organisational development plan - hmr · organisational development (od) plan has been developed to...
TRANSCRIPT

1
Organisational Development Plan
2012-2015
Version 3.0 (January 2013)

2
Contents
1.0 Foreword ........................................................................................................................ 3
2.0 Executive summary ........................................................................................................ 4
3.0 Introduction .................................................................................................................. 10
4.0 A brief history of our development ................................................................................ 11
5.0 Strategy ........................................................................................................................ 12
6.0 Structure ....................................................................................................................... 16
7.0 Systems ....................................................................................................................... 24
8.0 Style ............................................................................................................................. 27
9.0 Staff .............................................................................................................................. 30
10.0 Skills ............................................................................................................................. 32
11.0 Shared Values .............................................................................................................. 35
Appendix 1 .............................................................................................................................. 37
Appendix 1 .............................................................................................................................. 37
Appendix 2 .............................................................................................................................. 38
Appendix 3 .............................................................................................................................. 41
Appendix 4 .............................................................................................................................. 42
Appendix 5 .............................................................................................................................. 43
Appendix 6 .............................................................................................................................. 44

3
1.0 Foreword
1.1 Heywood Middleton and Rochdale Clinical Commissioning Group‟s (HMRCCG) Organisational Development (OD) Plan has been developed to support the emergent CCG on its journey to become a fully constituted, well governed, authorised and successful Clinical Commissioning Group.
1.2 Recent changes to the NHS offers us a unique opportunity to lead and shape safe, effective, clinically led services for the people of the borough of Rochdale and secure better quality of life and health for our population who experience some of the poorest health outcomes in the country.
1.3 HMR CCG wants the people of Rochdale borough to enjoy longer, healthier lives. We want those who need healthcare to receive it at the right time and at the highest quality. This can only come about by inclusive patient, public and stakeholder engagement in the work of our CCG, built on a foundation of transparency, openness and trust.
1.4 Working together with local providers, patient groups and our Local Authority, we aim to build on the positive legacy left to us by our Primary Care Trust (PCT), and to continue to bring health benefits to the whole population.
1.5 As always in times of great change, ever increasing demand, and the need to make the best of all of the funding we receive, we face a challenging and exciting future. Working with our partners we need to shape people‟s expectations of healthcare and enable them to make the best lifestyle choices they can to manage their own health and health care. This may mean making some tough but fair decisions, which are based on sound evidence and agreed through meaningful consultation.
1.6 Vital to our success will be a talented, committed and highly competent workforce. We will, therefore, progress and implement a programme of ongoing development to enable our staff and our member practices to be the best they can be and to reach their potential. As a local employer, we are sure that staff working for and within HMRCCG will join us and be proud to serve the local population.
Dr Chris Duffy
Clinical Chair
Lesley Mort
Chief Officer

4
2.0 Executive summary
2.1 The transition towards the implementation of the Clinical Commissioning Group (CCG) for Heywood, Middleton and Rochdale (HMR) presents both challenges and opportunities in ensuring that our population‟s health needs continue to be met and improved upon.
2.2 HMR‟s Organisational Development (OD) plan for 2012 to 2015 has been produced to support HMRCCG in becoming fully authorised and therefore deliver on our mission, values, aims, objectives and strategic priorities, whilst meeting the requirements of the NHS Outcomes Framework and Operating Framework.
2.3 This document is intended to be organic and it is recognised that it will need to be reviewed and updated regularly in order to keep pace with the changes and actions that are currently being completed. To this end a further review will take place to ensure that it reflects the CCGs requirements up to transition and beyond.
2.4 Our Mission, Aims, Objectives and Values
Our mission, aim, objectives and values have been developed through engagement with the CCG Governing Body, including LiNKs and Rochdale Metropolitan Borough Council (RMBC), and GP member practices.
2.5 Our Mission
‘Healthier People, Better Lives’
2.5.1 The mission of NHS Heywood, Middleton and Rochdale Clinical Commissioning Group is „To ensure the people living in Rochdale Borough are healthier and have a better future”. We want the people of Rochdale Borough to enjoy longer, healthier lives. We want those who need healthcare to receive it at the right time and at the highest quality.
2.5.2 Good corporate governance arrangements are critical to achieving the group‟s
objectives. The group will promote good governance and proper stewardship of public resources in pursuance of its goals and in meeting its statutory duties.
2.6 Our Aims
2.6.1 The group‟s aims are to:
a) Work closely with our local authority to influence policy
b) Build a great relationship with local people
c) Engage and secure good partnerships with a range of statutory and voluntary organisations
d) Live by example, creating a healthy workforce and workplace
e) Give clear direction, commissioning services that ensure integration

5
f) Improve the health and wellbeing of our local people
g) Work closely with our providers and other partners to deliver joined up services
h) Use finances wisely investing in those things that will make a difference to the health and wellbeing of our population
2.7 Our Strategic Themes
2.7.1 The delivery of our mission is underpinned by four strategic themes, each supported by a number of objectives which have been defined in the Plan on a Page, given in Appendix 1. A series of measurable outcomes have been agreed at objective level to support our understanding of delivery against the strategic themes.
a) To improve the population‟s health and well-being and to improve the health of the poorest fastest
b) Commission a transformed health system with a focus on prevention and restorative health that responds to the changing demographics of the Borough and is safe and high quality
c) Improve quality and access in primary care services for all sections of the community
d) Be a high performing CCG and deliver the best outcomes against return on investment with decreasing levels of funding
2.8 Our Values
2.8.1 The values that lie at the heart of the group‟s work are:
a) No decision about me, without me, applicable to all stakeholders
b) Care and compassion in everything we do
c) Being honest, open and visible
d) Providing constructive challenge and being open to challenge
e) Being bold, radical, innovative and aspirational

6
Figure 1: HMR CCG Values
2.9 Our Clinical Commissioning Priorities
2.9.1 Our clinical commissioning priorities have been identified through the development of our commissioning plan. Each of these reflects a key clinical commissioning programme within HMR CCG.
a) Respiratory disease, diabetes and vascular
b) Cancer
c) Mental Health, including Dementia
d) End of Life Care
e) Alcohol
2.9.2 Each programme will produce a programme plan and will be led by a defined Clinical Lead.
2.9.3 In addition, there are several cross cutting themes that remain the focus of clinical commissioning within HMRCCG and that are integral to the achievement of our mission, aims and objectives as follows:
No decision about me
without me applicable to all
stakeholders
Care and compassion in everything we
do
Being honest, open, visible and having
integrity
Being radical, innovative and
aspirational
Providing constructive
challenge and being open to
challenge

7
a) Children and Young People
b) Long Term Conditions
c) Elective Care
d) Non Elective/Urgent Care
e) Prescribing
2.9.4 The latter areas will also be managed as clinical programmes and be led by a Clinical Lead. Long Term Conditions and Children‟s and Young People will be key themes within each programme area and will be the focus of our developing integrated commissioning strategy. They will also be CCG Governing Body level accountabilities.
2.9.5 The urgent care and prescribing workstreams are also pivotal to delivering planned financial efficiencies to enable further investment in our clinical commissioning priority areas.
2.10 Organisational Development Priorities
2.10.1 The following steps have been undertaken to identify key areas for development to ensure the delivery of HMRCCG‟s mission and strategic themes:
a) Analysis of the results of the „CCG Diagnostic Tool‟ which is based upon the 6 CCG authorisation domains:
i. A strong clinical and professional focus which brings real added value
ii. Meaningful engagement with patients, carers and their communities;
iii. Clear and credible plans which continue to deliver the QIPP (quality, innovation, productivity and prevention) challenge within financial resources, in line with national outcome standards and local joint health and wellbeing strategies
iv. Proper constitutional and governance arrangements, with the capacity and capability to deliver all their duties and responsibilities, including financial control, as well as effectively commission all the services for which they are responsible
v. Collaborative arrangements for commissioning with other CCGs, local authorities and the NHS Commissioning Board as well as the appropriate external commissioning support
vi. Great leaders who individually and collectively can make a real difference
b) Discussions with individual members of the governing body regarding individual, team and organisational development needs.
c) Meetings and development sessions with HMRCCG‟s 3 localities led by HMRCCG‟s Governing Body members.
d) Meetings with key members of the Health and Well Being Board.

