organizational learning and service quality in … · organizational learning and service quality...
TRANSCRIPT
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 1
ORGANIZATIONAL LEARNING AND SERVICE QUALITY IN HEALTHCARE INDUSTRY
Thilageswary Arumugam (Corresponding author)
University Putra Malaysia (UPM)-Malaysia E-mail: [email protected]
Khairuddin Idris
University Putra Malaysia (UPM)-Malaysia
E-mail: [email protected]
Zoharah Omar
University Putra Malaysia (UPM)-Malaysia
E-mail: [email protected]
Komati Munusamy University Putra Malaysia(UPM)-Malaysia
E-mail: [email protected]
ABSTRACT The aim of this work is to establish the relationship between organisational learning and service quality in the public healthcare industry. Unit of analyses consists of clinical and clinical support departments in public hospitals. Service quality perception is obtained from patients and organizational learning assessed by the head of departments. Utilizing the AMOS Structural Equation Modelling and SPSS, data were analysed. The hypothesised model has provided a model fit between the constructs contributing to the theoretical body of knowledge. Study reports that the level of organizational learning and service quality are at the moderate level among public hospital departments. Findings reveal that the hypothesis is supported. Organizational Learning
Action has significant and positive relationship with Service Quality. Keyword: Organizational Learning Systems Model, Organizational Learning, Learning Action, Service Quality
1. INTRODUCTION Public health care is part of the key areas of national economic growth. However, one
significant problem encountered here is the increase of aging population in Malaysia
(Economic Intelligence Unit, 2014) despite the data highlighting that Malaysia’s
healthcare quality is progressing (Human Development Index, 2015). The GDP for
healthcare expenditure in Malaysia is 4.03 in 2013 according to World Bank. The Malaysian population is estimated 30 million in beginning 2015. The age dependency ratio
of population in Malaysia is 52.9% which is relatively high based on United Nation, 2015.
Based on Malaysian population distribution is pyramid is an expanding type. The
pyramid indicates relatively short life expectancy, low level of education and poor
healthcare (United Nation, 2015). Public hospitals in Malaysia have excess demand
where demand for subsidy exceeds the supply highlighting significant problem like longer waiting time of patients to obtain treatment (Pillay, et al., 2011). Thus, the
challenge is uprooted to sustain the hospital care progressively. Adversely, there have been
steady increases in admission rate, outpatient attendance, pathology workload and
inadequate human resource skilled workforce (Yusof, 2014). From the patient's
perspective, there is an increase of population, especially aging population, burden of diseases and dependency on hospital facility (Yusof, 2014). MOH shows an increase in
non-communicable diseases which is 250% increase from year 2002 to 2012 (EIU, 2014).
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 2
One problem claimed by the President of Malaysian Medical Association is attention needed to improve healthcare service and especially public healthcare that faces brain
drain (Star, 2015). Another factor that contributes to poor service is also due to
inefficient process, time wastage, over- processing imbalance of bed utilization, lack of
specialist care, and so on (Pillay et al., 2011; Rose, Uli, Abdul, & Ng, 2004). Notably, the
government has looked into the concept of lean management rooted since 2013 as a way
to tackle these issues (Lani, 2014). This new approach is swayed towards patient centered to avoid congestion, waiting time, long process, etc. (Yusof, 2014). Looking into this
scenario, there seem to be more to be done from the administration and the
management part in order to deliver a quality service to the patients in public hospitals.
The Malaysian healthcare issue is also seen along this trail of literature whereby numerous studies had been done to measure the level of quality service delivery or patient
satisfaction in Malaysian public and private healthcare in the past (Manaf, 2005; Pillay et
al., 2011; Rashid, & Jusoff, 2009; Suki, Lian, & Suki, 2011). However, specifically in the
research conducted, Malaysian healthcare has found service quality in some aspects
needs improvement (Lam, 2010; Manaf, 2012; Pillay, et al. 2011; Rose, et al., 2004;
Sohail, 2003). One of the improvement needed is to achieve patient satisfaction which has always been an important method to measure in quality aspects ( Chakravarty, 2011;
Kapoor 2011; Rasiah, Wan Abdullah, & Tumin, 2011).Hence, customers [patients] play
an important role in measuring quality service delivery of healthcare in the organization
(Babakus & Mangold,1992; Bakar, Akgün, & Assaf,2008; Elluech, 2007; Kapoor,2011;
Pillay et al., 2011; Rad, 2005; Rose et al., 2004;).
Service quality is generally measured by customer satisfaction that reflects the
organizational performance (Ramayah, Samat, & Lo, 2011). Quality service is a perceived
quality which means a customer's judgment about a service (Cuiberg & Rojšek, 2010).
Quality is the service that occurs during delivery of intangible, heterogeneous and
inseparable service delivery during and interaction between customer and provider (Zeithaml, Parasuraman, & Berry, 1990).This is crucial especially in healthcare industry
where patients’ perception on the service are significant (Brahmbahatt,2011) because
hospitals’ service is highly prone to errors compared to other industries (Natarajan,
2006). There has been an increase in quality in the healthcare sector. This is an
important question to adhere in hospitals and has been supported empirically by numerous studies (Pillay et al., 2011;Bakar, et al. 2007; Elluech, 2007; Kapoor, 2011;
Manaf, 2012; Rad, 2005; Rose et al,. 2004). Service quality output has been measured
from vast paradigm; customer experience, customer satisfaction, number of errors,
customer awareness, people management, waiting time, quality management empirically
(Bakar et al., 2008; Elleuch, 2008; Elluech, 2007; Kapoor, 2011; Manaf, 2012;Pillay et
al., 2011; Raja, Deshmukh, & Wadhwa, 2007; Rad, 2005; Rose, 2004;) and customer dissatisfaction (Jamali,2008). This is evident empirically that there is significant and
positive relationship between quality and customer satisfaction (Boulding, et al., 1993).
Service quality based on patient satisfaction of public hospital, which consists medical
services and overall service (Aagja & Garg, 2010). This service quality dimensions are designed for public hospitals. The root work is based on (Parasuraman, 2010) (There are
two dimensions used here. Medical service is defined as having knowledgeable doctors,
nurses, staff and prevent acquired disease. The second dimension is overall service which are defined below (Aagja & Garg, 2010): Tangible. This term refers to the use of modern
equipment, appealing material and facilities and professional appearance of staff (Sohail, 2003); Reliability. This term refers to the ability of the hospitals to provide promised
service and error-free record (Sohail, 2003); Responsiveness. This term refers to prompt services given and willingness to help patients (Sohail, 2003); Assurance. This term refers
to the ability to handle patients’ problems, instil confidence, courteous and knowledgeable
(Sohail, 2003).
On the other hand, studies indicate organizational is lacking in organizational learning
(Maden, 2011) and that many studies have ascertain the importance of learning in healthcare delivery (e.g. Damschroder, et al., 2009; Lipshitz, & Popper, 2000; Tucker,
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 3
Nembhard, & Edmondson, 2007). Organizational learning important in the healthcare industry mainly to overcome mistakes and errors (Kim, Newby-Bennet, Song,2011) and to
face the various pressure in public healthcare (de Burca, 2000).Numerous empirical
research focuses on how organizational learning works in action at workplace through
learning (Gorelick, 2005; Johnson,2000; Lakhani, 2005; Mauchet, 2011). Although
some theories of learning had been studied only in workplace learning, some have
identified learning transferred into action. This approach is the sociological perspective. Comprehensively, OLSM identifies workplace learning into learning actions (Johnson &
Bailey, n.d). Schwandt & Marquardt (2000) adopted this sociological perspective of
organizational learning in their systemic model to reconcile several of the dissimilitude
extent in previous theories. Schwandt’s OLSM underpins Parson’s (1956) social action
theory. The learning model consists of four subsystem acquisitions, creation, sharing and retention and reuse of knowledge based on Parsons Adaptation (A), Goal attainment
(G), Integrative (I), Latent (L) which referred as AGIL. The study attempts to look into
the Organizational Learning perspective by applying the OLSM (Schwandt, 1997) which is
grounded from Parsonion Social Action theory (Johnson, 2000) to understand the gap in
the quality of service provided by hospital staff.
It is comprehensible that the service quality concept is a significant performance output
(Brady, Cronin & Brand, 2002). Past literature has taken tremendous effort in measuring
the delivery of quality service to patients as an indicator of performance level (Cronin &
Taylor, 1994). On the other hand, learning in the workplace has been quite significant in
improving this type of organizational performance (Maden, 2012) along with the current popular approach to innovation concept. Further to what have been discussed,
it is judicious to study the link between organizational learning and service quality.
This research contributes to fill the gap in the public healthcare in Malaysia, as this
industry plays the role as a key economic area to the nation’s growth and progress. In
order to fill the service quality gap, the study objective examines whether organizational
learning has relationship with service quality. The proposed research framework comprises of exogenous variables Organizational Learning while the endogenous Service
Quality. As a result, this model has second order construct and based on this, the
following four research hypothesis have been formulated:
H1: There is a positive relationship between Organizational Learning and Service Quality
2.0 LITERATURE REVIEW 2.1 Service Quality Definitions and Models
Service quality generally means ‘perceived serviced quality’ and evaluation should
come from the ‘customer perspective’ (Padma, Rajendran, & Sai, 2009). Parasuraman et
al. (1985) defined service quality as ‘the global evaluation or attitude of overall excellence of service’. (Wang & Shieh, 2006) defined ‘service quality is the difference between customers’ expectation and perceptions of services delivered by service firm’.
In a review of service quality models it has been identified that about 19 existing service quality models (Seth, Deshmukh, & Vrat, 2005); some to name are technical
and functional quality model by Gronroos, (1984), GAP model by Parasuraman et al.,(1984), synthesised model of service quality by Brogowicz, Delene, & Lyth, (1990).
(Cronin & Taylor, 1992). Most studies rely on several service quality model namely,
technical and functional quality model by Groonroos, (1984), and GAP model by
Parasuraman et al.(1985). Performance only model developed by Cronin and Taylor (1992), Rashid and Jusoff, (2009) and Seth et al., (2005).
2.2 Quality Service in Healthcare
Defining quality and even the scale used in healthcare is difficult as there are so many subjective meaning. Quality in healthcare as stated by Joint Commission is ‘the degree to which patient care services increase the probability of desired outcome and reduce the probability of desired outcome’ which is similar to Washington Institute of Medicine
(WIM) (Kapoor 2011). Kapoor (2011) however defined quality in healthcare as ‘degree of adherence to pre-established standards based upon prevailing knowledge and practices’.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 4
‘Service quality’ in healthcare refers to all other aspects of the patient experience such as hospital comfort and patient can judge service quality more accurate than clinical
quality (e.g. surgical skill) (Bakar et al., 2008). It broadly defined by the authors as
meeting customer expectations or providing perfect service and ability of an
institution to meet or surpass customer expectations.
