertically.
BIOMECHANICS OF OPEN BITE TREATMENTWITH MICROSCREW IMPLANTS
Although the importance of the axial inclinationof the anterior teeth has been widely discussed, theaxial inclination of the posterior teeth has not at-tracted attention. Kim2 found patients who had nor-mal overbite relationships even with high mandibularplane angles and obtuse gonial angles—ie, longfaces. He also found that they have coincidingmaxillary and mandibular occlusal planes and up-right dentition in relation to the occlusal plane, andemphasized the importance of uprighting the denti-tion in treating open bite.
Extracting the second molars could minimizeresistance to uprighting the posterior teeth in adoles-cents who have well-shaped and well-positionedthird molars. This approach could upright the poste-rior teeth and establish functional occlusion, thuscorrecting the open bite; however, the facial profilechange was less than desirable, especially in patientswho had mild arch length discrepancies or protrudinglips. Extracting the premolars should be considered
to improve the facial profile. When treating patients627
l post
American Journal of Orthodontics and Dentofacial OrthopedicsNovember 2004
628 Park, Kwon, and Kwon
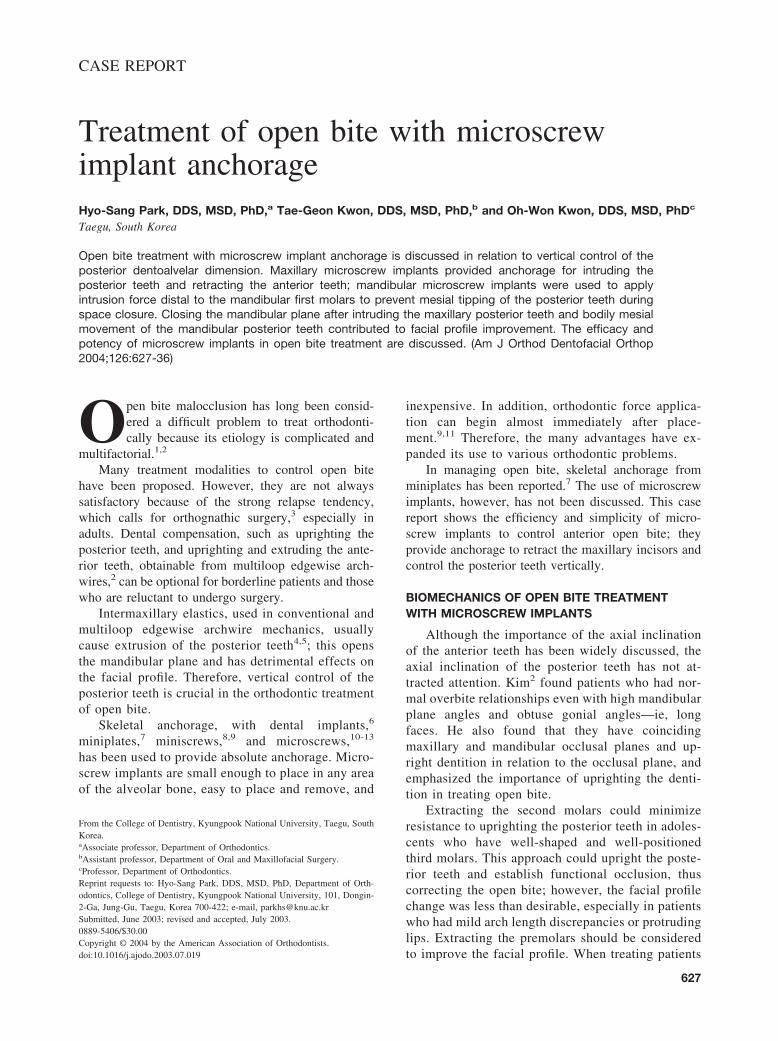
with premolar extractions, the molars tend to tipmesially during space closure; this should be pre-vented (Fig 1, A).
