ors sanooz
TRANSCRIPT
What is Diarrhea ?
Types of serious diarrhoea in childrenAcute watery diarrhea- If <14 days ,sever
dehydration Ecoli,cholera ,malnutrition
Persistent diarrhea-If >14 days, 20-30 % death, under nourished and HIV exposed
Dysentery-(atisar) with blood ,with or without mucus 10%-15 % of deaths
Why are children more prone to diarrhoeaProportion of water is more in children ,so
dehydration occur early.Metabolic rate is high and use more water as
compared to adultsKidney can conserve less water ,so loss is
more Sodium loss can be 70-110 m mol/kgChloride and potassium loss is balanced
&same
Assessment of diarrheaDid child vomit? Did child pass urine? What type of liquids did the child get ?Did the child get sufficient food before this
episode ?During diarrhea is child getting food that is
different and is less calorie dense? Look for cough ,fever ,otitis
media ,sepsis ,h/o measles Weight /nutrition
ASSESS:
Degree of Dehydration
DECIDE:
Plan of treatment
Does the child have diarrhea?
If yes, ask:For how long? How many? Has the child been vomiting Is there blood in stool?
LOOK AT THE CHILD’S GENERAL CONDITIONIS THE CHILD◦ Lethargic or Unconscious?◦ Restless or Irritable?
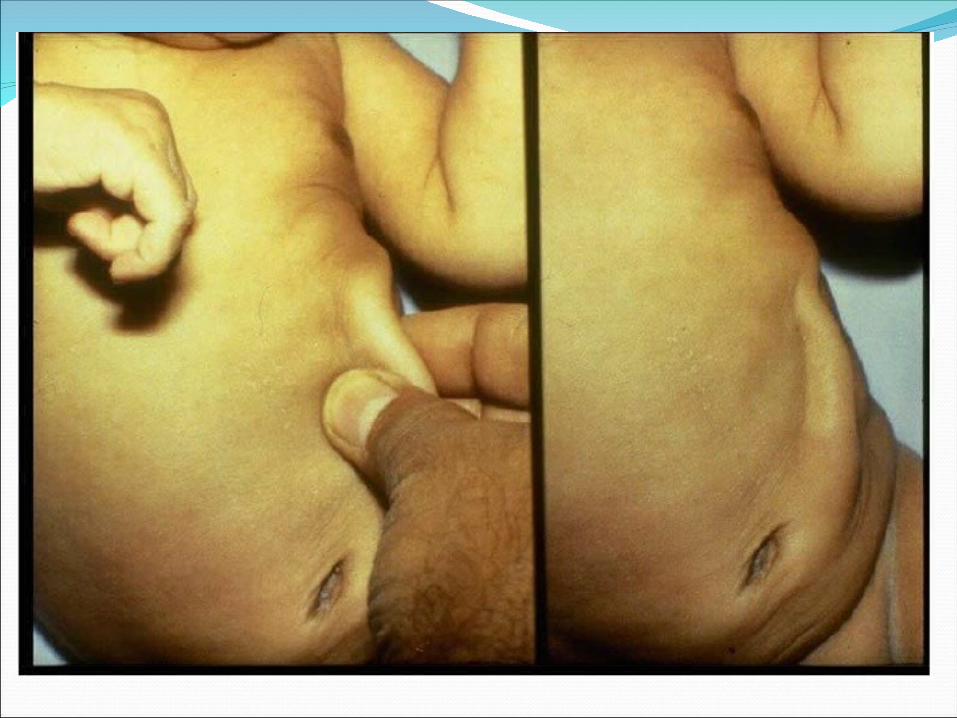
LOOK FOR SUNKEN EYES Look for skin pinch -goes back
promptly/slowly/ very slowly OFFER THE CHILD FLUID TO DRINK –THIRSTY Not able to drink or drinking poorly?
Drinking eagerly, appears thirsty?
Drinking normally?