Quality is used in every organization to meet the standard performance of the internal and external requirement of an organization. Nevertheless, the external standards need like
the customers seemed to be more important. Additionally what need to be met in
‘quality’ differs from one industry to another or rather what aspects. In the era of
beginning of industrialization, quality attention was directed towards manufacturing
the goods. Then later, organizations swayed its interest in quality in providing service and it has become a sensitive term over the years. Though service quality is significant
for many countries, and is significant in many industries, but healthcare services is
always as its high risk involvement (Rashid & Jusoff, 2008). Service quality is not only
seen as technical quality but also functional quality is seen as on how service is
delivered to customer (Rashid & Jusoff, 2008). Customers in healthcare are the patients
who to be the focus, who carries different values and views (Duggirala, Rajendran, & Anantharaman, 2008). Though efforts taken on quality improvement in healthcare but
shortcoming in the delivery of effective and reliable care remain (Boyer, Gardner, &
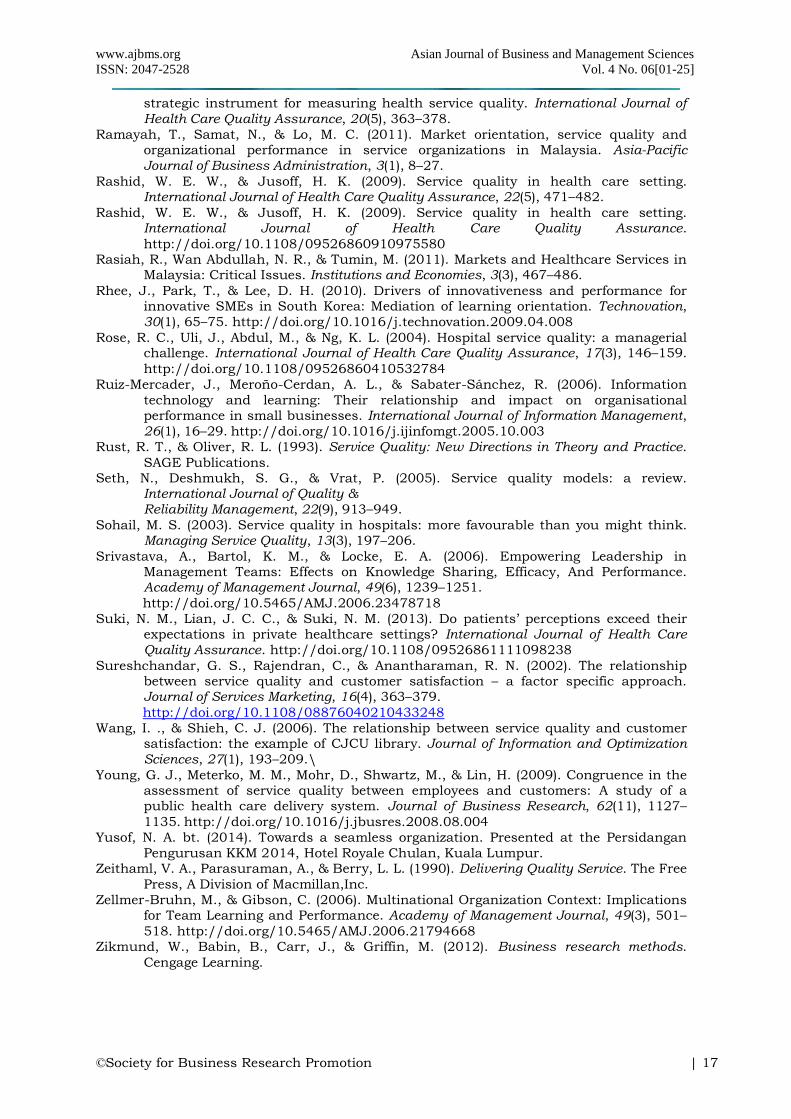
Schweikhart, 2012; Carman 1990). The extent of importance of service quality in the
healthcare setting can be viewed in Table 1. There been numerous service quality scale
development by many researchers to suit the countries healthcare setting. The dimensions use/developed by researchers are generally have some similarity. With regards
to this, it is notable that SERVQUAL (see Table 2) becomes the underlying model for the
instrument and studies conducted. Some of common analyses can be grouped into
services and empathy by hospital staff (doctors, nurses, etc.), amenities and facilities.
Some have gone for detail in developing scale precise for hospital setting.
Recently, Aagja and Garg (2010) attempted to adapt the measurement for public
hospitals which partly based on Duggirala’s work. The authors developed a scale for
measuring service quality from the patient perspective. Standard scale development
research procedure was followed based on experts. A reliable and valid scaled called
public hospital service quality (PubHosQual) measuring 5 dimension of hospital service quality; admission, medical service, overall service, discharge process and social
responsibility. However, it is emphasize that the dimensions are mainly grounded from
the work of Parasuraman, Cronin and Taylor. The dimensions were adapted from Carman
(1990) and (Rust & Oliver, 1993) on admission, medical service, overall service and
discharge.
Some research find SERVQUAL is reliable in healthcare but some doesn’t capture
healthcare dimension (Babakus & Mangold, 1992). SERVQUAL scale is important to tailor
to sector specific needs, culture or nation (Butt & Run, 2010; Parasuraman et al. 1991).
Critics argue that performance based measure is more appropriate for measuring service
quality (Sureshchandar et al., 2001). Many researchers has discarded the expectation in measuring service quality through SERVQUAL is still a preferred model in many sectors
(Butt & Run, 2010; Parasuraman, Zeithaml, & Berry, 1985). Andaleeb, (1998). Bowers
et al (1994) human interaction and relief from pain and suffering following treatment
not included in SERVQUAL. Many of the item adapted based from SERVQUAL,
SERVPERF and functional and technical quality. Based on these scales studies are
conducted in the healthcare industry. These studies have contributed to the development of quality clinical service and setting and identification of patient needs and expectations
or demands. In fact, customer satisfaction has an important outcome of service quality.
Bowers, Swan and Koehler (1994). In this notion, patient satisfaction and/or expectation
is examined to determine the level of service quality. Thus as many empirical evidence
have used patients or family members or friends to determine quality level (Padma et al.,
2009; Prasanna, Bashith, & Sucharitha, 2009). Patient or customer is important in Asian context because countries like India, Malaysia always accompanied by their family
members.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 5
Similar to other developing countries, Malaysia has been keen in managing service quality in the healthcare industry (Rose et al., 2004). Since, complaints has been prolonging
like long wait hours, unfriendliness, apathetic and uncaring attitude of staff are some
issues in Malaysia (Yusof, 2002). In comprehensive national study conducted found
issues on average lengthy waiting time employee attitude and work process, heavy
workload, management and supervision problems and adequate facilities are some
issues highlighted as problems in public hospitals in Malaysia(Pillay et al., 2011). Other service quality problem is intangibility of nature of service, maintaining the variability of
customer-employee relationship, educating patients of service provided (Rashid & Jusoff,
2009). It was found that medical staffs play an important role in determining customer
quality evaluation (Elleuch, 2008).
In 23 public hospitals Malaysian study, physical and clinical dimensions measured.
Results found that inpatient and outpatient were more satisfied with clinical dimensions
(Manaf & Nooi, 2007). The measure used was adaption of Institute Health Malaysia.
Similarly in another Malaysian context used SERVQUAL measure private healthcare
quality (Butt & Run, 2010). The instrument was based on modified for Malaysian context
but capture the five service dimensions. There was negative gap found between perception and expectation especially in service reliability
In healthcare setting patients rely on functional aspects like facility, food quality and
employee attitude, etc. (Rashid & Jusoff, 2009). Sohail (2003) analyzed patient expectation
and perception of the quality service using SERVQUAL in Malaysian setting. Results indicate that patients perceived value of service exceed expectations for all variables
unlike countries like Hong Kong (Sohail, 2003). On the other hand (Butt & Run, 2010)
used modified SERVQUAL to measure Malaysian private healthcare quality. Results
shows moderately negative quality gap on each service quality scale dimension. Seven(7)
point likert scale used in assessing the patients in private hospitals. It is found that
SERQUAL is robust for Malaysian context. However, the results indicate expectations are higher than the perception thus giving a negative gap in private hospitals. Service
‘reliability’ and ‘responsiveness’ indicates highest negative score. Malaysian healthcare is
still in need to find solution to solve problem not on ad hoc but long term.
Service quality is a complex performance construct (Young, Meterko, Mohr, Shwartz, & Lin, 2009). Employees may not be best in assessing the service quality that they tend to
assess lower than the customers. This study is about investigating of whether and to what
degree employees assess their service quality of their organization similar to their
customers. However employees tend to underestimate the service quality as compared
to patients. Longer tenure was associated with greater congruency, suggesting employee
more experience in organization gain skill in interpreting customer related cues about quality. Organization with stronger customer service oriented work climates presumably
have an infrastructure for collecting, analyzing, disseminating to employees information
about their customers attitude and opinions concerning service quality. Physicians
assessment of service quality were more congruent with customer assessments than
were the assessment of other employees. This is because they may have first-hand information about the quality issues. Thus, the connectivity physician and customer is
important.
As to meet this research context, adapts Aagja and Grag (2010) measurement on two
dimension; medical service and overall service. So far this is the preferred scale for this
study justifying that; the two dimension has got the validity and reliability test and most suitable for the Malaysian patients, has got lesser number of question as per field
experts concern, measures has SERVPERF & SERVQUAL context in more short and
concise manner except for ‘empathy’ as Aagja and Grag derive in separate dimension, and
finally the scale is meant for the Asian context. The other three dimensions (medical
service and overall service) were not adapted because it is non-feasibility; some
questions are not suitable for outpatient that violates the study methodology. Next, the section discusses the antecedent variable for the service quality study. Organizational
learning from the Parsons Social Action theory is elaborated.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 6
2.3 Parsons Action Theory
Talcott Parson has based his work from Pareto, Durkheim, Weber and Compte (Parsons,
1966), Shills and Bells (Schwandt & Marquadt, 2000). This is called system of social
action (Schwandt & Marquardt, 2000). Some of the other theorists whom have used the
Parsons theory are like Denison(1990), Silverman(1973), Burrell and Morgan (1979) and
Schwandt (2009). However Parsons theory used as foundation study is the Schwandt Organizational Model as the sociological perspective.
Action in Parsons theory is dependent on situation of goal oriented: situation of means
and condition, end/goal, norms and values, relating end to situation (Rocher, 1975).