8
e) Review of HMR PCT‟s current strategic plan.
f) Review of the feedback from the bi-lateral Board meetings with NHS Greater Manchester held in January and August.
2.10.2 All of the above resulted in the organisational development priorities being defined under four broad areas:
a) Communication, collaboration and engagement
b) Developing robust systems and governance arrangements
c) Clear and credible plans in place that support delivery of the CCG mission and strategic themes
d) Clinical leadership and Governing Body development
2.10.3 Since December 2011, when the diagnostic tool was initially completed, considerable work has been done to progress these priorities. The diagnostic tool was completed again in August 2012 to assess this progress and to identify any areas requiring additional focus.
2.10.4 Specifically, the August 2012 diagnostic results indicated four areas assessed as “in development” which require focus:
a) Values and behaviours
b) Continuous improvement
c) Administrative functions
d) Emerging CCG structure and capability: Learning and development
2.10.5 Specific actions have been developed to address these areas which these are detailed in the “what needs to be done” sections of this OD Plan. In addition they are presented in and action plan in Appendix 6.
2.11 Organisational Development Framework
2.11.1 NHSHMR have utilised McKinsey‟s 7S (shown in Figure 2) as its organisational development framework. This framework consists of seven elements which all have interdependencies with each other.

9
Figure 2: McKinsey 7S Model
2.11.2 Figure 3 describes each of the elements set within the context of HMRCCG OD plan.
Figure 3: OD Context for 7S Model
Element Meaning
Strategy The strategic direction we intend to take to be effective clinical commissioners
Structure The shape, infrastructure and governance of the CCG Systems The processes we have developed to enable us to meet
our strategy Shared Values The core values of the CCG that shape how we work and
underpin everything that we do Style How we present and engage with others and manage key
relationships Staff How we lead, support and develop staff from both the
CCG and wider health economy Skills The capabilities that we need to continually develop
2.11.3 Part of the authorisation process required the CCG to undertake an initial diagnostic using a validated toolkit. HMRCCG undertook this exercise in December 2011 and has now repeated this diagnostic in August 2012 to assess progress. Significant improvement has been demonstrated and a comparison of both of these assessments is given in Appendix 2.

10
3.0 Introduction
3.1 The health challenges in the Rochdale borough are significant. The level of health inequality is high and life expectancy in certain parts of the borough, whilst improving, is still amongst the poorest in the North West. HMR has been ranked as the 25th most deprived borough in England with 1 in 2 children in some of its wards living in poverty.
3.2 The registered population of the borough is circa 240,000; encompassing a wide range of diverse communities and facing particular health challenges in relation to:
a) Cardiovascular Disease (CVD) and Chronic Obstructive Pulmonary Disease (COPD) linked to smoking prevalence
b) Alcohol abuse and a growing number of related hospital admissions
c) Mortality rates
d) Increasing childhood obesity
3.3 These health challenges have focussed the CCG in the development of their commissioning intentions. These intentions will drive our OD plan towards being a fully authorised CCG.
3.4 The OD plan will therefore ensure that we acquire and develop the skills, capacity and capability to enable full authorisation and achieve excellence in clinical commissioning. The OD plan is a living document that we will refresh quarterly and at key strategic points in order to reflect our evolving development needs, to fully consider improvement and innovation within our commissioning practice and to reflect the changing health care landscape.
3.5 We plan to build upon the strong commissioning and financial legacy that we have inherited from NHS PCT and its strategic partnership working with the Local Authority, across the North East Sector of Greater Manchester and within the NHS Greater Manchester cluster.
3.6 Our organisational development plan facilitates HMRCCG‟s realisation of its mission, aims and outcomes, articulation of its values and the achievement of key outcomes for the people of Rochdale borough.

11
4.0 A brief history of our development
4.1 NHS HMR operated with three Practice Based Commissioning (PBC) Clusters, one in each locality, namely Heywood and Middleton, GP Care (Rochdale East) and Rochdale West and consisted of 39 GP Practices.
4.2 The development of HMRCCG saw the joining of these PBC clusters to form a single, shadow CCG. This was supported in late 2011 by a 92% majority vote from the 39 local practices that recognised the need to achieve critical mass and to work together on an increasing number of common issues of each of the three locality populations. In supporting this, each locality cluster was clear on its desire to retain a strong locality focus and identity and, at the request of the member practices, this is reflected in the structure of the CCG Governing Body where each locality is clearly resourced and represented.
4.3 The transition from three clusters to one CCG presents some cultural challenges. The CCG will need to shift hearts and minds into the new ways of working whilst ensuring that the best practice from the old system is carried forward for the benefit of the new.
4.4 In becoming one CCG, HMR has also ensured co-terminosity with its Local Authority. In turn, this has and will continue to enable HMRCCG to jointly develop greater integration of care pathways and commissioning arrangements for vulnerable adults and children. In addition, co-terminosity has allowed HMRCCG to continue to develop its already strong relationships with the developing Health and Well Being Board, where GPs have been involved since its inception.

12
5.0 Strategy
5.1 The strategic direction we intend to take to enable us to achieve our mission, aim, objectives and to live by our values.
5.2 Strategy – Our Legacy
5.2.1 NHS HMR has a track record in working closely with partners and it is expected that this will be further enhanced by the clinical leadership in place within the CCG. NHS HMR engaged with the three Practice Based Commissioning clusters and intends building on the knowledge gained during this time to support engagement with the three localities within the CCG and with the member practices.
5.2.2 HMRCCG has inherited a strong strategic legacy from NHS HMR on the importance of partnership working and developing a joined up approach to improve health and wellbeing outcomes in the borough. A Health and Wellbeing Partnership was established for the borough, bringing together a range of key partners, to lead on the delivery of the Health and Wellbeing Strategy and drive forward joint action to tackle health inequalities.
5.2.3 Joint working has been at the heart of our Joint Strategic Needs Assessment (JSNA) process since 2008 when RMBC and the PCT NHS HMR jointly produced the first JSNA for Life Expectancy. The priorities from the JSNA were adopted by Rochdale‟s Health and Wellbeing Partnership and have since been integrated into the strategic plans of both the Council and the NHS.
5.2.4 Since then, further JSNAs have been produced on:
a) The Health and Wellbeing of the 3% most deprived Lower Super Output Areas in Rochdale Borough
b) The Health and Wellbeing of Older People
c) Stroke in Rochdale Borough
d) Children and Young People
5.2.5 NHS HMR had a strong business planning legacy which built on JSNA‟s and patient and public consultations to describe key strategic themes and objectives which formed the basis of the Strategic Commissioning Plan. This business planning process has been taken forward in the development of the Plan on a Page shown in Appendix 1.
5.3 Strategy – Where we were
5.3.1 In December 2011 NHS HMR completed a diagnostic tool which supported the identification of priority areas for development in the journey to becoming a fully authorised CCG.
5.3.2 Scores in Table 1 are given out of 5 with 0 being the minimum score and 5 being the maximum.

