osteoporosis - website staff...
TRANSCRIPT

1
OSTEOPOROSISOSTEOPOROSIS
ERROL U. HUTAGALUNGERROL U. HUTAGALUNG
Div. Of Orthopaedic & TraumatologyDiv. Of Orthopaedic & TraumatologyFaculty of Medicine, Univ. of IndonesiaFaculty of Medicine, Univ. of Indonesia

2
OSTEOPOROSIS
OSTEOPOROSIS (OP) :• Systemic skeletal disease• Low Bone Mass• Changes in microarchitectural of bone tissue Bone Fragility > OP Fx/ Fragility Fx.
• New def 2001: Decreased Bone Strength
3
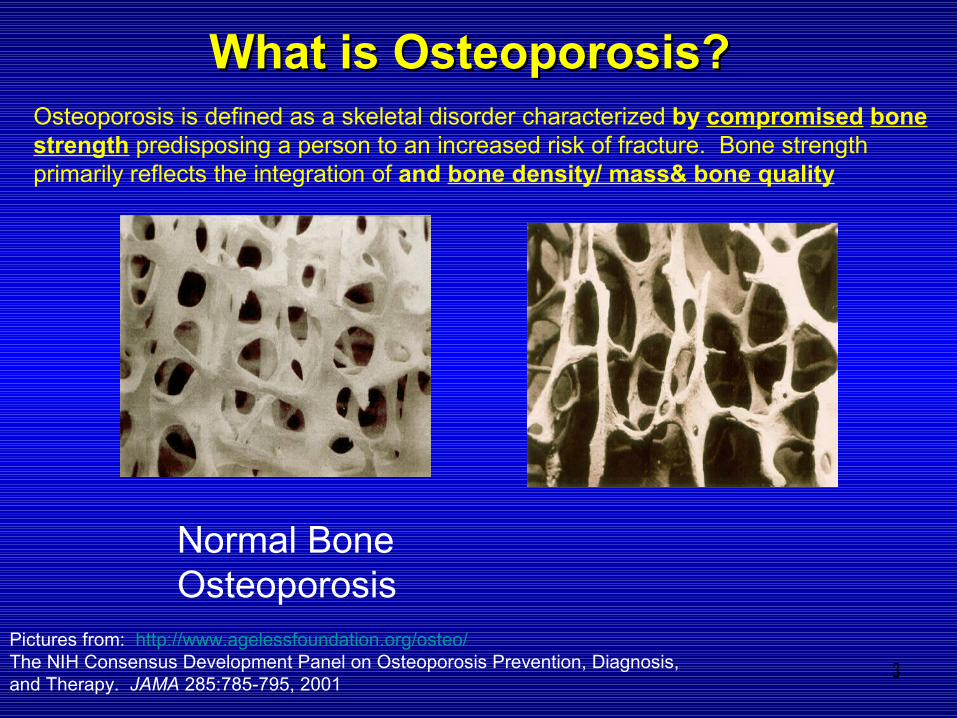
Normal Bone Osteoporosis
Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength primarily reflects the integration of and bone density/ mass& bone quality
What is Osteoporosis?What is Osteoporosis?
Pictures from: http://www.agelessfoundation.org/osteo/The NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. JAMA 285:785-795, 2001

4

5

6

7

8
OSTEOPOROSIS.
PATHOGENESIS OF OP :• Adult healthy bone- renewal process-
remodelling process resorption (osteoclast) & formation (osteoblast) process.
• Resorption-Formation process coupling process.

9
OSTEOPOROSIS
• EACH YEAR 10 % OF SKELETAL BONE IS REPLACED BY NEW BONE.• EVERY 3 – 10 YRS ALL BONES HAS UNDERGONE REMODELLING PROCESS.• IN OP : REMODELLING PROCESS UNCOUPLING PROCESS IMBALANCE OF RESORPTION
& FORMATION PROCESSLOSS OF BONE MASS FRAGILEEASY TO BREAK.• POST MENOPAUSE ESTROGEN DEF.(INHIBITS OSTEOCLAST) RESORPTION >
FORMATION OSTEOPOROSIS +.

