outcomes following endoscopic, expanded endonasal ... · sions with secondary suprasellar...
TRANSCRIPT
6 J. Neurosurg. / Volume 109 / July 2008
HE microscopic, transsphenoidal approach for theresection of certain craniopharyngiomas is well es-tablished and generally accepted,6,13–15,17,20–24,29,30 and
there are several studies comparing this approach with atranscranial approach.21,24,30 Although the transsphenoidalapproach is traditionally limited to predominantly sellar le-sions with secondary suprasellar extension,23 the develop-ment and application of the “extended approach” have pro-vided greater access to suprasellar lesions.17,20,25 Despite thismodification, outcomes from the transsphenoidal approachfor the resection of suprasellar tumors with adherence tocritical surrounding structures have led to more frequent
recurrences and poorer overall outcomes compared withpurely sellar tumors.17 Some of the limitations of this ap-proach, as previously described, may be secondary to theuse of the microscope,2 distance from the surgical target,the small portal of entry to the surgical field (that is, thenostril), and the need for a speculum. Attempting to reme-dy these issues, in 1979 Halves and Bushe10 recognized thefacilitatory role of the endoscope when accessing supra-sellar lesions. To date, however, the endoscope has playeda limited role in most studies of craniopharyngioma, andthere are few studies7 in which the outcomes followingendoscopic, endonasal craniopharyngioma resection havebeen evaluated.
We present a series of 16 cases in which we undertook apurely endoscopic EEA for the resection of craniopharyn-giomas. Short-term ophthalmological and endocrine out-comes along with extent of resection were examined. Thisreport is meant to be an early evaluation of the technique’svalue in the management of these formidable lesions. By
J Neurosurg 109:6–16, 2008
Outcomes following endoscopic, expanded endonasalresection of suprasellar craniopharyngiomas: a case series
PAUL A. GARDNER, M.D.,1 AMIN B. KASSAM, M.D.,1–4 CARL H. SNYDERMAN, M.D.,1,3
RICARDO L. CARRAU, M.D.,1,4 ARLAN H. MINTZ, M.D.,1 STEVEN GRAHOVAC, M.D.,5,6
AND SUSAN STEFKO, M.D.7
Departments of 1Neurological Surgery, 4Otolaryngology, 5Radiology (Division of Neuroradiology),and 7Ophthalmology; 2Minimally Invasive endoNeurosurgery Center; and 3Center for Cranial BaseSurgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania; and 6Departmentof Radiology, Christiana Hospital, Newark, Delaware
Object. Craniopharyngiomas are challenging tumors that most frequently occur in the sellar or suprasellar regions.Microscopic transsphenoidal resections with various extensions and variations have been performed with good results.The addition of the endoscope as well as the further expansion of the standard and extended transsphenoidal approach-es has not been well evaluated for the treatment of this pathological entity.
Methods. The authors performed a retrospective review of all patients who underwent a purely endoscopic, expand-ed endonasal approach (EEA) for the resection of craniopharyngiomas at their institution between June 1999 and Feb-ruary 2006. Endocrine and ophthalmological outcomes, extent of resection, and complications were evaluated.
Results. Sixteen patients underwent endoscopic EEA for the resection of craniopharyngiomas. Five patients (31%)presented with recurrent disease. Complete resection was planned in 11 of the 16 patients. Three elderly patients withvision loss underwent planned debulking, 1 patient with vision loss and a moderate-sized tumor had express wishes fordebulking, and 1 patient had a separate, third ventricular nodule that was not resected. Of those in whom completeresection was planned, 91% underwent near-total (2/11) or gross-total (8/11) resection. No patient who underwentgross-total resection suffered a recurrence. The mean follow-up period was 34 months. Of the 14 patients who presentedwith vision loss, 93% had improvement or complete recovery and 1 patient’s condition remained stable. No patient ex-perienced visual worsening. Eighteen percent of patients (without preexisting hypopituitarism) developed panhypopi-tuitarism and 8% developed permanent diabetes insipidus. There were no cases of new obesity. The postoperative cere-brospinal fluid leak rate was 58%. All leaks were resolved, and there were no cases of bacterial meningitis. There was1 vascular injury (posterior cerebral artery perforator branch) resulting in the only new neurological deficit. No patientdied.
Conclusions. Endoscopic EEA for the resection of craniopharyngiomas provides acceptable results and holds the po-tential to improve outcomes. (DOI: 10.3171/JNS/2008/109/7/0006)
KEY WORDS • craniopharyngioma • endonasal resection • endoscopic resection •outcome
T
See the Editorials and the Response in this issue, pp 1–5.
Abbreviations used in this paper: CSF = cerebrospinal fluid; DI =diabetes insipidus; EEA = expanded endonasal approach; GH =growth hormone; GKS = Gamma Knife surgery; ICP = intracranialpressure; PCA = posterior cerebral artery; TSH = thyroid-stimulat-ing hormone; VP = ventriculoperitoneal.

comparing these results with those previously published forother approaches, we hope to better judge both approachesin terms of their respective advantages and disadvantages.
Although authors of many past studies have assessed cra-niopharyngioma resection via a transsphenoidal route,2,17,
23,24,29 few7 have used a purely endoscopic technique andmost are biased toward the resection of tumors with mini-mal supra- or parasellar extension. Our series consists oftumors located above and/or with extension superior andlateral to the sella, superior and posterior to the chiasm, andeven extending into the third ventricle.
Methods
After obtaining institutional review board approval, wereviewed the medical records and imaging studies of all pa-tients with the histopathological diagnosis of craniopharyn-gioma treated via an EEA between June 1999 and February2006. No patient was excluded or lost to follow-up, result-ing in a series of 16 patients (Table 1). Patients’ ages rangedfrom 36 to 80 years (mean age 55 years). There was a male/female ratio of 5:3. Five patients (31%) presented to uswith recurrent disease. One patient had undergone pri-or transsphenoidal resection, 4 had prior craniotomies (1of whom also underwent prior stereotactic cyst drainagewith intracystic brachytherapy), and 1 had undergone ra-diosurgery. In addition, 1 patient underwent a previoustranssphenoidal procedure for a pituitary adenoma (his-topathology verified). Other complicating conditions in-cluded obesity, chronic obstructive pulmonary disease, andpregnancy. Most patients (14 [87.5%] of 16) presented withprogressive visual deficit as the primary indication for sur-gery (Table 2). We report ophthalmological and endocrineoutcomes, as well as extent of resection and complications.The follow-up period for this study ranged from 2 to 82months (mean follow-up 34 months).