13
Table 1: Strategy Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Clinical Focus and Added Value:
Clinical Leadership that Brings About Change
Starting with Population Health/Clinical Needs
Values and Behaviours
Continuous Improvement
3
4
1
2
4
4
3
3
Clear and Credible Plan:
Strategy Development and Implementation
Mission
Case for Change
3
2
2
5
4
5
Collaborative Arrangements:
Engagement with Other Commissioners
Engagement with Local Authority and Others
Existing Relationships and Processes
2
2
2
4
4
4
5.3.3 In December 2011 the key development areas were clearly around values and
behaviours and improving engagement and relationships. Significant progress has
now been made in particular in the engagement and relationships area.
5.3.4 Whilst measureable progress has been achieved it is recognised that further
improvements can be made in the areas of values and behaviours and continuous
improvement.
5.4 Strategy – What has been done
5.4.1 A significant amount of work has already been completed to support the CCG strategy going forward including:
a) Clinical engagement has been supported by the agreement of Clinical Leads, Clinical Leads Supporting roles and three Locality Clinical Chair roles. As a result clinicians have been involved in all aspects of strategy development and implementation.
b) Several Commissioning Plan development sessions were held with clinicians, ensuring that the plan focussed on the key clinical areas. This has led to a plan that is robust, clinically led and ratified.
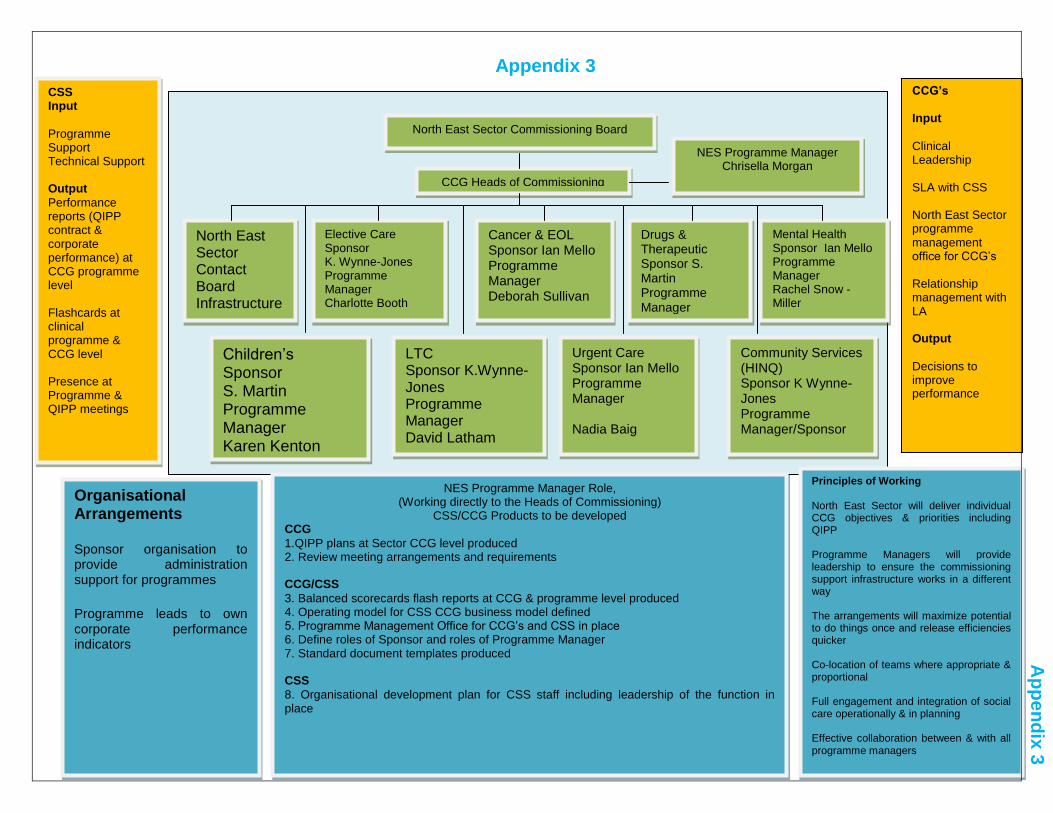
c) HMRCCG have jointly implemented a commissioning infrastructure across the North East Sector (NES) to support capacity and capability development. The governance arrangements for this structure are shown in Appendix 3.
d) HMRCCG collaborative working arrangements with NHS Greater Manchester and NES have supported increased engagement with our providers and significant improvements have been demonstrated in performance against

14
Operating Framework Measures in the last six months. This provides an excellent foundation for the CCG.
e) HMRCCG constitution has been developed which sets out the arrangements for the CCG to meet its responsibilities for commission care for people in the borough. It describes the governing principles, rules and procedures that will be established to ensure probity and accountability in the day to day running of the CCG, ensuring that decisions are taken in an open and transparent way and that the interests of patients and the public remain central to everything that the CCG does.
f) A Variation Group has been established which supports the continuous improvement of Primary Care.
g) The CCG mission, aims and values have been defined as detailed in the Executive Summary of this document.
h) A CCG newsletter has been developed which is circulated to all GPs, Practice Staff and all other stakeholders. This clearly outlines the direction of travel of the CCG. This together with Locality Meetings, website communication and staff briefings provide up to date information and ensure that the key messages around change are communicated. Engagement began with a launch event in September 2012, followed by a local media page explaining the CCG.
i) A culture of honesty, openness and trust is prevalent which will facilitate a robust handover from PCT to CCG.
5.4.2 Following the NHS reforms and building on previous processes, we have developed a new JSNA for 2012 based on a high level, overarching approach and led by the Borough‟s Health and Wellbeing Board. This new approach is an on-going process of developing a shared understanding and mission for health and social care in the Rochdale borough and how we can best improve health and wellbeing across the borough, and is built on three different strands of intelligence:
a) Quantitative service and outcome data, segmented into five socio-economic categories using MOSAIC geographic population data.
b) Knowledge of existing research and intelligence
c) Qualitative information and feedback from key stakeholders
5.4.3 As part of the JSNA process in 2012, the Rochdale Borough Health and Wellbeing Board, in consultation with a wide range of stakeholders, identified a long list of priorities for action. Using a priority setting framework and following further consultation and sign off by the Health and Wellbeing Board, the following Top 5 Priorities for 2012 were identified:
a) Children & Young People – Giving Every Child the Best Start in Life
b) Early Prevention/Preventative Services
c) Tackling Inequalities
d) Wellbeing

15
e) Lifestyles
5.4.4 These strategic priorities have informed the development of a Draft Joint Health and Wellbeing Strategy (JHWS) for the borough. The Health and Wellbeing Board is currently identifying a number of strategic objectives to support the delivery of these strategic priorities. Together with the Joint Strategic Needs Analysis and the Joint Health and Wellbeing Strategy these provide a tool for joint, evidence-based commissioning.
5.5 Strategy- What needs to be done
5.5.1 There is still work to be done in this area, a high level summary of which is included below:
a) To communicate the developed “Organisation on a Page” to all stakeholders, including internally, the public and all partner and provider organisations. The Organisation on a Page is shown in Appendix 4 and details the vision, values and goals of the CCG.
b) Continue to build relationships with providers to ensure delivery of performance targets, increase productivity and subsequently improve outcomes for the local population in support of the QIPP agenda.
c) Continue to develop our communication and engagement strategy with clear focus on relationships with providers and neighbouring CCGs.
d) Continue to develop the NES commissioning infrastructure arrangements to ensure that sufficient capacity and capability is directed at our key priority areas.
e) Ensure that all CCG member practices sign up to the constitution and therefore agree to adhere to the rules and regulations and values and behaviours of the CCG.
f) Progress the Variation Group by using the new Locality Engagement Officer posts and Data Analyst posts to be the conduit by which information is devolved to locality and practice level in an appropriate way so as to facilitate continuous improvement.
g) Improve links with the Third Sector at locality level.

16
6.0 Structure
6.1 The shape and form of HMRCCG and the governance and infrastructure we use to assure, organise and co-ordinate our activities.
6.2 Structure – Our Legacy
6.2.1 The structure inherited from NHS HMR has enabled some organisational evolution to take place and resilience to be maintained during the transition. This is principally because many of the senior roles had diverse portfolios of responsibility that enabled flexibility and evolution in order to meet objectives and emerging challenges.
6.2.2 HMRCCG has also inherited a robust governance structure with designated roles and committee structures that enable quality assurance of the commissioning process. These are being reviewed and adapted for use within the CCG in the context of the CCG as a membership oprganisation .
6.2.3 NHSHMR has provided a sound financial platform on which HMRCCG can build. In 2011/12 NHSHMR delivered:
a) A control total of a £2m surplus against which we out turned £2,155K
b) A cash releasing efficiency programme of c. £11K and demand management
and provider efficiencies of c. £14.5K
c) A strong recurring position c. £14K
6.3 Structure – Where we are now
6.3.1 Scores in Table 2 are given out of 5 with 0 being the minimum score and 5 being the maximum.