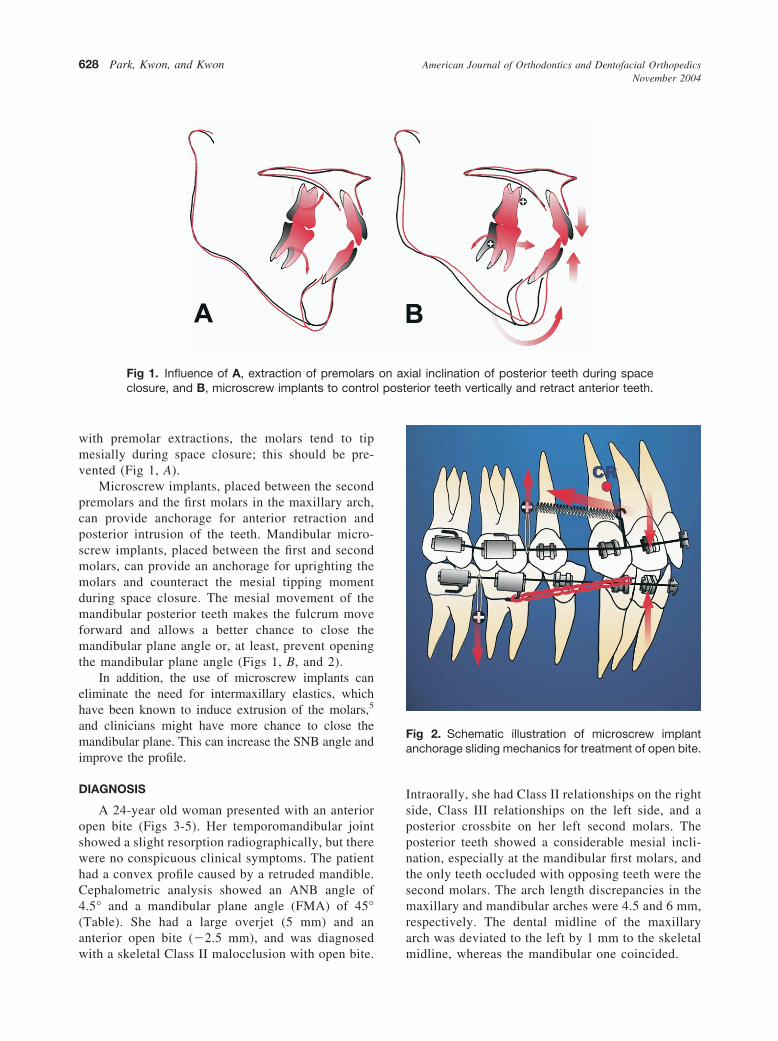
Microscrew implants, placed between the secondpremolars and the first molars in the maxillary arch,can provide anchorage for anterior retraction andposterior intrusion of the teeth. Mandibular micro-screw implants, placed between the first and secondmolars, can provide an anchorage for uprighting themolars and counteract the mesial tipping momentduring space closure. The mesial movement of themandibular posterior teeth makes the fulcrum moveforward and allows a better chance to close themandibular plane angle or, at least, prevent openingthe mandibular plane angle (Figs 1, B, and 2).
In addition, the use of microscrew implants caneliminate the need for intermaxillary elastics, whichhave been known to induce extrusion of the molars,5
and clinicians might have more chance to close themandibular plane. This can increase the SNB angle andimprove the profile.