Operative Technique
We detail the operative technique elsewhere.19 As such,only a brief overview will be provided here. The operationswere all performed by 2 surgeons (A.B.K. or P.A.G. andC.H.S. or R.L.C.), a neurosurgeon, and an otolaryngologist.A binarial, purely endoscopic, image-guided approach wasused. The patient was placed supine, the head fixed in pins,the neck in a neutral or slightly extended position (10–15°,depending on the anterior/superior extent of the tumor),and the head turned 5–10° toward the surgeon to allowcomfortable hand position and improve access. First, oxy-metazoline-soaked pledgets were placed into the nares forseveral minutes, prior to preparation. Then, the image-guided system was calibrated with the patient. We pre-ferred to use MR imaging, but we used CT angiography incases in which the patient was unable to undergo MR imag-ing or the bone anatomy or involved vasculature was criti-cal for resection. Next, the abdomen (for fat graft harvest)and midface were prepared with Betadine-soaked sponges.The patient was then draped, leaving only the nose and pre-pared abdomen exposed. Imaging guidance was once moreconfirmed, using external landmarks.
Entering the right nostril, the middle turbinate was eitherlateralized or removed under endoscopic guidance and theanterior wall of the sphenoid was entered. The contralater-
al nostril was then entered and the sphenoid similarly ap-proached, with lateralization of the middle turbinate. Next,the critical step of partial removal of the posterior internasalseptum (~ 1 cm) was performed. This permitted introduc-tion of instrumentation from the contralateral naris withoutobscuring the endoscopic view. After the posterior wall ofthe sphenoid sinus was exposed, the image guidance wasonce more introduced to confirm bone landmarks as well astumor location. This step is important, as the normal sellaranatomy is often greatly distorted by tumor. The bone overthe tumor’s dural covering was next drilled and complete-ly removed using angled rongeurs. Through this process,the surrounding anatomy was defined, with special atten-tion given to the location of the cavernous sinuses, carotidarteries, and optic nerves. The bone over the superior inter-cavernous sinus was removed next (if necessary) using acombination of drill and rongeur. At this point, the criticalportion of the sellar bone removal, over the medial opti-cocarotid recess, was carried out as described elsewhere.19
This variable indentation on the sphenoid sinus side of thelateral tuberculum represents the medial confluence of theoptic nerve, carotid artery, and anterior skull base, provid-ing a “keyhole” of sorts for this access. When necessary,the superior intercavernous sinus was carefully and com-pletely coagulated using bipolar cautery, prior to its divi-sion. This additional rostral exposure often provided thestarting point for tumor surgery and/or dural entry, espe-cially when approaching a supra- or retrochiasmatic lesion.In suprasellar lesions, the dura was opened in a cruciatemanner, and the tumor was located if not immediately ap-
J. Neurosurg. / Volume 109 / July 2008
Outcomes following EEA for resection of craniopharyngiomas
7
TABLE 1Characteristics in patients who underwentan endoscopic EEA for craniopharyngioma
Case Age (yrs), Date of Op TumorNo. Sex (mo/day/yr) Comment Type*
1 42, M 06/08/99 none I2 36, F 04/12/02 presented 14 wks pregnant I3 46, F 10/21/02 previous stereotactic cyst drainage, IIIb
intracystic brachytherapy & eyebrow craniotomy
4 43, M 11/05/02 none IIIa & b5 50, M 05/08/03 recurrent tumor (previous bicoro- II
nal craniotomy)6 58, M 07/16/03 obese/severe COPD IIIb7 69, M 08/20/03 transsphenoidal adenoma resec- II
tion 7/17/028 34, M 08/25/03 recurrent tumor (previous bicoro- I
nal craniotomy)9 56, F 01/26/04 none IIIb
10 51, F 06/21/04 none IIIa & b11 55, F 07/02/04 recurrent tumor II12 52, F 09/01/04 presented w/ increased thirst II13 79, M 12/06/04 none IIIa14 80, M 01/10/05 prior craniotomy SRS; ataxia w/ IIIb
recurrence (pontine compres-sion)
15 48, M 08/08/05 panhypopituitarism, gland IIcompletely calcified
16 79, M 02/20/06 none IIIa & b
* Type I denotes preinfundibular; Type II, transinfundibular; and Type III,retroinfundibular (a, rostral extension [interpeduncular cistern]; b, caudal ex-tension [prepontine cistern]). Abbreviations: COPD = chronic obstructivepulmonary disease; SRS = stereotactic radiosurgery.
parent. An extracapsular dissection allowed the surgeon todefine tumor as well as key surrounding structures (for ex-ample, the optic chiasm and perforating vessels, pituitarygland and stalk, and major arteries). The tumor capsule wasthen entered, and debulking was performed. Finally, the ex-tracapsular dissection was completed, and the tumor was re-moved from any adherent normal structures by using sharpdissection. After a final inspection, the dural closure wasbegun. This reconstruction step has undergone considerableevolution during our experience and continues to be eval-uated for improvement. By the end of the series, a lumbardrain was used only in cases in which the third ventricle wasentered or in communication as a result of the resection.
