outflow tracts’ anomalies - türkiye maternal fetal tıp...
TRANSCRIPT
Pag. 1
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Diagnosis of Outflow Tract Anomalies in the Fetus
General Framing
D.Paladini
Fetal Medicine & Surgery Unit
Gasllini Children’s Hospital - Genoa [email protected]
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Malalignement VSD
Tetralogy of Fallot (TOF)
Pulmonary Atresia + VSD (PAVSD)
Common Arterial Trunk (CAT)
Double Outlet Right Ventricle (DORV)
Complete Transposition of GA (TGA)
[Corrected Transposition of GA (cTGA)]
Critical aortic stenosis
Critical pulmonary stenosis
Pulmonary atresia + intact ventricular septum (PAIVS)
Outflow Tracts’ Anomalies
Pag. 2
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Embriology - looping
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Embriology

Pag. 3
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Embriology
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
All anomalies affecting the splitting
mechanism of the Bulbus Cordis (or Conus) are called Conotruncal Anomalies,
and, as such these share:
a perfectly normal 4-chamber view (in most instances)
Conotruncal Anomalies

Pag. 4
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Axial views of the thorax – 2D
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Categorization of OT abnormalities
Abnormal septo-aortic continuity (malalign. VSD)
TOF, PAVSD, APVS, CAT, DORV
Abnormal crossover (parallel vessels +/- VSD)
TGA, DORV, (cTGA)
Abnormal (obstructed) semilumar valve
Critical aortic/pulmonary stenosis, PAIVS
Pag. 5
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
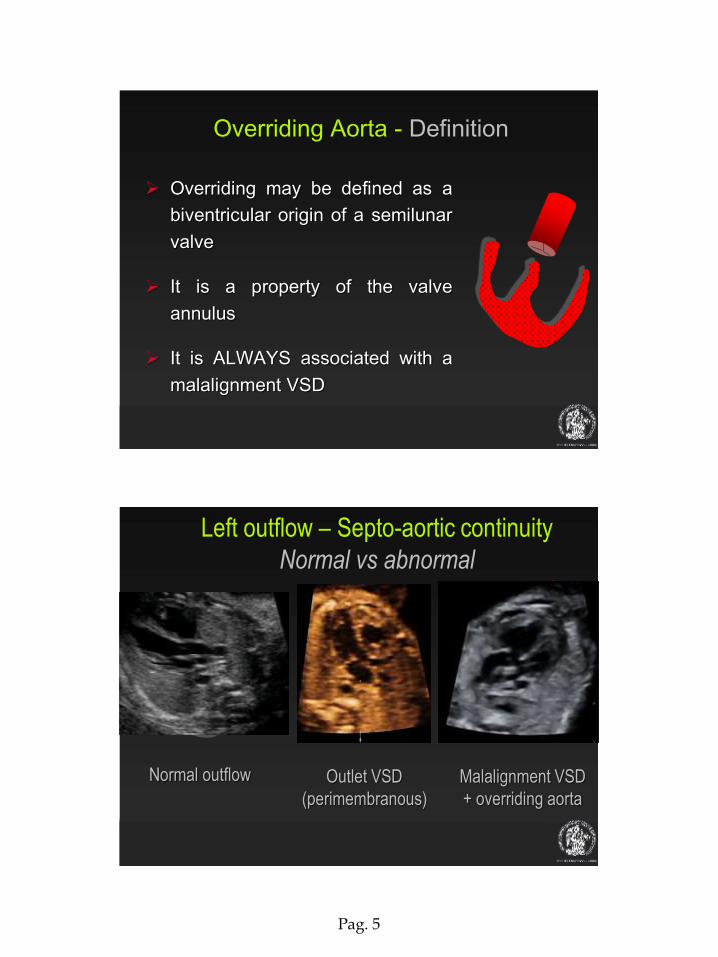
Overriding may be defined as a
biventricular origin of a semilunar
valve
It is a property of the valve
annulus
It is ALWAYS associated with a
malalignment VSD
Overriding Aorta - Definition
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Left outflow – Septo-aortic continuity
Normal vs abnormal
Normal outflow Outlet VSD
(perimembranous)
Malalignment VSD
+ overriding aorta

Pag. 6
Abnormality of the septo-aortic junction
Outlet VSD vs Malalignment VSD
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Left Outflow – Challenges
…sometimes the VSD is missed or
hidden, and the Pa-Ao disproportion is
the most striking feature
Pag. 7
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
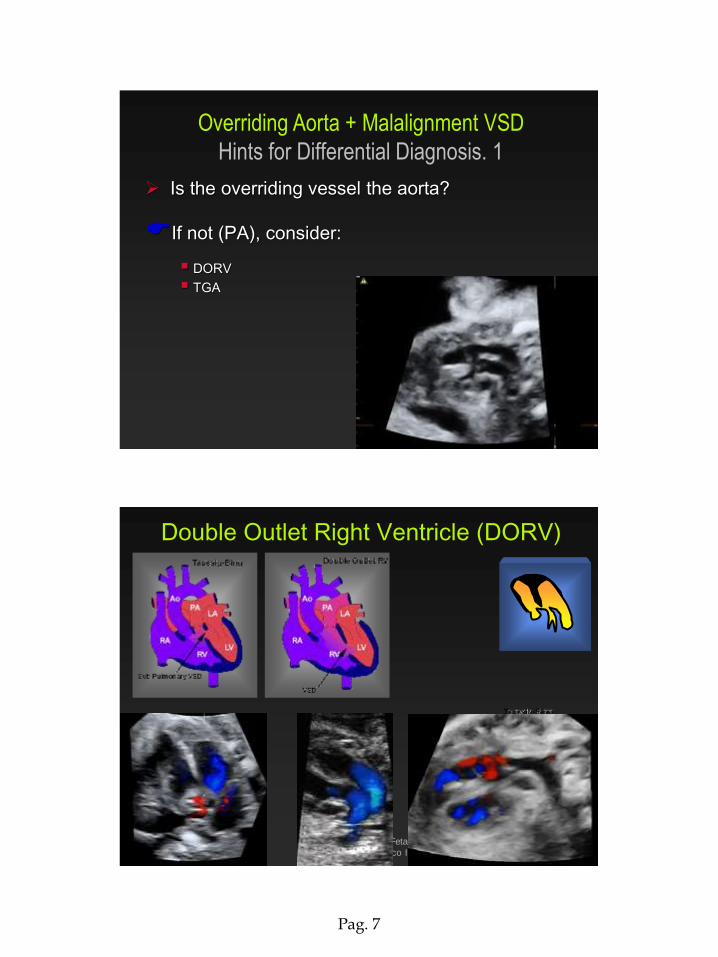
Overriding Aorta + Malalignment VSD
Hints for Differential Diagnosis. 1
Is the overriding vessel the aorta?
If not (PA), consider:
DORV
TGA
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Double Outlet Right Ventricle (DORV)

Pag. 8
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Is the aortic root particularly wide?
If yes, consider:
CAT (common arterial trunk)
PAVSD (pulmonary atresia + VSD)
…all the blood passes through the LV-Ao:
Overriding Aorta + Malalignment VSD
Hints for Differential Diagnosis. 2
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Is the aortic valve dysplastic?
