os acromiale rupture associated with a massive rotator cuff tear causing deltoid insufficiency and...
TRANSCRIPT
Os Acromiale Rupture Associated with a Massive Rotator Cuff Tear Causing Deltoid Insufficiency and Superior
Escape of the Humeral Head
by Gregory J. Pinkowsky, and April D. Armstrong
JBJS Case ConnectVolume 4(1):e17
February 12, 2014
©2014 by The Journal of Bone and Joint Surgery, Inc.

Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.

Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
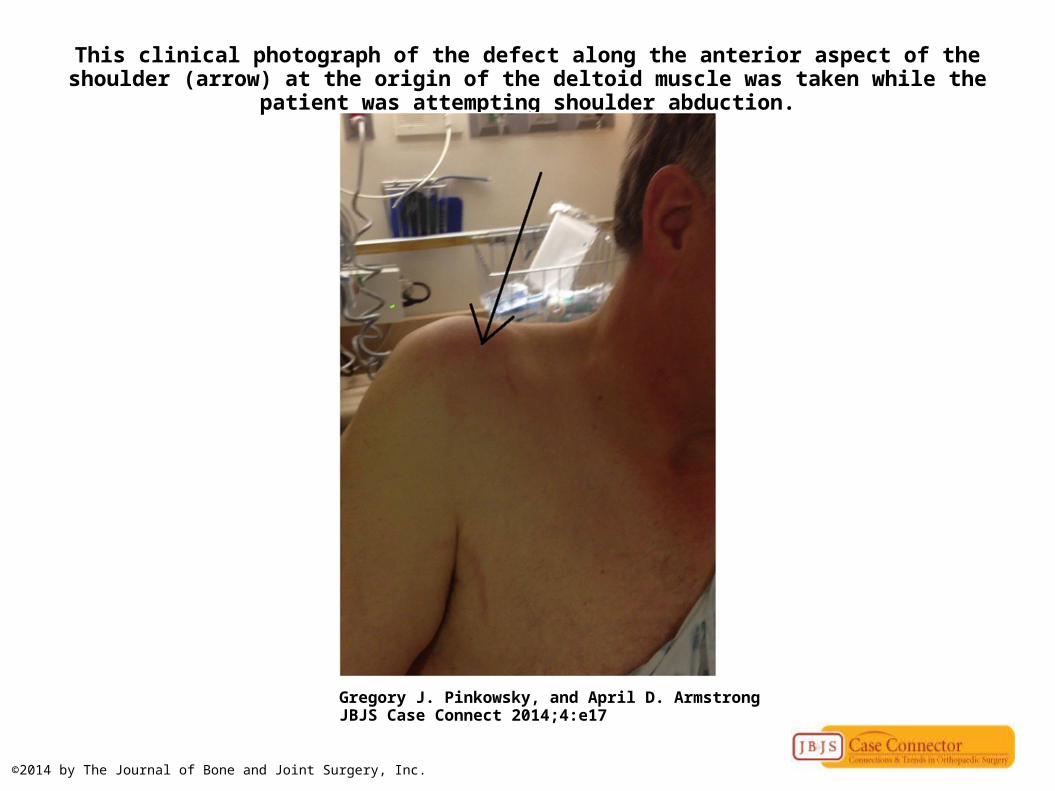
This clinical photograph of the defect along the anterior aspect of the shoulder (arrow) at the origin of the deltoid muscle was taken while the patient was attempting shoulder abduction.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.