Throughout this series, some type of onlay graft, fol-lowed by fat graft has been used. At the end of the series,this has progressed to an inlay of DuraGen (Integra Lifesci-ences Corp.), followed by an acellular dermal onlay graft.The sphenoid sinus was ultimately packed with fat, whichwas covered with Surgicel (Ethicon) and followed by nasalstents and either pledgets or a Foley catheter balloon as abuttress. Since then, we have begun using a vascularizednasal septal mucosal flap as a final layer over the onlaygraft with promising results.9
Results
Ophthalmological Results
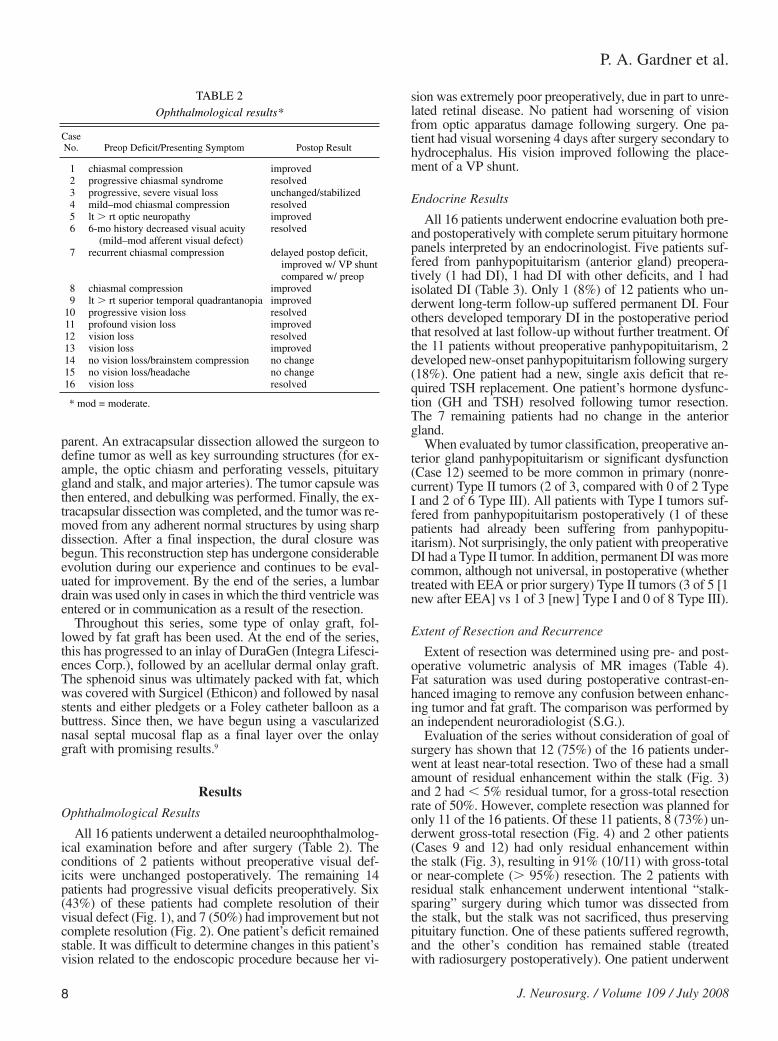
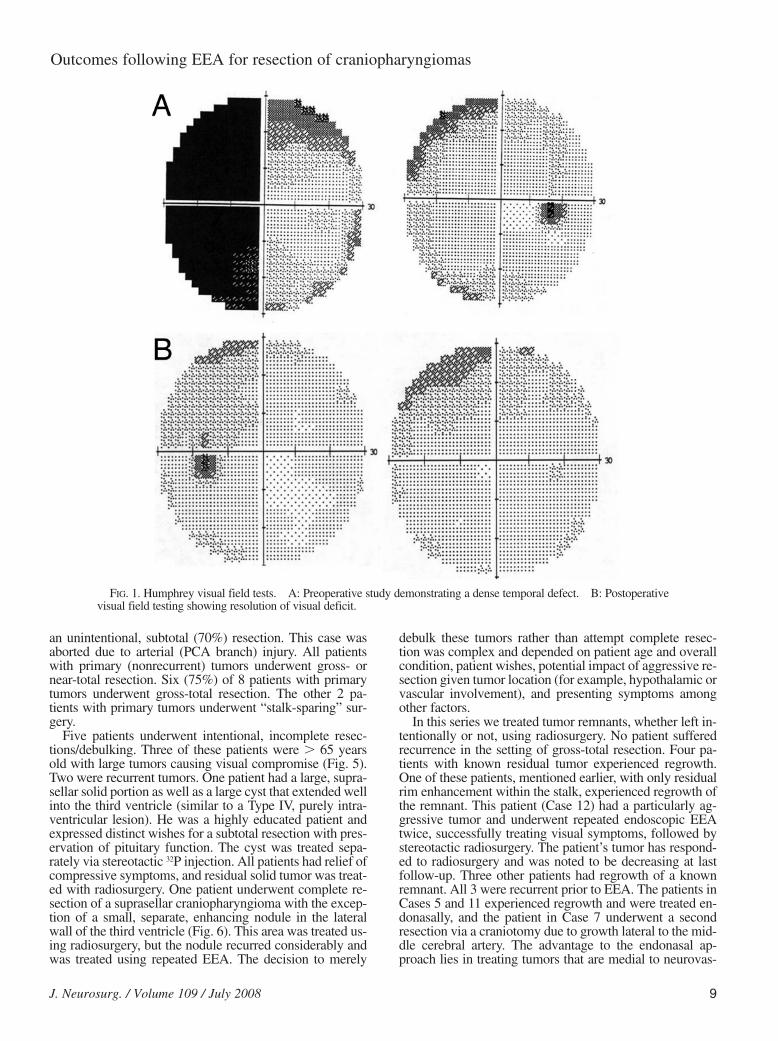
All 16 patients underwent a detailed neuroophthalmolog-ical examination before and after surgery (Table 2). Theconditions of 2 patients without preoperative visual def-icits were unchanged postoperatively. The remaining 14patients had progressive visual deficits preoperatively. Six(43%) of these patients had complete resolution of theirvisual defect (Fig. 1), and 7 (50%) had improvement but notcomplete resolution (Fig. 2). One patient’s deficit remainedstable. It was difficult to determine changes in this patient’svision related to the endoscopic procedure because her vi-
sion was extremely poor preoperatively, due in part to unre-lated retinal disease. No patient had worsening of visionfrom optic apparatus damage following surgery. One pa-tient had visual worsening 4 days after surgery secondary tohydrocephalus. His vision improved following the place-ment of a VP shunt.
