outpatient diabetes care for older · pdf fileslide 1 with the population ... it is not...
TRANSCRIPT

Joslin Diabetes Center has created a new Geriatric Care Clinical Center on the Joslin Professional Education Continuum (www.jpec.joslin.org). Through online learning activities and educational materials, the care center will help practices provide the individualized care needed by older adults with diabetes.
In the care center you can access the full version of this CME-certified e-monograph and, by completing the posttest, obtain a printable certificate of credit. You can also engage in an interactive online enduring activity and guide a virtual patient through several clinic visits. In addition, you will also find tools and educational materials for both providers and patients that you can down-load and print to use in your practice. Log in to JPEC today and improve your understanding about elderly patient care.
Outpatient Diabetes Care for Older Adults: Individualizing Strategies for Safety and Control
Supported by an independent educational grant from sanofi-aventis U.S. LLC
Joslin eMonograph
www.jpec.joslin.org

2
Managing Diabetes in an Aging Population
Introduction
Providing diabetes treatment to elderly patients is more than just replicating adult care in an aging population. The pathophysiology of aging, in and of itself, confers a mul-titude of comorbidities that have to be factored into the approach to treatment and its design and implementa-tion, as would be done in someone who had any other significant medical condition. The more we recognize the subtle and not so subtle ways that aging impacts diabetes treatment, the more we can adapt our approaches and thus provide more effective care, insuring that elderly patients receive treatment that is effective, provides rea-sonable outcomes, and optimizes quality of life. The recent evolution of the gerontologist as a specialist has been a welcome addition to the medical care team, and to this end, the perspectives and support provided by gerontologists with diabetes expertise can help clinicians become more effective care providers to this growing seg-ment of the population.
Scope of the Problem: Diabetes in Elderly Patients
Slide 1
With the population growth of the last few decades, the need to provide care to older people will be a very impor-tant healthcare delivery issue in the future. Over the next 2 decades, the number of people in the U.S. over 65 years of age is projected to increase markedly, with an anticipated level of 70 million by the year 2030. Slide 1 shows how the number of older adults is projected to increase rapidly in next few decades compared to the last century.
Slide 2
The prevalence of diabetes in this older population is thought to be about 20%, compared to about 6% in the younger population, and is projected to increase to over 30% in the next half-century. Slide 2 shows the current and projected prevalence of diabetes.1
The socioeconomic cost of the diabetes epidemic among elderly patients is also significant. Compared to their younger counterparts, elderly patients with diabetes have a higher rate of diabetes-related hospitalizations and comprise 65.1% of all diabetes-related healthcare expenditures compared to 34.8% in patients <65 years. In addition, elderly patients with diabetes have higher all-cause mortality and morbidity compared to elderly people without diabetes.
Pathophysiology of Diabetes in Elderly Patients
Many of the differences between elderly patients and younger patients with diabetes stem from the pathophysi-ology of aging. Inherent in the aging process is a progres-sive alteration in all aspects of glucose metabolism, including insulin secretion, insulin action, and hepatic glucose me-tabolism. These changes are superimposed on a patient’s genetic background to magnify the incidence of type 2 diabetes as aging progresses. Many obese elderly patients with diabetes have normal insulin secretion, but marked resistance to insulin-mediated glucose disposal. On the other hand, many lean elderly patients who have diabetes have profound impairment in glucose-induced insulin secre-tion, but normal insulin action. In some elderly patients with diabetes, the loss of first-phase insulin release occurs with the absence of the initial surge in postprandial insulin. Some evidence suggests that autoimmunity may play a role in the impairment of glucose-induced insulin secretion that occurs in lean elderly patients with diabetes.

3
The key is that diabetes in elderly patients can be as heterogeneous in etiology as it can be in younger patients, and some of these processes can be further augmented by the aging process itself.
Presentation and Heterogeneity in Elderly Patients with Diabetes
It is not surprising that the clinical presentation of diabetes in the elderly patient can be different from that of younger patients. It is important for clinicians to be aware of these differences so that they can adequately assess and accu-rately diagnose patients as they age. In some patients, a dysglycemic state (not frank diabetes) may be magnified over time or in the context of a sudden superimposed comorbidity.
With age, the renal threshold for glucose increases, which means that the blood glucose level will be higher than in younger patients before glucosuria is evident. Hence, poly-uria may not be as prominent, and with less glucosuria, urine dipsticks will be even less likely to detect abnormality. Fur-ther, polydipsia may be absent because of impaired thirst mechanisms in older adults. The net result is that the classic symptoms of hyperglycemia—polyuria and polydipsia—are often not present in elderly patients. In fact, dehydration is more common because of altered thirst perception. As a result of all of these factors, infections, neuropathic pain, and failure to thrive may be the only clues of a diagnosis of diabetes in elderly patients, leading to the serious complica-tion of nonketotic hyperosmolar coma.
Slide 3
Elderly patients with diabetes are a heterogeneous group with variable clinical, psychosocial, and functional back-grounds. Some older individuals developed diabetes years earlier and may have significant complications with aging, while others may present with newly diagnosed diabetes
at an older age. Some elderly patients are frail and have other underlying chronic conditions or limited physical or cognitive functioning; others have few comorbidities and are very active. Elderly patients with diabetes can be highly functional, community-living individuals, or dependent on caregivers for their daily activities, or reside in assisted-care facilities or nursing homes (Slide 3).
The prevalence of diabetes in frail elderly patients living in nursing homes may be well over 25%. Compared with older individuals living in the community, nursing home patients with diabetes have a higher incidence of macro-vascular complications, skin infections, and renal disease. The key point, therefore, is that these people need to be assessed in the context of their overall health and func-tional status, recognizing that adverse clinical, functional, and social circumstances act as barriers to the elderly patient’s ability to perform diabetes self-management.
Comorbidities and Complex Interactions
Slide 4
As individuals age, they have a higher likelihood of devel-oping multiple medical conditions, and with each of these conditions comes the probability that they will need to take multiple daily medications. In the past, the significant health burden in elderly patients with diabetes was attributed primarily to higher risk of macrovascular and microvascular complications. However, many coexisting medical condi-tions (such as cognitive dysfunction, depression, functional disability, falls, urinary incontinence, and chronic pain, as well as polypharmacy) not typically associated with diabetes occur at higher frequency in elderly patients with diabe-tes (Slide 4). These conditions, termed geriatric syndrome, may interfere with the patient’s ability to perform self-care tasks, including glucose monitoring, understanding the role of diet and exercise in glucose excursions, and following a complex insulin regimen. Difficulty with self-management may lead to increased risk of nonadherence or treatment

