oral health overview - legislative news, studies and … · oral health overview 2 introduction...
TRANSCRIPT

Oral Health Overview
Oral Health Overview
Health Care Safety-Net Toolkit for Legislators

Oral Health Overview
2
Introduction
Good oral health is key to good overall health, yet millions of Americans lack access to basic, affordable oral health care. Large-ly preventable, poor oral health can negatively impact quality of life by affecting speech, nutrition, growth and social develop-ment. Growing evidence links oral diseases to health conditions such as diabetes, heart and lung disease, and potential pregnan-cy complications.
If untreated, certain oral health conditions can lead to chronic pain, missed days of school and work, inappropriate use of emergency depart-ments, and even death. Poor oral health results in poor overall health for many Americans—at a substantial cost to society. The American public, health care providers, and policymakers have long considered oral care less important than other medical health needs. This outlook, combined with a general lack of public understanding and awareness of the importance of oral health, contribute to the current state of oral health in the United States.
Oral Health DisparitiesThe 2000 report, Oral Health in America: A Re-port of the Surgeon General, found that, despite significant improvements in Americans’ oral health since the 1970s, gaps and disparities persist in ac-cess and care.
Oral health care eludes many of the nation’s most vulnerable and underserved populations, includ-ing children and older adults, low-income people, racial and ethnic minorities, pregnant women, and those living in underserved areas, among others. Residents of underserved areas—whether rural or urban—also disproportionately suffer from oral health conditions.
Dental caries, commonly known as tooth decay, for example, is the most common chronic illness among children in the United States. According to the surgeon general’s report, tooth decay is five times more common than asthma among children between the ages of 5 and 17. Children of poor families are even more likely than their peers to experience dental disease. This group is more than twice as likely to have tooth decay and the disease often is more severe, yet more than a quarter of poor children have not visited a dentist in the past year.

Health Care Safety-Net Toolkit for Legislators
3
What Legislators Need to Know About Oral Health
• Tooth decay is largely preventable, yet remains one of the most common chronic conditions in the United States.
• Poor oral health affects overall health and can increase the risk of heart and lung disease, diabetes and pregnancy complications.
• More than 47 million Americans live in areas where there is a shortage of oral health providers.
• Tooth decay is the most common chronic disease for children—five times more common than asthma.
• About one in five low-income children do not receive dental care each year.
• Children, the elderly, low-income residents, and racial and ethnic minorities disproportionately suffer from oral health conditions.
• Medical insurance is a strong predictor of access to dental care.
• About 130 million Americans do not have dental insurance coverage and, in 2011, nearly one in eight cited cost as a reason for forgoing dental care.
• For every adult without health insurance, approximately three do not have dental insurance.
• Medicaid and CHIP must provide dental coverage for children; adult dental insurance is optional.
• States are using a variety of policy options to improve oral health care for their citizens.