Endocrine Results
All 16 patients underwent endocrine evaluation both pre-and postoperatively with complete serum pituitary hormonepanels interpreted by an endocrinologist. Five patients suf-fered from panhypopituitarism (anterior gland) preopera-tively (1 had DI), 1 had DI with other deficits, and 1 hadisolated DI (Table 3). Only 1 (8%) of 12 patients who un-derwent long-term follow-up suffered permanent DI. Fourothers developed temporary DI in the postoperative periodthat resolved at last follow-up without further treatment. Ofthe 11 patients without preoperative panhypopituitarism, 2developed new-onset panhypopituitarism following surgery(18%). One patient had a new, single axis deficit that re-quired TSH replacement. One patient’s hormone dysfunc-tion (GH and TSH) resolved following tumor resection.The 7 remaining patients had no change in the anteriorgland.
When evaluated by tumor classification, preoperative an-terior gland panhypopituitarism or significant dysfunction(Case 12) seemed to be more common in primary (nonre-current) Type II tumors (2 of 3, compared with 0 of 2 TypeI and 2 of 6 Type III). All patients with Type I tumors suf-fered from panhypopituitarism postoperatively (1 of thesepatients had already been suffering from panhypopitu-itarism). Not surprisingly, the only patient with preoperativeDI had a Type II tumor. In addition, permanent DI was morecommon, although not universal, in postoperative (whethertreated with EEA or prior surgery) Type II tumors (3 of 5 [1new after EEA] vs 1 of 3 [new] Type I and 0 of 8 Type III).
Extent of Resection and Recurrence
Extent of resection was determined using pre- and post-operative volumetric analysis of MR images (Table 4).Fat saturation was used during postoperative contrast-en-hanced imaging to remove any confusion between enhanc-ing tumor and fat graft. The comparison was performed byan independent neuroradiologist (S.G.).
Evaluation of the series without consideration of goal ofsurgery has shown that 12 (75%) of the 16 patients under-went at least near-total resection. Two of these had a smallamount of residual enhancement within the stalk (Fig. 3)and 2 had , 5% residual tumor, for a gross-total resectionrate of 50%. However, complete resection was planned foronly 11 of the 16 patients. Of these 11 patients, 8 (73%) un-derwent gross-total resection (Fig. 4) and 2 other patients(Cases 9 and 12) had only residual enhancement withinthe stalk (Fig. 3), resulting in 91% (10/11) with gross-totalor near-complete (. 95%) resection. The 2 patients withresidual stalk enhancement underwent intentional “stalk-sparing” surgery during which tumor was dissected fromthe stalk, but the stalk was not sacrificed, thus preservingpituitary function. One of these patients suffered regrowth,and the other’s condition has remained stable (treatedwith radiosurgery postoperatively). One patient underwent
P. A. Gardner et al.
8 J. Neurosurg. / Volume 109 / July 2008
TABLE 2Ophthalmological results*
CaseNo. Preop Deficit/Presenting Symptom Postop Result
1 chiasmal compression improved2 progressive chiasmal syndrome resolved3 progressive, severe visual loss unchanged/stabilized4 mild–mod chiasmal compression resolved5 lt . rt optic neuropathy improved6 6-mo history decreased visual acuity resolved
(mild–mod afferent visual defect)7 recurrent chiasmal compression delayed postop deficit,
improved w/ VP shuntcompared w/ preop
8 chiasmal compression improved9 lt . rt superior temporal quadrantanopia improved
10 progressive vision loss resolved11 profound vision loss improved12 vision loss resolved13 vision loss improved14 no vision loss/brainstem compression no change15 no vision loss/headache no change16 vision loss resolved
* mod = moderate.
an unintentional, subtotal (70%) resection. This case wasaborted due to arterial (PCA branch) injury. All patientswith primary (nonrecurrent) tumors underwent gross- ornear-total resection. Six (75%) of 8 patients with primarytumors underwent gross-total resection. The other 2 pa-tients with primary tumors underwent “stalk-sparing” sur-gery.
Five patients underwent intentional, incomplete resec-tions/debulking. Three of these patients were . 65 yearsold with large tumors causing visual compromise (Fig. 5).Two were recurrent tumors. One patient had a large, supra-sellar solid portion as well as a large cyst that extended wellinto the third ventricle (similar to a Type IV, purely intra-ventricular lesion). He was a highly educated patient andexpressed distinct wishes for a subtotal resection with pres-ervation of pituitary function. The cyst was treated sepa-rately via stereotactic 32P injection. All patients had relief ofcompressive symptoms, and residual solid tumor was treat-ed with radiosurgery. One patient underwent complete re-section of a suprasellar craniopharyngioma with the excep-tion of a small, separate, enhancing nodule in the lateralwall of the third ventricle (Fig. 6). This area was treated us-ing radiosurgery, but the nodule recurred considerably andwas treated using repeated EEA. The decision to merely
debulk these tumors rather than attempt complete resec-tion was complex and depended on patient age and overallcondition, patient wishes, potential impact of aggressive re-section given tumor location (for example, hypothalamic orvascular involvement), and presenting symptoms amongother factors.
In this series we treated tumor remnants, whether left in-tentionally or not, using radiosurgery. No patient sufferedrecurrence in the setting of gross-total resection. Four pa-tients with known residual tumor experienced regrowth.One of these patients, mentioned earlier, with only residualrim enhancement within the stalk, experienced regrowth ofthe remnant. This patient (Case 12) had a particularly ag-gressive tumor and underwent repeated endoscopic EEAtwice, successfully treating visual symptoms, followed bystereotactic radiosurgery. The patient’s tumor has respond-ed to radiosurgery and was noted to be decreasing at lastfollow-up. Three other patients had regrowth of a knownremnant. All 3 were recurrent prior to EEA. The patients inCases 5 and 11 experienced regrowth and were treated en-donasally, and the patient in Case 7 underwent a secondresection via a craniotomy due to growth lateral to the mid-dle cerebral artery. The advantage to the endonasal ap-proach lies in treating tumors that are medial to neurovas-
J. Neurosurg. / Volume 109 / July 2008
Outcomes following EEA for resection of craniopharyngiomas
9
FIG. 1. Humphrey visual field tests. A: Preoperative study demonstrating a dense temporal defect. B: Postoperativevisual field testing showing resolution of visual deficit.

cular structures, thus allowing resection without traversingthese structures. This advantage was negated in this situa-tion, making an endonasal approach impractical. This pa-tient eventually died (3 years after EEA) secondary to com-plications associated with stereotactic cyst treatment.