DIAGNOSIS
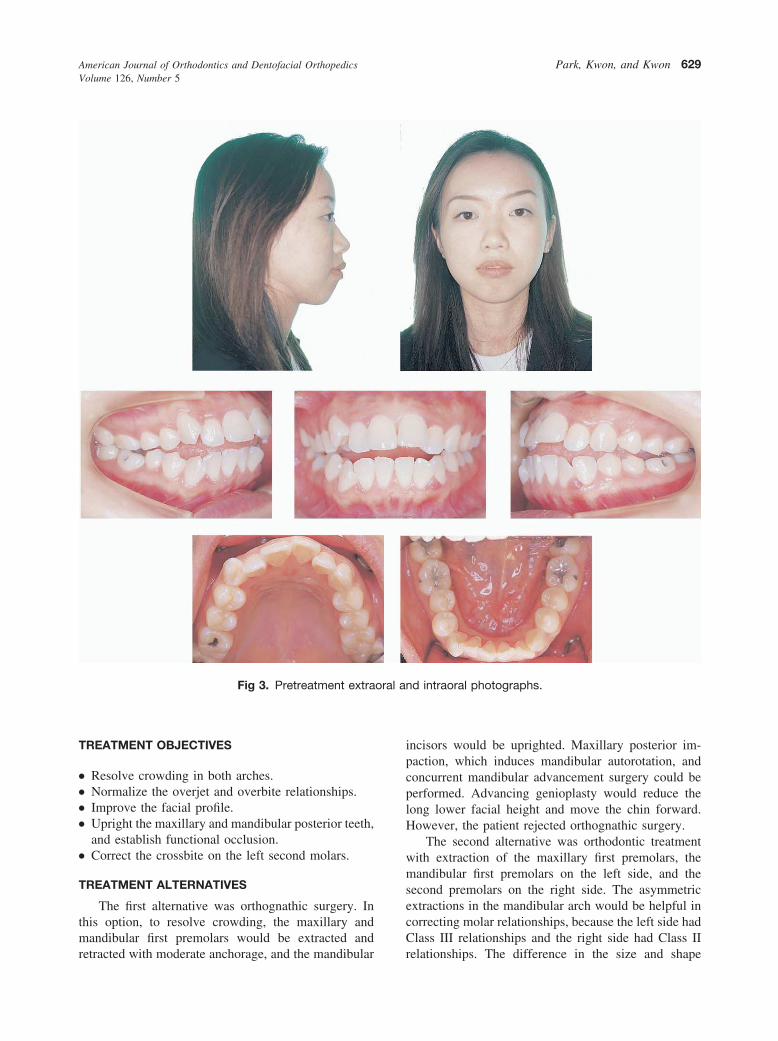
A 24-year old woman presented with an anterioropen bite (Figs 3-5). Her temporomandibular jointshowed a slight resorption radiographically, but therewere no conspicuous clinical symptoms. The patienthad a convex profile caused by a retruded mandible.Cephalometric analysis showed an ANB angle of4.5° and a mandibular plane angle (FMA) of 45°(Table). She had a large overjet (5 mm) and ananterior open bite (�2.5 mm), and was diagnosed
Fig 1. Influence of A, extraction of premolarsclosure, and B, microscrew implants to contro
with a skeletal Class II malocclusion with open bite.
Intraorally, she had Class II relationships on the rightside, Class III relationships on the left side, and aposterior crossbite on her left second molars. Theposterior teeth showed a considerable mesial incli-nation, especially at the mandibular first molars, andthe only teeth occluded with opposing teeth were thesecond molars. The arch length discrepancies in themaxillary and mandibular arches were 4.5 and 6 mm,respectively. The dental midline of the maxillaryarch was deviated to the left by 1 mm to the skeletal
ial inclination of posterior teeth during spaceerior teeth vertically and retract anterior teeth.
Fig 2. Schematic illustration of microscrew implantanchorage sliding mechanics for treatment of open bite.
on ax
midline, whereas the mandibular one coincided.
oral a
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 126, Number 5
Park, Kwon, and Kwon 629
TREATMENT OBJECTIVES
● Resolve crowding in both arches.● Normalize the overjet and overbite relationships.● Improve the facial profile.● Upright the maxillary and mandibular posterior teeth,
and establish functional occlusion.● Correct the crossbite on the left second molars.