Oral Health Overview
4
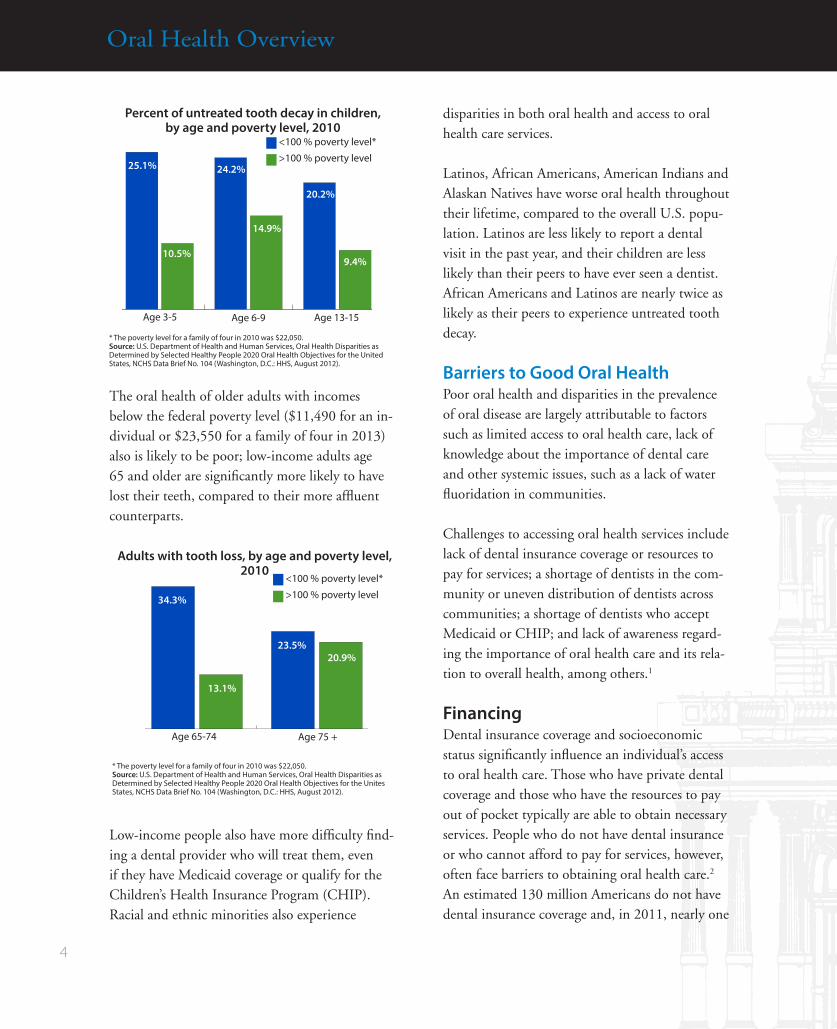
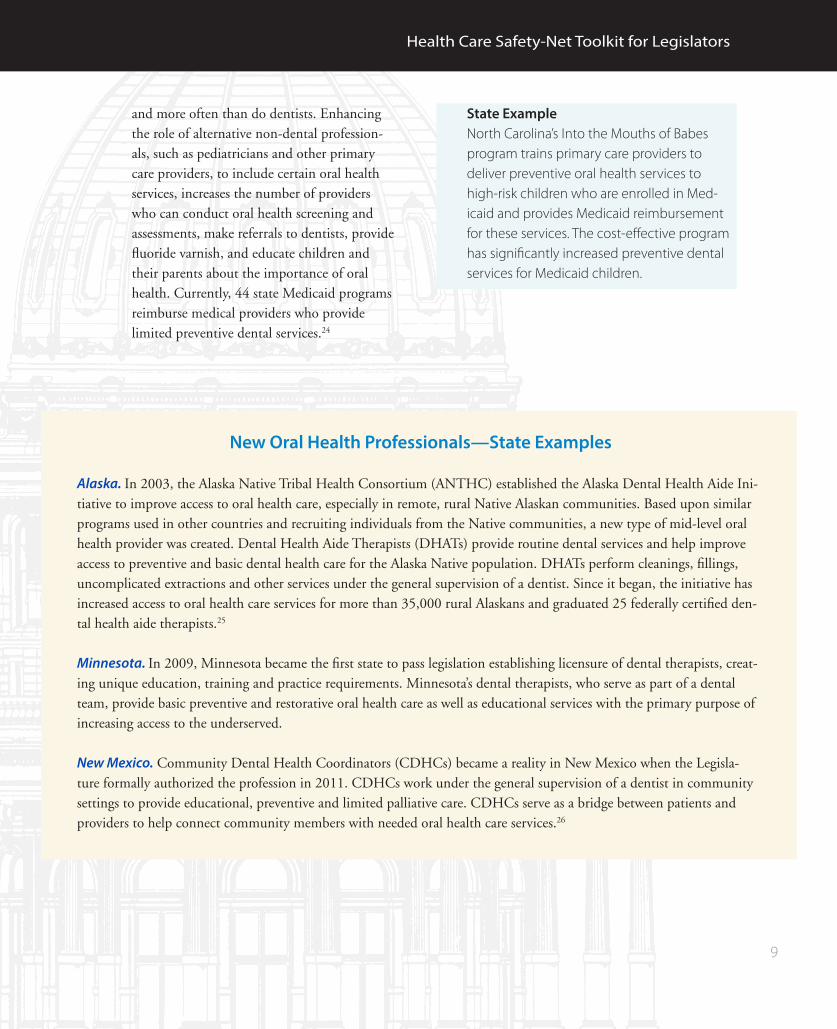
The oral health of older adults with incomes below the federal poverty level ($11,490 for an in-dividual or $23,550 for a family of four in 2013) also is likely to be poor; low-income adults age 65 and older are significantly more likely to have lost their teeth, compared to their more affluent counterparts.