17
Table 2: Structure Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Capacity and Capability:
Structure and culture of change
Clinical elements of governance
Emerging CCG structure and capability: Learning and Development Integration of Governance
Financial management capacity and capability
Financial planning controls
External financial control requirements
2
3
1
2
3
2
4
4
5
3
4
4
4
5
6.4 Structure – What has been done
6.4.1 The in - house structure covers the following core functions of the CCG:
Accountable Officer (AO)
Finance
Commissioning and Provider Management
Quality and Safety
Operations and performance
Communications and Engagement with constituent members and other partners
6.4.2 This has been designed to align and embed clinical and managerial leadership in all aspects of CCG business delivery. This will ensure due process is maintained for governance, decision making and planning, and that the CCG maintains its resolute intention to be a clinically-led and managerially- enabled organisation.
6.4.3 The structures for the CCG have been designed to deliver both its core in-house commissioning and other corporate functions and those which will be bought from the GM Commissioning Support Unit. The finalisation of the internal structure has provided a robust basis upon which the conclusion of the negotiations with the GM CSU is being achieved.
6.4.4 Table 4, page 21 indicates that relationship management roles will be held by the executive leadership of the CCG with the CSU, to ensure that CSU-provided services operate to optimum performance and deliver the needs of the CCG in the agreed areas of CSU product delivery, and to maintain strategic oversight and management of commissioning support arrangements. More detailed structure charts are available in the evidence file submitted to support the authorisation threshold 4.3.1C.
6.4.5 The internal structure is now complete, and a high level overview is provided in Figure 4, page 20, and detailed information is provided in the detailed structure charts as signposted above. The majority of posts have been appointed to since the site visit in

18
November 2013. Whilst we are confident that we have a robust structure, it will be operationally tested on an ongoing basis to:
ensure sufficient capacity and capability to deliver the CCG‟s work programme and objectives.
ensure ongoing affordability within running costs
ensure compliance with any further guidance on additional CCG responsibilities that may emerge
ensure a robust capacity cross check with CSU products delivery, during product testing phase and on an ongoing basis following full product launch
6.4.6 The CCG has been committed to appointing to all structures through robust, transparent and contested recruitment processes and the following work has been completed in accordance with this principle.
a) Appointed to Chief Officer Designate and Clinical Chair Designate, via the national processes.
b) Appointed to clinical Governing Body posts (through formal recruitment processes, including assessment of leadership competencies) including Vice Chair and 3 locality GP Governing Body members, one each for Heywood and Middleton, Rochdale East and Rochdale West localities. The appointment of clinical posts followed a robust competency based process which assessed candidates against the following competencies:
i. Communication skills
ii. Leadership
iii. Patient and Public Focus
iv. Stakeholder Engagement and Collaboration
v. Financial Awareness
vi. Corporate Accountability
c) Appointed to Governing Body level posts (again through formal recruitment processes), including Director of Finance (shared post across North East Sector), Locality Director of Finance, Head of Operations and Engagement, Head of Commissioning and Provider Management and Head of Quality and Safety/Executive Nurse.
d) Appointed 3 Lay Governing Body Members with specific areas of expertise in commissioning, audit and governance and patient and public engagement, as set out in the CCG constitution.
e) HMR CCG has continued to work closely with North East Sector CCG‟s and the GM CSU to determine how the CCG business will be resourced and appropriate capacity and capability secured. This work has allowed the CCG to determine

19
its make/share/buy decisions both locally and at a sector level, and to ensure that these are deliverable within the available running cost envelope. The CSU product offers and associated costs have now reached an advanced stage of development which has allowed the CCG to establish the financial viability of the proposed HMR internal structure (make – see Figure 4) and its support services relations with the CSU (buy – see Figure 5) which is described in an SLA with the CSU
f) The final version of the SLA and the Heads of Terms has been signed, with an
agreed commitment to continue to continue to work with the CSU to address any
outstanding issues. The North East Sector CCGs will continue to explore how their
collaborative working practices can help to reduce the cost drivers for the CSU.
This work will continue during the first quarter of 2013/14 to ensure products
deliver to the expected quality and cost. The CCG recognises that the signed SLA
with the CSU covers up to the end March 2014.The CCG will continue to closely
monitor CSU service delivery to support its ongoing strategy with regard to
commissioning support provision, which will inform the design of the procurement
process to secure such services beyond this date.
g) The CCG is currently working with Greater Manchester CCGs and the CSU to
“road test” CSU product delivery, with each CCG taking a lead role on a specific
product. This will highlight any issues or gaps in capacity and capability which can
be addressed before the go live date of 1 April 2013.
h) Following go live, robust monitoring of CSU product delivery will be carried out by
the Executive and Senior management teams. Feedback and escalation
mechanisms are in place in order to address any issues as they arise. Each
product has been assigned to an Executive Management Team member‟s
portfolio. This arrangement is shown in Table 4. The Executive lead has other
capacity within their internal teams who will operationally support this monitoring
process. A collective review of performance against the SLA/contract will be taken
by the Executive Management Team and Governing Body.
i) The CCG has assessed its communication and engagement capacity and capability requirements. In order to ensure the delivery of the Communication and Engagement Strategy, the Communications product will be bought from the CSU. This product includes design printing and copywriting, digital marketing, internal communications, media relations, social marketing campaigns and strategic communications and engagement. In addition to this a communications and engagement post has been included in the CCG structure to support operational communications and engagement. The three Locality Engagement Officer posts will support engagement.
j) Governance structures have been defined to ensure that the CCG Governing Body can effectively and efficiently discharge their clinical and corporate responsibilities and are shown in Figure 6.

20
Figure 4: CCG Structure
Table 3: CSU Buy Decisions Buy from CSU Comments
Medicines Management (strategic product only)
Threshold and policy setting and strategic advice
HR ( People services) Already a shared GM service
Communications and Engagement
Some internal operational communications will be done by CCG communications and engagement post holder post.
Governance and Risk Management support
Patient services Includes PALS, Complaints, FOI and Claims
Financial planning and management
IMT all elements Includes Information Governance and Business Intelligence ( BI is nationally mandated as a buy)
Resilience Emergency preparedness training and gold control - although we will have a coordinating role to play locally
Market management Nationally mandated buy
Total Provider Management
Transactional aspects of contracting from the point where CCG issues its commissioning intentions, CQUINS and KPIs. CCG clinicians lead negotiations and reviews with management support. CSU supports and enables the translation of intention to contract by a provider footprint-based contract team working on all aspects of contract negotiation, compliance and remedial action. This would also align with EUR product in terms of transactional management
EUR threshold and policy setting
Includes day to day approvals handling (although the CCG would still need to lead panels and be responsible ultimately for the decisions it takes.
Equality and Diversity NE sector shared buy
Service Redesign
SIRO – Chief Finance Officer

