original article comparison of biofilm formation … · original article comparison of biofilm...
TRANSCRIPT

ORIGINAL ARTICLE
COMPARISON OF BIOFILM FORMATION ON NEW PHONAXAND PROVOX 2 VOICE PROSTHESES—A PILOT STUDY
Matthias Leonhard, MD,1 Doris Moser, MD,2 Adrian Reumueller,1 Gudrun Mancusi, MD,1
Wolfgang Bigenzahn, MD,1 Berit Schneider-Stickler, MD1
1Department of Otorhinolaryngology, Medical University of Vienna, Vienna, Austria.E-mail: [email protected] of Cranio-Maxillofacial and Oral Surgery, Medical University of Vienna, Vienna, Austria
Accepted 27 August 2009Published online 27 October 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.21276
Abstract: Background. In voice rehabilitation for laryngec-
tomized patients, voice prosthetic biofilm formation is still an
unsolved problem. Design and materials of voice prostheses
have been altered by manufacturers to improve function and
extend the lifetime of devices. The goal of the study was to
investigate biofilm formation on Provox 2 and Phonax, recently
introduced voice prostheses made of thermoplastic
polyurethane.
Methods. Five laryngectomized patients were equipped
with both Phonax and Provox 2 voice prostheses. Microbial
colonization was analyzed using standard microbiological
methods. Biofilm formation and material infiltration were illus-
trated using scanning electron microscopy, fluorescence mi-
croscopy, and thin-section light microscopy.
Results. Although no differences in quality or quantity of
microbial colonization were assessed, microscopic imaging
revealed differences in material surfaces, biofilm composition,
and infiltration morphologies; the polyurethane material seems
to destabilize biofilm architecture by inhibition of hypheal Can-
dida growth forms.
Conclusions. Polyurethane material for voice prostheses
seems to reduce biofilm stability and infiltrative processes.VVC 2009 Wiley Periodicals, Inc. Head Neck 32: 886–895, 2010
Keywords: biofilm adhesion; Candida albicans; polyurethane;
silicone; voice prostheses
In laryngectomized patients, voice prostheticbiofilm formation is a well-studied but stillunsolved problem. Microbial deposits on thevalve lead not only to aspiration of nutritionalcomponents and saliva but also to luminalobstruction with speaking difficulties. In thiscase, replacement of the malfunctioning prosthe-ses is necessary, but usually has to be performedby a physician. Thus, the short lifetime of thedevice causes discomfort for the patient.
Various attempts have been made to extenddevice lifetime and to improve material resist-ance of voice prostheses to yeasts and bacteria:surface treatments with active agents, altera-tion of surface properties by laser, and admix-ture of silver oxide into the silicone material.1–6
Various valve designs, such as the hinged valveflap (Provox 1, Provox 2, Provox Activalve), theslit valve type (Groningen Button), the tripod-ball valve type (Voicemaster), and even valvelessdesign (Nijdam) have been used in prosthesisconstruction. However, the vulnerability of thevalve mechanism to biofilm colonization still
Correspondence to: M. Leonhard
VVC 2009 Wiley Periodicals, Inc.
886 Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010
remains unsolved. Recently, the Phonax voiceprosthesis by Heimomed (Kerpen, Germany)was introduced and licensed for voice rehabilita-tion of laryngectomized patients. The hingedvalve flap design of Phonax bears resemblanceto that of Provox 2 (Atos Medical, Horby, Swe-den). However, Phonax is manufactured of ther-moplastic polyurethane (TPU), a polymermaterial considered to be more resistant to fun-gal colonization, whereas Provox 2 is made ofmedical-grade silicone.7–9 Provox 2 is the mostcommonly used prosthesis in voice rehabilitationof laryngectomized patients in Europe; recentmulticenter studies revealed a median lifetimeof 92 to 135 days.10–13
Surface biofilm formation evolves in phases.In the beginning, microorganisms from the tra-chea and the upper airway loosely adhere to thepolymer surface of the voice prosthesis. Thenthe microbes multiply and form a continuousgrowing biofilm layer. Local nutritional and oxy-gen gradients within the biofilm provide livingconditions for more sophisticated microbial spe-cies and bring forward the growth of complexsymbiotic microecosystems.14 This microbialcommunity encases itself in a protective extrac-ellular polysaccharide matrix (EPS), whichreduces the impact of environmental fluctua-tions in moisture, pH value, and drug therapyon the microbial population.15 Mature biofilmsconsist of multiple cell layers that can partlydetach and disseminate onto new surfaces.16
Candida species are most often isolated fromvoice prostheses. They possess specific skills tocolonize and to cause deterioration of medical-grade silicone.17,18 The tight bonding of biofilmdeposits to surfaces of voice prostheses with-stands even daily cleaning procedures (manual
brushing) by the patient. The growth of biofilmdeposits is accompanied with initial deteriora-tion of the smooth polymer surface and consecu-tive infiltration. Biofilm-resistant elastomers,such as TPU in Phonax, might play a key rolein exceeding device lifetimes of voice prostheses.More data on the process of material disintegra-tion itself are still needed to establish compara-ble criteria for evaluation of polymer biofilmresistance.
The goal of this study was the examinationof biofilm formation on Phonax and Provox 2voice prostheses using standard microbiologicaland imaging techniques (scanning electron mi-croscopy, fluorescence microscopy, and thin-sec-tion light microscopy).