The subsystem of actions is necessary for the social subsystem to function (AGIL). The
AGIL has mutual exchange:
1. Adaptation to environment(A)
2. Allocation of resources and goal attainment(G)
3. Interaction of systems Action(I)
4. Latent motivation patent (L)
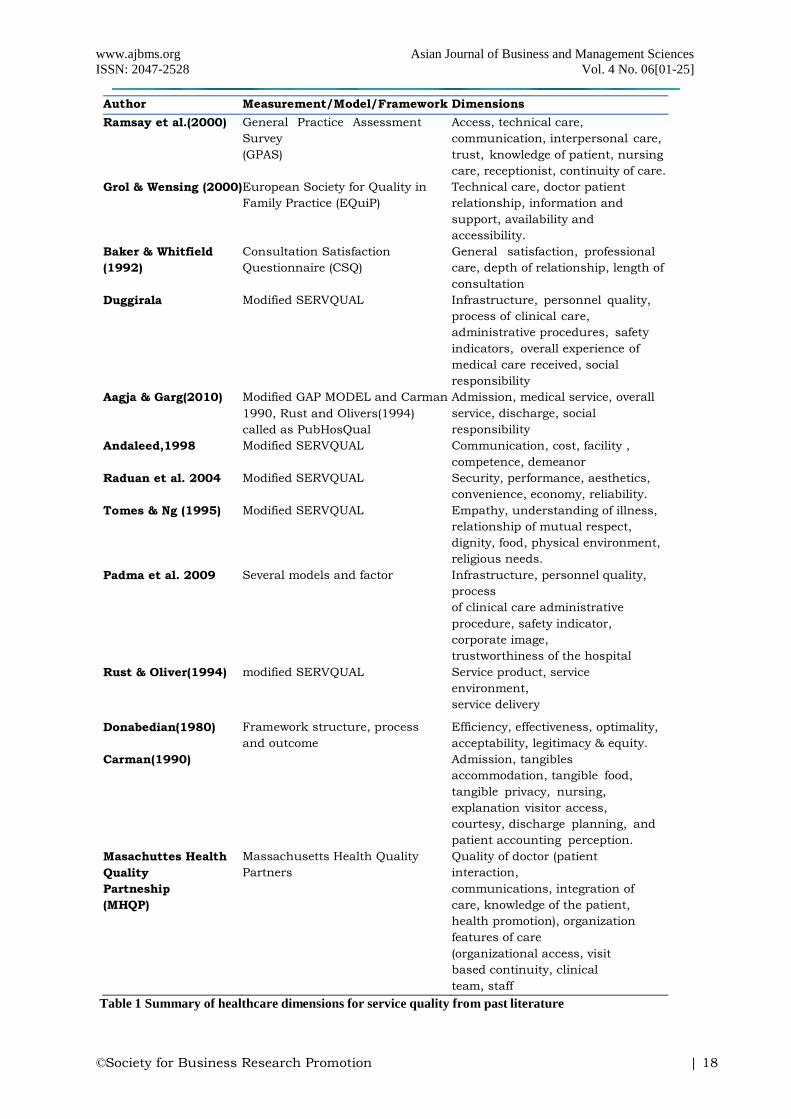
The four functions of Parsons General Theory of Social Action are applicable at all level of
analysis with integration of social, psychological and cultural element of organizational
dynamics depicted in Figure 1 (Gorelick, 2005; Johnson & Bailey, n.d.; Schwandt and
Marquardt, 2000). 2.4 Organizational Learning Systems Model
The Organizational Learning System Model is dependent on the collective learning for
change to take place. Schwandt & Marquardt (1990) finds that organizations are social
system that change based on performance and learning (Gorelick, 2005). This is
because on the Parsonion Theory of Social Action. Social Action Theory of Parsons is based on four integrated elements of social action (Gorelick, 2005; Johnson & Bailey,
n.d.; Schwandt,1997).
1. Actor/subject: an individual, group or collective
2. Situation: the physical and social objects which actor relates 3. Symbols: the means through which the actor relates to different situation and assigns
meaning to them, and
4. Rules, norms, values: the guiding factors for the actors relations with the
social objects in his/her environment.
Each subsystem has its functional prerequisites. Then the functional perquisites is interacts through the medium of interchange (input and output). With this the
subsystem continuously interacted with each subsystem. This is illustrated in Figure 2.
Later Schwandt (1997) emphasize the learning aspect of change in Parsons General
Theory of Social Action based in Figure 2 and described further in Table 3.
1. Environmental Interface Subsystem (adaptation): information obtained requires to
secure, filter and expel information [output: new information]
2. The Action/reflection subsystem (goal attainment): creation of valued knowledge from
new information, goal of learning system [output: goal referenced knowledge]
3. Dissemination/Diffusion (Integration): transfer the information and knowledge within
organization through informal and formal way [output: structuring] 4. The Meaning and Memory Subsystem (culture or pattern maintenance):
establishment of criteria for judgment, selection, focus, control of Organizational
Learning system. Beliefs, values, assumptions and artifacts - cultural component of
organization.[output: sensemaking]
The interchange medium for the learning subsystems are new information, goal reference knowledge, structuring and sensemaking (Schwandt and Marquardt, 2000).
OLSM signifies empirical evidence from sociological perspective reconciles the gap of
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 7
organizational theories (Lakhani, 2005). Action is can be associated with performance, or only with learning or both simultaneously as in Table 3. It should be understood that
any change occur through learning and performance actions. For the purpose of
analysis in this research these actions are separate to two independent system
(performance and learning). The analogy of performance and learning reflects in the
actions of organizations. It is actually difficult to see the learning act, however to
understand learning which may be seen in cognitive or behavior changes (performance). OLSM focuses on Organizational Learning as a social system and how it learns to
survive in the environment (Schwandt & Marquardt, 1990). It is grounded from
Parsonian theory which rooted from works of Pareto, Durkheim and Weber (Parsons,
1966). The OLSM comprise of subsystem, functions and output for each tabled as
below. The symbolic patterning, performance defined as maintaining the system structure while the physical and social objects are acquired as possessions, used as
facilities possibility consumed, created or change in the system values (Johnson and
Bailey, n.d, p.3). Learning from symbolic perspective is processes of change in the
symbolic-meaning pattern of the system. Based on parsons work and Schwandt work
organizational performing action and organizational learning action:
“…Learning action complex social system of actions, actors, symbols and
process that enables an organization to transform information into valued
knowledge, which in turn increases its long run adaptive capacity.”
(Johnson 2000, p.57)
Studies through confirmatory factor analysis found organizational learning action are
valid through the OAS measurement (Johnson, 2000; Krishna 2008; Doiron, 2012;
Mauchet, 2011). Johnson (2000) found the reliability for the four dimensions ranging from 0.64 to 0.78.
2.5 Organizational Learning and service quality as performance outcome
Parson(1966) general theory of social action has performance and learning element.
Schwandt and Marquadt (2000) views learning process as integrated with performance
and learning. Unlike other scholars like Argris & Schön(1978), Huber(1991), Garvin
(1985) views learning as a process only. To sustain performance in organization performance and learning is important (Gorelick). In comparison with Schwandt’s
learning concept though it is integrated performance and learning but not sufficient to
ensure the organizations sustainability (Gorelick, 2005). Customer satisfaction is seen
as important provision in measuring health system performance (Brambhat et al., 2011). Customer performance is positively link to business performance (Peltier, Zahay,
& Lehmann, 2013). It is evaluated from customer retention for a long time and customer satisfaction, providing services. Scholars argue that performance based measure is more
appropriate for measuring service quality because is basically measure the consumer
attitude (Sureshchandar, Rajendran, & Anantharaman, 2002). Better service quality is
positively related to organizational performance. Service quality also has mediating effect
between market orientation and endogenous organizational performance (Ramayah,
Samat & Lo, 2011). Full involvement of entire workforce and continuous improvement is achieved for customer satisfaction (Evans & Lindsay, 2006).
Learning evidence-based decision support system in healthcare organization has
resulted in recognition of data quality improvement as key area of both strategic and
operational management in US healthcare. Managers are being to understand the
importance of formal, continuous data quality assessment in health services delivery and quality management (Lorence & Jameson, 2002). Learning error is to the extent of
frequency, severity, understanding, awareness of errors has improved their hospital during
last 3 years. On a particular factor of creating safety climate for patient to error learning
has shown significant and positive relationship indicating the structural model fit (Boyer
et al., 2012).
Quality healthcare can be achieved when task is refocused on learning organization (de Burca, 2000). Thus, having superior performance requires innovation to strengthen this
value chain, greater learning in organization is most needed (Weerawardena, 2003). This
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 8
can be supported by generative learning (March, 1991) that learning internally and externally is prerequisite to generative learning (Weerawardena, 2003). Lifvergren,
Docherty, & Shani (2011) argues sustainability of healthcare system depends on one of
learning mechanism to meet the dynamic challenges. Learning mechanism at cognitive
based (practice based) are concepts, values, frameworks expressed in the value
statement, strategy and policies of the organization. The other two is procedural based
(routines, tools, etc.) and structural (organizational infrastructure).
Organizational Learning is sequential information processing activities with assumption
that any process of knowledge socialization and collective learning is based on the
relationship that consist of building and sharing (Morrison& Sandmeier, 2008). OLSM
conceptualizes this notion of creating and sharing knowledge. Fiol & Lyles (1985) sees
this as process of Action (Morrison& Sandmeier, 2008). Companies make more profit
when integrated the customer know how into innovation process as Fiol & Lyles (1985) sees this as process of Action (Morrison & Sandmeier, 2008).
There is abundance of conceptual literature that concerns the relationship between
learning and performance (Chonko, Dubinsky, Jones, & Roberts, 2003). There is still
confusion in the organizational learning as yet to have appropriate measurement
development (Jyothibabu, Farooq, & Pradhan, 2010). There have been numerous study linked with organizational learning and organizational performance. However, both the
concepts are very wide in nature as there have been many theories and models pertaining
to it in the literature. This has been discussed above. Since the study is on healthcare,
performance of this industry is very much based on quality service delivery. Therefore,
further discussion highlights the possible type of relationship between organizational
learning and service quality. Organizational learning evidently enhance organizational performance (Kim, Newby-Bennett, & Song, 2013). The creation of a quality healthcare
when a task is refocused to creation of learning (de Burca, 2000).
Action learning is another concept that part of Schwandt’s organizational learning model.
Action learning able to create inquiry, share and create problem solving culture among
individuals and groups. Action learning able to measure return on investment, which
relates directly to workplace and impacts on organizational performance (Pounder, 2009). Peltier et al. (2013) finds that customer retention has positive link to business
performance. The business performance is evaluated from return on investment from
customer basis.
In South West London hospital study the term on evidence-based practice shows positive
effect on service provided in the hospitals. Learning can be obtained through library
information, problem or error based. An empirical analysis by Manaf (2005) in Malaysian public hospitals which sampled 23 hospitals studied in quality management practice.
Continuous improvement, strategic planning, quality assurance, teamwork, leadership
and management commitment, employee involvement and training and management by
fact and supplier partnership are aspects studied under the quality management aspect.
It was found that physicians as the important contributor of hospital is perceived lowest
among other category of staff.
One research on Indian power plant tried to identify an integrated scale for Organizational Learning through learning enablers, learning outcome achieved and
performance outcome (Jyothibabu, Pradhan, & Farooq, 2011). They argued that there is
yet to have appropriate scale to be developed for organizational learning which leads to
conceptual confusion. In their study they used Watkins & Marsick’s to measure the
facilitator of Organizational Learning. Organizational size studied as control variable in
past literatures as its large number of employees have more difficult time to share knowledge. Organizational level dimensions are employee empowerment, embedded
system, system connection and leadership for learning which found closely associated
with each other. Organizational Learning also directly contributes to performance than at
an individual or group. The OLSM model used focusing on Action/reflection (goal
referenced knowledge) and meaning/memory (sensemaking) (Schwandt & Marquardt, 2000).
