oral agents—the old and new in the management of t2dm · echo -diabetes. july 21, 2016. veronica...
TRANSCRIPT
ECHO-DiabetesJuly 21, 2016
VERONICA BRADY, PHD, FNP-BC, BC-ADM, CDE
ORAL AGENTS— OLD & NEW FOR THE
MANAGEMENT OF T2DM
Overview of Diabetes Oral hypoglycemic agents Define various classes of medications Describe mechanisms of action Define indications/contraindications for use
Q & A
OBJECTIVES
CDC.gov/diabetes, 2014
29.1 million in US ( 9.3% of population)
Nearly 1/3 (27.8%) unaware that they have diabetes
7th leading cause of death in the US in 2010
More than 234,051 death certificates list diabetes as underlying cause in 2010
Cost of care $245 billion—2.3 x higher medical expenditures for people with DM
Increasing prevalence in children and adults
DIABETES – THE FACTS
As many as 1 in 3 US adults could have diabetes by 2050
C DC . g ov / d ia betes
Formerly Non-insulin Dependant Diabetes (NIDDM)
Heterogeneous disorder
Variable plasma insulin levels-low or high
Peripheral insulin resistance
Associated with increased CV risk
TYPE 2 DM
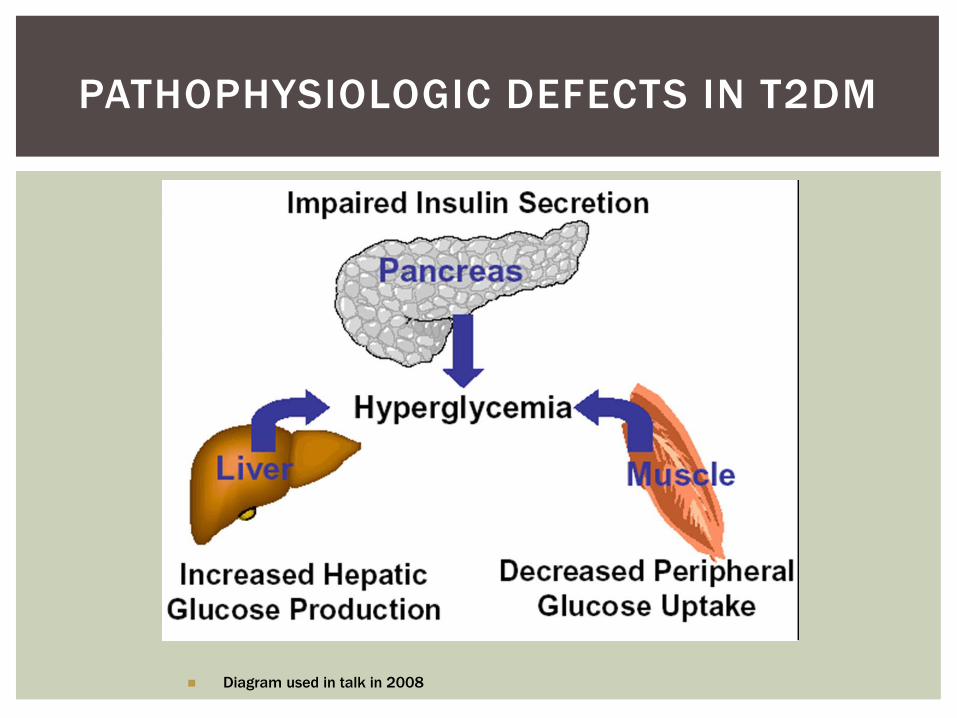
Diagram used in talk in 2008
PATHOPHYSIOLOGIC DEFECTS IN T2DM
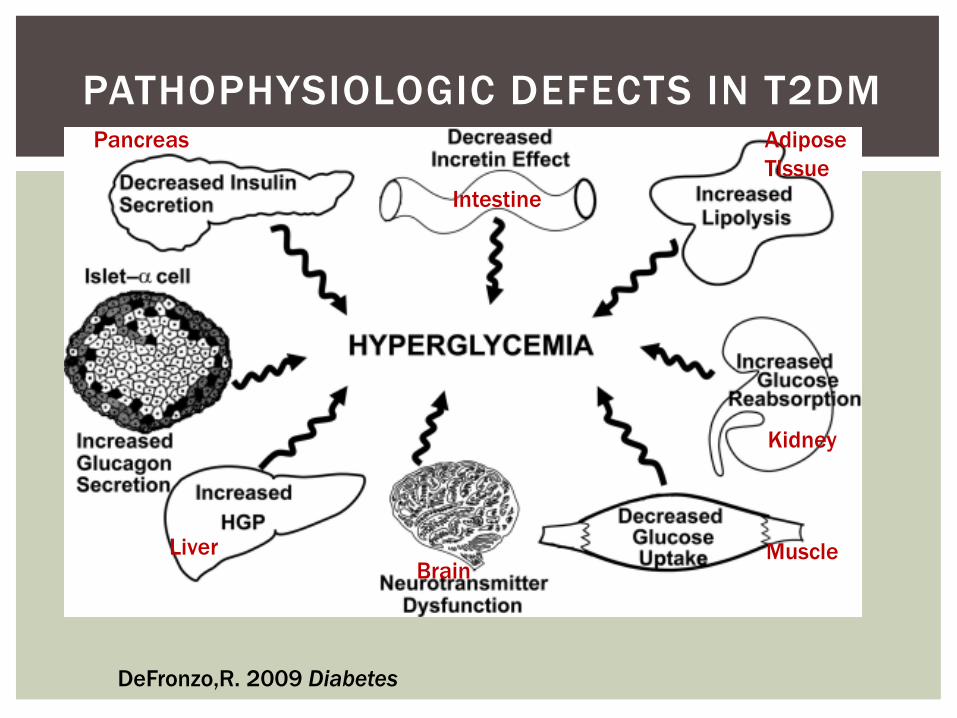
DeFronzo,R. 2009 Diabetes
Intestine
Kidney
Liver MuscleBrain
Pancreas AdiposeTissue
PATHOPHYSIOLOGIC DEFECTS IN T2DM
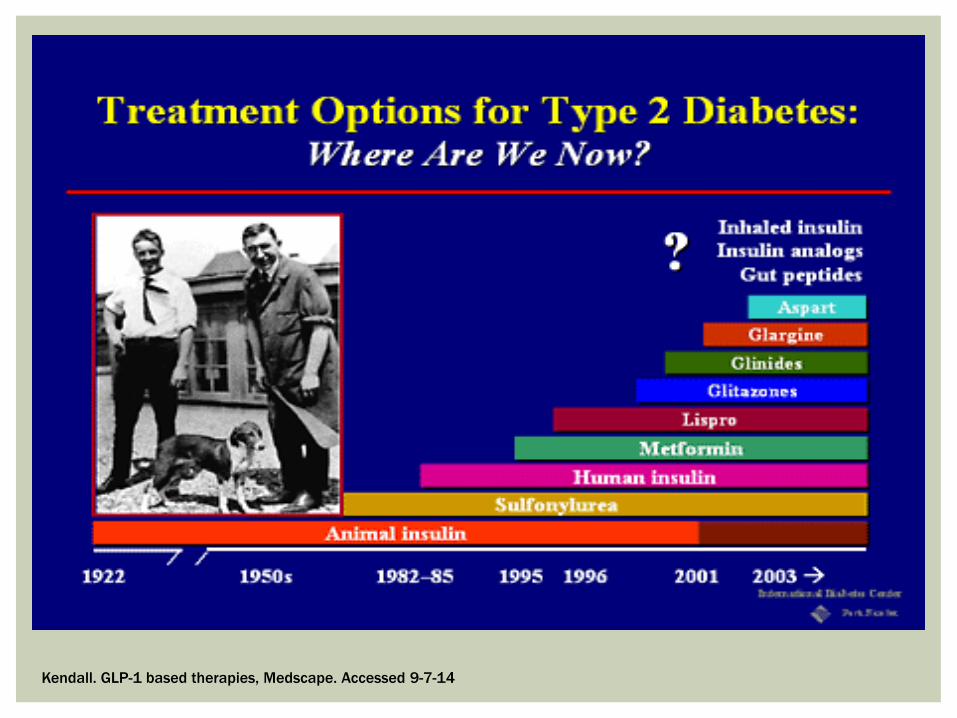
Kendall. GLP-1 based therapies, Medscape. Accessed 9-7-14
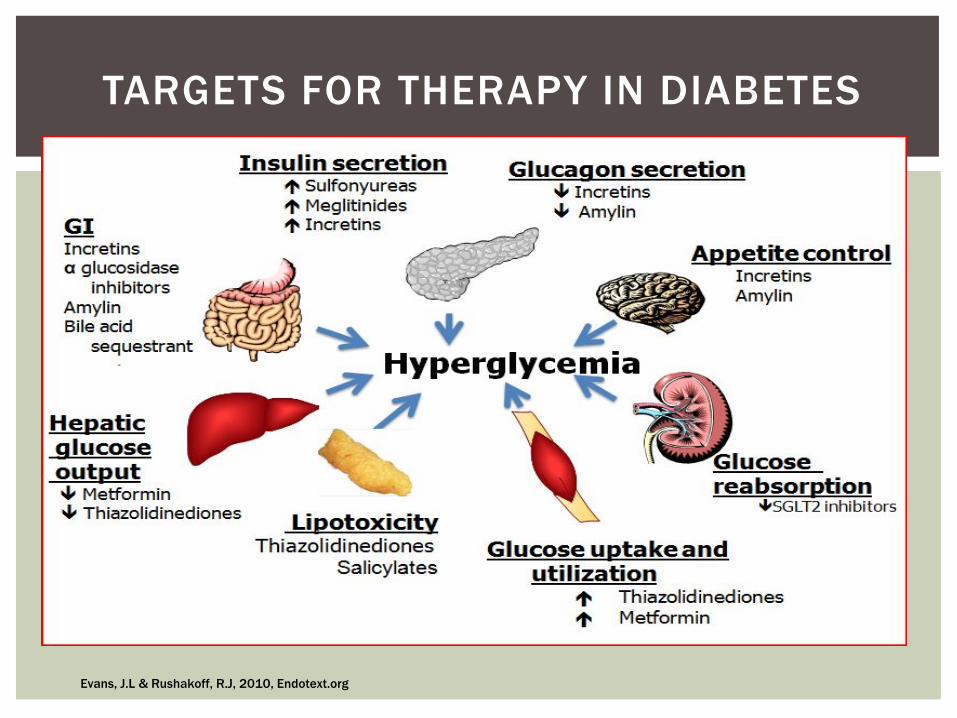
Evans, J.L & Rushakoff, R.J, 2010, Endotext.org
TARGETS FOR THERAPY IN DIABETES
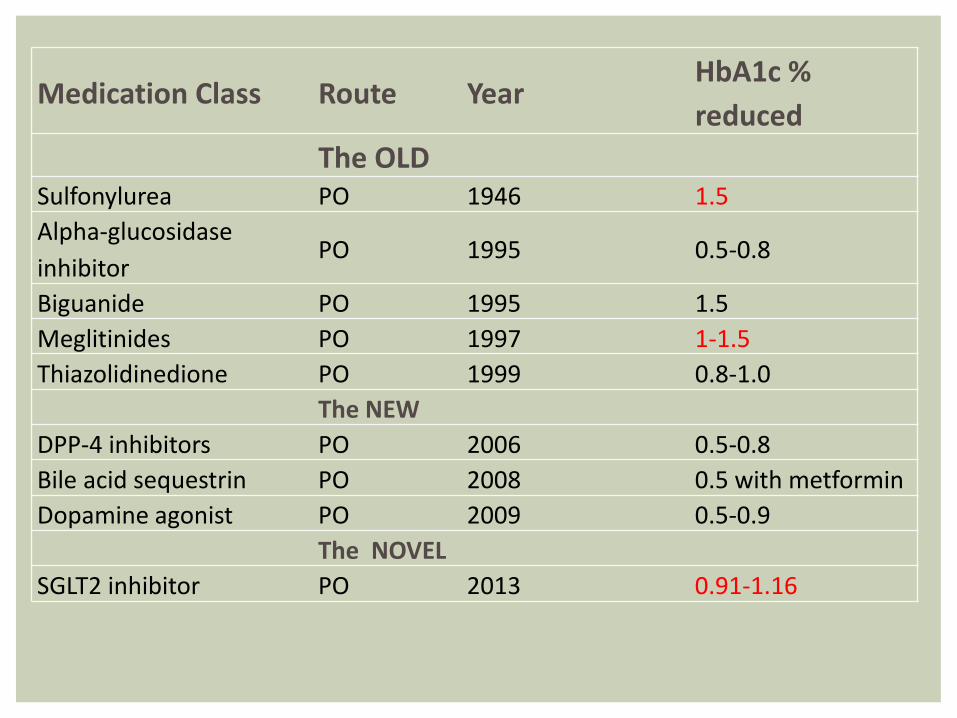
HbA1c % Medication Class Route Year
reducedThe OLD
Sulfonylurea PO 1946 1.5Alpha-glucosidase inhibitor
PO 1995 0.5-0.8
Biguanide PO 1995 1.5Meglitinides PO 1997 1-1.5Thiazolidinedione PO 1999 0.8-1.0
The NEWDPP-4 inhibitors PO 2006 0.5-0.8Bile acid sequestrin PO 2008 0.5 with metforminDopamine agonist PO 2009 0.5-0.9
The NOVELSGLT2 inhibitor PO 2013 0.91-1.16
ORAL HYPOGLYEMIC AGENTS (OHA)
Increases insulin secretion in people with capacity to produce insulin, may also decrease the rate of hepatic glucose production, and increase insulin receptor sensitivity and increase the number of insulin receptors