If yes, consider:
CAT (common arterial trunk)
…always dysplastic valve from non-separation of Pa and Ao valves’ cusps (up to 6 cusps)
Overriding Aorta + Malalignment VSD
Hints for Differential Diagnosis. 3
Pag. 9
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
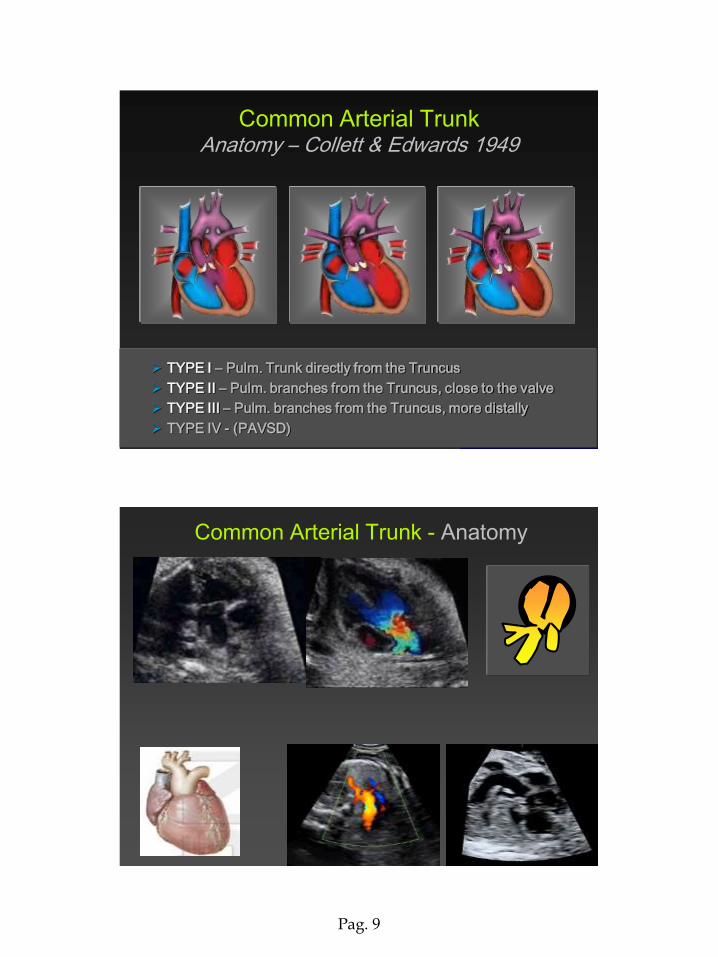
Common Arterial Trunk Anatomy – Collett & Edwards 1949
TYPE I – Pulm. Trunk directly from the Truncus
TYPE II – Pulm. branches from the Truncus, close to the valve
TYPE III – Pulm. branches from the Truncus, more distally
TYPE IV - (PAVSD)
Common Arterial Trunk - Anatomy
Pag. 10
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
I
Common Arterial Trunk - Anatomy
II III
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
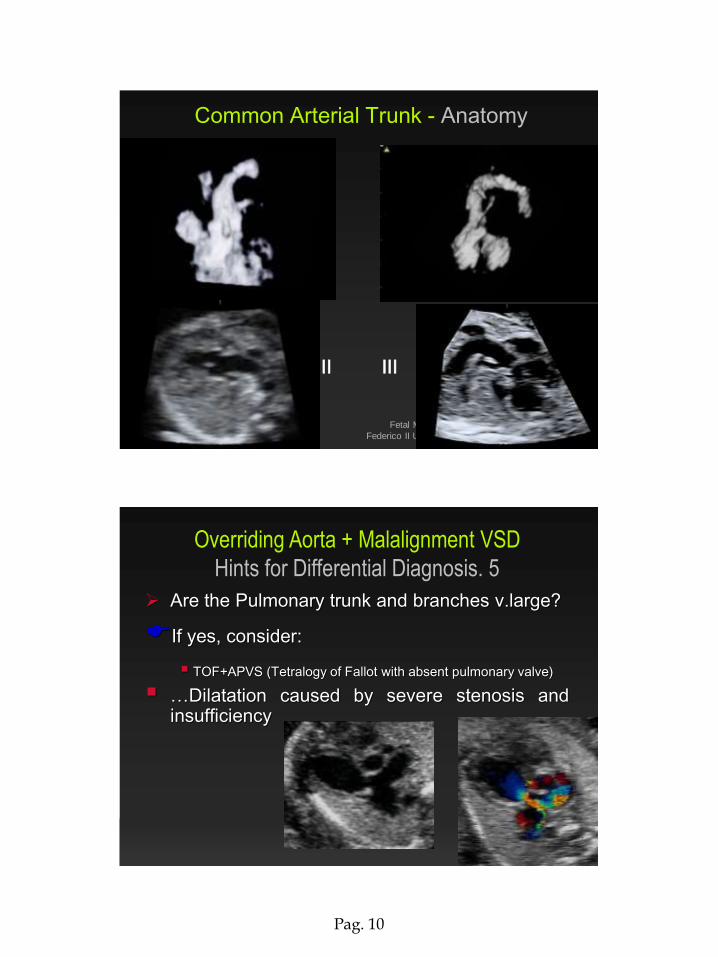
Are the Pulmonary trunk and branches v.large?
If yes, consider:
TOF+APVS (Tetralogy of Fallot with absent pulmonary valve)
…Dilatation caused by severe stenosis and insufficiency
Overriding Aorta + Malalignment VSD
Hints for Differential Diagnosis. 5
Pag. 11
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
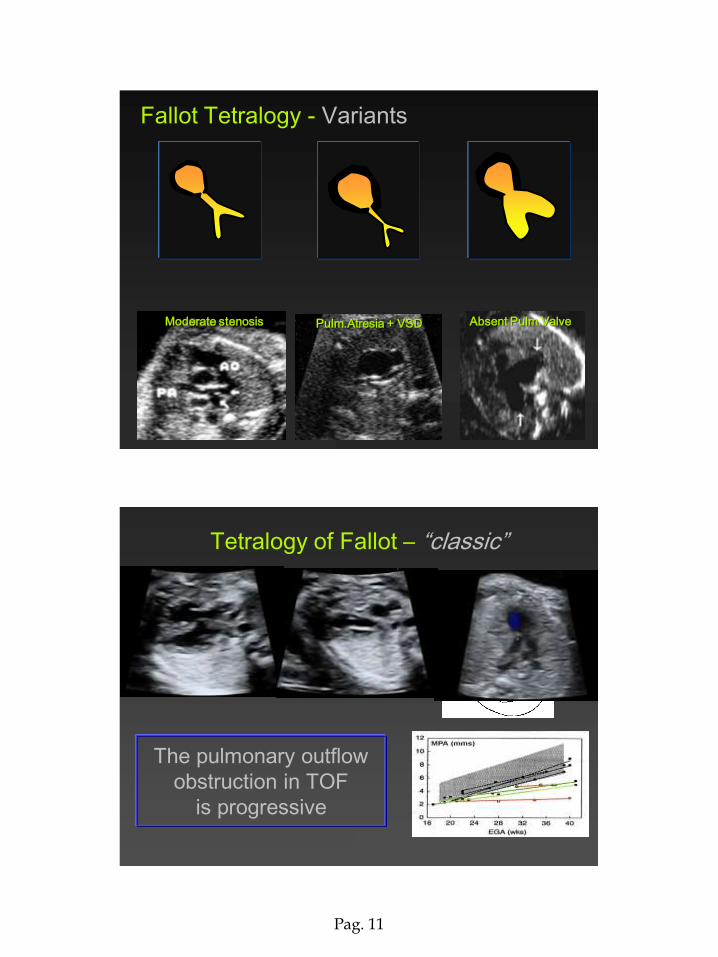