4
errors, contributing to increased risks of hypoglycemia and poor glycemic control, which in turn lead to further difficulty with self-management and ultimately increased risk of mor-bidity and mortality. Thus, before developing treatment and management plans for elderly patients, it is imperative that clinicians conduct a careful and comprehensive assessment for all potential comorbidities, which usually will impact the therapeutic approach.
Cognitive Impairment
Cognitive dysfunction has been associated with both type 1 and type 2 diabetes, with a 1.5-fold greater risk of cognitive decline and 1.6-fold increase in risk of future dementia.
Slide 5
In our study (the Health and Retirement Study), 34% of elderly patients seen in a geriatric diabetes clinic screened posi-tive for cognitive dysfunction compared to 18.5% of elderly patients without diabetes. (Slide 5).2
Slide 6
Although head-to-head comparison of studies is not possi-ble due to different methods of assessment, this and many other studies have shown higher prevalence of cognitive dysfunction in elderly patients with diabetes. The patients with cognitive dysfunction in the Health and Retirement Study had higher A1C levels compared to those without cognitive dysfunction (Slide 6).2
Cognitive dysfunction in elderly patients with diabetes may manifest as deficits in psychomotor efficiency, global cog-nition, episodic memory, semantic memory, and working memory. In particular, executive functioning, which is medi-ated by the frontal lobe, affects behaviors such as prob-lem-solving, planning, organization, insight, reasoning, and attention. Many elderly patients with cognitive dysfunction remain undiagnosed, particularly in the early stages as sub-tle declines in cognitive function remain unrecognized by family or healthcare providers.
Cognitive dysfunction complicates the diabetes picture, because it can make it difficult for patients with diabe-tes to follow medical, nutritional, and exercise regimens, thus increasing the risk of treatment complications. For example, omission of meals leading to hypoglycemia, or in-correct dose or timing of insulin injections or antidiabetes medications, may occur in this population. In an everyday practice, short screening tools (such as a clock drawing test) are useful to assess executive function. If hypoglyce-mia or deterioration of glycemic control occurs in an elderly patient after reasonable efforts at utilizing a treatment plan, or if the patient seems overwhelmed by the management of diabetes, cognitive function should be assessed before patient nonadherence is assumed.
To help those with cognitive dysfunction, simpler treatment plans should be formulated to avoid complications such as hypoglycemia from missing a meal or incorrect dosing or timing of insulin. These patients also may not recog-nize hypoglycemic episodes and/or may forget to report them to providers. Thus, it is important to provide diabetes education to family members or other caregivers to ensure patient safety. If a patient is suspected of having cognitive dysfunction, referral to an appropriate specialist, such as a neurologist, a geriatrician, or a mental healthcare provider, is recommended for a definitive diagnosis. In addition, refer-rals for home health care or to other community resources may be needed. Assessing the caregiver’s ability to manage diabetes is also important, particularly if the caregiver is also elderly or has health issues.
Depression
Depression is about twice as common in people with dia-betes compared to the general population. The estimated prevalence of depression in this population is 15% to 30%. In addition, diabetes and depression have a bidirectional

5
relationship of increased risk, meaning that the presence of one increases risk for the other. Depression is frequently undiagnosed and untreated in this high-risk population.
Slide 7
The Health and Retirement Study also found that 32% of elderly men and 35% of elderly women in a geriatric diabetes clinic screened positive for depressive symptoms compared with 11% of elderly men and 18% of elderly women without diabetes (Slide 7).2
Slide 8
Again, head-to-head comparison is not possible due to different methods of assessment used among different studies; however, data from multiple studies illustrate a higher prevalence of depression in elderly patients with diabetes. The patients with depression in the Health and Retirement Study were more likely to have difficulty performing daily activities (Instrumental Activities of Daily Living [IADL], Slide 8),2 which suggests there is a greater need for caregivers for elderly patients with diabetes who have depression.
The risk of major depression is increased in patients with diabetes who also have two or more coexisting chronic conditions, such as hypertension, coronary artery disease, or arthritis. Depression in elderly patients with diabetes is associated with poor glycemic control, decreased adher-ence to treatment strategies, increased functional disability, increased risk of coronary heart disease, higher mortality, and increased healthcare costs to society. Therefore, timely identification and treatment of depression may increase adherence and improve glycemic control along with overall quality of life for elderly patients.
The Geriatric Depression Scale is a 15-point questionnaire commonly used as a screening tool for depression in the elderly patient with diabetes. The U.S. Preventive Services Task Force suggests the “two simple questions” approach:
“Over the past 2 weeks have you felt down, depressed, or hopeless?”
“Over the past 2 weeks have you felt little interest or plea-sure in doing things?”
If the person answers yes to either of these questions, ad-ditional questioning and referral to establish diagnosis and a treatment plan are suggested.
Polypharmacy
Polypharmacy is commonly defined as use of five or more medications per day. Use of multiple drugs is a complex, challenging aspect of caring for elderly patients, who often require multiple medications to optimally manage their dia-betes and associated conditions. Although polypharmacy is unavoidable in some patients to achieve glycemic con-trol and to adequately control cardiovascular risk factors, a focus on appropriate prescribing, increased regimen adher-ence, and financial feasibility is important. Polypharmacy increases the probability of nonadherence and the potential for drug interactions. In addition, certain medications (such as antihypertensives) and conditions (such as autonomic neuropathy) impair the patient’s ability to recognize the symptoms of hypoglycemia. Side effects of monotherapy or combination therapy may exacerbate comorbidities and impede the patient’s diabetes management.