Coronal T2-weighted fat-suppressed MRI (left) indicates a full-thickness rotator cuff tear with substantial retraction; a large effusion is present.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
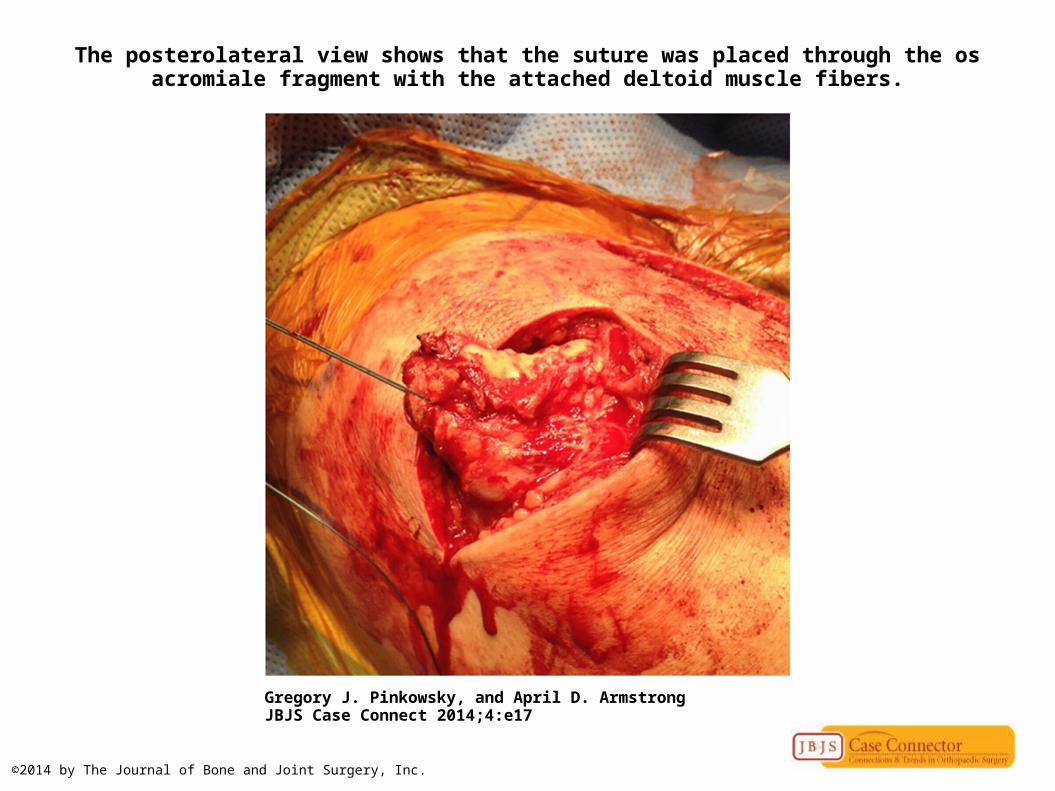
The posterolateral view shows that the suture was placed through the os acromiale fragment with the attached deltoid muscle fibers.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
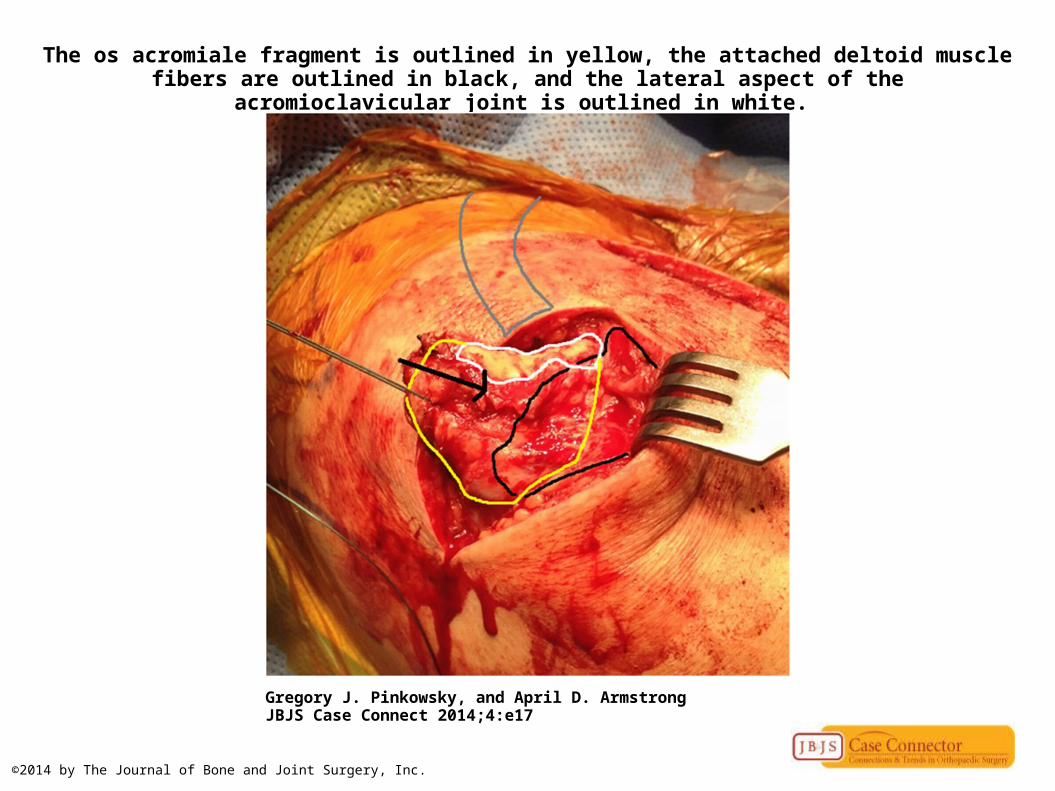
