outbreak plan for all facilities in nhs dumfries ... · discharge summaries. ... this plan was...
TRANSCRIPT

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 1 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Outbreak Plan for all Facilities in NHS Dumfries & Galloway
Printed copies must not be considered the definitive version
DOCUMENT CONTROL
POLICY NO.
Policy Group Infection Control Committee
Author Dr Hamilton Version no. 2
Reviewer Infection Control
Team
Implementation date November
2011
Status Approved Next review date November
2013
Approved by Infection Control
Committee
Last review date: January 2008

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 2 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Summary ............................................................................................................................ 5
1. Identifying an Outbreak .......................................................................................... 7
1.1 Do we have an outbreak? ..................................................................................... 7
1.2 What to do if you suspect there may be an outbreak ........................................... 7
1.3 Confirming an outbreak ......................................................................................... 7
1.4 Scale of Outbreak .................................................................................................. 8
2 Background ................................................................................................................ 9
2.1 Introduction ............................................................................................................ 9
2.2 Aims of the plan ..................................................................................................... 9
2.3 Causes ................................................................................................................... 9
3 Control Measures ..................................................................................................... 13
3.1 Restriction on patient movement ......................................................................... 13
3.2 Barrier precautions .............................................................................................. 15
3.3 Cohort nursing ..................................................................................................... 15
3.4 Ward closure ........................................................................................................ 16
3.5 Patient movement ................................................................................................ 17
3.6 Visiting ................................................................................................................. 19
3.7 Recording information ......................................................................................... 22
3.8 Specimens ........................................................................................................... 22
3.9 Hand hygiene ....................................................................................................... 23
3.10 Personal protective equipment ........................................................................ 23
4. Cleaning ................................................................................................................. 24
4.1 Cleaning affected rooms ..................................................................................... 24
4.2 Cleaning a spill of vomit or diarrhoea .................................................................. 25
4.3 Contaminated by stool or vomit ........................................................................... 26
4.4 Deep cleans during an outbreak ......................................................................... 26
4.5 End of an outbreak: the terminal clean ............................................................... 26
4.6 Steam Cleaning ................................................................................................... 27
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 3 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5. Responsibilities in the Event of an Outbreak .................................................... 27
5.1 Infection Control Doctor ....................................................................................... 28
5.2 Infection Control Manager ................................................................................... 28
5.3 Prevention and Control of Infection Nurse .......................................................... 29
5.4 Infection Control Administrator ............................................................................ 29
5.5 Microbiologist ....................................................................................................... 30
5.6 Consultant in Public Health Medicine.................................................................. 30
5.7 Nurse in Charge of affected unit ......................................................................... 31
5.8 Medical Director ................................................................................................... 31
5.9 Duty Nurse Manager ........................................................................................... 32
5.10 Director of Nursing ........................................................................................... 32
5.11 Receiving Consultant ....................................................................................... 33
5.12 Cleanliness Champions ................................................................................... 33
5.13 Domestic Services Manager or Deputy ........................................................... 34
5.14 Superintendent Physiotherapist ....................................................................... 34
5.15 Lead Occupational Therapist ........................................................................... 34
5.16 Area Radiologist ............................................................................................... 34
5.17 Manager with responsibility for Portering ........................................................ 35
5.18 Laboratories General Manager ........................................................................ 35
5.19 Visitors .............................................................................................................. 35
6. Management of the Outbreak Control Process ............................................... 35
6.1 Objectives of Outbreak Control Team ................................................................. 37
6.2 Guiding principles ................................................................................................ 37
6.3 Membership of the Outbreak Control Team........................................................ 38
6.4 OCT decision process ......................................................................................... 39
6.5 Outbreaks in smaller units ................................................................................... 39
6.6 The First meeting of the OCT .............................................................................. 40
6.7 Subsequent meetings .......................................................................................... 44
6.8 Escalation Plan .................................................................................................... 46
6.9 Declaring the outbreak over ................................................................................ 47
6.10 The outbreak review meeting ........................................................................... 49
6.11 The final report ................................................................................................. 51
6.12 How change can be achieved .......................................................................... 53
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 4 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendices
Appendix 1 ....................................................................................................................... 54
Appendix 2 ....................................................................................................................... 55
Appendix 3 ....................................................................................................................... 56
Appendix 4 ....................................................................................................................... 57
Appendix 5 ....................................................................................................................... 58
Appendix 6 ....................................................................................................................... 60
Appendix 7 ....................................................................................................................... 61
Appendix 8 ....................................................................................................................... 62
Appendix 9 ....................................................................................................................... 63
Appendix 10 ..................................................................................................................... 64
Appendix 11 ..................................................................................................................... 65
Appendix 12 ..................................................................................................................... 66
Appendix 13 ..................................................................................................................... 67
References: ...................................................................................................................... 68
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 5 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Summary
As some organisms spread quickly in the healthcare environment and some such as norovirus leave only short term immunity it is difficult to prevent all outbreaks. Careful adherence to Infection Control precautions and the guidance in this document will reduce the number significantly and will limit the personal and service impact of those that do occur. Who is this policy for?(section 2.1): All staff in all NHS wards and facilities in NHS Dumfries and Galloway. What is an outbreak? (section 2.1): 2 or more of the same unusual infection: e.g. strep A, rash illness or a greater than expected rate of a common illness: e.g. gastrointestinal symptoms that might be gastroenteritis. What do I do if I think we might have an outbreak? (section 2.2): Call Infection Control on 33627 or via switchboard. Someone is always available 24 hours a day. Any member of staff in NHS Dumfries and Galloway can call; it is all of our responsibility as part of our duty to protect patients. It is better to have a false alarm than miss a real outbreak. Also let your unit manager know your suspicion and that you have notified Infection Control. Who will help me manage the outbreak? (section 2 and 6): Most outbreaks (Section 1), will be led by the Outbreak Control Team and this policy applies. The Infection Control doctor will decide when to escalate to the Major Incident Plan which covers more major outbreaks. To manage the outbreak an outbreak control team will be formed. It will include ward staff, management and Infection Control. This group will meet daily to direct the management of the outbreak, communicate with those involved and afterwards consider the lessons learned.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 6 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
What control measures will be applied?: See section 3 for details but in general Symptomatic patients should not be moved from their current bed
space without discussion with Infection Control and drug and ward rounds should visit these patients last though patient care should be disrupted as little as possible.
Contacts should be barrier nursed but should also be protected from
exposure to symptomatic patients. Patients from closed rooms or wards should not be moved to other
units if at all possible and if essential the receiving unit and transport must be made aware.
Staff should use stool charts to understand when patients recover
(Appendix 5), Keep accurate lists of patients progress (Appendix 4) and record in nursing and medical notes that a patient has been involved in an outbreak Include this information in all handovers and discharge summaries.
Ward closure is often vital in containing an outbreak The decision
requires a balance between the risk of not doing so and the disruption closure causes.
Visiting an affected ward should be postponed if at all possible.
Children should not visit. Visitors should not visit more than one patient, or use facilities such
as toilets on the ward or visit the canteen. They should not bring uncovered food and should clean their hands on arrival and on leaving the ward.
Who should I contact for further advice?: The Infection Control team can be contacted 24 hours a day on 33627 or via switchboard.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 7 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
1. Identifying an Outbreak
1.1 Do we have an outbreak?
An outbreak can be:
a. 2 or more of the same unusual infection: e.g. strep A, rash illness b. A greater than expected rate of a common illness: e.g. gastrointestinal
symptoms that might be gastroenteritis c. Any cases of rare serious infections possibly acquired in hospital: e.g.
TB, Salmonella food poisoning or legionella pneumonia d. Suspect gastroenteritis in any patient with three or more loose stools,
two or more episodes of vomiting without a clear alternative cause.
The quicker control measures are in place the less the risk an outbreak will spread. The first step is to suspect that there is an outbreak. All staff have the responsibility to protect our patients and this includes being alert for outbreaks and acting quickly to help control it.
1.2 What to do if you suspect there may be an outbreak (patients
on your ward or unit meet the criteria above):
Call Infection Control on 33627 or via switchboard. Someone is always available 24 hours. They might ask:
1. What organism or symptoms 2. Are there other explanations for those symptoms 3. How many patients 4. When did it start 5. Are staff involved 6. Have stool charts and patient lists been started
Any member of staff in NHS Dumfries and Galloway can call: it is the responsibility of all staff as part of our duty to protect patients. It is better to have a false alarm than miss a real outbreak. Also let your unit manager know your suspicion and that you have notified Infection Control.
1.3 Confirming an outbreak
The Infection Control Doctor decides if the incident should be treated as an outbreak. This decision will be taken after discussion with ward or unit staff and other members of the ICT. Appendix 5 gives an example of the process by which the ICD would decide to declare an outbreak.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 8 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
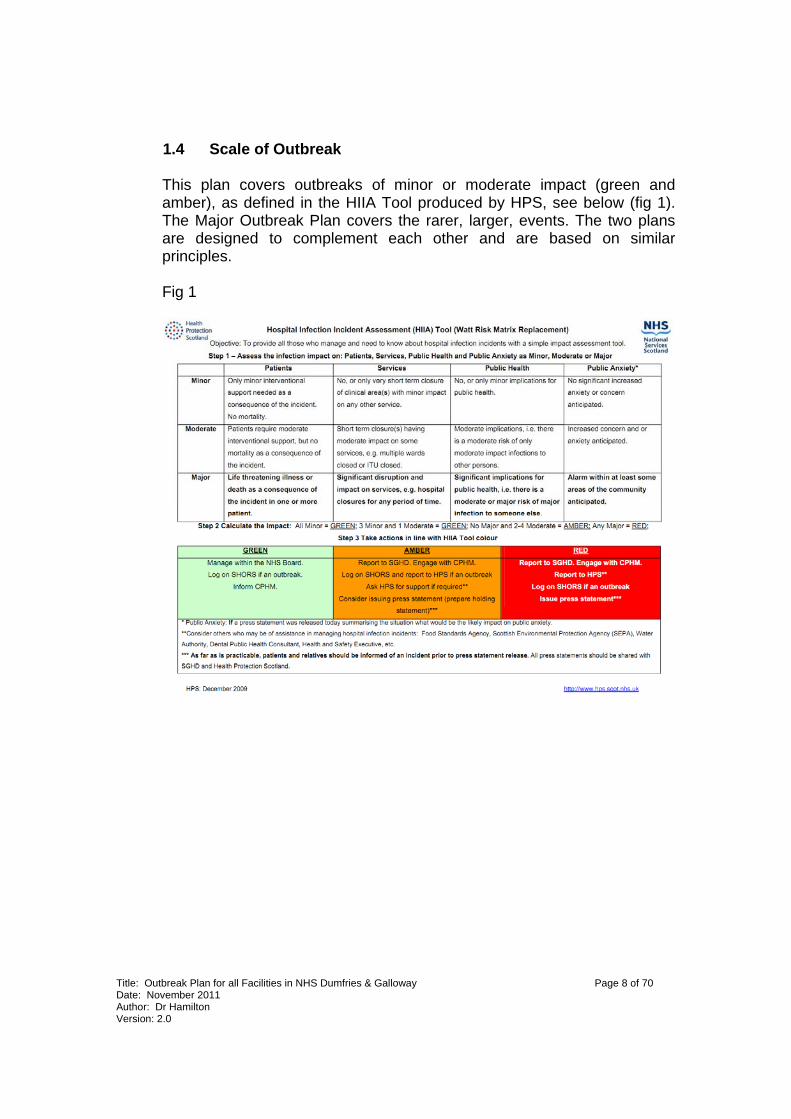
1.4 Scale of Outbreak
This plan covers outbreaks of minor or moderate impact (green and amber), as defined in the HIIA Tool produced by HPS, see below (fig 1). The Major Outbreak Plan covers the rarer, larger, events. The two plans are designed to complement each other and are based on similar principles. Fig 1