6
Slide 9
In our geriatric diabetes clinic, we found that for women living alone, glycemic control worsened as the number of daily medications increased (Slide 9).3
While it may be necessarily to treat with multiple medications, and the potential for drug interactions may be unavoidable, it is important to be cognizant of the potential implications of these pharmacologic events, adjust treatments for them as much as possible, and address them with patients and care-givers. To effectively achieve this, the medication list must be kept current and reviewed at each medical visit. Family mem-bers or caregivers can be enlisted to help with this process if patients are unable to. They can also help with preparation of daily pill boxes and insuring that the patient is properly taking (and obtaining/ordering in advance) all prescribed medications.
Physical Disability and Falls
Elderly patients with diabetes have reduced physical function and overall health status compared to age-matched controls living in the same community and are more likely to use a mobility aid, such as a cane or a walker. They may have dif-ficulty performing activities of daily living (bathing, toileting, eating, dressing, and grooming) as well as IADLs (traveling, shopping, using the telephone, managing finances, doing housework, and taking medications). Individuals with these disabilities may require assistance from caregivers or family members to implement diabetes-related tasks, such as self-monitoring of blood glucose (SMBG), insulin injections, meal preparation, and physical activity. A social worker can help establish a support network for these patients.
Falls, especially those resulting in injury, are also more com-mon in older adults. The increased risk of falls in elderly patients with diabetes is usually multifactorial. Presence of peripheral and/or autonomic neuropathy, cardiovascular dis-ease, reduced renal function, muscle weakness, lower limb dysfunction, functional disability, loss of vision, polypharmacy, and comorbidities such as osteoarthritis may contribute
to, and worsen the impact of, falls in frail elderly patients. Although good glycemic control prevents progression of some diabetes complications, and therefore may decrease the risk of falls, hypoglycemia that occurs as a result of diabetes treatment may increase the risk of falls. Thus, the benefits of improved glycemic control to reduce diabetes-related complications must be balanced with the possible increased risk of falls with treatment-induced hypoglycemia. Even a mild episode of hypoglycemia in a frail individual can result in falls and injury.
People who develop a fear of falling are also usually reluc-tant to follow physical activity recommendations. Referral to an exercise physiologist and a supervised program for physical activity may help such people reduce their fear of falling, and thus lead to increased exercise and physical training. Accomplishing this may in turn help reduce the risk of falling.
Urinary Incontinence
Diabetes increases a woman’s risk of developing urinary incontinence. The etiology of this condition in elderly patients with diabetes, especially women, is multifactorial. Risk factors include urinary tract infection, vaginal infection, autonomic neuropathy (resulting in either neurogenic bladder or fecal impaction), and polyuria due to hyperglycemia. Although there is no direct evidence to suggest a deleteri-ous effect of incontinence on diabetes control, identification and treatment are recommended to improve quality of life in women.
Chronic Pain
Pain is considered the fifth vital sign, and should be evaluated at each medical visit. Many elderly patients are reluctant to complain about pain; however, pain can increase depres-sion, distract people from diabetes self-care, reduce activity levels, and increase adrenalin levels, which can impact glu-cose levels. Pain management improves overall quality of life in this population, in addition to increasing the efficacy and outcomes of diabetes treatments.

7
Slide 10
Thus, numerous, complex interactions are seen in elderly patients with diabetes (Slide 10), Diabetes increases the risk of both micro- and macrovascular diseases. Diabetes also increases the risk of geriatric syndrome. The presence of these multiple comorbidities increases morbidity and func-tional disability, which in turn increases the risk of hypogly-cemia and decreases adherence to treatment regimens and overall quality of life. The combination of these interrelated factors makes it difficult for an elderly patient to follow the diabetes regimen and self-care, which in turn leads poor glycemic control, potentially hypoglycemia, and ultimately increased morbidity and mortality.
Hypoglycemia
Hypoglycemia is usually the limiting factor in achieving recommended levels of glycemic control at any age. In the geriatric population specifically, hypoglycemia can lead to poor outcomes, such as precipitation of cardiovascular or cerebrovascular events and exacerbation of cognitive dysfunction.
Slide 11
Three large, randomized, prospective trials recently showed lack of cardiovascular outcome benefit with intensive glycemic control compared to standard treatment. One of these studies (ADVANCE; the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified- Release Controlled Evaluation) analyzed hypoglycemia data and showed that both major and minor hypoglycemic episodes occur at higher rates in patients randomized to an intensive treatment arm. Authors in this study concluded that hypoglycemia indeed was associated with a variety of adverse clinical outcomes, and was probably a marker of vulnerability (Slide 11).4
Slide 12
The risk factors for hypoglycemia in this cohort included advanced age and other factors (Slide 12)4 that are frequently seen in elderly patients with diabetes. Thus, avoidance of hypoglycemia is an important consideration before estab-lishing goals for glycemic control and choosing specific therapeutic interventions in elderly patients.
The risks of hypoglycemia are multifactorial. There is a pharmacokinetic change that occurs with aging affecting metabolism and excretion of many antidiabetes medica-tions as well as insulin. Gastroparesis (a slowing of gastro-intestinal function due to neuropathy) may also precipitate hypoglycemia immediately after meals, if medications are not adjusted for the delay in food absorption. Forgetting to eat meals on time, the inability to self-prepare meals on schedule, or anorexia and weight loss after acute illness are common causes of hypoglycemia in the geriatric population.
In considering elderly patients, it is important to remember that they frequently present with neuroglycopenic manifes-tations of hypoglycemia (e.g., cognitive changes, delirium, weakness, dizziness) compared to the adrenergic manifes-tations (e.g. tremors, sweating, palpitations) seen in younger patients. Some reasons for this phenomenon are diminished glucose counterregulation involving glucagon, epinephrine, and growth hormone responses to hypoglycemia, as well