TREATMENT ALTERNATIVES
The first alternative was orthognathic surgery. Inthis option, to resolve crowding, the maxillary andmandibular first premolars would be extracted and
Fig 3. Pretreatment extra
retracted with moderate anchorage, and the mandibular
incisors would be uprighted. Maxillary posterior im-paction, which induces mandibular autorotation, andconcurrent mandibular advancement surgery could beperformed. Advancing genioplasty would reduce thelong lower facial height and move the chin forward.However, the patient rejected orthognathic surgery.
The second alternative was orthodontic treatmentwith extraction of the maxillary first premolars, themandibular first premolars on the left side, and thesecond premolars on the right side. The asymmetricextractions in the mandibular arch would be helpful incorrecting molar relationships, because the left side hadClass III relationships and the right side had Class II
nd intraoral photographs.
relationships. The difference in the size and shape

American Journal of Orthodontics and Dentofacial OrthopedicsNovember 2004
630 Park, Kwon, and Kwon
between the first and second premolars made thisoption unfeasible.
The third alternative was extraction of the maxillaryfirst premolars and the mandibular second premolarsand microscrew implants for anchorage control. Wethought that, by moving the mandibular molars forwardafter extracting the second premolars, the fulcrum on
Fig 4. Pretrea
Fig 5. Pretreatment cephalometric radiograph.
the terminal molars could be moved forward, thus
closing the mandibular plane. By using microscrewimplants to control the amount of tooth movementanteroposteriorly in the mandibular arch, we couldavoid asymmetric extractions.
After evaluating the expected results and the man-dibular response, a decision was made to treat thepatient with third alternative. The treatment plan calledfor extracting the maxillary first premolars to resolveanterior crowding and improve the profile and themandibular second premolars to move the mandibularposterior teeth forward in hope of moving the fulcrumforward, followed by fixed appliance treatment and
dental casts.
Table. Cephalometric measurements
Pretreatment Posttreatment
SNA(°) 77 77SNB(°) 72.5 73ANB(°) 4.5 4FMA(°) 45 44PFH/AFH 0.52 (39/75) 0.50 (36/72.5)FH to Occ P(°) 15.5 17Ui to FH(°) 119.5 103IMPA(°) 100.5 85Z angle(°) 52 60
tment
microscrew implants for anchorage control.

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 126, Number 5
Park, Kwon, and Kwon 631
TREATMENT PROGRESS
A complete fixed preadjusted edgewise appliancewith .022-in slots was attached, and a .014-in nickel-titanium (Ni-Ti) archwire was placed.
Maxillary microscrew implants (8 mm long, 1.2mm in diameter, Osteomed, Dallas, Tex) were placedinto interradicular bone between the maxillary secondpremolars and the first molars, and mandibular implants(6 mm long, 1.2 mm in diameter, Osteomed) wereplaced into the cortical bone of the mandibular archbetween the first and second molars, as described inprevious reports.11-13
The microscrew implants were loaded 2 weeks afterplacement at a force of 150 g. To apply uprighting forceto the mesially tipped mandibular first molars, elasticthreads were connected from the microscrew implantsto the distal end of the archwire. Additionally, the Ni-Ticlosing coil spring force was applied from the maxillarymicroscrew implants to the canine brackets on bothsides, retracting the maxillary canine to create enoughspace to align the anterior teeth. A transpalatal bar wasplaced to prevent distortion of the arch form andbuccoversion of the posterior teeth during intrudingforce application (Fig 6).
After the maxillary anterior teeth were aligned, a.016 � .022-in stainless steel archwire with anteriorhooks was placed, Ni-Ti retraction force was appliedfrom the maxillary microscrew implants, and the 6anterior teeth were retracted simultaneously. In themandibular arch, a .017 � .025-in titanium-molybde-num alloy archwire was placed during space closure.Meanwhile, the intruding force was applied to thelower archwire from the mandibular microscrew im-plants; this was converted to a counterclockwise mo-ment on the first molars and an intruding force on thesecond molars (Fig 7). These force systems preventedthe mandibular molars from tipping mesially, as usuallyoccurs in conventional mechanotherapy.