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 9 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
2 Background
2.1 Introduction
This plan describes how we control outbreaks in Dumfries and Galloway. Preventing an outbreak requires continuous and carefully applied Infection Control precautions: every patient with gastroenteritis is potentially the start of an outbreak. We must be vigilant for the first signs that infection has spread and must work together to control an outbreak when one occurs. It is the responsibility of every employee of NHS Dumfries and Galloway to play their part. This plan is written in some detail because our aim is to provide clear, concise and thorough advice so all staff can do so.
2.2 Aims of the plan
The aims of the plan are: To ensure prompt action To ensure early recognition of any outbreak of infectious diseases To prevent secondary spread or recurrence, by adequate control
measures. To ensure the outbreak is fully investigated. To provide comprehensive, detailed advice to staff on their role To learn lessons from the incident so that appropriate measures to
prevent recurrence may be taken. 2.3 Causes
Nationally the number of outbreaks of gastroenteritis in both hospitals and the community have increased over the last decade. 95% of outbreaks in Dumfries and Galloway are now caused by norovirus. Occasionally C. difficile, or other bacteria or viruses may be responsible for gastroenteritis outbreaks.
Other potential outbreaks of e.g. MRSA, Flu or TB do occasionally occur in healthcare settings. These are now rare. Details can be found in the specific organism section of the Infection Control Manual. This plan was created with gastroenteritis in mind but the criteria for detecting an outbreak (see section 1 above) will apply to any outbreak.
We have consulted widely to ensure it is as useful as possible but if there are any suggestions please feel free to contact the Infection Control Team or me directly, the numbers are in Appendix 10.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 10 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Noroviruses
Noroviruses (NV), previously known as small round structured viruses (SRSV’s) and Norwalk Like Viruses (NLV’s) are the most common cause of outbreaks of gastro-enteritis in Dumfries and Galloway both in hospitals and nursing/ residential homes. These viruses can be highly infectious causing high attack rates among patients and staff within these setting. Attack rates can reach as high as 70%-90% in patients and staff resulting rapidly in large outbreaks over many clinical areas. It is by incapacitating staff that most harm to patients occurs.
Gastro-enteritis caused by Norovirus infection produces a self-limiting, mild to moderate disease with clinical symptoms of nausea, vomiting (often projectile), diarrhoea, abdominal pain, myalgia (muscle ache), headache, malaise, low grade fever or a combination of these symptoms which can last 12 – 72 hours. The diarrhoea never contains blood and rarely mucus, there is no rash or high fever. These should suggest other causes of gastroenteritis. The incubation period is usually 12 to 48 hours.
The elderly and patients with pre-existing chronic medical conditions may develop more serious symptoms. Treatment in most cases is by rehydration. Staff incapacity can cause considerable problems during outbreaks.
Source: HPS 2011.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 11 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Only humans can be infected with spread mainly by the faecal-oral route, although indirect transmission from environmental contamination and via aerosol help produce the rapid spread in hospital settings. Food may also be a vehicle for transmission of infection but this is rare in hospitals. Norovirus can survive on any surface for a week and on food in a fridge for 10 days.
Source: Gastro-intestinal and foodborne infections: General outbreaks of infectious intestinal disease reported to HPS during 2010, HPS 2011
The incubation period is usually 12-48 hours. The period of communicability is during the symptomatic stage of disease and up to 48 hours after diarrhea/vomiting stops. Virus is found in stool for up to 2 weeks more but if the patient is continent and washes their hands after defecation, the risk is small. After infection short-term immunity lasts up to 14 weeks. This means an individual may contract the same strain again, for instance from environmental contamination. A rapid test is now available making same day diagnosis a possibility. Back up molecular tests are available via the Regional Virus Laboratory. Typing of strains is not routinely carried out, but can occasionally be useful to investigate the dynamics of an outbreak: e.g. in December 2006 this showed that an outbreak in DGRI was actually three separate outbreaks.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 12 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Sapovirus
This recently identified virus is similar to norovirus but usually causes infection only in young children. Symptoms and control are similar to norovirus. A stool sample is required for diagnosis.
Clostridium Difficile C. difficile is a potentially serious cause of often unrecognised outbreaks. This policy should be read with the C difficile policy in the Infection Control Manual.
Salmonella and Campylobacter
Person to person spread of these organisms can occur though food is a more important cause of outbreaks. Rarely healthcare outbreaks can be very serious and deaths can occur. Bloody diarrhea or severe systemic upset may indicate infection with one of these organisms.
E coli 0157
Again spread by food, contact with infected animals or contaminated water. Outbreaks in healthcare are rare but as the infective dose is very low occasionally infections in healthcare workers occur. Careful attention to personal protective equipment is required to prevent cross-infection. A stool sample sent to the laboratory will be routinely tested for salmonella, campylobacter, E coli 0157 and if over 15 years old C. difficile. If an outbreak is suspected the lab will also test for norovirus and if appropriate food poisoning organisms.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 13 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
3 Control Measures
Various control measures may be required to contain an outbreak. Their use is a balance between the effect they will have in containing the infection and the disruption they cause to our care of patients. The Outbreak Control Team therefore judge each outbreak individually. Discussions will be quicker if the patient list in the ward outbreak pack is kept up to date. It is very important that accurate stool charts are kept for each symptomatic patient.
3.1 Restriction on patient movement
Reducing patient movement is the single most important control measure. Attempts to manage norovirus outbreaks without doing so have usually resulted in prolonged outbreaks that are far more disruptive and affect many more patients. The risks are that a patient may have an episode of diarrhoea or vomiting or may simply pass on the virus by touching as it is present on mucous membranes and can be carried on clothing, bedding etc.
The symptomatic patient
Apart from going to the room toilet patients should remain at their bed space. If this would compromise an element of care this should be discussed with Infection Control who will risk assess the care (see Providing Care below). Patients should not leave the ward area to visit the shop, smoke outside or sit with visitors in public areas. They must never visit the canteen.
Virus will be found in stool for several weeks after symptoms end. when formed motions return The risk of cross infection seems to drop to near zero. Diarrhoea may return intermittently after symptoms seem to have settled, often on introduction of a normal diet. For this reason retaining precautions for 48 hours is important.
Best practice statements: 1. Symptomatic patients should not be moved from their current bed
space without discussion with Infection Control. 2. Patient care should be disrupted as little as possible

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 14 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Patients are barrier nursed for 48 hours after the last vomit or loose stool. Incontinent patients, those who may wander or who will not manage a normal level of hygiene e.g. young children, may require a longer period of barrier nursing. Such patients should be discussed with the Outbreak Control Team as their care should be carefully considered.
Patients in contact with a symptomatic patient
The virus is present on mucous membranes shortly before symptoms begin. This means the patient is infectious from 1 hour before they have symptoms. The diarrhoea and especially the vomiting can begin with very little warning, with the risk of contamination of public areas. For these reasons there have to be restrictions on the movements of contact patients.
They remain at risk of contracting the gastroenteritis as long as they are in contact with symptomatic patients. There is therefore a balance between protecting the contact and minimising the risk of them spreading infection if they contract the gastroenteritis. The Infection Control Team will help assess these risks.
Contact patients may use their room toilet but otherwise should remain at their bed space. If this would compromise an element of care this should be discussed with Infection Control who will risk assess the care (see Providing Care below). Patients should not leave the ward area to visit the shop, smoke outside or sit with visitors in public areas. They must never visit the canteen
Where possible symptomatic patients and their contacts should be nursed separately and accommodated in separate rooms. In practice this is not always possible. Contacts are barrier nursed for 48 hours after their last contact with a symptomatic patient.
Best practice statements: 1. Contact patients should not be moved from their current bed
space without discussion with Infection Control. 2. Patient care should be disrupted as little as possible 3. Contacts should be protected from exposure to symptomatic
patients
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 15 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
3.2 Barrier precautions
These are described in the Standard Infection Control Precautions policy and in detail in the Patient Placement guidance. Some infections such as E coli 0157 and norovirus are very infectious. Careful application of the precautions is required to protect staff and other patients.
In addition to those described in the Isolation Precautions the following should be in place:
1. Room doors are kept shut. 2. Outbreak notices from the ward outbreak pack are displayed on room
doors. 3. Detergent wipes with usage information are provided at the door and in
the room. 4. Information for other healthcare staff patients and visitors is made
available as described in communications below.
The patient should be barrier nursed in a single room if at all possible. The Infection Control Team can assist in assessing the patients to nurse in a single room.
3.3 Cohort nursing
Nursing those affected patients together can help by physically separating them from those not affected. It also makes nursing easier. Ward functions such as drug rounds and ward rounds can then visit affected rooms last, reducing the risk of cross contamination. Asymptomatic patients in a cohorted room should be treated as patients in contact with a symptomatic patient as above.
Where an outbreak is more extensive in a ward area it may be the asymptomatic patients who are cohort nursed to protect them.
Best practice statements: 1. Cohort nursing is an efficient way of caring for patients during
an outbreak 2. Drug and ward rounds should visit these patients last

