outbreak of post-lasik infectious keratitis from single laser center takefumi yamaguchi 1, yoshiko...
TRANSCRIPT

Outbreak of Post-LASIK Infectious Keratitis from Single Laser Center
Takefumi Yamaguchi1, Yoshiko Hori-Komai1, Hiroko Bissen-Miyajima2, Yukihiro Matsumoto3, Kazuo Tsubota3, Jun Shimazaki1,3
1. Department of Ophthalmology, Ichikawa Hospital, Tokyo Dental College, Chiba, Japan2. Department of Ophthalmology, Suidobashi Hospital, Tokyo Dental College, Tokyo, Japan
3. Department of Ophthalmology, Keio University School of Medicine, Tokyo, Japan
The authors have no financial interest in any of the materials mentioned in the presentation.

Introduction
Bacterial keratitis following laser-assisted in situ keratomileusis (LASIK) is a rare complication.
Between October 2008 and March 2009, we experienced an outbreak of infectious keratitis after LASIK performed by the same surgeon.
The Japanese health authorities reported an estimated number of infectious cases of 70, which is the largest in reported cases to our knowledge. The authorities reported the cause of this outbreak was nosocomial infection due to the improper sterilization procedures at the clinic in question.

Purpose
To elucidate the cause and characteristics of the outbreak of infectious keratitis after LASIK and to report clinical outcomes following the treatment.

MethodsData collection In March 2009, we requested 12 major
hospitals in the Tokyo Metropolitan area to report any recent cases of infectious keratitis originating from this particular LASIK clinic, using a standardized questionnaire.
Questionnaire •Surgery and onset•Visual acuities•Characteristics•Microbiological profile•Treatment •Outcome
Patients Thirty-nine eyes in 30 patients were
identified as exhibiting post-LASIK infectious keratitis from 12 different hospitals.
Mean age: 34 years (range, 18-64) Gender: Female/Male : 32/7 eyes
A12
B8
C5
D5
E2
F2
G1
H1
I1
J1
K1
Total39
eyes
No. of eyes
A-K : Hospitals near Tokyo Metropolitan area.

Number of patients, dates of surgery and onset
The first patient involved in this outbreak underwent bilateral LASIK in September 2008. He then developed mycobacterial keratitis in October 2008. Despite the subsequent increase in the number of such cases in other patients treated at the same clinic, the surgeon continued to perform LASIK until the public health authorities launched an inquiry into the clinic and ordered him to stop in January 2009, resulting in a large-scale outbreak of post-LASIK infectious keratitis.
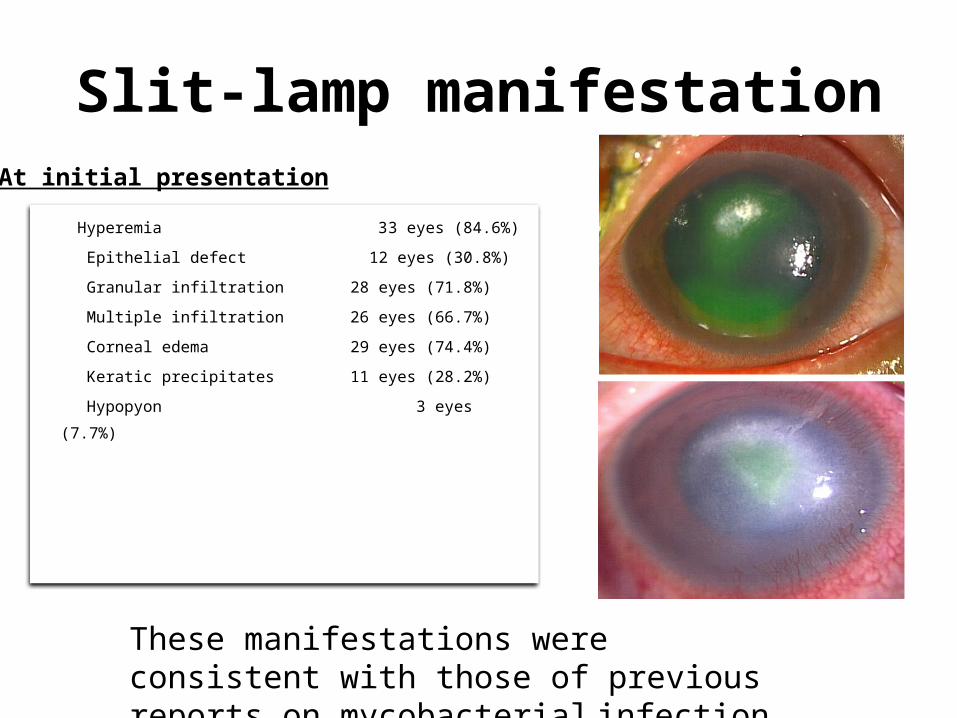
Slit-lamp manifestation
Hyperemia 33 eyes (84.6%)
Epithelial defect 12 eyes (30.8%)
Granular infiltration 28 eyes (71.8%)
Multiple infiltration 26 eyes (66.7%)
Corneal edema 29 eyes (74.4%)
Keratic precipitates 11 eyes (28.2%)
Hypopyon 3 eyes (7.7%)
At initial presentation
These manifestations were consistent with those of previous reports on mycobacterial infection.