SULFONYLUREAS
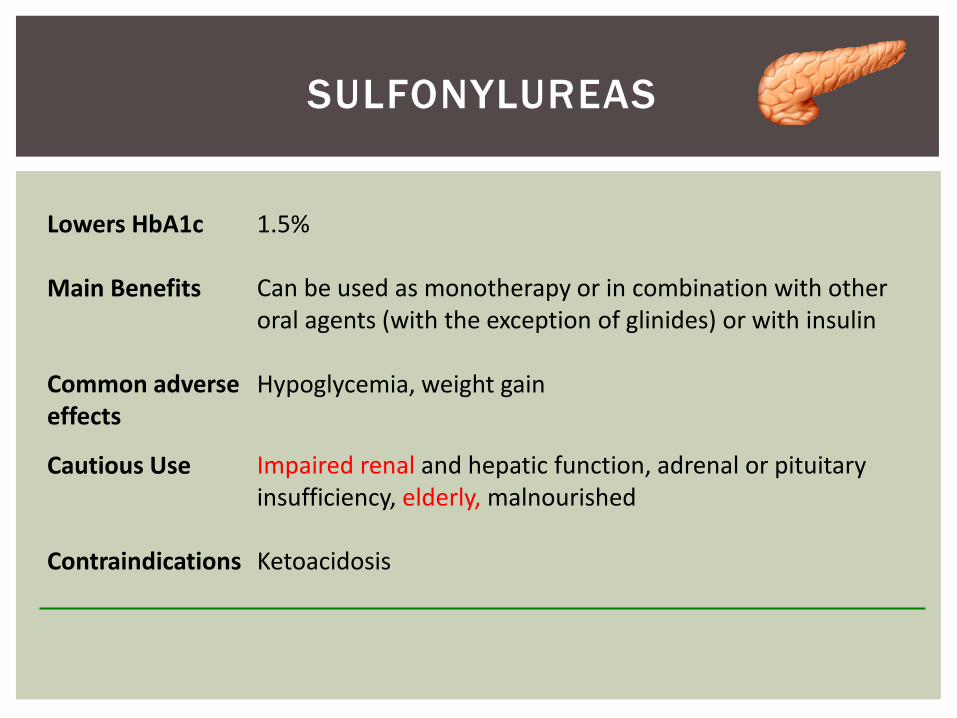
Lowers HbA1c 1.5%
Main Benefits Can be used as monotherapy or in combination with other oral agents (with the exception of glinides) or with insulin
Common adverse Hypoglycemia, weight gaineffects
Cautious Use Impaired renal and hepatic function, adrenal or pituitary insufficiency, elderly, malnourished
Contraindications Ketoacidosis
SULFONYLUREAS
Considerations: Lead to progressive decline in β-cell function
No protective effect against atherosclerotic cardiovascular complications
Within 3 years most patients require 2nd anti-diabetic medication
Defronzo, 2009. Diabetes
SULFONYLUREAS
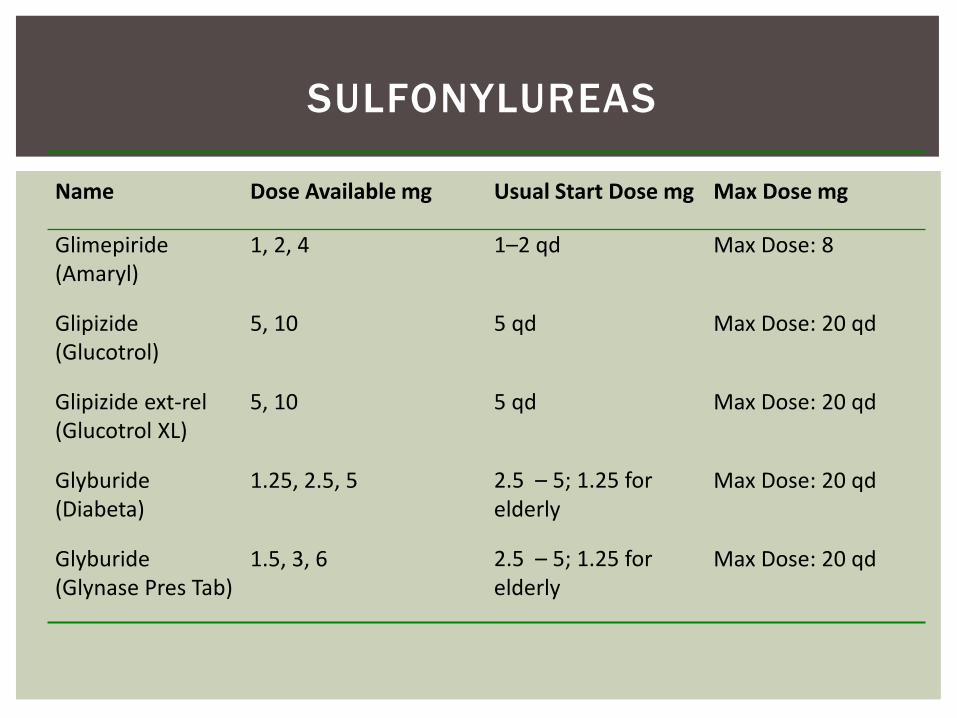
Name Dose Available mg Usual Start Dose mg Max Dose mg
Glimepiride (Amaryl)
1, 2, 4 1–2 qd Max Dose: 8
Glipizide (Glucotrol)
5, 10 5 qd Max Dose: 20 qd
Glipizide ext-rel (Glucotrol XL)
5, 10 5 qd Max Dose: 20 qd
Glyburide (Diabeta)
1.25, 2.5, 5 2.5 – 5; 1.25 for elderly
Max Dose: 20 qd
Glyburide (Glynase Pres Tab)
1.5, 3, 6 2.5 – 5; 1.25 for elderly
Max Dose: 20 qd
SULFONYLUREAS
Inhibits enzyme that facilitates breakdown of complex sugars to glucose in the small intestine, causes malabsorption of carbohydrates
ALPHA-GLUCOSIDASE INHIBITORS
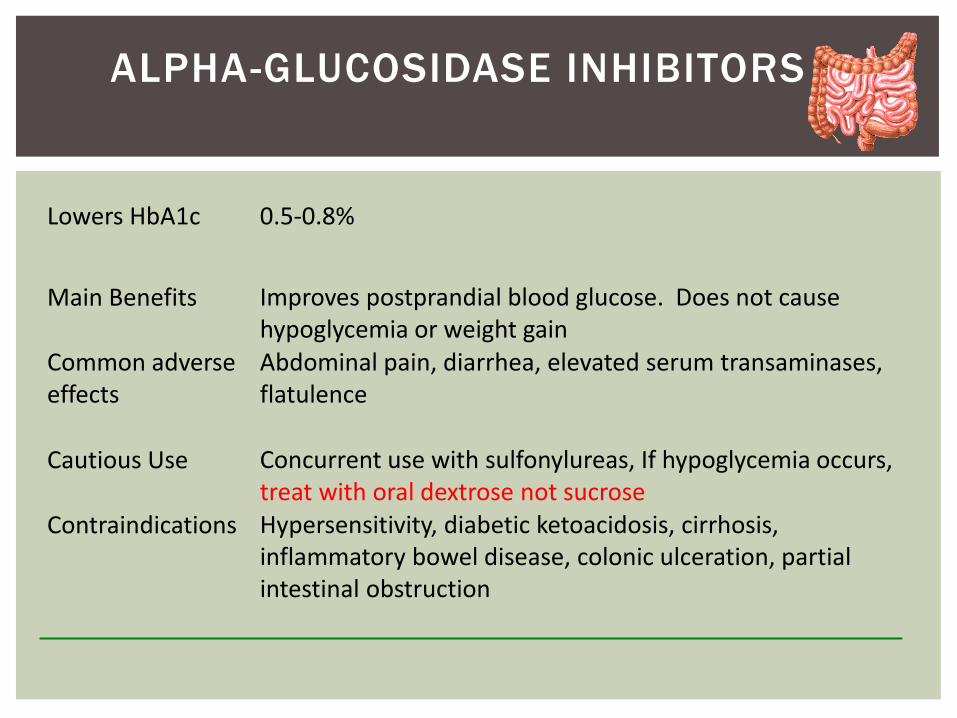
Lowers HbA1c 0.5-0.8%
Main Benefits Improves postprandial blood glucose. Does not causehypoglycemia or weight gain
Common adverse effects
Abdominal pain, diarrhea, elevated serum transaminases, flatulence
Cautious Use Concurrent use with sulfonylureas, If hypoglycemia occurs, treat with oral dextrose not sucrose
Contraindications Hypersensitivity, diabetic ketoacidosis, cirrhosis, inflammatory bowel disease, colonic ulceration, partial intestinal obstruction
ALPHA-GLUCOSIDASE INHIBITORS
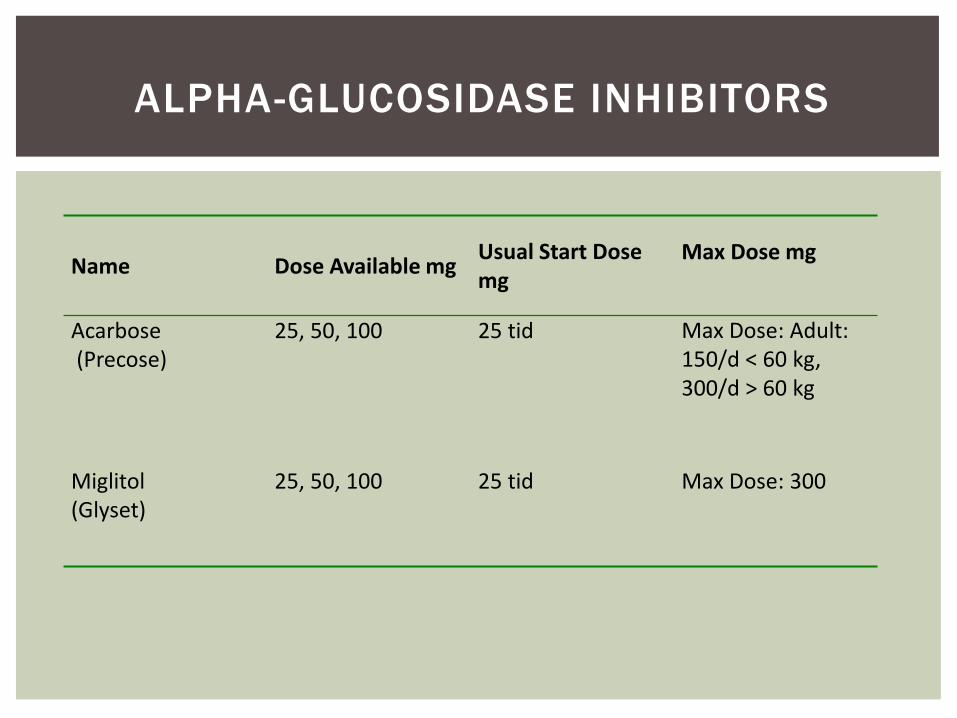
Usual Start Dose Max Dose mgName Dose Available mg mg
Acarbose(Precose)
25, 50, 100 25 tid Max Dose: Adult: 150/d < 60 kg, 300/d > 60 kg
Miglitol (Glyset)
25, 50, 100 25 tid Max Dose: 300
ALPHA-GLUCOSIDASE INHIBITORS
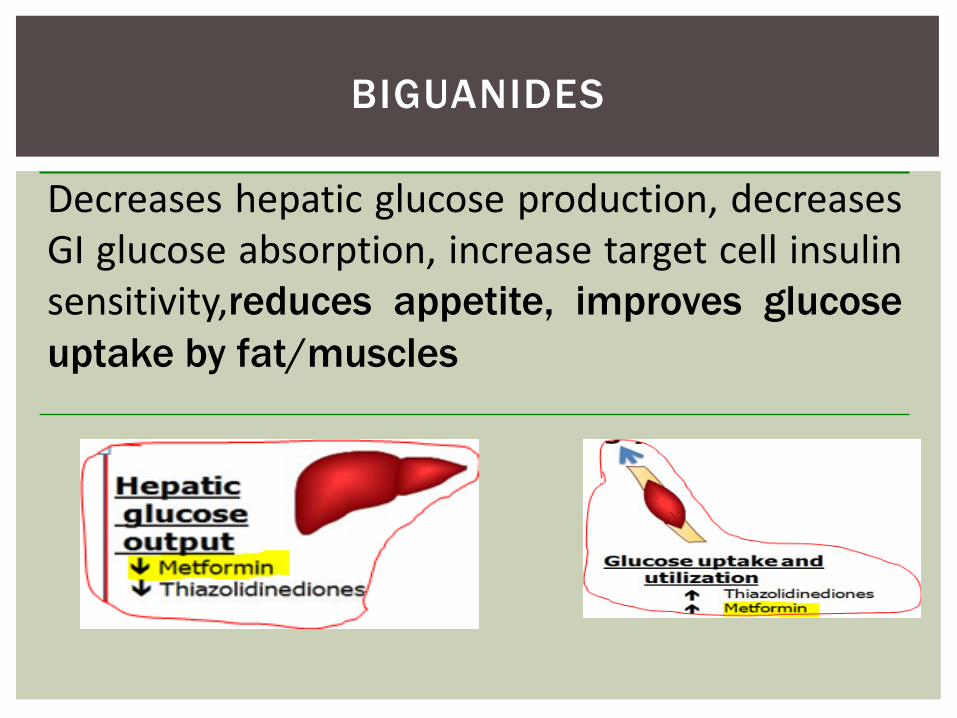