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 16 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
3.4 Ward closure
Why a ward may be closed
This can be disruptive to the care of patients affected. While every effort should be made to limit the impact on patients care it is difficult to maintain normal care. Ward closure is therefore only used where other precautions alone will not control the outbreak. It should usually be applied at the discretion of the Infection Control Doctor in the first instance and the Outbreak Control Team thereafter. Issues considered in coming to a decision to close include:
1. What is the likely outcome of not closing the ward. 2. Can the outbreak course be predicted from the initial spread dynamics,
likely organisms and course of recent similar outbreaks. 3. How clear is the evidence for an outbreak. 4. What will be the impact on current patients of closure. 5. What care will be compromised. 6. Will any discharges to Nursing Homes etc be delayed (see below). 7. What is the impact on future patients – will admissions be delayed, will
patients be cared on less specialist units. 8. Will the visiting restrictions adversely affect patient care.
There is good evidence that prompt ward closure in the correct circumstances can significantly shorten the duration of closure (Lopman et al 2004).
Best Practice Statement: 1. Ward closure is often vital in containing an outbreak 2. The decision requires a balance between the risk of not doing
so and the disruption closure causes. The precautions remain the same as for single room isolation or cohort nursing but are applied ward wide making segregation easier.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 17 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
When a ward is closed to admissions and transfers
Precautions are applied as in barrier precautions and cohort nursing above, but to the whole ward or unit and in addition:
1. Ward or unit doors are kept shut. 2. Outbreak notices from the ward outbreak pack are displayed on ward
entry doors. More may be obtained from the ICT 3. Detergent wipes are provided at the ward or unit entrance, nurses
station and all clinical areas. 4. Gastroenteritis and laundry leaflets are available for all patients and
visitors (in the ward outbreak pack). 5. Information for other healthcare staff is made available as described in
communications below. 6. where present kitchen and pantry doors should be kept closed. 7. Review and remove any equipment that cannot be easily
decontaminated, 8. Stop using fans in ward areas
3.5 Patient movement
Movement within the restricted unit may be required for control reasons. These are time consuming and disruptive to patients. The Outbreak Control Team will minimise such moves. Ward staff will know the patient best so they should make any concerns about the appropriateness of movements clear to the Outbreak Control Team.
Best practice Statements: 1. Patients from closed rooms or wards should not be moved to other
units if at all possible. 2. If it is essential then Infection Control must assess the precautions of
the receiving unit 3. Transport and the receiving unit must be informed of the patient’s
status 4. Transfers home should not normally be delayed though ambulance
control should be informed.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 18 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Transfers within healthcare facilities This includes DGRI, Galloway Community Hospital and the Community Units. Transferring a patient who is symptomatic or a contact poses a significant risk of spreading the outbreak. It should be avoided if at all possible. This applies to any patient who is symptomatic or is a contact. Where a ward or Unit is closed then it will apply to any patient on the unit. An example of a transfer essential for patient care would be a deteriorating patient being taken to ICU. The infection Control Team should be consulted first to assess the risks but also to make arrangements to minimise the risk to the receiving unit. Transfers to community care This would include Nursing homes, rehabilitation centres etc The same rules should apply as for health care facilities. Such units are rarely comfortable taking transfers until clear, and some have their own rules e.g. 72 hours clear rather than 48. Infection Control can help interpret the advice if required. Transfers home Where the transfer is to the patients own home there is rarely any reason to restrict the discharge. Occasionally where there are other vulnerable at home it might be prudent to delay the discharge. Such occasions are rare and should be discussed with Infection Control before a discharge is delayed. If the discharged patient is due Social or Healthcare input at home then the appropriate practitioners should be informed. Being symptomatic is rarely a reason, and a contact never a reason, for such care to be delayed. If the patient is due to attend for treatment then the assessment described in ‘Symptomatic visitors attending’ as patients should be applied (see section 3.6.1 below). It would be rare for a discharge to be delayed except where the patient’s condition gives cause for concern or they are unlikely to be able to care for themselves until recovered. With the patients permission family and carers should be informed of the diagnosis and symptoms to look out for. Transfer to other hospitals out-with Dumfries and Galloway The advice in Transfers within Healthcare Facilities above should be applied. The patients status (symptomatic, awaiting 48 hours, a contact etc) should always be disclosed.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 19 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Transport The ambulance service should always be able to transport a patient even if symptomatic. Such transfers may be more time-consuming (the patient may not be able to share transport) and there may be cleaning required. It is important to disclose the patient’s status fully when booking transport. Infection Control can help if there are difficulties around transfers.
3.6 Visiting
To cause gastroenteritis there must be a source of the virus or bacteria. This is usually by person to person spread from the community. Occasionally a symptomatic or incubating patient may be admitted (refer to isolation policy) and potentially may be a member of staff. It may also be by visitors attending hospital who have or have just had gastroenteritis. We now know that there is even a risk from those carrying virus on their clothing etc. It is very important that visitors comply with simple precautions to limit this risk. It is the responsibility of all staff to help visitors comply.
Symptomatic visitors attending as patients: Outpatients and others with symptoms of diarrhoea or vomiting should not attend without contacting the clinic or unit first. If this is not possible they should explain on arrival. Whether they can be accommodated will depend on the available facilities and the urgency of the appointment. Infection Control can help clinical staff make this assessment. As for patients the risk period is from the start of symptoms until 48 hours after the last loose stool.
Best practice statements: 1. visitors have an important part to play during outbreaks 2. visitors must comply with simple precautions during outbreaks 3. It is the responsibility of all staff to help visitors comply
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 20 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
In accommodating a symptomatic patient staff should consider the following:
1. Will the patient suffer if attendance is delayed 2. Will hospital transport be required – they must be informed and may
not be able to accommodate the patient 3. Is there a separate area for the patient to wait in 4. Which toilet would be used – it should be only for that patient and
cleaned afterwards 5. Which examination/treatment rooms will be used – they must be
cleaned before another patient can use them 6. How will these precautions affect the running of the clinic/unit.
Infection Control can help assess these issues
Symptomatic visitors visiting other patients Visitors with diarrhoea, vomiting or any other infection must not visit. Occasionally on compassionate grounds e.g. where a partner is terminally ill arrangements may be made. This requires careful consideration by clinical staff and the Infection Control Team, balancing the benefit to the patient and visitors and the risks to staff and other patients. Issues to consider include:
1. How will the patient and visitor suffer if unable to visit. 2. What is the risk to the patient if they contract the infection 3. What is the risk to and impact on other patients if they contract the
infection 4. Will hospital transport be required – they must be informed and may
not be able to accommodate the visitor 5. Is there a separate area for the visit to be accommodated 6. Which toilet would be used – it should be only for that visitor and
cleaned afterwards 7. How will these precautions affect the running of the clinic/unit.
Infection Control can help assess these issues.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 21 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Healthy visitors visiting an outbreak ward Most healthcare outbreaks of viral gastroenteritis occur on a background of high community prevalence. There is therefore a risk of further introductions. Simple precautions can reduce this risk substantially and are in place in many hospitals.
The organisation will make efforts to alert the public of outbreaks. Public information will also be available at hospital entrances and at the ward entrance.
This information will ask visitors not to visit an outbreak ward during the period of the outbreak. This is mainly to prevent reintroduction of virus when the level in the community may also be high.
Children should not visit. It is harder for children to comply with non touch policies and to be restricted to one bedside. There is also evidence that children can carry far higher numbers of norovirus viruses than adults.
On arrival at the ward visitors are asked to read the warning notices which will be placed prominently at the doors (Appendix 6, Appendix 7). They should ask advice of ward staff (or contact Infection Control) if further advice is required. The Infection Control number will be on these notices.
They must then cleanse their hands with the detergent hand wipes provided. Alcohol gel should not be used as it is not as effective for gastroenteritis germs. Visitors are asked to go directly to their patient’s bedside and to avoid touching or using facilities such as phones and televisions. Visitors should use the toilets for visitors outside the ward. At no time should visitors use patient toilets. Visitors should not use ward catering facilities to prepare drinks etc.
Best practice statements 1. Visiting an affected ward should be postponed if at all possible 2. Children should not visit 3. Visitors should not visit more than one patient 4. Visitors should not touch or use facilities such as toilets on the ward 5. Visitors should not bring uncovered food 6. Visitors should clean their hands on arrival and on leaving the ward 7. Visitors should not use other facilities during their visit e.g. the
canteen
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 22 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
On leaving the ward visitors should cleanse their hands again as on arrival with the detergent wipes.
Visitors who have visited an outbreak ward should not then use other facilities such as the shop or canteen.
3.7 Recording information
It is important that anyone caring for patients during an outbreak understands that the patient has been involved, whether symptomatic or a contact. Nursing and medical notes should record this as should any hand over between shifts or wards. Discharge summaries should also include the information. On the daily review with the outbreak control team it is important to have an accurate record of numbers and their progress. All the planning in the outbreak control meeting depends on this information.
3.8 Specimens
Different pathogenic organisms spread in different ways, require different control measures and in some cases may require treatment. It is vital that samples of eg stool, in a gastroenteritis outbreak, are sent to the Area Microbiology Laboratory promptly from all symptomatic patients possible.
Remember to fill all details on the specimen and lab form. It is important to include ‘outbreak’ in the clinical details as many of the tests will not otherwise be undertaken. Some tests such as C difficile are available within hours. Others such as norovirus PCR may take longer as the test is performed in a reference lab. Advice on obtaining a suitable stool sample can be found on the Lab Intranet Site and in Appendix 12.
Best practice statements 1. Use stool charts to understand when patients recover 2. Keep accurate lists of patients progress 3. Record in nursing and medical notes that a patient has been
involved in an outbreak 4. Include this information in all handovers 5. Include this information in all discharge summaries

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 23 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
3.9 Hand hygiene
Hands are one of the most important ways of transmitting infection. During outbreaks hand hygiene remains very important. The technique remains unchanged but in a gastroenteritis outbreak it is important NOT to use alcohol gel as both norovirus and C difficile spores are less susceptible.
Staff Staff should use soap and water. Visitors Visitors should use the detergent wipes provided. Patients Patients should be encouraged to wash their hands after using toilets or commodes. Detergent hand wipes can be used if this is not practicable – for instance an immobile patient.
3.10 Personal protective equipment
This should be used as per Standard Infection Control Precautions. Remember to wash your hands after removing gloves (see 3.9). Outbreak Packs Each ward has been supplied with an outbreak pack. This includes stool charts, patient record, ward plan, patient information leaflets door signage and basic checklist. When an outbreak is suspected the pack should be used to record the basic information to help the conversation with the ICD. Remember to call Infection Control when you suspect an outbreak. Infection Control can be contacted via switchboard out of hours at any time. As cases occur it is important that the patient charts are kept up to date and stool charts used for each patient. This information will form the basis of the ICT daily assessment.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 24 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
After the outbreak the ICT will supply a new pack, but fresh leaflets, forms etc can be supplied by Infection Control at any time. The ward door signs should be put prominently on the outside of the ward doors (which will be kept shut) even if the outbreak is contained to part of the ward. The room signs remind staff that the room is involved and give visitors basic instructions. For outbreaks in DGRI the Infection Control Team will place large signs in the hospital entrance alerting visitors to the location of the outbreak.
4. Cleaning
C. difficile and Gastroenteritis viruses survive long periods in the environment. Unless they are removed by careful cleaning further patients may become infected prolonging the outbreak or causing further outbreaks.
4.1 Cleaning affected rooms
These are cleaned as per the Domestic Services Cleaning Specification. Inform Domestic Services of the need for outbreak cleaning by using the notification forms on each ward. Supplies may be obtained from domestic services. This allows the Domestic Services managers to balance the resources to allow the correct cleaning.
Cleaning frequency Cleaning of affected clinical areas will increase, the frequency being set at the OCM, including toilets. Overnight this frequency may be different as set at the OCM. Any concerns as to the frequency or nature of testing should be directed to the ICT or OCT. Disinfection The general environment, including frequently touched surfaces and patient equipment. Use Actichlor plus at 1000 PPM Chlorine.
Best practice statement Inform domestic services promptly using the forms available on the ward – this ensures they increase the cleaning promptly