10
OSTEOPOROSIS
TYPE OF OSTEOPOROSIS :• PRIMARY :
– TYPE I : POSTMENOPAUSAL OP-MEDIATED BY OSTEOCLAST– TYPE II: SENILE OSTEOPOROSIS- MEDIATED BY OSTEOBLAST-OCCUR IN MEN & WOMEN
> 70 YRS –FORMATION OF BONE <.
• 70 – 80 % ARE PRIMARY TYPE• SECONDARY :
– CAUSED BY AN UNDERLYNG DISEASE/DRUG THERAPY- OCCUR AT ANY AGE

11
OSTEOPOROSIS
SECONDARY OP :• UNDERLIYNG DISEASE :
– HORMONAL IMBALANCE-CUSHING SYNDR.– CANCER, CRF, GI DISORDERS CAUSING MALABSORPTION, HYPOGONADISM IN MEN– DRUG USE – CORTICOSTEROID- GIOP.– POOR NUTRITION
• 30 – 45 % OF AFFECTED INDIVIDUAL NO CAUSE CAN BE IDENTIFIED

12
OSTEOPOROSISOSTEOPOROSISIncidence of OP :Incidence of OP :
-- OP : World study: after 50 yrs :OP : World study: after 50 yrs :- Female 1 out of 3- Female 1 out of 3- Male 1 out of 5- Male 1 out of 5
- World study : 200 mill with OP- World study : 200 mill with OP
- USA,EUROPE,JAPAN : >75 mill- USA,EUROPE,JAPAN : >75 mill -China : 7 % of pop-China : 7 % of pop > 70 mill > 70 mill -Indonesia : > 45 yr : men – 20 %%-Indonesia : > 45 yr : men – 20 %% women- 32 %women- 32 % > 70 yr : men- 38 %> 70 yr : men- 38 % women- 54 %women- 54 %

13
Clinical diagnosis• “ Silent Disease”:• No complain until fracture happens.• Most common location :- Prox femur,Distal radius,Vertebra. Vertebra: due to microfractures/VCF chronic-intermitent back pain,loss of height, increase of dorsal kyphosis-Dowager’s hump-

14
Radiological Diagnosis
• Rarefaction of metaphysis of long bones,
• Thinning of cortex, vertebral bodiesevidence Of deformity.

15
Laboratory diagnosis
• Serum Ca & Phosphor normal • Marker of bone formation : SAP/BSAP,Osteocalcin• Marker of bone destruction : NTX,CTX

16
OSTEOPOROSIS
DIAGNOSIS OF OP :• GOLD STANDARD : EXAMINATION OF BMD (BONE MINERAL DENSITY)• WITH DEXA (DUAL ENERGY X-RAY ABSORPTIOMETRY) METHOD.• pDEXA – ultra sound method – os calcis- for screening purposes- must be
confirmed with DEXA.

17
OSTEOPOROSIS
• INTERPRETATION OF DEXA EXAMINATION ;
• WHO : Normal : T score : > - 1• Osteopeni : T score : - 1 ~~ - 2.5• Osteoporosis : T score : < - 2.5• Severe OP : T score < - 2.5 with one fragility/insuff. fx.

18
OSTEOPOROSIS
• OP –SILENT DISEASE/Asymptomatic• Clinical Problem Fracture +• Fracture Morbidity-Quality Of Life (QOL)• Mortality.• Most common OP Fx:Hip, Vertebra, Wrist• Most seriuos : Hip Fractures

19
Fragility or Osteoporotic Fractures
• Fractures occurring at a site associated with low bone mineral density and which increase in incidence after the age of 50 years
Kanis J, Osteoporos Int 2001; 12(5):417-27

20
Sites associated with low BMD
HIP SPINE WRIST

21
HIP FRACTURESHIP FRACTURES
♦Hip fx is the most serious complication of OP fx in term of Morbidity, Mortality, Economic & Social cost and impact on QOL

22
Hip Fractures

23

24
OSTEOPOROSISOSTEOPOROSISOP HIP FRACTURESOP HIP FRACTURES In spite of up to date tx of hip OP fx:In spite of up to date tx of hip OP fx:
- 20% died within one year mostly as- 20% died within one year mostly as a result of preexisting medical conditiona result of preexisting medical condition- 1/3 remain bed/chair ridden- 1/3 remain bed/chair ridden- 1/3 suffer functional limitations and - 1/3 suffer functional limitations and require assistance require assistance - Only 1/3 return to full function- Only 1/3 return to full function
∴Fractures in elderly OP patients do not only affectFractures in elderly OP patients do not only affect quality of life but also life threatening quality of life but also life threatening
WHO 2003, Perren SM 2005WHO 2003, Perren SM 2005