LOOK
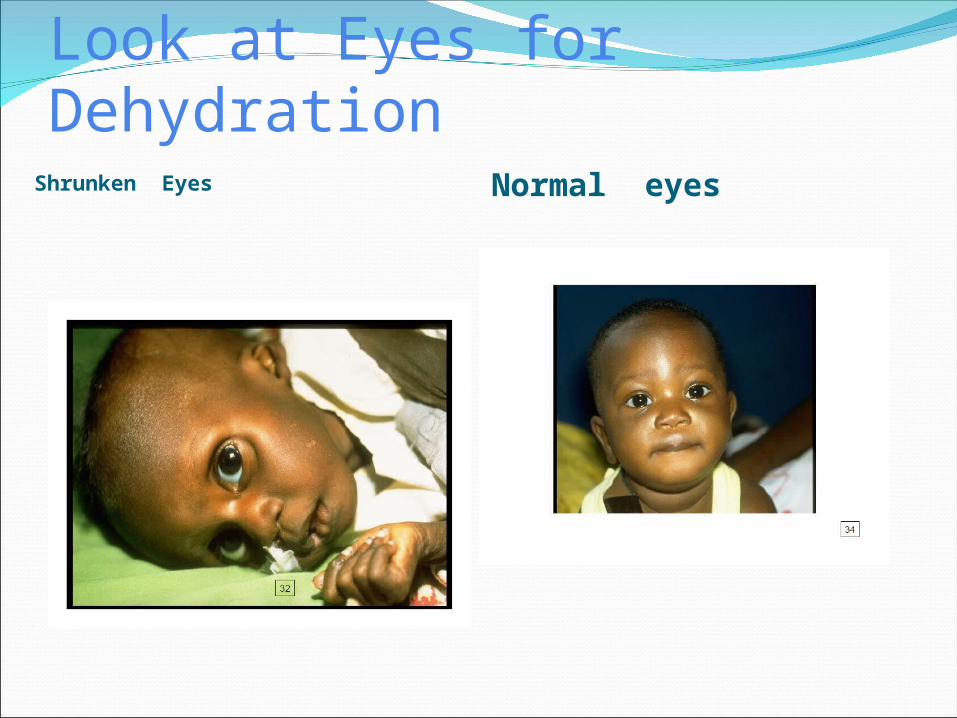
Look at Eyes for Dehydration Shrunken Eyes Normal eyes

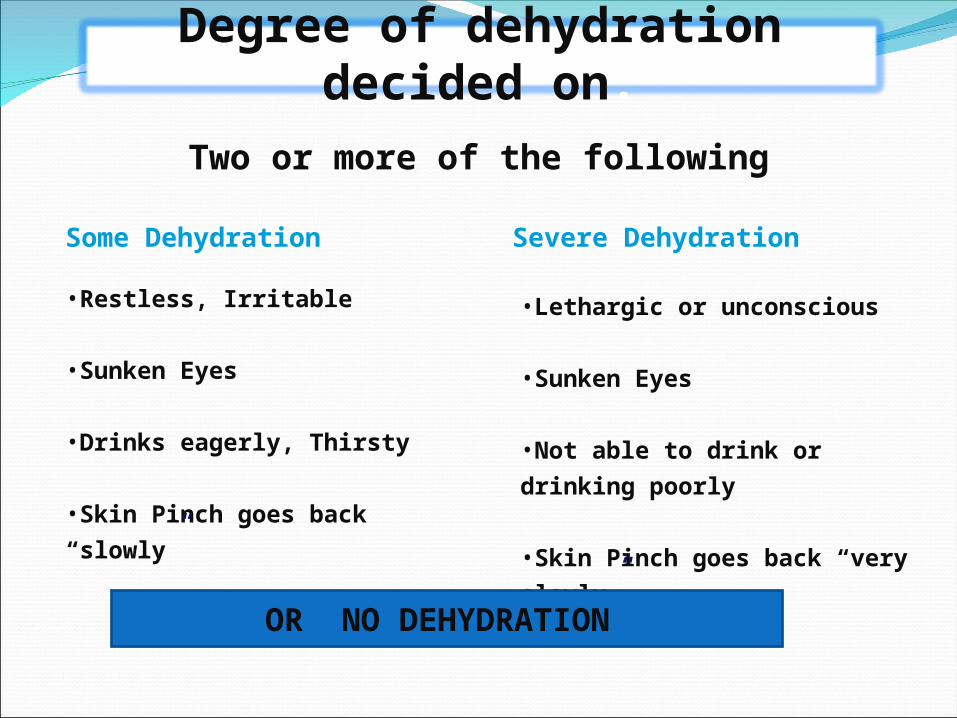
Two or more of the following
Degree of dehydration decided on:
•Restless, Irritable
•Sunken Eyes
•Drinks eagerly, Thirsty
•Skin Pinch goes back “slowly”
Some Dehydration Severe Dehydration
•Lethargic or unconscious
•Sunken Eyes
•Not able to drink or drinking poorly
•Skin Pinch goes back “very slowly”
OR NO DEHYDRATION
No Dehydration: PLAN-A
Some Dehydration: PLAN-B
Severe Dehydration: PLAN-C
Treat Diarrhea at Home.