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 25 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
4.2 Cleaning a spill of vomit or diarrhoea
A patient vomiting is an excellent way of spreading norovirus infection. There are two elements to the risk, the aerosol and the clinical spill itself. Diarrhoea can have up to 1010 (ten billion) virus particles per ml. As few as 100 can be infectious. It is very important therefore that spills are cleaned up promptly and carefully.
The aerosol: staff and patients should be moved away from the vomit spill immediately if possible and doors closed. The area affected should be ventilated by opening windows if possible. Ideally it should be left for 10 minutes before entering to clean the spill. If this is not practical then the best practice points are to keep as many people as far away as possible for up to 10 minutes. Should staff need to enter the area within this time they should minimise contact. It is not now necessary to wear a mask. Evidence suggests the risk when vomit is contained in a bowl or toilet is considerably lower and a mask is therefore only required where there has been a spill. Gloves and an apron should also be worn even if not in direct contact with the spill, again because of the aerosol. Contact with mucous membranes is a potential route of infection but there is no evidence that wearing a visor reduces this risk.
The spill should be cleaned as per the Management of Blood and Body Fluids Policy (Infection Control Manual). It is the responsibility of clinical staff to clean spills. Remember to dissolve the Actichlor tablet in cold water.
Best practice statement 1. Ventilate the room if possible 2. Keep staff and patients away for 10 minutes if possible 3. Gather your equipment and PPE (as per Standard Infection Control
Precautions) 4. Clean the spill with disposable paper towels 5. Then apply Actichlor plus and rinse off. 6. It is NOT necessary to wear an FFP3 mask 7. Dispose of the materials carefully

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 26 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
4.3 Contaminated by stool or vomit
If your skin comes in contact directly with stool or vomit wash it immediately with soap and water. Do not use alcohol gel. Detergent wipes are an alternative but only if washing is not possible.
If a mucous membrane becomes contaminated, eg eyes or mouth,
rinse with copious quantities of water. Inform your line manager immediately.
Uniforms: This is described in detail in the Staff Dress Code and
Uniform Policy and reproduced in Appendix 13.
4.4 Deep cleans during an outbreak Occasionally where environmental soiling is substantial a deep clean may reduce the cross infection pressure. This may include steam cleaning, and will be at the request of the Outbreak Control Team.
4.5 End of an outbreak: the terminal clean
This is an important part of the outbreak control. It removes sufficient environmental contamination that the outbreak will not simply restart when new patients are moved into the affected area. The Outbreak Control Team with decide when a Terminal Clean is required. This will then be arranged by Domestic Services and the ward or unit staff. Close coordination is required between staff to ensure thorough, efficient cleaning. There are several steps which must be undertaken in turn.
1. Responsibilities for cleaning are defined in the Cleaning Policy. 2. First the screens/curtains will be removed for cleaning and sent by the
infected linen stream. 3. Fittings including glass are then cleaned though it is not necessary to
do more than remove marks and stains from walls. 4. Consumables are then replaced, and any stock in the room destroyed
as clinical waste. It is best therefore not to maintain more disposables such as urine bottles etc than are immediately needed.
5. Finally clean screens/curtains are hung and the room is available for patients.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 27 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
The Outbreak Control Team may also require further work, for instance steam cleaning to kill norovirus or C. difficile spores. This will be agreed at the Outbreak Control Meeting and will be undertaken by the Domestic Services team. There is little point in deep cleaning small areas of rooms or doing so without taking down the screens first. In larger outbreaks where there is a shortage of screens single use screens may be used at the discretion of Domestic Services.
4.6 Steam Cleaning
This can be an excellent method of killing gastroenteritis viruses and bacteria and even C difficile spores. It requires trained staff and is not effective on all surfaces or materials. If the ICT feel steam cleaning is required this will be arranged in consultation with the Domestic Services Manager or Supervisor.
5. Responsibilities in the Event of an Outbreak
All staff have a responsibility to safeguard our patients. This includes being alert for possible outbreaks. Section 2 describes the steps if you suspect an outbreak. In the event of an outbreak some staff will have specific duties. For an outbreak to be quickly contained it is important that this multidisciplinary group work well together and each undertakes their individual duties.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 28 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Some staff have specific responsibilities. They are listed below: 5.1 Infection Control Doctor
1. Liaise with Prevention and Control of Infection Nurse in assessing
the potential outbreak 2. Declare an outbreak 3. Categorise the outbreak 4. Liaise with microbiology to ensure adequate sampling has occurred
and laboratory procedures are in place 5. Inform the Procurator Fiscal of deaths of affected patients or
patients where care was compromised as a result of the outbreak. 6. Chair the Outbreak Control Team meetings 7. Lead the Outbreak Control Team 8. Liaise with the Board where significant issues of concern for patient
safety or service provision arise. 9. Responsible for drafting and distributing daily communications to
staff groups 10. Responsible for assisting Communications Manager in drafting
external communications 11. Usually responsible for drafting the outbreak report for OCT and the
ICC 12. Provide training and guidance as required or requested by the
Outbreak Control Meeting or required in the outbreak report. 13. Contribute if requested by the Outbreak Control Meeting to post
outbreak audit as detailed in the outbreak report
5.2 Infection Control Manager
1. Ensure outbreak management policies are in place 2. Ensure the ICT have the resources to manage an outbreak 3. Communicate issues which may impair an effective response to the
appropriate Board directors or unit managers 4. Ensure the Director responsible for HAI is aware of the state of
preparedness or which may impair an effective response 5. Attend OCT meetings if appropriate at the request of the ICD or
discretion of ICM 6. Attend the Outbreak Review Meeting and agree the report with the
ICD or chair. 7. Ensure communications with national organisations are as per
Board and National policies.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 29 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.3 Prevention and Control of Infection Nurse
1. Liaise with Infection Control Doctor in assessing potential outbreak. Assess the dynamics of the outbreak including:
a. Number of patients potentially involved daily. b. Their symptoms and date of onset. c. Any other potential causes of symptoms. d. Their severity and any patients giving cause for concern. e. Staff involved or awaiting 48 hours clearance. f. Update the Outbreak Control Meeting daily
2. Lead with the implementation of Infection Control precautions
including those required by the Outbreak Control Meeting. 3. Ensure ward or unit adherence to outbreak and other Infection
Control precautions. 4. Make the Outbreak Control Team aware of issues or concerns with
such adherence, usually through the Outbreak Control Meeting. 5. Attend and play a role in the decision making of the Outbreak
Control Meeting. 6. Advise the Outbreak Control Meeting on additional control
measures potentially required. 7. Liaise on behalf of the Outbreak Control Meeting with Occupational
Health and Domestic Services. 8. Assist the Outbreak Control Meeting in planning domestic services
involvement including deep cleaning. 9. Assess the appropriateness and quality of cleaning and deep
cleaning. 10. Advise the Outbreak Control Meeting on the need for other cleaning
such as steam cleaning. 11. Provide training and guidance as required or requested by the
Outbreak Control Meeting or required in the outbreak report. 12. Contribute if requested by the Outbreak Control Meeting to post
outbreak audit as detailed in the outbreak report. 13. Make ICD and ICM aware of resource issues around providing this
important and time consuming contribution.
5.4 Infection Control Administrator
1. Attend Outbreak Control Meetings and take minutes. 2. Agree the minutes with the chairperson. 3. Assist in creating the daily e-mail updates. 4. Assist in completing the outbreak report. 5. Assist in administration of audit required in the Outbreak Report.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 30 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.5 Microbiologist
1. Monitor numbers of samples received and communicate this to the Infection Control Doctor and the Outbreak Control Team.
2. Ensure laboratory procedures are in place for correct examination locally and nationally.
3. Promptly communicate results to the Infection Control Doctor and the Outbreak Control Team.
4. Make the Outbreak Control Team aware promptly of any issues that might delay or restrict testing for all common causes of gastroenteritis.
5. Promptly inform the Infection Control Doctor of samples whose number or clinical details suggests an outbreak on other wards or units.
5.6 Consultant in Public Health Medicine
1. Be aware of the outbreak, its location and categorisation. 2. To attend the Outbreak Control Meeting if he or she wishes or if
requested to do so by a member of the Outbreak Control Team or Director of Service.
3. To make the Infection Control Doctor or Outbreak Control Team meeting Chair aware of relevant community or national outbreaks of similar nature.
4. To make the Infection Control Doctor or Outbreak Control Team meeting Chair aware of relevant local or national legislation or guidance that may affect the outbreak management.
5. Assist the ICD in investigating an escalating outbreak if requested.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 31 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.7 Nurse in Charge of affected unit
1. Ensure all staff are familiar with the Infection Control Manual and this Outbreak Management Section.
2. Ensure all staff are able to identify a potential outbreak using the appropriate section of the outbreak management policy and feel able to raise the alarm.
3. Work with the Prevention and Control of Infection Nurse/ICD in the initial investigation.
4. Attend the Outbreak Control Meeting representing the affected ward or unit.
5. Work with the Prevention and Control of Infection Nurse in the daily review of progress, identifying new patients, each patients condition and any affected patient giving cause for concern.
6. Ensure stool charts are up to date for symptomatic patients. 7. Lead with the implementation of precautions as agreed at the
Outbreak Control Meeting. 8. Pass on concerns to the Outbreak Control Team. 9. Organise the timely clinical staff element of the deep clean in liaison
with Domestic Services 10. Contribute to the Outbreak Report and assist in the implementation
of any recommendations for the affected ward. 11. Assist in organising the post outbreak teaching and audit if
required.
5.8 Medical Director
1. Ensure Junior medical staff and consultants colleagues are available to provide medical care on affected units. This may involve short term re-allocation of duties.
2. Contribute to any communications with medical staff with regard to the outbreak.
3. Assist in liaison with general practice and other community staff in reducing or redirecting potentially infectious admissions if requested by the Outbreak Control Team.
4. Attend the Outbreak Control Team if the director feels it appropriate.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 32 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.9 Duty Nurse Manager
1. Inform the PCIN/ICD of potential outbreaks 2. Attend the Outbreak Control Meetings or arrange a deputy 3. Ensure affected wards or units are adequately staffed to provide care
safely 4. Ensure bank or agency staff working on an affected ward understand
the restrictions on working elsewhere for 48 hours. 5. In the event of a bed crisis discuss with the Infection Control Doctor or
Outbreak Control Team chairperson the placement of affected patients or placement of patients on the affected wards
6. Discuss with Outbreak Control Team any concerns about patient care among those affected
7. Discuss with Outbreak Control Team any patients affected who are seriously ill or have died, regardless of the causes.
5.10 Director of Nursing
1. Be aware of the outbreak through the daily updates 2. Raise matters of concern with the Outbreak Control Team 3. Attend the Outbreak Control Meeting if the director wishes 4. Assist in service delivery or nursing issues not resolved through other
routes 5. Provide comment on the Outbreak Report if appropriate
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 33 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.11 Receiving Consultant
1. Restrict admissions of patients with gastroenteritis by considering other methods of care.
2. Discuss with Infection Control Doctor any concerns about patient care among those affected.
3. Discuss with Infection Control Doctor any patients affected who are seriously ill or have died, regardless of the causes.
4. Discuss with Infection Control Doctor any concerns regarding the placement of patients affected and otherwise during an outbreak.
5. Consultants with patients on affected wards. 6. Attend the Outbreak Control Meetings if possible and the Outbreak
Review Meeting if at all possible. 7. Discuss with Infection Control Doctor any concerns about patient
care among those affected. 8. Discuss with Infection Control Doctor any patients affected who are
seriously ill or have died, regardless of the causes. 9. Discuss with Infection Control Doctor any concerns regarding the
placement of patients affected and otherwise during an outbreak. 10. Ensure discharges are to appropriate locations during the outbreak.
Symptomatic patients should not be discharged to other healthcare or nursing units during the outbreak. Occasionally it is in the patients interest to be discharged to another unit from an affected ward if the individual has not themselves been affected. This should be in discussion with the Outbreak Control Team and the other unit concerned. Discharges home are unaffected.
11. Inform the Infection Control Doctor of any medical staff who become symptomatic, and whether this occurred on the premises.
12. Ensure junior and other medical staff in their team do not return to work until 48 hours after the last symptom episode.
5.12 Cleanliness Champions
1. Be alert for potential outbreaks, informing nurse in charge. 2. Be alert for patients who may have symptoms meeting the case
definition, passing this information to nurse in charge. 3. Consider the appropriateness and thoroughness of precautions,
informing nurse in charge of any issues. 4. Discuss with Infection Control Team any concerns that remain. 5. Cooperate in post outbreak audit if required. 6. Return the post outbreak questionnaire.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 34 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.13 Domestic Services Manager or Deputy
1. Attend the Outbreak Control Meetings and the Outbreak Review Meeting.
2. Ensure appropriate cleaning is undertaken on affected wards. 3. Plan and arrange deep cleaning with and warn Outbreak Control
Meeting of logistical or resource issues affecting cleaning. 4. Make Outbreak Control Team aware of issues raised from ward
domestics regarding the control of the outbreak.
5.14 Superintendent Physiotherapist
1. Be aware of the outbreak. 2. Arrange provision of service to minimise risk to other patients. 3. Arrange provision of service to minimise disruption in patient care. 4. Ensure staff are aware of necessary precautions and risks. 5. Liaise with Outbreak Control Team with regard to any service
delivery or staff safety issues. 6. Inform the PCIN of staff who become symptomatic. 7. Make Outbreak Control Team aware of any concerns in control or
care noted during the outbreak.
5.15 Lead Occupational Therapist
1. Be aware of the outbreak. 2. Arrange provision of service to minimise risk to other patients. 3. Arrange provision of service to minimise disruption in patient care. 4. Ensure staff are aware of necessary precautions and risks. 5. Liaise with infection Control team of any service delivery or staff
safety issues. 6. Inform the PCIN of staff who become symptomatic. 7. Make Outbreak Control Team aware of any concerns in control or
care noted during the outbreak
5.16 Area Radiologist
1. Be aware of the outbreak 2. Arrange provision of service to minimise risk to other patients 3. Arrange provision of service to minimise disruption in patient care 4. Ensure staffs are aware of necessary precautions and risks 5. Liaise with infection Control team of any service delivery or staff
safety issues 6. Inform the PCIN of staff who become symptomatic 7. Make Outbreak Control Team aware of any concerns in control or
care noted during the outbreak
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 35 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5.17 Manager with responsibility for Portering
1. Be aware of the outbreak. 2. Arrange provision of service to minimise disruption in patient care. 3. Arrange provision of service to minimise risk to other patients. 4. Ensure staffs are aware of necessary precautions and risks. 5. Liaise with Infection Control team of any service delivery or staff
safety issues 6. Inform the PCIN of staff who become symptomatic. 7. Make Outbreak Control Team aware of any concerns in control or
care noted during the outbreak.
5.18 Laboratories General Manager
1. Liaise with microbiologist to manage workload 2. Ensure phlebotomists are aware of the outbreak and understand
the precautions required 3. Ensure that service to affected wards as normal as service
provision allows. 4. Ensure phlebotomy staff use the available lockers for their
uniforms.
5.19 Visitors
See the visitor section 3.6.
6. Management of the Outbreak Control Process
When an outbreak is identified the ICD will call together a multidisciplinary team, the Outbreak Control Team who will meet regularly as the Outbreak Control Meeting. It is this team, through its meetings, that manages the control strategy. A clear structure is therefore important for this to work and for clinical governance. To emphasise the different functions of each of the four types of meeting they are considered in separate sections below.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 36 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Fig 6.1: The management process
6.1 Objectives of the Outbreak Control Team:
Clinical staff member suspects an outbreak, calls Infection Control
Infection Control Doctor declares an Outbreak and applies the Outbreak Plan
Outbreak Control Team first meeting (section 6.5)
Subsequent meetings (section 6.6)
Outbreak Control team declare the Outbreak over (section 6.7)
Outbreak Review meeting (section 6.8)
Final report (section 6.9)
Achieve action (section 6.10)
Review decision to declare an outbreak Plan control measures Communicate these plans
Review progress Plan control measures Communicate these plans
Review progress, assess risks Declare outbreak over Plan cleaning
Review the appropriateness and effectiveness of control measures. Identify best practice
Summarise the events, make recommendations and demonstrate best practice
Infection Control Committee and Healthcare Governance Committee to monitor progress against recommendations
Identify an outbreak quickly
Manage the outbreak
Prevent further Outbreaks