25
Hip Surgery
• Another study :
• 25% full recovery 75 % will either :
Use a cane or a walker 50% Confined in a nursing home/ 20 – 40 %
self-care assistance (care-givers)Die within the first 12 months 15-20% (40%)
secondary to other chronic disease and consequences of immobilization, especially among age >50

26
OSTEOPOROSISOSTEOPOROSIS
VERTEBRAL FRACTURESVERTEBRAL FRACTURES Many are asymptomatic or cause too few Many are asymptomatic or cause too few
symptoms to provoke investigation.symptoms to provoke investigation. Localization: mid thoracic or thoracolumbar Localization: mid thoracic or thoracolumbar
junction junction weakest region weakest region Quality of life < than hip fx Quality of life < than hip fx 4% needs 4% needs
assistance in ADLassistance in ADL Economic burden: mainly due to outpatient care,Economic burden: mainly due to outpatient care,
provision of nursing care and lost of provision of nursing care and lost of working daysworking days
WHO 2003WHO 2003

27
Vertebral Fractures
• More commonly occur spontaneously• May be secondary to minimal trauma from
spinal loading during day-to-day activities, such as bending forward, lifting objects, and climbing stairs
• High risk of having another vertebral fracture – ~ 20% within the 1st year
1. Cooper C et al. J Bone Min Res. 1992;7:221–227.2. Frost HM. Orthop Clin North Am. 1981;12:671–681.
3. Parfitt AM, Duncan H. In: Rothman RH, Simeone FA, eds. The Spine. 2nd Edition. Philadelphia: WM Saunders;1982:775–905.
28
Vertebral Fracture: underdiagnosed
• Two thirds of new vertebral fractures are not diagnosed1,2
• Often asymptomatic
1. Nevitt MC, et al. Ann Intern Med 1998; 128: 793-800;
2. Cooper C, et al. J Bone Miner Res 1992; 7: 221-7;

29

30

31

32

33

34
75+ KyphoticAt risk for hip fracture
55+ PostmenopausalAt greater risk for vertebral
fracture than any other type of fracture
Healthy spine
Kyphotic spine
50 MenopausalExperiencing
vasomotor symptoms
The Osteoporosis Continuum
Reproduced with permission from MarketForce

35
Vertebral Fractures

36
OSTEOPOROSISOSTEOPOROSISWRIST FRACTURES- Colles FxWRIST FRACTURES- Colles Fx
Caused by a fall on the outstretched handCaused by a fall on the outstretched hand
Peak incidence 60 – 70 yrsPeak incidence 60 – 70 yrs
Less morbidity than hip fx, but painfulLess morbidity than hip fx, but painful
Arch Int. Med’91Arch Int. Med’91

37

38
OSTEOPOROSISOSTEOPOROSIS
1% needs assistance for ADL1% needs assistance for ADL
50%: fair/poor functional outcome50%: fair/poor functional outcome at 6 mosat 6 mos
Complication: Algodystrophy/Sudeck atrophy:Complication: Algodystrophy/Sudeck atrophy: pain, stiffness, swelling of the pain, stiffness, swelling of the
handhand
Brit J Rheu ‘94Brit J Rheu ‘94

