outcomes of topography-guided versus wavefront … of topography-guided versus wavefront-optimized...
TRANSCRIPT

ARTICLE
Q
Pub
1302
Outcomes of topography-guided versuswavefront-optimized laser in situ
keratomileusis for myopia in virgin eyesArun Kumar Jain, MD, DNB, Chintan Malhotra, MS, Anand Pasari, MS, Pawan Kumar, BSc,
Majid Moshirfar, MD
2016 A
lished
PURPOSE: To compare the outcomes of topography-guided and wavefront-optimized treatment inpatients having laser in situ keratomileusis (LASIK) for myopia.
SETTING: Advanced Eye Centre, Post Graduate Institute of Medical Education and Research, Chan-digarh, India.
DESIGN: Prospective contralateral-eye case study.
METHODS: Patients had topography-guided LASIK in 1 eye and wavefront-optimized LASIK in thecontralateral eye using the Customized Refractive Surgery Master software and Mel 80 excimerlaser. Refractive (residual manifest refraction spherical equivalent [MRSE], higher-orderaberrations [HOAs]), and visual (uncorrected distance visual acuity [UDVA] and photopic andmesopic contrast sensitivity) outcomes were prospectively analyzed 6 months postoperatively.
RESULTS: The study comprised 35 patients. The UDVA was 0.0 logMAR or better and the postop-erative residual MRSE was G0.50 diopter in 94.29% of eyes in the topography-guided group and85.71% of eyes in the wavefront-optimized group (P Z .09). More eyes in the topography-guidedgroup than in the wavefront-optimized group had a UDVA of �0.1 logMAR or better(P Z .04). Topography-guided LASIK was associated with less deterioration of mesopic contrastsensitivity at higher spatial frequencies (12 cycles per degree [cpd] and 18 cpd) and loweramounts of induced coma (P Z .04) and spherical aberration (P Z .04). Less stromal tissuewas ablated in the topography-guided group (mean 61.57 mm G 16.23 [SD]) than in thewavefront-optimized group (mean 79.71 G 14.81 mm) (P < .001).
CONCLUSION: Although topography-guided LASIK and wavefront-optimized LASIK gave excellentresults, topography-guided LASIK was associated with better contrast sensitivity, lower induction ofHOAs, and a smaller amount of tissue ablation.
Financial Disclosure: None of the authors has a financial or proprietary interest in any material ormethod mentioned.
J Cataract Refract Surg 2016; 42:1302–1311 Q 2016 ASCRS and ESCRS
Because of its efficacy and safety, laser in situ kerato-mileusis (LASIK) is one of the most popular proced-ures for the correction of refractive errors. However,there has always been a subset of patients who remaindissatisfied postoperatively because of side effectssuch as glare, halos, starbursts and reduced contrastsensitivity.1,2 This has been attributed in part to theablation profile of conventional LASIK, which causessignificant induction of positive spherical aberrationand other higher-order aberrations (HOAs).3,4 Thesein turn are known to be associatedwith a deterioration
SCRS and ESCRS
by Elsevier Inc.
in the point-spread function and modulation transferfunction of the eye, manifesting clinically as a deterio-ration in visual quality.5
Different ablation profiles have been developedover the years in an attempt to overcome theseundesirable postoperative symptoms. These includewavefront-optimized, wavefront-guided, and topo-graphy-guided ablation profiles.6 The wavefront-optimized profile is designed to limit the inductionof a positive spherical aberration without specificallytargeting the preexisting patterns of HOAs in the
http://dx.doi.org/10.1016/j.jcrs.2016.06.035
0886-3350

1303TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
eye by delivering an increased number of laserpulses to the corneal periphery rather than the center,which helps maintain the prolate shape of corneapostoperatively.7 The topography-guided ablationalgorithm, in addition to treating spherocylindricrefractive errors (ie, the lower-order aberrations[LOAs]), addresses the irregularities of the cornealelevation in an effort to reshape the cornea into anideal curve and achieve a planar wavefront postoper-atively.8 Unlike the wavefront-guided profiles, thetopography-guided ablation profiles do not attemptto correct the aberrations arising from the crystallinelens or other ocular structures. Although traditionallytopographic treatments have been used to treat irreg-ular corneas,9–13 studies have also documented theirsafety and efficacy in the treatment of primary myopiaand astigmatism.14–19
All these ablation profiles have been widely used inrefractive procedures; however, no treatment algo-rithm has shown definite clinical superiority overothers with regard to visual acuity and correction ofLOAs.7 The lack of direct comparisons betweenwavefront-optimized and topography-guided treat-ment using the Mel 80 excimer laser (Carl Zeiss Med-itec AG) and the paucity of contralateral-eye studiesprompted this prospective study to compare the effi-cacy and safety of the more commonly performedwavefront-optimized ablation profile with thetopography-guided ablation profile for the treatmentof myopia or myopic astigmatism in virgin eyes hav-ing LASIK.
PATIENTS AND METHODS
This prospective comparative contralateral-eye studyincluded patients having LASIK for the correction of myopiaor myopic astigmatism at the Cornea and Refractive
Submitted: December 11, 2015.Final revision submitted: May 24, 2016.Accepted: June 29, 2016.
From the Advanced Eye Centre (Jain, Malhotra, Parasi, Kumar),Post Graduate Institute of Medical Education and Research, Chan-digarh, India; the Department of Ophthalmology (Moshirfar), Fran-cis I. Proctor Foundation, University of California San Francisco,San Francisco, California, USA.