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 9
Based on Raja, Deshmukh, & Wadhwa (2007) some healthcare problem identified in India as lack of competence, low technical quality and response to patient needs and lack
of evaluation. It was found that relationship, resource management, people management
and customer satisfaction has shown positive influence on service quality in India.
Similar issues is highlighted by Hulton et al., (2007) and his associates like inappropriate
procedures, lack of professional attendance and delay.
Kuo (2011) use Delaney and Huselid, (1996) performance measure service quality and
customer satisfaction from seven elements. In this Taiwanese study, the organizational
learning consists of goal setting, flexibility of HR requirement, providing clear guideline,
team and cross-cultural interaction. Organizational learning was found to positively
influence to organizational performances. This reported the same by (Ruiz-Mercader, Meroño-Cerdan, & Sabater-Sánchez, 2006). In team learning also influence performance
(Zellmer-Bruhn & Gibson, 2006). (Hanvanich, Sivakumar, & Hult, 2006) finds learning
orientation and organizational memory related to organizational outcome. In Kuo (2011)’s
study, organizational learning is measured in terms of information sharing, inquiry
climate, learning practices and achievement mindset based on Huber (1991) theory.
In one study on knowledge sharing is not only able to improve organizational
performance but also considered to enhance patient safety (Kim, Newby-Bennet & Song,
2011). Knowledge sharing concept by (Srivastava, Bartol, & Locke, 2006) team members
share idea, information and suggestion’. It is emphasis that hospital should have
learning system to improve patient safety which through knowledge sharing. In a study in Chinese public healthcare system found unsatisfactory delivery of services highlighted by
Lee, Ng and Zhang (2007). In order to overcome this as solution on performance
management tool like Balance Scorecard able to achieved to improve accountability
among employees. Based on Schwandt’s model, this consists of Integrative Performance.
The link between input and the resulting outcome can be rather complex in healthcare industry. Lack of knowledge here is important because it involves diverse specialization
group, e.g. doctors and nurses. Thus according to (Natarajan, 2013) the making of
systems thinking is complex. Some of the serious obstacles identified among employees
lack of awareness on problems, responsibility, understanding on the work process that
undermines the healthcare system. This actually notifies the need of performing and learning action aspects. Some of the healthcare performance are safety, effectiveness,
patients-centeredness’, timeliness and efficiency (Natarajan, 2013).
Organizational learning scale by (Hult, Ferrell & Hurley, 2002) used. The four factors
measurement model includes team orientation learning orientation, memory orientation
and learning system orientation. The study sampled managers of purchasing units in one of Fortune 500 multinational corporations. This is tested on the effect of cycle time
performance (time taken from initiation to completion). This is positively with learning
seminars which has direct and significant effect.
The greater organizational and individual learning, greater the change success e.g. customer satisfaction (Chonko et al., 2003). Their empirical evidences measure
specifically on sales volume of salesperson. This is because traditional performance
measure in general may not be adequate. It has to be outcome based like sales volume
or service quality level.
In a study on learning orientation consist of creating and using knowledge to enhance competitiveness (Calantone et al., 2002; Baker & Sinkula, 1999). This consists of
obtaining and sharing information about customer needs, market changes and competitor
actions, new technology development. In this study learning orientation is a reflective
construct commitment to learning, shared vision, open mindedness and intra knowledge
sharing (Calantone et al., 2002). It works as stores knowledge and takes feedback from
customers and develop core competency. We can understand that numerous studies identified the effect between learning and performance (competitive advantage, financial,
non- financial, customer satisfaction, etc.). However, what we infer so from empirical
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 10
researches is, whether any learning model link directly with organizational performance by integrating customers understanding on service or product. OLSM from a social
action perspective to be tested the relationship from learning and performing action
perspective. As conclusion, though is rather wide in scope the relationship relating to
the two constructs, there is yet fill the gap in this relationship. Of note, it is
comprehensible that past literature scope is mainly on the common performance outcome
rather than specifically on service quality.
3. METHODOLOGY
The study aims to examine the correlation between Organizational Learning (OL) and
Service Quality (SQ). It contains a description on philosophy of research, research design,
population and sampling, instrument, validity and reliability, data collection procedure and data analysis (Zikmund, Babin, Carr, & Griffin, 2012).
It involves collecting and analyzing numerical data and applying statistical test
(Creswell, 2007). The research attempts to obtain information on the characteristics of the
problem and predicting action on the basis of hypotheses. Thus, the study is grounded on
descriptive and predictive research type (Hussesy & Hussey, 1997; Sekaran, 2003). The research is based on a non-experimental survey study using self-administered
questionnaires. For the purpose of this study, structural equation modelling (SEM) was
conducted in order to verify the degree to which organizational learning is associated with
service quality in the medical industry. Samples were obtained from the public hospitals
in Peninsula Malaysia. Questionnaires were administered among two dissimilar groups of respondents; patients and head of departments in the selected hospitals. Drop and pick
method was used for the paper based surveys whereas SPSS 19.0 and Analysis of a
Moment Structures (AMOS) 21.0 have been used as statistical tools. Structural
Equation Modelling (SEM) is use to test hypotheses about a particular factor structure,
which produces goodness- of-fit measure using AMOS software (Albright, Myoung & Park,
2009).
The samples consist of multi-specialty hospitals such as maternity, orthopaedic and other
specialties which managed by the government (Aagja & Garg, 2010) as in Table 4. There
is total of 87 multi-specialist government hospitals situated in Peninsula Malaysia
(Ministry of Health, 2013). There are 55 hospitals which have a bedding capacity of more than 100 beds and been selected for the purpose of this study. Thus, with a total of
825 departments, 488 questionnaires were distributed to 23 hospitals upon the
approval received. from the Ministry. The study uses disproportionate stratified
random sampling procedure (Israel, 1992; Awang, 2014). Since the study covers an
exclusive and selected number of respondents from Peninsula Malaysia, drop and pick
and also self-administered survey method was used to obtain sufficient response form. 3.8 Measurement Instruments
Organizational Learning instrument were administered to the head of departments’ of
clinical and clinical support department as in Table 5 . All items uses the seven (7) point
likert scale. The likert scale also acceptable to assess patient perception measure (Butt & Run, 2010). The questionnaires consist of two major parts for patient and head of
department participants where the dimension items displayed in Table 6 and Table 7: Questionnaire A (respondent: head of department)
1. Organizational learning
2. Demographic profile (gender, age, frequency of visit, education level, treatment expenses and ethnic group) Questionnaire B (respondent: patients)
1. Demographic profile (job category, department, age, education, position, years of
working experience, years in current position)
2. Service quality The OAS instrument is owned by George Washington University, in which validated
further by Johnson (2000). The OAS measure Organizational Learning from the
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 11
learning action and performing action. The instrument rooted from the theoretical grounds of Schwandt’s (1997) dynamic social Action learning. OAS consists of 15
items from two sub-constructs organizational performing action and organizational
learning action used for this study from which four items dropped. Each serves with
four subsystems. Each question items begins with ‘To what extent…’ and followed
by a seven(7) point Likert scale from strongly agree to strongly disagree. However,
only the Learning Action is measured for purpose of measuring Learning Action.
This instrument however, was not plausible based on the experts’ opinions from
Malaysian public hospitals as a short and concise instrument was recommended. Thus, a
similar grounded instrument was adapted. The instrument from PubHosQual was adopted from the scale developed by Aagja & Garg (2010). It has four dimensions namely,
admission, medical service, overall service, social responsibility. Two relevant dimensions
(medical services, overall service) consisting of 13 items were adopted as shown in Table 7.
One (1) item dropped from medical service. The other dimensions were not adopted
because it was considered unfit for this research as it involves both outpatient and
inpatient and the time consideration to not disturb the patients. The advantage of this scale is that it is more specifically designed for public hospitals (Aagja & Garg, 2010)
though its grounded from ‘gap model’ of service quality by Parasuraman (1994), Carman
(1990) and Rust & Oliver (1994). Based on the exploratory, the coefficient alpha scores for
scale validation of medical service was 0.5880 and overall service was 0.8194.
4. DATA ANALYSIS
This segment discusses the result for dimension Learning Action and Service Quality.
The mean, maximum, minimum, standard deviation, skewness and kurtosis for all
constructs in Table 12. The total score of the respondents for the scales computed to
determine the levels of the constructs in the study. Subsequently, the level for the scales
of seven(7) point likert scale is categorized to three levels; high, moderate and low.
Learning Action scale comprises of four subcontract; Adaptive learning, Goal Learning,
Integrative Learning and Adaptive Learning. The mean ratings for Learning Action
dimensions and its subscales are also presented in Table
12. The integrated learning scored highest (µ=4.0400, σ=0.82758). Next the goal oriented learning scale (µ= 4.0226, σ=0.92659) and followed by Latent Learning (µ= 3.9898,
σ=0.87969) and Adaptive Learning has (µ= 3.9661, σ=0.86601). It is notable that the
mean values are not far distinct among the subscales which is less than 0.1. The overall
mean score for Learning Action was computed in determining the level of Learning Action
in hospitals. Overall high mean score of Learning Action indicated 4.00 which is above the
midpoint. The summary of descriptive statistics is shown in Table 4.2. Standard deviation is 0. 56519. Based on 7 point likert scale, minimum Learning Action is 2.33 and
maximum of 6.33. These values implies that the overall level of mean score indicate at
moderate level based on Table 13.
The overall mean score for Service Quality scale was computed in determining the level of Organizational Innovativeness in hospitals. Overall mean score of Service Quality is 3.9749
which is above the moderate level as in Table 12. The summary of descriptive statistics is
shown in Table 12. Standard deviation is 0.78753. Based on seven(7) point likert scale,
minimum Service Quality is 1.85 and maximum of 6.08. These values implied that the
overall level of Service Quality mean is moderately high. An examination of the values for
skewness and kurtosis indicates that the assumption about normality of the distribution is not violated. Likewise, service quality in public hospitals is perceived at a moderate
level by patients, consists of 79.19%. Though score indicate 175 aggregated respondents
falls in moderate level, the actual number of frequency score that represents is
(N=175x4)700 out of 884 respondents. The low level contributes to 23(10.41%)
respondents and equivalent score at the high level score as well.
The CFA results showing fitness indexes and factor loading for every item is presented in
Figure 3. The text output explaining the results in Figure 3 are presented in Table 8,9,10
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 12
and 11. Item would be deleted if factor loading less than 0.6 is achieved or check Modification Indices (MI) if model fit is not achieved. High value of MI (more than 15)
indicate redundant item in the model (Awang,2014). The indexes RMSEA, GFI, CFI
and Chisq/df were assessed in this study as it is frequently reported in literatures as in
Table 8 (Hair, et al.2010; Awang, 2014). Table 10, output is based on individual CFA on
the constructs. The items that have low factor loading were dropped. Two items dropped
in service quality dimensions and 2 items in learning action dimensions. Based on the measurement model for this study; the uni-dimensionality, validity and reliability have
been assessed. The construct validity, convergent validity and discriminant validity meet
the model fit requirement. The reliability of the model is met based on the assessing of
composite reliability (CR) and Average Variance Extract (AVE) in Table 11. It can be
assumed that data for all constructs for Leaning Action and Service Quality are approximately normally distributed in terms of skewness and kurtosis based on
calculated z value is within -1.96 and +1.96. An examination of the values for skewness
and kurtosis indicates that the assumption about normality of the distribution is not
violated as shown in Table 9.