39
What are the psychosocial consequences
of fragility fractures?
40
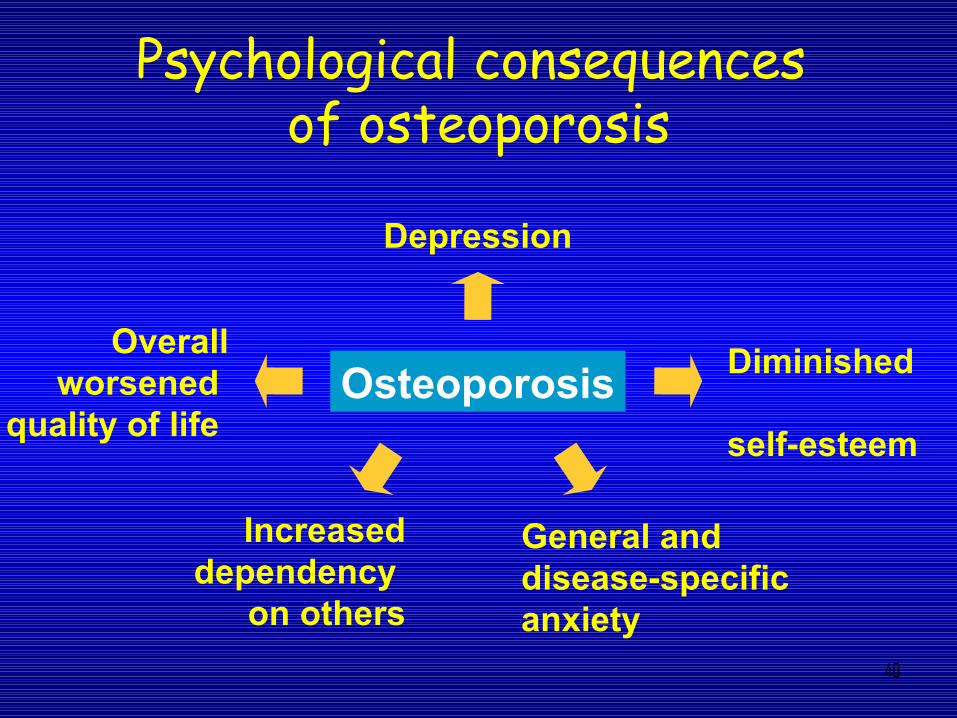
Psychological consequences of osteoporosis
General and disease-specific anxiety
Diminished
self-esteem
Depression
Overall worsened
quality of life Osteoporosis
Increased dependency
on others

41
OSTEOPOROSISOSTEOPOROSISTREATMENTTREATMENT Colles Fx: Colles Fx:
- undisplaced – cast immob.- undisplaced – cast immob.- displaced – closed reduction- displaced – closed reduction
cast immob.cast immob.- immob: 4-6 weeks- immob: 4-6 weeks- avoid prolonged immob - avoid prolonged immob complication complication ↑↑
Vertebral Fractures:Vertebral Fractures:- Lumbar corsett/bracing- Lumbar corsett/bracing- Vertebro plasty- Vertebro plasty- Kyphoplasty- Kyphoplasty

42
OSTEOPOROSISOSTEOPOROSIS
TREATMENTTREATMENT Hip Fx:Hip Fx: Goal: immediate return to mobility to avoidGoal: immediate return to mobility to avoid extended bed rest with it’s complicationextended bed rest with it’s complication
Achieved by Hemi/Total arthroplasty,ORIF to Achieved by Hemi/Total arthroplasty,ORIF to alleviate pain and allow early safe weight bearingalleviate pain and allow early safe weight bearing
After management of Fx After management of Fx DO NOT FORGETDO NOT FORGET TO TREAT OP !TO TREAT OP !

43

44

45
46
OSTEOPOROSISOSTEOPOROSIS
Economic cost of management OP fracturesEconomic cost of management OP fractures
England : £ 942 mill/year – probablyEngland : £ 942 mill/year – probably will will ↑↑ as the number of elderly as the number of elderly ↑↑
USA : $ 13.8 bill in’95 USA : $ 13.8 bill in’95 recently: recently: $ 18 bill/year$ 18 bill/year
and increasingand increasing
Highest cost : Hip fracturesHighest cost : Hip fractures
WHO 2003; Perren SM 2005WHO 2003; Perren SM 2005

47
OSTEOPOROSISOSTEOPOROSIS
USAUSA : - Hip fractures cost $ 21.000: - Hip fractures cost $ 21.000 - Vertebral fracture - Vertebral fracture $$ 1200 1200
- Colles fractures - Colles fractures $$ 800 800
Hong Kong : - Hip fracture : Hong Kong : - Hip fracture : $$ 11.00011.000 - Colles fracture : - Colles fracture : $$ 600 600
Worldwide projection; Annual cost of HipWorldwide projection; Annual cost of Hip fractures USD 3.6 bill in men andfractures USD 3.6 bill in men and USD 19.3 bill in women.USD 19.3 bill in women.Year 2050 would rise to USD 14 bill in menYear 2050 would rise to USD 14 bill in men and USD 73 bill in women.and USD 73 bill in women.Cost of OP fx : ASTRONOMICAL !.Cost of OP fx : ASTRONOMICAL !.
WHO 2003WHO 2003

48

49
OSTEOPOROSISOSTEOPOROSIS
- OP has a healthcare impact second - OP has a healthcare impact second only to C.V. diseaseonly to C.V. disease - Due to very high cost of OP fx - Due to very high cost of OP fx best best policy is avoid/prevent OP fractures policy is avoid/prevent OP fractures identify and treat OP before fx happens !identify and treat OP before fx happens !
I.O.F.I.O.F.