Decreases hepatic glucose production, decreasesGI glucose absorption, increase target cell insulinsensitivity,reduces appetite, improves glucoseuptake by fat/muscles
BIGUANIDES
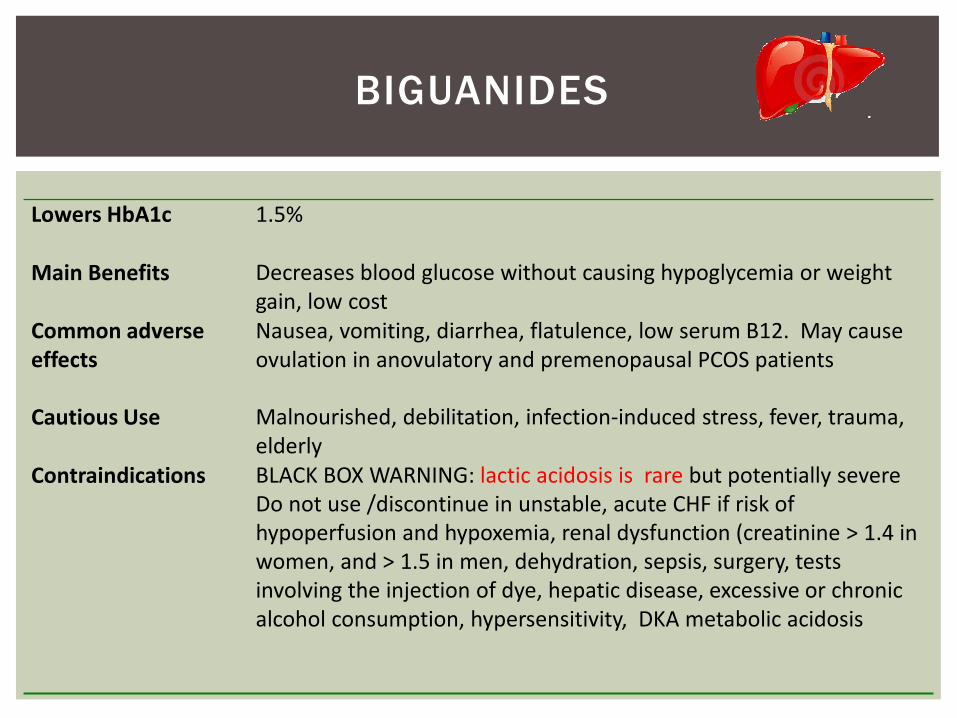
Lowers HbA1c 1.5%
Main Benefits Decreases blood glucose without causing hypoglycemia or weight gain, low cost
Common adverse effects
Nausea, vomiting, diarrhea, flatulence, low serum B12. May cause ovulation in anovulatory and premenopausal PCOS patients
Cautious Use Malnourished, debilitation, infection-induced stress, fever, trauma, elderly
Contraindications BLACK BOX WARNING: lactic acidosis is rare but potentially severe Do not use /discontinue in unstable, acute CHF if risk of hypoperfusion and hypoxemia, renal dysfunction (creatinine > 1.4 in women, and > 1.5 in men, dehydration, sepsis, surgery, tests involving the injection of dye, hepatic disease, excessive or chronic alcohol consumption, hypersensitivity, DKA metabolic acidosis
BIGUANIDES
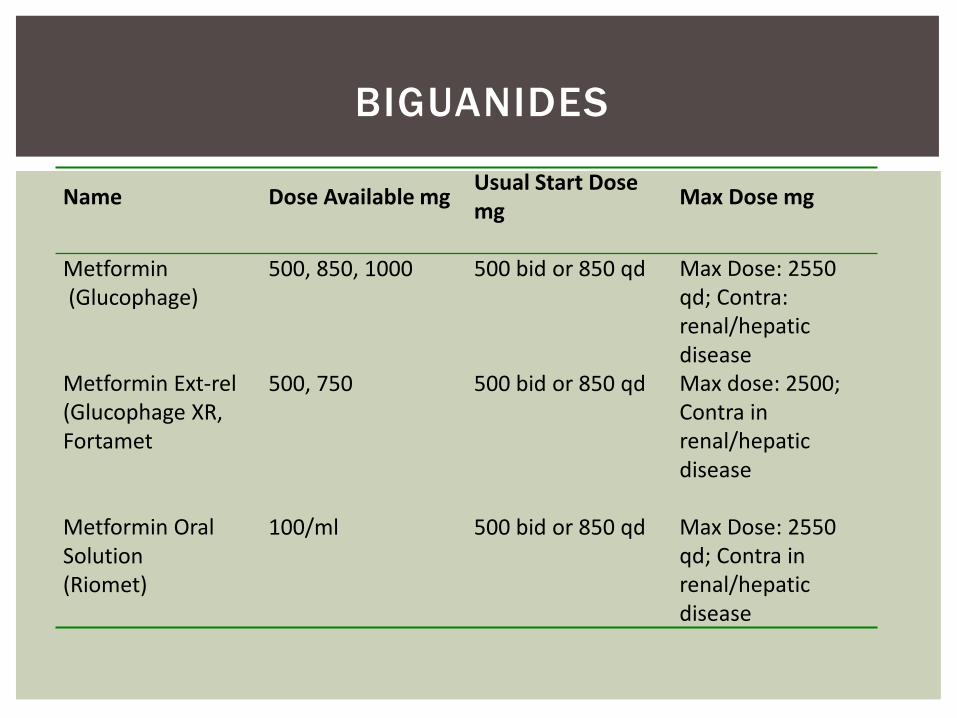
Name Dose Available mg Max Dose mgmgUsual Start Dose
Metformin(Glucophage)
500, 850, 1000 500 bid or 850 qd Max Dose: 2550 qd; Contra: renal/hepatic disease
Metformin Ext-rel (Glucophage XR, Fortamet
500, 750 500 bid or 850 qd Max dose: 2500; Contra in renal/hepatic disease
Metformin Oral Solution(Riomet)
100/ml 500 bid or 850 qd Max Dose: 2550 qd; Contra in renal/hepatic disease
BIGUANIDES
Considerations:
May be safe for use in patients with slightly elevated Cr—if it has been stable (1.4-1.7mg/dL), patient does not drink alcohol and dose not have large areas of tissue damageMay be used in patients with IFG/IGTMetformin is not metabolized and most of drug is
excreted in the urine (Barieri, et al. 2014. Uptodate)
BIGUANIDES
Increases insulin secretion by binding to K+ channels on beta islet cells. Repaglinide is metabolized by the liver enzymes CYP3A4 & CYP2C8. Nateglinide is metabolized by hepatic cytochrome P450 CYP2Cp (70%) and CYP34A (30%)
MEGLITINIDES
Lowers HbA1c 1-1.5%
Main Benefits Increases insulin levels for a short period of time compared to sulfonylurea agents. Meglitinides have a lower risk of hypoglycemia compared to sulfonylureas. Good for those who skip meals.
