overview of juvenile dermatomyositis pediatric rheumatology red team resident teaching series
TRANSCRIPT

Overview of Juvenile Dermatomyositis
Pediatric RheumatologyRed Team Resident
Teaching Series
What is Juvenile Dermatomyositis?
“A multisystem disease of uncertain origin that results in chronic inflammation of striated muscle and skin.” (Cassidy and Petty, 2011)
• A rare pediatric autoimmune disease, but the most common inflammatory myopathy in children• Average annual incidence rate: 3.2 cases per 1 million children
(Mendez, EP, et al. 2003)• 16-20% of all dermatomyositis patients have onset in childhood
• Girls > boys (2.2:1)• Peak age of onset: 7.6 years old, peak range: 5-14 years of age• No difference in incidence in different ethnicities

What is Juvenile Dermatomyositis?
• Systemic small vessel vasculopathy• Mainly muscle and skin involvement, but can involve other
organ systems• Presentation: insidious onset malaise, fever, fatigue, rash,
muscle weakness/pain• Don’t always have skin AND muscle manifestations at the same
time• Amyopathic JDM = JDM without evidence of muscle involvement
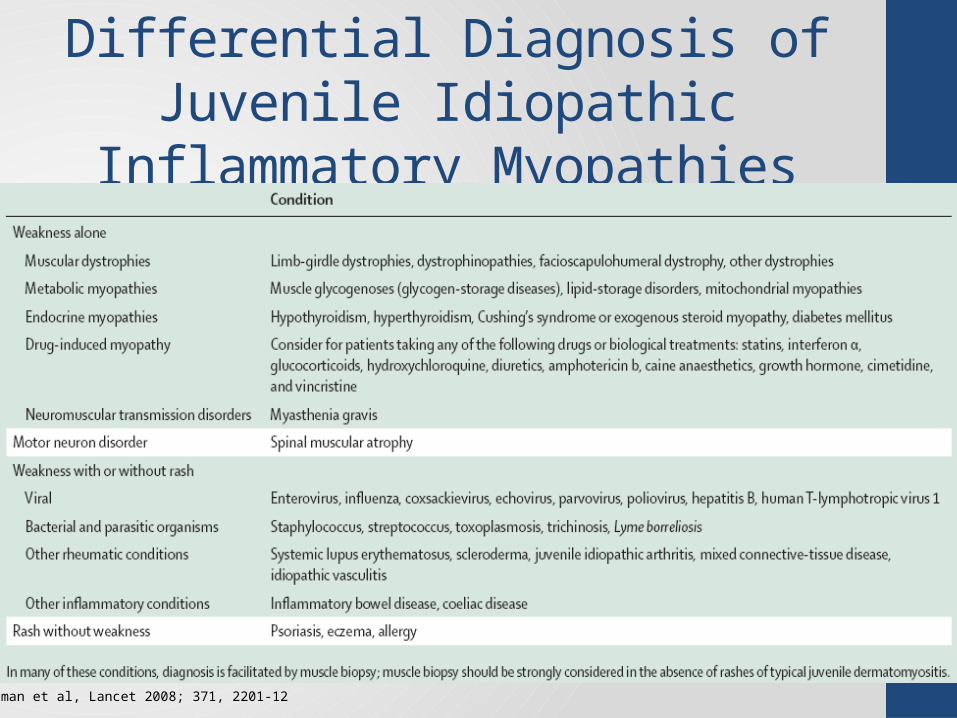
Differential Diagnosis of Juvenile Idiopathic Inflammatory Myopathies
Feldman et al, Lancet 2008; 371, 2201-12
JDM - Etiology & Pathogenesis
• Cause unknown• Likely autoimmune angiopathy• Environmental and genetic factors implicated• A history of infection prior to onset is common
• 65- 70% of patients have a history of a significant infection during the three months prior to first onset of symptoms
• Proposed triggers include various infectious agents, vaccines, medications, UV light
• Cellular and humoral immunity implicated• Complement-mediated injury important• Innate immune response: type I interferons and dendritic
cells
Cellular and Humoral Immunity