4 Rules of Home Treatment:
GIVE EXTRA FLUID
CONTINUE FEEDING
WHEN TO RETURN [ADVICE TO
MOTHER]
GIVE ORAL ZINC FOR 14 DAYS
PLAN – A
Plan-B is carried out at ORT Corner in
OPD/clinic/ PHC
Treat ‘some’ dehydration with ORS (50-100
ml/kg
If the child wants more, give more
After 4 hours:
Re-assess and classify degree of dehydration.
PLAN – B
PLAN -CSigns of sever dehydration Child not improving after 4 hours
Refer to higher center –give ORS on way /keep warm /BF
When child comes back follow up as other children
Start I. V. Fluid immediately
PLAN – C
Dysentery
Cholera
Severe malnutrition
Associated systemic infection
Antimicrobials should be given during diarrhea only for:
Increase amount of calories during convalescence with
energy dense foods (enrich foods with fats and sugar)
•Feed an extra meal (for at least 2 weeks after diarrhea
stops)
•Give an extra amount
•Use extra rich foods
•Feed with extra patience
•Give extra breastfeeds as often as child wants
Increase amount of calories during convalescence with
energy dense foods (enrich foods with fats and sugar)
•Feed an extra meal (for at least 2 weeks after diarrhea
stops)
•Give an extra amount
•Use extra rich foods
•Feed with extra patience
•Give extra breastfeeds as often as child wants
What Is ORS
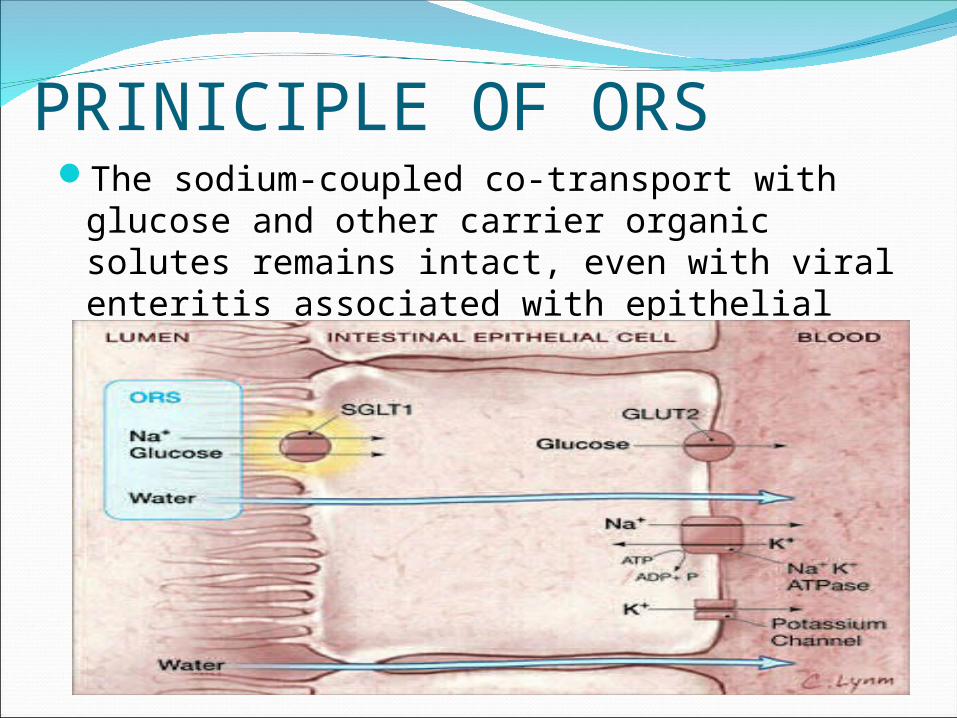
PRINICIPLE OF ORSThe sodium-coupled co-transport with
glucose and other carrier organic solutes remains intact, even with viral enteritis associated with epithelial damage .