Presented in part at the ASCRS Symposium on Cataract, IOL andRefractive Surgery, San Diego, California, USA, April 2015, andthe VII World Cornea Congress, San Diego, California, USA,April 2015.
Corresponding author: Arun Kumar Jain, MD, DNB, Room No 110,Advanced Eye Centre, Post Graduate Institute of Medical Educationand Research, Sector 12, Chandigarh 160012, India. E-mail:[email protected].
J CATARACT REFRACT SURG - V
Services, Advanced Eye Centre, Post Graduate Institute ofMedical Education andResearch (PGIMER), Chandigarh, In-dia, between July 2013 and February 2014. Patients wereenrolled after signing an informed consent form. The studywas approved by the Institutional Review Board of PGIMERand adhered to the tenets of Declaration of Helsinki.
For randomization, a coin toss was used to determine thetreatment algorithm for the right eye of each patient;wavefront-optimized treatment was performed if the tosswas a heads up, and topography-guided treatment was per-formed if the toss resulted in a tails up. The left eye had theopposite treatment algorithm.
Inclusion criteria for the studywere age 18 years to 35 years,stable refractive error with �0.50 to �6.00 diopters (D) ofspherical myopia, astigmatism between 0.00 D and 3.50 D,maximum manifest spherical equivalent of �6.00 D,and distance visual acuity correctable to 0.0 logMAR or better.Exclusion criteria were presence of significant dry eye, ante-rior segment abnormalities (ie, cataracts, corneal scarring, orneovascularization within 1.0 mm of intended ablationzone), basement membrane disease, history of recurrentcorneal erosions, progressive or unstable myopia, estimatedpostoperative residual stromal bed thickness of less than250 mm, established or forme fruste keratoconus, macular orretinal disease, current use of systemic corticosteroid orimmunosuppressive therapy, autoimmune disease, collagenvascular disease, diabetes mellitus, pregnancy, and lactation.
The preoperative examination for each patient includeduncorrected distance visual acuity (UDVA) using a standardSnellen eye chart, corrected distance visual acuity (CDVA)(with spectacles), manifest refraction, cycloplegic refrac-tion with cyclopentolate 1.0%, postmydriatic testing atleast 72 hours after cycloplegic refraction, intraocular pres-sure measurements, slitlamp biomicroscopy of the anteriorsegment, dilated fundus evaluation, Scheimpflug imagingwith the Pentacam HR device (Oculus Surgical, Inc.), com-bined corneal topography and corneal wavefront analysiswith the Atlas 9000 corneal topographer (Carl Zeiss MeditecAG), whole-eye wavefront analysis with the Wasca wave-front aberration–supported cornea ablation aberrometer(Carl Zeiss Meditec AG), and contrast sensitivity measure-ments (performed unioculary under photopic and mesopicconditions) with the Functional Vision Analyzer (Stereo Op-tical Co., Inc.). Contact lens users were asked to discontinuelenswear 2weeks before screening for soft contact lenses and6 weeks before screening for rigid gas-permeable contactlenses. Manifest refraction and wavefront measurementswere repeated at 2 visits to ensure refractive stability.
Eligible patients were scheduled for simultaneous bilateralLASIK, wavefront-optimized in 1 eye and topography-guided in the contralateral eye. The correction target wasbased on the manifest refraction, with emmetropia being thetarget in all patients. An Intralase FS 150Hz femtosecond laser(AbbottMedical Optics, Inc.) was used for flap creation and anMel 80 excimer laser for ablation in all eyes. The same surgeon(A.K.J.) performed all the LASIK procedures. The flap diam-eter varied from 8.5 to 9.5 mm, with a programmed thicknessbetween 90 mm and 110 mm.
Postoperatively, the patients were examined at 1 day,1 week, 1 month, 3 months, and 6 months. All postoperativefollow-up visits included measurement of UDVA, CDVA (ifindicated), wavefront aberration–supported cornea ablationaberrometry, corneal topography using the same topographeras preoperatively, and the Functional Acuity Contrast Test(FACT).
OL 42, SEPTEMBER 2016

1304 TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
Device Technology
Customized Refractive Surgery Master software (CarlZeiss Meditec AG) was locally networked with the Atlastopographer (which uses Placido disk technology) and theWasca wavefront aberration–supported cornea ablationanalyzer (a high-resolution Hartmann-Shack aberrometer),thus enabling integration of topographic and wavefrontdata. With this setup, aspheric spherocylindrical refractiveablations (wavefront-optimized ablations) are generated us-ing manifest refraction values entered manually. Twoaspheric profiles are available. One is designed to reducethe ablation depth in borderline corneas, and the other isoptimized for asphericity. The corneal topography–basedablation algorithms use topographic and corneal elevationdata and can be applied in the followingways: (1) as a purelytopographic smoothening algorithm for conditions such assmall optic zones, decentered ablations, or irregular astigma-tism, where the aim is to correct the corneal irregularitywithout targeting the spherocylindrical error (the limit forthe asymmetric ablation being 50 mm), or (2) as a topographicrefractive algorithm, which simultaneously corrects therefractive error and also smoothens the cornea, thus target-ing maintenance of corneal asphericity and minimal induc-tion of HOAs.