Low-income people also have more difficulty find-ing a dental provider who will treat them, even if they have Medicaid coverage or qualify for the Children’s Health Insurance Program (CHIP).Racial and ethnic minorities also experience
disparities in both oral health and access to oral health care services. Latinos, African Americans, American Indians and Alaskan Natives have worse oral health throughout their lifetime, compared to the overall U.S. popu-lation. Latinos are less likely to report a dental visit in the past year, and their children are less likely than their peers to have ever seen a dentist. African Americans and Latinos are nearly twice as likely as their peers to experience untreated tooth decay.
Barriers to Good Oral HealthPoor oral health and disparities in the prevalence of oral disease are largely attributable to factors such as limited access to oral health care, lack of knowledge about the importance of dental care and other systemic issues, such as a lack of water fluoridation in communities.
Challenges to accessing oral health services include lack of dental insurance coverage or resources to pay for services; a shortage of dentists in the com-munity or uneven distribution of dentists across communities; a shortage of dentists who accept Medicaid or CHIP; and lack of awareness regard-ing the importance of oral health care and its rela-tion to overall health, among others.1
Financing Dental insurance coverage and socioeconomic status significantly influence an individual’s access to oral health care. Those who have private dental coverage and those who have the resources to pay out of pocket typically are able to obtain necessary services. People who do not have dental insurance or who cannot afford to pay for services, however, often face barriers to obtaining oral health care.2 An estimated 130 million Americans do not have dental insurance coverage and, in 2011, nearly one
Percent of untreated tooth decay in children, by age and poverty level, 2010
0
5
10
15
20
25
30
13-156-93-5
<100 % poverty level*
>100 % poverty level
Age 3-5 Age 6-9 Age 13-15
* The poverty level for a family of four in 2010 was $22,050.Source: U.S. Department of Health and Human Services, Oral Health Disparities as Determined by Selected Healthy People 2020 Oral Health Objectives for the United States, NCHS Data Brief No. 104 (Washington, D.C.: HHS, August 2012).
25.1%
10.5%
24.2%
14.9%
20.2%
9.4%
<100 % poverty level*
>100 % poverty level
Adults with tooth loss, by age and poverty level, 2010
* The poverty level for a family of four in 2010 was $22,050.Source: U.S. Department of Health and Human Services, Oral Health Disparities as Determined by Selected Healthy People 2020 Oral Health Objectives for the Unites States, NCHS Data Brief No. 104 (Washington, D.C.: HHS, August 2012).
Age 65-74 Age 75 +0
5
10
15
20
25
30
35above
below
75+65-74
34.3%
13.1%
23.5%20.9%

Health Care Safety-Net Toolkit for Legislators
5
in eight cited cost as a reason for forgoing dental care. 3, 4
Medicaid and the Children’s Health Insurance Program help fill the dental insurance gap by providing coverage for certain low-income, under-served people. States must provide comprehensive dental services for children and pregnant women who are enrolled in Medicaid; coverage for other adults is optional, however. While most states cover emergency dental services for adult enroll-ees, less than half currently offer comprehensive services.5 In addition, women who gain Medicaid coverage and access to dental services while pregnant gener-ally lose coverage postpartum. Thus, many—especially low-income—adults lack necessary preventive or essential oral health treatment.