MATERIALS AND METHODS
Overview of Phonax and Provox 2 Voice Prosthe-
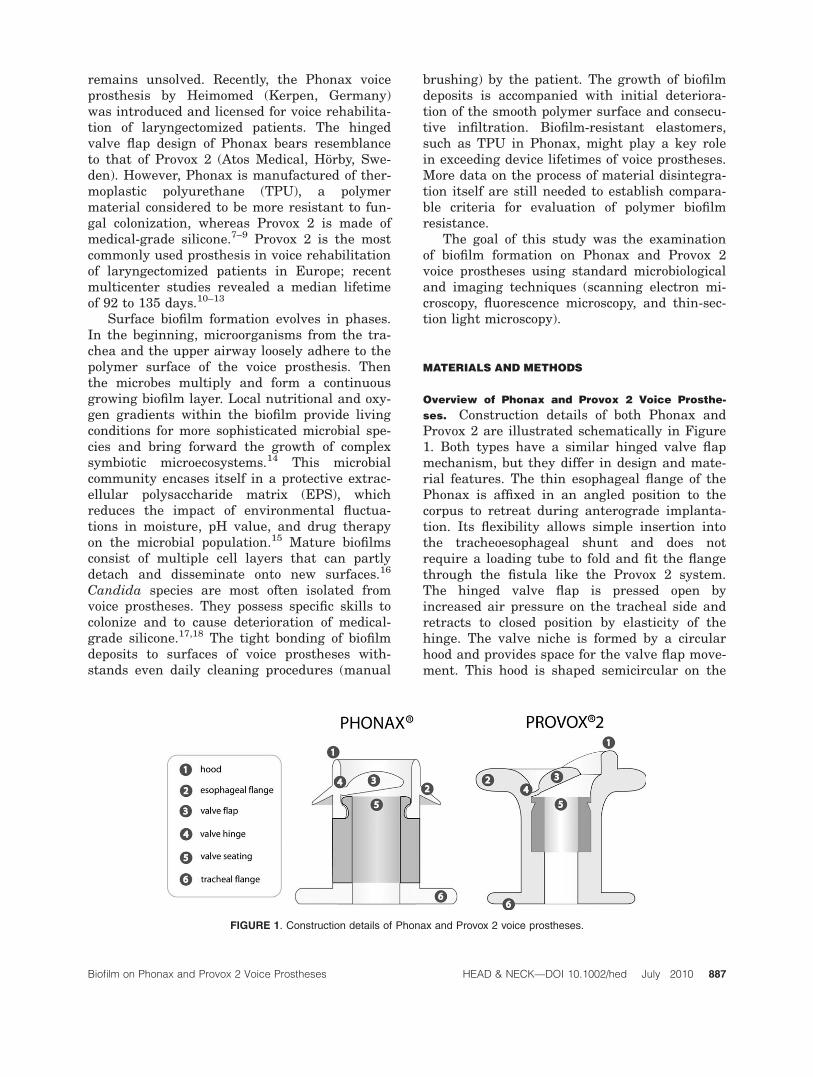
ses. Construction details of both Phonax andProvox 2 are illustrated schematically in Figure1. Both types have a similar hinged valve flapmechanism, but they differ in design and mate-rial features. The thin esophageal flange of thePhonax is affixed in an angled position to thecorpus to retreat during anterograde implanta-tion. Its flexibility allows simple insertion intothe tracheoesophageal shunt and does notrequire a loading tube to fold and fit the flangethrough the fistula like the Provox 2 system.The hinged valve flap is pressed open byincreased air pressure on the tracheal side andretracts to closed position by elasticity of thehinge. The valve niche is formed by a circularhood and provides space for the valve flap move-ment. This hood is shaped semicircular on the
FIGURE 1. Construction details of Phonax and Provox 2 voice prostheses.
Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010 887

Provox 2 and is localized on the opposite side ofthe hinge. The main difference is the prosthesismaterial: whereas the medical grade silicone ofProvox 2 appears smooth and transparent, Pho-nax is made of TPU with increased opacity andsurface roughness. Original surface structuresof unused voice prostheses of each type shouldbe assessed by examination with scanning elec-tron microscopy complying with identical prepa-ration methods.
Patients. In our department, the Provox 2 hasbeen the favored prosthesis type in the past dec-ade. In cases with difficult local situation of thetracheoesophageal fistula or discomfort with Pro-vox 2, patients are offered other prosthesis typesas an individual solution. With its introduction,Phonax was offered to the patients as an alterna-tive replacement. To collect comparable data ondevice lifetimes, 5 laryngectomized patients(mean age, 63.2 � 3.7 years; Table 1), who hadbeen using Provox 2 on average 5 years andagreed to be equipped with the Phonax, wereincluded in the study. Patients 2 and 3 were al-ready using other voice prostheses prior to Pro-vox 2. The patients were selected with respect toconsideration of regular previous replacementintervals (mean, 114 days over the past 5 years)and stable microbial spectra. All patientsreported good verbal communication skills afterprosthesis implantation. Prosthesis cleaning wasperformed by manual brushing at least once aday. Patients visited our office because of pros-thetic leakage and aspiration. For this study,Provox 2 prostheses were replaced by Phonax ofthe same size (either 6 or 8 mm). On follow-up,they were again replaced by Provox 2. Both pros-thesis types were collected and processed by thefollowing methods.