8
as reduction in autonomic warning symptoms of hypo-glycemia. The problem is further confounded when the neuroglycopenic symptoms are missed or misconstrued as a primary neurologic disease (such as a transient ischemic attack).
Even a mild episode of hypoglycemia may lead to adverse outcomes in the frail elderly patient; episodes of dizziness or weakness increase the risk of falls and fracture leading to severe compromise in quality of life. Thus avoidance of hypoglycemia is an important consideration in choosing therapeutic agents in elderly patients. Careful monitoring for hypoglycemia should be performed periodically in people who exercise; miss meals; abuse alcohol; have impaired renal, cardiac, or gastrointestinal disease; and after recent hospitalization. These issues may arise with change in overall health status in elderly patients with diabetes using some antidiabetes medications (particularly sulfonylurea) or insulin. Thus, hypoglycemia should be carefully assessed at each visit for these patients.
Glycemic Goals and Goal-Setting
The goals for glycemic control as well as risk factor manage-ment in elderly patients should be individualized, reflecting overall health status, ability to perform self-care, or any limitations. Acute complications of hyperglycemia in elderly patients include dehydration, impaired vision, and cogni-tion, all of which contribute to functional decline and an increased risk of falling. Conversely, however, the adverse effects of aggressive diabetes treatment, most notably hypoglycemia, can also result in poor outcomes, including traumatic falls and exacerbation of comorbidities. Obviously a careful balance must be sought.
Slide 13
To help design an appropriate treatment regimen and to assist with goal-setting, healthcare providers need to differentiate between the elderly patient’s chronologic age verses actual health status, as well as determine duration of disease and age of onset, presence of complications and comorbidities, variable life expectancy, social support sys-tems, and financial status. It is often these latter factors that are more important in setting therapeutic goals (Slide 13).
Joslin Diabetes Center, the American Geriatrics Society (AGS), and the American Diabetes Association (ADA) have all published guidelines for diabetes care specific to older adults. The Joslin Guideline and links to the ADA and AGS guide-lines can be found online in the JPEC (www.jpec.joslin.org) Geriatric Care Clinical Center. The emphasis is placed on individualized control based on health status (healthy or frail), presence of comorbidities, and life expectancy.
Slide 14
In the vulnerable elderly population, when the risks of aggres-sive control outweigh the benefits, an appropriate therapy goal may be seeking an A1C level < 8%. However, simply moderating the A1C goal to a higher level may not prevent hypoglycemia. The use of continuous glucose monitoring in elderly patients with diabetes for whom a higher A1C target has been established may still reveal frequent hypoglycemic episodes. As shown in the data on Slide 14, 65% of elderly patients with poor glycemic control (A1C >8%) had at least one episode of hypoglycemia (glucose value < 70 mg/dL).5

9
Slide 15
Nearly half of these patients had A1C > 9% (Slide 15).
Slide 16
In addition, 62% had type 2 diabetes (Slide 16).
Slide 17
Data on Slide 17 show that patients with similar A1C lev-els may show very different glycemic excursion patterns. In such instances, simplification of the treatment regimen to match the elderly patient’s coping skills may help achieve the best glycemic control that is balanced with a more significantly reduced risk of hypoglycemia.
It can take a very skilled and comprehensive approach to treatment design to reduce the risk of hypoglycemia while concurrently achieving reasonable glycemic control. Chasing high glucose levels with increased insulin doses, for example, for an elderly patient who does not recognize hypoglycemic symptoms can foster increased episodes of unrecognized hypoglycemia and rebound hyperglycemia, potentially prompting patients and providers to respond with more insulin. However, complex programs of unbal-anced insulin dosing in response to high and low glucose levels will not benefit the patient. Instead, in these instances, reconstructing and starting a new insulin program, often simpler, helps re-establish insulin patterns and allows a more appropriate—simple and effective—program to be utilized. The more appropriately balanced insulin program often can achieve desired goals more effectively and safely. A diabetes specialty team can be beneficial to help work through this process.
Monitoring Programs
Self-Monitoring of Blood Glucose (SMBG)
SMBG is a central component of self-care for all patients with diabetes. It allows them to visualize their glycemic pat-terns, and consider them in the context of other factors that impact glucose control, such as food intake, activity, timing of various daily activities, and stress. The ability to perform SMBG, as well as assess the implications of its results on a daily basis, is often a key factor in determining the type of diabetes treatment program that is appropriate for any given patient.
Comorbidities, such as cognitive dysfunction, visual im-pairment, arthritis, and low dexterity, should be taken into account before counseling elderly patients about SMBG. For all people with diabetes, one should first ask what information is needed from an SMBG program. In elderly patients with cognitive or physical difficulties, the caregiver can be involved in performing periodic SMBG. The monitor-ing numbers are important for the healthcare provider, to assess the effectiveness of treatment and risk of hypoglyce-mia. Devices such as talking meters for the visually impaired and large meters for patients with arthritis are available.