As many states expand Medic-aid and as state health insur-ance exchanges come online in 2014 under the Affordable Care Act, millions of unin-sured adults and children will gain both public and private
health insurance coverage. Existing gaps in dental coverage will remain largely unchanged, how-ever. The law requires qualified health plans in health insurance exchanges and Medicaid to offer “benchmark” plans that cover a minimum set of benefits. While oral health care is included as one of these “essential health benefits” for children, it is not for adults.6 In addition, exchanges may choose to bundle dental insurance with medical cover-age or to offer a separate dental plan altogether. If an exchange offers a separate dental plan, then medical insurance plans in the exchange need not include dental benefits. Nor, under federal law, must individuals or employers buy the stand-alone dental coverage. Therefore, many who gain medical insurance will continue to go without oral health coverage.7
Even those who currently have dental insurance through Medicaid are not guaranteed access to care. According to the Centers for Medicare and Medicaid Services, about 40 percent of Medicaid-enrolled children received dental services in 2010.8 While many Medicaid beneficiaries rely on safety-net providers (discussed below) for care, many also experience difficulty finding a provider who
<100 % poverty level*
>100 % poverty level
0
10
20
30
40
50
60above 100
below100
45-6425-44
Adult tooth retention, by age and poverty level, 2010
* The poverty level for a family of four in 2010 was $22,050.Source: U.S. Department of Health and Human Services, Oral Health Disparities as Determined by Selected Healthy People 2020 Oral Health Objectives for the United States, NCHS Data Brief No. 104 (Washington, D.C.: HHS, August 2012).
Age 25-44 Age 45-64
42.0%
55.4%
15.2%
31.6%
Geographic variation in the percentage of children receiving preventive dental services, FFY 2010
Source: Department of Health and Human Services, 2012 Annual Report on the Quality of Care for Children in Medicaid and CHIP, Health and Human Services Secretary Kathleen Sebelius, December 2012.
DC
47% to 58% (Top Quartile)
43% to 46%
37% to 41%
7% to 36% (Bottom Quartile)

Oral Health Overview
6
will accept public insurance. The Government Accountability Office reports that, in 25 states, less than half of dentists treat Medicaid recipi-ents.9 Providers cite low reimbursement rates and substantial administrative barriers as reasons for choosing not to participate in Medicaid.10
The Oral Health Safety Net Due to barriers to accessing private oral health care, many low-income, underserved people rely on the oral health “safety net” for services. In contrast to the notion of a coordinated “net” of providers that serve those who do not have access to the private health system, the dental safety net consists of various unrelated providers who play a part in providing services to the under-insured and uninsured. These providers include, but are not limited to, Federally Qualified Health Centers (FQHCs), FQHC look-alikes, other community health centers, dental schools, school-based health centers, mobile clinics, state and local health departments, and, often, costly hospital emergency departments. The scope of services provided and the number of patients served varies significantly by provider. Yet, even collectively, the safety net is unable to meet the oral health needs of the mil-lions of Americans who cannot access the private system.11
Oral Health Workforce A shortage of dentists, compounded by the uneven distribution of providers across the nation, makes it difficult for many Americans to access oral health care. In 2012, more than 47 million Ameri-cans lived in areas designated as having a shortage of dental professionals. Because dentists are heavily concentrated in urban areas, inner cities and rural communities often may have few available ser-vices.12 An additional 6,600 dentists are needed to address this shortage, according to the Health Resources and Services Administration, yet too
few dentists graduate from dental school to replace even the practitioners who retire each year.13 The shortage and geographical distribution of provid-ers make it difficult for those in underserved areas to access timely care, regardless of their insurance status.
Policy Options for States to Consider and State ExamplesStates play a key role in improving oral health. Many are pursuing a wide range of policies and exploring the potential of innovative models to address these problems.
Oral Health Literacy. Through media awareness campaigns, states are educating their citizens about the importance of oral health care and how to access it. Helping people understand the need for preventive services and sharing best practices for preventing oral diseases—before problems occur—empowers people to improve their oral health.