Qualitative and Quantitative Analysis of Microbial
Colonization. The withdrawn prostheses werecut in half under sterile conditions. One half
Table 1. Patient characteristics.
Patient Sex Age
Years since
laryngectomy
Neck
dissection
Postsurgical
RT
1 Male 64 4 Bilateral þ2 Male 67 6 None þ3 Female 57 7 Bilateral þ4 Male 64 5 Bilateral þ5 Male 64 5 Bilateral þAbbreviation: RT, radiation therapy.
Table
2.Microbialspectrum
andbiofilm
localizationonPhonaxandProvox2voiceprostheses.
Patient
Prosthesis
model
Insitu
time,
days
cfu/m
L
�106
Microbiologicalanalysis
Biofilm
type
Imagingtechniques(biofilm
localization)
C.albicans
C.krusei
C.glabrata
E.coli
S.aureus
S.oralis
S.parasanguinis
Multiple
colonies
Biofilm
cover
Esophageal
flange
Trachial
flange
Valve
flap
Hinge
Valve
seating
Intraluminal
stain
Infiltration
1Phonax
147
3.0
þþ
þþ
þþ
þþ
þþ
þProvox2
168
3.0
þþ
þþ
þþ
þþ
þþ
þþ
2Phonax
126
1.0
þþ
þþ
þþ
Provox2
105
1.0
þþ
þþ
þþ
þ3
Phonax
49
4.8
þþ
þþ
þþ
þþ
þþ
Provox2
60
3.4
þþ
þþ
þþ
þþ
þþ
4Phonax
11
3.8
þþ
þþ
þþ
þþ
þþ
þþ
Provox2
14
3.6
þþ
þþ
þþ
þþ
5Phonax
56
2.8
þþ
þþ
þþ
þþ
þþ
þþ
þProvox2
56
2.3
þþ
þþ
þþ
þþ
Rn¼
10
x¼
96
44
76
47
310
39
87
46
888 Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010
was vortexed in 10 mL of phosphate-buffered so-lution (PBS) for 30 seconds. Dilution series ofthe rinsing fluids were plated out onto trypticsoy agar (TSA) for quantitative analysis and onselective growth agars (Sabouraud agar, McCon-key agar, Columbia 5% agar, Columbia colistin-nalidixic acid agar (Columbia CNA), S. aureusID agar (SAID), Trimethoprim agar (TMP),Cetrimide agar, CHROMagar Candida) for qual-itative analysis. After incubation for 24 or 48hours, respectively, the grown colonies werecounted and identified according to the diagnos-tic protocol of each agar. Inaccurate results wereprocessed further using the Vitek 2 system (Bio-Merieux Inc., Durham, NC). The vortexed pros-thesis half was then prepared for examinationwith fluorescence or light microscopy.
Imaging Techniques for Capturing Biofilm Formation
and Material Alterations
Scanning Electron Micrography. The second prosthesishalf was retained in a solution of 2.5% glutaral-dehyde and 4% paraformaldehyde in cacodylatebuffer (pH 7.0) for 24 hours, dehydrated in a se-
ries of ethanol concentrations (70%, 80%, 96%,and 100%, 1 hour each), and stored dry in anexsiccator with silicagel. The surface was sput-tered with gold (Sputter Coater: SC502, Polaron,Fisons Instruments, Surface Science Division,Cambridge, UK), and examined by scanningelectron microscopy (JSM 6310, JEOL Ltd., To-kyo, Japan).
Fluorescence Microscopy. Fluorescence microscopywas used to visualize biofilm deposits. The fluo-rescent properties of organic material wereenhanced by sample preparation in 2% glutaral-dehyde for 24 hours. Examination under ultra-violet light increased the contrast betweenbiofilm structures and the nonfluorescent poly-mer materials, showing both superficiallyadhered deposits and material invasions.
Thin-section Light Microscopy. One Phonax prosthesisand 1 Provox 2 prosthesis with comparable bio-film adhesions were embedded in Technovit7200 VLC (Heraeus-Kulzer, Hanau, Germany)and prepared as thin sections for light
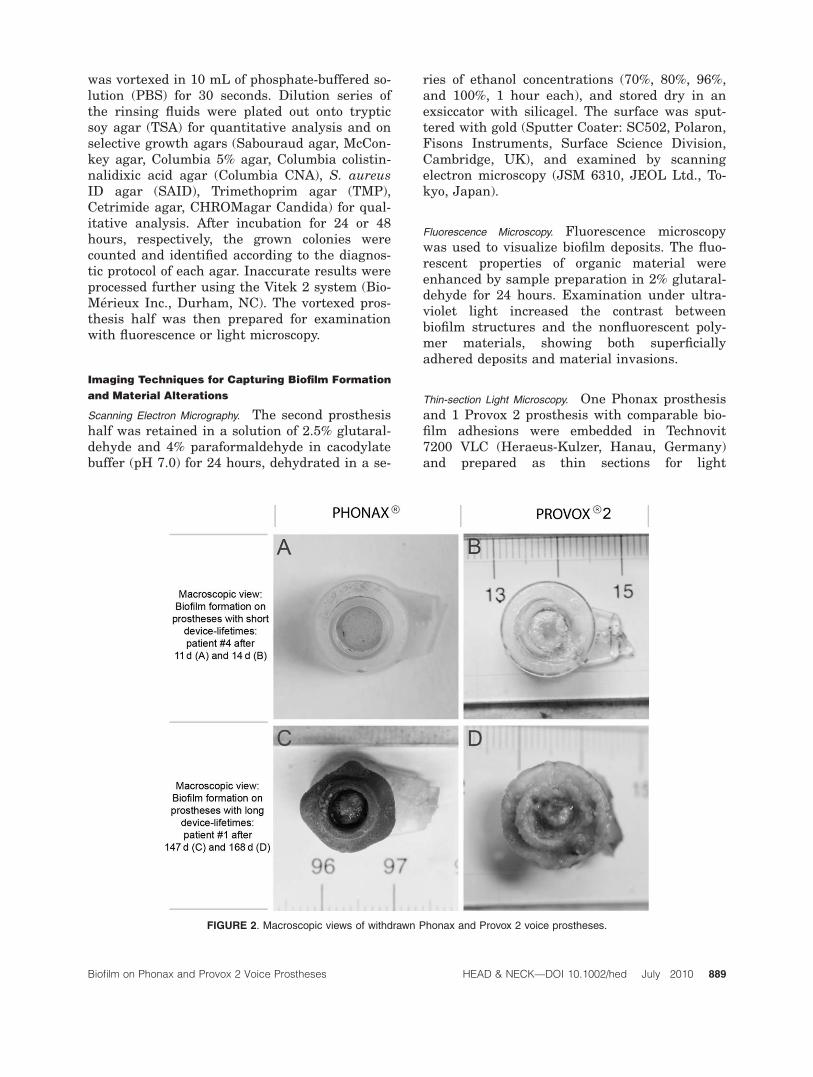
FIGURE 2. Macroscopic views of withdrawn Phonax and Provox 2 voice prostheses.
Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010 889

microscopy (Nikon Eclipse E800, Nikon ImagingInc., Tokyo, Japan). Thionin staining (1% thio-nin acetate solution [Sigma–Aldrich, St. Louis,MO], 45 minutes) was used to highlight organicmaterial.
RESULTS
Qualitative and Quantitative Analysis of Microbial
Colonization. Microbiological results and coloni-zation patterns for all prostheses examined areshown in Table 2. Microbial concentration of therinsing solutions averaged 2.9 � 106 colonyforming units per milliliter (cfu/mL). Phonaxprostheses showed a slightly elevated mean mi-crobial concentration of 3.1 � 106 cfu/mL and amean device lifetime of 77.8 days, shorter thanthat of Provox 2 (2.7 � 106 cfu/mL, 80.6 days).Candida species were identified on all prosthe-ses (n ¼ 10), with Candida albicans being themost frequent subspecies (n ¼ 9). Most often iso-lated bacteria were Staphylococcus aureus (n ¼7) and Streptococcus oralis (n ¼ 6). No affinityof specific microbial species to any of the 2 poly-mer materials was observed.
Macroscopic View on Microbial Colonization. Ma-croscopic comparison of the prostheses indicatedmore biofilm masses and mucus secrete adhe-
sion to the surface of Phonax. The esophagealsurfaces of both prosthesis types—in particularthe esophageal flange, the valve flap, and thevalve seating—were predominantly affected bybiofilm infestation. Colonization patterns rangedfrom single scattered biofilm deposits toextended covers of the esophageal valve. Thincontinuous biofilm covers were observed moreoften on Phonax prostheses, whereas bulged sol-itary deposits were encountered more often onProvox 2 (Figures 2A–2D). Removal of biofilmdeposits by careful scratching was not possiblewithout damaging the polymer surface.
Microscopic Examination of Native Polymer Surfa-
ces. Surfaces of the unused voice prostheses,examined by scanning electron microscopy, areshown in Figure 3. The TPU surface of Phonaxis characterized by asperities, whereas themedical-grade silicone of Provox 2 appearssmooth, with minor elongated embossments.Remnants of the manufacturing process, suchas irregular polymer flashes on the outer diam-eters of the flanges, were found on both pros-thesis types.
Microscopic Examination of Biofilm Formation
Scanning Electron Microscopy. All prostheses wereexamined by scanning electron microscopy. An
FIGURE 3. Native surfaces of unused Phonax and Provox 2 voice prostheses. Polyurethane shows an uneven surface structure with
asperities, whereas silicone appears smooth with marginal embossments. A remnant from manufacturing process (injection die mold-
ing) is visible on the top outer diameter of the esophageal flange of Phonax (A, marked by arrow).