Figure 4 presents the Standardized Regression Weight and Figure 5 presents the Regression Estimate. Based on the Standardised Regression Weight in Figure 4,
standardised beta estimate for Learning action (LA) effect to Service Quality(SQ) is 0.47 as
in Table 15. The value of coefficient of determination R2 is 0.22 in Table 16. It indicates the contribution of the exogenous constructs LA estimating SQ is 22%. The fitness index
assessment for the structural model is presented in Table 14. The standardised beta
estimate in Table 15, when LA goes up by 1 standard deviation, SQ goes up by 0.466
(SQ = 0.466LA). The probability of getting on critical ratio is 4.164 in absolute value is
less than 0.001 as in Table 15.
Hypothesis H1 findings reveals that Learning Action is found to have significant and
positive relationship with Service Quality. This implies that the higher the Learning
Action leads to higher Service Quality. This hypotheses was supported based on strong
path coefficient (β=0.376, t=2.625, ρ<0.05). When Learning Action goes up by 1 unit,
Service Quality goes up by 0.376. The regression weight for LA in the prediction of
Service Quality is significantly different from zero at the 0.05 level (two-tailed). Thus,
Learning Action has significant and positive effects on Service Quality. The result of hypothesis is presented in Table 17.
5. DISCUSSION
Organizational Learning to Service Quality is explained further since performing action
and learning action is a reflection of organizational learning. Both hypotheses H1 is
supported the study suggests that level of organizational learning has a substantial
criteria in defining their growth and success. It is being confirmed that the benefit of learning is through understanding patterns of behavior (Gillies & Maliapen, 2008)
Therefore, hospitals show a greater organizational learning, the higher the service
quality offered by the employees. At a time when quality and safety outcome of
healthcare institutions in limelight and sensitivity of the nature of services provided
(Jamali, Hallal, & Abdallah, 2010), calls for better management approach and increase responsibility is unlikely to be denied. Other factors in the organizational learning in the
systems model identified like structured, formalized incentives, team, collective individual
work and in collaboration shows quality healthcare is achieved through this (Ezziane,
Maruthappu & Wan, 2012) seems supporting the study. This represents the
action/reflection subsystem. The supports the finding that collaborative learning in team
improve patient safety and employee rewards improve as they identify critical mistakes (Goh, Chan, kuziemsky, 2013). It also agreeable that stronger group oriented culture
leads to better problem solving. Learning at work that generate actionable learning in
understanding organizational learning and provides change in work environment like
awareness on patient safety (Sujan, 2015). The influence of excellence care delivery,
ethical values, involvement, professionalism, value for money, commitment to quality and strategic thinking determines quality service delivery (Carney, 2013).
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 13
6. THEORETICAL AND PRACTICAL IMPLICATION These findings suggest that the theories may benefit from the incorporation of other constructs as suggested by the organizational learning scholars. The study examines specifically on one phase of performance outcome that is service quality. It evaluated the level of service quality based on employment actions that transformed from the hospital employees. This at once provides the value of planning and experience gained in the work and how it transforms to provide a total service to the patients. As discussed above, this research revealed the central role to deliver effectively and efficiently service to the patients. The research breaks a new ground by studying learning activities in healthcare context and by empirically distinguishing learning and performing action oriented, although the processes are the same (Gorelick,2007; Schwandt & Marquadt,2000;). In addition to advancing empirical understanding and methodological approach, this research also contributes to the development of the literature. The implication of this model fit suggests that knowledge based practices should
be carried out.
Lastly, the research suggests that future studies may consider a broader dimension of service quality recommended by service quality scholars in the healthcare industry. As the present study found lack of time, tedious procedures involve and need monetary aid for the current query. The organizational innovativeness measure was not being able to adopt at the wider scope based on dimensions developed by Wang and Ahmed (2004). This, however, can be carried out by the Clinical Research Centers in each state of Malaysia. Other than that, this study also provides several implications to the healthcare practices and MOH. On a practical ground, this work provides a stepping stone for hospitals seeking for better performance in servicing the outgrowing number of patients. Department heads can set up departments to act jointly and get along as a team to serve the patients. This helps to cut down on unnecessary processes. The learning organizational cultivation can be a source to improve quality of services provided. More generally, the departments will get to understand the factors that facilitate deliberate efforts to improve work practices, thus overcoming barriers to service output.
The study also provides insights for the practical field whereby practitioners and head of departments are able to connect the importance of creating a learning organization that subsequently affects the performance outcome. In fact, organizational learning enables them to cite the laggings in terms of competency among their department staff, which probably been a crucial thing to solve. The HRD professional and the Clinical Research Centers in every district and hospitals can create relevant interventions to tackle problems associated with providing quality service. This can be facilitated for competency training by MOH as well as in the performance management and quality management practice. To sum up, the findings help to understand better on the mechanism by which learning affect service quality. This reflects the need for combining clinical and administrative perspective in future research studies. It is hoped that the findings will lead to hospital administration and practices by the Ministry of Health and also future research that delves more deeply into these constructs.
7. RECOMMENDATION FOR FUTURE RESEARCH
This research is theoretically acceptable and practically applicable by presenting a model fit that links between the constructs. Future study should focus on the proposed practical model that clarifies more on the linkage of the constructs. The result of the study is directed to future research. As recommended by Babakus and Mangold(1992), functional quality isn’t just enough, besides the technical quality for long term quality management. Quality service recognition should not be the means to solve public hospitals’ problems, but organizational learning which should be the means that meets the ends for the hospitals. Organizational Learning System Model(OLSM) can also studied innovativeness as mediating effect. The cross-sectional nature of data gathered imposes the first methodological limitation. For this reason the other research design such as experimental and longitudinal are desirable when testing the causal study relationship between variable or in-depth case study. This probably gives a richer apprehension of the relationship of the constructs proposed in the model and serve further to examine the applicability and utility from a pragmatic tip of opinion.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 14
8. STUDY LIMITATION The study had both theoretical and methodological limitations. Although the empirical
effects of this study largely support the proposed research model, at least a few limitations
should be counted. The use of cross-sectional sample with questionnaires is a limitation.
Many similar studies find this methodology as a limitation (Rhee et al., 2010; Jiménez-
Jimenez, et al. 2008).Longitudinal may be more appropriate to study the linkage among
innovativeness, organizational and service quality established over time. The study was unable to consider all the departments, e.g. cardiology or psychiatry as it is highly
sensitive to approach patients and more time is require for that. Results may differ
pertaining to this. In addition the service quality measurement is more specific and,
not subjective based performance since performance has many different factors. The study
cannot be generalized to other industries as its focuses on public hospitals and caution should be taken when conducting research on private hospitals in Malaysia. Respondents
for service quality assessment are from mixed group; inpatient and outpatient, thus some
dimensions of the instrument were not able to be measured. In order to obtain
maximum response from all the departments without biasness and respondent
limitations, ‘attendants’ of patients were accepted for the questionnaire administration
e.g. Pediatrics department.
9. CONCLUSION
The result suggests that the organizational learning positive and significant effect on
service quality in the Malaysian public hospitals. This implies that, the governmental
policies and practice by MOH should aim more on creating learning organization that can stimulate more on learning and performing simultaneously. Given the growing
attention in healthcare problems (e.g. waiting hours, errors, treatment and
procedures) in service delivery in Malaysian public hospitals, this study provides
practical solutions for MOH in terms of facilitating learning and providing effective in
the service delivery to patients. Importantly, the study has contributed to the integration
of social system with organizational learning concept which this leads to path on future empirical enquiry.
REFERENCES
Aagja, J. P., & Garg, R. (2010). Measuring perceived service quality for public hospitals (PubHosQual) in the Indian context. International Journal of Pharmaceutical and
Healthcare Marketing, 4(1), 60–83. http://doi.org/10.1108/17506121011036033
Amaral, A. (2007). A self-assessment of higher education institutions from the perspective of the EFQM excellence model. In Quality assurance in higher education (pp. 181-
207). Springer Netherlands.
Andaleeb, S. S. (1998). Determinants of customer satisfaction with hospitals: a managerial model. International Journal of Health Care Quality Assurance.
http://doi.org/10.1108/09526869810231541
Babakus, E., & Mangold, W. G. (1992). Adapting the SERVQUAL scale to hospital services: an empirical investigation. Health Services Research, 26(6), 767–786.
Bakar, C., Akgün, H. S., & Al Assaf, A. F. (2008). The role of expectations in patient
assessments of hospital care: an example from a university hospital network, Turkey. International Journal of Health Care Quality Assurance, 21(4), 343–355.
Baker, W. E., & Sinkula, J. M. (1999). The Synergistic Effect of Market Orientation and Learning Orientation on Organizational Performance. Journal of the Academy of Marketing Science, 27(4), 411–427. http://doi.org/10.1177/0092070399274002
Boyer, K. K., Gardner, J. W., & Schweikhart, S. (2012). Process quality improvement: An
examination of general vs. outcome-specific climate and practices in hospitals. Journal of Operations Management, 30(4), 325– 339.
http://doi.org/10.1016/j.jom.2011.12.001
Butt, M. M., & Run, E. C. de. (2010). Private healthcare quality: applying a SERVQUAL model. International Journal of Health Care Quality Assurance.
http://doi.org/10.1108/09526861011071580 Calantone, R. J., Cavusgil, S. T., & Zhao, Y. (2002). Learning orientation, firm innovation
capability, and firm performance. Industrial Marketing Management, 31(6), 515–
524.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 15
Chonko, L. B., Dubinsky, A. J., Jones, E., & Roberts, J. A. (2003). Organizational and individual learning in the sales force: an agenda for sales research. Journal of
Business Research, 56(12), 935–946. http://doi.org/10.1016/S0148-
2963(01)00330-7
Cronin, J. J., Jr., & Taylor, S. A. (1992). Measuring Service Quality: A Reexamination and Extension. Journal of Marketing, 56(3), 55–68. http://doi.org/10.2307/1252296
Healthcare industry urged to improve services. (2015). The StarOnline. Retrieved
2015, from
http://www.thestar.com.my/News/Nation/2015/07/02 De Burca, S. (2000). The learning healthcare organization. International Journal for Quality
in Healthcare, 457- 458.
Delaney, J. T., & Huselid, M. A. (1996). The Impact of Human Resource Management Practices on Perceptions of Organizational Performance. Academy of Management Journal, 39(4), 949–969. http://doi.org/10.2307/256718
Duggirala, M., Rajendran, C., & Anantharaman, R. N. (2008). Patient-perceived dimensions of total quality service in healthcare. Benchmarking: An International Journal, 15(5),
560–583. http://doi.org/10.1108/14635770810903150
Economic Inteligence Unit. (2014, April 11). How sustainable is Malaysian Healthcare.