State Examples In 2008, Delaware’s Division of Public Health launched First Smile Delaware, a campaign to raise awareness, decrease the prevalence of den-tal disease, and inspire providers to focus on oral health issues in order to improve oral and overall health of children. Nearly 50 key partners were participating in the campaign as of 2012.14
Vermont’s Tooth Tutor Dental Access Program educates school children and aims to ensure every child has access to oral health care by connecting them with a dental home—creat-ing an ongoing relationship between a dentist and a child or family, in which the child receives comprehensive, accessible and coordinated care. Nearly three-quarters of children at participating schools were connected to a dental home dur-ing the 2008-09 school year.15

Health Care Safety-Net Toolkit for Legislators
7
Water Fluoridation. Research indicates that fluoridated water not only helps prevent tooth decay and other serious oral health conditions, but also yields a high return on investment—$38 in savings on the cost of dental treatment for every $1 spent.16 Nearly three-quarters of Americans currently have access to fluoridated water, yet around 100 million live in communities without fluoridation. While fluoridation policies generally are made at the community level, laws in 12 states and the District of Columbia currently require fluoridated water under certain circumstances. Forty-three of the nation’s 50 largest cities fluori-date their water.17
State ExamplesAt least eight states—Arkansas, California, Con-necticut, Louisiana, Nebraska, Nevada, Ohio and South Dakota—require water facilities that serve a specified number of people to comply with water fluoridation regulations.18
The Colorado General Assembly established a grant program to help communities ensure that water systems provide appropriate levels of fluo-ride, subject to appropriations.19
Insurance Coverage and Provider Participation. Medicaid and CHIP help fill the gap in dental insurance; together, they serve as the primary sources of dental coverage for underserved people and account for the bulk of public spend-ing on oral health care. Some states have expanded dental coverage to require a minimum dental ben-efit for adult Medicaid beneficiaries. Others have looked to increase oral health provider participa-tion in Medicaid by increasing reimbursement rates and/or reducing administrative barriers.
State ExamplesBetween 2000 and 2005, Alabama, Michigan, South Carolina, Tennessee and Virginia increased Medicaid reimbursement rates and reduced administrative barriers for dental providers. The rate of increase and type of administrative reforms varied by state, yet the results were strikingly similar: provider participation increased substantially—anywhere from 62 percent to 150 percent—as did the percentage of Medicaid-covered children who accessed oral health services.20
Addressing Workforce Shortages. States are exploring and implementing a variety of policies to expand the oral health workforce.
• Increase Supply of Dentists. To better match the supply of dentists with the demand for oral health care, states are enhancing educa-tion opportunities; recruiting students from low-income, minority and rural communi-ties; and providing financial support for those who are willing to work in underserved areas. Bridge and pipeline programs, for example, often target underserved minority, rural and low-income students with outreach activities, community-based educational opportunities and financial support. In addition, 35 states, the District of Columbia and the federal government offer financial incentives in the form of loan repayment programs for dentists who agree to work in an underserved area for a specific period of time.
State ExamplesEstablished with funding from the North Carolina General Assembly, the East Caro-lina University School of Dental Medicine aims to address the state’s shortage and distribution of dentists by recruiting North

Oral Health Overview
8
Carolinians from underrepresented groups and underserved areas. The relatively new program—its inaugural class matriculated in 2011—plans to build 10 service learning centers in underserved and rural areas to train dental students and residents while serving as a safety net for the state’s vulner-able populations.
In 2013, the Mississippi Legislature estab-lished the Rural Dentists Program and an associated scholarship fund to identify quali-fied university and college students from rural areas for dental school matriculation.
A 2008 Maine law offers tax incentives to dentists who practice in underserved areas.