890 Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010
overview of colonization patterns on the esopha-geal surfaces of both prosthesis types is pre-sented in Figure 4. The roughened TPUmaterial of Phonax is covered by an evenly con-tinuous layer of EPS matrix, apparently con-
touring the material surface beneath.Transitions between material and biofilm surfa-ces appear seamless. The flanges of the prosthe-ses shown in Figures 4A, 4G, and 4I wereclipped to assess multiple material samples with
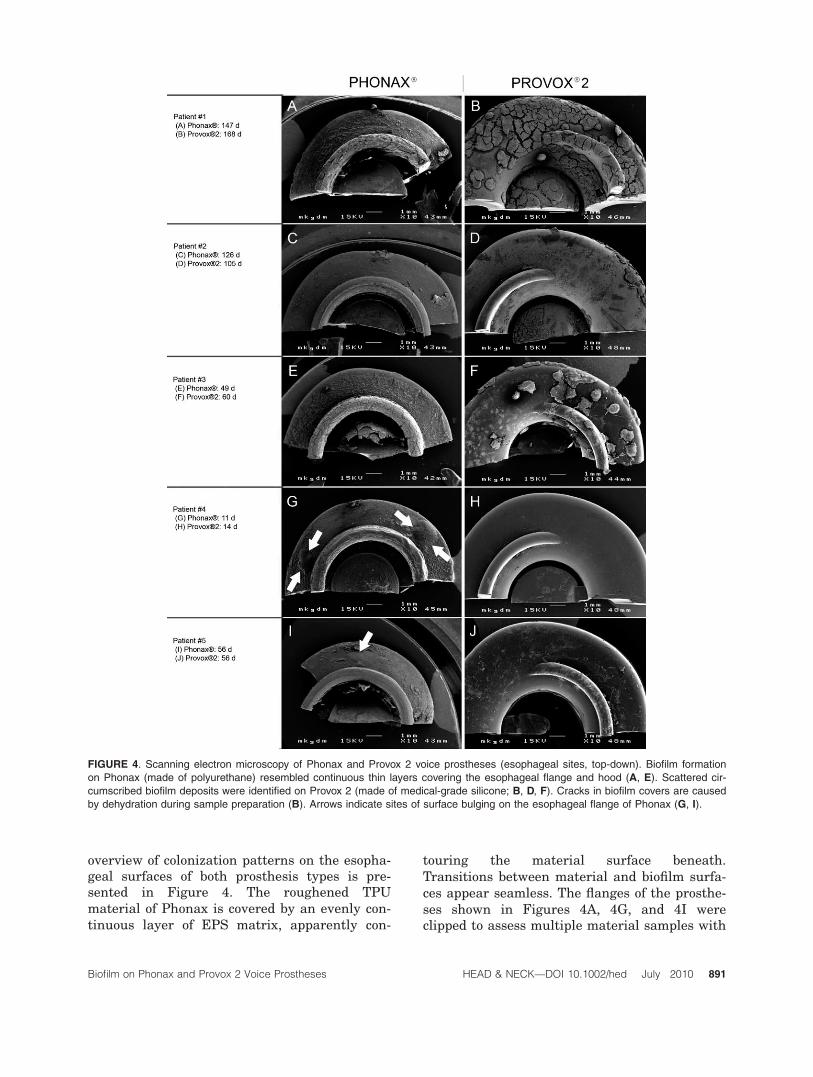
FIGURE 4. Scanning electron microscopy of Phonax and Provox 2 voice prostheses (esophageal sites, top-down). Biofilm formation
on Phonax (made of polyurethane) resembled continuous thin layers covering the esophageal flange and hood (A, E). Scattered cir-
cumscribed biofilm deposits were identified on Provox 2 (made of medical-grade silicone; B, D, F). Cracks in biofilm covers are caused
by dehydration during sample preparation (B). Arrows indicate sites of surface bulging on the esophageal flange of Phonax (G, I).
Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010 891

sagittal-section planes to screen for materialinfiltration. Material flashes located on the dis-tal perimeters of the flanges are visible rem-nants from manufacture by injection diemolding (Figure 3A, marked by arrow, and Fig-ures 4A, 4C, and 4G). The esophageal surfacesof Provox 2 showed insular biofilm depositsadhering to the smooth prosthesis material (Fig-ures 4B and 4F). Their circumscribed characterallows a clear distinction between biofilm andsilicone. Cracks in the biofilm surface arecaused by sample dehydration, which is anessential step for scanning electron microscopy(Figure 4B). Detailed imaging of the adhereddeposits revealed differences in biofilm composi-tion on the polymer surfaces (see Figure 5).Deposits on Provox 2 consisted of typical biofilmstructures with bacteria and both budded andfilamentous growth forms of Candida species.Fungal hyphae appeared interwoven with EPSmatrix and bacterial aggregations forming com-plex 3-dimensional structures (Figure 5B). Bio-film on the surface of Phonax was characterizedby a 2-dimensional layer of crowded microbesattached to the polymer material (Figure 5A).Cell boundaries submerged in an amorphousmass of EPS. No signs of stabilizing filamentousgrowth were detected.
All withdrawn prostheses were microscopicallyscreened for biofilm infiltration. On 6 prostheses(3 Phonax, 3 Provox 2) with minimum in vivoperiods of 56 days (Phonax) and 60 days (Provox2), respectively, biofilm ingrowth was detected.
Surface deteriorations appeared as minormaterial defects located close to the polymer
surface. They were mainly found in proximity toor underneath adhering biofilm deposits. OnPhonax, dense microbial colonies advanced fromthe surface into material fissures (Figure 6A).On Provox 2, the smooth material surface waslocally disrupted by ingrowing colonies. Excava-tions appeared filled with microbial content thatanchored larger biofilm deposits adhering to theprosthesis surface. Infiltrations of greater depthresembled voluminous ‘‘baglike’’ microbialdeposits inside the silicone (Figure 6B).
Fluorescence Microscopy. Fluorescence microscopyproved to be a fast and simple method to con-trast between polymer material and organicmatter. No hypheal infiltration, but sharp-edgedtransitions between ingrowing spherical depos-its and the prosthesis materials were visible.The TPU material was less infiltrated in depththan the medical-grade silicone, which showedvoluminous ‘‘baglike’’ deposits with expandinggrowth character inside the valve flaps (Figures6C and 6D). These infiltrations seemed to locallydeform the valve flap of Provox 2.