Except for the 2 treatment algorithms (ie, wavefront-optimized or topography-guided) no nomogram correctionwas performed for either arm of the study, the rationale be-ing that nomogram adjustment is required for treatinghighly irregular corneas, for which the topography-smooth ablation profile is used first to normalize the corneawithout targeting the LOAs of sphere and cylinder. How-ever, this ablation itself induces changes in LOAs andhence necessitates nomogram adjustment. Because virginmyopic eyes without significant corneal irregularitieswere included in the present study, no additional nomo-gram adjustment was performed.
Statistical Analysis
The continuous data are presented as the mean G SD orthe median and interquartile range, as appropriate. Thenormality of quantitative data was checked by measuresof Kolmogorov-Smirnov tests. The Mann-Whitney U testwas used for statistical analysis of skewed continuous vari-ables. For normally distributed data, the t test was used tocompare the 2 treatment groups. For time-related andrepeated measures of HOAs, 1-way analysis of variance fol-lowed by Bonferroni correction for multiple comparisonswere used. The qualitative or categorical variables weredescribed as frequencies and proportions. The proportionswere compared using the chi-square or Fisher exact test,whichever was applicable. A P value less than 0.05 wasconsidered to indicate statistical significance. All calcula-tions were performed using SPSS software (version 20,SPSS, Inc.).
RESULTS
The study comprised 35 patients (70 eyes; 35 ineach treatment group). Table 1 compares the pre-operative and intraoperative parameters betweenthe wavefront-optimized group and the topo-graphy-guided group.
J CATARACT REFRACT SURG - V
Refractive and Visual Outcomes
Figure 1 shows the refractive and visual outcomes inthe topography-guided group and Figure 2, in thewavefront-optimized group.
Efficacy
Both procedures were equally efficacious at the endof the 6-month follow-up, with a mean efficacy index(ratio of postoperative decimal UDVA to preoperativedecimal CDVA) of 1.013G 0.12 (SD) in the wavefront-optimized group and 1.053 G 0.11 in the topography-guided group (P Z .151). Thirty-three eyes (94.3%) inthe topography-guided group and 30 eyes (85.71%) inthe wavefront-optimized group had a UDVA of0.0 logMAR (20/20) or better (P Z .09) at the end of6 months. A significantly greater proportion of eyesin the topography-guided group (10 eyes [28.57%])than the wavefront-optimized group (5 eyes[14.29%]) had a UDVA better than 0.1 logMAR(20/16) (P Z .04).
Safety
The 2 ablation profiles had similar safety profiles.The mean safety index (ratio of mean preoperativedecimal CDVA to mean postoperative decimalCDVA) at 6 months was 1.054 G 0.09 in thewavefront-optimized group and 1.089 G 0.10 in thetopography-guided group (P Z .128). No patient ineither group had lost lines of CDVA at the end of6 months. The CDVA was 0.0 logMAR or better inall eyes in each group.
Predictability
The mean manifest refraction spherical equivalent(MRSE) 6 months postoperatively was �0.17 G 0.38 D(range �1.12 to 0.62 D) and 0.02 G 0.29 D(range �0.87 to 1.00 D) in the wavefront-optimizedgroup and topography-guided group, respectively(PZ .022). Both ablation profiles had similar predictabil-ity for MRSE within G1.0 D of emmetropia (P Z .15)and for MRSE withinG0.5 D of emmetropia (PZ .09).
Stability
Stability was similar in the 2 groups, with 4 eyes(11.42%) in the wavefront-optimized group and2 eyes (5.71%) in the topography-guided group havinganMRSE change ofmore than 0.5 D from 3 to 6monthspostoperatively (P Z .22).
Higher-Order Aberrations
Preoperatively, ocular (whole-eye) HOAs andcorneal HOAs at a 6.0 mm pupil diameter were com-parable between the 2 groups (Table 2). At 6 months,
OL 42, SEPTEMBER 2016

Table 1. Between-group comparison of preoperative characteristics and intraoperative parameters.
Parameter
Mean G SD
P ValueWFO Group (n Z 35) TG Group (n Z 35)
Sphere (D) �3.98 G 1.24 �4.19 G 1.30 .600Cylinder (D) �0.29 G 0.42 �0.30 G 0.38 .596MRSE (D) �3.89 G 1.85 �4.19 G 1.92 .817Pachymetry (mm) 542.20 G 23.86 540.70 G 25.38 .955Flat keratometry (D) 43.49 G 2.41 43.39 G 1.48 .404Steep keratometry (D) 44.02 G 1.58 43.82 G 1.52 .482Optical zone (mm) 6.21 G 0.15 6.28 G 0.14 .109Ablation depth (mm) 79.71 G 14.81 61.57 G 16.23 !.001*RSB (mm) 361.46 G 31.46 373.69 G 34.27 .125
MRSE Z manifest refraction spherical equivalent; RSB Z residual stromal bed; TG Z topography-guided; WFO Z wavefront-optimized*Statistically significant (P ! .05)
1305TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
there was a statistically significant induction ofa majority of the ocular HOAs (wavefront aberra-tion–supported cornea ablation aberrometry),including total HOA, coma, and spherical aber-ration, in both groups when compared with thepreoperative values (Table 3). Topography-guidedablation induced significantly lower coma(P Z .043) and spherical aberrations (P Z .04) than
Figure 1. Refractive and visual outcomes in the topography-guided groupdistance visual acuity; VA Z visual acuity).
J CATARACT REFRACT SURG - V
wavefront-optimized ablation (Table 3). At all time-points when HOAs were measured postoperatively,the majority of the ocular HOAs, including the totalHOA root mean square (RMS), coma, and sphericalaberrations, were lower in the topography-guidedgroup than in the wavefront-optimized group,whereas trefoil was comparable between the2 groups (Figure 3).