10
Resources on SMBG patterns can be found in the Joslin Professional Education Continuum (JPEC, www.jpec.joslin.org). Readers are encouraged to consult the Geriatric Care Clinical Center for information on SMBG patterns and strat-egies, where you will find downloadable, print-ready patient handouts, office system support tools, and clinical and office staff resources.
Essentially, results from SMBG convey inherent patho-physiologic processes contributing to hyperglycemia, the impact or medication on glycemic control, or the role of eating or activity on the glucose patterns. In this context, the frequency of monitoring is usually influenced by the stability of blood glucose excursions, the nature of the treatment strategy, the patients’ cognitive and physical abilities, and caregiver support. For example, for people using antidiabe-tes medications, the key questions may be as follows:
When are the hyperglycemic excursions more predomi-nant? Fasting? Immediately after meals? Drifting upward during the day? More after supper? This information in the absence of medication provides a sense of the spectrum of underlying pathophysiology for that patient, and helps direct the medication need, by indicating the need to target fasting glucose, target postprandial glucose, address rising glucose during the day, or focus on specific meals, such as supper.
How are the above patterns impacted by treatment? Or with treatment adjustments? It provides a guide to thera-peutic efficacy and adjustment.
How are these glycemic patterns trending over time? Stable? Changing? And what do those changes suggest about the current therapy and perhaps the overall patient condition? Rapid changes or unusual patterns may reflect the impact of a comorbidity, perhaps one that would oth-erwise have been unrecognized, such as a urinary tract or dental infection. Perhaps there is progression of one of the key etiologic factors contributing to the diabetes (changing insulin resistance or insulin secretory capacity). Perhaps there is a pattern reflective of a medication that is being used, such as a steroid injection.
With these goals for monitoring in mind, and thus asking the right questions, clinicians can design a monitoring sched-ule that provides the specific information that is needed without overtaxing the elderly patient whose willingness or ability to check the glucose frequently may be limited. Oftentimes, checking glucose levels once or twice daily at different times of the day (premeal and bedtime, perhaps occasionally after a meal) in a staggered fashion is ade-quate. Block checking (or block “testing”) may be helpful in balancing frequency of checks with the need to look at glycemic patterns. With this approach, patients will check glucose levels at a lower frequency, which provides an ongoing, low level of observation. Then the patient chooses
two to four consecutive, typical days per month to check more intensively, which provides the increased pattern detail that can help determine pathophysiology and treat-ment efficacy.
Hemoglobin A1C
Slide 18
A1C is the most commonly used test to assess average glycemic control and monitor treatment efficacy in pa-tients with diabetes. An A1C level is recommended every 6 months in elderly patients who are meeting treatment goals and who have stable glycemic control, and every 3 months in those whose therapy has changed or who are not meeting glycemic goals. In elderly patients, the frequently occurring comorbidities and conditions that affect red blood cell life span (e.g., anemia, erythropoietin therapy, iron supplement) also affect measurement of A1C (Slide 18). For these pa-tients, treatment decisions should be based on SMBG or alternative tests for glycemia, such as glycated albumin.