21
Table 4: Executive Management Responsibilities
Responsible Role Portfolio Linked CSU Products
Director of Commissioning and Provider Management
Commissioning
Medicines management
Continuing Health Care/Complex Care
GM Healthier Together and other collaborative commissioning programmes
RMBC Joint Commissioning
Referral and Booking Management service (shared with Bury CCG)
Primary Care improvement
Medicines Management strategy
Total Provider Management
Service re-design
EUR
CFO Finance (all elements)
Contracting
IM&T
Market Management (including procurement)
Internal Audit (subcontracting arrangement)
Estates, Health, Safety and Security (via PropCo)
IM&T
Total Provider Management (Finance element)
Market Management including procurement
Information Governance (specifically SIRO)
Director of Operations and Engagement
Corporate Governance and Administration
Information Governance
Engagement
Communication
Patient Services
Governance and Risk
Equality and Diversity
Information Governance
Communications
Patient services (PALS, Complaints, FOI and Claims)
HR and OD
Governance and Risk
Equality and Diversity
Director of Quality and Safety and Executive Nurse
Safeguarding
Quality and safety
Research Governance
Total Provider Management (CQUIN)
Figure 6: CCG Governance Infrastructure
Sub committees
HMR CCG Governing
BodyLocal Public Sector BoardHealth & Well Being
Board
Clinical
Commissioning Committee
Quality & Safety
Committee
Audit Committee Remuneration
Committee (ad hoc post
authorisation)
Locality
Engagement Groups
Heywood &
Middleton
Rochdale East
Rochdale West
NHS GM Board
Operational
Business and Clinical Meetings
22
h) Identified and allocated key responsibilities to all Governing Body roles, including lay members.
i) Extended and developed NHSHMRs clinical leadership responsibilities to include its local clinical population and the following operational clinical leadership roles have been identified as being crucial to success:
i. Clinical Chair and Lead for Long Term Conditions
ii. Clinical Vice Chair and Lead for Community Services, Adult Safeguarding, Children and Maternity
iii. Rochdale East CCG Locality Lead and Lead for Hospital Care, Heart and Lung Care, Cancer, Palliative and End of Life Care
iv. Rochdale West CCG Locality Lead and Lead for Prescribing
v. Heywood and Middleton CCG Locality Lead and Lead for IM&T and Mental Health and Caldicott Guardian
vi. Clinical Leads Supporting Roles have been agreed for End of Life Care, Children‟s Diabetes and Renal, IM&T, Maternity, Mental Health, Unscheduled Care, TAG, Veterans Health, Health and Wellbeing, Variation Group, Vascular, COPD and Long Term Conditions.
vii. Each locality has appointed a clinical chair for their Locality Meetings with direct links to the Governing Body Locality Leads.
6.5 Structure - What needs to be done
6.5.1 Further to the recruitment into the CCG Structure that has been ongoing since the last iteration of this Organisational Development Plan, the majority of posts have now been appointed to. A development plan for all CCG staff is currently being produced. This will initially focus on an induction programme into the new organisation to include mandatory training requirements, values and behaviours, corporate expectations and culture, what it means to work in a membership organisation that operates within a system of distributed leadership, and news ways of working.
6.5.2 The following details the posts that are still to be appointed and the expected timescales:
a) Hospital Doctor Governing Body Post – Interviews scheduled for 30 January 2013.
b) Senior Commissioning Manager – Out to open advert; interviews scheduled for 8
February 2013
c) Investment Programme and QIPP finance officer – Out to open advert, interviews
mid February 2013
d) Quality and Safety lead – Interviews scheduled for 28 January 2013
e) Performance and Quality Manager – Out to open advert, interviews mid February
2013

23
f) Locality Engagement Officers (2 posts) – Interviews scheduled for 1 February
2013
6.5.3 Develop succession plans for Governing Body members and clinical leads by developing
the wider pool of clinicians in supporting roles. Clinical Support roles were appointed
through an interview process.
6.5.4 All post holders will participate in Personal Development Review processes during
January and February 2013, and the outcomes of this will be used to support the design
of individual and team development programmes. In addition the Clinical Support role
holders are Clinical Commissioning Committee members which will support their
corporate development.
6.5.5 Work continues in the CCG to ensure that ways of working and relationships are built to
facilitate matrix working and optimum flexibility across the structure. This will be essential
in order to ensure that our available resource is used to maximum effectiveness and
efficiency, as the work of the CCG required a clear recognition of the interdependencies
that exist, particularly between Commissioning, Quality and safety and Operations and
Engagement. Resource levels will be monitored closely to ensure any gaps in capacity
and capability can be addressed, for example the CCG is considering whether it has a
requirement for a Primary Care commissioning/ Improvement post to support the Primary
Care Improvement Plan and future primary care commissioning strategy. Discussion are
being progressed re this particular issue with the GM NCB Area team Director of
Commissioning and his team to inform the design and role content of this post

24
7.0 Systems
7.1 The processes we have developed to allow us to deliver on our strategies.
7.2 Systems – Our Legacy
7.2.1 NHSHMR had many well designed and cohesive commissioning systems and processes in place that the CCG have been able to effectively adapt and develop. NHSHMR has previously utilised an approach to commissioning that considers the commissioning cycle as a whole and the provision of cross directorate teams to provide support through each stage. The previous level of clinical engagement within the commissioning process through the involvement of the three PBC Clusters again means that there has been a good platform to enable CCG to move forwards.
7.2.2 HMRCCG also inherits a robust system of programme and project management where there is strategic alignment of all commissioning programmes and associated projects with organisational objectives and with sound financial oversight.
7.2.3 A robust performance and business intelligence regime is also inherent which, along with contract management and quality monitoring ensures that our commissioned services are fit for purpose and deliver in line with contract terms and to meet national requirements.
7.2.4 There is a strong legacy of achieving value for money which was monitored through the Service /Investment Review Panel. Services were assessed through this panel using standardised criteria to support open and transparent decision making.
7.3 Systems – Where we are now
7.3.1 Scores in Table 4 are given out of 5 with 0 being the minimum score and 5 being the maximum.
Table 4: Systems Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Clear and Credible Plan:
Getting the best out of the system
Contracting and Procurement
Administrative functions
2
2
2
4
4
3
Leadership Capacity and Capability:
Business Intelligence
2
4
7.3.2 This represents significant improvements since December 2011. Structures have now been populated and an operating model agreed for administrative functions which is currently being put in place.

25
7.4 Systems – What has been done
7.4.1 We have continued to build on the robust systems already in place by:
a) Established a Programme Management Office (PMO) which maintains an overview of HMRCCGs programme of investment for 2012/13 and beyond. This links quality, finance and delivery of a series of investments to ensure that money is spent appropriately, in the right areas, ensuring appropriate improvements in performance and outcomes.
b) The Service Review Panel has developed into the Service Review and Investment Panel to reflect the CCG financial landscape. This panel has representation from Finance, Governing Body Lay members, clinicians, commissioning, Public Health and Patient and Public Engagement. It is responsible for reviewing existing services against set criteria to support commissioning decisions. In addition it is the investment review body which reviews business cases and supports the decision making process around investments, which follows a clearly set out governance route depending on business case value. This process ensures that CCG resources are invested wisely ensuring it gets the most out of the system.
c) Identified our priorities and established the clinical leadership and support arrangements
d) Devised a performance management dashboard for reporting provider performance within our governance structure to support the identification of key quality improvements.
e) Established and implemented referral gateway to support the continual quality improvement of primary care services.
f) The CCG has established and delivered robust procurement processes, with positive outcomes, and is therefore able to demonstrate the skills and capacity around procurement, including a collaborative approach with Greater Manchester and CSU.
g) The CCG has developed internal structures and identified those which it will buy from the GM CSU which will support organisational administration to ensure the smooth running of the CCG. It is recognised that whilst this structure has been identified, work is still ongoing to recruit to and embed this way of working.
7.5 Systems - What needs to be done
7.5.1 HMRCCG has made significant progress since the site visit and is ensuring that we have the systems in place to support the delivery of the mission and aim of the organisation. Going forward we will:
a) Continue to work closely with the CSU to ensure that optimum service delivery and best value is delivered to the CCG by the CSU.
26
b) Establish processes and systems to ensure appropriate monitoring of CSU product delivery, in line with the SLA
c) Continue to work closely with RMBC to establish and embed new working arrangements following the transition of Public Health and the development of joint commissioning arrangements.
d) To explore the potential engagement opportunities with individual service users, community services and voluntary organisations to support the delivery of “Healthier People, Better Future”. This work will look particularly at reinvigorating the Locality Patient and Public Engagement groups as discussed in section 8.4.1b.