The os acromiale fragment is outlined in yellow, the attached deltoid muscle fibers are outlined in black, and the lateral aspect of the acromioclavicular joint is outlined in white.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
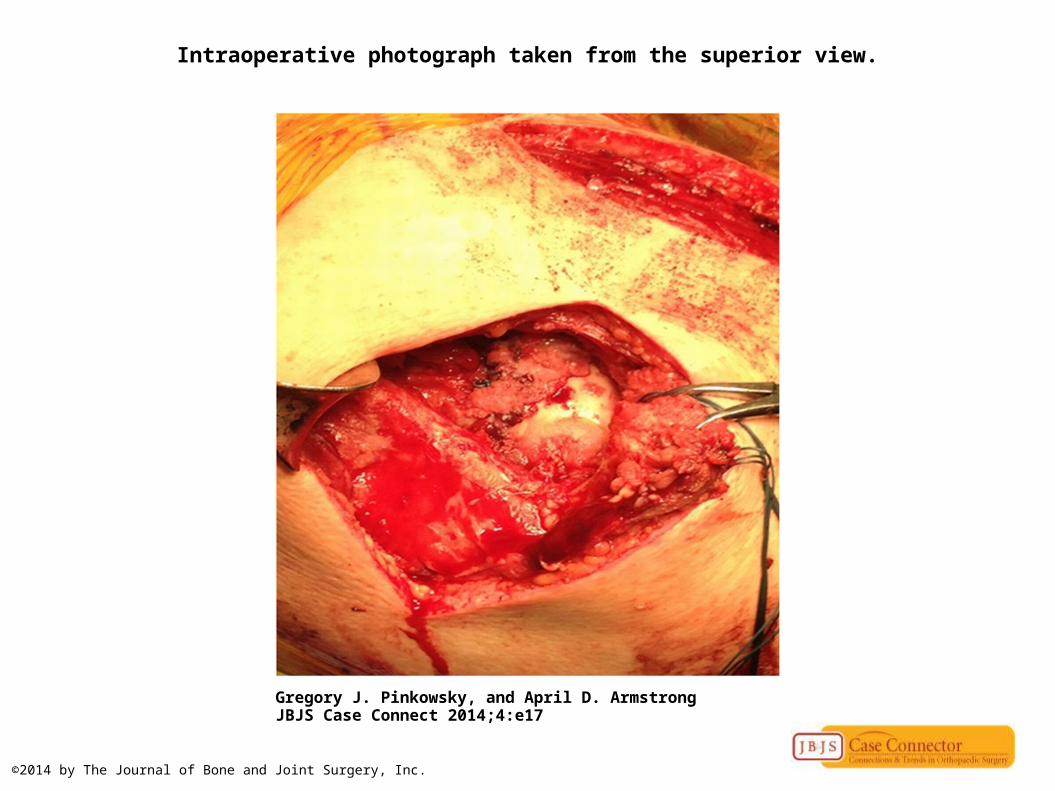
Intraoperative photograph taken from the superior view.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
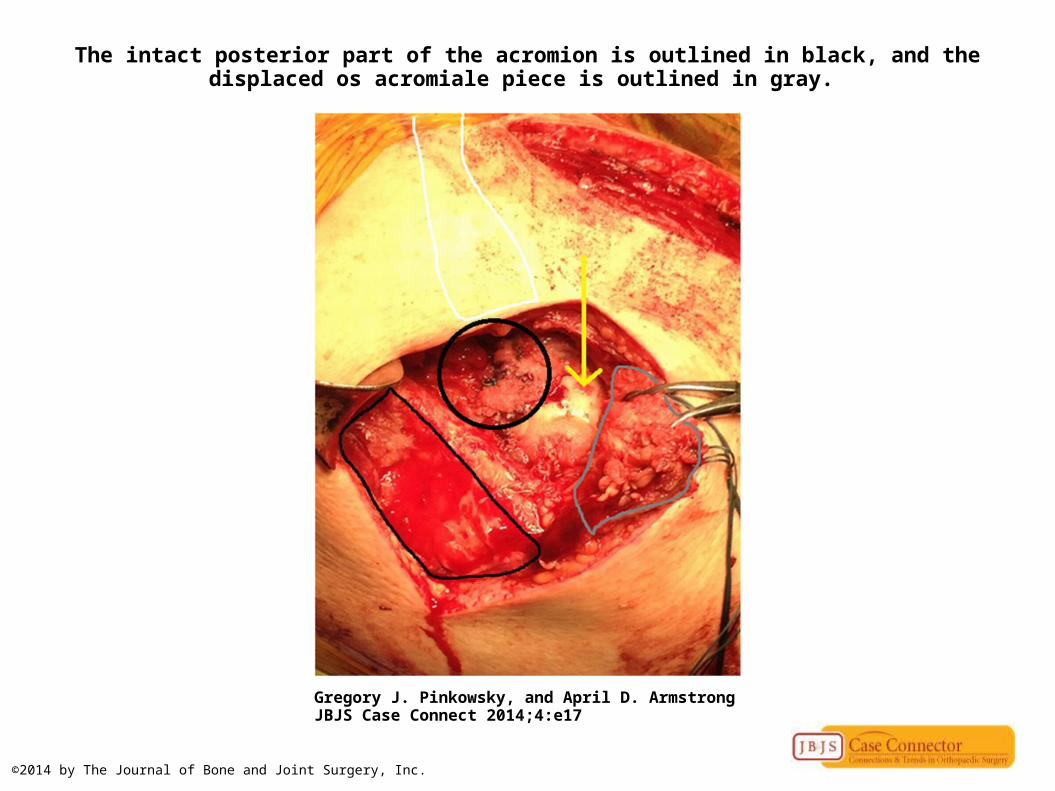
The intact posterior part of the acromion is outlined in black, and the displaced os acromiale piece is outlined in gray.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.

Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.

Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.

Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.
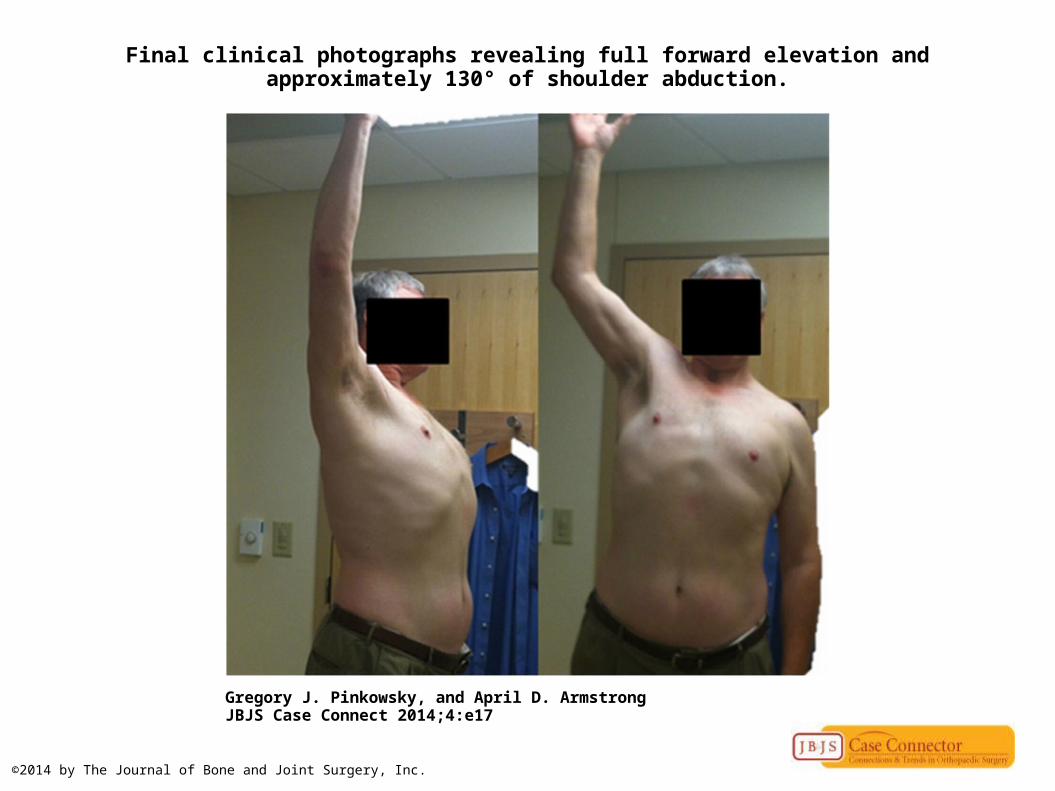
Final clinical photographs revealing full forward elevation and approximately 130° of shoulder abduction.
Gregory J. Pinkowsky, and April D. Armstrong JBJS Case Connect 2014;4:e17
©2014 by The Journal of Bone and Joint Surgery, Inc.