Fallot Tetralogy - Variants
Moderate stenosis Pulm.Atresia + VSD Absent Pulm.Valve
Tetralogy of Fallot – “classic”
The pulmonary outflow
obstruction in TOF
is progressive
Pag. 12
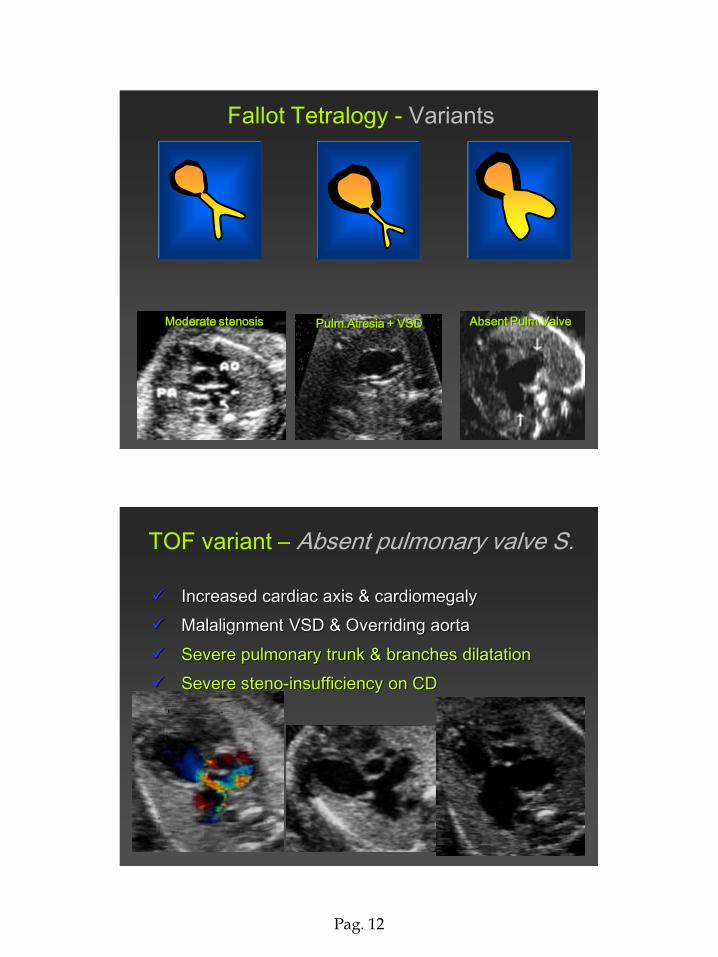
Fallot Tetralogy - Variants
Moderate stenosis Pulm.Atresia + VSD Absent Pulm.Valve
TOF variant – Absent pulmonary valve S.
Increased cardiac axis & cardiomegaly
Malalignment VSD & Overriding aorta
Severe pulmonary trunk & branches dilatation
Severe steno-insufficiency on CD
Pag. 13
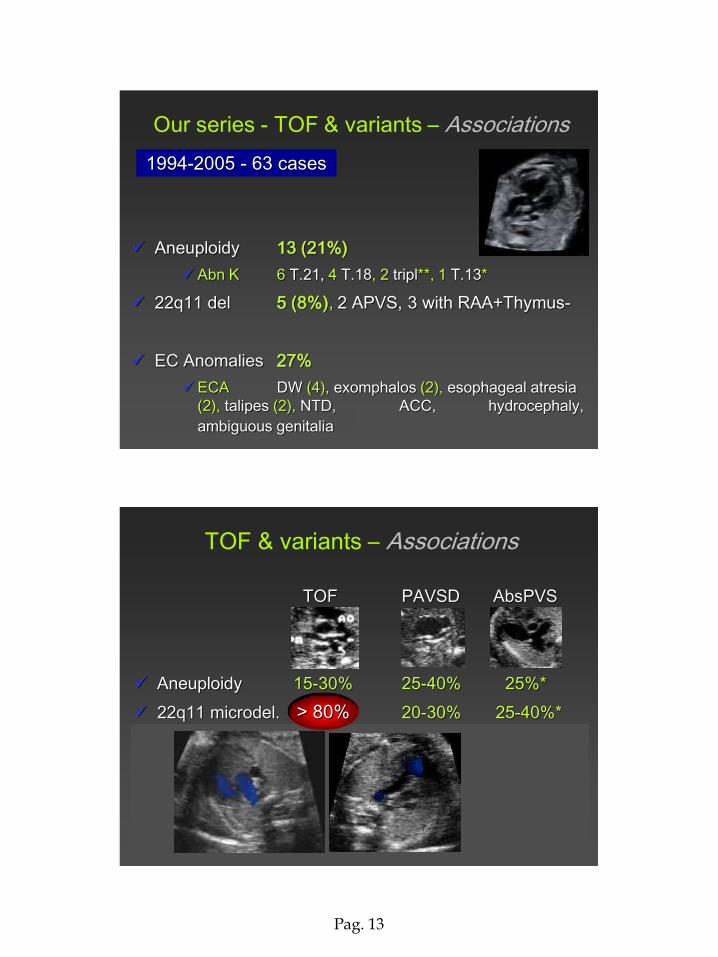
Aneuploidy 13 (21%)
Abn K 6 T.21, 4 T.18, 2 tripl**, 1 T.13*
22q11 del 5 (8%), 2 APVS, 3 with RAA+Thymus-
EC Anomalies 27%
ECA DW (4), exomphalos (2), esophageal atresia
(2), talipes (2), NTD, ACC, hydrocephaly,
ambiguous genitalia
Our series - TOF & variants – Associations
1994-2005 - 63 cases
TOF PAVSD AbsPVS
Aneuploidy 15-30% 25-40% 25%*
22q11 microdel. 6-20% 20-30% 25-40%*
EC Anomalies 10-30% 10-20% 45%*
TOF & variants – Associations
*Volpe P, Paladini D, Marasini M, et al. Characteristics, associations and outcome of
absent pulmonary valve syndrome in the fetus.