At 11 months of treatment, the patient’s facialprofile showed improvement. The intruding force wasapplied in the maxillary arch in addition to the man-dibular arch, by connecting elastic threads from themaxillary microscrew implants to the maxillary arch-wire (Fig 8). The microscrew implants did not loosenduring treatment and were removed by unscrewingthem (Fig 9).
TREATMENT RESULTS
At 23 months of treatment, a well-aligned dentitionand a harmonious facial profile were obtained (Figs10-13). Harmonious facial balance was achieved by
retracting the maxillary and mandibular anterior teethand closing the mandibular plane after slight intrusionof the maxillary posterior teeth and forward movementof the mandibular posterior teeth with the uprighting.The long lower-lip-to-menton length decreased, and themuscle strain of the mentalis was eliminated. Thesechanges contributed to improvement of the facial pro-file.
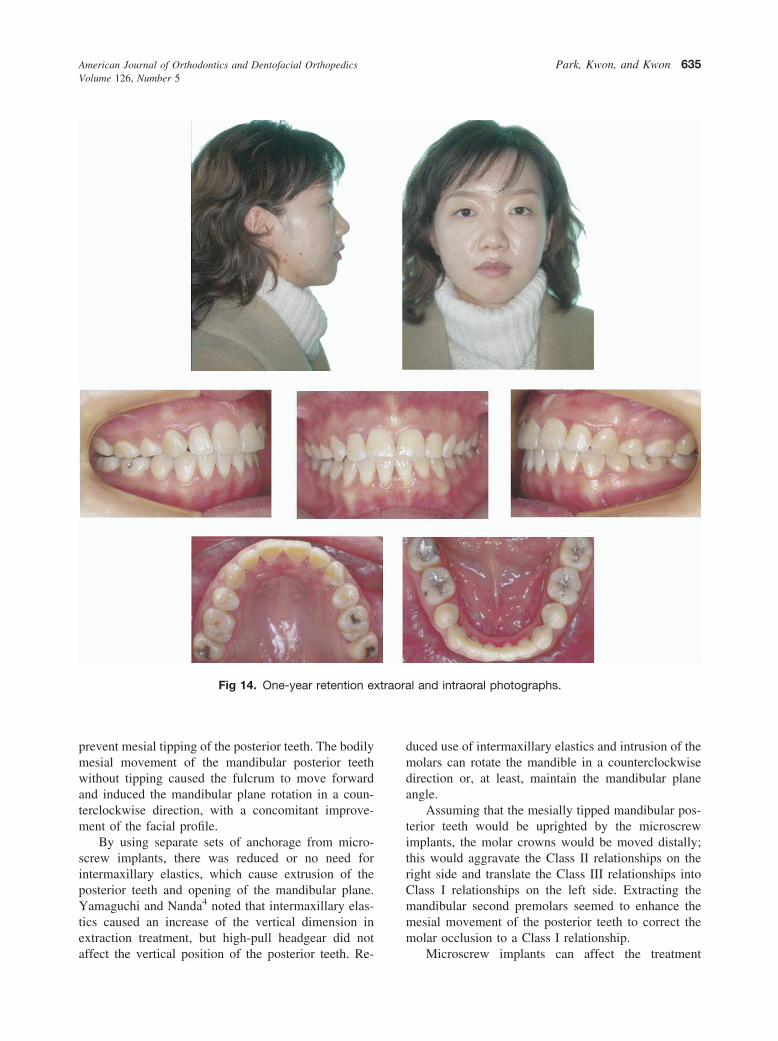
The patient had Class I canine and molar relation-ships, normal buccal overjet, and a small amount ofopen bite on the posterior teeth on right side; this hadsettled at the 1-year retention records (Fig 14). Theanterior teeth had normal overjet and overbite relation-ships, which were maintained during retention.
The initial difference of the lower border of themandible between the right and left sides disappearedwith establishment of the occlusion. Individual occlusalplanes, separated from each other initially, were cor-rected into 1 plane, and all posterior teeth were up-righted to the occlusal planes.