(CDVA Z corrected distance visual acuity; UDVA Z uncorrected
OL 42, SEPTEMBER 2016
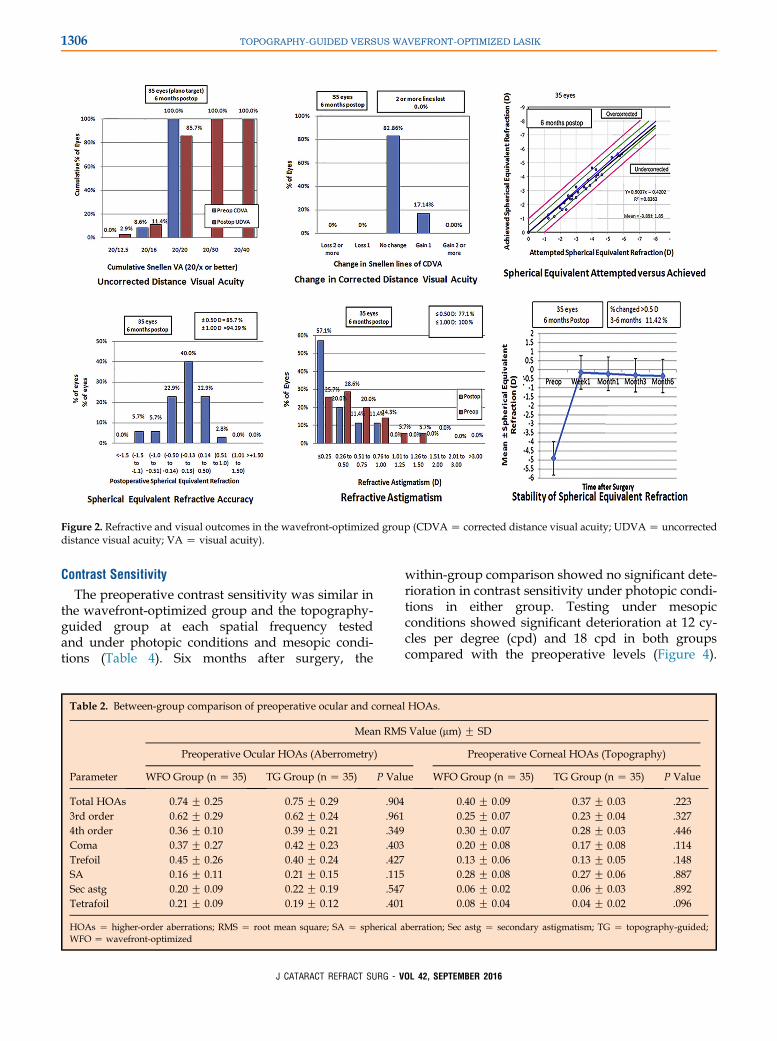
Figure 2. Refractive and visual outcomes in the wavefront-optimized group (CDVAZ corrected distance visual acuity; UDVAZ uncorrecteddistance visual acuity; VA Z visual acuity).
1306 TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
Contrast Sensitivity
The preoperative contrast sensitivity was similar inthe wavefront-optimized group and the topography-guided group at each spatial frequency testedand under photopic conditions and mesopic condi-tions (Table 4). Six months after surgery, the
Table 2. Between-group comparison of preoperative ocular and cornea
Parameter
Mean RMS
Preoperative Ocular HOAs (Aberrometry)
WFO Group (n Z 35) TG Group (n Z 35) P Val
Total HOAs 0.74 G 0.25 0.75 G 0.29 .9043rd order 0.62 G 0.29 0.62 G 0.24 .9614th order 0.36 G 0.10 0.39 G 0.21 .349Coma 0.37 G 0.27 0.42 G 0.23 .403Trefoil 0.45 G 0.26 0.40 G 0.24 .427SA 0.16 G 0.11 0.21 G 0.15 .115Sec astg 0.20 G 0.09 0.22 G 0.19 .547Tetrafoil 0.21 G 0.09 0.19 G 0.12 .401
HOAs Z higher-order aberrations; RMS Z root mean square; SA Z spherical aWFO Z wavefront-optimized
J CATARACT REFRACT SURG - V
within-group comparison showed no significant dete-rioration in contrast sensitivity under photopic condi-tions in either group. Testing under mesopicconditions showed significant deterioration at 12 cy-cles per degree (cpd) and 18 cpd in both groupscompared with the preoperative levels (Figure 4).
l HOAs.
Value (mm) G SD
Preoperative Corneal HOAs (Topography)
ue WFO Group (n Z 35) TG Group (n Z 35) P Value
0.40 G 0.09 0.37 G 0.03 .2230.25 G 0.07 0.23 G 0.04 .3270.30 G 0.07 0.28 G 0.03 .4460.20 G 0.08 0.17 G 0.08 .1140.13 G 0.06 0.13 G 0.05 .1480.28 G 0.08 0.27 G 0.06 .8870.06 G 0.02 0.06 G 0.03 .8920.08 G 0.04 0.04 G 0.02 .096
berration; Sec astg Z secondary astigmatism; TG Z topography-guided;
OL 42, SEPTEMBER 2016

Table 3. Comparison of within-group preoperative and 6-month postoperative ocular HOAs (aberrometry) and between-group compari-sons of magnitude of surgically induced aberrations.