Ultrasound Obstet Gynecol, 2005
> 80%
Pag. 14
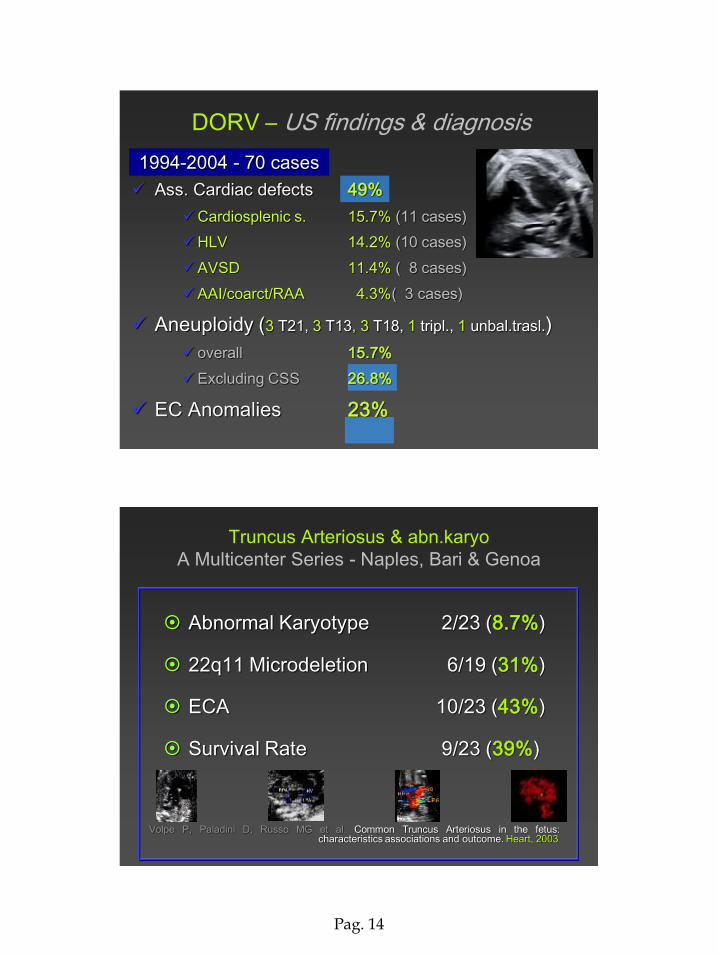
Ass. Cardiac defects 49%
Cardiosplenic s. 15.7% (11 cases)
HLV 14.2% (10 cases)
AVSD 11.4% ( 8 cases)
AAI/coarct/RAA 4.3%( 3 cases)
Aneuploidy (3 T21, 3 T13, 3 T18, 1 tripl., 1 unbal.trasl.)
overall 15.7%
Excluding CSS 26.8%
EC Anomalies 23%
1994-2004 - 70 cases
DORV – US findings & diagnosis
Truncus Arteriosus & abn.karyo
A Multicenter Series - Naples, Bari & Genoa
Abnormal Karyotype 2/23 (8.7%)
22q11 Microdeletion 6/19 (31%)
ECA 10/23 (43%)
Survival Rate 9/23 (39%)
Volpe P, Paladini D, Russo MG et al. Common Truncus Arteriosus in the fetus: characteristics associations and outcome. Heart, 2003
Pag. 15
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
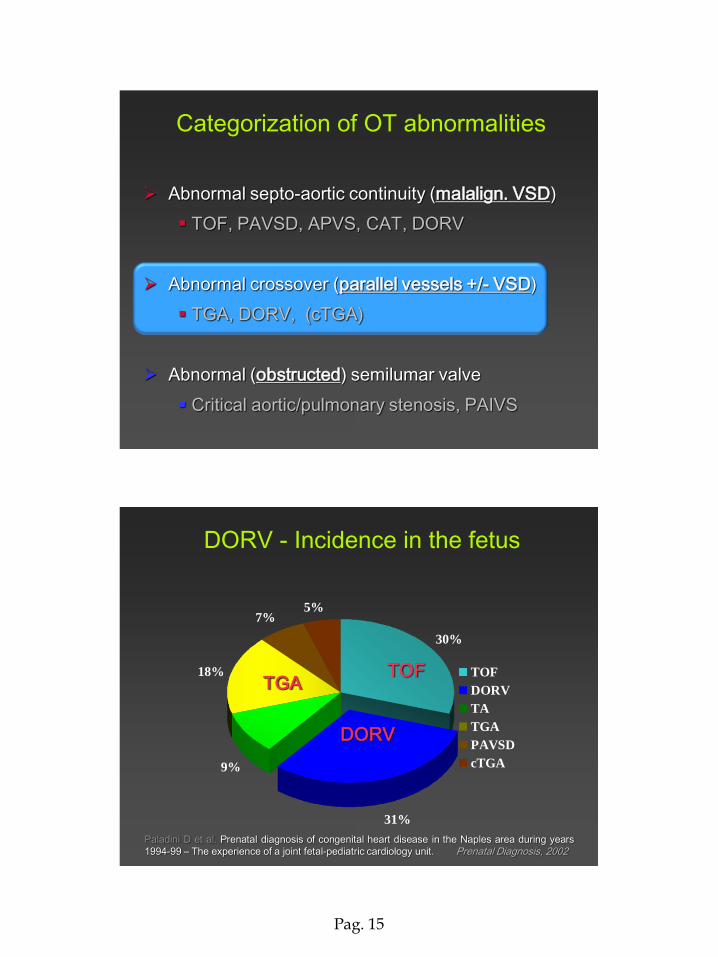
Categorization of OT abnormalities
Abnormal septo-aortic continuity (malalign. VSD)
TOF, PAVSD, APVS, CAT, DORV
Abnormal crossover (parallel vessels +/- VSD)
TGA, DORV, (cTGA)
Abnormal (obstructed) semilumar valve
Critical aortic/pulmonary stenosis, PAIVS
30%
31%
18%
7%5%
9%
TOF
DORV
TA
TGA
PAVSD
cTGA
Paladini D et al. Prenatal diagnosis of congenital heart disease in the Naples area during years
1994-99 – The experience of a joint fetal-pediatric cardiology unit. Prenatal Diagnosis, 2002
TGA TOF
DORV
DORV - Incidence in the fetus
Pag. 16
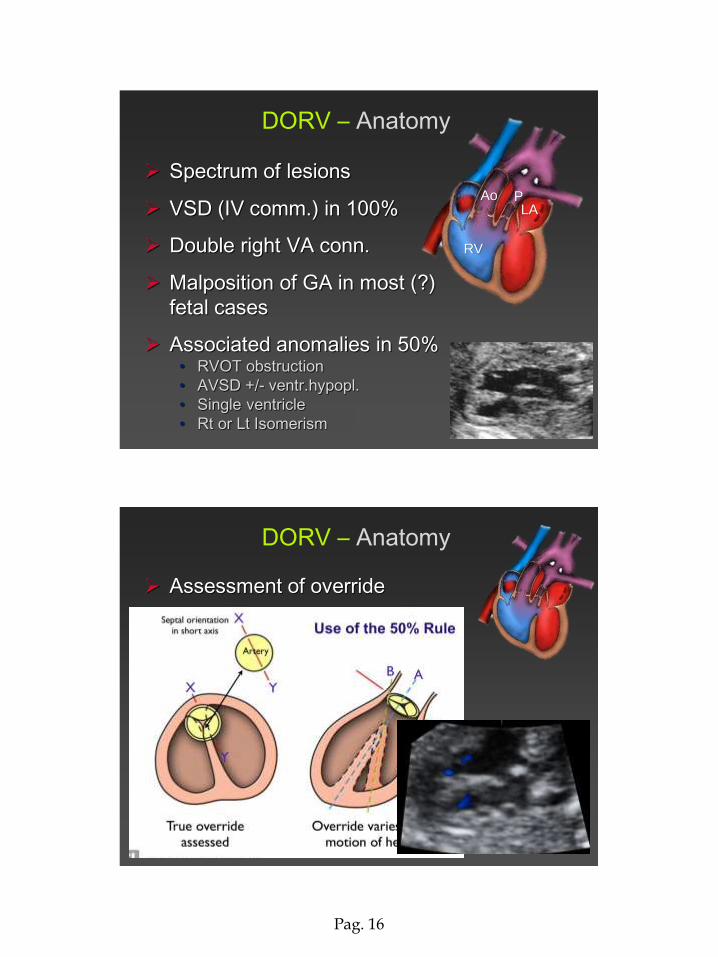
Spectrum of lesions
VSD (IV comm.) in 100%
Double right VA conn.