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 37 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.1 Objectives of Outbreak Control Team As described in the Major Outbreak plan:
1. To identify the extent of the outbreak (section 1). 2. To investigate the source and cause of the outbreak. 3. To agree on any measures necessary to limit the spread of
disease, balancing the benefit of such measures against the risk from disruption caused.
4. To ensure the timely implementation of these measures. 5. To ensure the constitution of the team is appropriate and adequate. 6. To monitor the effectiveness of the control measures. 7. To communicate with the general public, health care workers and
other appropriate staff and agencies directly and through the Board Communications Manager.
8. To ensure adequate media management. 9. To declare the outbreak over. 10. Retrospectively to evaluate the control of the outbreak, co-ordinate
the findings of the investigation, make recommendations for the future and implement the lessons learned.
11. To produce a final report and disseminate it as appropriate.
6.2 Guiding principles
It is the responsibility of OCT members:
1. To carry out tasks they have agreed to undertake, or refer them to their executive officer if unable to carry them out, and inform the OCT Chairperson of this.
2. To maintain accurate and up-to-date records of operational details. 3. To maintain clear lines of communication to all persons concerned
with the investigation and control of the outbreak. 4. To ensure there is a co-coordinated approach to an outbreak
situation. 5. To refer all-important decisions to the OCT for consideration. 6. To retain all documentation, including hand written notes, draft
copies of items and computer generated information relating to the outbreak.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 38 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.3 Membership of the Outbreak Control Team
The Infection Control Doctor will chair the OCT. The chairperson will ensure that minutes of the OCT are taken detailing actions agreed and by whom. NHS Dumfries and Galloway should provide secretarial and information services support. It is important that the number of participants on the OCT is kept manageable. However, core members may well need operational support teams to undertake duties arising from OCT meetings. The OCT should have the power to co-opt other members or request that they attend for agenda items as appropriate.
Core Members
1. Infection Control Doctor (Chairperson) 2. Prevention and Control of Infection Nurses 3. Health Protection Administrator &/or Infection Control Administrator. 4. Site manager 5. Capacity manager 6. Press Officer/ duty manager 7. Domestic Services manager 8. Unit manager/senior nurse for each affected ward or unit 9. Consultants with affected patients
Request Members These will vary according to nature and scale of the outbreak but may include:
1. IT/secretarial support 2. General manager 3. Medical Director 4. Occupational Health Nurse/Doctor 5. Superintendent physiotherapist 6. Superintendent occupational therapist 7. Senior estates manager 8. Nursing Manager(s) 9. Receiving consultant 10. Consultant in Public Health Medicine
Other staff wishing to attend may do so at the discretion of the chair. They may wish to do so to aid communication, contribute by way of professional insight, or for self-education.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 39 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.4 OCT decision process
Model processes have been produced by HPS (Appendix 6 and 7). At the first meeting the Chair should remind the OCT participants of their roles and responsibilities and status as members of the group. Core or requested members who cannot attend should send a deputy. Failure to do so seriously damages the clarity of action of the team.
6.5 Outbreaks in smaller units
At the discretion of the ICD uncomplicated outbreaks in units where most OCT members would be off site can be managed by the ICD on site on their behalf. Agreement should be sought from the Nurse in Charge and Locality Manager. The ICD should communicate carefully with all OCT members, keeping them informed and incorporating their concerns and advice. This should be recorded in a daily log that replaces the OCM minutes as the legal record. Meetings should be held if:
The outbreak is serious Extensive Slow to resolve An OCT member requests it A senior member of clinical or management request it
The ICD should in his or her communications cover the elements of each meeting. It may still be appropriate to hold a review meeting (section 6.8). A report with recommendations (section 6.9) should always be produced and the ICC and HGC (section 6.10) retain their role.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 40 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.6 The First meeting of the OCT
Venue
To allow ward staff to attend OCT meetings for green and single ward yellow outbreaks they should usually be held on the affected ward in a non-clinical area such as the day room or ward office. Outbreaks involving multiple wards will require a larger OCT and will require a suitable off ward venue. The OCT administrator should arrange such a venue after discussion with the chairperson. Issues to consider in choosing a venue include:
1. Likely number of attendees 2. Need for privacy 3. Easy to find 4. Close to clinical areas 5. Risk to the OCT in an affected area 6. Must be free at 10am for 2 hours 7. Should move venue as little as possible
The first meeting
Using the Agenda in appendix 1
1. The chairperson should:
a. Explain the function of the OCM b. Introduce all members c. Describe the meeting arrangements d. Emphasize the importance of attendance
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 41 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
2. The OCT should then consider the following:
a. Hear an overview of the outbreak so far including issues of concern and breaches of Infection Control and other Board policy
b. Outbreak epidemiology including current affected cases and attack rates if appropriate
c. Discuss if necessary the ICD decision to declare an outbreak d. Discuss and agree the risk allocation made using the HIIA Tool
in section 1.4. e. Agree a case definition f. Assess likely pathogens g. Assess likely route of transmission h. Review any available microbiology from cases i. Review relevant information as to the incidence of the potential
pathogens in the affected ward over recent weeks, other NHS Dumfries and Galloway wards and units and in the community at present.
3. Control Measures
a. Review the initial control measures arranged by the unit and
Infection Control team b. Discuss and agree specific control measures which might
include: c. Restrictions on patient movements and to where they should
apply d. Enhanced cleaning and to where it should apply e. Review of staff groups attending the ward and any alterations to
their provision of service f. Sampling required
4. Patient Care
a. Patients giving cause for concern b. Impact of control measures on patient care