After debonding and debanding, a lingual bondedretainer on the 8 anterior teeth was delivered andstabilized in the mandibular arch, and a wraparoundretainer with an anterior clear resin band was prescribedfor retention.
On cephalometric superimposition, the maxillaryanterior teeth were retracted with intrusion, and themaxillary posterior teeth were intruded and moveddistally; the mandibular teeth showed uprighting.
DISCUSSION
In treating open bite, the importance of verticalcontrol of the posterior dentoalveolar height has beenextensively discussed.2,4,14,15 Many clinicians in theTweed Foundation have emphasized anchorage prepa-ration to prevent extrusion of the mandibular molars;this might be caused by Class II elastics.14,15 Propervertical control of the posterior teeth enhanced themandibular response—in other words, forward mandib-ular rotation.
Kim2 stressed the importance of correcting thecants of the occlusal planes and uprighitng the posteriorteeth against the occlusal plane in managing open bite.A multiloop edgewise archwire has been used to correctopen bite with good clinical results. However, anteriorvertical elastics can create a vertical extruding force onthe anterior teeth and an uprighting force on theposterior teeth, but do not produce sufficient force todistalize the teeth.5 As a result, the facial profile aftertreatment can be less than desirable.
To achieve a harmonious facial profile, the anteriorteeth should be retracted, in addition to open bitecorrection by uprighting the posterior teeth and extrud-
ing the anterior teeth; therefore, extraction of premolars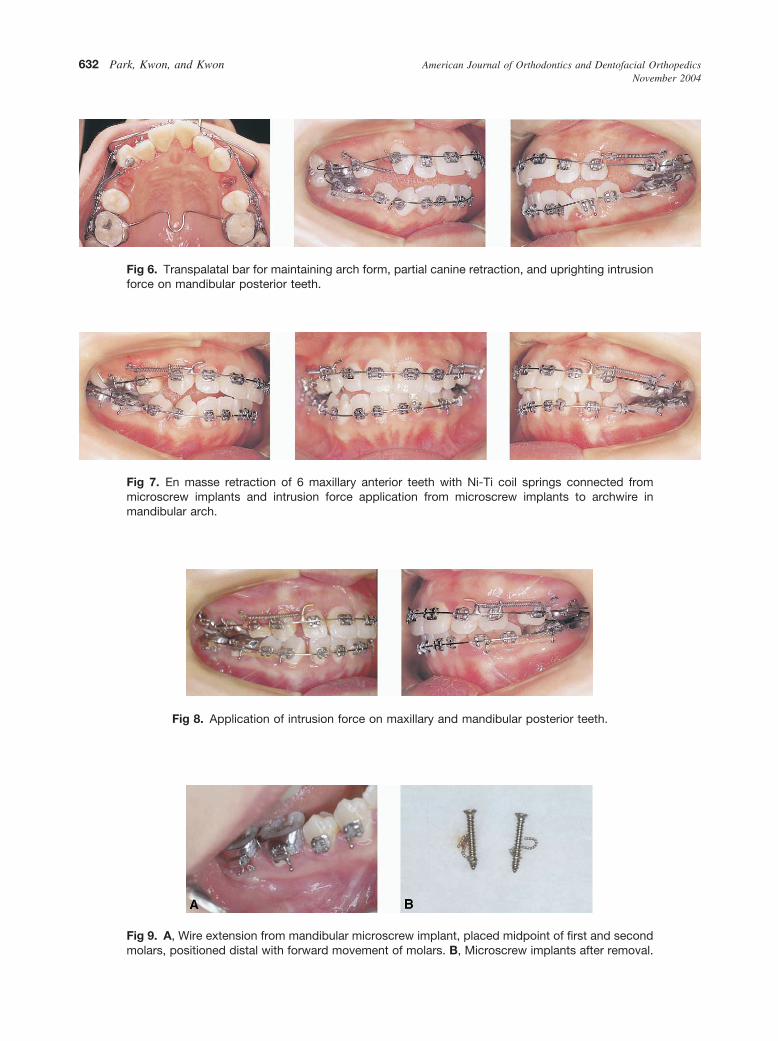
American Journal of Orthodontics and Dentofacial OrthopedicsNovember 2004
632 Park, Kwon, and Kwon
Fig 6. Transpalatal bar for maintaining arch form, partial canine retraction, and uprighting intrusion
force on mandibular posterior teeth.Fig 7. En masse retraction of 6 maxillary anterior teeth with Ni-Ti coil springs connected frommicroscrew implants and intrusion force application from microscrew implants to archwire in
mandibular arch.Fig 8. Application of intrusion force on maxillary and mandibular posterior teeth.