Malposition of GA in most (?)
fetal cases
Associated anomalies in 50% • RVOT obstruction
• AVSD +/- ventr.hypopl.
• Single ventricle
• Rt or Lt Isomerism
DORV – Anatomy
RV
LA Ao P
Assessment of override
DORV – Anatomy
Pag. 17
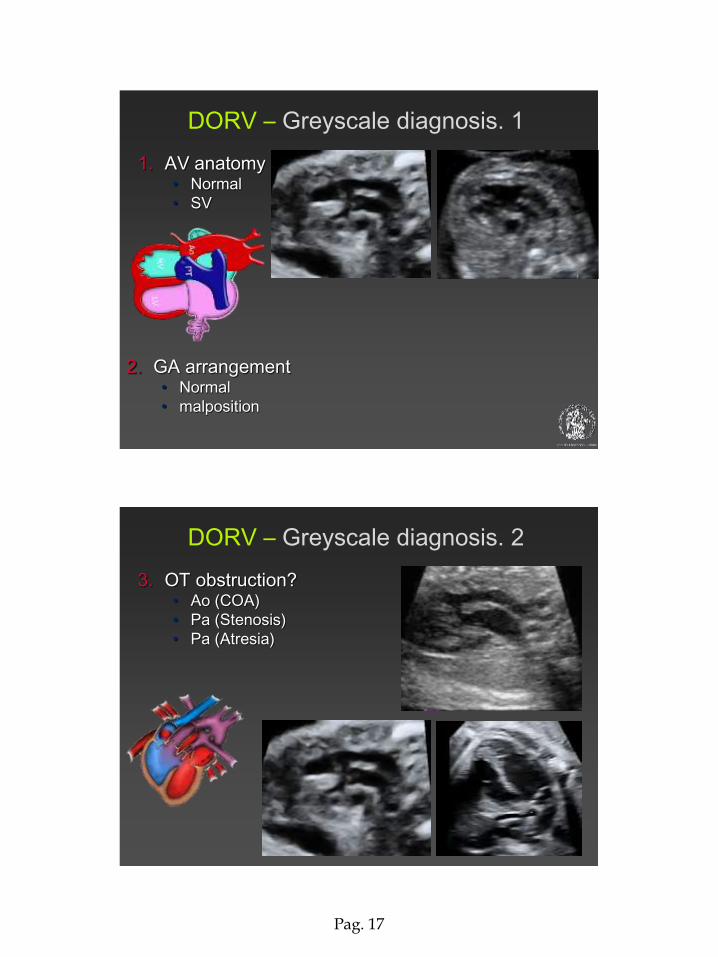
DORV – Greyscale diagnosis. 1
1. AV anatomy • Normal
• SV
2. GA arrangement • Normal
• malposition
DORV – Greyscale diagnosis. 2
3. OT obstruction? • Ao (COA)
• Pa (Stenosis)
• Pa (Atresia)
Pag. 18
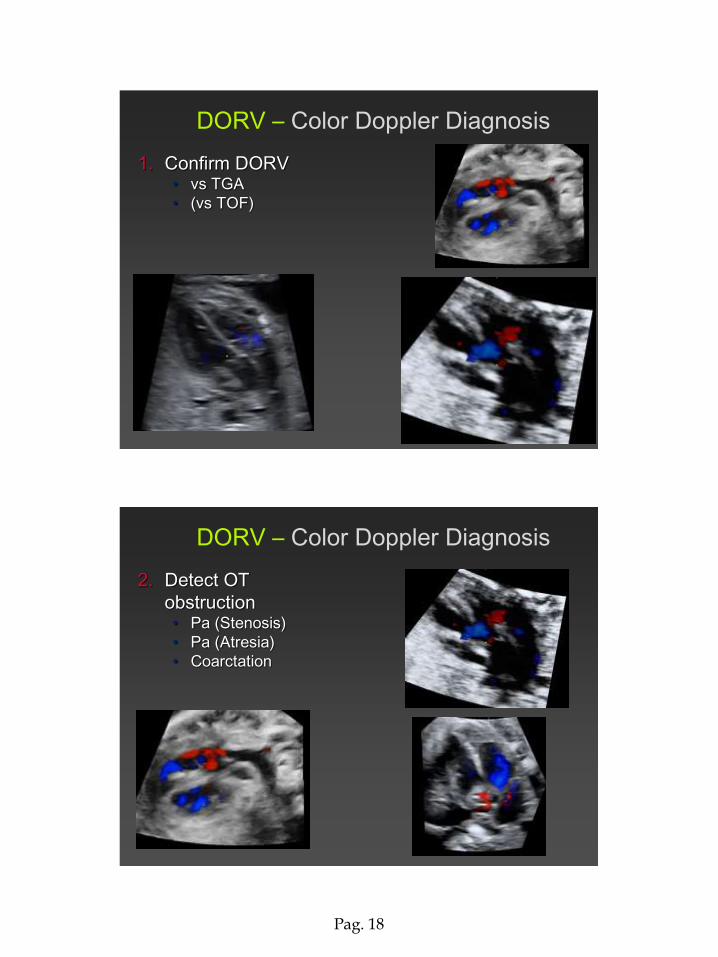
DORV – Color Doppler Diagnosis
1. Confirm DORV • vs TGA
• (vs TOF)
DORV – Color Doppler Diagnosis
2. Detect OT
obstruction • Pa (Stenosis)
• Pa (Atresia)
• Coarctation
Pag. 19
Ass. Cardiac defects 49%
Cardiosplenic s. 15.5%
HLV 14.2%
AVSD 11.4%
AAI/coarct/RAA 4.3%
Aneuploidy (3 T21, 3 T13, 3 T18, 1 tripl., 1 unbal.trasl.)