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 42 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
5. Communications The meeting should discuss what communications are required specifically with:
a. Patients and visitors. b. Affected ward staff of all grades and disciplines. c. Senior clinical staff and management. d. All staff on the affected site. e. General Practitioners. f. Other Dumfries and Galloway staff groups. g. Local Authority and other local organisations h. Health Protection Scotland and the Scottish Executive
Health Department. i. The media.
6. Responsibilities:
a. Outline/allocate responsibilities between members.
7. Summary:
a. The chairperson should then: b. Ensure each member has the opportunity to raise relevant
issues. c. Summarise the decisions of the meeting and in particular
any control measures agreed or confirmed. d. Agree a venue and confirm a time for the next meeting, and
frequency of meetings (usually daily).
After the meeting
The meeting administrator should then agree any email communications, letters with the chairperson, and the Board communications officer if required. Email updates should be sent within one hour of the end of the OCT meeting. The more prompt the communication the more useful it is to staff and the more rapid their contribution to containing the outbreak.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 43 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Communications
With colleagues
A standard distribution list will be amended during the OCM (section 6.5.2 above). An email prepared by the ICD or meeting chair will be sent daily as soon as possible following the OCM. This short message is intended to alert colleagues to the outbreak.
With Service managers/ Directors of Service
A copy of the OCM minutes will be sent to Managers of affected services and the Medical and Nursing Directors and CPHM.
With NHS Dumfries and Galloway Communications Team
For minor incidents the outbreak notification email will be sent to the Communications Team. For Outbreaks with service impact or with significant cases or public, patient or staff concern the Comms Team will be invited to the OCM or if this is not possible the meeting findings will be communicated directly by the ICD or chair of the OCM. The chair will assist the Comms Team in creating a press release if required.
With National Organisations
Communicate with HPS and SHGD as appropriate to HIIA Tool risk level (section 1.4 above). Details are described in Standard Operating Procedure for the HIIA Tool (Appendix 3). The HAI ORT template (Appendix 11) should be used for communications with the SGHD.
Between meetings:
As further information becomes available and the outbreak evolves the control measures may need to change. The Prevention and Control of Infection Nurse should visit the affected area at least once later in the afternoon to assess the control measures and their impact. If this is not possible the nurse in charge should be contacted. He or she should be warned in advance of the need for this call and the information to have gathered (see section 5.7). Any significant change to control measures should be discussed with the Infection Control Doctor at that point. He or she will agree major changes on behalf of the OCT; assess any further communications required, and whether to call an extra meeting of the OCT.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 44 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.7 Subsequent meetings Frequency
Meetings should usually be daily at 10 am in a venue arranged as above (see section 6.4.1). Serious yellow outbreaks may require twice daily meetings. This will have been agreed at a previous OCT meeting. Logistics may mean in green outbreaks responsibility for decision making is delegated to the Infection Control Doctor on Sundays, but a meeting should always be held on other days.
The OCT should consider the following: Hear an overview of the outbreak over the last 24 hours including issues of concern and breaches of Infection Control and other Board policy
1. Outbreak epidemiology
a. Discuss the risk allocation made b. Review the case definition c. Review likely pathogens and the route of transmission d. Calculate affected cases and possible cases by the case
definition e. Review any available microbiology from cases, and any
typing or reference laboratory results.
2. Control measures
f. Summarize the control measures implemented up to that point including any alterations made since the last meeting.
g. Review any such changes. h. Discuss and agree specific control measures which might
include: i. Restrictions on patient movements and to where they should
apply j. Review of staff groups attending the ward and any
alterations to their provision of service k. Sampling required
3. Patient Care
l. Patients giving cause for concern m. Impact of control measures on patient care

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 45 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
4. Domestic Issues
n. Review the cleaning arrangements and recommend changes as appropriate
o. Plan and coordinate terminal cleaning of bays and wards when appropriate, mindful of ward/unit and domestic services resources.
p. Agree issues of major capital expense such as steam cleaning or carpeting replacement.
5. Communications
q. The meeting should discuss what communications are
required specifically with: r. Patients and visitors s. Affected ward staff of all grades and disciplines t. Senior clinical staff and management u. All staff on the affected site v. General Practitioners w. Other Dumfries and Galloway staff groups x. Local Authority and other local organisations y. Health Protection Scotland and the Scottish Executive
Health Department z. The media
6. Responsibilities:
a. Review responsibilities between members and progress not already discussed.
2. Summary:
The chairperson should then:
a. ensure each member has the opportunity to raise relevant issues.
b. Summarise the decisions of the meeting and in particular any control measures agreed or confirmed.
c. Agree a venue and confirm a time for the next meeting.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 46 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
After the meeting
The meeting administrator should then agree any email communications, letters with the chairperson, and the Board communications officer if required. Email updates should again be sent within one hour of the end of the OCT meeting.
Communications
As for section 6.5.4 above. A daily communication by email should be prepared even if n OCM has not been held.
6.8 Escalation Plan
When control measures fail to stop or contain an outbreak there are two main reasons:
The control measures have not been applied correctly Or the measures are insufficient.
The OCT will therefore consider the current measures on the basis of these two categories. Evidence will be sought that measures are in place. This can be done in part by more detailed direct observation. Ward records will be reviewed for evidence of sustained best practice. The ICD with help of others such as the CPHM may seek evidence of multiple introduction of the causative organism. Healthcare outbreaks are often on a background of high community prevalence. With the Medical Director the ICD may review the admission of symptomatic patients or their contacts and may contact GP’s and others to temporarily restrict such admissions. Details of other potential considerations are detailed in the Control Measures guidance from HPS. Early advice will be taken from HPS to use the national learning base from other outbreaks.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 47 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.9 Declaring the outbreak over Definition
One definition of the end of an outbreak is where there has been no symptomatic patient for 72 hours. In practice that cannot be applied to gastroenteritis outbreaks as a tail of symptomatic patients is common. This would artificially prolong the outbreak. The outbreak will be declared over by the OCT at the OCT meeting. In reaching this conclusion:
The OCT should consider the following: Hear an overview of the outbreak over the last 24 hours including issues of concern and breaches of Infection Control and other Board policy
1. Outbreak epidemiology
a. Review likely pathogens and the route of transmission b. calculate affected cases and possible cases remaining by the
case definition c. Ascertain accurately the onset of the last probable and possible
cases, and their location. d. review any available microbiology from cases, and any typing or
reference laboratory results.
2. Control measures
e. Summarize the control measures implemented up to that point including any alterations made since the last meeting.
f. Review any such changes. g. Discuss and agree specific control measures which might still be
required:
i. Restrictions on patient movements and to where they should apply.
ii. Enhanced cleaning remaining and to where it should apply.
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 48 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
3. Patient care
h. Patients giving cause for concern. i. Impact of control measures on patient care.
4. Domestic issues
j. Review the cleaning arrangements, k. Whether arranged terminal cleaning has been completed and to
an appropriate standard, requiring further cleaning if required. l. Plan and coordinate remaining terminal cleaning of bays and
wards when appropriate, mindful of ward/unit and domestic services resources.
m. Agree issues of major capital expense such as steam cleaning or carpeting replacement.
5. Agree the outbreak is over
The chair should ensure that there is a consensus that the risk of further transmission is sufficiently low that the outbreak can be declared over. In reaching this conclusion the OCT will consider:
n. The time since last definite and possible new cases o. Remaining symptomatic cases and their location p. The logistics of continuing to barrier nurse these cases q. The risk of reopening other beds and reducing the supervision
by the OCT r. The nature of the pathogen concerned, its estimated infectivity
and the local attach rate s. The severity of infection and risk to patients from recurrence of
the outbreak.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 49 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6. Communications
The meeting should discuss what communications are required specifically with:
t. Patients and visitors u. Affected ward staff of all grades and disciplines v. Senior clinical staff and management w. All staff on the affected site x. General Practitioners y. Other Dumfries and Galloway staff groups z. Local Authority and other local organisations aa. Health Protection Scotland and the Scottish Executive Health
Department bb. The media
Summary: The chairperson should then:
cc. ensure each member has the opportunity to raise relevant issues.
dd. Summarise the decisions of the meeting. ee. Agree a venue and confirm a time for the review meeting.
After the meeting
The meeting administrator should then agree any Email communications, letters with the chairperson, and the Board communications officer if required. Email updates should again be sent within one hour of the end of the OCT meeting.
6.10 The outbreak review meeting
This meeting looks back at the events leading up to the outbreak, its management and makes recommendations to prevent subsequent outbreaks. The more of those invited who can attend the more comprehensive and effective the recommendations.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 50 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Membership
This should include all members of the outbreak Control team, members of the Infection Control Committee and others at the request of the Chief Executive or other board members, or the Infection Control Doctor. The Infection Control Doctor or a board member should chair the meeting.
Timing This should be one to two weeks after the outbreak is declared over. Difficulties in arranging attendance should not delay the meeting. Any member who cannot attend should send comments and observations, structured on the agenda to the Infection Control Doctor or administrator.
Principles The Outbreak review meeting has four functions:
1. To establish any avoidable factors that led to the outbreak 2. to review the control measures, and process of control 3. to make recommendations through the Infection Control and
Healthcare Governance Committees to prevent further outbreaks 4. to highlight areas of best practice
Conduct of the meeting: Using the Agenda in Appendix 2
1. The meeting should hear a brief summary of the outbreak, covering the
a. Epidemiology b. Microbiology c. Clinical issues d. Control measures
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 51 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
2. The meeting should consider the outbreak and its management based on the following structure:
a. The days prior to the outbreak should be examined to identify
factors contributing to the outbreak. b. Recent outbreaks with similar syndromes or pathogens should
be considered. c. The control measures should be assessed for their prudence,
appropriateness and success. d. Consideration should be given to whether other measures might
have been useful. e. The impact of the control measures on the service should be
estimated. f. Areas of best practice should be identified.
6.11 The final report
Every outbreak should have a final report. The structure should be as described in the Control Measures guidance from HPS. The outbreak review meeting is structured along these lines. The report should therefore reflect the summaries, considerations and recommendations of the meeting and therefore represent the consensus view from those attending the meeting. Who should write the report The Outbreak Review Meeting should agree an author. In practice this will often be the Infection Control Doctor.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 52 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Structure The following sections should be included:
1. The summary of events Including the number of patients, staff and wards affected. The length of ward closures. 2. Background Known contributing factors 3. Epidemiology Including attack rates 4. Microbiological The causative organism, any typing and number of potential specimens actually received. Result turnaround time. 5. Clinical issues Whether patient health and care was affected. Any potential death should be discussed in detail. 6. Control measures 7. Examples of good practice 8. Assessment of what did not go well As learning points for future episodes 9. Lessons learned and recommendations 10. Suggested audit and clinical assurance 11. Outbreak Review Meeting Membership
Distribution The report should be sent to the ICC, HGC, HMG, members of the OCT, ORG, CPHM, Medical and Nursing Directors, General Managers and others on request or at the discretion of the Chair of the ORM. A copy will be available on the Infection Control Manual pages of the Intranet. The aim is for the report to be a learning tool and so should be available to everyone who can help manage outbreaks.