• Autoimmunity• ~70-80% JDM patients have positive ANA• ~10% children have classic myositis specific antibodies (MSA)
compared to >50% adults• Some auto-antibodies that you might see positive in these
patients: anti-Jo1, anti-SSA, anti-SSB, anti-topoisomerase, anti-U1RNP
• Abnormalities of cell-mediated immunity• MHC class I antigens strongly expressed by muscle cells of JDM
patients but not normal controls• Association with immunodeficiency• Occurrence in children with hypogammaglobulinemia,
selective IgA deficiency, & C2 deficiency
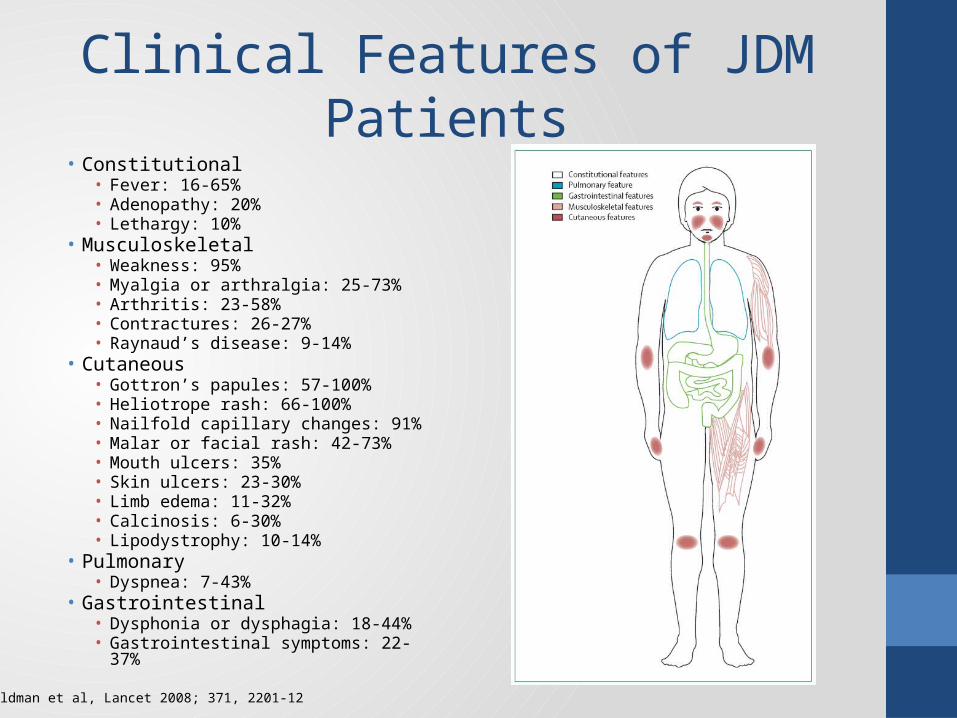
Clinical Features of JDM Patients• Constitutional
• Fever: 16-65%• Adenopathy: 20%• Lethargy: 10%
• Musculoskeletal• Weakness: 95%• Myalgia or arthralgia: 25-73%• Arthritis: 23-58%• Contractures: 26-27%• Raynaud’s disease: 9-14%
• Cutaneous• Gottron’s papules: 57-100%• Heliotrope rash: 66-100%• Nailfold capillary changes: 91%• Malar or facial rash: 42-73%• Mouth ulcers: 35%• Skin ulcers: 23-30%• Limb edema: 11-32%• Calcinosis: 6-30%• Lipodystrophy: 10-14%
• Pulmonary• Dyspnea: 7-43%
• Gastrointestinal• Dysphonia or dysphagia: 18-44%• Gastrointestinal symptoms: 22-37%
Feldman et al, Lancet 2008; 371, 2201-12

Dermatomyositis – other organ involvement
•Gastrointestinal vasculitis- gut wall perforation• Arthritis - common but usually early and mild, non-
erosive• Cardiac - inflammation, fibrosis, conduction defects• Renal - glomerular hypercellularity• Pulmonary - fibrosis, pneumothorax• Central nervous system - behavior changes, seizures• Alopecia• Eyes - exudative vasculitis of retina•Derm – calcinosis, subcutaneous nodules, ulcerations• Lipodystrophy

The Pictures of Juvenile Dermatomyositis
Heliotrope Rash with periorbital edema
• Malar rash• Rash on extensor
surfaces
Gottron’s Papules
V Sign Shawl Sign Calcinoses
Heliotrope: The flower for which the rash is named!