Common adverse effects
Hypoglycemia (less risk compared to sulfonylureas)
Cautious Use Renal insufficiency, liver disease, use with insulin, adrenal insufficiency, surgery, trauma, elderly, pituitary insufficiency, malnourished
Contraindications Ketoacidosis, allergy to medication, Type 1 diabetes, used with gemfibrozil results in increased repaglinide plasma concentrations 8-fold and may result in severe hypoglycemia
MEGLITINIDES
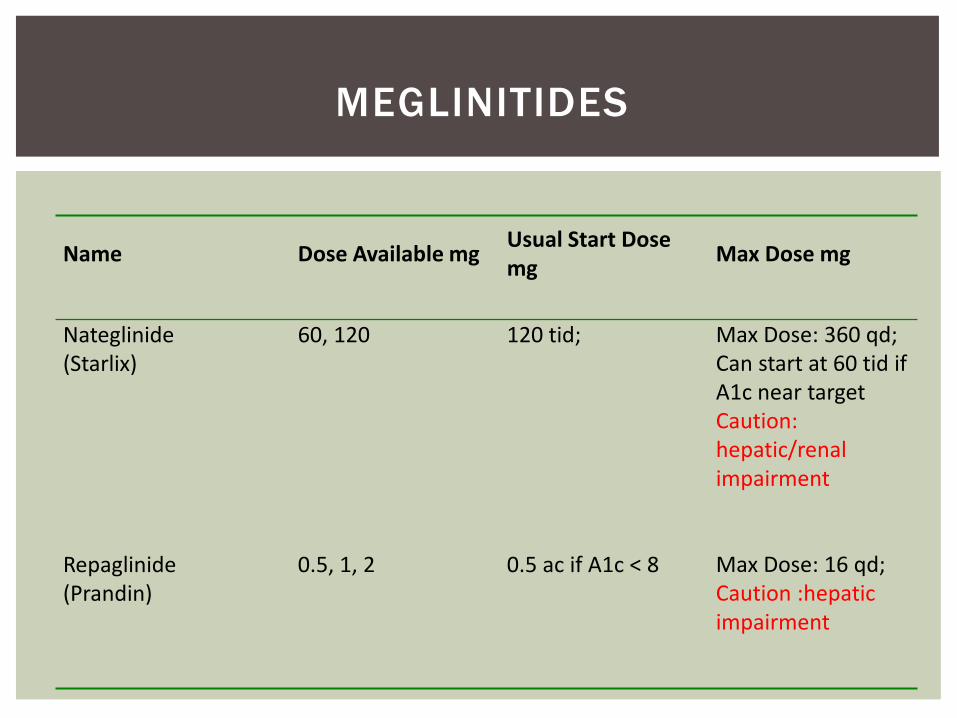
Usual Start Dose Name Dose Available mg Max Dose mgmg
Nateglinide(Starlix)
60, 120 120 tid; Max Dose: 360 qd; Can start at 60 tid if A1c near target Caution:hepatic/renal impairment
Repaglinide(Prandin)
0.5, 1, 2 0.5 ac if A1c < 8 Max Dose: 16 qd; Caution :hepatic impairment
MEGLINITIDES
Improves target cell response to insulin, Increases glucose uptake by muscle and fat and decreases hepatic gluconeogenesis. Metabolized to active metabolites by hepatic CYP2C8 & CYP34A
THIAZOLIDINEDIONES
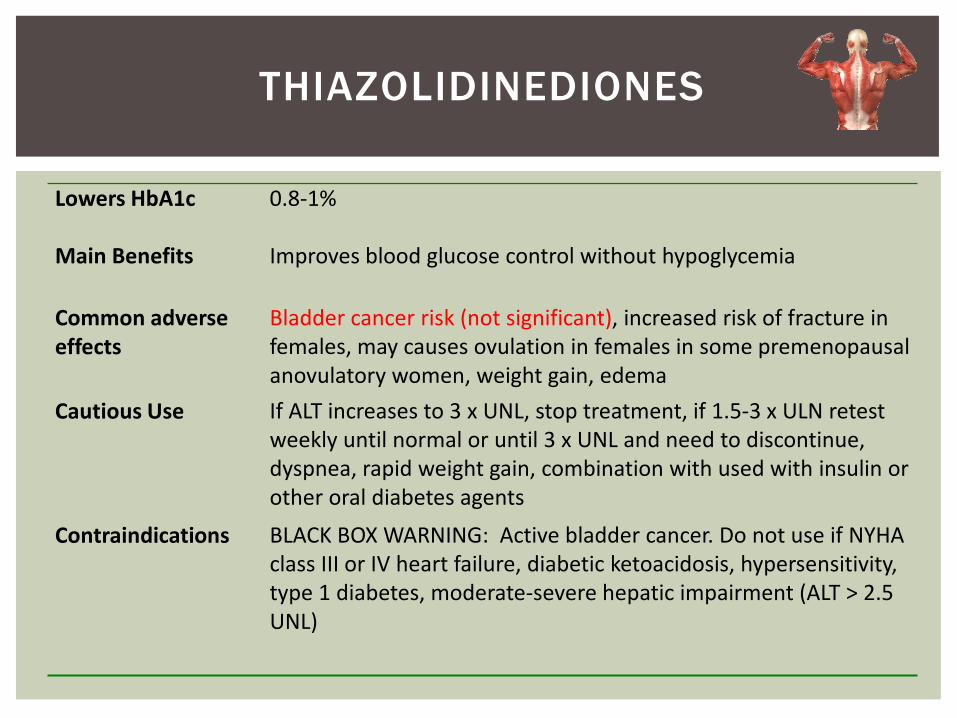
Lowers HbA1c 0.8-1%
Main Benefits Improves blood glucose control without hypoglycemia
Common adverse effects
Bladder cancer risk (not significant), increased risk of fracture in females, may causes ovulation in females in some premenopausal anovulatory women, weight gain, edema
Cautious Use If ALT increases to 3 x UNL, stop treatment, if 1.5-3 x ULN retest weekly until normal or until 3 x UNL and need to discontinue, dyspnea, rapid weight gain, combination with used with insulin or other oral diabetes agents
Contraindications BLACK BOX WARNING: Active bladder cancer. Do not use if NYHA class III or IV heart failure, diabetic ketoacidosis, hypersensitivity, type 1 diabetes, moderate-severe hepatic impairment (ALT > 2.5 UNL)
THIAZOLIDINEDIONES
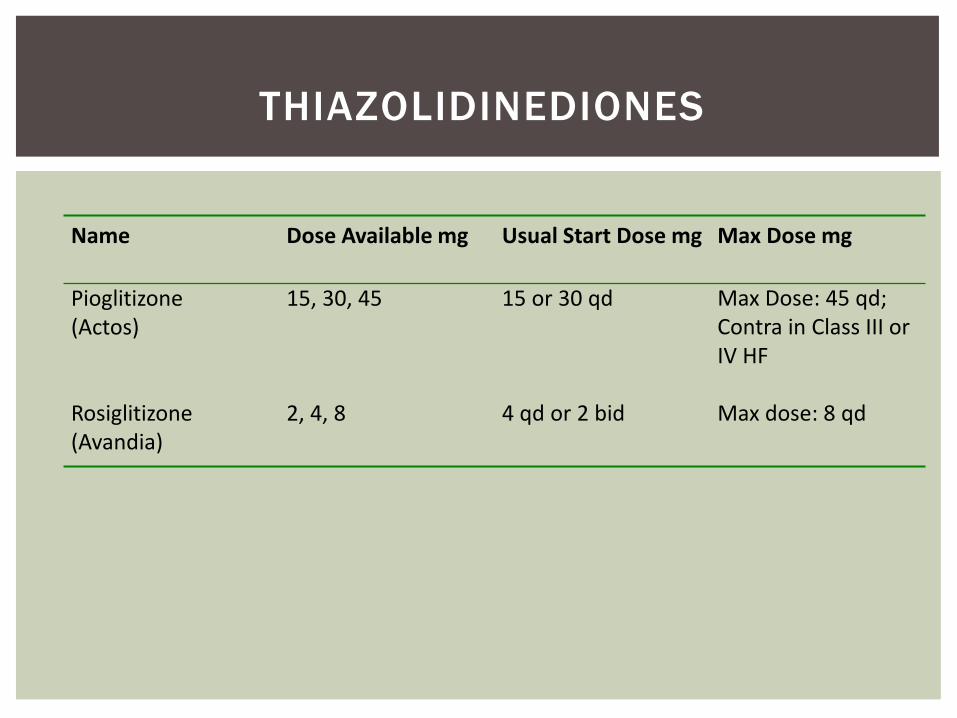
Name Dose Available mg Usual Start Dose mg Max Dose mg
Pioglitizone (Actos)
15, 30, 45 15 or 30 qd Max Dose: 45 qd; Contra in Class III or IV HF
Rosiglitizone (Avandia)
2, 4, 8 4 qd or 2 bid Max dose: 8 qd
THIAZOLIDINEDIONES
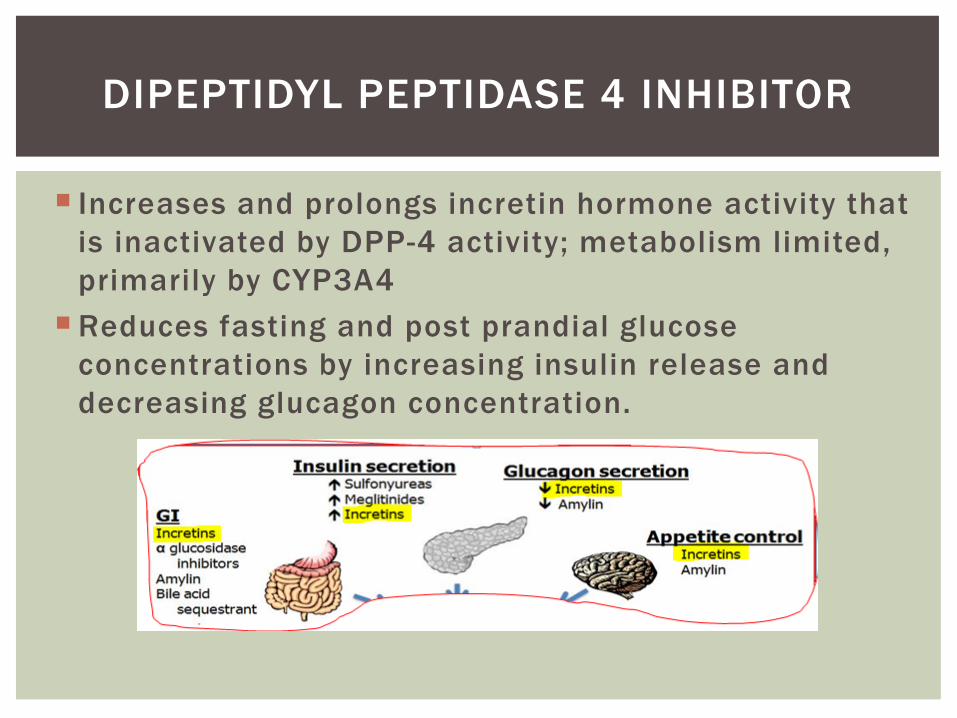
Increases and prolongs incretin hormone activity that is inactivated by DPP-4 activity; metabolism limited, primarily by CYP3A4
Reduces fasting and post prandial glucose concentrations by increasing insulin release and decreasing glucagon concentration.