11
Pharmacotherapy
Slide 19
All types of antidiabetes medications and insulin are safe in older patients when careful attention is paid to factors such as renal and hepatic function, concurrent use of medications for other conditions, concomitant illnesses, mental status, living situation, risk of hypoglycemia, and appropriate glycemic goals. The 15 classes of medications (insulin and antidiabetes medications) are listed in Slide 19, showing dosing, A1C-lowering effect, target of action (fasting glucose, postprandial glucose, or both), and safety issues.6-12 For additional guidance, you can find Joslin Diabetes Cen-ter’s management guidelines in the JPEC (www.jpec.joslin.org) Geriatric Care Clinical Center.
Other important factors to consider when selecting medi-cations include potential adverse drug effects, drug interactions, medication costs, and adherence related to dosing frequency. Complicated treatment regimens frequently fail, and may even cause harm if the person can-not follow the given instructions. Most people with diabetes and their medical providers prefer to use the antidiabetes medications as the first-line therapy. However, patients with significant hyperglycemia and glucose toxicity with very high glucose values at presentation may need insulin initially to establish control. It is usually possible to change the regimen to an antidiabetes medication once the glu-cose levels are controlled and the effects of glucose toxicity have resolved. The glucagon-like peptide-1 (GLP-1) ago-
nists, while not insulin, are given by injection. Although a potential barrier is that they require injection, their glucose- dependent response may make them desirable in this population. “Start low and go slow” is a good principle to follow when starting new medications or adjusting insulin in the elderly patient.
Antidiabetes Medications
Metformin is an attractive agent to use due to a low risk of hypoglycemia in elderly patients with diabetes. A common contraindication to metformin use in this population is renal insufficiency. It is important to remember that in frail elderly patients with reduced muscle mass, serum creatinine may not reflect true renal function. Calculated creatinine clear-ance or glomerular filtration rate (GFR) are used for treatment dosing and monitoring. If the GFR is < 60, careful and frequent monitoring should be conducted. If the GFR is < 50, metformin should be avoided. Elderly patients are also at increased risk for developing other conditions that further reduce renal function or cause lactic acidosis (e.g., myo-cardial infarction, stroke, cardiac failure, pneumonia). Gas-trointestinal side effects and weight loss may also be limit-ing factors in elderly patients taking metformin. All elderly patients treated with metformin should stop taking the drug immediately if they become ill for any reason, or if they are to undergo a procedure requiring the use of iodinated con-trast material.
Insulin secretagogues include longer- and shorter-acting agents. The longer-acting secretagogues, the sulfonylureas (glipizide, glyburide, glimepiride), are well tolerated and used commonly in elderly patients. Risk of hypoglycemia is the primary concern. The shorter-acting secretagogues, repa-glinide and nateglinide, act similarly to the sulfonylureas but with more focused action just after meals. The advantage of this latter approach is that repaglinide and nateglinide are taken just before a meal, and if a meal is skipped or added, a dose of the medication can be skipped or added, respectively. The dose may also be adjusted if a person has a variable appetite. This approach is especially useful in frail nursing home patients with variable food intake. These two medications are not chemically related to sulfonylureas; therefore, they can be used instead of a sulfonylurea in the setting of a sulfa allergy. However, these drugs cost more than a generic sulfonylurea and they need to be taken more frequently, which potentially increases the likelihood of a missed dose.
The thiazolidinediones are a class of antidiabetes medica-tions that increase insulin sensitivity. Of the two thiazolidin-ediones currently on the market, it was recently suggested that rosiglitazone might have a higher risk of cardiovascular adverse events. This concern is controversial and opinions are varied. However, prescribers should use this information and the latest information on this issue to gauge their level
12
of caution when using this medication in elderly patients. Pioglitazone appears to be a safe choice, when combined with liver function monitoring, even in elderly patients. This group of drugs does not pose a hypoglycemia risk, making them an excellent choice for some elderly patients. Other side effects of interest in this group include fluid retention, leg edema, and osteoporosis. Thiazolidinediones should not be used in patients with class IIII or IV heart failure.
Alpha-glucosidase inhibitors (acarbose and miglitol) inhibit the gastrointestinal enzyme alpha-glucosidase, which results in a slower rise in postprandial blood glucose con-centrations. These drugs have relatively lower efficacy. They are fairly safe in elderly patients. The main side effects that limit their use are flatulence and diarrhea, which are very common, and can be issues in this group.
The incretin-mimetic agents include the GLP-1 analogs (exenatide, liraglutide) and the dipeptidyl peptidase 4 (DPP-4) inhibitors (sitagliptin, saxagliptin). GLP-1 analogs are useful for elderly patients, provided they are able to self-inject. They have a tendency to promote weight loss, which may be useful in overweight individuals. The most common adverse events are nausea, vomiting, and diarrhea. The DPP-4 inhibitors, are well-tolerated in elderly patients without weight loss, and can be used with renal dosing in patients with renal insufficiency. These agents do not cause hypoglycemia and are weight-neutral, making them attrac-tive for use in elderly patients.
Pramlintide is a synthetic analog of amylin, which is a natu-rally occurring hormone normally cosecreted with insulin. Its pharmacologic form is administered by mealtime subcuta-neous injection along with doses of insulin. It is available for the treatment of both type 1 and insulin-treated type 2 dia-betes. It requires multiple subcutaneous injections, and its role in the management of diabetes in the elderly is limited.
Designing Antidiabetes Treatment Programs for Type 2 Diabetes
Most patients with type 2 diabetes are thought to benefit from the initiation of “combination” (multiple medication) therapy sooner rather than later. This is because the mech-anisms that cause the hyperglycemia of type 2 diabetes are often multiple—combinations of insulin resistance, insulin secretory deficiencies, and incretin dysfunction. Thus, using multiple medications that target different pathophysiologic mechanisms can provide a more comprehensive coverage of the causes of hyperglycemia and more effectively restore normoglycemia. Also, for some of these medications, us-ing lower doses as in multiple medication programs can avoid the problems that can be seen with higher doses of one medication, such as hypoglycemia potential and ad-verse effects. The most important factors in making therapy choices will be the degree of β-cell dysfunction as well as
the current renal and hepatic function. Multiple combina-tions are available, and the choice depends on the individual patient and the goals set for control. If glycemic goals are not met after reasonable efforts, the patient should be eval-uated for contributing causes, such as difficulty adhering to the medication, side effects, or poor understanding of the nutrition/dietary plan. In elderly patients who require more than one agent, pill boxes are recommended for improved adherence.
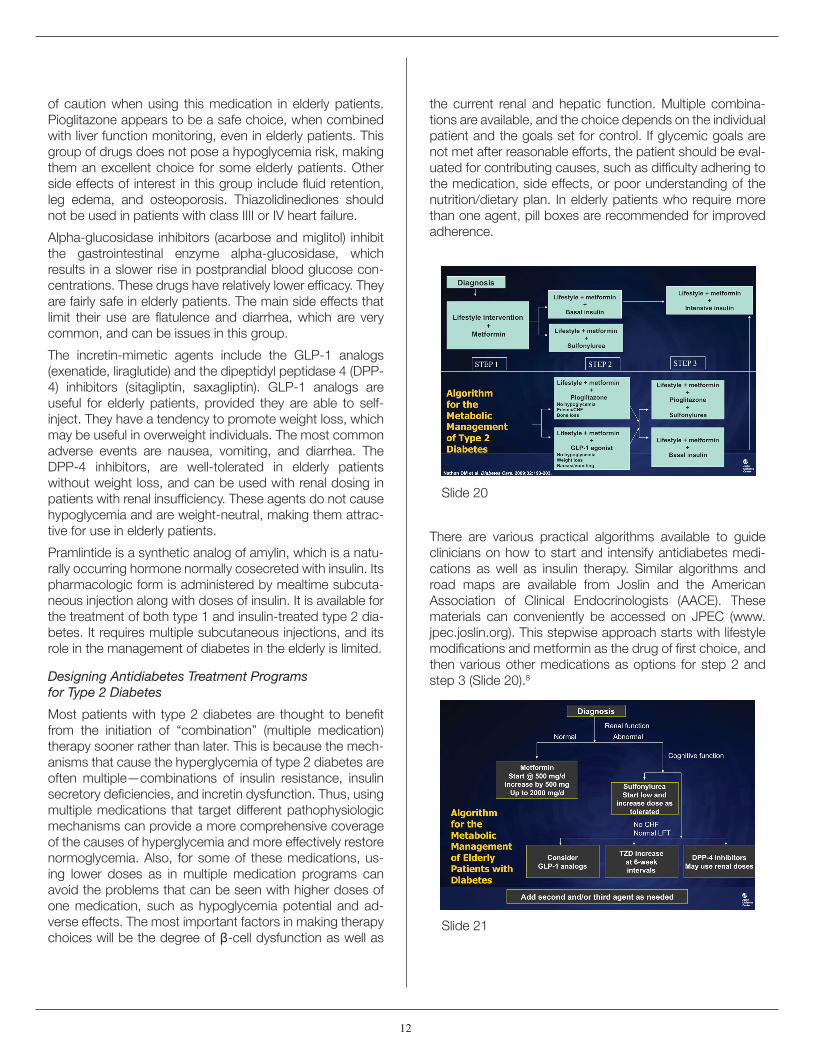
Slide 20
There are various practical algorithms available to guide clinicians on how to start and intensify antidiabetes medi-cations as well as insulin therapy. Similar algorithms and road maps are available from Joslin and the American Association of Clinical Endocrinologists (AACE). These materials can conveniently be accessed on JPEC (www.jpec.joslin.org). This stepwise approach starts with lifestyle modifications and metformin as the drug of first choice, and then various other medications as options for step 2 and step 3 (Slide 20).8
Slide 21