overall 15.7%
Excluding CSS 26.8%
EC Anomalies 23%
1994-2014 - 85 cases
DORV – US findings & diagnosis
DORV & variants can be diagnosed in utero
DORV can be associated with AVSD, atresias, cardiosplenic syndromes in up to 49% of cases
The aneuploidy & ECA risks is very high (> 20%)
The 22q11 risk is relatively lower for DORV, unless it is associated with RAA
DORV - Conclusions
Fetal Medicine & Surgery Unit
Gasllini Children’s Hospital - Genoa
Pag. 20
Whenever such a conotruncal CHD is
diagnosed in a fetus:
Detailed anatomy scan
Karyotype with G banding
FISH analysis for the 22q11 locus
DORV Management
TOF, DORV & CAT can be diagnosed in utero
DORV can be associated with AVSD, atresias, cardiosplenic syndromes in up to 49% of cases
The aneuploidy & ECA risks are very high for all CHD (> 20%)
The 22q11 risk is very high for PAVSD, CAT and
APVS and/or in all CHD if associated with Right Aortic Arch – lower for DORV
TOF, DORV, CAT
Conclusions
Pag. 21
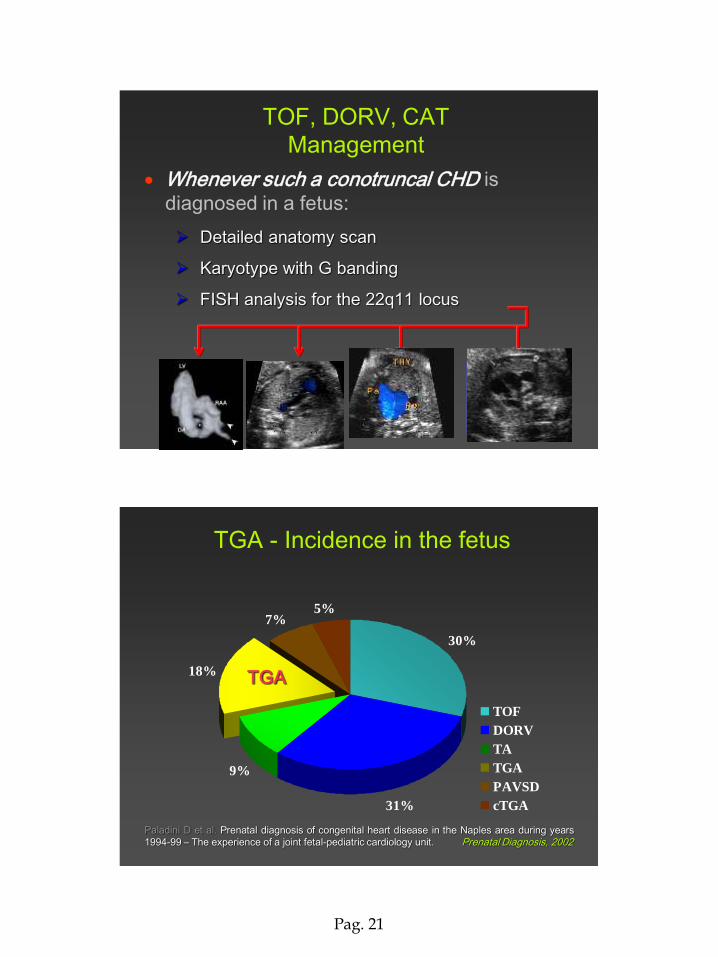
Whenever such a conotruncal CHD is
diagnosed in a fetus:
Detailed anatomy scan
Karyotype with G banding
FISH analysis for the 22q11 locus
TOF, DORV, CAT
Management
TOF +
RAA or
Thymus
PAVSD
also if
isolated
APVS-CAT
also if
isolated
AAI-B also
if isolated
30%
31%
18%
7%5%
9%
TOF
DORV
TA
TGA
PAVSD
cTGA
TGA
TGA - Incidence in the fetus
Paladini D et al. Prenatal diagnosis of congenital heart disease in the Naples area during years
1994-99 – The experience of a joint fetal-pediatric cardiology unit. Prenatal Diagnosis, 2002
Pag. 22
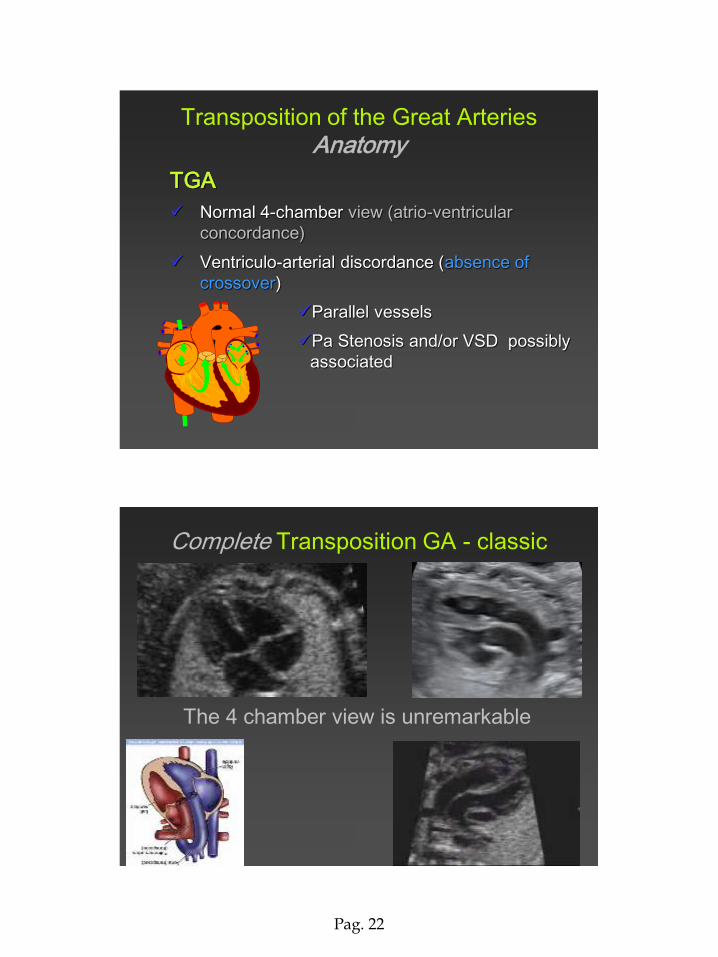
Transposition of the Great Arteries
Anatomy
TGA
Normal 4-chamber view (atrio-ventricular
concordance)
Ventriculo-arterial discordance (absence of
crossover)
Parallel vessels
Pa Stenosis and/or VSD possibly
associated
Complete Transposition GA - classic
The 4 chamber view is unremarkable
Pag. 23
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
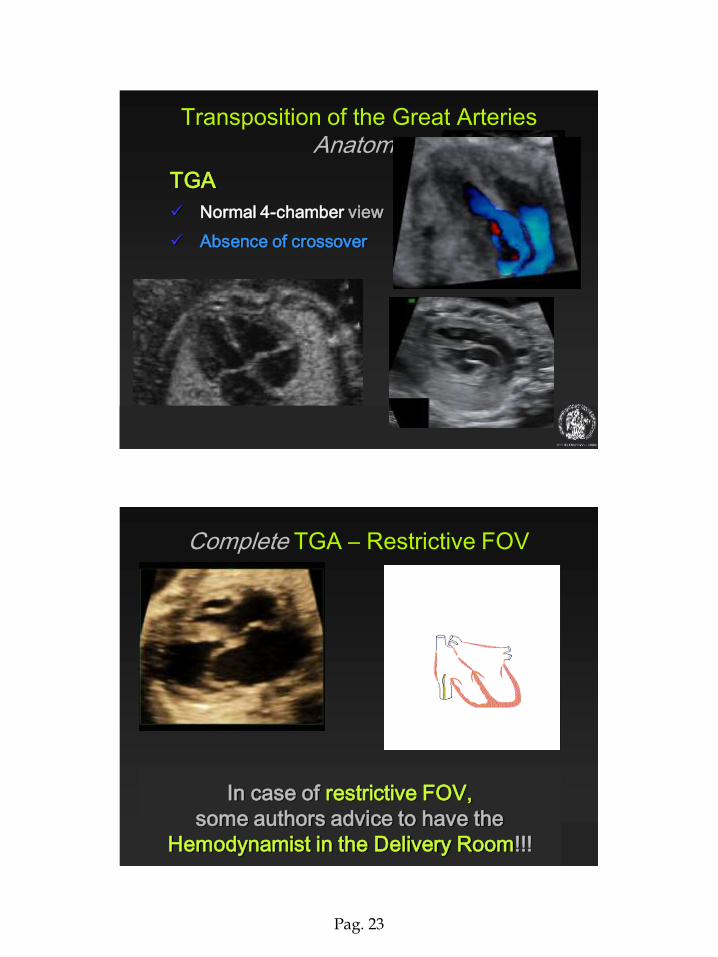
Transposition of the Great Arteries
Anatomy
TGA
Normal 4-chamber view
Absence of crossover
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
Complete TGA – Restrictive FOV
In case of restrictive FOV,
some authors advice to have the
Hemodynamist in the Delivery Room!!!