Parameter
Mean RMS Value (mm) G SD
WFO Group TG Group Magnitude of Surgically Induced HOAs
Preop (n Z 35) Postop (n Z 35) P Value Preop (n Z 35) Postop (n Z 35) P Value WFO Group TG Group P Value
Total HOAs 0.74 G 0.25 1.17 G 0.45 .001* 0.75 G 0.29 1.07 G 0.38 .012* 0.43 0.32 .343rd order 0.62 G 0.29 0.97 G 0.41 .004* 0.62 G 0.24 0.88 G 0.39 .029* 0.35 0.26 .464th order 0.36 G 0.10 0.63 G 0.27 !.001* 0.39 G 0.21 0.57 G 0.24 .049* 0.2 0.28 .63Coma 0.37 G 0.27 0.87 G 0.41 !.001* 0.42 G 0.23 0.71 G 0.44 .036* 0.50 0.29 .043*Trefoil 0.45 G 0.26 0.38 G 0.28 .121 0.40 G 0.24 0.35 G 0.33 .466 �0.07 �0.05 .92SA 0.16 G 0.11 0.54 G 0.29 !.001* 0.21 G 0.15 0.48 G 0.27 .001* 0.38 0.27 .04*Sec astg 0.20 G 0.09 0.17 G 0.10 .135 0.22 G 0.19 0.18 G 0.11 .317 �0.03 �0.04 .63Tetrafoil 0.21 G 0.09 0.20 G 0.10 .223 0.19 G 0.12 0.15 G 0.09 .091 �0.01 �0.04 .70
HOAs Z higher order aberrations; RMS Z root mean square; SA Z spherical aberration; Sec astg Z secondary astigmatism; TG Z topography-guided;WFO Z wavefront-optimized*Statistically significant (P ! .05)
1307TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
Intergroup comparison at 6 months showed thatalthough the decrease in postoperative photopiccontrast sensitivity at all tested frequencies was com-parable in the 2 groups, mesopic contrast sensitivity
Figure 3.Comparison of wavefront-optimized LASIK and topography-guidperiod (HOAs Z higher-order aberrations; RMS Z root mean square; TG
J CATARACT REFRACT SURG - V
at the higher spatial frequencies (ie, 12 cpd and18 cpd) had deteriorated significantly less in thetopography-guided group than in the wavefront-optimized group (Figure 5).
ed LASIKwith respect to induced ocular HOAs in the postoperativeZ topography guided; WFO Z wavefront optimized).
OL 42, SEPTEMBER 2016

Table 4. Intergroup comparison of preoperative photopic and mesopic contrast sensitivity on FACT (log units).
Frequency (Cpd)
Photopic Contrast Sensitivity (85 cd/m2) Mesopic Contrast Sensitivity (3 cd/m2)
WFO Group (n Z 35) TG Group (n Z 35) P Value WFO Group (n Z 35) TG Group (n Z 35) P Value
1.5 1.58 1.6 .547 1.57 1.56 .7973.0 1.99 1.97 .547 1.95 1.95 .7326.0 1.93 1.92 .731 1.81 1.82 .86812.0 1.63 1.64 .717 1.43 1.44 .82718.0 0.81 0.8 .697 0.72 0.74 .369
cd Z candelas; Cpd Z cycles per degree; TG Z topography-guided; WFO Z wavefront-optimized
1308 TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
DISCUSSION
Expectations for the outcomes of refractive surgery areincreasing progressively, with patients wanting notonly spectacle independence but also excellent visual
Figure 4. Comparison of preoperative and 6-month postoperativephotopic and mesopic contrast sensitivity in each group(* Z statistically significant [P ! .05]; cpd Z cycles per degree;TG Z topography guided; WFO Z wavefront optimized).
J CATARACT REFRACT SURG - V
quality and increased safety. Attempts to address pre-existing HOAs by wavefront-guided or topography-guided treatments are steps in this direction.
Compared with wavefront measurement withaberrometers, topographic measurements from thecorneal surface can measure more points, includingthose in the corneal periphery, which is where mostof the aberrations lie. Also, corneal topography, unlikewavefront data, is unaffected by factors such as pupilsize, accommodative status of the eye (which itself caninduce some spherical refractive changes and HOAs),and centroid shift or by internal optical componentssuch as early cataract. This makes the topographicallyacquired data a far more stable parameter than thewavefront data. In addition, topographic measure-ments can be used in highly aberrated eyes for whichwavefront data might be unreliable. However, unlikewavefront analyzers, topographers do not provide in-formation about the spherocylindrical refraction of theeye. Hence, topographic refractive treatment algo-rithms should be combined with measurements ob-tained from manifest refraction rather than based on
Figure 5. Comparison of wavefront-optimized LASIK andtopography-guided LASIK with respect to 6-month postoperativephotopic and mesopic contrast sensitivity (* Z statistically signifi-cant [P ! .05]; cpd Z cycles per degree; TG Z topography guided;WFO Z wavefront optimized).
OL 42, SEPTEMBER 2016

1309TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
information acquired by the topographer alone. A po-tential concern with topography-guided treatmentsmight be that treating only the corneal aberrationscould unmask some lenticular HOAs (which in the vir-gin eye are usually balanced byHOAs arising from thecornea up to approximately age 30 years), thus leadingto a less favorable ablation profile with reduced qual-ity of vision postoperatively.