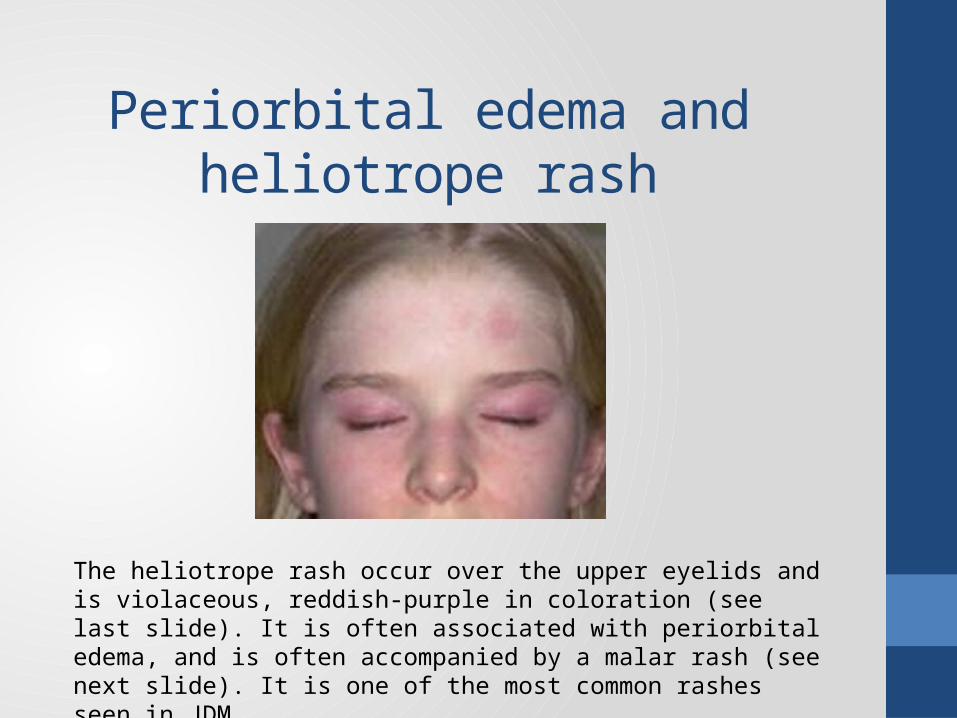
Periorbital edema and heliotrope rash
The heliotrope rash occur over the upper eyelids and is violaceous, reddish-purple in coloration (see last slide). It is often associated with periorbital edema, and is often accompanied by a malar rash (see next slide). It is one of the most common rashes seen in JDM.
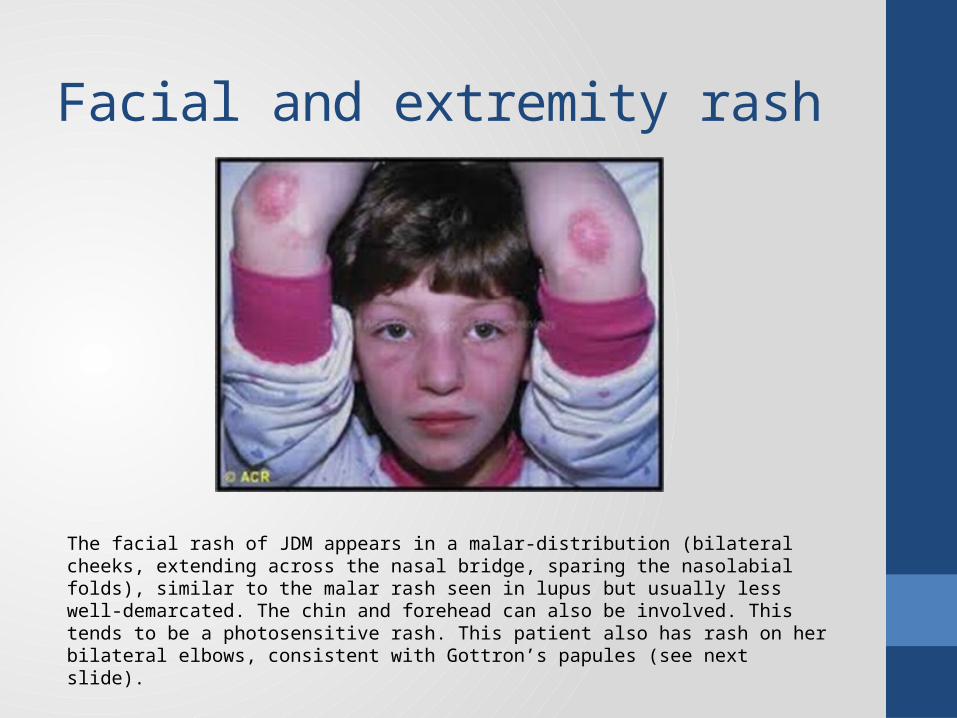
Facial and extremity rash
The facial rash of JDM appears in a malar-distribution (bilateral cheeks, extending across the nasal bridge, sparing the nasolabial folds), similar to the malar rash seen in lupus but usually less well-demarcated. The chin and forehead can also be involved. This tends to be a photosensitive rash. This patient also has rash on her bilateral elbows, consistent with Gottron’s papules (see next slide).