13
There are no modifications suggested by this guideline for elderly patients. However, using this guideline as a starting point, certain adaptations may, in fact, be needed for elderly patients (Slide 21). In this author’s opinion, it is rec-ommended that the clinician first assess renal function in elderly patients. If not contraindicated based on the creati-nine clearance, metformin remains the drug of choice due to its benefits in reducing risk of cardiovascular diseases and low risk of hypoglycemia. For the next step, it is rec-ommended to assess patients’ cognitive function. In those elderly patients who are able to avoid, recognize, and treat hypoglycemia appropriately, a sulfonylurea such as glipi-zide can be used safely. Next, the patient is assessed with liver function tests and for history of congestive heart fail-ure (CHF). Pioglitazone can be used, with the advantage of no risk of hypoglycemia in patients who have normal liver function tests and no history of CHF. Alternatively, DPP-4 inhibitors, such as sitagliptin or saxagliptin, are also well-tolerated in most elderly patients and can be used as a second or third medication, gauging the needed versus anticipated efficacy. GLP-1 agonists may also be used, but with caution to avoid excessive weight loss in frail elderly patients. Although they need to be injected, their advantage over insulin is a low risk of hypoglycemia.
Insulin
When antidiabetes medications are not able to adequately control hyperglycemia, insulin can be used safely in elderly patients. The risk of hypoglycemia is higher with insulin compared to antidiabetes medications. In addition, the elderly patient’s ability to manage a complicated insulin regimen may change with increasing age or worsening overall health. Physical and/or mental capacity also may decline over a period of time; therefore, the benefit/burden of aggressive glycemic control, especially with a compli-cated regimen, should be periodically assessed in elderly patients. With the availability of various types of insulin with different time-action curves, simplification of the regimen is possible, to avoid overwhelming these patients.
Adding a bedtime dose of basal insulin can be a good way of initiating insulin therapy along with antidiabetes medica-tions in those with suboptimal glycemic control. Insulin is sometimes underutilized in the elderly because of fear (by the physician, patient, or family) that it is too complicated or dangerous. However, in many elderly patients, glycemic control improves substantially when they take one or two daily doses of intermediate- or long-acting insulin. Thus, insulin treatment has to be individualized and monitored carefully with regular follow-up.
Before beginning insulin therapy, it is important to evaluate whether the patient is physically and cognitively capable of drawing up and giving the appropriate dose of insulin using syringes and vials or using an insulin pen, monitor-
ing blood glucose, and recognizing and treating hypoglyce-mia. Errors in insulin technique are frequently seen in elderly patients, even after many years of previously successful self-managed insulin treatment. Thus, periodic assess-ment and education about the correct injection technique is important in this population. For elderly patients taking a fixed daily dose of insulin and who are capable of giving the insulin injection but are not able to draw it up, a phar-macist or family member may have to draw up a supply of syringes (week’s worth) and refrigerate them for the patient. As time progresses, the regimen may have to simplified for those patients struggling to self-administer the insulin program. If the patient moves to a care facility where the responsibility of insulin administration switches to the staff, the simplification of the regimen may not be an issue. For some, the elimination of potential adverse effects and drug interactions from antidiabetes medications in favor of insulin treatment may be preferred.
Slide 22
Guidelines for insulin initiation and intensification are also well-designed for adult patients with diabetes (Slide 22).7
Slide 23

14
These guidelines can be used in elderly patients with a few caveats (Slide 23). It is important to keep the insulin regimen as simple as possible. For example, using a long-acting in-sulin injection once daily in combination with antidiabetes medications is well-tolerated in elderly patients. Caution should be used when using NPH or mixed insulin twice daily in this population because this group tends to eat supper earlier. If intermediate-acting insulin (NPH) is given before supper at an early hour, it may peak in middle of the night, increasing the risk of hypoglycemia. If possible, NPH should be used at bedtime. It is best to avoid short-acting insulin at bedtime. The timing of the insulin can be matched to a caregiver’s availability for those patients who are not able to take insulin reliably by themselves.
Educational Strategies in Elderly Patients with Diabetes
In light of the unique needs of elderly patients, effective geriatric diabetes education programs are increasingly important. However, elderly patients are under-represented in diabetes education research studies; evidenced-based guidelines specifically targeted towards elderly patients are difficult to formulate. The American Association of Diabetes Educators (AADE) and the AGS have formulated guidelines for diabetes education in the elderly largely based on expert consensus. Both guidelines—AADE’s Special Consider-ations in the Management and Education of Older Persons with Diabetes and AGS’ Clinical Practice Guideline: Diabetes Mellitus in Older Persons—can be found on the respective organizations’ Web sites. Links to these guidelines can conveniently be found in the Geriatric Care Clinical Center on JPEC (www.jpec.joslin.org)
Both AGS and AADE guidelines appreciate that the care of elderly patients with diabetes is complicated by their clinical and functional heterogeneity. To positively impact self-care and quality of life in elderly patients with diabetes, educa-tion programs must be tailored to patients’ individual needs. A comprehensive assessment of each patient should be performed to determine individual goals, strengths, and deficits. Health literacy, coexisting health conditions, poly-pharmacy, functional limitations, and financial limitations all have a significant impact on the ability of geriatric popula-tions to benefit from diabetes education and to success-fully engage in self-care activities. These factors need to be assessed in all elderly patients presenting for diabetes education and reassessed on a regular basis, because new issues can arise as age and medical conditions progress.
Practical Issues in the Care of Elderly Patients with Diabetes
Decision aids and algorithms are important for successful management of most chronic diseases. However, the deci-sion process to manage chronic diseases in elderly patients often requires a more complex combination of data, clini-cal skills, and formal evaluation for multiple diseases and conditions. It may therefore be necessary for providers to combine disparate data sources and then conduct a com-plex mental calculation about the potential risks and benefits of a given decision. When managing diabetes in elderly patients, such decisions are further complicated by con-siderations needed for the unique challenges of aging regarding pathophysiology, diagnostic criteria, doses and side effects of medications, dietary considerations, exercise strategies, and impact of disease on quality of life. Thus, simple algorithms often do not work well in this population.
When evaluating the elderly patient with diabetes, goal-setting for both hyper- and hypoglycemia is equally important. One could argue that in patients > 80 years or in frail patients with limited life expectancy, hypoglycemia has higher risks than hyperglycemia. It is important to inquire about hypoglycemia in detail, because elderly patients are frequently poor historians. The unique presen-tation of hypoglycemia and hypoglycemic unawareness also need to be considered in elderly patients with diabetes.
Further, many of the elderly patients with diabetes who are cared for today have had diabetes for many years. They may have been diagnosed before blood glucose monitoring, during the time when they did urine testing, with the goal of keeping the urine “sugar-free.” These patients often have the mindset that they need to “knock down the high sugar levels,” and never quite feel comfortable with patterns as the current monitoring paradigm. This behavior is seen more commonly in elderly patients with type 1 diabetes who have spent their entire adult life with a strict diet and exercise regimen. For these patients, when clinicians have to compromise the efforts to chase high glucose levels, acknowledge that hypoglycemia may be more harmful than hyperglycemia, and accept higher A1C levels, the change runs counter to the patient’s lifelong approach to care and they may have difficulty accepting it. They may “chase” high glucose levels themselves, even without the physician’s rec-ommendation or approval. Some patients may think that, if the physician does not want them to take more insulin when their glucose levels are high, then they should eat less instead. It is important to recognize these incorrect per-ceptions and self-care tendencies, and address them with clinical skill and careful communication. For the elderly patient, it is not uncommon to have to repeat conversations about these issues at every visit.