In the present study, the LASIK outcomes in thetopography-guided group were better than or equiva-lent to those in the wavefront-optimized group for thevarious parameters analyzed. The number of patientsachieving a postoperative UDVA of �0.1 logMAR(28.57% in topography-guided group versus 14.29%in wavefront-optimized group; PZ .04) is comparableto the results ofWaring et al.8 in their series of 131 eyeshaving topography-guided LASIK using the NidekCX II custom aspheric treatment zone (CATz) algo-rithm. They found that at �0.1 logMAR or betterlevels, the 6-month postoperative UDVA exceededthe preoperative CDVA in more than 25% of cases. Again of 1 Snellen line of visual acuity over the pre-operative CDVA was also seen in significantly morepatients in the topography-guided group (28.47%)than in the wavefront-optimized group (17.14%) inour series (PZ .04). In a contralateral-eye comparisonof topography-guided versus wavefront-optimizedablation, El Awady et al.15 reported similar results,with 19% of eyes in the topography-guided groupand 12% of eyes in the wavefront-optimized groupgaining 1 line of CDVA.
In our study, predictability was similar between the2 groups, with 94.3% of eyes in the topography-guidedgroup and 85.71% of eyes in the wavefront-optimizedgroup being within G0.5 D of emmetropia (P Z .09).Various studies14,17,20,21 have also reported a postoper-ative MRSE within G0.5 D of emmetropia in 75.0% to96.1% cases after topography-guided ablation. Thislevel of predictability for MRSE within G0.5 D ofmyopia seen with the topography-guided ablation inour series also compares favorably with the results re-ported byKermani et al.17 (76%), Padmanabhan et al.22
(93%), and Moshirfar et al.23 (88%) for wavefront-guided treatments and by Padmanabhan et al.22
(89%) for wavefront-optimized treatments.El Awady et al.,15 in their contralateral-eye compara-
tive study, found that vertical comaandhigher cylindri-cal aberrations were lower in the topography-guidedgroup than in the wavefront-optimized group. In thepresent series, the topography-guided profile inducedsignificantly less coma and spherical aberration thanthe wavefront-optimized profile. Our results oftopography-guided ablation are also similar to thoseof Du et al.,18 who found that HOAs were increased af-ter LASIK regardless of whether the treatment was
J CATARACT REFRACT SURG - V
conventional or topography guided; however, the in-crease in HOAs after topography-guided ablation wasless than that after conventional ablation.
Spatial contrast sensitivity is a sensitive perfor-mance index of the functional quality of vision afterrefractive surgery because it assesses the combined ef-fects of light scattering, optical aberrations, and defo-cus.24 In the present study, a significant drop wasseen under the high-frequency (12 cpd and 18 cpd)mesopic testing conditions in both groups. Ourresults are consistent with those in a study byMont�es-Mic�o et al.,25 which found that LASIK inducedsignificant reductions in contrast sensitivity undermesopic conditions at high spatial frequencies only,even though the photopic contrast sensitivity functionwas normal. However, the deterioration in our serieswas less in the topography-guided group than in thewavefront-optimized group, and the differenceachieved statistical significance. It has been shownpreviously that induced changes in the contrast sensi-tivity function correlate significantly with increases inocular HOAs (especially spherical aberration), whichin turn are affected by the amount of stromal abla-tion.26 In our study, the topography-guided grouphad lower amounts of induced HOAs, includingcoma and spherical aberration, as well as less cornealablation than the wavefront-optimized group, whichmight explain the better contrast sensitivity inthe topography-guided group. In their series oftopography-guided LASIK using the FACT, Dough-erty et al.27 found a slight but significant gain incontrast under photopic and mesopic testing withglare at the lower frequencies (3 cpd and 6 cpd);whereas at 18 cpd under mesopic conditions, their re-sults were similar to those in our study, with a signif-icant drop from the preoperative levels (P Z .03).
Another important outcome in the present studywas that significantly less stromal tissue was ablatedin the topography-guided group than in thewavefront-optimized group (mean 61.57 G 16.23 mmversus 79.71 G 14.81 mm; P ! .001), even though therefractive error to be corrected (ie, the preoperativeMRSE) was slightly higher in the topography-guidedgroup (mean �4.19 G 1.92 D in the topography-guided group versus �3.89 G 1.85 D in thewavefront-optimized group). This finding, if repro-ducible in other studies, could have significant clinicalimplications because saving corneal tissue can helpexpand the pool of candidates eligible for refractivesurgery or the amount of refractive error that can besafely corrected.
Outcomes obtained in the topography-guidedgroup in the present study compare favorably withthe results in the U.S. Food and Drug Administration(FDA)-approved multicenter topography-guided
OL 42, SEPTEMBER 2016
1310 TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
treatment study group.A The postoperativeMRSEwaswithinG0.5 D of plano and a postoperative UDVA of0.0 logMAR or greater and 1 line gain of visual acuityover preoperative CDVA were achieved in 94.29%,94.29%, and 28.57% of patients, respectively, in our se-ries and in 94.8%, 92.6%, and 29.6% of patients, respec-tively, in the FDA trial. That mesopic contrastsensitivity at higher spatial frequencies (12 cpd and18 cpd) deteriorated less in the topography-guidedgroup than the wavefront-optimized group in our se-ries might explain the improvement in visual symp-toms (eg, difficulty in night driving, readingdifficulty, and glare) that occurred in a significantnumber of patients in the postoperative periodcompared with preoperative levels with habitualcorrection in the FDA study.