50
OSTEOPOROSIS
• First Step : Identify/Evaluation of RISK FACTORS Case Finding Strategy-CFS- can be
done by GP as front liners, then start taking necessary action

51
OSTEOPOROSIS
• WITH CFSBMD EXAMINATION CAN BE CONFINED TO A MINORITY OF WOMEN 20 % OF POP.
• MOST COUNTRIES ADOPT CFS IN THE MANAGEMENT OF OP.
• USA: POP. SCREENING WITH BMD FOR WOMEN > 65 YRS

52
• RISK FACTORS : -Advanced Age, Low Body Weight/BMI, Early menopause, Maternal history of hip fx, History of fx after age of 40, Gender, Low BMD, Life Style, Specific Medication, Long period of immob., Low sun exposure, Genetics/Family history.
OSTEOPOROSIS

53
Non-Modifiable• Age• Female sex• Maternal family history of hip
fracture• Low birth weight• Disease predisposing to
osteoporosis
Risk factors taken from Jordan & Cooper Best Practice and Res Clin Rheumatol, 2002Categorized by Eli Lilly & Co.
Potentially Modifiable• History of falls• Body mass index• Drug therapy (e.g. corticosteroid use,
use of anti-convulsants)• Primary or secondary amenorrhea• Early menopause• Smoking• Excessive alcohol consumption• Dietary calcium and vitamin D
deficiency
Risk Factors for Osteoporosis and Fracture

54

55
OSTEOPOROSISOSTEOPOROSIS
Combination of several independentCombination of several independent
clinical risk factors clinical risk factors sufficient sufficient
for treatment w/o BMD examfor treatment w/o BMD exam
Kanis OP Int. 2005Kanis OP Int. 2005

56
OSTEOPOROSISOSTEOPOROSIS
TreatmentTreatment
Goal :Goal : - Improve bone quality and- Improve bone quality and strengthstrength -Prevent OP fx. -Prevent OP fx.
IOF VISION : A World w/o OP Fractures !IOF VISION : A World w/o OP Fractures !

57
• MANAGEMENT OF OSTEOPOROSIS.
• NON PHARMACOLOGIC
• PHARMACOLOGIC

58
OSTEOPOROSIS
• NON PHARMACOLOGIC MEASURES : -Adequate exercises, Balanced diet, Intake Ca , Vit D, Life style (smoking, sedentary, alcohol) Fall prevention.
• NON PHARMACOLOGIC MEASURES : -Adequate exercises, Balanced diet, Intake Ca , Vit D, Life style (smoking, sedentary, alcohol) Fall prevention.
• NON PHARMACOLOGIC MEASURES :– Adequate exercises, – Balanced diet, – Intake Ca ,– Vit D, – Life style (smoking, sedentary, alcohol)– Fall prevention
59
OSTEOPOROSISOSTEOPOROSIS
MANAGEMENT OF OPMANAGEMENT OF OP
Pharmacologic measures :Pharmacologic measures : FDA approved :FDA approved : -Antiresorptives : Biphosphonates,Estrogen-Antiresorptives : Biphosphonates,Estrogen CalcitoninCalcitonin -Stimulates Bone Formation : Parathyroid-Stimulates Bone Formation : Parathyroid HormonHormon -Dual Mode Action : Strontium Ranelate.-Dual Mode Action : Strontium Ranelate.