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 53 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
6.12 How change can be achieved The draft should be prepared within one week of the Outbreak Review Meeting and sent to all who attended. Usually a period of one week will be given for review. A final report will then be prepared by the author and submitted to the next Infection Control Committee. If a recommendation is sufficiently urgent that it cannot be delayed the Infection Control Team will take responsibility for pursuing the issue. If agreed by the Infection Control Committee (or once amendments have been made) further distribution will be arranged as in 6.10.3 above. The Infection Control Committee will take responsibility, led by its chairperson for implementing or taking forward for implementation any recommendations in the report. In practice simple issued may best be undertaken by the Infection Control Team, more complex issues as directed by the ICC and HGC, both of whom should be updated at their next meeting of any problems in resolution. Serious issues should be considered for inclusion in the Infection Control Risk Register.
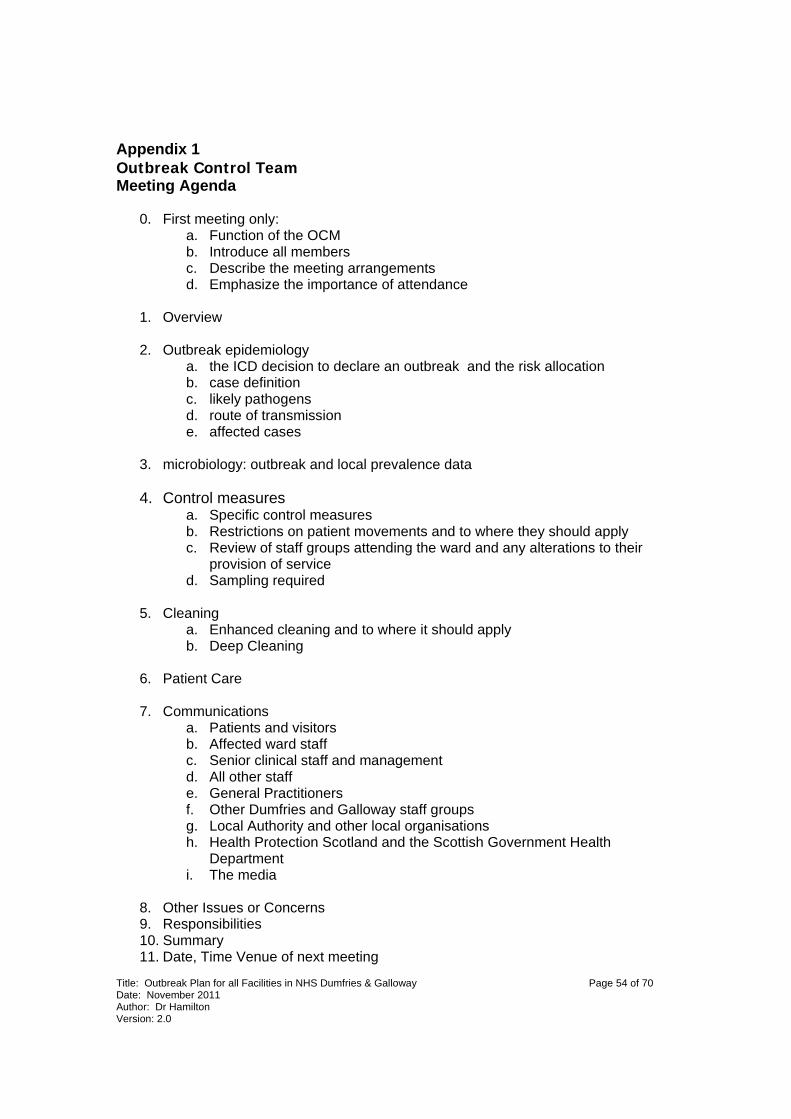
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 54 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendix 1 Outbreak Control Team Meeting Agenda
0. First meeting only: a. Function of the OCM b. Introduce all members c. Describe the meeting arrangements d. Emphasize the importance of attendance
1. Overview 2. Outbreak epidemiology
a. the ICD decision to declare an outbreak and the risk allocation b. case definition c. likely pathogens d. route of transmission e. affected cases
3. microbiology: outbreak and local prevalence data 4. Control measures
a. Specific control measures b. Restrictions on patient movements and to where they should apply c. Review of staff groups attending the ward and any alterations to their
provision of service d. Sampling required
5. Cleaning a. Enhanced cleaning and to where it should apply b. Deep Cleaning
6. Patient Care 7. Communications
a. Patients and visitors b. Affected ward staff c. Senior clinical staff and management d. All other staff e. General Practitioners f. Other Dumfries and Galloway staff groups g. Local Authority and other local organisations h. Health Protection Scotland and the Scottish Government Health
Department i. The media
8. Other Issues or Concerns 9. Responsibilities 10. Summary 11. Date, Time Venue of next meeting

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 55 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendix 2
Outbreak Control Team Review Meeting Agenda
1. Summary of events
2. Background
3. Outbreak epidemiology
a. Numbers of cases
b. Timing
c. Spread
d. Relevant similar outbreaks
4. Microbiology: outbreak and local prevalence data
5. Cinical issues:
a. Symptom profile
b. Severity
c. Deaths
6. Control measures
a. The days prior to the outbreak
b. Restrictions
c. Cleaning
d. Service impact
7. Examples of good practice
8. Lessons learned and recommendations
9. Suggested audit and clinical assurance
10. The final report

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 56 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendix 3 HPS 2009

Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 57 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendix 4 Outbreak Schematic for Norovirus HPS 2009
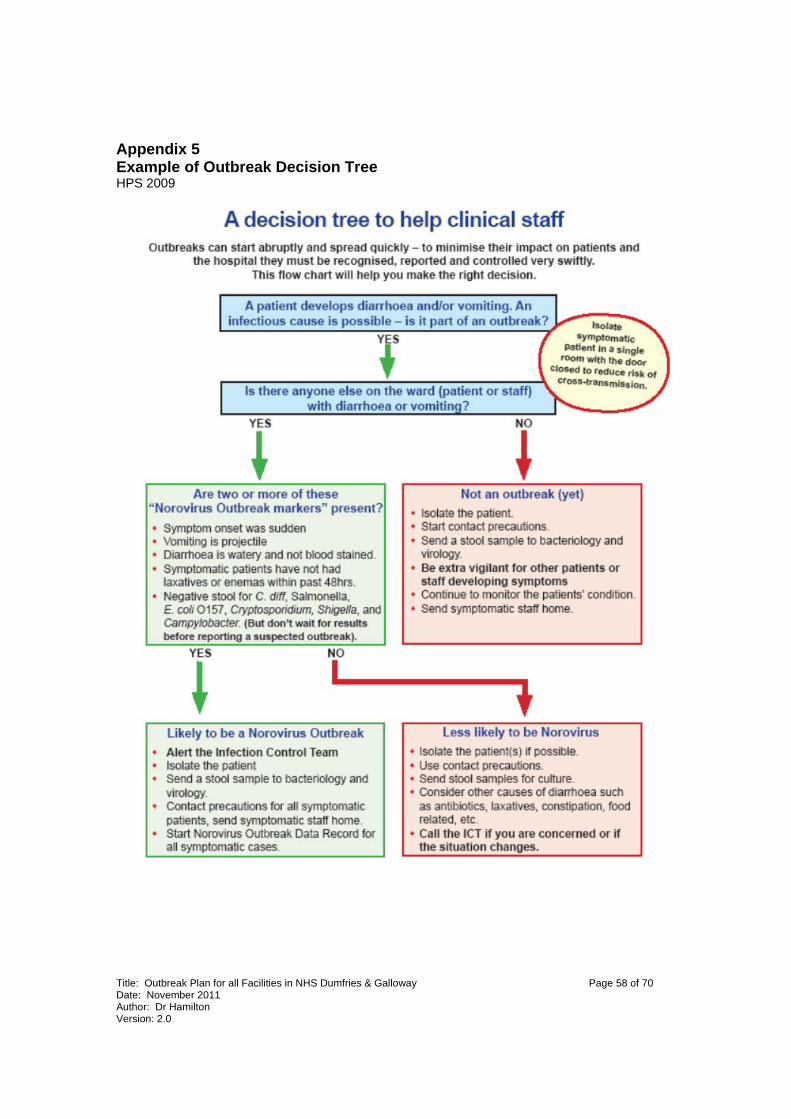
Title: Outbreak Plan for all Facilities in NHS Dumfries & Galloway Page 58 of 70 Date: November 2011 Author: Dr Hamilton Version: 2.0
Appendix 5 Example of Outbreak Decision Tree HPS 2009