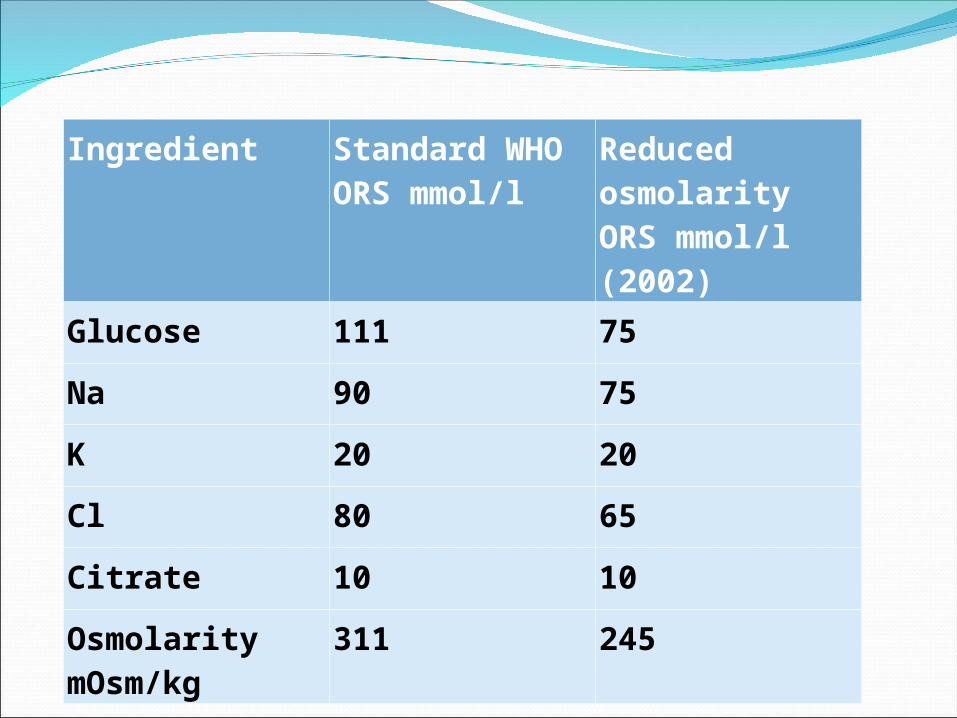
Ingredient Standard WHO ORS mmol/l
Reduced osmolarity ORS mmol/l (2002)
Glucose 111 75
Na 90 75
K 20 20
Cl 80 65
Citrate 10 10
Osmolarity mOsm/kg
311 245
Limitation of high osmolarity ORS
Does not lower volume, frequency and duration of diarrhoea.
Induces vomiting due to taste, so acceptability poor.
More chances of dehydration, more chances of requiring iv fluid.
Hypernatremia.Good to correct fluid deficit, not good for
maintenance fluid.
LOW OSMOLARITY ORSCompared to WHO standard ORS , hypo-
osmolar ORS is associated with
a) fewer unscheduled intravenous fluid infusions(33%)
b)lower stool volumes (20%), and
c) less vomiting(30%)
Clinical relevance - low osmolarity ORSReduction in need of IV therapy results in
reduced hospitalization and in turn results:
Reduced risk of hospital acquired infections.
Reduced disruption of breastfeeding. Reduced use of needles and interventions Reduced therapy cost. Reduced risk of diarrheal deaths in areas
where IV therapy is not readily available.
Rice-based ORS, Maltodextrin-containing and Amino acid-containing ORS—SUPER ORS
They are not superior to glucose-based ORS for acute non-cholera diarrhea, provided that feeding was promptly resumed after initial rehydration of the child.
Flavored/Colored ORS Studies showed neither an advantage nor
disadvantage for the flavoured and coloured ORS when compared to the standard ORS with regard to safety, acceptability and correct use.
Concerns about the type of sweetners ,coloring and flavouring agents used.
More expensive
Limitations for ORS
Altered mental status with concern for aspiration
Abdominal ileusUnderlying disorder that limits intestinal
absorption of ORT (e.g, short gut, carbohydrate malabsorption)
PRACTICAL PROBLEMSVomiting: Give less amount more
frequently,wait for 10 minutes and try again.Give food in the form of Kanji,Amylase rich food.