Fig 9. A, Wire extension from mandibular microscrew implant, placed midpoint of first and second
molars, positioned distal with forward movement of molars. B, Microscrew implants after removal.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 126, Number 5
Park, Kwon, and Kwon 633
should be considered. As previously mentioned, mesialtipping of the posterior teeth can easily occur withpremolar extractions. Therefore, microscrew implantsshould be used to control the posterior teeth verticallyand to retract the anterior teeth.
Microscrew implants have been used to provideanchorage for various types of tooth movements, in-cluding intrusion of the anterior and posterior teeth,retraction of the anterior teeth and the whole dentition,protraction of the posterior teeth, and molar uprighting.Their absolute anchorage, small size, and simple andless invasive surgical procedure could increase theirclinical use. Most importantly, the small size of micro-
Fig 10. Posttreatment extr
screw implants could expand possible locations for
placement, because dental implants need a largeamount of bone.
Maxillary microscrew implants were placed intointerradicular bone between the second premolars andthe first molars. By placing these at 30° to 40° to thelong axes of the teeth, not perpendicular to bonesurface, the horizontal depth of the embedded micro-screw implants from the bone surface was decreased by3 mm; the embedded portion would have been 6 mm.Therefore, the apices of the microscrew implants couldbe placed apart from the root. The thick mandibularcortical bone (3.1-3.2 mm on average16) and the 30° to40° of the placement angle could bear the 6 mm
and intraoral photographs.
aoralmicroscrew implants; with 4 mm of the microscrew

American Journal of Orthodontics and Dentofacial OrthopedicsNovember 2004
634 Park, Kwon, and Kwon
implants embedded into the bone, there was no possi-bility of root damage during placement and toothmovement. During surgical placement, the cliniciancan feel too much resistance if the microscrew implanttouches the root and should place it again with adifferent angulation to avoid root contact. The smallarea of damage to the root can be repaired with normalcementum.17
Fig 11. Posttre
Fig 12. Posttreatment cephalometric radiograph.
In this study, the maxillary posterior teeth, which
act as anchorage in conventional mechanics, showedposterior movement and intrusion during anterior teethretraction. The 6 anterior teeth could be retracted in themaxillary arch against the microscrew implants withoutanchorage loss so that the improvement of the facialprofile could be obtained in the early phase of treat-ment, and treatment time could be shortened.
Intrusion force was applied from the mandibular
t dental casts.
Fig 13. Cephalometric superimposition.
atmen
microscrew implants to the mandibular archwire to
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 126, Number 5
Park, Kwon, and Kwon 635
prevent mesial tipping of the posterior teeth. The bodilymesial movement of the mandibular posterior teethwithout tipping caused the fulcrum to move forwardand induced the mandibular plane rotation in a coun-terclockwise direction, with a concomitant improve-ment of the facial profile.
By using separate sets of anchorage from micro-screw implants, there was reduced or no need forintermaxillary elastics, which cause extrusion of theposterior teeth and opening of the mandibular plane.Yamaguchi and Nanda4 noted that intermaxillary elas-tics caused an increase of the vertical dimension inextraction treatment, but high-pull headgear did not
Fig 14. One-year retention e
affect the vertical position of the posterior teeth. Re-
duced use of intermaxillary elastics and intrusion of themolars can rotate the mandible in a counterclockwisedirection or, at least, maintain the mandibular planeangle.