Retrieved from http://www.eiu.com/industry/article/1991716983 Elleuch, A. (2008). Patient satisfaction in Japan. International Journal of Health Care
Quality Assurance, 21(7), 692–705.
Gorelick, C. (2005). Organizational learning vs the learning organization: a
conversation with a practitioner. Learning Organization, The, 12(4), 383–388.
Hanvanich, S., Sivakumar, K., & Hult, G. T. M. (2006). The Relationship of Learning and
Memory With Organizational Performance: The Moderating Role of Turbulence. Academy of Marketing Science. Journal, 34(4), 600–612.
Healthcare industry urged to improve services. (2015). The StarOnline. Retrieved
2015, from
http://www.thestar.com.my/News/Nation/2015/07/02 Hult, G. T. M., Ferrell, O. C., & Hurley, R. F. (2002). Global organizational learning effects
on cycle time performance. Journal of Business Research, 55(5), 377–387.
http://doi.org/10.1016/S0148-2963(00)00161- 2
Hulton, L. A., Matthews, Z., & Stones, R. W. (2007). Applying a framework for assessing the quality of maternal health services in urban India. Social Science & Medicine,
64(10), 2083–2095. http://doi.org/10.1016/j.socscimed.2007.01.019
Jamali, D. (2007). A study of customer satisfaction in the context of a public private partnership. International Journal of Quality & Reliability Management, 24(4), 370-
385.
Jamali, D., Hallal, M., & Abdallah, H. (2010). Corporate governance and corporate social responsibility: evidence from the healthcare sector. Corporate Governance, 10(5),
590–602. http://doi.org/10.1108/14720701011085562
Jiménez-Jimenez, D., Valle, R. S., & Hernandez-Espallardo, M. (2008). Fostering innovation: the role of market orientation and organizational learning. European Journal of Innovation Management, 11(3), 389–412.
Johnson, C. G., & Bailey, M. R. (n.d.-a). VALIDATING AN ORGANIZATIONAL ACTION
SYSTEM MODEL FROM A LEARNING AND PERFORMING PERSPECTIVE.
Johnson, C. G., & Bailey, M. R. (n.d.-b). VALIDATING AN ORGANIZATIONAL ACTION
SYSTEM MODEL FROM A LEARNING AND PERFORMING PERSPECTIVE. Retrieved from:
http://www2.warwick.ac.uk/fac/soc/wbs/conf/olkc/archive/olk4/papers/johnso
n.pdf
Jyothibabu, C., Farooq, A., & Pradhan, B. B. (2010). An integrated scale for measuring an organizational learning system. Learning Organization, The, 17(4), 303–327.
Jyothibabu, C., Pradhan, B. B., & Farooq, A. (2011). Organisational learning and performance – an empirical study. International Journal of Learning and Change.
Retrieved from:
http://www.inderscienceonline.com/doi/abs/10.1504/IJLC.2011.041872 Kapoor, B. P. (2011). Why quality in healthcare? MJAFI, 67(3), 206–208.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 16
http://doi.org/10.1016/S0377- 1237(11)60040-3
Kim, Y.-M., Newby‐Bennett, D., & Song, H.-J. (2013). Knowledge sharing and institutionalism in the healthcare industry. Journal of Knowledge Management.
http://doi.org/10.1108/13673271211238788
Kuo, T. H. (2011). How to improve organizational performance through learning and knowledge? International Journal of Manpower, 32(5/6), 581–603.
Lakhani, M. A. (2005). Relational linkages between visionary leadership and organizational learning across the United States, Malaysia, and India (D.M.). University of Phoenix,
United States -- Arizona. Retrieved from:
http://ezproxy.upm.edu.my:2087/docview/305364099/abstract/9196137329F44
C38PQ/11?
Lani, A.b. (2014) A Paradigm Shift In The Public Service Delivery System. Presented at the Persidangan Pengurusan KKM 2014, Hotel Royale Chulan, Kuala Lumpur.
http://www.moh.gov.my/index.php/pages/view/1035
Lam, S. S. K. (2010). SERVQUAL: A tool for measuring patients’ opinions of hospital service quality in Hong Kong. Total Quality Management.
http://doi.org/10.1080/0954412979587
Lorence, D. P., & Jameson, R. (2002). Adoption of information quality management practices in US healthcare organizations: A national assessment. International Journal of Quality & Reliability Management, 19(6), 737–756.
Manaf, N. H. A. (2005). Quality management in Malaysian public health care. International Journal of Health Care Quality Assurance, 18(3), 204–216.
Manaf, N. H. A., & Nooi, P. S. (2007). Patient Satisfaction as An Indicator of Service Quality In Malaysian Public Hospitals. Asian Journal on Quality, 8(3), 113–122.
Natarajan, R. N. (2013). Transferring best practices to healthcare: opportunities and challenges. The TQM Magazine. http://doi.org/10.1108/09544780610707084
Padma, P., Rajendran, C., & Sai, L. P. (2009). A conceptual framework of service quality in healthcare: Perspectives of Indian patients and their attendants. Benchmarking: An International Journal, 16(2), 157–191.
http://doi.org/10.1108/14635770910948213
Parasuraman, A. (2010). Service productivity, quality and innovation: Implications for service-design practice and research. International Journal of Quality and Service Sciences, 2(3), 277–286.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1985). A Conceptual Model of Service Quality and Its Implications for Future Research. Journal of Marketing, 49(4), 41–
50. http://doi.org/10.2307/1251430 Parsons, T. (1966). The structure of Social Action: A study in Social Theory with special
reference to a group of recent european writers. (2nd ed.). The Free Press. Retrieved
from www.bookos.org
Peltier, J. W., Zahay, D., & Lehmann, D. R. (2013). Organizational Learning and CRM Success: A Model for Linking Organizational Practices, Customer Data Quality, and Performance. Journal of Interactive Marketing, 27(1), 1–13.
http://doi.org/10.1016/j.intmar.2012.05.001
Pillay, D. I. M. S., Ghazali, R. J. D. M., Manaf, N. H. A., Abdullah, A. H. A., Bakar, A. A.,
Salikin, F., … Ismail,
W. I. W. (2011). Hospital waiting time: the forgotten premise of healthcare service delivery? International Journal of Health Care Quality Assurance, 24(7), 506–522.
http://doi.org/10.1108/09526861111160553
Pounder, T. (2009). Using action learning to drive organizational learning and performance. Strategic HR Review, 8(3), 17–23. http://doi.org/10.1108/14754390910946530
Prasanna, K., Bashith, M., & Sucharitha, S. (2009). Consumer Satisfaction about Hospital
Services: A Study from the Outpatient Department of a Private Medical College Hospital at Mangalore. Indian Journal of Community Medicine : Official Publication of Indian Association of Preventive & Social Medicine, 34(2), 156–159.
http://doi.org/10.4103/0970-0218.51220
Rad, A. M. M. (2005). A survey of total quality management in Iran: Barriers to successful implementation in health care organizations. Leadership in Health Services, 18(3),
12–34. http://doi.org/10.1108/13660750510611189
Raja, M. P. N., Deshmukh, S. G., & Wadhwa, S. (2007). Quality award dimensions: a
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 17
strategic instrument for measuring health service quality. International Journal of Health Care Quality Assurance, 20(5), 363–378.
Ramayah, T., Samat, N., & Lo, M. C. (2011). Market orientation, service quality and organizational performance in service organizations in Malaysia. Asia-Pacific Journal of Business Administration, 3(1), 8–27.
Rashid, W. E. W., & Jusoff, H. K. (2009). Service quality in health care setting. International Journal of Health Care Quality Assurance, 22(5), 471–482.
Rashid, W. E. W., & Jusoff, H. K. (2009). Service quality in health care setting. International Journal of Health Care Quality Assurance.
http://doi.org/10.1108/09526860910975580 Rasiah, R., Wan Abdullah, N. R., & Tumin, M. (2011). Markets and Healthcare Services in
Malaysia: Critical Issues. Institutions and Economies, 3(3), 467–486.
Rhee, J., Park, T., & Lee, D. H. (2010). Drivers of innovativeness and performance for innovative SMEs in South Korea: Mediation of learning orientation. Technovation,
30(1), 65–75. http://doi.org/10.1016/j.technovation.2009.04.008
Rose, R. C., Uli, J., Abdul, M., & Ng, K. L. (2004). Hospital service quality: a managerial challenge. International Journal of Health Care Quality Assurance, 17(3), 146–159.
http://doi.org/10.1108/09526860410532784
Ruiz-Mercader, J., Meroño-Cerdan, A. L., & Sabater-Sánchez, R. (2006). Information
technology and learning: Their relationship and impact on organisational performance in small businesses. International Journal of Information Management, 26(1), 16–29. http://doi.org/10.1016/j.ijinfomgt.2005.10.003
Rust, R. T., & Oliver, R. L. (1993). Service Quality: New Directions in Theory and Practice.
SAGE Publications. Seth, N., Deshmukh, S. G., & Vrat, P. (2005). Service quality models: a review.
International Journal of Quality &
Reliability Management, 22(9), 913–949.
Sohail, M. S. (2003). Service quality in hospitals: more favourable than you might think. Managing Service Quality, 13(3), 197–206.
Srivastava, A., Bartol, K. M., & Locke, E. A. (2006). Empowering Leadership in Management Teams: Effects on Knowledge Sharing, Efficacy, And Performance. Academy of Management Journal, 49(6), 1239–1251.
http://doi.org/10.5465/AMJ.2006.23478718
Suki, N. M., Lian, J. C. C., & Suki, N. M. (2013). Do patients’ perceptions exceed their expectations in private healthcare settings? International Journal of Health Care Quality Assurance. http://doi.org/10.1108/09526861111098238
Sureshchandar, G. S., Rajendran, C., & Anantharaman, R. N. (2002). The relationship between service quality and customer satisfaction – a factor specific approach. Journal of Services Marketing, 16(4), 363–379.
http://doi.org/10.1108/08876040210433248
Wang, I. ., & Shieh, C. J. (2006). The relationship between service quality and customer satisfaction: the example of CJCU library. Journal of Information and Optimization Sciences, 27(1), 193–209.\
Young, G. J., Meterko, M. M., Mohr, D., Shwartz, M., & Lin, H. (2009). Congruence in the assessment of service quality between employees and customers: A study of a public health care delivery system. Journal of Business Research, 62(11), 1127–
1135. http://doi.org/10.1016/j.jbusres.2008.08.004
Yusof, N. A. bt. (2014). Towards a seamless organization. Presented at the Persidangan
Pengurusan KKM 2014, Hotel Royale Chulan, Kuala Lumpur. Zeithaml, V. A., Parasuraman, A., & Berry, L. L. (1990). Delivering Quality Service. The Free
Press, A Division of Macmillan,Inc.
Zellmer-Bruhn, M., & Gibson, C. (2006). Multinational Organization Context: Implications for Team Learning and Performance. Academy of Management Journal, 49(3), 501–
518. http://doi.org/10.5465/AMJ.2006.21794668 Zikmund, W., Babin, B., Carr, J., & Griffin, M. (2012). Business research methods.