Pag. 24
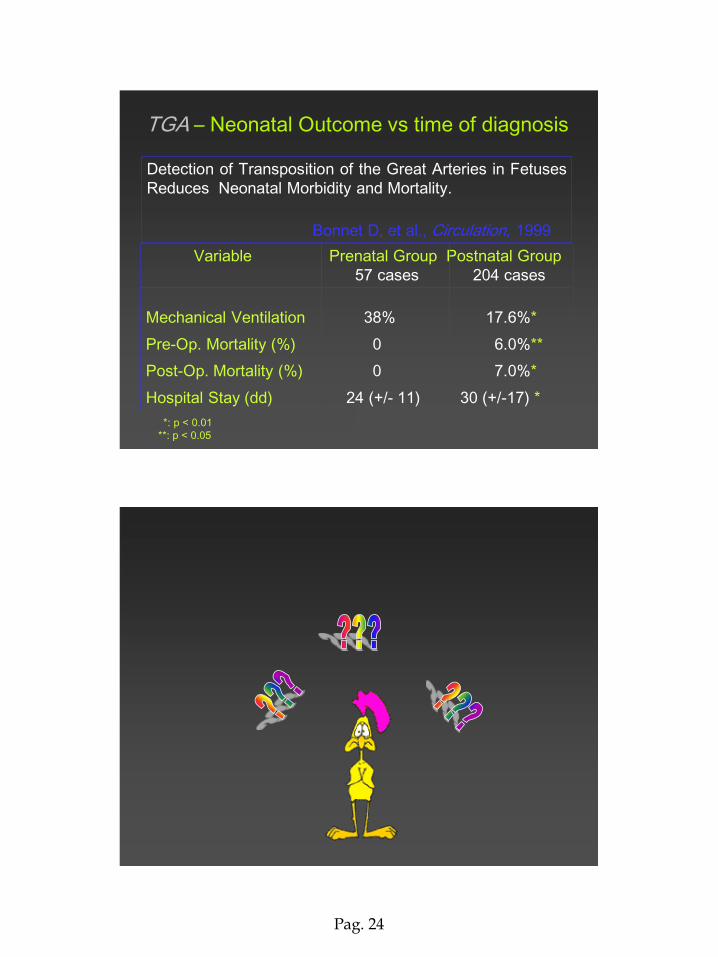
Variable Prenatal Group Postnatal Group
57 cases 204 cases
Mechanical Ventilation 38% 17.6%*
Pre-Op. Mortality (%) 0 6.0%**
Post-Op. Mortality (%) 0 7.0%*
Hospital Stay (dd) 24 (+/- 11) 30 (+/-17) *
Detection of Transposition of the Great Arteries in Fetuses
Reduces Neonatal Morbidity and Mortality.
Bonnet D, et al., Circulation, 1999
*: p < 0.01
**: p < 0.05
TGA – Neonatal Outcome vs time of diagnosis
Fetal Cardiology Unit
Dept. Ob./Gyn.
Univ. Federico II Naples
Pag. 25
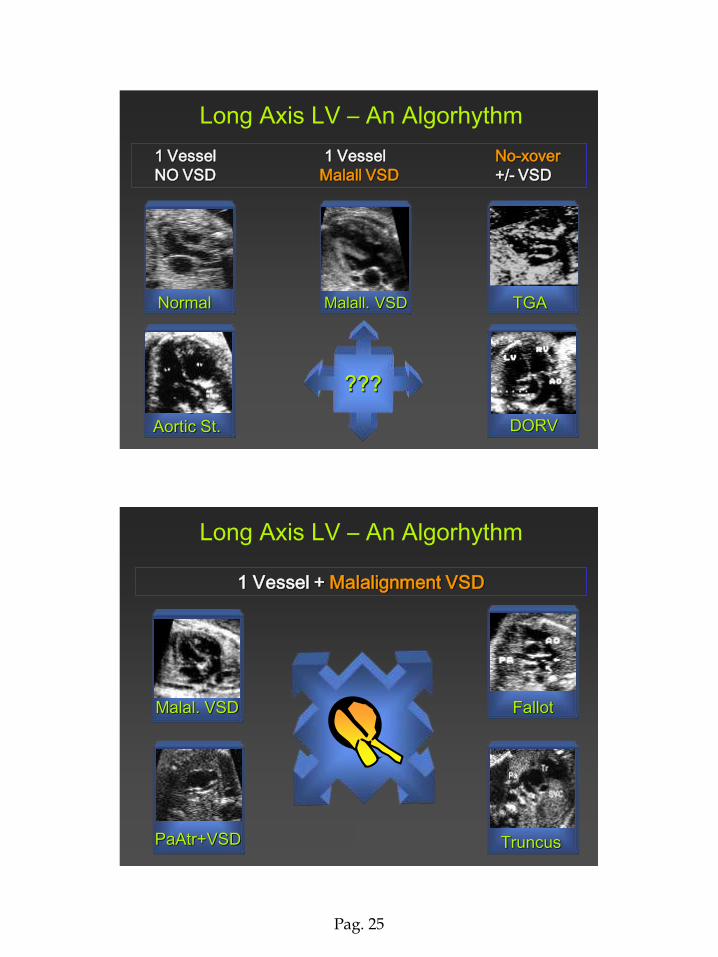
Aortic St.
1 Vessel 1 Vessel No-xover
NO VSD Malall VSD +/- VSD
Long Axis LV – An Algorhythm
Normal Malall. VSD TGA
DORV
1 Vessel + Malalignment VSD
Fallot Malal. VSD
PaAtr+VSD Truncus
Long Axis LV – An Algorhythm
Pag. 26
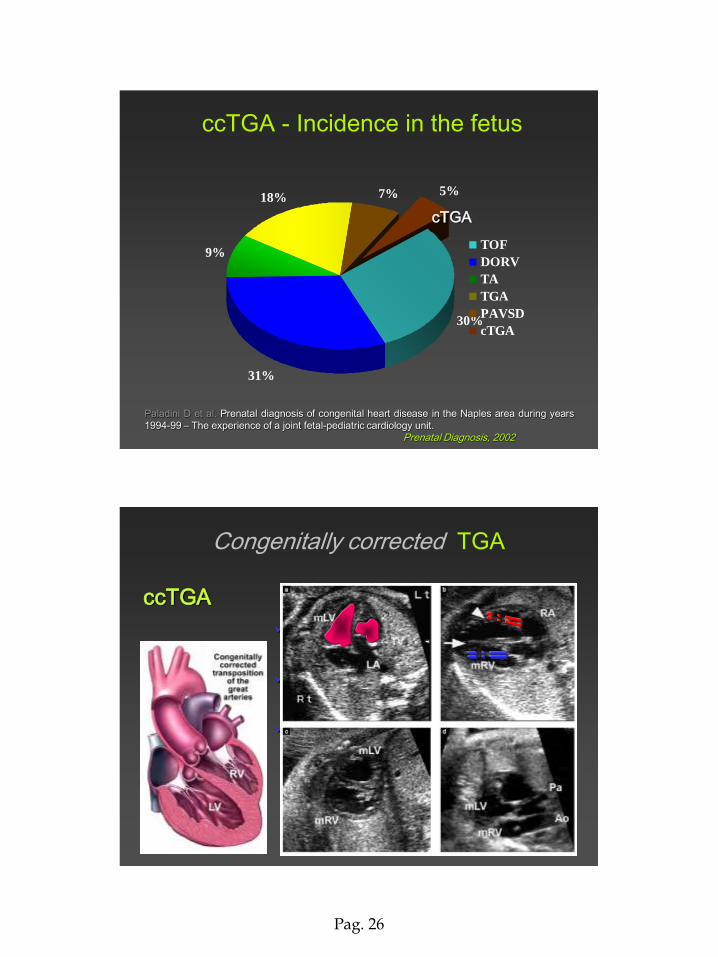
30%
31%
18% 7% 5%
9%TOF
DORV
TA
TGA
PAVSD
cTGA
ccTGA - Incidence in the fetus
cTGA
Paladini D et al. Prenatal diagnosis of congenital heart disease in the Naples area during years
1994-99 – The experience of a joint fetal-pediatric cardiology unit.