DIPEPTIDYL PEPTIDASE 4 INHIBITOR
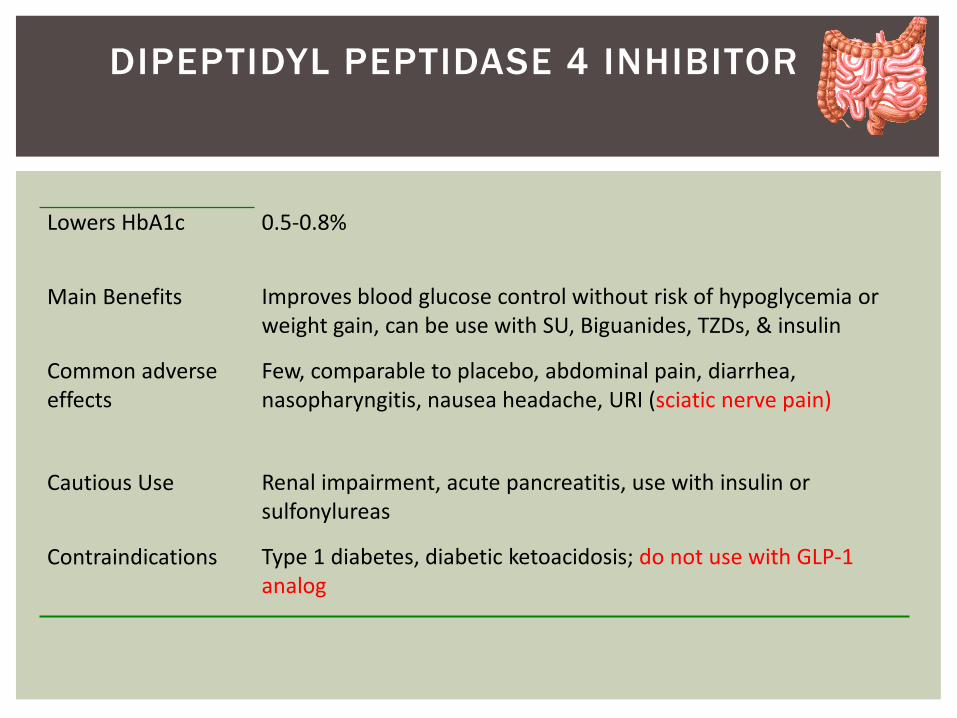
Lowers HbA1c 0.5-0.8%
Main Benefits Improves blood glucose control without risk of hypoglycemia or weight gain, can be use with SU, Biguanides, TZDs, & insulin
Common adverse effects
Few, comparable to placebo, abdominal pain, diarrhea, nasopharyngitis, nausea headache, URI (sciatic nerve pain)
Cautious Use Renal impairment, acute pancreatitis, use with insulin or sulfonylureas
Contraindications Type 1 diabetes, diabetic ketoacidosis; do not use with GLP-1 analog
DIPEPTIDYL PEPTIDASE 4 INHIBITOR
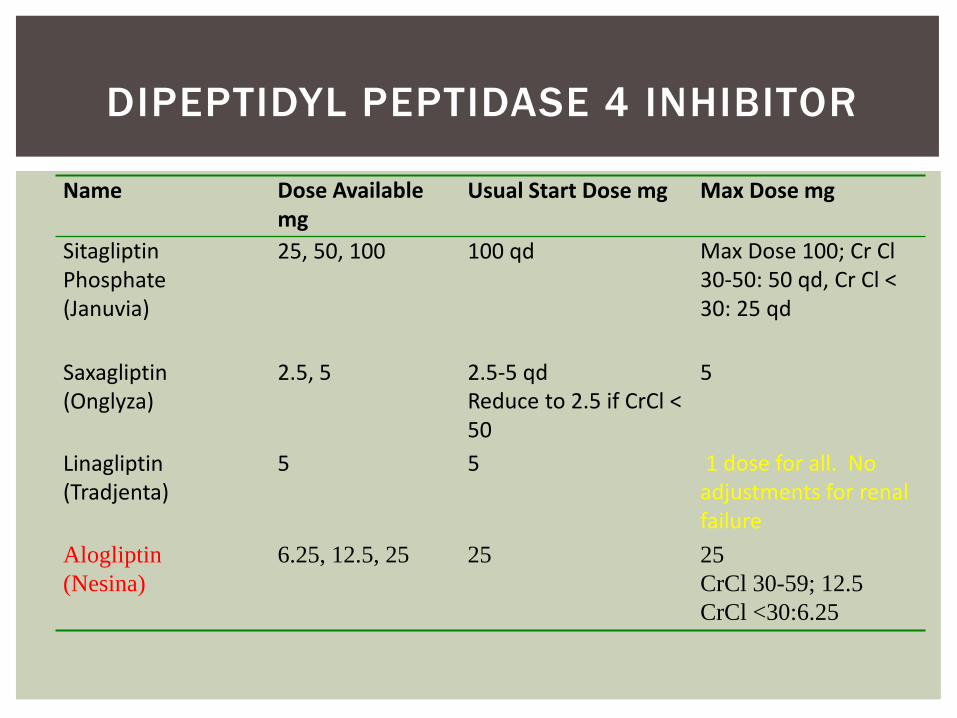
Name Dose Available Usual Start Dose mg Max Dose mgmg
Sitagliptin Phosphate (Januvia)
25, 50, 100 100 qd Max Dose 100; Cr Cl 30-50: 50 qd, Cr Cl < 30: 25 qd
Saxagliptin (Onglyza)
2.5, 5 2.5-5 qdReduce to 2.5 if CrCl < 50
5
Linagliptin(Tradjenta)
5 5 1 dose for all. No adjustments for renal failure
Alogliptin(Nesina)
6.25, 12.5, 25 25 25CrCl 30-59; 12.5CrCl <30:6.25
DIPEPTIDYL PEPTIDASE 4 INHIBITOR
Binds with bile acids in the intestine thereby impeding their reabsorption. As the bile acid pool is depleted, the hepatic enzyme, cholesterol 7-alpha-hydroxylase is upregulated, which increases the conversion of cholesterol to bile acids. The mechanism of action for reducing blood glucose is unknown.