Bacterial investigation
29
10
Culture or staining NP
9
11
18
MycobacteriumCorynebacteriumGram-positive coccusNot Detected
Total 39 eyes Total
29 eyes
No. of eyes No. of eyes
The causative organisms were identified as Mycobacterium in 9 eyes (30.3%). No causative organism could be detected in 18 eyes (62.1%).
Culture or stain examinations of corneal scrapings were performed in 29 eyes (76.7%). NP: Not performed

Treatment
Initial treatment at LASIK clinic
• Topical (GFLX, TFLX, TOB) 100%
• Flap lift and irrigation 56%
• Systemic antibiotics (CMX) 28%
Treatment after referral
• Topical (AMK, AMK, EM/CL etc.) 100%
• Flap excision 41%
• Systemic antibiotics (CAM etc.) 28%
Initial treatment could not prevent deterioration of the infection
AMK: amikacin, ABK: arbekacin, EM/CL:erythromycin/colistin, GFLX: gatifloxacin, TFLX: tosufloxacin, TOB: tobramycin, CMX: cefmenoxime, CAM: clarithromycin,
Resolution of the infection was obtained within 1 to 6 months of initial presentation.
Representative case

Visual outcome
1.0≦10
0.6-0.97
0.2-0.58
≦0.114
1.0≦21
0.6-0.911
0.2-0.55
≦0.12
Initial visual acuity after referral Final visual acuity
Decimal visual acuity
No. of eyes No. of eyes
Residual corneal scar was left in all eyes to varying degrees.
Total 39 eyes
Total 39 eyes

On antibiotics• The initial treatment by gatifloxaxin and tosufloxacin
at the clinic did not prevent the development of keratitis, although topical fourth-generation fluoroquinolones have been reported to be more effective than third-generation for the treatment of mycobacterial keratitis.
• Resistant mycobacterial infection wasreported in several cases. Fortified clarithromycin and amikacin might be effective in addition to fourth-generation fluoroquinolones in cases of this study.
Discussion

Discussion On the social issue of medical administration This study revealed the potential possibility of an
epidemic infectious keratitis, which could not be detected until many patients were involved. Patients with severe infection were referred to many different hospitals, making it difficult for this outbreak to be detected.
On visual outcome Final visual acuities in the cases in this study were
almost the same as, or favorable compared with the previous studies.1,2

Conclusion
• Mycobacterium was identified as one of the causative organisms.
• This multicenter study showed comparable outcomes to previous infectious reports.
REFERENCES1. Chang MA, Jain S, Azar DT. Infections following laser in situ keratomileusis: an integration of the
published literature. Surv Ophthalmol 2004;49(3):269-80. 2. John T, Velotta E. Nontuberculous (atypical) mycobacterial keratitis after LASIK: current status and
clinical implications. Cornea 2005;24(3):245-55.