Postoperative Complications
The most common complication in this series was post-operative CSF leak. There were 11 CSF leaks (58%) dur-ing 19 total operations (including 3 reoperations for re-currence/regrowth; 69% not including reoperations) (Table5). Lumbar drain diversion in the immediate postoperativeperiod is used in all cases requiring extensive arachnoiddissection or ventricular transgression. One leak resolvedwith lumbar drainage alone, and 10 leaks were managedwith reexploration and repair. Long-term CSF diversionwas required in 6 (40%) of 15 patients who had lumbarpuncture–proven chronic elevation in ICP. Another patientdeveloped delayed visual decline postoperatively becauseof documented hydrocephalus. This condition resolved tothe immediate postoperative, improved state after shunttreatment.
The overall shunt placement rate was 7 (44%) of 16, anddespite CSF leaks there were no cases of bacterial menin-
gitis. Shunt treatment was not used as a primary modal-ity for CSF leak repair. Rather, it was used as an adjuvantin those patients with recurrent leakage and documented(lumbar puncture) increase in ICP.
Several tumors were closely associated with or attachedto posterior and anterior circulation arteries. During onesuch case, a PCA (P1) perforating vessel was injured. Copi-ous irrigation with the aid of a ventriculostomy catheter in-serted into the naris revealed the site of arterial avulsion,and a successful repair/closure was achieved using hemo-static agent (Syvek marine polymer [off-label use]) withgentle compression. The patient did suffer a small thalam-ic infarction from this arterial injury with resultant aphasia,but fortunately has recovered well with minimal residualaphasia. The overall vascular injury rate for all surgeries8
was 5% (1 of 19). The rate of permanent neurological def-icit is the same (same patient).
No patient died during or as a result of surgery or duringthe 30-day postoperative period. As mentioned earlier, 1patient died following a stereotactic cyst treatment 3 yearsafter EEA. One patient died of complications of anticoagu-lation therapy (acute subdural hematoma, distant from thesite of surgery) 2 months following surgery. Another pa-tient died of an unrelated medical condition ~ 2 years aftersurgery.
P. A. Gardner et al.
10 J. Neurosurg. / Volume 109 / July 2008
FIG. 2. Humphrey visual field tests. A: Preoperative study showing dense bilateral defects, greatest bitemporally. B:Postoperative study performed in the same patient demonstrating significant improvement compared with preoperativetesting.

Discussion
Although small, this series demonstrates the potential ofthe purely endoscopic EEA as another aid in the treatmentof suprasellar craniopharyngiomas. The addition and soleuse of the endoscope in the expanded, microscopic ap-proaches described by others17,20,25 allows improved visual-ization, which, in turn, allows the further expansion of thepreviously described approaches.
Craniopharyngiomas are notoriously difficult to cure, butcomplete resection has been shown to provide a survivalbenefit.1,3–5,8,16,27,33,34 Complete resection rates reported in theliterature range from 6 to 0%,3,5,6,12,13,24,26,27,31,32,34–36 with theexception of the study by Yasargil et al.,36 in which the au-thors reported a 90% gross-total resection rate (at the costof a 16.7% mortality rate). Our small series of suprasellartumors has a 73% gross-total resection rate for tumors in-tended for complete resection (50% for the overall series).The series’ size limits direct comparisons; however, thusfar, the rates of resection compared with historical case se-ries do seem to be equivalent or better. Even more diffi-cult to quantify is the patient’s quality of life followingtumor resection. Although the aim in most cases is com-plete resection and cure, there is a greater potential forsome decrement in the patient’s function, whether neu-rological, ophthalmological, or endocrinological, followingradical surgery. In our study, all patients were function-al postoperatively. Indeed, only 1 patient suffered a decre-ment in function (the patient with a PCA branch infarct).This resulted in a significant aphasia that recovered overthe course of a year. This patient is living independently athome. In this series, the extent of resection was evaluatedusing an emphasis on an intent-to-treat analysis; only thosetumors in which complete resection was the goal based onclinical factors were used in the analysis. Han et al.11 havepreviously reported on surgical cohorts using this type ofintention-to-treat analysis.
No patient who underwent a gross-total resection experi-enced recurrence. The regrowth rate for the series is 25%(9% for those intended for complete resection). It is worthnoting that all patients in our series who suffered recurrenceor regrowth were patients with Type II (transinfundibular)tumors (Table 4), which grow and presumably originatefrom within the infundibulum. These tumors are perhaps
J. Neurosurg. / Volume 109 / July 2008
Outcomes following EEA for resection of craniopharyngiomas
11
TABLE 3Endocrine results*
Posterior Pituitary Function (DI)Anterior Pituitary Function
Case Postop/ PermanentNo. Preop Deficit Postop Deficit (long term) Preop DI Transient DI Postop DI
1 none panhypopitism (except ACTH) no yes yes2 none panhypopitism no yes no3 panhypopituitarism no change no no no4 none none no yes no5 none none yes† NA NA6 panhypopituitarism panhypopituitarism no no no7 hypothyroidism & hypogonadism no change no no no8 panhypopituitarism no change yes† NA NA9 GH & thyroid axis deficits normal no no no
10 IGF-I deficit & TSH elevation continued hypothyroidism, Hashimoto no yes nothyroiditis & papillary carcinomadiagnosed
11 hypothyroidism, borderline adrenal in- hypothyroid & adrenal insufficiency no no nosufficiency
12 hypothyroidism, adrenal insufficiency no change yes NA NA13 hypogonadism, borderline adrenal in- 1-mo FU (hypothyroidism at discharge), no yes NA; 1-mo FU (DI
sufficiency lost to FU at discharge)14 panhypopituitarism no change no no no15 panhypopituitarism no change no yes no16 thyroid & testosterone deficiencies no change no no no
* ACTH = adrenocorticotropic hormone; FU = follow-up; IGF-I = insulin-like growth factor–I; NA = not applicable.† The DI was present following a prior craniotomy.