15
All medications have potentially higher side effects in older adults. Thus, choosing an agent that is least harmful to the patient with his/her comorbidities is appropriate. Medications with low risk of hypoglycemia are preferred in general. Metformin, pioglitazone, and DPP-4 inhibitors are used safely and easily when contraindications are care-fully avoided. In patients who are on antidiabetes medi-cation with hypoglycemia risk or insulin therapy, a safety assessment should be conducted at each visit and after any health event, such as hospitalization, weight loss, etc. Edu-cating patients and caregivers about higher glucose goals helps to avoid anxiety about hyperglycemia and lowers risk of hypoglycemia.
Slide 24
When patients on complex insulin regimens are found to be unable to cope with them, simplification of the regimen lowers the risk of hypoglycemia without deterioration of glycemic control. In patients with long duration of diabetes, measurement of serum C-peptide levels provides a rough estimate of endogenous production of insulin. If there are detectable levels of C-peptide, antidiabetes medications can be added and the number of insulin injections can be decreased to simplify the regimen.
In a study evaluating patients from a geriatric diabetes clinic, it was shown that many elderly patients having difficulty with their insulin regimen were able to decrease the number of insulin injections. Such simplification resulted in decreased number of hypoglycemia episodes without deterioration of A1C (Slide 24).13
Slide 25
Based on this study, we have designed a reverse algorithm to simplify the insulin regimen in elderly patients who are unable to cope with complex regimens (Slide 25).
Slide 26
Patient’s age, renal and hepatic function, and availability of caregiver support should be assessed first. Antidiabetes medications should be added based on these patient characteristics. The use of antidiabetes medications in combination with once-daily injection of long-acting insulin can improve hyperglycemia with less complexity. In those patients who truly require insulin due to significant insulin secretory loss or who cannot tolerate antidiabetes medi-cations, simplification of the insulin regimen may include decreasing the number of insulin injections by using mixed insulin or by changing the insulin injection regimen so that caregivers are able to help with injections (Slide 26).

16
It is important to remember that health is dynamic in older adults. Patients who are stable on one type of regimen may get sick and then require a change in their medications. Hospitalization, anorexia, weight loss, and deconditioning are seen frequently in the elderly who get sick. Patients should be carefully evaluated for increased or decreased need in medications or insulin due to illnesses. Elderly pa-tients value higher functionality and independence for a good quality of life. The diabetes treatment regimen should not adversely impact these aspects.
Elderly patients who are living with an able spouse, family member, or caregiver can be treated safely as long as care-givers are well versed with self-care. Similarly, well-trained nursing home staff can safely manage the insulin regimen if appropriate protocols are set up.
Conclusions
The principles discussed in this monograph should provide a good starting point for the approach to diabetes care in the elderly patient. Other resources for the care of older patients are in the Geriatric Care Clinical Center on JPEC. You will also find Lou, an 85-year-old diagnosed with diabe-tes and showing signs of poor glycemic control, in the Virtual Clinic on JPEC. You can improve your knowledge of how to care for your own elderly patients by logging in and making clinical decisions for this virtual patient online. A wealth of other information on management of type 2 diabetes, advancing therapy for type 2 diabetes, insulin therapy, and cardiometabolic risk stratification and reduction available in other clinical care centers in the Joslin Professional Edu-cation Continuum (JPEC, www.jpec.joslin.org) can provide more in-depth information on the specifics of treatment. Feel free to consult with this material to help complete your base of knowledge and skills in the treatment of elderly pa-tients with diabetes. In particular, when used in the context of this material that focuses on specific issues in the care of elderly patients, it is hoped that clinicians will be able to more effectively set therapeutic goals and design treatment programs for this growing segment of the population.
References
1. Venkat Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005–2050. Diabetes Care. 2006;29:2114-2116.
2. Munshi M, Grandel L, Hayes M, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care. 2006;29:1794-1799.
3. Hayes M et al.2006;A212:908P. Abstract presented at American Diabetes Association meeting.
4. Zoungas S, Patel A, Chalmers J, et al.; ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363:1410-1418.
5. Munshi M et al. Arch Intern Med. In press.
6. Nathan DM, Davidson MB, DeFronzo RA, et al.; American Diabetes Association. Impaired fasting glucose and impaired glucose tolerance: implications for care. Diabetes Care. 2007;30:753-759.
7. Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2006;29:1963-1972.
8. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193-203.
9. American Diabetes Association. Standards of medical care in diabetes-2008. Diabetes Care. 2008;31:S12-S54.
10. Welchol (colesevelam hydrochloride) prescribing information. Sankyo Parke Davis, Parsippany, NJ, January 2008.
11. Cycloset (bromocriptine mesylate) prescribing information. Santarus, Inc., San Diego, CA, May 2009.
12. Buse JB, Rosenstock J, Sesti G, et al. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet. 2009;374:39-47.
13. Munshi M, Hayes M, Sternthal A, Ayres D. Use of serum C-peptide level to simplify diabetes treatment regimens in older adults. Am J Med. 2009;122:395-397.