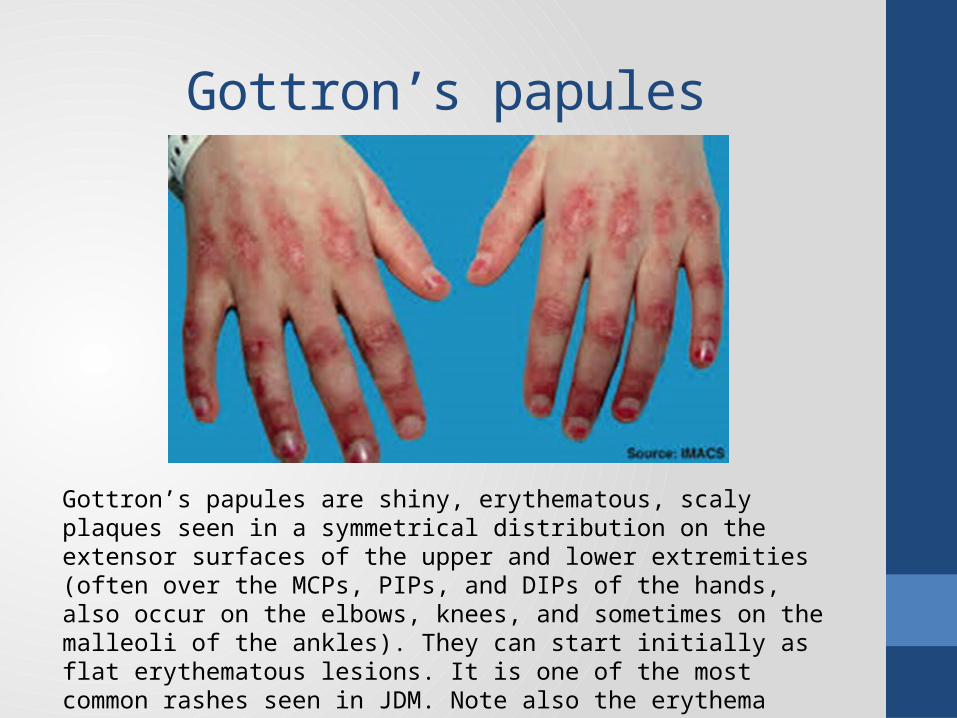
Gottron’s papules
Gottron’s papules are shiny, erythematous, scaly plaques seen in a symmetrical distribution on the extensor surfaces of the upper and lower extremities (often over the MCPs, PIPs, and DIPs of the hands, also occur on the elbows, knees, and sometimes on the malleoli of the ankles). They can start initially as flat erythematous lesions. It is one of the most common rashes seen in JDM. Note also the erythema around the nailbeds, reflecting nailbed capillary abnormalities, another common finding (see next slide).