• Expand Scope of Practice. By expanding scope of practice laws for certain dental pro-fessionals, such as hygienists and dental assis-tants, states enable a wider range of oral health professionals to treat patients and to perform more procedures independently.21 Many states, for example, have expanded the services dental hygienists can perform for underserved populations. According to the American Dental Hygienists’ Association, 35 states allow dental hygienists to provide certain preven-tive services without direct supervision of a dentist. Fifteen states allow direct Medicaid reimbursement to hygienists.22
State Example In 2013, Nevada passed legislation autho-
rizing a licensed dental hygienist, who has been endorsed to practice public health dental hygiene, to perform a variety of ser-vices without the approval or supervision of a licensed dentist.
• Create New, Mid-Level Oral Health Professionals. Another strategy states are exploring is creating a new type of dental health professional. While Alaska and Min-nesota are the only states that currently license these mid-level oral health providers—whose role is similar to that of a nurse practitioner in the medical field—numerous others are considering similar legislation. Dental thera-pists, for example, work on-site with a dentist, serving low-income, uninsured and under-served patients, or in areas where a shortage of providers exists. They provide a wide range of preventive and restorative services. Dental therapists and other similar providers help im-prove access to care by increasing the number of patients for whom they can provide preven-tive care, thus freeing dentists to devote their time for more advanced procedures.
Although some dentists have expressed
concern about consumer safety issues or the effect these new providers might have on their practices, research indicates dentists are able to serve more patients and improve their financial bottom line by adding a mid-level provider to their team.23
State Examples Alaska and Minnesota currently license mid-
level oral health providers. (See New Oral Health Professionals—State Examples box for more information.)
• Enhance the Role of Primary Care Provid-ers. States increasingly are looking to primary care providers to help improve oral health. Pediatricians, for example, are in a prime position to provide oral health screening and offer certain preventive services and referrals for children, who they see at a younger age
Health Care Safety-Net Toolkit for Legislators
9
and more often than do dentists. Enhancing the role of alternative non-dental profession-als, such as pediatricians and other primary care providers, to include certain oral health services, increases the number of providers who can conduct oral health screening and assessments, make referrals to dentists, provide fluoride varnish, and educate children and their parents about the importance of oral health. Currently, 44 state Medicaid programs reimburse medical providers who provide limited preventive dental services.24
New Oral Health Professionals—State Examples
Alaska. In 2003, the Alaska Native Tribal Health Consortium (ANTHC) established the Alaska Dental Health Aide Ini-tiative to improve access to oral health care, especially in remote, rural Native Alaskan communities. Based upon similar programs used in other countries and recruiting individuals from the Native communities, a new type of mid-level oral health provider was created. Dental Health Aide Therapists (DHATs) provide routine dental services and help improve access to preventive and basic dental health care for the Alaska Native population. DHATs perform cleanings, fillings, uncomplicated extractions and other services under the general supervision of a dentist. Since it began, the initiative has increased access to oral health care services for more than 35,000 rural Alaskans and graduated 25 federally certified den-tal health aide therapists.25
Minnesota. In 2009, Minnesota became the first state to pass legislation establishing licensure of dental therapists, creat-ing unique education, training and practice requirements. Minnesota’s dental therapists, who serve as part of a dental team, provide basic preventive and restorative oral health care as well as educational services with the primary purpose of increasing access to the underserved.
New Mexico. Community Dental Health Coordinators (CDHCs) became a reality in New Mexico when the Legisla-ture formally authorized the profession in 2011. CDHCs work under the general supervision of a dentist in community settings to provide educational, preventive and limited palliative care. CDHCs serve as a bridge between patients and providers to help connect community members with needed oral health care services.26
State Example North Carolina’s Into the Mouths of Babes
program trains primary care providers to deliver preventive oral health services to high-risk children who are enrolled in Med-icaid and provides Medicaid reimbursement for these services. The cost-effective program has significantly increased preventive dental services for Medicaid children.