TABLE 4Extent of resection
Vol (cm3)Case % Resection FUNo. Preop Postop (solid & cystic portion) (mos)
1 1.6 0.0 100.0 822 3.7 0.0 100.0 593 9.7 0.0 100.0 524 5.8 3.2 44.3*; cyst progression 485 2.5 0.1† 96.0†; regrowth* 456 8.3 0.0 100.0 437 12.0 3.0 75.0; regrowth* 368 6.6 0.0 100.0 219 7.2 0.3 (residual rim enhance- 95.8 37
ment w/in stalk)10 4.3 0.0 100.0 3311 6.8 2.0 69.8; regrowth 1512 4.3 0.4 (residual enhancement 90.7; regrowth 29.5
w/in stalk)13 51.5 18.3 64.5* 214 14.1 0.3 97.9* 1015 4.3 0.0 100.0 1816 7.5 0.0 100.0 10
* Complete resection not planned.† Small separate enhancing nodule in the lateral wall of the third ventricle
not resected.

P. A. Gardner et al.
12 J. Neurosurg. / Volume 109 / July 2008
FIG. 3. Preoperative (left) and postoperative (right) coronal MR images showing suprasellar, Type II (infundibular) cra-niopharyngioma treated using a stalk-sparing resection. The enhancement seen under the chiasm has not progressed dur-ing follow-up (see text on recurrence).
FIG. 4. Contrast-enhanced T1-weighted MR images. Preoperative sagittal (A) and coronal (B) images showing a com-plex craniopharyngioma with suprasellar extension. Postoperative sagittal (C) and coronal (D) images showing gross-totalresection.

J. Neurosurg. / Volume 109 / July 2008
Outcomes following EEA for resection of craniopharyngiomas
13
FIG. 5. Contrast-enhanced T1-weighted MR images. Preoperative sagittal (A) and coronal (B) images showing a giant,complex craniopharyngioma, with extension into the third and lateral ventricles in an elderly man with vision loss. Post-operative sagittal (C) and coronal (D) images showing debulking of this giant tumor. Debulking was chosen due to the pa-tient’s advanced age and concern over potential hypothalamic and thalamic injury with aggressive resection.
FIG. 6. Coronal contrast-enhanced T1-weighted MR images. Left: Preoperative image showing a suprasellar cranio-pharyngioma with a separate nodule (arrow) in the lateral wall of the third ventricle. Resection of the nodule was notplanned as the floor of the third ventricle appeared intact on preoperative imaging. In retrospect and with further experi-ence, perhaps this nodule would have been accessible. Right: Postoperative image obtained in the same patient showingresection of the suprasellar tumor, with the third ventricular nodular residual lesion (arrow).

the most difficult to cure surgically (3 of the 4 in this studyhad been previously resected). In all of these cases, an at-tempt was made to preserve the stalk, with resultant preser-vation of existing endocrine function.13 Although this wassuccessful, in the future, it may be wiser to merely sacrificethe stalk in those cases in which there is no other remnant.Although certain to provide worse endocrine outcomes, inthe long term, this practice may benefit the patient by re-ducing recurrence rates.28
As an initial evaluation of the endoscopic EEA tech-nique, this series shows it to be effective in chiasmal de-compression. Although published studies have reportedrates of postoperative visual decline ranging from 2 to15%,5,6,26,32,34,35 there were no such occurrences in this series.Furthermore, the likelihood of improvement in or completerecovery of vision was 92%.
In terms of endocrinopathy, panhypopituitarism and DIare particularly common following the resection of cranio-pharyngiomas; rates in the literature have ranged from 24to 66% and 43 to 79%,6,31,34–36 respectively. In our series,18% of patients developed panhypopituitarism and 8% de-veloped permanent DI.
Perhaps most surprising is the high rate of panhypopitu-itarism following resection of Type I tumors. This may bedue to the fact that both Type I tumors without preoperativedysfunction were resected early (first) in the series. There-fore, it is difficult to know if this finding is a result of tumorlocation or a reflection of our learning curve. In contrast,Type III tumors had a very low rate of dysfunction (1[20%] of 5).
The aggressiveness of resection obviously has a signifi-cant effect on the aforementioned rates. This small series,however, appears to support the use of purely endoscopictechniques to provide a high rate of endocrine functionpreservation, while concurrently achieving respectable re-
sections. This is especially true for Types I (preinfundibu-lar) and III (retroinfundibular) tumors, where the stalk canbe separated and potentially preserved. In this series, this isillustrated by Type III tumors, where there was a very lowrate of postoperative pituitary dysfunction. Although thereare only a few patients in whom complete resection withpreservation of current hormonal status can be achieved (2in this series, both with Type III tumors), we believe thatan attempt at preservation of pituitary gland and stalk isreasonable and at times successful. Given the tumor typeand locations, some degree of postoperative pituitary dys-function is expected and preservation of function must beweighed against the recurrence risk. Once again, this is em-phasized by Type II tumors, in which the tumor has ofteninvaded the pituitary stalk. This problem illustrates the dif-ficulty in dealing with such a pathological entity.
Our experience with EEA resection of craniopharyngio-mas has demonstrated the need for new techniques that pre-vent postoperative CSF leaks. Leakage rates were higherin this series than in our experience with other sellar andsuprasellar lesions, and there are several reasons for this.One is the extensive, intentional violation of the anteriorskull base dura that is necessary for lesion access. This larg-er opening is more difficult to effectively seal, and its prox-imity to critical neurovascular structures (carotid arteries,optic nerves, and so on) increases the challenge of obtain-ing a watertight repair.