The better refractive and visual outcomes, lower in-duction of HOAs, and less tissue ablation in thetopography-guided group compared with thewavefront-optimized group might be the outcome ofthe principles on which the Customized RefractiveSurgery Master software topography-guided ablationalgorithm is based. The algorithm uses the cornealwavefront data as well as the corneal elevation datato derive the ablation profile. Corneal regularization(performed to smoothen the subtle corneal irregular-ities present even in otherwise normal eyes) is basedon elevation data. However, the target corneal surfaceis determined by analysis of the corneal wavefrontdata and the clinical manifest refraction. Thetopography-guided ablation profile is thus based onthe individual corneal topography in which the exci-mer laser spots are targeted to flatten the peaks andsteepen the flatter areas by ablating around them.This combined method of simultaneous hyperopicand myopic treatment removes much less tissue andstill maintains the prolate shape of the cornea. In addi-tion, the topography-guided ablation is centered onthe corneal apex rather than the pupil center and hencealso addresses the issue of angle k. Wavefront-optimized ablations, on the other hand, derive theablation pattern from population-based data for thecorrection of myopia and astigmatism and attemptto produce an aspheric profile by delivering morepulses to the peripheral cornea. Thus, wavefront-optimized treatments are not individualized, andthey are associated with more laser pulses leading tomore tissue ablation and possibly with more sourcesof error. This might have caused a greater inductionof HOAs in the postoperative period in eyes havingwavefront-optimized treatment in our series.
There were a few limitations in the present study. Asubjective comparison of postoperative patient satisfac-tion relating to quality of vision and postoperative
J CATARACT REFRACT SURG - V
symptoms such as glare or halos between the 2 eyeswas not performed. Such data would help validatethe objectively measured parameters and more effec-tively establish superiority, or lack thereof, of 1 tech-nique over the other. The eyes were not stratified interms of those having anHOARMS less than or greaterthan 0.3 mm for intergroup comparison, andwe also didnot correlate changes in coma in eyes with a higher cyl-inder with those with a lower cylindrical component.Such stratification was beyond the scope of this study,although it could be a part of future studies. However,a major strength of this study was that because it wasa contralateral-eye study, the confounding effect ofvarying wound healing and biomechanical propertiesof the cornea on the various parameters studied wasavoided because fellow eyes of the same individualwere generally accepted as having similar biomecha-nical characteristics and healing properties.
The results in this study suggest a promising role forthe more widespread use of topography-guided abla-tions in virgin eyes with myopia or myopic astigma-tism. Future studies with a longer follow-up periodmight be useful to determine the effect of factors,such as changing lenticular aberrations, on the visualoutcomes in patients who had topography-guidedLASIK.
OL
WHAT WAS KNOWN
� Topography-guided LASIK, although mainly used for treat-ing irregular corneas, has shown reasonably good visualand refractive outcomes when used as a primary treat-ment for correction of myopia and myopic astigmatismin virgin eyes.
� A previous study that compared wavefront-optimizedLASIK with topography-guided LASIK did not find signifi-cant differences in the induced HOAs and the contrastsensitivity between these 2 groups.
WHAT THIS PAPER ADDS
� Compared to wavefront-optimized LASIK, topography-guided LASIK induced a significantly lower amount ofHOAs, especially coma and spherical aberrations, andwas associated with better contrast sensitivity at high fre-quencies (12 cpd and 18 cpd) under mesopic testingconditions.
� Topography-guided LASIK resulted in significantly lessstromal tissue ablation than wavefront-optimized LASIK.
� Topography-guided LASIK might be safely used as a pri-mary treatment for myopia in virgin eyes as an alternativeto wavefront-optimized LASIK.
42, SEPTEMBER 2016

1311TOPOGRAPHY-GUIDED VERSUS WAVEFRONT-OPTIMIZED LASIK
REFERENCES1. Chalita MR, Chavala S, Xu M, Kreuger RR. Wavefront analysis
in post-LASIK eyes and its correlation with visual symptoms,
refraction, and topography. Ophthalmology 2004; 111:447–453
2. MutyalaS,McDonaldMB,ScheinblumKA,OstrickMD,Brint SF,
Thompson H. Contrast sensitivity evaluation after laser in situ
keratomileusis. Ophthalmology 2000; 107:1864–1867
3. Holladay JT, Janes JA. Topographic changes in corneal aspher-
icity and effective optical zone after laser in situ keratomileusis.