BILE ACID SEQUESTRANT
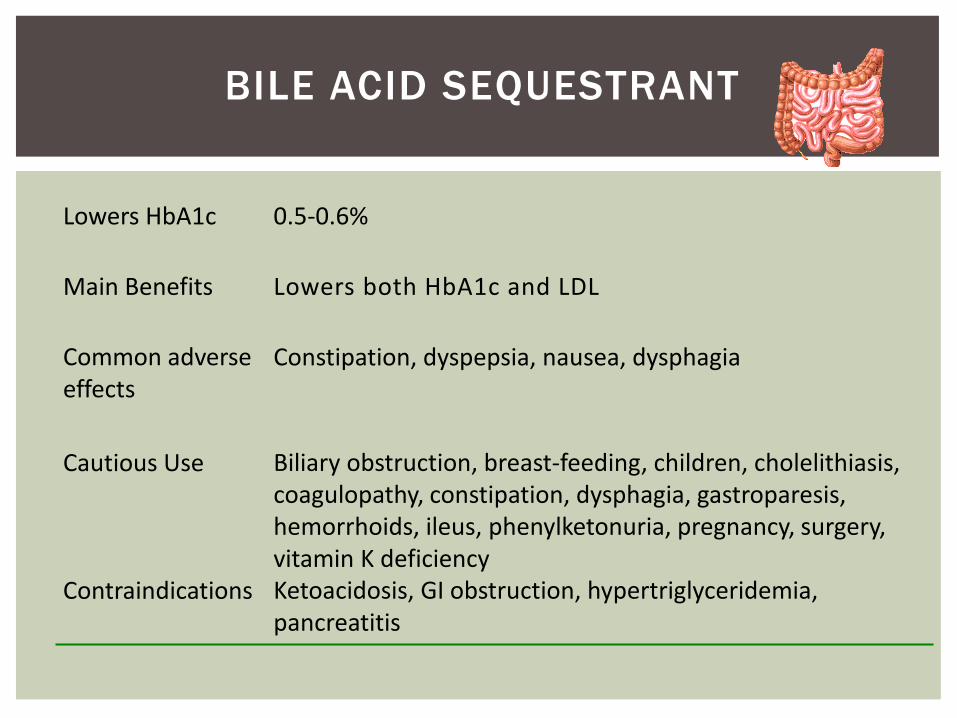
Lowers HbA1c 0.5-0.6%
Main Benefits Lowers both HbA1c and LDL
Common adverse effects
Constipation, dyspepsia, nausea, dysphagia
Cautious Use Biliary obstruction, breast-feeding, children, cholelithiasis, coagulopathy, constipation, dysphagia, gastroparesis, hemorrhoids, ileus, phenylketonuria, pregnancy, surgery, vitamin K deficiency
Contraindications Ketoacidosis, GI obstruction, hypertriglyceridemia, pancreatitis
BILE ACID SEQUESTRANT
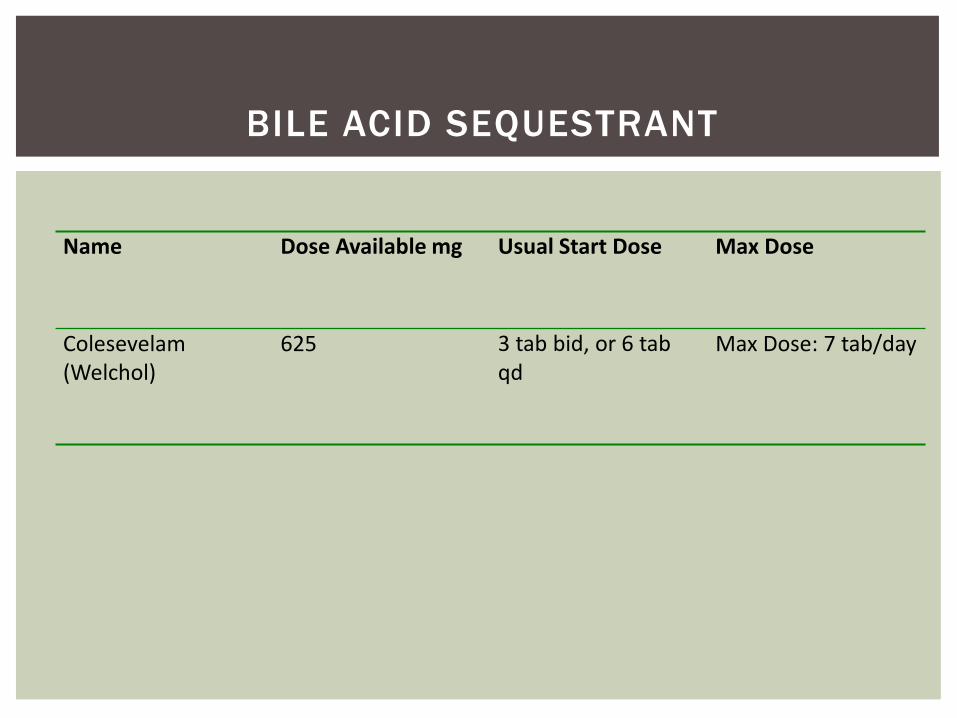
Name Dose Available mg Usual Start Dose Max Dose
Colesevelam(Welchol)
625 3 tab bid, or 6 tab qd
Max Dose: 7 tab/day
BILE ACID SEQUESTRANT
Synthetic dopamine agonist. The mechanism of action is not understood but thought that stimulating dopamine receptors in the brain at certain times of the day “resets” the biological clock and improves metabolism.
DOPAMINE AGONIST
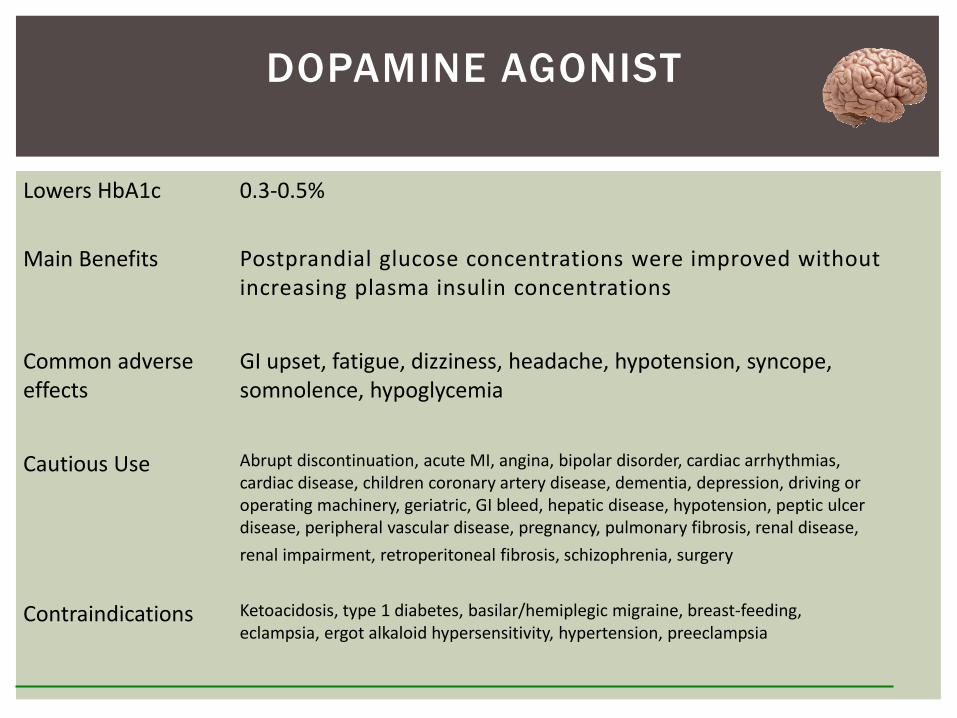
Lowers HbA1c 0.3-0.5%
Main Benefits Postprandial glucose concentrations were improved without increasing plasma insulin concentrations
Common adverse effects
GI upset, fatigue, dizziness, headache, hypotension, syncope, somnolence, hypoglycemia
Cautious Use Abrupt discontinuation, acute MI, angina, bipolar disorder, cardiac arrhythmias, cardiac disease, children coronary artery disease, dementia, depression, driving or operating machinery, geriatric, GI bleed, hepatic disease, hypotension, peptic ulcer disease, peripheral vascular disease, pregnancy, pulmonary fibrosis, renal disease, renal impairment, retroperitoneal fibrosis, schizophrenia, surgery
Contraindications Ketoacidosis, type 1 diabetes, basilar/hemiplegic migraine, breast-feeding, eclampsia, ergot alkaloid hypersensitivity, hypertension, preeclampsia
DOPAMINE AGONIST
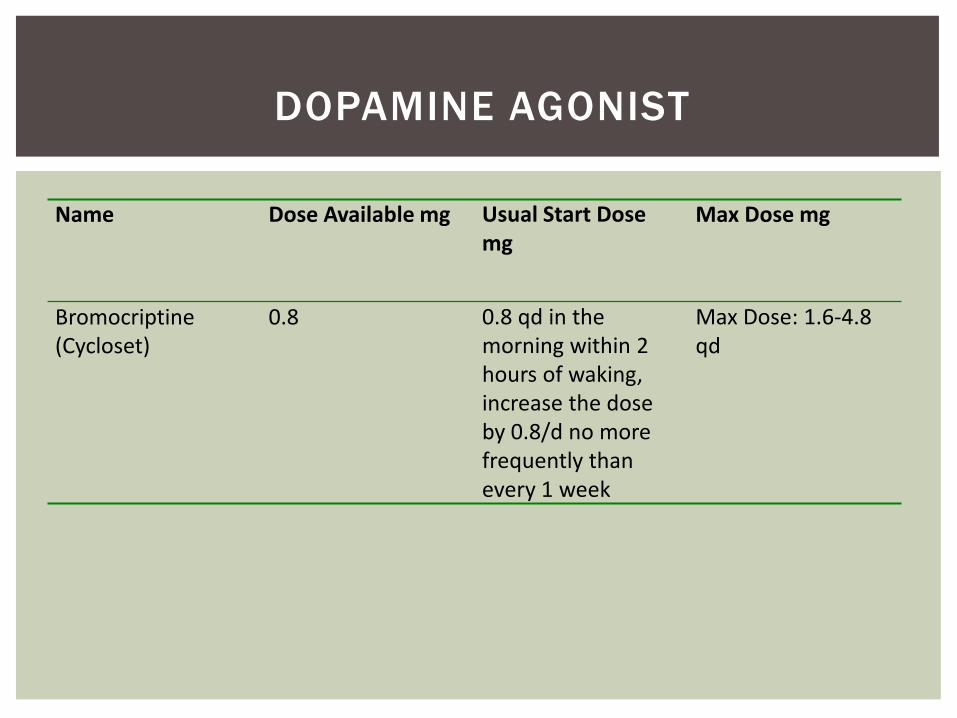
Name Dose Available mg Usual Start Dose Max Dose mgmg
Bromocriptine(Cycloset)
0.8 0.8 qd in the morning within 2 hours of waking, increase the dose by 0.8/d no more frequently than every 1 week