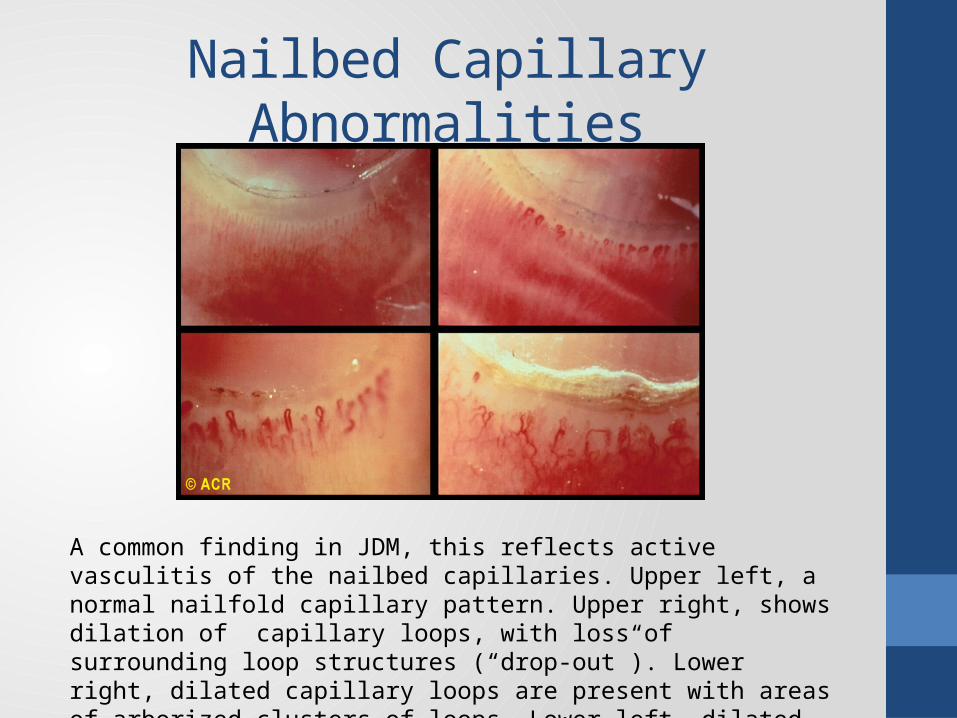
Nailbed Capillary Abnormalities
A common finding in JDM, this reflects active vasculitis of the nailbed capillaries. Upper left, a normal nailfold capillary pattern. Upper right, shows dilation of capillary loops, with loss of surrounding loop structures (“drop-out”). Lower right, dilated capillary loops are present with areas of arborized clusters of loops. Lower left, dilated and prominent capillary loops.

Other Skin Manifestations• Photosensitive rash can also occur on the chest, neck, extremities, scalp (this is
the V-sign and shawl sign seen on Slide #7)• May evolve into poikiloderma (hyper or hypopigmentation with atrophy and
telangiectasia)• Mechanic’s hands• Pruritis, psoriasiform scalp dermatitis
Poikiloderma: Confluent violaceous papules with mottled dyspigmentation and telangiectasias
Mechanic’s hands: Scaly, fissured, hyperkeratotic skin suggestive of manual labor
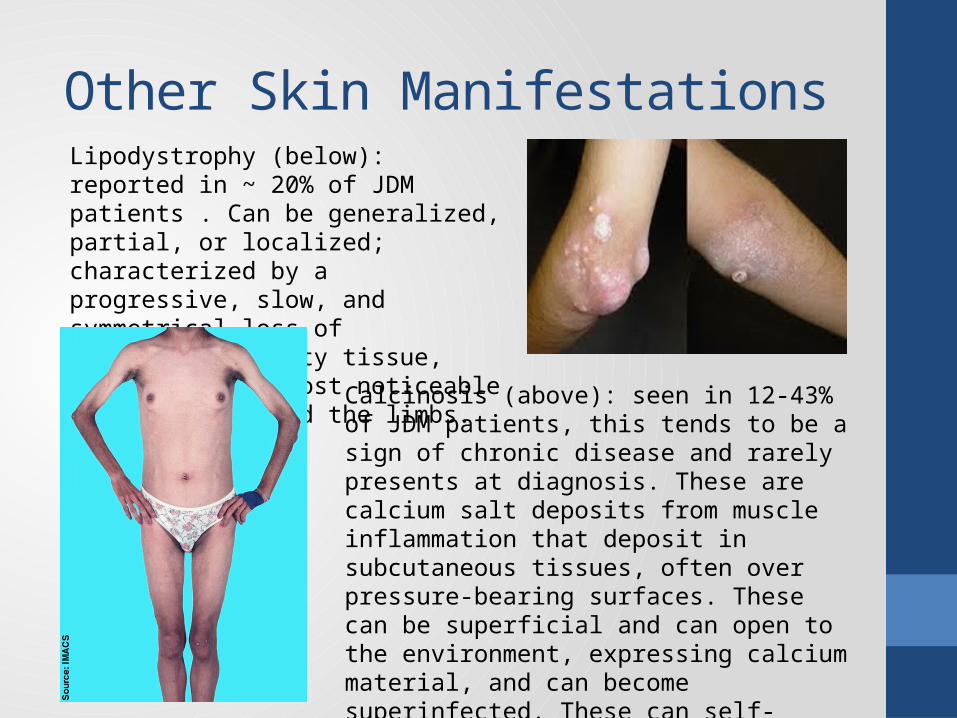
Other Skin ManifestationsLipodystrophy (below): reported in ~ 20% of JDM patients . Can be generalized, partial, or localized; characterized by a progressive, slow, and symmetrical loss of subcutaneous fatty tissue, which is often most noticeable over the face and the limbs.