Oral Health Overview
10
Federal ActionThe U.S. Department of Health and Human Ser-vices (HHS) supports a wide range of oral health activities through the Oral Health Initiative. Included are oral health financing, research, work-force development, public health action, quality initiatives and a focus on technology. Within HHS, the Health Resources and Services Admin-istration (HRSA), offers loans, scholarships, loan repayment and workforce development programs for oral health care providers.27 HRSA’s State Oral Health Workforce Program helps states develop and implement innovative programs to improve the dental workforce in areas where a shortage of dental health professionals exists.28 In addition, HRSA’s Title V program (MCH Block Grant) pro-vides financial support to states to establish public health programs for oral health service delivery, as well as disease monitoring and surveillance activi-ties.29
The Centers for Disease Control and Prevention also provides support to states through funding for oral health programs, training and technical assistance, information and resources.30 HHS also administers programs such as Federally Qualified
Health Centers, the Indian Health Service and, through CMS, provides financing for oral health services under Medicaid and CHIP.
Finally, the Affordable Care Act contains various provisions related to oral health. These range from defining children’s oral health services as an essen-tial health benefit to prohibiting insurance plans from imposing copayments for certain preventive services and authorizing various infrastructure, surveillance, prevention and treatment programs. Many authorized initiatives remain unfunded, however.
ConclusionStates play a key role in improving oral health. Through a wide variety of policies, state lawmak-ers can improve access to oral health care, thus improving not only oral health, but also the overall health of residents. As evidenced by states’ experi-ences, increasing access to oral health services, improving oral health literacy and addressing other systemic challenges effectively helps reduce health disparities and the unnecessary costs associated with preventable oral health conditions.
For More Information: Oral Health Resources
NCSL, Children’s Oral Health resources http://www.ncsl.org/default.aspx?tabid=14495
CDC, Division of Oral Health, www.cdc.gov/OralHealth/index.htm
HRSA, Oral Health, www.hrsa.gov/publichealth/clinical/oralhealth/index.html
HRSA, State Oral Health Workforce, http://bhpr.hrsa.gov/grants/dentistry/index.html
HHS Oral Health Initiative 2010, www.hrsa.gov/publichealth/clinical/oralhealth/hhsinitiative.html

Health Care Safety-Net Toolkit for Legislators
11
Notes 1. Institute of Medicine and National Research Council, Improving access to oral health care for vulner-able and underserved populations, 57. 2. Ibid., 193. 3. Ibid., 198. 4. Centers for Disease Control and Prevention and National Center for Health Statistics, National Health Interview Survey, Table 79. 5. Medicaid.gov, Dental Care. 6. CMS.gov and the Center for Consumer In-formation and Insurance Oversight, Essential Health Benefits Standards: Ensuring Quality, Affordable Cover-age (Washington, D.C.: CMS, 2013), www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/ehb-2-20-2013.html. 7. Jennifer Wheeler and Tara Lubin, States Imple-ment Health Reform: Oral Health (Denver: National Conference of State Legislatures, 2011). 8. Ellen Bouchery, Medicaid Policy Brief: Utiliza-tion of Dental Services Among Medicaid Enrolled Chil-dren, Brief 9, prepared for the Centers for Medicare and Medicaid Services (Princeton, N.J.: Mathematica Policy Research, 2012). 9. U.S. Government Accountability Office, Efforts Underway to Improve Children’s Access to Dental Services, But Sustained Attention Needed to Address Ongoing Concerns, GAO-11-96 (Washington, D.C.: U.S. GAO, November 2010), www.gao.gov/new.items/d1196.pdf. 10. U.S. Department of Health and Human Services, Oral Health in America: A Report of the Surgeon General; and Centers for Medicare and Medicaid Ser-vices, Center for Medicaid, CHIP and Survey and Cer-tification, Medicaid/Chip Oral Health Services Fact Sheet (Washington, D.C.: CMS, 2010), http://medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Ben-efits/Downloads/2010-Dental-Factsheet.pdf. 11. Institute of Medicine and National Research Council, Improving access to oral health care for vulner-able and underserved populations,162. 12. Ibid., 91. 13. The Pew Charitable Trusts, Help Wanted: A Policy Maker’s Guide to New Dental Providers (Washing-ton D.C.: The Pew Charitable Trusts, 2009). 14. Delaware Health and Social Services, Division of Public Health; for more information, see First Smile Delaware at http://dhss.delaware.gov/dph/hsm/ohp-firstsmilede.html. 15. Vermont Department of Health; for more information, see Tooth Tutor Dental Access Program at http://healthvermont.gov/family/dental/tooth-tutor.aspx. 16. Centers for Disease Control and Prevention, Community Water Fluoridation: Fluoridation Basics (Washington, D.C.: CDC, 2012), www.cdc.gov/fluori-dation/benefits/background.htm.