27
8.0 Style
8.1 How we present and engage with others and manage key relationships.
8.2 Style – Our Legacy
8.2.1 NHSHMR has always recognised that organisational style influences how people behave and therefore how strategies are delivered. It has always strived to be an organisation that engages with providers and other partners and developed strong relationships with RMBC. It recognised that an individual‟s health and wellbeing is influenced by many factors that are outside of the remit of the NHS and therefore developed and maintained purposeful alliances with other agencies and with its local partners.
8.2.2 It has a strong track record in engaging with PBC clusters and had clinical leads linked closely with commissioning teams and the Clinical Commissioning Committee.
8.2.3 It is recognised that this is an excellent foundation on which to build the CCG.
8.3 Style – Where we are now
8.3.1 Scores in Table 5 are given out of 5 with 0 being the minimum score and 5 being the maximum.
Table 5: Style Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Clinical Focus and Added Value:
Clinical Leaderships that brings about Change
3
4
Leadership Capacity and Capability:
Leadership Roles
Internal Engagement
3
2
4
4
Collaborative Arrangements
Managing Relationships
Engaging with Providers
2
2
4
4
Engagement with Patients and Communities
Patients, Public and Populations
Communities
2
2
4
4
8.3.2 This demonstrates significant improvements in the area of communication and engagement which were identified as key priorities in the December 2011 assessment.
8.4 Style – What has been done
8.4.1 Significant work has already been done to define the style of the CCG going forward. This is detailed in our mission, aims and values in sections 2.5, 2.6 and 2.8. We have:

28
a) Held externally facilitated Governing Body development sessions to articulate the type of organisation that the CCG wants to be, developing its corporate identity, and defining the Organisation on a Page (Appendix 4)
b) Agreed the ethos of “No decision about me, without me, incorporating all stakeholders” describing the desire to be an engaging organisation. In order to support this ethos the three localities have Locality Meetings which are chaired by a GP and are attended by a GP representative and Practice Manager from each member practice. The three Locality Chairs then have mechanisms in place with their Locality Governing Body Clinical Lead to ensure two way feedback from the Governing Body to member practices and member practices to Governing Body. This facilitates real engagement with all member practices.
c) Defined what matters to us as an organisation and engaging with the public is the key to achieving this. The CCG wants people to aspire to be healthier than they are and to believe that they can be.
d) Defined a communication and engagement strategy which puts the public and clinicians at the heart of what we do.
e) Improved internal communication and engagement through regular staff briefings, both face to face and electronic.
f) Supported improvement of engagement with the public by launching a monthly page in the local media.
g) Launched a public CCG newsletter.
h) Developed a CCG website including involvement, consultation and feedback pages.
i) Launched an internal CCG newsletter in May 2012 which is circulated to all GPs, Practice staff, other staff and all other stakeholders. This clearly outlines the direction of travel of the CCG.
j) On 22 May 2012, health and council leaders from across the Rochdale borough gathered together at Rochdale Infirmary to sign a commitment to the future of the hospital and how to transform and enhance health and social care services. The joint statement of intent agreement was signed by Heywood, Middleton and Rochdale shadow Clinical Commissioning Group Chair and Interim Accountable Officer, The Pennine Acute Hospitals NHS Trust Chair and Chief Executive, Pennine Care NHS Foundation Trust Chief Executive and the Leader of Rochdale Council, Councillor Colin Lambert. The agreement acknowledges the important heritage of Rochdale Infirmary and some of the concerns that local people have about the services that have moved out of the hospital. Going forward, plans are focussed on the services that could be provided at the hospital and in the community and local people are being asked to get involved.
k) On 14 September 2012 the CCG held an interactive engagement event with patients, carers, the public and local stakeholders. The aim of the event was to begin a dialogue with local communities and interested parties on the work of the CCG and the future planning of health services for the borough. The day was attended by representatives from local community groups, charitable and voluntary organisations, officers of the local authority, local councillors, partner

29
health care provider organisations, patients and members of the public. The day event was very successful and enabled the CCG to inform attendees on their future role as lead commissioner for health services and gain an understanding of delegates views on recent changes to local NHS services, how they felt the CCG could improve on local services and the importance delegates placed on meaningful engagement/involvement of local communities and stakeholders in the future planning and design of services.
8.5 Style - What needs to be done
8.5.1 It is recognised that there is still work to do in continuing to define the organisation and to ensure clear and engaging communication around this. Work is therefore ongoing to:
a) Reinvigorate the Locality Patient Participation Groups. These groups involve a patient representative from each member practice in the Locality and are a discussion/improvement forum which feeds directly into the Locality Meetings. Thereby facilitating patient engagement and ensuring that patient feedback is at the heart of what the CCG does.
b) Establish robust links between the role of the Patient and Public Engagement Lay Governing Body member and its interaction with the Locality Engagement Officers and member practices to facilitate effective engagement.
c) Continue to improve the relationship with our providers, clinician to clinician, to support and influence patient experience and improved outcomes.
d) Ensure that recruitment process and working practices reflect the organisational style.
e) Explore accessible local health communities and engagement using digital formats including TV, via Digital First (Department of Health programme).

30
9.0 Staff
9.1 How we lead, support and develop staff from both the CCG and wider health economy
9.2 Staff – Our Legacy
9.2.1 NHSHMR had a workforce it was proud to employ, that was highly valued and made significant contributions to the design and development of health care in HMR. In moving forward to the establishment of HMRCCG their contribution is acknowledged and the CCG expects that those staff who have joined the CCG from the PCT will continue to bring their skills, knowledge and experience to work in health care commissioning.
9.3 Staff – Where we are now
9.3.1 The diagnostic tool does not relate to directly employment of staff.
9.4 Staff – What has been done
9.4.1 Recognising that employment is a key determinant of health, NHSHMR worked closely with staff to support them through the transition. A resilience programme, based on Appreciative Inquiry, was made available to all staff to provide guidance in recognising individual‟s key strengths and how to build on these to support their aspirations for the future.
9.4.2 HMRCCG aspire to be an „employer of choice‟ and as such, will work with dedicated HR and OD resource to implement a wide range of employee engagement methods that will ensure a healthy and motivated workforce. The HR and OD shared resource across Greater Manchester has developed a series of workshops and support mechanisms to help staff with CV writing and recruitment processes.
9.4.3 Work has already been completed in the following areas:
a) Recruited to Chief Officer Designate and Clinical Chair Designate posts via the national process and is continuing to follow national/GM guidance to recruit to the Chief Finance Officer post.
b) Recruited to clinical leadership roles
c) Recruited to all governing body posts and clearly assigned areas of responsibility
d) Identified CCG staffing capacity and capability (and whether this should be made or bought) and signed an SLA with the GM CSU to deliver what will be bought from outside of the CCG.
e) Recruited to interim shared NES commissioning roles to pilot shared delivery of core commissioning services.

31
9.5 Staff - What needs to be done
9.5.1 The following need to be completed:
a) Continue to evaluate the success and working practices of the shared NES commissioning roles and how this might develop.
b) Ensure that directly employed staff have access to appraisal and performance
review that enables implementation and evaluation new ways of working.
c) Ensure that all workforce requirements are effectively managed and monitored
to ensure full compliance with our equality duty objectives.
d) Ensure that all staff employed by the CCG have completed mandatory training
in line with statutory requirements and seek assurance that all CSU staff have
also completed mandatory training.

32
10.0 Skills
10.1 The capabilities that we need to continually develop.
10.2 Skills – Our Legacy
10.2.1 A strong appraisal and performance management system was developed and implemented by NHSHMR. All individual objectives are directly linked to the Strategic Objectives of the organisation, supporting staff to clearly recognise the contribution that they make. Appraisal was also the key to linking development of commissioning skills with staff learning needs and the appropriate access to personal and professional development.
10.2.2 NHSHMR had a robust learning and development infrastructure and resource that was used to manage skills development and access to learning. Much of this resource migrated to provider organisations under the Transforming Community Services initiative. The remaining resource has been managed through the NHS Greater Manchester Shared HR/OD Service. This still provides access to all of the above opportunities but across the NHS Greater Manchester conurbation.
10.2.3 PCT Board development was viewed as an integral part of the organisation‟s continued development and NHSHMR ensured there was a full and continuing programme of development to facilitate this and to enable the Board to effectively manage all the PCTs statutory responsibilities.
10.2.4 NHSHMR implemented a full mandatory training package via on line training tools. This included online training sessions, each with a pass/fail test. All staff were required to achieve the set pass rate in order to complete the training. Completion of these mandatory training packages was closely monitored by the Locality Leadership Team to ensure compliance.
10.3 Skills – Where we are now
10.3.1 Scores in Table 6 are given out of 5 with 0 being the minimum score and 5 being the maximum.
Table 6: Skills Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Capacity and Capability:
Emerging CCG Structure and Capability: Learning &
Development
1
3
Leadership Capacity and Capability:
Leading a Commissioning Organisation
3
4