Calcinosis (above): seen in 12-43% of JDM patients, this tends to be a sign of chronic disease and rarely presents at diagnosis. These are calcium salt deposits from muscle inflammation that deposit in subcutaneous tissues, often over pressure-bearing surfaces. These can be superficial and can open to the environment, expressing calcium material, and can become superinfected. These can self-resolve, lessen in size, or remain unchanged. Trauma can be associated with formation. If they occur over joints they can cause joint contractures.
Muscle Weakness
• Probably affects all muscle groups, but proximal > distal•Most obvious in limb-girdle, neck flexors, and trunk
muscles•May be tender, edematous, indurated• Respiratory weakness• In one report, ~ ¼ patients had involvement of
pharyngeal, hypopharyngeal, and palatal muscles• Difficulty swallowing, dysphonia, nasal speech, regurgitation
of liquids through nose• Aspiration risk
•May have Gowers’ or Trendelenberg’s sign
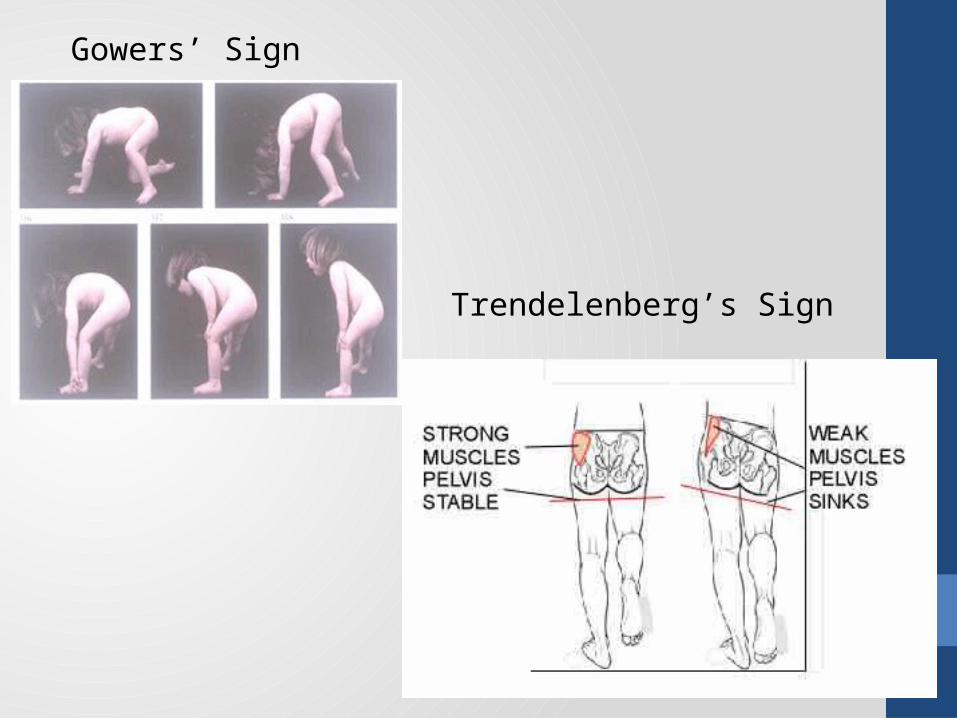
Gowers’ Sign
Trendelenberg’s Sign
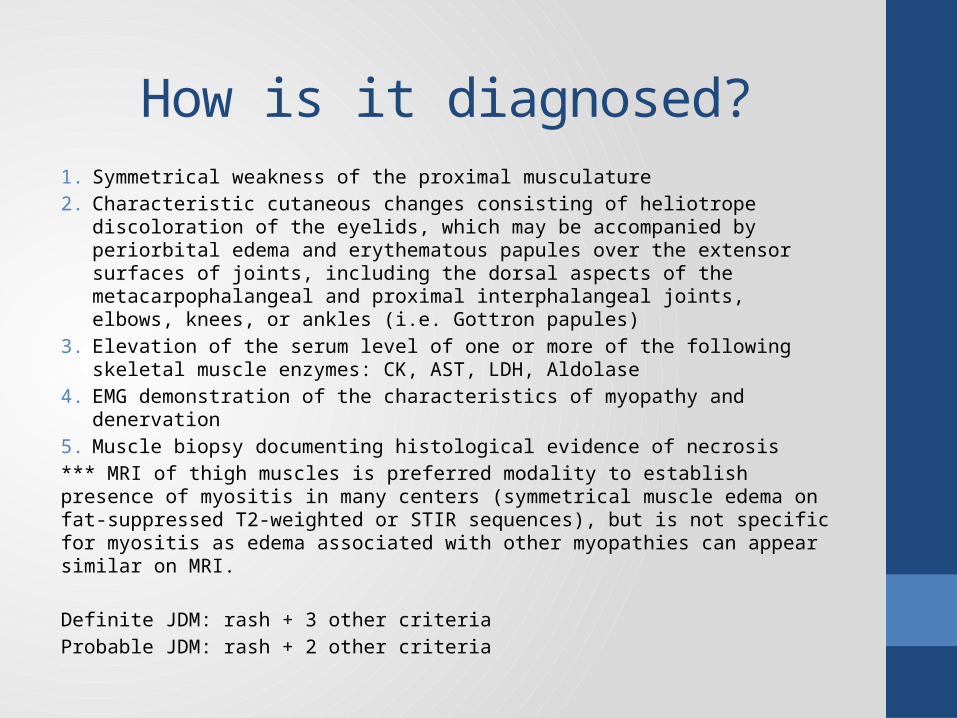
How is it diagnosed?1. Symmetrical weakness of the proximal musculature2. Characteristic cutaneous changes consisting of heliotrope discoloration of the
eyelids, which may be accompanied by periorbital edema and erythematous papules over the extensor surfaces of joints, including the dorsal aspects of the metacarpophalangeal and proximal interphalangeal joints, elbows, knees, or ankles (i.e. Gottron papules)