Cengage Learning.
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 18
Author Measurement/Model/Framework Dimensions
Ramsay et al.(2000) General Practice Assessment
Survey
(GPAS)
Access, technical care,
communication, interpersonal care,
trust, knowledge of patient, nursing
care, receptionist, continuity of care.
Grol & Wensing (2000) European Society for Quality in
Family Practice (EQuiP)
Technical care, doctor patient
relationship, information and
support, availability and
accessibility.
Baker & Whitfield
(1992)
Consultation Satisfaction
Questionnaire (CSQ)
General satisfaction, professional
care, depth of relationship, length of
consultation
Duggirala Modified SERVQUAL Infrastructure, personnel quality,
process of clinical care,
administrative procedures, safety
indicators, overall experience of
medical care received, social
responsibility
Aagja & Garg(2010) Modified GAP MODEL and Carman
1990, Rust and Olivers(1994)
called as PubHosQual
Admission, medical service, overall
service, discharge, social
responsibility
Andaleed,1998 Modified SERVQUAL Communication, cost, facility ,
competence, demeanor
Raduan et al. 2004 Modified SERVQUAL Security, performance, aesthetics,
convenience, economy, reliability.
Tomes & Ng (1995) Modified SERVQUAL Empathy, understanding of illness,
relationship of mutual respect,
dignity, food, physical environment,
religious needs.
Padma et al. 2009 Several models and factor Infrastructure, personnel quality,
process
of clinical care administrative
procedure, safety indicator,
corporate image,
trustworthiness of the hospital
Rust & Oliver(1994) modified SERVQUAL Service product, service
environment,
service delivery
Donabedian(1980) Framework structure, process
and outcome
Efficiency, effectiveness, optimality,
acceptability, legitimacy & equity.
Carman(1990) Admission, tangibles
accommodation, tangible food,
tangible privacy, nursing,
explanation visitor access,
courtesy, discharge planning, and
patient accounting perception.
Masachuttes Health
Quality
Partneship
(MHQP)
Massachusetts Health Quality
Partners
Quality of doctor (patient
interaction,
communications, integration of
care, knowledge of the patient,
health promotion), organization
features of care
(organizational access, visit
based continuity, clinical
team, staff
Table 1 Summary of healthcare dimensions for service quality from past literature
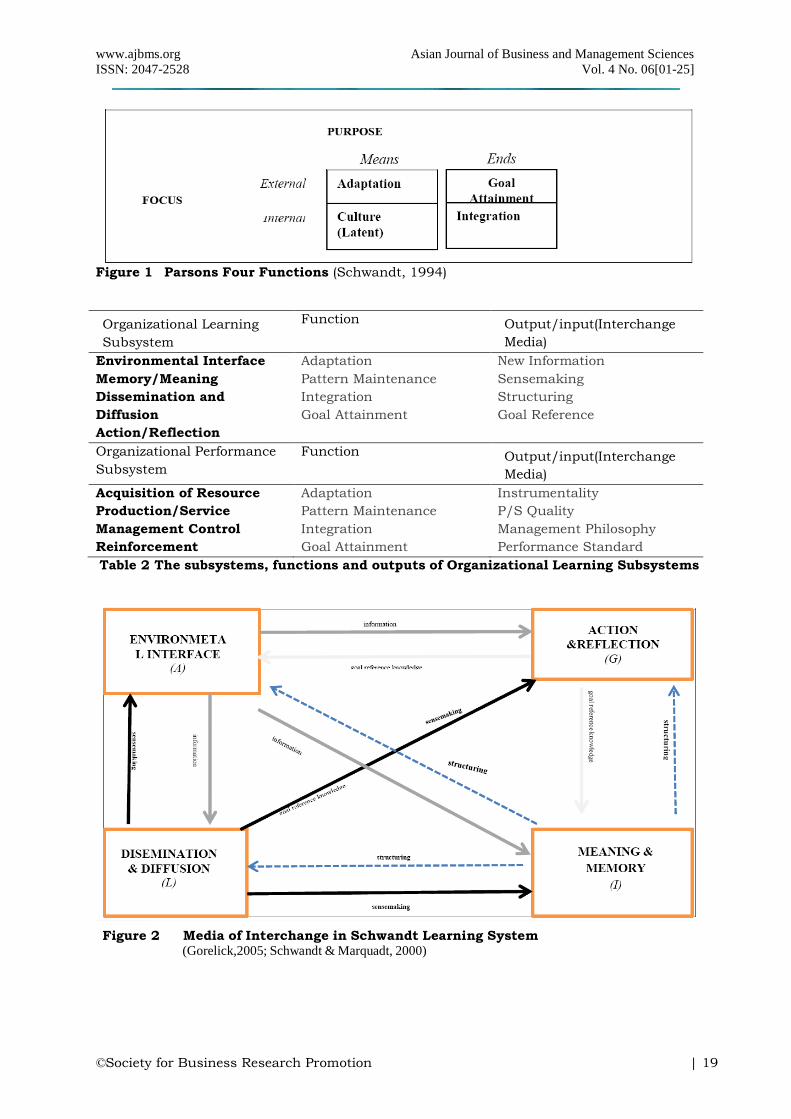
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 19
Figure 1 Parsons Four Functions (Schwandt, 1994)
Organizational Learning
Subsystem
Function Output/input(Interchange
Media)
Environmental Interface
Memory/Meaning
Dissemination and
Diffusion
Action/Reflection
Adaptation
Pattern Maintenance
Integration
Goal Attainment
New Information
Sensemaking
Structuring
Goal Reference
Organizational Performance
Subsystem
Function Output/input(Interchange
Media)
Acquisition of Resource
Production/Service
Management Control
Reinforcement
Adaptation
Pattern Maintenance
Integration
Goal Attainment
Instrumentality
P/S Quality
Management Philosophy
Performance Standard
Table 2 The subsystems, functions and outputs of Organizational Learning Subsystems
Figure 2 Media of Interchange in Schwandt Learning System (Gorelick,2005; Schwandt & Marquadt, 2000)
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 20
SERVQUAL Dimensions
(Original Dimensions)
Definition
Tangibles(tangibles) Appearance of physical facilities, equipment,
personnel, and communication materials
Reliability (reliability) Ability to perform the promised service
dependably and accurately
Responsiveness (responsiveness) Willingness to help customers and provide prompt
services
Assurance (competence,
courtesy, credibility, security)
Knowledge and courtesy of employees and their
ability to convey trust and confidence
Empathy (access, ommunication,
understanding the customer)
Caring, individualized attention the firm
provides its customers
Table 3 Correspondences between SERVQUAL dimensions with original five(5) definitions for evaluating service quality
Source: Babakus & Mangold (1992), Elluech (2008)
CLINICAL SERVICE CLINICAL SUPPORT
1. Dermatology Dietetics & Catering
2. Emergency & Trauma Imaging Diagnostics
3. General Medicine Nursing Service
4. General Medicine Occupational Therapy
5. General Surgery Pharmacy
6. Hemodialysis Physiotherapy
7. Neurology/Nephrology Psychiatry & counselling
8. Obstetrics & Gynecology
9. Oncology
10. Ophthalmology/Optometry
11. Oral Surgery (Dental)
12. Orthopedics & Traumatology
13. Otorhinolaryngology
14. Out-patient
15. Psychiatry & mental
16. Pediatric Dentistry
17. Pediatric Medicine
18. Radiology (Diagnostic Imaging)
19. Rehabilitation
20. Rheumatology
21. Specialist Clinic
22. Traditional & Complementary
Table 4 Sampled Departments
No. Measure No. Items
Source Respondent
1 Organizational Learning Action (15 items)
15 (Johnson & Bailey, n.d.-a); George Washington University; Mauchet,2011) (OL1-OL15)
Head of department
2 Service Quality (SQ) Medical Service (4 items), Overall ServiceDimension (9 items)
13 (Aagja & Garg,2010) (SQ1-SQ13)
Patients
Table 5 Constructs, Items, Sources and Respondent Type

www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 21
Environmental Interface (AdaptLrng)
OL1... do members of your organization share external information? OL2...does your organization
predict the changes occurring in the industry?
OL3...does your organization continuously track how your competitors improve their products,
services and operation?
OL4...does your organization deliberately reflect upon and evaluate external information?
Action Reflection (GoalLrng)
OL5... does your organization have set goals for researching and developing new products and/or
services?
OL6 ... do members of the organization effectively use organizational structures (e.g., chain of
command, personal networks) when sharing ideas and innovations?
OL7 ...this organization has clear goals for individual and organizational development.
Dissemination and Diffusion (IntgLrng)
OL8 ...does your organization provide opportunities for employees to develop their knowledge, skills,
and capabilities?
OL9 ...do your organization's leaders support quick and accurate communication among all
employees?
OL10 ...there are established ways to share new operational processes and procedures throughout
the organization.
OL11 ...this organization has established work groups, networks, and other collaborative
arrangements to help the organization adapt and change.
Meaning and Memory (LatentLrng)
OL12 ...does your organization use ideas and suggestions from its employees?
OL13 ...this organization believes that continuous change is necessary.
OL14 ...people in this organization believe that evaluating what customers say is critical to reaching
organizational goals.
OL15 ...this organization has a strong culture of shared values that support individual and
organizational development.
Table 6 Organizational learning items Medical service
1. … knowledgeable and experienced physicians. 2. … knowledgeable and experienced nurses. 3. … knowledgeable and experienced staff members. Overall service 4. … Materials associated with the service (such as pamphlets or statements) will be visually 5. … appealing in a hospital. 6. … visually attractive and comfortable facilities. 7. … clean washrooms, clean rooms/wards without foul smell. 8. …When patients have problems, excellent hospitals will show a sincere interest in solving it. 9. … Service providers in hospitals are dependable. 10. … give prompt service to customers.
11. … always be willing to help patients. 12. …will never be too busy to respond to patient’s request. 13. … have the patient’s best interests at heart.
Table 7 Service quality items
Minimum Maximum
Mean Std. Deviation
Skewness Kurtosis Std.