Assuming that the mesially tipped mandibular pos-terior teeth would be uprighted by the microscrewimplants, the molar crowns would be moved distally;this would aggravate the Class II relationships on theright side and translate the Class III relationships intoClass I relationships on the left side. Extracting themandibular second premolars seemed to enhance themesial movement of the posterior teeth to correct themolar occlusion to a Class I relationship.
l and intraoral photographs.
xtraoraMicroscrew implants can affect the treatment

American Journal of Orthodontics and Dentofacial OrthopedicsNovember 2004
636 Park, Kwon, and Kwon
plan—eg, determining extraction or nonextractiontreatment, selecting teeth for extraction, or deciding onorthognathic surgery. Because of their ability to movethe whole dentition distally, nonextraction treatmentcould be increased. Clinicians can conserve healthyfirst premolars by extracting decayed second premolars,even though extracting the first premolars is necessaryto improve the facial profile.
CONCLUSIONS
Maxillary microscrew implants can provide anchor-age for retracting anterior teeth and simultaneouslyintruding posterior teeth, and mandibular microscrewimplants can prevent mesial tipping during space clo-sure. Microscrew implants provide good anchorage tocontrol open bite.
REFERENCES
1. Speidel TM, Isaacson RJ, Worms FW. Tongue-thrust therapyand anterior dental openbite. Am J Orthod 1972;62:287-95.
2. Kim YH. Anterior openbite and its treatment with multiloopedgewise archwire. Angle Orthod 1987;57:290-321.
3. Epker BN, Fish LC. Surgical-orthodontic correction of open-bitedeformity. Am J Orthod 1977;71:278-99.
4. Yamaguchi K, Nanda RS. The effects of extraction and nonex-traction treatment on the mandibular position. Am J OrthodDentofacial Orthop 1991;100:443-52.
5. Küçükkels N, Acar A, Demirkaya, AA, Evrenol B, Enacar A.
Cephalometric evaluation of open bite treatment with NiTiarchwire and anterior elastics. Am J Orthod Dentofacial Orthop1999;116:555-62.
6. Shapiro PA, Kokich VG. Uses of implants in orthodontics. DentClin North Am 1988;32:539-50.
7. Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H.Skeletal anchorage system for open bite correction. Am J OrthodDentofacial Orthop 1999;115:166-74.
8. Creekmore TD. The possibility of skeletal anchorage. J ClinOrthod 1983;17:266-9.
9. Costa A, Raffini M, Melsen B. Miniscrews as orthodonticanchorage. Int J Adult Orthod Orthog Surg 1998;13:201-9.
10. Kanomi R. Mini-implant for orthodontic anchorage. J ClinOrthod 1997;31:763-7.
11. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchor-age for treatment of skeletal Class I bialveolar protrusion. J ClinOrthod 2001;35: 417-22.
12. Park HS. Intrusion molar con anclaje de microimplantes (MIA,micro-implants anchorage). Orthodoncia Clinica 2003;6:31-6.
13. Park HS, Kyung HM, Sung JH. A simple method of molaruprighting with micro-implant anchorage. J Clin Orthod 2002;36:592-6.
14. Klontz HA. Facial balance and harmony: an attainable objectivefor the patient with a high mandibular plane angle. Am J OrthodDentofacial Orthop 1998;114:176-88.
15. Lamarque S. The importance of occlusal plane control duringorthodontic mechanotherapy. Am J Orthod Dentofacial Orthop1995;107:548-58.
16. Champy M, Pape H, Gerlach KL, Lodde JP. Mandibular fracture.In: Kruger E, Schilli W editors. Oral and maxillofacial trauma-tology. Vol 2. Chicago, London, Berlin, Rio de Janeiro, Tokyo:Quintessence; 1986. p. 19-43.
17. Tsukikochi, M. Autotransplantation of teeth. Tokyo: Quintes-
sence; 1999. p. 29.