33
10.4 Skills – What has been done
10.4.1 HMRCCG completed a programme of development for CCG Clinical Leads that has included a series of learning sessions providing information on the following areas; Finance, Continuing Health Care, Quality and Clinical Governance, JSNA, Mental Health and Learning Disabilities, Equality and Diversity, Communications and Engagement, Children‟s Commissioning, Emergency Planning, Internal Audit, Information Governance and Security, Voluntary and Community Sector, Safeguarding, Health and Safety and Troubled Families. These sessions have been delivered by internal and external experts in these areas.
10.4.2 Governing Body members have also attended various external development sessions including Media Training, Chairing Meetings, Strategic Planning and Implementation, Data Protection, Safeguarding Children and Adults, Equality and Diversity and Leaders for Change.
10.4.3 HMRCCG‟s Clinical Chair Designate and the Chief Officer Designate have engaged the services of an external coach and mentor to support Personal Development Plans following their appointment.
10.4.5 HMRCCG has undertaken a Skills Audit which assessed the Governing Body‟s competence against the core competencies set out in the National Commissioning Boards “Clinical Commissioning Group Governing Body Members: Role Outlines, Attributes and Skills”. The outcomes of this audit are given in Appendix 5. This skills audit was completed via self-assessment and this will be further tested by a buddy or group challenge exercise.
10.5 Skills - What needs to be done
10.5.2 Personal Development Reviews are scheduled during January and February 2013 resulting in Personal Development Plans for all Governing Body members. As the CCG matures, this will be extended to determine base line skills, knowledge and experience of its wider clinical and primary care workforce.
10.5.3 The skills audit provides a high level view of competence across all of the Governing Body and a number of key areas were highlighted where further development would be beneficial. These include understanding the role of governance and seeing it as a supportive tool, finance and contracting and IT skills. The following ongoing development has been planned:
a) Two development days have been planned for the Governing Body and CCG Senior Management Team. These two sessions have been designed to support the CCG to fully understand how a distributed leadership model can work best in a membership organisation, testing out the challenges of being both “corporate” and “local” and developing the associated leadership skills and behaviours.
b) A facilitated session with NW Leadership Academy will take place in March 2013. This session will be a diagnostic tool to help the CCG measure its

34
capacity and capability by a series of good practice statements that describe the processes, structures, capabilities and skills that a high performing, fully authorised Governing Body will need to display.
c) Coaching for the CCG Team will be taken forward by the NW Leadership
Academy.
d) The Financial Governance Framework will be utilised to support the development of the financial plan for the next three years and to widen and enhance Governing Body members understanding of financial management and good governance.
10.5.4 A full mandatory training programme for all staff will be implemented via the GM Shared HR and OD service and will be monitored via the CCG Executive Team to ensure compliance. This will include Safeguarding (Children and Adults), Equality and Diversity, Information Governance, Fire Safety and Health and Safety. In addition the Designated Safeguarding Nurse is undertaking an audit of Safeguarding training annually which will be presented to Governing Body for assurance.
10.5.5In addition to the mandatory training for Safeguarding of Children and Adults (Level 1) there will be a requirement for all staff to undergo a needs analysis to ensure that they received appropriate role specific training in Safeguarding. These individual training needs will form part of their personal development plan agreed by their line manager.
10.5.6In addition to the mandatory training for Equality and Diversity the CCG will need to complete a Training Needs Analysis to ensure that it will meet the requirements of the Equality and Diversity Strategy Competency Framework, and procure and appropriate provider to deliver this.
10.5.7Training needs for all employees will continue to be monitored via the Personal Development Review (PDR) process.
10.5.8 The CCG is committed to the education and training of the NHS workforce and it will work in partnership with the Local Education and Training Board to ensure that the system for the planning, commissioning and delivery of education and training is able to respond to service commissioning priorities.

35
11.0 Shared Values
11.1 The capabilities that we need to continually develop
11.2 Shared Values – Our Legacy
11.2.1 NHSHMR had a fully developed set of values that were developed to be an integral part of the internal organisation but also to be an expression of the way that business was conducted and to further develop and maintain internal and external relationships. All staff were fully aware of the values and associated behaviours.
11.3 Shared Values – Where we are now
11.3.1 Scores in Table 7 are given out of 5 with 0 being the minimum score and 5 being the maximum.
Table 7: Shared Values Diagnostic Results
Domain Assessment Result
December 2011 August 2012
Clinical Focus and Added Value:
Values and Behaviours
1
3
11.3.2 Whilst it is recognised that much has been achieved in this area in defining the organisation as described in sections 2.5, 2.6 and 2.8, this is still a development area.
11.4 Shared Values – What has been done
11.4.1 As detailed in sections 1.1 to 1.4 HMRCCG has worked hard to define the organisational mission, aim and values. These values define the standards and behaviours expected of individuals within the organisation. They are the “ethos” by which we will achieve our goals and provide a broad framework for individuals to operate in. Values must support the purpose of the organisation and most importantly, must be shared. They should be shared not only internally but with our stakeholders and providers all must understand that this is the way that the CCG will do business.
11.4.2 A Constitution has been developed by the CCG which also includes detail in relation to the mission and values of the organisation. All member practices have signed this document.

36
11.5 Shared Values - What needs to be done
11.5.1 Ongoing work includes:
a) Embedding of organisational values with all staff and member practices
b) Communication and engagement with all staff and stakeholders, including all providers, regarding our shared values.
c) Continue to review CCG values and how these are articulated and integrated within our daily work and activities.
d) Ensure that our values and those of the NHS Constitution are reflected in mature organisational behaviour that enables effective partnering and respectful business relationships. The CCG considers this to be critical to our future success given the many challenges that lie ahead.
e) Continue to improve and develop communication and engagement across the CCG and with our partners and stakeholders.
f) Review our engagement mechanisms with the public and ensure that all three localities are reached and all views heard. Engagement events are likely to be at locality or neighbourhood level with Locality Engagement Officers, with Clinical Leads taking pivotal roles.

37
Plan on a Page NHS Heywood, Middleton and Rochdale
Appendix 1
STRATEGIC THEMES OBJECTIVES OUTCOMES PROGRAMMES
To improve the population’s health and well-being and to improve the health of the poorest fastest
Support people to choose take responsibility to choose and maintain a healthy lifestyle
Reduce alcohol related admissions by 50% from 2009-2014 (support to min pricing in GM) Reduce prevalence of smoking by 2.7% to 26% by 2014 Reduce death rate for CHD to 55.7 per 1000 by 2014 Reduce health inequality gap with improvement in health/dis domains by 3% in worst SOAs
Childhood obesity Generic brief interventions Reduce tobacco use and alcohol related harm Integrated health improvement system
To prevent ill health and reduce the number of people living with preventable ill health
Increase in life expectancy for men by 18 months and women by 12 months by 2014 Achieve cancer waiting time targets/screening targets
AAACM mortality plan Suicide prevention strategy Early diagnosis of cancer/waiting times
Commission a transformed health system with a focus on prevention and restorative health that responds to the changing demographics of the Borough and is safe and high quality
Implement agreed commissioning strategy action plans (LTCs, unscheduled care, scheduled care, primary care, mental health)
Measures of improvements in mental health (see mental health strategy) Children‟s outcomes (see joint plan) 10% increase in people dying at home by 2014 % funding shift to primary/community care
Strategic Plans – action plan Re-ablement L Dis self assessment Transport Carers
Development of health visiting strategy Modernised HV service Health visiting
Agree joint commissioning scope for adults and children
Agreed budgets aligned and agreements secured Joint commissioning (with HWBB)
Re-design healthcare system for Rochdale post Healthy Futures/TCS programme (including future of Rochdale Infirmary)
Health system refocused on needs of current and future population Commissioned transport alternatives Improved access to diagnostics
Re-designed ophthalmology, dermatology AQP
Improve quality and access in primary care services for all sections of the community
Implement primary care strategy Reduced unjustified variation in GP practices 90% of expected population on registers for COPD/hypertension
GMS/PMS/enhanced services/EA review Same day access Variation (peer review) QUOF validation
Cost effective prescribing expenditure and improve quality of prescribing
Prescribing improvement in areas of unjustified variation QIPP prescribing NE prescribing
Be a high performing CCG and deliver the best outcomes against return on investment with decreasing levels of funding
Agree and implement governance framework
Open, transparent and efficient decision making processes in place Statutory duties delivered E and D duties delivered
Authorisation programme
Deliver safeguarding duties effectively Effective safeguarding in place for adults and children Safeguarding boards
Agree and deliver best value programme (quip)
£11m saved in 2011/12. £4m savings planned for our QIPP target for 2012/13 Commissioning specifications improved
Best value
Drive organisational performance to deliver agreed targets and objectives
Performance targets monitored and delivered Risk management and assurance frameworks in place
Performance mgt Risk mgt
Ensure effective monitoring frameworks are in place that provide assurance on provider performance and drive improvements
Quality schedule in place Contracts agreed and levers clarified and implemented Quality framework Improved patient experience
NE Sector collaboration and integration
Achieve authorization for CCG Authorisation achieved by April 2013 (latest) Authorisation programme
CONTEXT : Population 240,000, 25th
most deprived borough, health challenges CVD and COPD linked to smoking prevalence, alcohol – growing numbers of admissions,
mortality rates, childhood obesity increasing. Most services provided by Pennine Acute and Pennine Care, 39 practices – 1 CCG with three localities
VISION : To improve and protect the health of people living in the Rochdale Borough by using resources fairly, openly and innovatively and cooperatively
Ap
pe
nd
ix 1