Of particular interest has been our realization that despitesimilar size exposures for other anterior skull base and para-sellar pathological entities such as pituitary adenomas andmeningiomas, craniopharyngiomas have a disproportion-ately higher incidence of CSF leakage following surgery.7,18
This increased rate may be related to a higher incidence ofeither transient or permanent hydrocephalus associated withcraniopharyngiomas.5,12,36 This is also reflected in the high
P. A. Gardner et al.
14 J. Neurosurg. / Volume 109 / July 2008
TABLE 5Surgical complications*
Case No. Complication Treatment Result
1 none NA NA2 CSF leak reexploration resolution3 CSF leak reexploration/VP shunt resolution4 delayed CSF leak w/ HCP reexploration/VP shunt resolution5 none NA NA6 CSF leak w/ chemical meningitis, re- reexploration, awaiting reop resolution
currence7 postop HCP/cyst chiasm compression VP shunt improvement
(delayed vision deficit)8 none NA NA9 PCA/P1 injury (avulsion) w/ resultant therapy & brief rehab hospital stay, antico- recovered except trace dysarthria &
partial lt thalamic CVA, DVT, de- agulants, reexploration twice/VP shunt facial droop, no sequelae, resolu-layed CSF leak w/ HCP tion
10 CSF leak LD only resolution11 CSF leak reexploration/VP shunt resolution12 CSF leak, recurrence reexploration/VP shunt, resection twice resolution
(1/05 & 5/05) w/o postop CSF leak,GKS
13 CSF leak, DVT reexploration/VP shunt, IVC filter, resolved, then died of SDH while anticoagulation taking anticoagulants
14 none NA NA15 CSF leak reexploration/LD placed resolved16 CSF leak reexploration resolved
* CVA = cerebrovascular accident; DVT = deep venous thrombosis; HCP = hydrocephalus; IVC = inferior vena cava; LD = lumbardrain; rehab = rehabilitation; SDH = subdural hematoma.

rate of permanent CSF diversion demonstrated in this se-ries. Given the early and often ineffective reconstructiontechniques used in this series, any increased ICP, whethertransient or permanent, was detrimental. However, the mostimportant differentiating factor for increased CSF leakageis likely that resection of craniopharyngiomas, more thanother parasellar lesions, involves the violation of arachnoidcisterns and offers entry into the third ventricle. This viola-tion inevitably creates a greater obstacle to defect closure.Further modification of closure techniques will hopefullyprovide reduction in the CSF leakage rate, as has been thecase after changes instituted later in this series. Throughconstant modification, the CSF leakage rates decreasedconsiderably over the course of this study (Fig. 7). From1998 to 2004, the leakage rate was 69%. The following yearit was reduced to 20% (including the reoperations for tumorregrowth in this group, not listed in Table 5), once suturingand balloon buttresses were used. The recent addition of avascularized, nasal septal flap9 to our reconstructions ap-pears to hold tremendous promise.
It is important to note that all CSF fistulas were eventu-ally sealed without associated morbidity. This result wasassociated with a high permanent CSF diversion rate in thisseries. There were no cases of bacterial meningitis and nocomplications associated with reoperation or shunt place-ment, although the potential for serious complication clear-ly exists. With careful management and awareness of thisissue, CSF leakage is not believed to be an insurmountableproblem and does not negate the efficacy of this approachfor craniopharyngioma.
As for vascular injury, perhaps the most feared compli-cation of endoscopic manipulation of neurovascular struc-tures, our rate of injury was low (5%). Just as importantwas the ability to successfully manage an arterial injuryduring a purely endoscopic endonasal approach.
Conclusions
The incorporation of the transplanum modification intotraditional transsphenoidal approaches, facilitated by theuse of the endoscope, has provided access to many tumorswith suprasellar or even retrochiasmatic extension, pre-viously thought to be unresectable via a transsphenoidalroute. Craniopharyngioma is one such tumor. In our opin-ion, the use of the endoscope as the sole means of visual-ization in the EEA provides surgeons improved visualiza-tion of a region inherently fraught with potential disasterand helps to expand the indications for transsphenoidalresection of sellar region tumors in general and craniopha-ryngiomas in particular.
Comparison of our results with those previously de-scribed is best left to others. Hopefully, however, these datawill help guide the future development of endoscopic tech-niques. This series illustrates the ability to access complexsuprasellar, parasellar, and retrosellar craniopharyngiomasvia an EEA, regardless of the degree of sellar expansion.Difficulties with preventing postoperative CSF leakageare highlighted by this series. Together with standard ap-proaches and other technological advances such as ste-reotactic cyst therapies and radiosurgery, the endoscopicEEA may prove a valuable weapon in the armamentariumagainst this truly challenging tumor. Expansion of the se-
ries, both in terms of number of patients and period of fol-low-up is critical for complete and accurate evaluation ofthe approach and technique.
References
1. Chakrabarti I, Amar AP, Couldwell W, Weiss MH: Long-termneurological, visual, and endocrine outcomes following transna-sal resection of craniopharyngioma. J Neurosurg 102:650–657,2005
2. Couldwell WT, Weiss MH, Rabb C, Liu JK, Apfelbaum RI, Fuku-shima T: Variations on the standard transsphenoidal approach tothe sellar region, with emphasis on the extended approaches andparasellar approaches: surgical experience in 105 cases. Neuro-surgery 55:539–547, 2004
3. De Vile CJ, Grant DB, Kendall BE, Neville BG, Stanhope R, Wat-kins KE, et al: Management of childhood craniopharyngioma: canthe morbidity of radical surgery be predicted? J Neurosurg 85:73–81, 1996
4. Dhellemmes P, Vinchon M: Radical resection for craniopharyn-giomas in children: surgical technique and clinical results. J Pedi-atr Endocrinol Metab 19 (1 Suppl):329–335, 2006
5. Duff JM, Meyer FB, Ilstrup DM, Laws ER, Schleck CD, Scheit-hauer BW: Long-term outcomes for surgically resected cranio-pharyngiomas. Neurosurgery 46:291–302, 2000
6. Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M: Sur-gical treatment of craniopharyngiomas: experience with 168 pa-tients. J Neurosurg 90:237–250, 1999
7. Frank G, Pasquini E, Doglietto F, Mazzatenta D, Sciarretta V, Far-neti G, et al: The endoscopic extended transsphenoidal approachfor craniopharyngiomas. Neurosurgery 59 (1 Suppl):ONS75–ONS83, 2006
8. Gupta DK, Ojha BK, Sarkar C, Mahapatra AK, Sharma BS, Meh-ta VS: Recurrence in pediatric craniopharyngiomas: analysis ofclinical and histological features. Childs Nerv Syst 22:50–55,2006
9. Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A,Snyderman CH, et al: A novel reconstructive technique followingendoscopic expanded endonasal approaches: vascular pedicle na-soseptal flap. Laryngoscope 116:1881–1885, 2006
10. Halves E, Bushe KA: Transsphenoidal operation on craniopharyn-giomas with extrasellar extensions. The advantage of the operat-ing endoscope. Acta Neurochir Suppl (Wien) 28:362, 1979
11. Han PP, Ponce FA, Spetzler RF: Intention-to-treat analysis ofSpetzler-Martin grades IV and V arteriovenous malformations:
J. Neurosurg. / Volume 109 / July 2008
Outcomes following EEA for resection of craniopharyngiomas
15
FIG. 7. Bar graph illustrating CSF leakage rates early in the seriescompared with the last year of the series. The time periods are mis-leading, as only 1 case of CSF leakage occurred prior to 2003, mak-ing this comparison largely one of 2003–2004 and 2005.