J Cataract Refract Surg 2002; 28:942–947
4. Moreno-Barriuso E, Merayo Lloves J, Marcos S, Navarro R,
Llorente L, Barbero S. Ocular aberrations before and after
myopic corneal refractive surgery: LASIK-induced changes
measured with laser ray tracing. Invest Ophthalmol Vis Sci
2001; 42:1396–1403. Available at: http://iovs.arvojournals.org/
article.aspx?articleidZ2162653. Accessed July 17, 2016
5. Artal P, Navarro R. Monochromatic modulation transfer function
of the human eye for different pupil diameters: an analytical
expression. J Opt Soc Am A Opt Image Sci Vis 1994; 11:246–
249
6. Smadja D, Reggiani-Mello G, Santhiago MR, Krueger RR.
Wavefront ablation profiles in refractive surgery: description, re-
sults, and limitations. J Refract Surg 2012; 28:224–232
7. Mrochen M, Donitzky C, W€ullner C, L€offler J. Wavefront-opti-
mized ablation profiles: theoretical background. J Cataract
Refract Surg 2004; 30:775–785
8. Waring G, Dougherty PJ, Chayet A, Fischer J, Fant B,
Stevens G, Bains HS. Topographically guided LASIK for mopia
using the Nidek CXII customized aspheric treatment zone
(CATz). Trans AmOphthalmol Soc 2007; 105:240–246; discus-
sion 247–248 Available at: http://www.ncbi.nlm.nih.gov/pmc/ar
ticles/PMC2258119/pdf/1545-6110_v105_p240.pdf. Accessed
July 17, 2016
9. Knorz MC, Jendritza B. Topographically-guided laser in situ ker-
atomileusis to treat corneal irregularities. Ophthalmology 2000;
107:1138–1143
10. Lin DY,MancheEE. Custom-contoured ablation patternmethod
for the treatment of decentered laser ablations. J Cataract
Refract Surg 2004; 30:1675–1684
11. Kanellopoulos AJ. Comparison of sequential vs same-day
simultaneous collagen cross-linking and topography-guided
PRK for treatment of keratoconus. J Refract Surg 2009;
25:S812–S818
12. Cosar CB, Acar S. Topography-guided LASIK with the Wave-
Light laser after penetrating keratoplasty. J Refract Surg 2006;
22:716–719
13. Lee D-H, Seo SJ, Shin S-C. Topography-guided excimer laser
ablation of irregular cornea resulting from penetrating injury.
J Cataract Refract Surg 2002; 28:186–188
14. Tan J, Simon D, Mrochen M, Por YM. Clinical results of
topography-based customized ablations for myopia and myopic
astigmatism. J Refract Surg 2012; 28:S829–S836
15. El Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized
ablation versus topography-guided customized ablation in
myopic LASIK: comparative study of higher order aberrations.
Ophthalmic Surg Lasers Imaging 2011; 42:314–320
16. Kanjani N, Jacob S, Agarwal A, Agarwal A, Agarwal S,
Agarwal T, Doshi A, Doshi S. Wavefront- and topography-
guided ablation in myopic eyes using Zyoptix. J Cataract
Refract Surg 2004; 30:398–402
J CATARACT REFRACT SURG - V
17. Kermani O, Schmiedt K, Oberheide U, Gerten G. Topographic-
and wavefront-guided customized ablations with the NIDEK-
EC5000CXII in LASIK for myopia. J Refract Surg 2006;
22:754–763
18. Du C-X, Yang Y-B, Shen Y, Wang Y, Dougherty PJ. Bilateral
comparison of conventional versus topographic-guided custom-
ized ablation for myopic LASIK with the NIDEK EC-5000.
J Refract Surg 2006; 22:642–646
19. Farooqui MA, Al-Muammar AR. Topography-guided CATz
versus conventional LASIK for myopia with the NIDEK EC-
5000: a bilateral eye study. J Refract Surg 2006; 22:741–745
20. Knorz MC, Neuhann T. Treatment of myopia and myopic astig-
matism by customized laser in situ keratomileusis based on
corneal topography. Ophthalmology 2000; 107:2072–2076; dis-
cussion by RS Rubinfeld, 2076
21. Cummings AB, Mascharka N. Outcomes after topography-
based LASIK and LASEKwith theWaveLight Oculyzer and Top-
olyzer platforms. J Refract Surg 2010; 26:478–485
22. Padmanabhan P, Mrochen M, Basuthkar S, Viswanathan D,
Joseph R. Wavefront-guided versus wavefront-optimized laser
in situ keratomileusis: contralateral comparative study.
J Cataract Refract Surg 2008; 34:389–397
23. Moshirfar M, Schliesser JA, Chang JC, Oberg TJ, Mifflin MD,
Townley R, Livingston MK, Kurz CJ. Visual outcomes after
wavefront-guided photorefractive keratectomy and wavefront-
guided laser in situ keratomileusis: prospective comparison.
J Cataract Refract Surg 2010; 36:1336–1343
24. Mont�es-Mic�o R, Charman WN. Choice of spatial frequency for
contrast sensitivity evaluation after corneal refractive surgery.
J Refract Surg 2001; 17:646–651
25. Mont�es-Mic�o R, Espa~na E, Menezo JL. Mesopic contrast sensi-
tivity function after laser in situ keratomileusis. J Refract Surg
2003; 19:353–356
26. Yamane N, Miyata K, Samejima T, Hiraoka T, Kiuchi T,
Okamoto F, Hirohara Y, Mihashi T, Oshika T. Ocular higher-
order aberrations and contrast sensitivity after conventional
laser in situ keratomileusis. Invest Ophthalmol Vis Sci 2004;
45:3986–3990. Available at: http://iovs.arvojournals.org/article.
aspx?articleidZ2124587. Accessed July 17, 2016
27. Dougherty PJ, Waring G III, Chayet A, Fischer J, Fant B,
Bains HS. Topographically guided laser in situ keratomileusis
for myopia using a customized aspherical treatment zone.
J Cataract Refract Surg 2008; 34:1862–1871
OTHER CITED MATERIALA. U.S. Food and Drug Administration. Summary of Safety and
Effectiveness Data [for the ALLEGRETTO WAVE� Eye-Q Ex-
cimer Laser]. PMA P020050/S12, September 27, 2013; page
5. Available at: http://www.accessdata.fda.gov/cdrh_docs/
pdf2/p020050s012b.pdf. Accessed July 17, 2016
OL
42, SEPTEMBER 2016First author:Arun Kumar Jain, MD, DNB
Advanced Eye Centre, Post GraduateInstitute of Medical Education andResearch, Chandigarh, India