17. The Pew Charitable Trusts, Water Fluoridation: Frequently Asked Questions (Washington, D.C.: Pew), 2011), www.pewstates.org/research/analysis/water-fluoridation-frequently-asked-questions-85899379776. 18. NCSL original research by Megan Comlossy, May 2013. 19. Colo. Rev. Stat. § 25-21.5-108. 20. Alison Borchgrevink, Andrew Snyder, and Shelly Gehshan, Issue Brief: Increasing Access to Dental Care in Medicaid: Does Raising Provider Rates Work? (Oakland, Calif.: California HealthCare Founda-tion, 2008), www.chcf.org/~/media/MEDIA%20LIBRARY%20Files/PDF/I/PDF%20IncreasingAccess-ToDentalCareInMedicaidIB.pdf. 21. Institute of Medicine and National Research Council, Improving access to oral health care for vulner-able and underserved populations, 6. 22. American Dental Hygienists’ Association, Facts about the Dental Hygiene Workforce in the United States (Chicago, Ill.: ADHA, 2012), www.adha.org/resources-docs/75118_Facts_About_the_Dental_Hygiene_Work-force.pdf. 23. The Pew Charitable Trusts, Expansion of the Dental Workforce: Frequently Asked Questions (2012): www.pewstates.org/research/analysis/expansion-of-the-dental-workforce-frequently-asked-ques-tions-85899381323. 24. American Academy of Pediatrics, More State Medicaid Programs Pay for Children’s Oral Health Preven-tion Services in Doctors’ Offices (Washington, D.C.: AAP, 2013), www2.aap.org/oralhealth/docs/CelebratingOur-Wins.pdf. 25. DENTEX Dental Health Aide Therapist Program, http://depts.washington.edu/dentexak/who-we-are/history/. 26. Karen Fox, “New Mexico First State to Autho-rize ADA’s CDHC model,” ADA News, May 2, 2011, www.ada.org/news/5769.aspx. 27. Health Resources and Service Administration, Oral Health Workforce (Washington, D.C.: HRSA, 2013), www.hrsa.gov/publichealth/clinical/oralhealth/workforce.html. 28. Health Resources and Service Administration, State Oral Health Workforce (Washington, D.C.: HRSA, 2013), http://bhpr.hrsa.gov/grants/dentistry/sohw.html. 29. As part of the Oral Health Initiative, the Centers for Disease control and Prevention and the National Institutes of Health also collaborate on sur-veillance activities through the National Oral Health Surveillance Plan. 30. Centers for Disease Control and Prevention, Division of Oral Health, Oral Health Resources (Wash-ington, D.C.: CDC, 2013), www.cdc.gov/oralhealth/.

7700 East First Place l Denver, CO 80230 l (303) 364-7700 l www.ncsl.org
This brief was written by Megan Comlossy.
The National Conference of State Legislatures thanks Dianne Mondry, Renee Joskow, Hyewon Lee and Julie Sadovich from the Health Re-sources and Services Administration (HRSA) for their time and com-mitment to make this publication as thorough as possible.
The author also thanks the following NCSL staff who reviewed the primer and made recommendations: Laura Tobler, Martha King, Hollie Hendrikson and Jennifer Saunders. In addition, thanks go to Leann Stelzer for editing.
This publication was made possible by grant number UD3OA22893 from the HRSA. Its contents are solely the responsibility of the author and do not necessarily represent the official views of the HRSA.
© 2013 by the National Conference of State Legislatures. All rights reserved.
ISBN 978-1-58024-700-9