3. Elevation of the serum level of one or more of the following skeletal muscle enzymes: CK, AST, LDH, Aldolase
4. EMG demonstration of the characteristics of myopathy and denervation5. Muscle biopsy documenting histological evidence of necrosis*** MRI of thigh muscles is preferred modality to establish presence of myositis in many centers (symmetrical muscle edema on fat-suppressed T2-weighted or STIR sequences), but is not specific for myositis as edema associated with other myopathies can appear similar on MRI.
Definite JDM: rash + 3 other criteriaProbable JDM: rash + 2 other criteria

Revisiting the Criteria for JDM
•Although criteria used for JDM, sensitivity and specificity not validated in children (estimated 45-90% & 90%)• For JDM diagnosis, require rash and 2 of 4
other criteria for diagnosis•Most institutions don’t do EMG or biopsy if
diagnosis is clear.•MRI often being used in difficult cases, less
painful and invasive than EMG or biopsy

Typical Laboratory Findings:
• Elevated muscle enzymes: Creatinine Kinase, Aldolase, LDH, AST, ALT
• Elevated inflammatory markers: ESR, CRP• May have lymphopenia, but leukopenia and anemia are
uncommon at onset of disease• Positive ANA in ~ 70-80% of patients• Other autoantibodies commonly tested that might be positive in