P. A. Gardner et al.
16 J. Neurosurg. / Volume 109 / July 2008
natural history and treatment paradigm. J Neurosurg 98:3–7,2003
12. Hoffman HJ, DeSilva M, Humphreys RP, Drake JM, Smith ML,Blaser SI: Aggressive management of craniopharyngiomas inchildren. J Neurosurg 76:47–52, 1992
13. Honegger J, Buchfelder M, Fahlbusch R: Surgical treatment ofcraniopharyngiomas: endocrinological results. J Neurosurg 90:251–257, 1999
14. Honegger J, Buchfelder M, Fahlbusch R, Daubler B, Dorr HG:Transsphenoidal microsurgery for craniopharyngioma. Surg Neu-rol 37:189–196, 1992
15. Im SH, Wang KC, Kim SK, Chung YN, Kim HS, Lee CH, et al:Transsphenoidal microsurgery for pediatric craniopharyngioma:special considerations regarding indications and method. PediatrNeurosurg 39:97–103, 2003
16. Isaac MA, Hahn SS, Kim JA, Bogart JA, Chung CT: Managementof craniopharyngioma. Cancer J 7:516–520, 2001
17. Kaptain GJ, Vincent DA, Sheehan JP, Laws ER Jr: Transsphe-noidal approaches for the extracapsular resection of midline su-prasellar and anterior cranial base lesions. Neurosurgery 49:94–100, 2001
18. Kassam AB, Carrau RL, Snyderman CH, Gardner P, Mintz A:Evolution of reconstructive techniques following endoscopic ex-panded endonasal approaches. Neurosurg Focus 19(1):E8, 2005
19. Kassam AB, Gardner PA, Snyderman CH, Carrau RL, Mintz AH,Prevedello DM: Expanded endonasal approach, a fully endoscop-ic transnasal approach for the resection of midline suprasellar cra-niopharyngiomas: a new classification based on the infundibulum.J Neurosurg 108:715–728, 2008
20. Kouri JG, Chen MY, Watson JC, Oldfield EH: Resection of supra-sellar tumors by using a modified transsphenoidal approach. Re-port of four cases. J Neurosurg 92:1028–1035, 2000
21. Laws ER Jr: Comment on: Surgical treatment of craniopharyngio-mas: an evaluation of the transsphenoidal and pterional approach-es. Neurosurgery 36:724, 1995
22. Laws ER Jr: Transsphenoidal microsurgery in the management ofcraniopharyngioma. J Neurosurg 52:661–666, 1980
23. Laws ER Jr: Transsphenoidal removal of craniopharyngioma. Pe-diatr Neurosurg 21:57–63, 1994
24. Maira G, Anile C, Rossi GF, Colosimo C: Surgical treatment ofcraniopharyngiomas: an evaluation of the transsphenoidal andpterional approaches. Neurosurgery 36:715–724, 1995
25. Mason RB, Nieman LK, Doppman JL, Oldfield EH: Selectiveexcision of adenomas originating in or extending into the pituitarystalk with preservation of function. J Neurosurg 87:343–351,1997
26. Matson DD, Crigler JF Jr: Radical treatment of craniopharyngi-oma. Ann Surg 152:699–704, 1960
27. McMurry FG, Hardy RW, Dohn DF, Sadar E, Gardner J: Longterm results in the management of craniopharyngiomas. Neuro-surgery 1:238–241, 1977
28. Minamida Y, Mikami T, Hashi K, Houkin K: Surgical manage-ment of the recurrence and regrowth of craniopharyngiomas. JNeurosurg 103:224–232, 2005
29. Norris JS, Pavaresh M, Afshar F: Primary transsphenoidal micro-surgery in the treatment of craniopharyngiomas. Br J Neurosurg12:305–312, 1998
30. Patterson RH: Comment on: Surgical treatment of craniopharyn-giomas: an evaluation of the transsphenoidal and pterional ap-proaches. Neurosurgery 36:724, 1995
31. Shirane R, Su C, Kusaka Y, Jokura H, Yoshimoto T: Surgical out-comes in 31 patients with craniopharyngiomas extending outsidethe suprasellar cistern: an evaluation of the frontobasal approach.J Neurosurg 96:704–712, 2002
32. Symon L: An approach to radical excision of craniopharyngiomaby the temporal route. Pediatr Neurosurg 21 (1 Suppl):64–68,1994
33. Tena-Suck ML, Salinas-Lara C, Arce-Arellano RI, Rembao-Bo-jórquez D, Morales-Espinosa D, Sotelo J, et al: Clinico-patholog-ical and immunohistochemical characteristics associated to recur-rence/regrowth of craniopharyngiomas. Clin Neurol Neurosurg108:661–669, 2006
34. Van Effenterre R, Boch AL: Craniopharyngioma in adults andchildren: a study of 122 surgical cases. J Neurosurg 97:3–11,2002
35. Weiner HL, Wisoff JH, Rosenberg ME, Kupersmith MJ, CohenH, Zagzag D, et al: Craniopharyngiomas: a clinicopathologicalanalysis of factors predictive of recurrence and functional out-come. Neurosurgery 35:1001–1011, 1994
36. Yasargil MG, Circic M, Kis M, Siegenthaler G, Teddy PJ, Roth P:Total removal of craniopharyngiomas: approaches and long-termresults in 144 patients. J Neurosurg 73:3–11, 1990
Manuscript submitted October 26, 2006.Accepted June 6, 2007.Sources of support: none reported.Address correspondence to: Amin Kassam, M.D., Department
of Neurological Surgery, Suite B-400, Presbyterian University Hos-pital, 200 Lothrop Street, Pittsburgh, Pennsylvania 15213. email:[email protected].