38
Appendix 2

39

40
41
Appendix 3
CSS Input
Programme Support Technical Support Output
Performance reports (QIPP contract & corporate performance) at CCG programme level Flashcards at clinical programme & CCG level Presence at Programme & QIPP meetings
CCG’s Input
Clinical Leadership SLA with CSS North East Sector programme management office for CCG‟s Relationship management with LA Output
Decisions to improve performance
Organisational Arrangements
Sponsor organisation to provide administration support for programmes
Programme leads to own corporate performance indicators
NES Programme Manager Role, (Working directly to the Heads of Commissioning)
CSS/CCG Products to be developed CCG
1.QIPP plans at Sector CCG level produced 2. Review meeting arrangements and requirements CCG/CSS
3. Balanced scorecards flash reports at CCG & programme level produced 4. Operating model for CSS CCG business model defined 5. Programme Management Office for CCG‟s and CSS in place 6. Define roles of Sponsor and roles of Programme Manager 7. Standard document templates produced CSS
8. Organisational development plan for CSS staff including leadership of the function in place
Principles of Working North East Sector will deliver individual CCG objectives & priorities including QIPP Programme Managers will provide leadership to ensure the commissioning support infrastructure works in a different way The arrangements will maximize potential to do things once and release efficiencies quicker Co-location of teams where appropriate & proportional Full engagement and integration of social care operationally & in planning Effective collaboration between & with all programme managers
North East Sector Commissioning Board
CCG Heads of Commissioning
NES Programme Manager Chrisella Morgan
North East Sector Contact Board Infrastructure
Elective Care Sponsor K. Wynne-Jones Programme Manager Charlotte Booth
Cancer & EOL Sponsor Ian Mello Programme Manager Deborah Sullivan
Drugs & Therapeutic Sponsor S. Martin Programme Manager
Naomi Ledwith
Mental Health Sponsor Ian Mello Programme Manager Rachel Snow -Miller
Children‟s Sponsor S. Martin Programme Manager Karen Kenton
LTC Sponsor K.Wynne-Jones Programme Manager David Latham
Urgent Care Sponsor Ian Mello Programme Manager Nadia Baig
Community Services (HINQ) Sponsor K Wynne-Jones Programme Manager/Sponsor
Naomi Ledwith
Ap
pe
nd
ix 3

42
Ap
pe
nd
ix 4

43
Appendix 5
Clinical Commissioning Group Skills Audit
Initial Anonymised Data
Introduction
The NHS Commissioning Board document “Clinical Commissioning Group Governing Body Members: Role Outlines, Attributes and Skills” published in April 2012 sets out the competency expectations for the CCG Governing Body.
The aim of this skills audit was to establish a high level baseline of competencies to support ongoing Governing Body development as described in the Organisational Development plan.
All Governing Body members have now completed the audit and the anonymous data is presented in this report.
Anonymised Data
The following tables show the anonymised data for each of the competencies measured expressed as the highest, lowest and average scores.

44
The ratings are provided below for reference:
Rating Description of Competency Level
1 No current knowledge or skill (no competency)
2 Some awareness but not sufficiently competent to use it
3 Familiar with and able to use the competency (some competency)
4 Proficient in the knowledge or skill and able to show others how to use it (high level of competency)
5 Expert with a high degree of skill and/or comprehensive knowledge (fully competent)
Additional Development Areas
The skills audit gave individuals an opportunity to share any other development areas they believed important, outside of the competencies listed above.
A high level summary of these is provided below. Please note where comments provided have been very specific to an individual‟s role, these have not been included:
Development of influencing skills
Support in widening input into areas outside of individuals specific expertise
IT skills improvement
Presentation skills
Regular Media Training
Strategic Thinking
Governance as a support tool
Improved understanding of contracting arrangements
Conclusion
It should be stressed that no accurate conclusions can be drawn from the data expressed in this high level format. However, the following points should be noted:
The Governing Body has a high level of combined competence across all of the competencies
measured. The average scores range from 3.4 to 4.1.
All but one competence (Leadership Essence) have 1 or more individual rating themselves as
5.

45
The low scores show more variation ranging from 1 to 3. However, this is only meaningful if
individual roles are considered.
In addition it should be noted that this data is based entirely on self-assessment.
Recommendations
There are two clear recommendations that will support this skills audit adding real value and becoming a meaningful measurement and assessment tool:
A mechanism should be found to share individual results in order to support individuals to
ensure that their self-assessment is an accurate reflection of their competence in these areas.
This will need to be agreed in a manner which is comfortable for all members.
A more detailed analysis of individual scores should be carried out, in comparison with job
roles within the Governing Body, to determine if there are any key development areas for
either individuals or the Governing Body as a whole.

46
Identified Development Area
Action Deadline Responsible Person(s)
Values and Behaviours
Communicate “Organisation on a Page” to all stakeholders, including via new CCG website
Complete Head of Operations & Engagement
Gain sign up to the Constitution from all member Practices Complete Head of Operations and Engagement
Ensure that recruitment processes reflect the style of the organisation
Complete Head of Operations & Engagement
Ensure that Personal Development Reviews reflect the stye of the organisation
End Feb 2013 Head of Operations & Engagement
Identified Development Area
Action Deadline Responsible Person(s)
Continuous Improvement
Progress the Variation Group by exploring the role of Locality Engagement Officer and Data Analysts
Complete Head of Operations & Engagement
Continue to improve clinician to clinician relationships with providers to support improved outcomes
Ongoing Chief Officer, CCG Chair and Clinical Leads
Review our engagement mechanisms with the public to ensure that all localities are reached
Ongoing Head of Operations & Engagement
Reinvigorate Patient Participation and Engagement groups Ongoing Head of Operations & Engagement
Ap
pe
nd
ix 6

47
Identified Development Area
Action Deadline Responsible Person(s)
Administrative Functions
Establish processes and systems to ensure appropriate monitoring of CSU products, in line with SLA
Complete Chief Officer
Finalise CSU arrangements by resolving outstanding issues End Feb 2013 Chief Officer
Work closely with RMBC to establish new working arrangements following the transition to Public Health.
End Feb 2013 Chief Officer
Identified Development Area
Action Deadline Responsible Person(s)
Emerging CCG structure and capability
Appoint to Governing Body Designate roles Complete Chief Officer, CCG Chair
Appoint to Governing Body Lay Member roles Complete Chief Officer, CCG Chair
Appoint to planned CCG Structure Mid Feb 2013 Executive Management Team
Appoint to the Secondary Care Doctor Governing Body Post End Jan 2013 Chief Officer, CCG Chair
Develop succession plans for Clinical Leadership Roles End Feb 2012 Chief Officer, CCG Chair
Develop a skills audit for Governing Body Complete Head of Operations & Engagement
Complete skills audit for Governing Body once appointed into designate roles
Complete Head of Operations & Engagement
Complete PDR for all Governing Body members Jan/Feb 2013 Chief Officer, CCG Chair
Complete PDRs for all CCG Staff Feb 2013 Appropriate Managers
Deliver development plan for all CCG staff including induction, mandatory training, values & behaviours, ways of working
March 2013 Head of Operations & Engagement

48