Taste: It is a MEDICINE and the most important medicine in diarrhea. Convince the parents. First drug in your prescription.
If affording, flavoured ORS may help.
ORS IV fluids Once ORT has been initiated, intervention
with intravenous hydration is indicated:
If stool output continues to be excessive, and ORT is unable to adequately rehydrate the child
If there is severe and persistent vomiting, and inadequate intake of ORS
WHO Statement2006: The World Health Organization states
that, “there is no evidence to support the ongoing use of IV therapy for the first-line management of most cases of childhood gastroenteritis.”
Safe & effectiveCan alone successfully rehydrate 95-97% patients with diarrhea,
Reduces hospital case fatality rates by 40 - 50%
Cost savingReduces hospital admission rates by 50% and cost of treatment by 90%
39% reduction in need for unscheduled IV fluids
19% reduction in stool output
29% reduction in vomiting
Hahn et al, 2001; WHO/FCH/CAH 0.1.22, 2001
Should be given to young infants (< 2m) including neonates
if there is dehydration
In exclusively breastfed young infants with no dehydration
encourage exclusive breastfeeding more frequently and for
longer
Low osmolarity ORS is safe and effective for all ages
Advice to parentsStoringHow to give Measuring Home remedies
WHY ZINC?
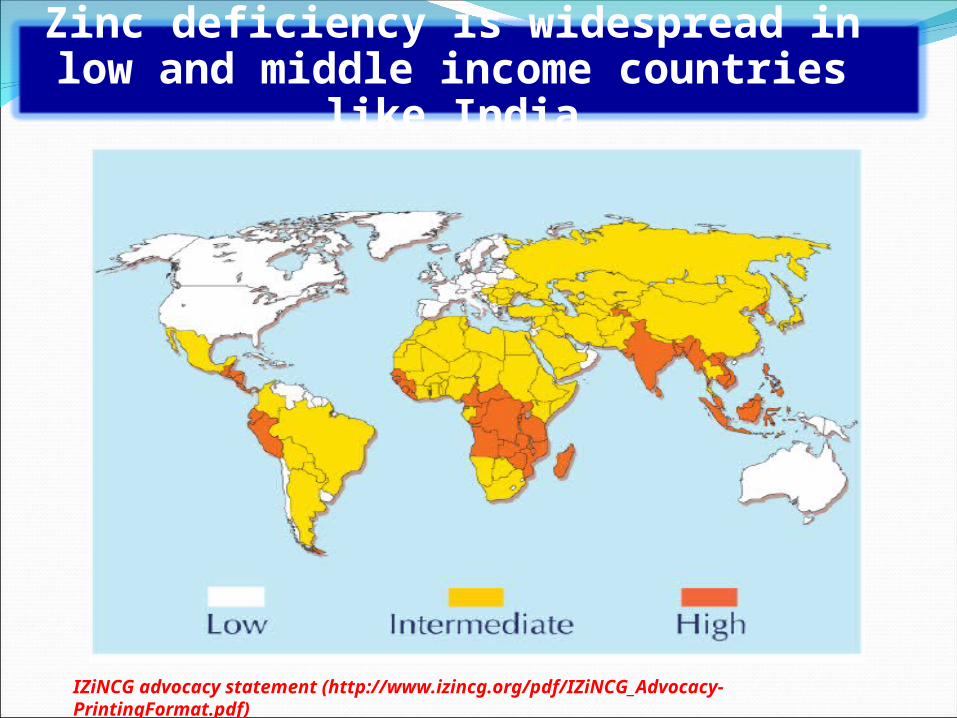
IZiNCG advocacy statement (http://www.izincg.org/pdf/IZiNCG_Advocacy-PrintingFormat.pdf)
Zinc deficiency is widespread in low and middle income countries like India
Disrupts intestinal mucosa
Reduces brush border enzymes
Increases mucosal permeability
Increases intestinal secretion
Roy 1992, Hoque 2005
Zinc deficiency has direct effects on mucosal functions
20 mg/day (10 mg/day for infants 2-6 mo) of zinc supplementation for 14 days starting as early as possible after onset of diarrhea
WHO/UNICEF Joint statement (2001), IAP 2003, GOI 2007
Recommendations for Use of Zinc in Acute Diarrhea
Preventing and Treating Diarrhea
THANK YOU