Max Dose: 1.6-4.8 qd
DOPAMINE AGONIST
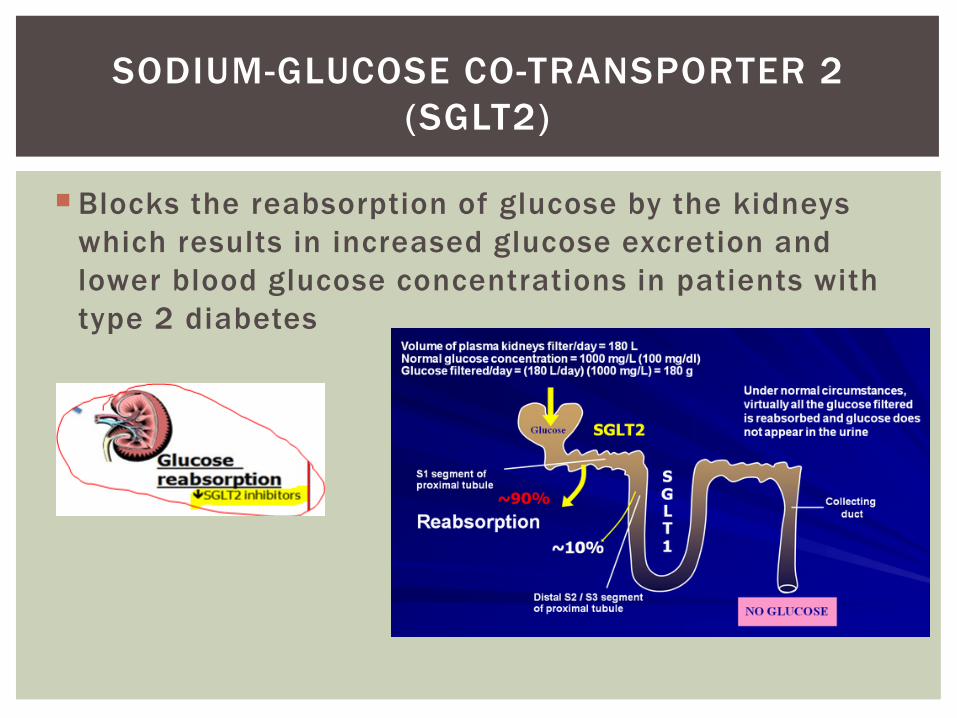
Blocks the reabsorption of glucose by the kidneys which results in increased glucose excretion and lower blood glucose concentrations in patients with type 2 diabetes
SODIUM-GLUCOSE CO-TRANSPORTER 2 (SGLT2)
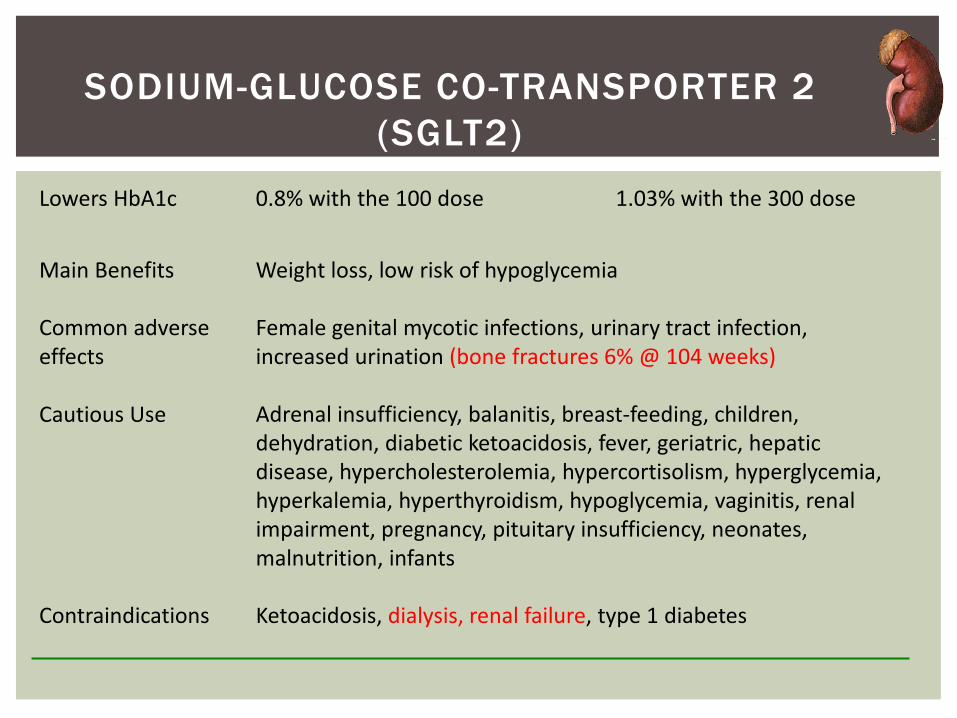
Lowers HbA1c 0.8% with the 100 dose 1.03% with the 300 dose
Main Benefits Weight loss, low risk of hypoglycemia
Common adverse effects
Female genital mycotic infections, urinary tract infection, increased urination (bone fractures 6% @ 104 weeks)
Cautious Use Adrenal insufficiency, balanitis, breast-feeding, children, dehydration, diabetic ketoacidosis, fever, geriatric, hepatic disease, hypercholesterolemia, hypercortisolism, hyperglycemia, hyperkalemia, hyperthyroidism, hypoglycemia, vaginitis, renal impairment, pregnancy, pituitary insufficiency, neonates, malnutrition, infants
Contraindications Ketoacidosis, dialysis, renal failure, type 1 diabetes
SODIUM-GLUCOSE CO-TRANSPORTER 2 (SGLT2)
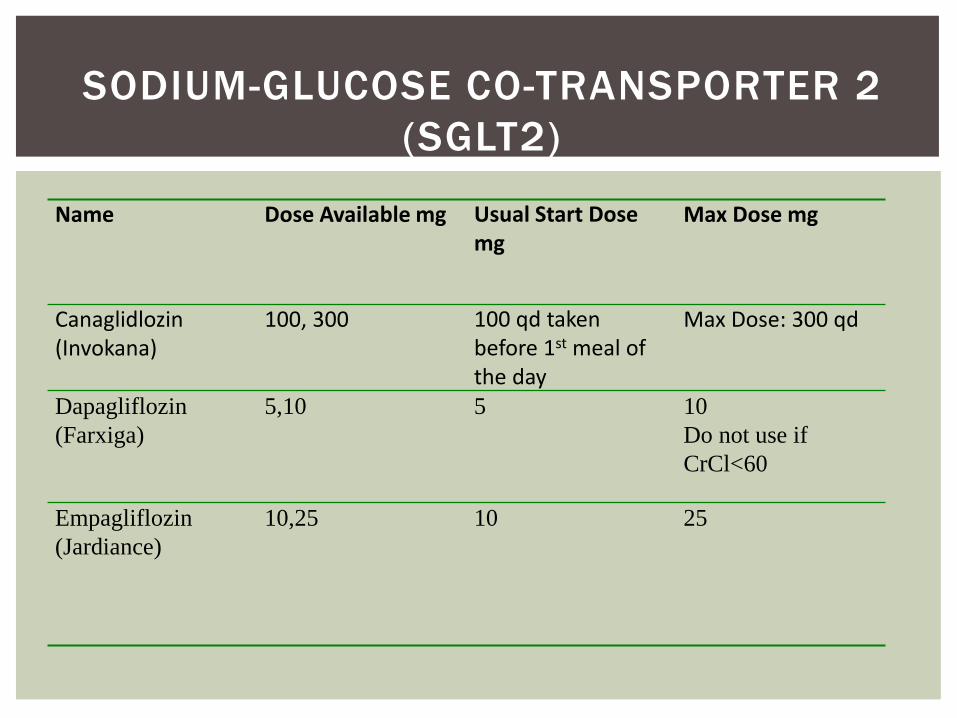
Name Dose Available mg Usual Start Dose Max Dose mgmg
Canaglidlozin(Invokana)
100, 300 100 qd taken before 1st meal of the day
Max Dose: 300 qd
Dapagliflozin(Farxiga)
5,10 5 10Do not use if CrCl<60
Empagliflozin(Jardiance)
10,25 10 25
SODIUM-GLUCOSE CO-TRANSPORTER 2 (SGLT2)
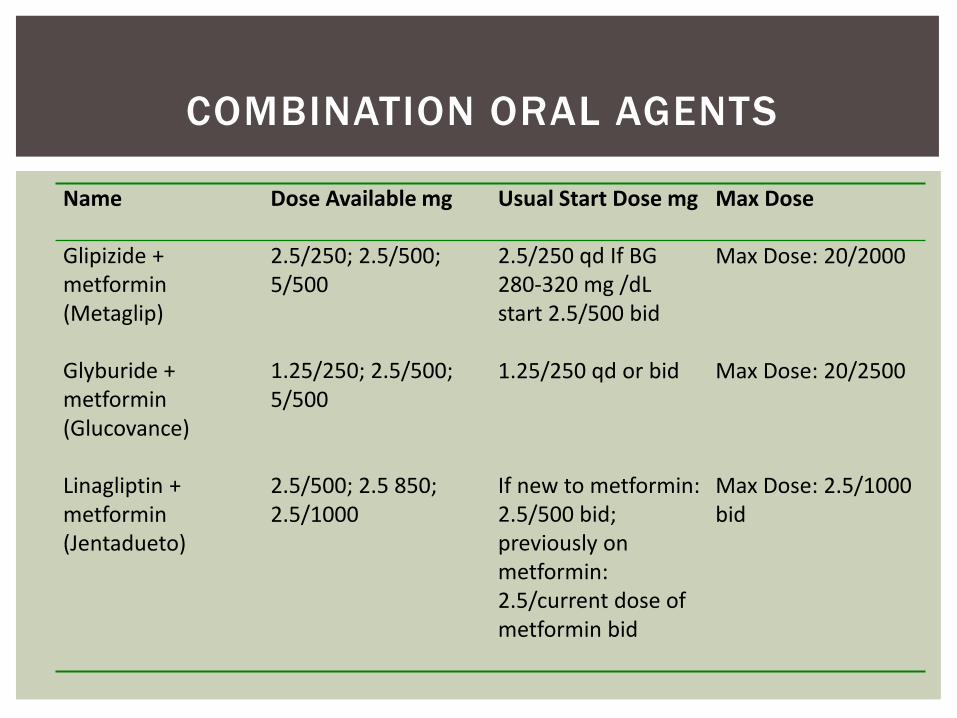
Name Dose Available mg Usual Start Dose mg Max Dose
Glipizide + metformin (Metaglip)
2.5/250; 2.5/500; 5/500
2.5/250 qd If BG 280-320 mg /dL start 2.5/500 bid
Max Dose: 20/2000
Glyburide + metformin (Glucovance)
1.25/250; 2.5/500; 5/500
1.25/250 qd or bid Max Dose: 20/2500
Linagliptin + metformin(Jentadueto)
2.5/500; 2.5 850; 2.5/1000
If new to metformin: 2.5/500 bid; previously on metformin: 2.5/current dose of metformin bid
Max Dose: 2.5/1000 bid
COMBINATION ORAL AGENTS
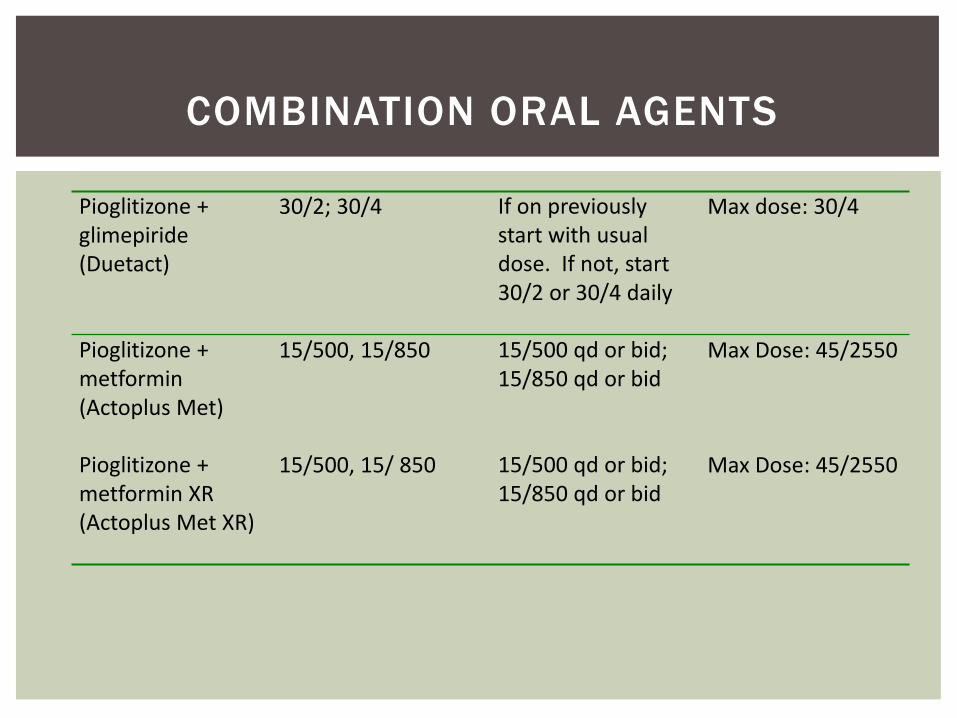