Thin-section Light Microscopy. Ingrowing fungalhyphae were identified in thin-section light mi-croscopy. They were located underneath superfi-cially adhering biofilm deposits. Solitary violet-stained hyphae penetrated ‘‘rootlike’’ into thesilicone material of the Provox 2. Hypheal inva-sion was also found on Phonax, although to a
FIGURE 5. Scanning electron microscopy of biofilm deposits on Phonax and Provox 2. Biofilm deposits on Phonax show the absence
of germ tubes and appear as plane microbial crowds submerged in EPS matrix. Mature mixed biofilm, showing 3-dimensional netting
of fungal filaments, budded growth, EPS matrix, and bacterial conglomerates, was detected on Provox 2. EPS, extracellular polymeric
substance.
892 Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010
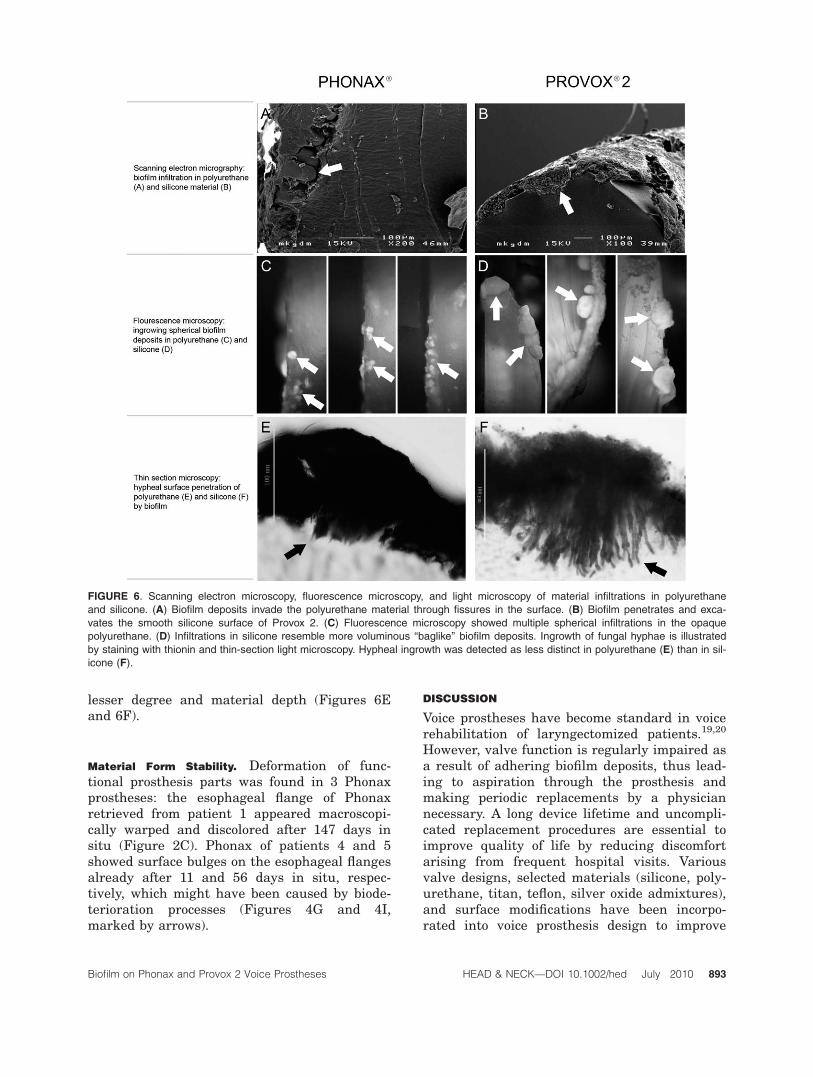
lesser degree and material depth (Figures 6Eand 6F).
Material Form Stability. Deformation of func-tional prosthesis parts was found in 3 Phonaxprostheses: the esophageal flange of Phonaxretrieved from patient 1 appeared macroscopi-cally warped and discolored after 147 days insitu (Figure 2C). Phonax of patients 4 and 5showed surface bulges on the esophageal flangesalready after 11 and 56 days in situ, respec-tively, which might have been caused by biode-terioration processes (Figures 4G and 4I,marked by arrows).
DISCUSSION
Voice prostheses have become standard in voicerehabilitation of laryngectomized patients.19,20
However, valve function is regularly impaired asa result of adhering biofilm deposits, thus lead-ing to aspiration through the prosthesis andmaking periodic replacements by a physiciannecessary. A long device lifetime and uncompli-cated replacement procedures are essential toimprove quality of life by reducing discomfortarising from frequent hospital visits. Variousvalve designs, selected materials (silicone, poly-urethane, titan, teflon, silver oxide admixtures),and surface modifications have been incorpo-rated into voice prosthesis design to improve
FIGURE 6. Scanning electron microscopy, fluorescence microscopy, and light microscopy of material infiltrations in polyurethane
and silicone. (A) Biofilm deposits invade the polyurethane material through fissures in the surface. (B) Biofilm penetrates and exca-
vates the smooth silicone surface of Provox 2. (C) Fluorescence microscopy showed multiple spherical infiltrations in the opaque
polyurethane. (D) Infiltrations in silicone resemble more voluminous ‘‘baglike’’ biofilm deposits. Ingrowth of fungal hyphae is illustrated
by staining with thionin and thin-section light microscopy. Hypheal ingrowth was detected as less distinct in polyurethane (E) than in sil-
icone (F).
Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010 893

function and device lifetime. Phonax (Hei-momed) is a voice prosthesis manufactured ofTPU. This thermoplastic elastomer is reportedto be more resistant to biofilm infestation.21 Thepresent pilot study investigated in vivo biofilmformation on Phonax and Provox 2 in 5 laryng-ectomized patients, with special emphasis on re-ciprocal effects between biofilm and thedifferent polymer materials.
In this study, prostheses remained in situuntil leakage was reported by the patients. Allprostheses were examined not only with stand-ard microbiological methods, but also with mi-croscopic imaging techniques after withdrawal.Microbiological findings are consistent withrecent data and confirm Candida species andbacteria originating from the oropharyngealspace as the main biofilm-forming colonizers ofthe esophageal valve surfaces. The microbiologi-cal spectrum and quantity proved to be similarboth on Phonax and on Provox 2, which indi-cates no specific microbial affinities toward TPUor medical grade silicone. However, scanningelectron microscopy of the unused prosthesesrevealed an increased surface roughness of TPUmaterial, which seemed to facilitate initial mi-crobial in vivo adhesion. This might explain thecontinuous thin microbial coating of the esopha-geal surfaces of the Phonax, whereas the smoothsilicone surface of Provox 2 restrains initial bio-film formation to corners and niches of the valvering and the valve flap. Upon withdrawal, thePhonax prosthesis was coated with more looselyattached mucus of low viscosity. Provox 2showed less mucus, but solid and circumscribedbiofilm deposits continuously spreading in diam-eter and increasing number according to in vivotime. These macroscopically visible differencesin biofilm configuration might be ascribed toalterations in biofilm architecture, as illustratedin the results of scanning electron microscopy:the plane biofilm structure on TPU is character-ized by an amorphous EPS matrix and the ab-sence of germ tubes. The hypheal growth formof Candida species seems to enhance biofilmstability by complex cellular netting inside theEPS matrix and was found constantly in bio-films on Provox 2 prostheses. A similar impactof surface-modified polyurethane material onCandida biofilms has also been reported byChandra et al22 in an in vitro assay.
Various explanations on how biofilm is ableto cause deterioration of polymer material havebeen discussed, but the exact processes involved
remain unclear. A combination of lytic processesand extraction of soluble material compounds bymicrobial agents may lead to focal embrittle-ment and structural damage of the polymers.23
These areas and fissures might be subject to fur-ther active microbial attack in the form ofhypheal advance or expansive growing microbialdeposits. To fully illustrate morphologies of ma-terial damages, examination by scanning elec-tron microscopy was completed by fluorescencemicroscopy and light microscopy. The revealedmorphologies comply with forms of microbialintrusion into silicone that were described andclassified earlier by Neu et al24 on GroningenButtons and by van Weissenbruch et al25 onProvox 1. On Provox 2, biofilm infiltrationoccurred mainly on the esophageal surface ofthe valve flap. Infiltrations resembled multiplebaglike deposits excavating and expanding intothe silicone. Voluminous and compact depositsanchored the superficial biofilm layer, explain-ing its tight bonding to the prosthesis. The TPUof Phonax showed ingrown microbial deposits ofcomparably smaller dimension and depth, whichindicates improved material resistance to biofilminfiltration. This resistance might also be associ-ated with the described absence of hyphealgrowth forms on TPU. As illustrated in Figure6F, a direct infiltration of germ tubes into thesilicone material of Provox 2 was found,whereas no similar equivalent was detected inTPU. The deformation of the esophageal flangeof Phonax in patient 1 after 147 days in situ(Figure 2C) might be attributable to less formstability of the TPU material. Another explana-tion is a passive adaption of the flange to sur-rounding mucosal structures of the fistula. Thebulges located on the flanges (Figures 4G and4I, marked by arrows) could be caused by localmoisture expansion of the deteriorated polymermaterial or may be the image of a circumscribedlifting of the biofilm layer. Further investigationon long-term material stability of Phonax underbiofilm exposure is required to evaluate theobserved material alterations.
The impact of the found differences betweenbiofilm formation on Phonax and Provox 2 onclinical practice was not investigated in thisstudy, although device lifetimes and microbialloads were revealed to be similar for both pros-theses types tested. The use of multiple exami-nation methods restricted the number ofprostheses included in the study. However, thefindings might contribute to interpretation of
894 Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010

future results of clinical trials of Phonax onlarger scales.
CONCLUSIONS
In summary, the Phonax voice prosthesis showsqualitative and quantitative microbial coloniza-tion similar to that of Provox 2. The TPU sur-face structure seems to facilitate biofilmadherence, but the material also seems to in-hibit filamentous growth of Candida species.Compared with biofilms on Provox 2, this mightlead to less-stable biofilm configuration, lesshypheal infiltration, and smaller subsurface bio-film deposits. The presented results with Pho-nax indicate that TPU reduces the vulnerabilityof voice prostheses to biofilm damage, althoughthe impact on clinical practice and on in vivo de-vice lifetimes still needs to be verified on alarger scale. Further in vitro and in vivo investi-gation on biofilm formation, composition, andstability on TPU are required.
Acknowledgments. The authors gratefullyacknowledge the support by C. Schofer on theexpertise on fluorescence microscopy. The studywas supported by Heimomed (Kerpen, Ger-many) for providing the Phonax voiceprostheses.