60
OSTEOPOROSISOSTEOPOROSIS
NON PHARMACOLOGICNON PHARMACOLOGIC . .
Elderly patient: Exercise include balance training Elderly patient: Exercise include balance training best outcome Tai Chi best outcome Tai Chi reduced fall reduced fall by 50%by 50%
Exercise may increase BMD and strength of Exercise may increase BMD and strength of bone: 30-50% if start before pubertybone: 30-50% if start before puberty
Type of activity: - Tennis, Badminton, Type of activity: - Tennis, Badminton, Aerobics,Dance, etcAerobics,Dance, etc
- Endurance training: - Endurance training: not as efficient not as efficient
MOVE IT OR LOSE IT !!MOVE IT OR LOSE IT !!- JBJS’05- JBJS’05- IOF 2005- IOF 2005

61
OSTEOPOROSISOSTEOPOROSISNON PHARMACOLOGICNON PHARMACOLOGIC
Elderly: Avoid Fall in the HomeElderly: Avoid Fall in the Home Eliminate all possible elements of risk whichEliminate all possible elements of risk which could lead to fall in the homecould lead to fall in the home slippery floor, loose carpet, stairs,slippery floor, loose carpet, stairs,
medicationmedication
Especially if history of previous fx (+)Especially if history of previous fx (+)
Safe environment Safe environment falls reduced 30-60% falls reduced 30-60%
Hip protector Hip protector Fx Fx ↓↓ 34% 34% Compliance difficultCompliance difficult
Lancet’99/JBJS’05Lancet’99/JBJS’05

62
OSTEOPOROSISOSTEOPOROSIS
Lifestyle change may improve skeletalLifestyle change may improve skeletal health: stop smoking, alcohol, health: stop smoking, alcohol,
maintenance of ideal body weightmaintenance of ideal body weight
Body Mass Index (BMI): Europeans: Body Mass Index (BMI): Europeans: Risk of hip fx Risk of hip fx ↑↑ if BMI < 19 kg/m2 if BMI < 19 kg/m2
WHO 2003WHO 2003

63
OSTEOPOROSISOSTEOPOROSIS
PHARMACOLOGIC.PHARMACOLOGIC.HRT-HRT-H0rmonal Replacement TheraphyH0rmonal Replacement Theraphy
Currently not recommended as the Currently not recommended as the primary prevention of OP in most primary prevention of OP in most
countriescountries
Long term use : questionable Long term use : questionable
Controversy (+)Controversy (+)
WHO 2003; JAMA 2002WHO 2003; JAMA 2002NEJM 2003NEJM 2003

64
OSTEOPOROSISOSTEOPOROSIS
PHARMACOLOGIC .PHARMACOLOGIC .
Parathyroid Hormone (PTH): RecombinantParathyroid Hormone (PTH): Recombinant PTH (teriparatide) PTH (teriparatide) stimulates bone formation stimulates bone formation
Strontium ranelate: dual mode of action Strontium ranelate: dual mode of action antiresorptive & stimulates bone formationantiresorptive & stimulates bone formation
Alfacalcidol and calcitriol (vit D analogues),Alfacalcidol and calcitriol (vit D analogues), Vit K, growth hormone Vit K, growth hormone can improve BMD can improve BMD

65
OSTEOPOROSIS
PREVENTION : ACCORDING TO WOOLF & DIXON :4 PHASES OF PREVENTION : 1. Embryonal phase : NUTRITION during pregnancy
2. Born ~Closure of epiphysis : Diet/Nutrition & Exercise very important.3. Adult : Exercise, optimal Ca, Vit D/Sun exposure
PEAK BONE MASS: Achieved 3rd decadeAfter this bone loss beginMax. gain to minimize bone loss after menopause.4. Menopause : Exercise, Nutrition, Biphosphonate

66
OSTEOPOROSIS
• MANAGEMENT OF OP NEED MULTIDISC. APPROACH
• Nutritionist, Sp.OG, Sp.KO, Sp.RM, Sp.OT, Sp.Geriatrics, Paediatrician-SpA.
• Penyuluh Kesehatan, Ahli Bangunan, Dll.

67
OSTEOPOROSISOSTEOPOROSISCONCLUSIONCONCLUSION OP fx is universal problemOP fx is universal problem Very high economic cost Very high economic cost
Best policy: - Prevention fx in OP and Best policy: - Prevention fx in OP and treat OP before fx happentreat OP before fx happen
- After tx of the fx: - After tx of the fx: DO NOTDO NOT FORGET TO TREAT OPFORGET TO TREAT OP
Intervention/treatment of OP should Intervention/treatment of OP should NOTNOT be guided solely of on the basis of BMD be guided solely of on the basis of BMD
-MANAGEMENT : Multidisc. Approach.-MANAGEMENT : Multidisc. Approach.

68

69

70