Pioglitizone + 30/2; 30/4 If on previously Max dose: 30/4glimepiride start with usual (Duetact) dose. If not, start
30/2 or 30/4 daily
Pioglitizone + metformin (Actoplus Met)
15/500, 15/850 15/500 qd or bid; 15/850 qd or bid
Max Dose: 45/2550
Pioglitizone + metformin XR(Actoplus Met XR)
15/500, 15/ 850 15/500 qd or bid; 15/850 qd or bid
Max Dose: 45/2550
COMBINATION ORAL AGENTS
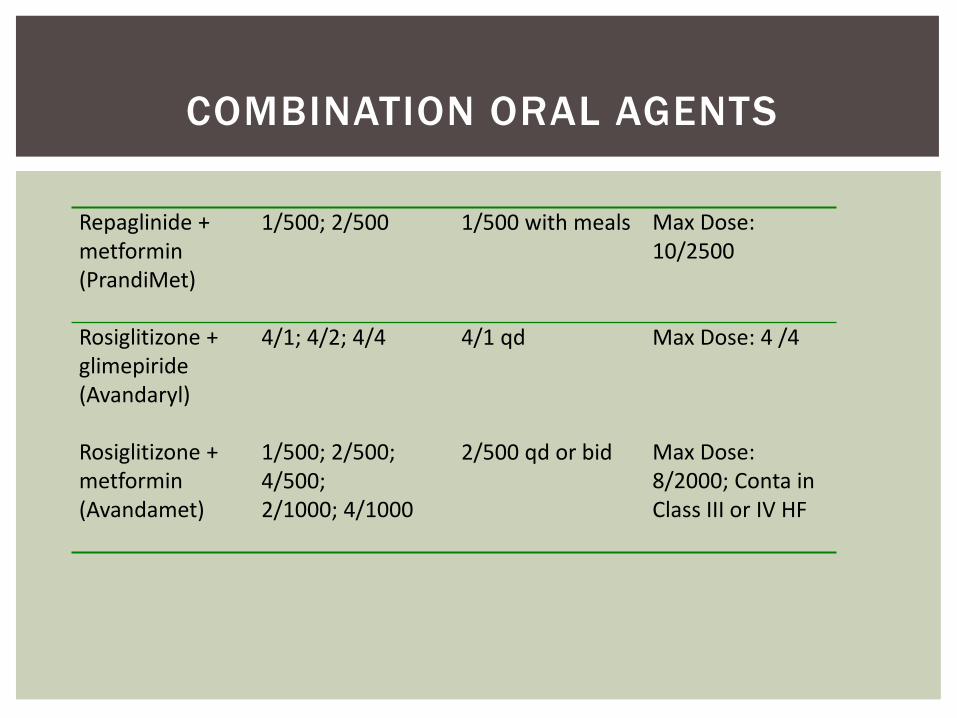
Repaglinide + 1/500; 2/500 1/500 with meals Max Dose: metformin 10/2500(PrandiMet)
Rosiglitizone + glimepiride (Avandaryl)
4/1; 4/2; 4/4 4/1 qd Max Dose: 4 /4
Rosiglitizone + metformin (Avandamet)
1/500; 2/500; 4/500; 2/1000; 4/1000
2/500 qd or bid Max Dose: 8/2000; Conta in Class III or IV HF
COMBINATION ORAL AGENTS
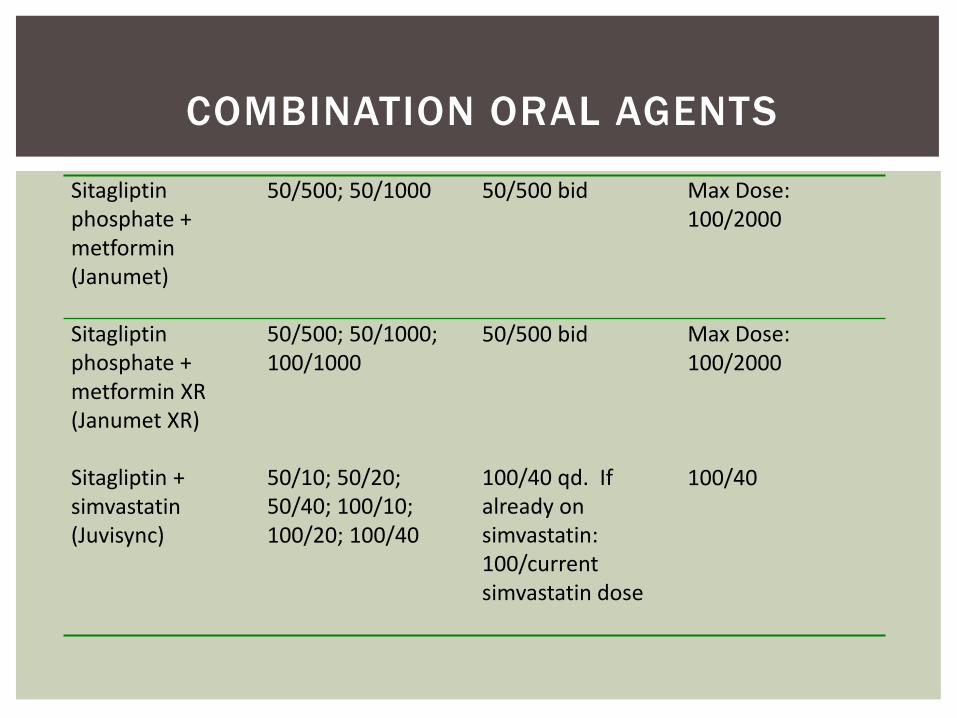
Sitagliptin 50/500; 50/1000 50/500 bid Max Dose: phosphate + 100/2000metformin (Janumet)
Sitagliptin phosphate + metformin XR(Janumet XR)
50/500; 50/1000; 100/1000
50/500 bid Max Dose: 100/2000
Sitagliptin + simvastatin(Juvisync)
50/10; 50/20; 50/40; 100/10; 100/20; 100/40
100/40 qd. If already on simvastatin: 100/current simvastatin dose
100/40
COMBINATION ORAL AGENTS
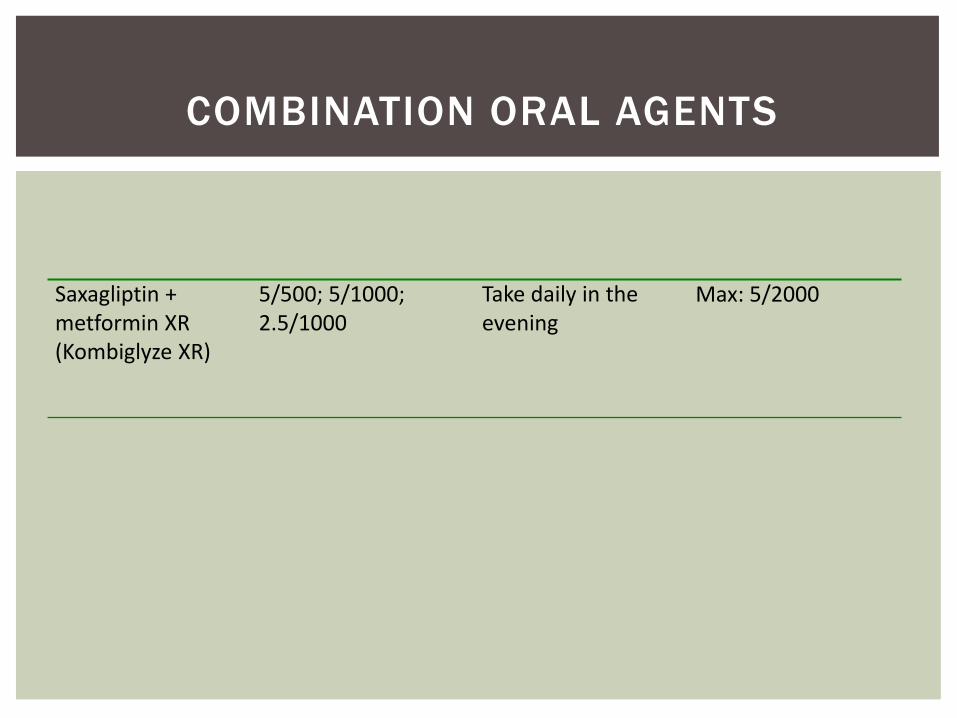
Saxagliptin + 5/500; 5/1000; Take daily in the Max: 5/2000metformin XR 2.5/1000 evening(Kombiglyze XR)
COMBINATION ORAL AGENTS
Glycemic targets & BG-lowering therapies must be individualized.
Diet, exercise, & education: foundation of any T2DM therapy program
Unless contraindicated, metformin = optimal 1st-line drug.
After metformin, data are limited. Combination therapy with 1-2 other oral / injectable agents is reasonable; minimize side effects.
KEY POINTS (ADA-EASD)DIABETES CARE, DIABETOLOGIA . 19 APRIL 201 2
Ultimately, many patients will require insulin therapy alone / in combination with other agents to maintain BG control.
All treatment decisions should be made in conjunction with the patient (focus on preferences, needs & values.)
Comprehensive CV risk reduction - a major focus of therapy.
KEY POINTS (CONT)
QUESTIONS?