REFERENCES
1. Everaert EP, van de Belt-Gritter B, van der Mei HC,et al. In vitro and in vivo microbial adhesion and growthon argon plasma-treated silicone rubber voice prosthe-ses. J Mater Sci Mater Med 1998;9:147–157.
2. Ameye D, Honraet K, Loose D, Vermeersch H, Nelis H,Remon JP. Effect of a buccal bioadhesive nystatin tableton the lifetime of a Provox silicone tracheoesophagealvoice prosthesis. Acta Otolaryngol 2005;125:304–306.
3. Rodrigues L, van der Mei H, Banat IM, Teixeira J, Oli-veira R. Inhibition of microbial adhesion to silicone rub-ber treated with biosurfactant from Streptococcusthermophilus A. FEMS Immunol Med Microbiol 2006;46:107–112.
4. Everaert EP, Mahieu HF, van de Belt-Gritter B, et al.Biofilm formation in vivo on perfluoro-alkylsiloxane-modified voice prostheses. Arch Otolaryngol Head NeckSurg 1999;125:1329–1332.
5. Dijk FWM, Busscher HJ, van Luyn MJ, van der MeiHC. In vitro formation of oropharyngeal biofilms on sili-cone rubber treated with a palladium/tin salt mixture.J Biomed Mater Res 2000;51:408–412.
6. Kress P. Klinische Anwendung einer Stimmprothese mitsilberoxidhaltigem Ventil (Blom-Singer Advantage): bio-
filmresistenz, prothesenverweildauer und indikation.Laryngo-Rhino-Otol 2006:893–896.
7. Cannon RD, Chaffin WL. Oral colonization by Candidaalbicans. Crit Rev Oral Biol Med 1999;10:359–383.
8. Tang RY, Gonzalez JB, Roberts GD. Polyurethane elas-tomer as a possible resilient material for denture prothe-ses: a microbiological evaluation. J Dent Res 1975;54:1039–1045.
9. Hawser SP, Douglas LJ. Biofilm formation by Candidaspecies on the surface of catheter materials in vitro.Infect Immun 1994;62:915–921.
10. Op de Coul BMR, Hilgers FJM, Balm AJM, Tan IB, vanden Hoogen FJA, van Tinteren H. A decade of postlar-yngectomy vocal rehabilitation in 318 patients: a singleinstitution’s experience with consistent application ofProvox indwelling voice prostheses. Arch OtolaryngolHead Neck Surg 2000;126:1320–1328.
11. Ackerstaff AH, Hilgers FJM, Meeuwis CA, et al. Multi-institutional assessment of the Provox 2 voice prosthesis.Arch Otolaryngol Head Neck Surg 1999;125:167–173.
12. Schafer P, Klutzke N, Schwerdtfeger FP. Voice restora-tion with voice prosthesis after total laryngectomy.Assessment of survival time of 378 Provox-1, Provox-2and Blom-Singer voice prosthesis. Laryngorhinootologie2001;80:677–681.
13. Graville D, Gross N, Andersen P, Everts E, Cohen J.The long-term indwelling tracheoesophageal prosthesisfor alaryngeal voice rehabilitation. Arch OtolaryngolHead Neck Surg 1999;125:288–292.
14. Watnick P, Kolter R. Biofilm, city of microbes. J Bacter-iol 2000;182:2675–2679.
15. Flemming HC, Neu TR, Wozniak DJ. The EPS matrix:the ‘‘house of biofilm cells.’’ J Bacteriol 2007;189:7945–7947.
16. Beule AG, Hosemann W. Bacterial biofilms. Laryngorhi-nootologie 2007;86:886–898.
17. Ramage G, Saville SP, Thomas DP, Lopez-Ribot JL.Candida biofilms: an update. Eukaryot Cell 2005;4:633–638.
18. Ramage GMJ, Lopez-Ribot JL. Candida biofilms onimplanted biomaterials: a clinically significant problem.FEMS Yeast Res 2006;6:979–986.
19. Bien S, Rinaldo A, Silver CE, et al. History of voice reha-bilitation following laryngectomy. Laryngoscope 2008;118:453–458.
20. Gerwin JM, Culton GL. Quality of life in prostheticvoice users. Otolaryngol Head Neck Surg 2005;133:685–688.
21. Traissac LCG, Devars F, Houliat T, Essalki I, Bekhar H,Rousseau A. Voice rehabilitation after total laryngec-tomy using the Newvox voice prosthesis. Rev LaryngolOtol Rhinol (Bord) 2007;128:163–172.
22. Chandra J, Patel JD, Li J, et al. Modification of surfaceproperties of biomaterials influences the ability of Can-dida albicans to form biofilms. Appl Environ Microbiol2005;71:8795–8801.
23. Flemming H. Relevance of biofilms for the biodeteriora-tion of surfaces of polymeric materials. Polym DegradStab 1997;59:309–315.
24. Neu TR, Van der Mei HC, Busscher HJ, Dijk F, VerkerkeGJ. Biodeterioration of medical-grade silicone rubberused for voice prostheses: a SEM study. Biomaterials1993;14:459–464.
25. van Weissenbruch R, Albers FW, Bouckaert S, et al.Deterioration of the Provox silicone tracheoesophagealvoice prosthesis: microbial aspects and structuralchanges. Acta Otolaryngol 1997 May;117:452–458.
Biofilm on Phonax and Provox 2 Voice Prostheses HEAD & NECK—DOI 10.1002/hed July 2010 895