Prenatal Diagnosis, 2002
Congenitally corrected TGA
ccTGA
Atrio-ventricular + ventriculo-arterial
discordance (double discordance)
The double discordance hemody_
namically corrects the circle
Several anomalies associated in
most instances
TV Ebstein-like
VSD
Pag. 27
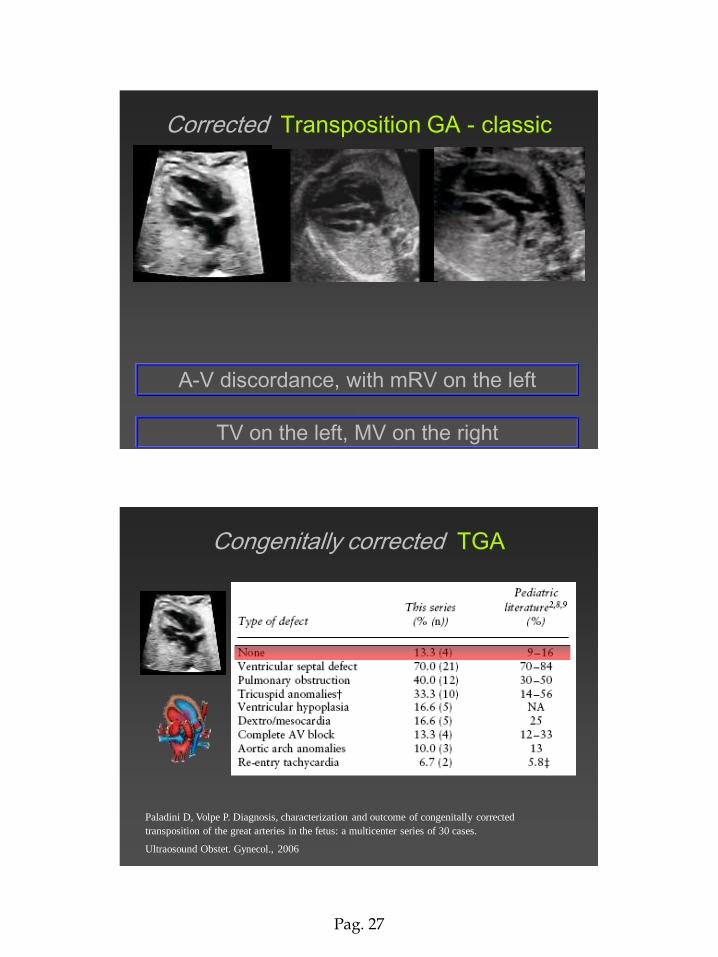
Corrected Transposition GA - classic
A-V discordance, with mRV on the left
TV on the left, MV on the right
Congenitally corrected TGA
Paladini D, Volpe P. Diagnosis, characterization and outcome of congenitally corrected
transposition of the great arteries in the fetus: a multicenter series of 30 cases.
Ultraosound Obstet. Gynecol., 2006
Pag. 28
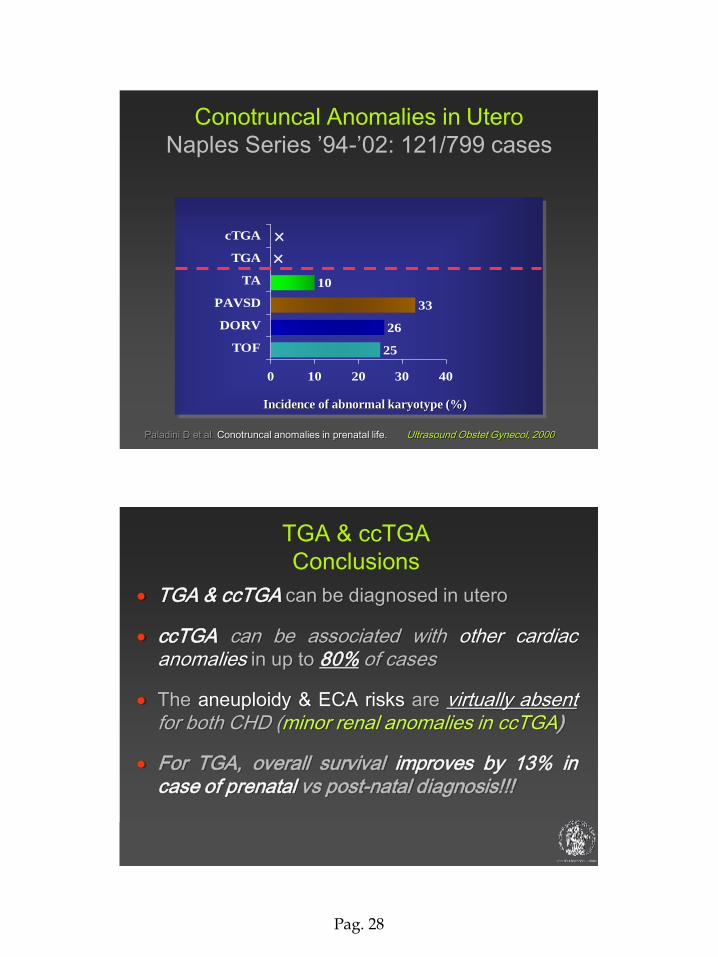
Conotruncal Anomalies in Utero
Naples Series ’94-’02: 121/799 cases
10
33
26
25
0 10 20 30 40
TOF
DORV
PAVSD
TA
TGA
cTGA
Incidence of abnormal karyotype (%)
Paladini D et al. Conotruncal anomalies in prenatal life. Ultrasound Obstet Gynecol, 2000
TGA & ccTGA can be diagnosed in utero
ccTGA can be associated with other cardiac anomalies in up to 80% of cases
The aneuploidy & ECA risks are virtually absent for both CHD (minor renal anomalies in ccTGA)
For TGA, overall survival improves by 13% in case of prenatal vs post-natal diagnosis!!!
TGA & ccTGA
Conclusions
Pag. 29
Fetal Medicine & Cardiology Unit
Federico II University Hospital - Naples, Italy
CHD sharing an overriding aorta + malalignment VSD are
CAT, PAVSD, TOF, APVS
CHD featuring absent crossover are TGA & DORV
CHD at risk of microdeletion 22q11 & chromosomal
aberrations are CAT, PAVSD, TOF, APVS
CHD protecting from aneuploidies are TGA, cTGA (&
cardiosplenic syndromes)
Conotruncal anomalies - Conclusions