Error Std. Error
Learning Action AL 2.0
0 6.50
3.9661
.86601
.137 .164
-.194
.326 GL 2.0
0 7.00
4.0226
.92659
.098 .164
.020
.326 IL 1.5
0 6.50
4.0419
.82758
.034 .164
.218
.326 LL 1.5
0 6.25
3.9898
.87169
.071 .164
.151
.326 Overall LA 2.3
3 6.33
4.0087
.60638
.246 .164
.691
.326 *Service Quality 1.8
5 6.08
3.9749
.78735
.160 .164
.144
.326 *Score based on aggregated data from 884 cases to 221 cases
Table 8 Descriptive Statistics of Learning Action and Service Quality Scales
(N= 221)
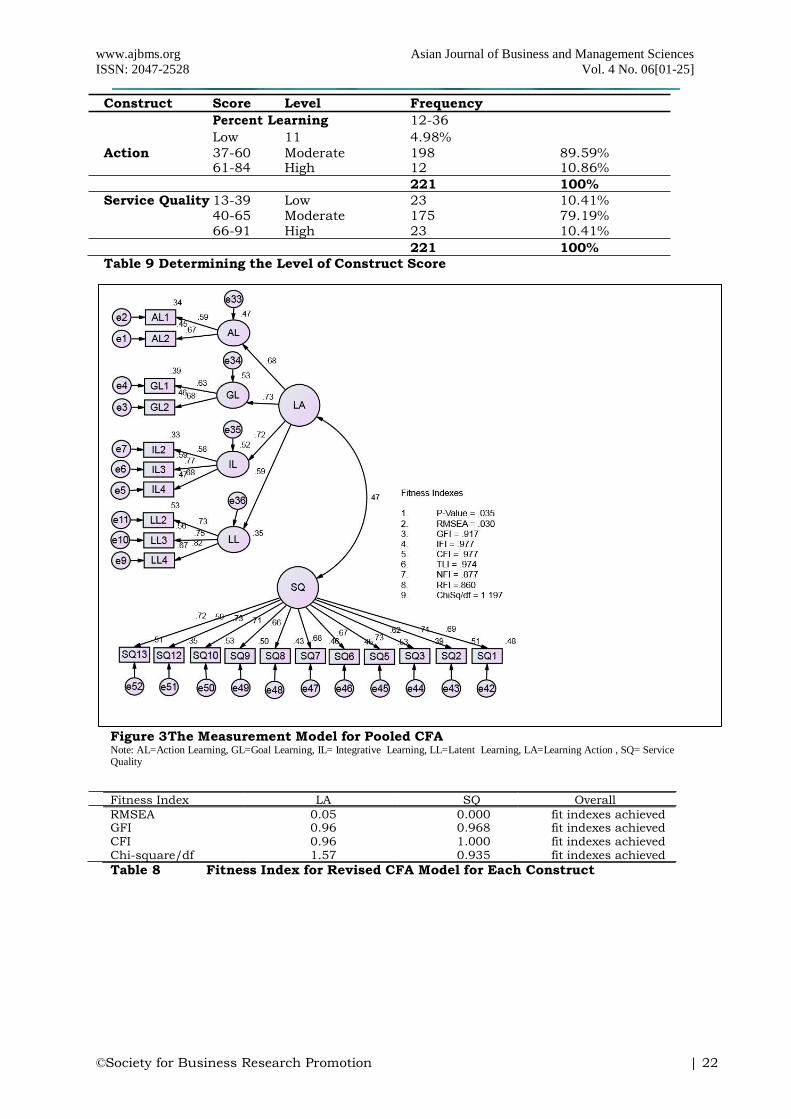
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 22
Construct Score Level Frequency
Percent Learning 12-36
Low 11 4.98%
Action 37-60 Moderate 198 89.59% 61-84 High 12 10.86%
221 100%
Service Quality 13-39 Low 23 10.41% 40-65 Moderate 175 79.19% 66-91 High 23 10.41%
221 100%
Table 9 Determining the Level of Construct Score
Figure 3The Measurement Model for Pooled CFA Note: AL=Action Learning, GL=Goal Learning, IL= Integrative Learning, LL=Latent Learning, LA=Learning Action , SQ= Service Quality
Fitness Index LA SQ Overall
Comment RMSEA 0.05
1
0.000 fit indexes achieved GFI 0.96
1
0.968 fit indexes achieved CFI 0.96
9
1.000 fit indexes achieved Chi-square/df 1.57
9
0.935 fit indexes achieved
Table 8 Fitness Index for Revised CFA Model for Each Construct

www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 23
Variable min max skew c.r. kurtosis c.r.
SQ3 2.000 6.000
.079 .477 .170 .514 SQ13 2.000 6.00
0 .009 .055 -.230 -.699
SQ12 1.000 7.000
.140 .848 -.359 -1.089 SQ10 2.000 7.00
0 .114 .694 -.067 -.202
SQ9 1.000 7.000
-.038 -.228 .376 1.140
SQ8 1.000 7.000
.105 .637 .886 2.687 SQ7 1.000 6.00
0 -.286 -1.735 .223 .676
SQ6 1.000 6.000
-.054 -.327 .145 .440 SQ5 2.000 7.00
0 .077 .467 -.065 -.198
SQ2 2.000 6.000
-.003 -.016 -.439 -1.333 SQ1 1.000 7.00
0 .120 .728 -.109 -.332
LL2 1.000 7.000
.114 .694 -.034 -.104 LL3 2.000 7.00
0 -.020 -.120 .266 .807
LL4 1.000 7.000
.005 .031 .046 .138 IL2 2.000 7.00
0 .222 1.349 .731 2.218
IL3 2.000 7.000
.196 1.187 .110 .334 IL4 1.000 7.00
0 -.127 -.771 .060 .181
GL1 2.000 7.000
.198 1.199 .300 .911 GL2 1.000 7.00
0 -.108 -.658 -.398 -
1.208 AL1 2.000 7.000
.081 .494 -.078 -.235 AL2 2.000 7.00
0 .003 .018 .176 .536
Multivariate 2.142 .512
Table 9 Assessment of Normality Distribution for Items in the Respective Constructive
SQ Factor Loading LA Factor Loading
SQ1 .696 AL2 0.674
SQ2 .711 AL1 0.581
SQ5 .735 GL2 0.677
SQ6 .674 GL1 0.629
SQ7 .668 IL4 0.685
SQ8 .651 IL3 0.763
SQ9 .705 IL2 0.58
SQ10 .730 IL1 Dropped
SQ12 .590 LL4 0.82
SQ13 .716 LL3 0.752
SQ3 .620 LL2 0.729
SQ4 Dropped LL1 Dropped
SQ11 Dropped
Note: LA=Learning Action; SQ=Service Quality
Table 10 Standardized Estimate based on Figure 3
Item Unstandardized Estimate
S.E. C.R. P Standardized Estimate
CR (≥0.6)
AVE (≥0.5)
AL .476
.081 5.844 *** .684
0.774 0.462 GL .44
4 .078 5.707 *** .72
5
IL .586
.088 6.658 *** .712
LL .51
5 .078 6.625 *** .59
6
SQ13 1.000
.716
0.938 0.733 SQ12 1.01
4 .121 8.374 *** .59
0
SQ10 1.068
.103 10.361 *** .730
SQ9 1.02
7 .103 10.018 *** .70
5
SQ8 .867
.094 9.252 *** .651
SQ7 .89
0 .094 9.484 *** .66
8
SQ6 .915
.095 9.579 *** .674
SQ5 1.06
0 .102 10.437 *** .73
5
SQ3 .805
.091 8.804 *** .620
SQ2 1.05
2 .104 10.101 *** .71
1
SQ1 1.016
.103 9.879 *** .696 Table 11 CFA Results for Measurement Model
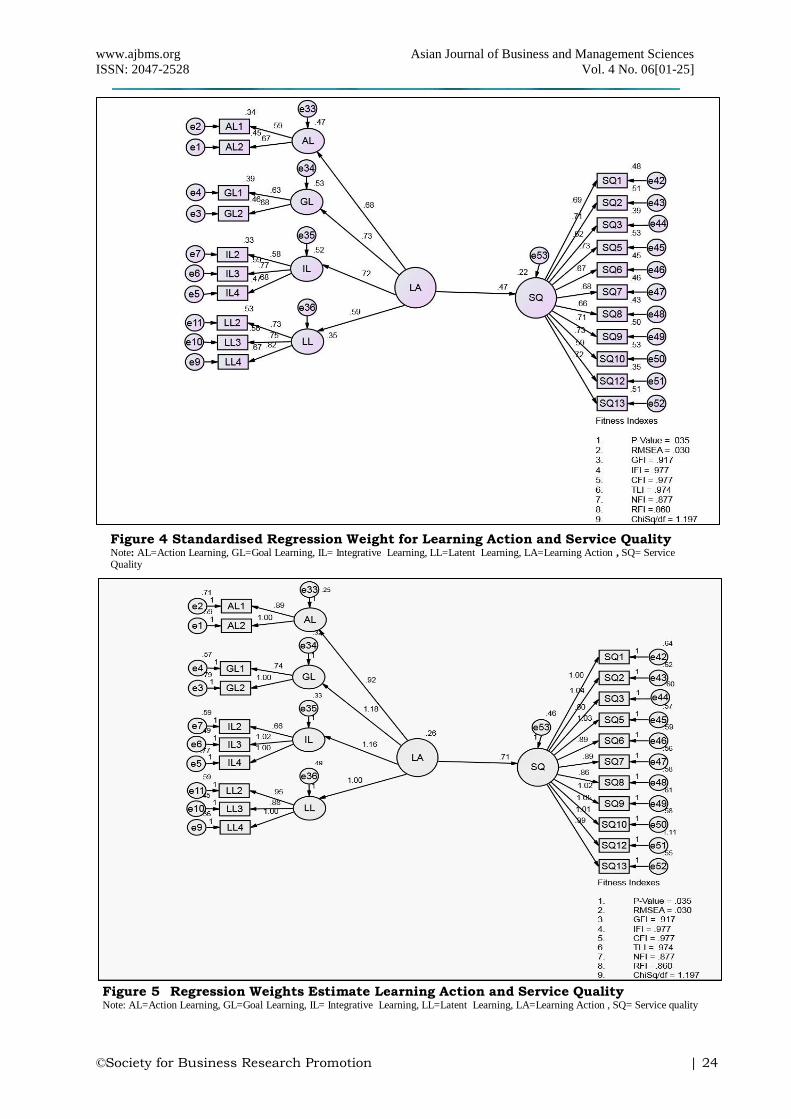
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 24
Figure 4 Standardised Regression Weight for Learning Action and Service Quality Note: AL=Action Learning, GL=Goal Learning, IL= Integrative Learning, LL=Latent Learning, LA=Learning Action , SQ= Service Quality
Figure 5 Regression Weights Estimate Learning Action and Service Quality Note: AL=Action Learning, GL=Goal Learning, IL= Integrative Learning, LL=Latent Learning, LA=Learning Action , SQ= Service quality
www.ajbms.org Asian Journal of Business and Management Sciences
ISSN: 2047-2528 Vol. 4 No. 06[01-25]
©Society for Business Research Promotion | 25
Variable Estimate (R2)
Service Quality 0.22
Name of category Name of Index Index Value Comments
Absolute value RMSEA 0.030 The required level achieved (≤ 0.08)
GFI 0.917 The required level achieved (≥0.80)
Incremental Fit CFI 0.977 The required level achieved (≥ 0.90)
Parsimonious fit Chi/square 1.197 The required level achieved (< 3.00)
Table 12 The fitness Indexes Assessment for structural model for Learning Action and Service Quality
Path Standardized Standard Critical P value Unstandardized
Deviation Ration SQ <--- LA 0.466 .169 4.164 *** .706 Note:***Sig. at 0.001
Table 13 Testing the causal effect of LA and SQ
Table 14 Squared Multiple Correlations (R2)
Hypothesis Statement of Path Analysis Estimate P-value Results on hypothesis
H1 : There is a positive relationship between Learning Action and Service Quality
0.706 *** Supported
Note:***Sig at 0.001
Table 15 Hypotheses Statemen