60 of 70
Appendix 6 ICT Management Process
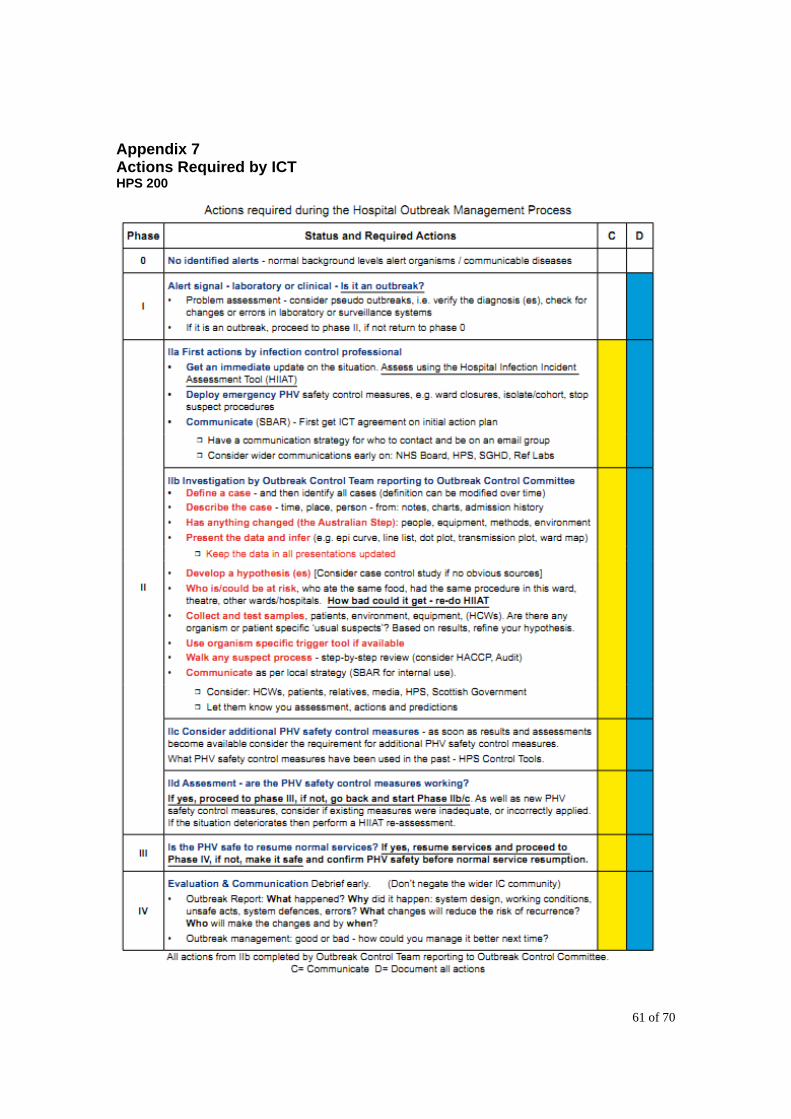
61 of 70
Appendix 7 Actions Required by ICT HPS 200

62 of 70
Appendix 8 Contact list for outbreak notifications TO BE ADDED
63 of 70
Appendix 9 Abbreviations used in this policy: ICT: Infection Control Team ICD: Infection Control Doctor ICM: Infection Control Manager PCIN: Prevention and Control of Infection Nurse OCT: Outbreak Control Team: the group who will manage the outbreak and lead with its review. OCM: Outbreak Control Meeting: the regular meetings of the OCT, where most decisions regarding the outbreak are taken. HIIA: Hospital Infection Incident Assessment Tool HPS: Health Protection Scotland SGHD: Scottish Government Health Department
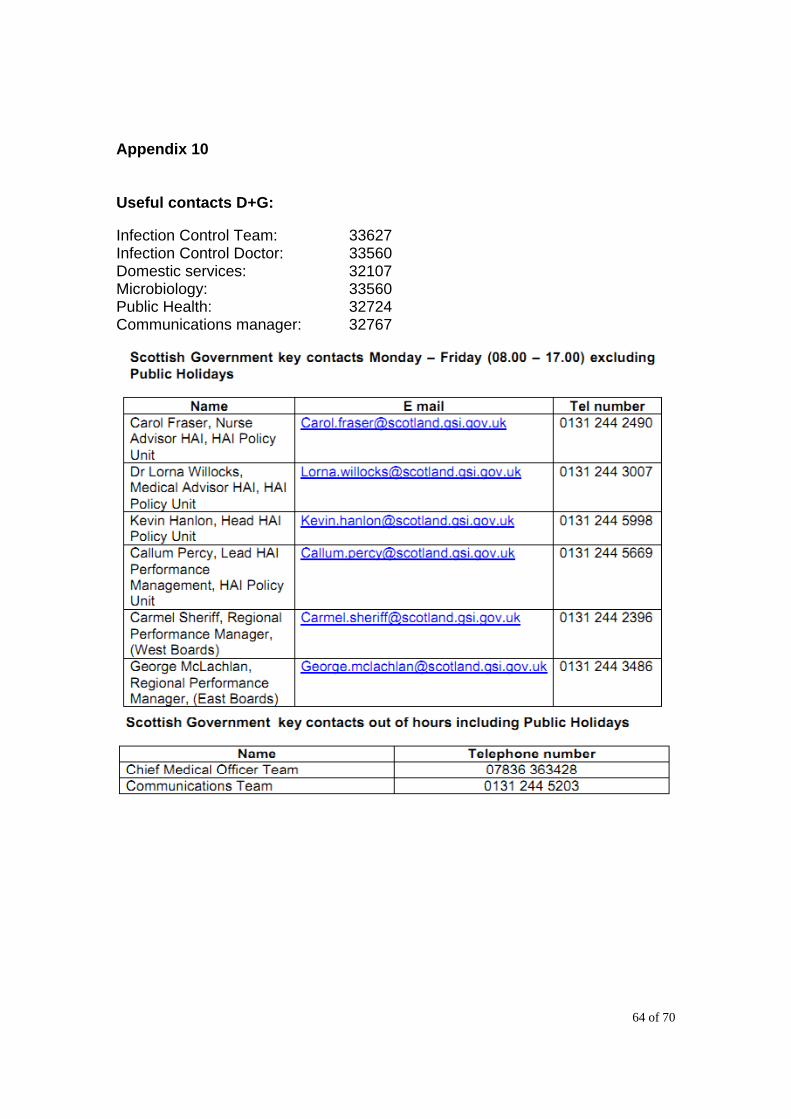
64 of 70
Appendix 10
Useful contacts D+G: Infection Control Team: 33627 Infection Control Doctor: 33560 Domestic services: 32107 Microbiology: 33560 Public Health: 32724 Communications manager: 32767

65 of 70
Appendix 11 HAI ORT template SGHD 2009

66 of 70
Appendix 12 When and how to Obtain a Faecal Specimen from a Patient HPS 2009

67 of 70
Appendix 13 When uniforms are contaminated during an outbreak This extract is taken from the Staff Dress Code and Uniform Policy which can be accessed in full on the intranet:
5.3 Procedure to be followed if a uniform is contaminated with blood/body fluids. Appropriate PPE must be worn to protect uniforms from contamination. The following guidance is for uniforms which are lightly soiled with blood/body fluid: · If a uniform is contaminated by a blood/body fluid, the member of staff must change their clothing immediately, placing the soiled garment/s into a patient “Dissolvo” (dissolvable seal) clothing bag. These bags are available at ward level. Hands must be thoroughly washed and dried after placing the clothes into the bag. · The bag must then be placed into another outer plastic bag to transport the clothing home · The “Dissolvo” clothing bag should be placed directly into the washing machine, and laundered separately at as high a temperature as possible (minimum 60ºC) using normal laundry detergent. Hands must be thoroughly washed and dried at this point. · The “Dissolvo” clothing bag should be removed from the washing machine and disposed in the household domestic waste. · Hands must be thoroughly washed and dried at this point. · At the end of the cycle the clothing should be thoroughly dried and ironed with a hot iron. 5.3.1. If the uniform is grossly soiled, consideration must be given to having the uniform destroyed. · Staff should change the uniform immediately. · Staff should seek approval from their line manager or Infection Control Nurse to condemn the uniform with appropriate records maintained. · Grossly soiled uniforms should be disposed of via the clinical waste stream.

68 of 70
References:
1. Norovirus Outbreak: Control Measures and Practical Considerations for Optimal Patient Safety and Service Continuation in Hospitals. HPS 2009.
2. M K. Estes et al. Noroviruses everywhere: has something changed? Curr. Opin Infect Dis
2006;19:467–474.
3. M Widdowson. Are Noroviruses Emerging? Emerging Infectious Diseases www.cdc.gov/eid 2005;Vol. 11, No. 5.
4. Harris JP et al. Infection control measures for norovirus: a systematic review of outbreaks
in semi-enclosed settings. J Hosp Infect 2010; 74(1): 1-9.
5. MCW Chan Fecal Viral Load and Norovirus Gastroenteritis. Emerg Infectis Dis. www.cdc.gov/eid August 2006; Vol. 12:
6. Dancer SJ. The role of environmental cleaning in the control of hospital-acquired
infection. J Hosp Infect 2009 Dec;73(4):378-85.
7. Working Group of the former PHLS Advisory Committee on Gastrointestinal Infections Preventing person-to-person spread following gastrointestinal infections: guidelines for public health physicians and environmental health officers Commun Dis Public Health 2004; 7(4): 362-384.
8. P. R. Chadwick. Management Of Hospital Outbreaks Of Gastro-Enteritis Due To Small
Round Structured Viruses. Report Of The Public Health Laboratory Service Viral Gastro Enteritis Working Group Journal Of Hospital Infection. 2000; 45: 1–10.
9. Lopman et al. Epidemiology and cost of nosocomial gastroenteritis, Avon, England 2002-
3. norovirus Emerg Infect Dis 2004; 10(10): 1827-34.
10. Y.S. Malik , P.B. Allwood , C.W. Hedberg , S.M. Goyal. Disinfection of fabrics and carpets artificially contaminated with calicivirus: relevance in institutional and healthcare centres Journal of Hospital Infection 2006; 63: 205-210
11. Scottish Government Health Department HAI Incident and Outbreak Reporting Template.
SGHD HAI Team 2009.
12. Sample Standard Operating Procedure for Using the NHSScotland Hospital Infection Incident Assessment (HIIA) Tool. HPS 2009.
13. Said MA et al. Healthcare epidemiology: gastrointestinal flu: norovirus in health care and
long-term care facilities. Clin Infect Dis. 2008;47(9):1202-8.

69 of 70
DOCUMENT CONTROL SHEET 1. Document Status Title
Standard Infection Control Precautions
Author
Dr Hamilton
Approver
ICC
Document reference
1.03
Version number
2.0
2. Document Amendment History Version Section(s) Reason for update 3. Distribution Name Responsibility Version number 4. Associated documents 5. Action Plan for Implementation Action Lead Officer Timeframe
70 of 70
MONITORING FORM
Policy / Strategy Implications None – the policy will work with all other Board policy.
Staffing Implications Reduced staff flexibility will be offset by reductions in staff sickness.
Financial Implications A small increase in the use of personal protective equipment is expected. Reduction in service disruption as a consequence of shortened outbreak duration will result in a significant net saving.
Consultation Wide staff consultation. HPS based guidance has been widely consulted on by patient and partnership groups.
Consultation with Professional Committees
Hospital Management Team
Risk Assessment Not required
Best Value Not applicable
Compliance with Corporate Objectives
Not applicable
Impact Assessment Equality Impact Assessment undertaken