JDM patients:• Anti-Jo1 – 2-5%• Anti-Ro (SSA) – 2-8%• Anti-La (SSB) – 1%• Anti-U1RNP – 5-6%
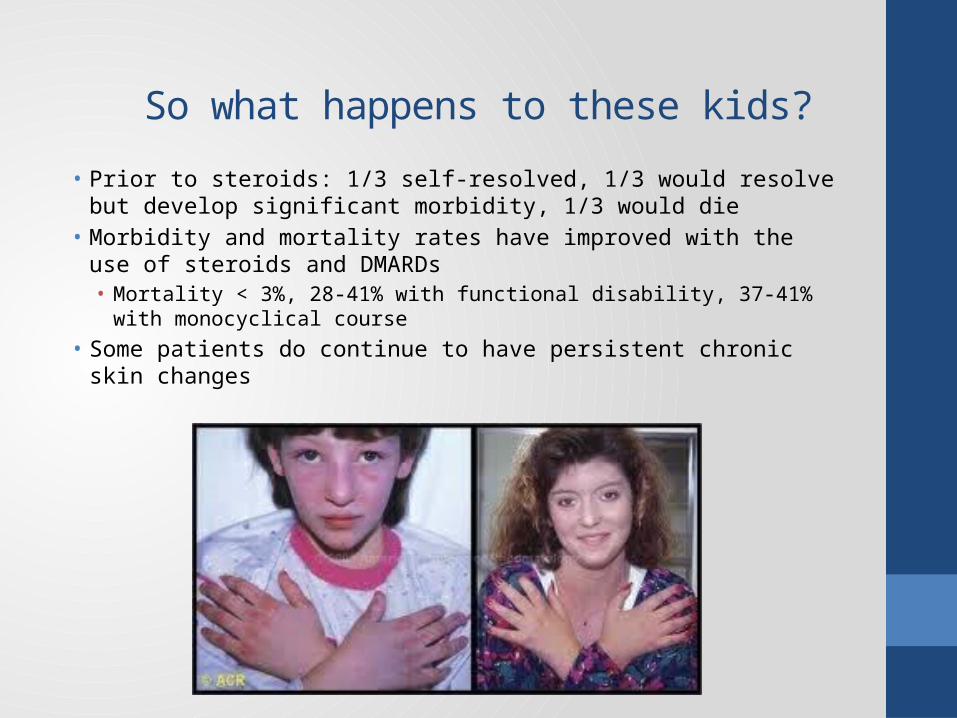
So what happens to these kids?• Prior to steroids: 1/3 self-resolved, 1/3 would resolve but develop
significant morbidity, 1/3 would die• Morbidity and mortality rates have improved with the use of
steroids and DMARDs• Mortality < 3%, 28-41% with functional disability, 37-41% with
monocyclical course• Some patients do continue to have persistent chronic skin changes
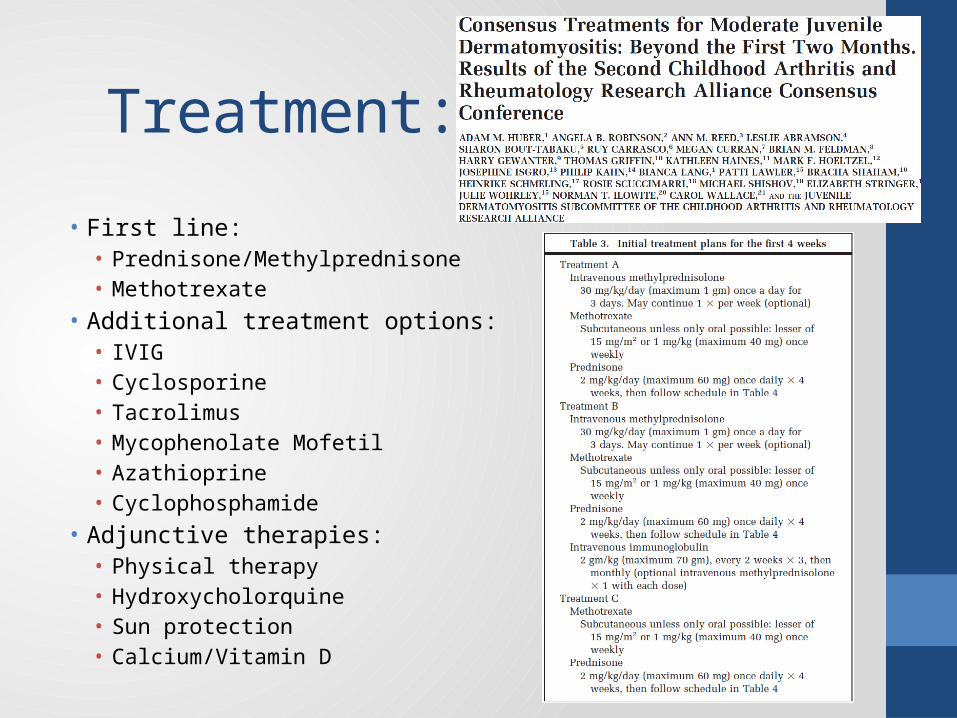
Treatment:
• First line:• Prednisone/Methylprednisone• Methotrexate
• Additional treatment options:• IVIG• Cyclosporine• Tacrolimus• Mycophenolate Mofetil• Azathioprine• Cyclophosphamide
• Adjunctive therapies:• Physical therapy• Hydroxycholorquine• Sun protection• Calcium/Vitamin D

Board Review Question
A 7 year old girl has a 2 month history of generalized weakness and a rash. Findings on exam include a violaceous discoloration of the malar regions, erythematous papules over the interphalangeal joints, and nailfold telangiectasias. Proximal muscle strength is 3/5.
Of the following, the MOST appropriate intial step in evaluating this patient’s symptoms is to obtain a(n):
a. antinuclear antibody titerb. creatine kinase concentrationc. electromyogramd. magnetic resonance image of musclee. muscle biopsy